






γλώσσες
Σελίδες
Νομικός


Δρ. Δημήτρης Π. Παπαδόπουλος-FESC
Υπεύθυνος Αντιυπερτασικού Ιατρείου
Καρδιολογικής Κλινικής Π.Γ.Ν.Α. «ΛΑΪΚΟ»
Clinical Assist. Professor George Washington University
Clinical Hypertension Specialist ESH``
Οι β-αποκλειστές αποτελούν
πρώτη θεραπευτική επιλογή για
την αρτηριακή υπέρταση?


0
20
40
60
80
100
120
140
160
180
0
20
40
60
80
100
120
140
160
180 Men
Women
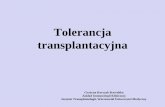
Number of People with Hypertension Aged 20 Years and Older
by World Region and Sex in 2000 and 2025
2000
2025
Nu
mb
er o
f p
eop
le w
ith
hy
per
ten
sio
n (
mil
lio
ns)
Establishedmarket
countries
Formersocialist
economies
India LatinAmericaand the
Caribbean
Middleeasterncrescent
China OtherAsia andislands
Sub-Saharian
Africa
Overall(developed +
developingcountries)
116.2123.3
40.652.5
60.4 57.8 60.054.3
35.9 37.9
98.5
83.1
38.433.0 38.2
41.6972 million
(333 + 639)
147.9
161.8
44.0
59.7
107.3106.2 102.1 98.5
72.280.4
151.7147.5
67.362.1
73.6 77.1
1.56 billion
Kearney et al Lancet 2005;365:217-23

TIA = transient ischemic attack; LVH = left ventricular hypertrophy; CHD = coronary heart disease;
HF = heart failure.
Cushman WC. J Clin Hypertens. 2003;5(Suppl):14-22.
Renal
failurePeripheral vascular
disease
Complications of Hypertension:
LVH, CHD,
HF
TIA, stroke
Hypertension
is a risk factor



• Η βξαβεπκέλε κε Nobel αλαθάιπςε ησλ β-
αλαζηνιέσλ ήηαλ έλαο από ηνύο ζξηάκβνπο
ηεο ζύγρξνλεο θαξκαθνινγίαο.
• Εθηνηε νη β-αλαζηνιείο έρνπλ θαζηεξσζεί ζαλ
αλαγθαία θαη απνηειεζκαηηθά θάξκαθα γηα
πνιιέο θαξδηαγγεηαθέο παζήζεηο, όπσο ε
ΑΤ, ε θαξδηαθή αλεπάξθεηα, ε ζηεθαληαία
λόζνο, ε πξόιεςε ηνπ αηθλίδηνπ ζάλαηνπ,
θαη δηάθνξεο αξξπζκίεο.


Καξδηαθή ζπρλόηεηα θαη
πξνζδόθηκν
δσήο
Καλόλαο:
3 ζπζηνιέο ιηγόηεξεο αλά ιεπηό
παξάηαζε δσήο θαηά 3 ρξόληα

GOALS OF ANTIHYPERTENSIVE
TREATMENT
BP reduction
Risk
Factors
HT
Prevention
TOD
regression/
prevention
NOD
PreventionESRDAF
PreventionCHD StrokeCHF Cognitive
Dysfunction
Dementia
LVH
IMT
Microalbuminaria
Arterial stiffness
Endotheliadysfunction
Cardiacfibrosis

BP Reduction and CV Events in LIFE
Dahlöf B et al Lancet 2002; 359: 995-1003
0 6 12 18 24 30 36 42 48 54
Study Month
40
50
60
70
80
90
100
110
120
130
140
150
160
170
180
Systolic
Diastolic
Mean Arterial
mmHg
Atenolol 145.4 mmHg*
Losartan 144.1 mmHg*
Atenolol 80.9 mmHg*
Losartan 81.3 mmHg*
* Mean BP at last visit
Atenolol 102.4 mmHg*
Losartan 102.2 mmHg*
0
2
4
6
8
10
12
14
16
Pro
po
rtio
n o
f p
ati
ents
wit
h f
irst
even
t (%
)
Composite of CV death, stroke and MI
Losartan
Atenolol
Study Month
0 6 12 18 24 30 36 42 48 54 60 66
Losartan 4605 4524 4460 4392 4312 4247 4189 4112 4047 3897 1889 901Atenolol 4588 4494 4414 4349 4289 4205 4135 4066 3992 3821 1854 876
Adjusted Risk Reduction 13.0%, p=0.021
Unadjusted Risk Reduction 14.6%, p=0.009
Number
at Risk
BP

Ακινδηπίλε ± Πεξηλδνπξίιε
vs.
β-απνθιεηζηή ± Γηνπξεηηθό

Ακινδηπίλε 5-10 mg Αηελνιόιε 50-100 mg
Πεξηλδνπξίιε 4-8 mgBFZ-K
1.25-2.5 mg
Δνμαδνζίλε GITS 4-8 mg
+
+ +
Άιια θάξκαθα π.ρ. κνμνληδίλε/ζπηξνλνιαθηόλε
+
Αλγόριθμος μείωζης ηης ΑΠΑλγόριθμος μείωζης ηης ΑΠ << 140/90 140/90
mmmm HgHg ή <130/80ή <130/80 mmmm HgHg ζε ζε
διαβηηικούς αζθενείςδιαβηηικούς αζθενείς
DahlDahlööf B et alf B et al. Lancet. 2005;366:895. Lancet. 2005;366:895--906. 906.

-14%
-10%
-16%
-14%
-12%
-10%
-8%
-6%
-4%
-2%
0%
ALL CAUSE MORTALITY PRIMARY END POINT
ASCOT: Preliminary results
p=0,005
p=0,12
REASON FOR STOPPING THE
TRIAL

ASCOT Trial: Endpoints for amlodipine and perindopril
versus atenolol and thiazide
-13%
-16%
-24%
-16%
-34%
-29%
-24%
-19%
-14%
-9%
-4%
-13%-11%
-23%
Total
coronary
endpoint
Non-fatal myocardial
infarction
(excluding silent)
and fatal coronary
heart disease
Total
cardiovascular
events and
proceduresAll-cause
mortality
Cardiovascular
mortality
Fatal and
non-fatal
heart failure
Fatal and
non-fatal
stroke

Beta-Blockers in Hypertension - Disadvantages
Dysmetabolic effects
Protection against subclinical organ
damage
Side effects
Less central BP reduction?
Less prevention of stroke?
Less BP reduction / CVD protection in the
elderly?

Potential Adverse Metabolic Effects
of β-blockers
Insulin-resistance
P-insulin levels
P-glucose levels
LDL/HDL
Triglycerides

Antihypertensive Treatments and Incidence of New Onset Diabetes
Lancet 1999;353:611-16. Lancet 2003;362:759-66. JAMA 2003;290:2805-2816. Lancet 2000;356:366-72. Lancet 2002;359:995-1003. JAMA 2002;288:2981-97. N Engl J Med 2000;342:145-53. J Hypertension 2003;21:1563-1574.
Study% Higher Incidence in Patients Using
Diuretics, b-Blockers
CAPPP diuretics, b-blockers 13% vs. captopril
CHARM placebo ± SOC 16% vs. candesartan ± SOC
INVESTatenolol ± HCTZ or trandolapril
17%vs. atenolol ± HCTZ or trandolapril
INSIGHT co-amiloride ± b-blocker 30% vs. nifedipine GITS
LIFE atenolol 33% vs. losartan
ALLHAT chlorthalidone18%
43%
vs. amlodipine
vs. lisinopril
HOPE placebo ± SOC 50% vs. ramipril ± SOC
ALPINE HCTZ ± atenolol 720%vs. candesartan ± felodipine

From Elliott WJ, Lancet 2007; 369: 201
Results of a Meta-analysis for Incident Diabetes -
Twenty-two Clinical Trials of 143,153 Hypertensive Patients
ARB
ACE inhibitor
CCB
Placebo
Beta-blocker
Diuretic
0.57 (0.46-0.72) p < 0.0001
0.67 (0.56-0.80) p < 0.0001
0.75 (0.62-0.90) p = 0.002
0.77 (0.63-0.94) p = 0.009
0.90 (0.75-1.09) p = 0.30
Referent
50 70 90 126
Odds ratio of incident diabetes Incoherence = 0.000017


ύκθσλα κε ηηο λέεο επξσπατθέο νδεγίεο:
►Οη β-αλαζηνιείο εμαθνινπζνύλ λα απνηεινύλ κία από ηηο πξώηεο επηινγέο ηνπ ηαηξνύ ηόζν γηα έλαξμε όζν θαη γηα ζπλέρηζε ηεο ζεξαπείαο
►Επεηδή νη β-αλαζηνιείο έρνπλ αξλεηηθή επίδξαζε ζε ζεκαληηθέο κεηαβνιηθέο παξακέηξνπο, δελ πξέπεη λα πξνηηκνύληαη ζε ππεξηαζηθνύο κε κεηαβνιηθό ζύλδξνκν ή ηα επηκέξνπο πξνβιήκαηα απηνύ
2007 Guidelines for the Management of Arterial Hypertension:
European Heart Journal, June 11, 2007

►Αυτό μπορεί να μην ισχύει για τους
αγγειοδιασταλτικούς β-αναστολείς, όπως
η καρβεδιλόλη και η νεμπιβολόλη, οι
οποίοι έχουν λιγότερη ή καθόλου
δυσμενή επίπτωση στις μεταβολικές
παραμέτρους και εμφανίζουν λιγότερα
περιστατικά νέου διαβήτη συγκριτικά με
τους κλασικούς β-αναστολείς
2007 Guidelines for the Management of Arterial Hypertension:
European Heart Journal, June 11, 2007

Propranolol
Metoprolol
Atenolol
Pindolol
Carvedilol
Percentage change (%)
20-20-40 0-10-30 10
Jacob S et al. Am J Hypertens 1998
Effects of b Blockers on Insulin Sensitivity
Nebivolol

Επίδραζη ζε μεηαβολικές παραμέηροσς
-30
-20
-10
0
10
20
30
carvedilol
atenolol
metoprolol
Εσαιζθηζία ζηην
ινζοσλίνηΤριγλσκερίδια HDL
+13%
-22% -21%
0%
+18%
+30%
0%
-9% -7%
Jacob S et al, Am J Hypertens 1998;11:1258-65

Επηβεβαίσζε : Μειέηε
GEMINI
► Καξβεδηιόιε – Μεηνπξνιόιε
► 1235 αζζελείο
► Δηαβεηηθνί ηύπνπ 2, Τπεξηαζηθνί
► ΑΠ>130mmHg, ΔΑΠ>80mmHg)
► ε ΑΜΕΑ / ΑΣ-Ι
► ηαζεξνπνηεκέλε αληηδηαβεηηθή ζεξαπεία
γηα 3 κήλεο
► ηαζεξνπνηεκέλε αληηππεξηαζηθή
ζεξαπεία γηα 1 κήλα
Bakris G et al. JAMA 2004;292:2227-2236

Αξηεξηαθή Πίεζε : θαξβεδηιόιε + ΑΜΕΑ/ΑΣ-Ι
87
131.3
77.1
149.4
-40
10
60
110
160
ΑΠ ΔΑΠ
Έλαξμε
Μήλαο 5
(n=454) (n=454)
Bakris G et al. JAMA 2004;292:2227-2236
GEMINI
mmHg

Αληίζηαζε ζηελ ηλζνπιίλε
5.6
5.7
5.8
5.9
6
6.1
6.2
6.3
Καξβεδηιόιε Μεηνπξνιόιε
Έλαξμε
Μήλαο 5
p=0,004
p=0,48
p=0,004
↑↑
(n=371) (n=540)
Bakris G et al. JAMA 2004;292:2227-2236
GEMINI
HOMA-IR

Μεηαβνιή ζηε γιπθνδπιησκέλε αηκνζθαηξίλε
7
7.1
7.2
7.3
7.4
7.5
Καξβεδηιόιε Μεηνπξνιόιε
Έλαξμε
Μήλαο 5
p=0,65
p<0,001
p=0,004
Μέζ
ε H
bA
1c
(%
)
↑
(n=454) (n=657)
Bakris G et al. JAMA 2004;292:2227-2236
GEMINI

Change in Insulin and HOMA Index Induced by Nebivolol and Metoprolol
after 24 Wks in HTN
Insulin κU/ml
0
2
4
6
8
10
12
* p< 0.006
Nebivolol
16
18
14
Placebo Placebo Metoprolol
HOMA index
0
1
2
* p< 0.008
Nebivolol
4
3
Placebo Placebo Metoprolol
Celik et al. J Hypertens 2006

Changes in Lipids Induced by Nebivolol and Metoprolol after 24 Wks in HTN
-4.6
-20
-15
-10
-5
0
5
10
15
20
-2.4
-10.1
-2.7
-11.5
+8.7
-2.0
+16.3
TC LDL-C LDL-C/HDL-C TG
Nebivolol (5 mg)
Atenolol (50 mg)
Pesant et al. Amer J Therap 1999
%

Reappraisal of European Guidelines on Hypertension Management:
an ESH Task Force Document
Journal of Hypertension 2009
…when discussing β-blockers, however, it should not be
ignored that they are no homogeneous class, and that
vasodilating β-blockers such as carvedilol and nebivolol
appear not to share some of the negative properties
described for other compounds

Beta-Blockers in Hypertension - Disadvantages
15805 M
Dysmetabolic effects
Protection against subclinical organ
damage
Side effects
Less central BP reduction?
Less prevention of stroke?
Less BP reduction / CVD protection in the
elderly?

Η ΠΡΟΛΗΦΗ ΣΗ ΒΛΑΒΗ ΣΧΝ ΟΡΓΑΝΧΝΣΟΥΧΝ ΑΠΟΣΕΛΕΙ ΕΠΙΠΡΟΘΕΣΟΜΕΛΗΜΑ / ΚΟΠΟ ΠΕΡΑΝ ΣΗ ΡΤΘΜΙΗΣΗ ΑΠ, ΓΙΑ ΣΗ ΒΕΛΣΙΧΗ ΣΗΠΡΟΓΝΧΗ ΣΧΝ ΑΘΕΝΧΝ
B. Dahlof Eur H J 2003;5:SF(F33-F39).

“Specific” Protective Effects of Antihypertensive Drugs
on Subclinical Organ Damage
Diuretics
Beta-
blockers
CCB
ACEI
ARB
Arterial thickening /
Atherosclerosis
Endothelial
dysfunction
Arterial stiffening
Coronary Ca++
depletion
Arteriolar remodelling
Diastolic
dysfunction?
Cognitive
dysfunction /
Dementia
LVH
Nephroprotection
MA / Proteinuria
Mancia G, 2006

Proportion of patients
with first event (%)
0
2
4
6
8
10
12
14
16
0 6 12 18 24 30 36 42 48 54 60 66
Adjusted Risk Reduction:
13.0%, p = 0.021
Time (months)
Change from baseline (%)
in LVH determined by electrocardiography
-18
-16
-14
-12
-10
-8
-6
-4
-2
0
p < 0.0001
p < 0.0001
4.4%
10.2%
15.3%
9.0%
Atenolol
Losartan
Dahlöf B et al. Lancet 2002;359:995–1003.
LIFE: Παπόμοια μείωζη ΑΠ Τποζηποθή
ΤΑΚ
Atenolol
Losartan
CornellVoltage-Duration
Product
Sokolow-LyonVoltage
Composite of CV Death, stroke and MI

Μετα-ανάλσση μελετών σποστρουής ΥΑΚ στην σπέρταση
Schmieder RE et al. Am J Med 2003; 115:41-6.
-16
-14
-12
-10
-8
-6
-4
-2
0Diuretics b-blockers
Ca-antagonist
ACE-inhibitors ARBs
-8%
-6%
-11%-10%
-13%
LV massreduction
(%)
80 Μελέηερ;4,113 αζθενείρ

Έζσ θαξσηίδα (IC)Έμσ θαξσηίδα (EC)
Δέξκα
Κνληηλό
ηνίρσκα
Μαθξηλό
ηνίρσκα
1.0 cm
0.5-1.0 cm
1.0 cm
CBMmax
Μέζνο όξνο ηνπ κέγηζηνπ
IMT από 4 καθξηλά
ηνηρώκαηα (+ 4 θνληηλά
ηνηρώκαηα)
ζε CC θαη Bif,
ακθνηεξόπιεπξα
Δηραζκόο (Bif)
Κνηλή
θαξσηίδα (CC)
Ορισμός του πάχους του έσω –μεσου
χιτωνα (ΙΜΤ)

Μειέηε
PREVENT
PART-2
SECURE
BCAPS
MIDAS ns
VHAS ns
INSIGHT
DAPHNE
ELSA
Αζζέλεηα
CHD
VD
Υς.Κίλδ.
VD
HT
HT
HT
HT
HT
Θεξαπεπηηθέο αγσγέο
Ακινδηπίλε έλαληη Placebo
Ρακηπξίιε έλαληη Placebo
Ρακηπξίιε έλαληη Placebo
Μεηνπξνιόιε έλαληη Placebo
Ιζξαδηπίλε έλαληη HCTZ
Βεξαπακίιε έλαληη
Χισξνζαιηδόλεο
Νηθεδηπίλε GITS έλαληη
Cν-Ακηινδίδεο
Γνμαδνζίλε έλαληη HCTZ
Λαζηδηπηλε - Αηελνινιε
Μέηξεζε
IMT
Mmax
CC-IMT
Mmax
Bif
Mmax
Mmax
CC-IMT
C + Fem
IMT-CBM
Αζζελείο
(n)
373
617
732
793
833
498
324
80
2255
Πξόζθαηεο Μειέηεο Αληηππεξηαζηθώλ Παξαγόλησλ ζην Καξσηηδηθό IMT

Beta-blockers in Patients with Intermittent Claudication and Arterial Hypertension:
Results from the Nebivolol or Metoprolol in Arterial Occlusive Disease Trial
Espinola-Klein C et al. Hypertension 2011; June ahead print
Results:
After a 48-week treatment period, ABI and absolute
claudiacation distance improved significantly in both
groups (p<0.05 for both)
A significant increase 39% of initial claudication distance
was found in Nebivolol group (p< 0.003)
vs 16.6% in Metoprolol group (p: NS)

Nebivolol but not Atenolol Reduces
Arterial Stiffness
McEniery, et al. Hypertension 2004;44:305
3.0
3.3
3.7
4.0
Atenolol
* p<0.05 vs baseline
Nebivolol
** p<0.01 vs baseline
n=12
3.1
3.2
3.4
3.5
3.6
3.8
3.9 *
Saline 250 500
Dose (nmol/min)
**
PW
V (
m/s
ec)

BB and Subclinical Organ Damage
ESH Task Force Document, J Hypertens 2009
Increased LVM
Carotid IMT thickening
Aortic stiffness
Increased small artery wall/lumen ratio
“…BBs have been shown to be less powerful than other agents
in studies using subclinical organ damage as an endpoint”

Beta-Blockers in Hypertension - Disadvantages
Dysmetabolic effects
Protection against subclinical organ
damage
Side effects
Less central BP reduction?
Less prevention of stroke?
Less BP reduction / CVD protection in the
elderly?

CAFÉ Study Circulation 2006
Differential Effect of β-bl/D and
ACE-I/CCB’s On BP in ASCOT

Beta-Blockers in Hypertension - Disadvantages
Dysmetabolic effects
Protection against subclinical organ
damage
Side effects
Less central BP reduction?
Less prevention of stroke?
Less BP reduction / CVD protection in the
elderly?

Beta-blockers (BB) and Withdrawal from Side Effects -
Data from 15 Placebo-controlled Trials (n > 35000)
12512 M Ko DT et al., JAMA 2002; 288: 351
0
1
2
3
Placebo
BB
%
Depression Fatigue Sexual dysfunction
0.94
(0.44-2.01)
2.63
(1.16-5.94)
4.89
(2.98-8.03)
RR
0.50.4
0.5
2.4
1.3
0.3


Cumulative Incidence of Discontinuation of Initial Antihypertensive Monotherapy
over 1 Year (Lombardia Data-base; n = 445356)
0.
5
1.
0
2.
0
Diuretics
Beta-blockers
Alpha-blockers
Calcium channel blockers
ACE-inhibitors
Angiotensin-receptorblockers
1.83 (1.81-1.85)
1.64 (1.62-1.67)
1.23 (1.20-1.27)
1.08 (1.06-1.09)
0.92 (0.90-0.94)
- +
Corrao, Zambon, Parodi, Poluzzi, Baldi, Merlino, Cesana, Mancia, J Hypert 2008; 26: 819-824

Beta-Blockers in Hypertension - Disadvantages
Dysmetabolic effects
Protection against subclinical organ
damage
Side effects
Less central BP reduction?
Less prevention of stroke?
Less BP reduction / CVD protection in the
elderly?

Diuretic b-Blocker Placebo
Total stroke 7.3* 9.0 10.8
Total coronary heart disease 7.7* 12.8 12.7
Total cardiovascular disease 17.4* 24.6 25.2
Total mortality 21.3 26.4 24.7
* significantly better than placebo
MEDICAL RESEARCH COUNCIL TRIAL (MRC)
Treating Elderly with Diuretic and Beta Blockers Is Beneficial(1992)
MRC Working Party. Br Med J 1992; 304:405


Beta-Blockers in Hypertension - Disadvantages
Dysmetabolic effects
Protection against subclinical organ
damage
Side effects
Less central BP reduction?
Less prevention of stroke?
Less BP reduction / CVD protection in the
elderly?

13 ηςσαιοποιημένερ μελέηερ (n=105.591) :
β- blockers vs other antihypertensive
7 ηςσαιοποιημένερ μελέηερ (n=27.433) :
β - blockers vs placebo
Aνάλςζη έγινε για όλοςρ ηοςρ β αναζηολείρ και για 3 ςποομάδερ αςηών:
> non atenolol b-blockers
> Mixed b-blockers and diuretics (>50% of pts started on a b blocker)
Atenolol
Eξεηάζθηκε η επίδπαζη ζε ΑΕΕ, ΕΜ, θνηηόηηηα όλων ηων αιηιών
The Lancet Vol 366 October 29
2005


Reappraisal of European Guidelines on Hypertension Management
A European Society of Hypertension (ESH) Task Force Document
ESH Task Force:
G. Mancia, Co-Chairperson (Italy), S. Laurent, Co-Chairperson (France),
E. Agabiti-Rosei (Italy), E. Ambrosioni (Italy), M. Burnier (Switzerland),
R. Cifkova (Czech Republic), D. Clement (Belgium), A. Coca (Spain),
A. Dominiczak (UK), S. Erdine (Turkey), R. Fagard (Belgium), C. Farsang (Hungary), G.
Grassi (Italy), SE. Kjeldsen (Norway), W. Kiowski (Switzerland),
A. Manolis (Greece), K. Narkiewicz (Poland), P. Nilsson (Sweden), M. Olsen
(Denmark), J. Redón (Spain), J. Rodicio (Spain), L. Ruilope (Spain), RE. Schmieder
(Germany), HAJ. Struijker-Boudier (The Netherlands), P. van Zwieten (The Netherlands),
Mancia G. et al., J Hypert, Nov 2009
M. Viigimaa (Estonia), A. Zanchetti (Italy)

< 140 / 90 if low and moderate CV risk
< 130 / 80 if high CV risk
Diabetes
Renal dysfunction
Established CV disease
2007 ESH Guidelines for the Management of Hypertension.
J of hypertension 2009;27:2121–58
2007 Blood pressure targets

2003 ESH/ESC Guidelines
Evidence of CV protection with 5 drug classes
- Diuretics
- Beta-blockers
- ACE-inhibitors
- Calcium channel blockers
- Angiotensin II antagonists
All above classes suitable for initiation / maintenance of
antihypertensive treatment
Effective BP fundamental

2009 ESH/ESC Guidelines
Combinations between Some Classes of Antihypertensive Drugs
Thiazide diuretics
ACE inhibitors
Calcium
antagonists
ß-
blockers
AT1-
receptor
antagonists
α-blockers
Thiazide diuretics
ACE inhibitors
Calcium
antagonists
AT1-
receptor
antagonists
• Pronounced antihypertensive
effect
• CV protection
• Optimal tolerability
ACCOMPLISH
ADVANCE
HYVET
ASCOT
ONTARGET

Beta blockers are still first line
therapy in arterial hypertension???
Yes for individual patients and
vasodilatory agents
Top Related