Violet 405 nm light: A novel therapeutic agent against β … · Violet 405nm Light: A Novel...
-
Upload
trinhnguyet -
Category
Documents
-
view
213 -
download
1
Transcript of Violet 405 nm light: A novel therapeutic agent against β … · Violet 405nm Light: A Novel...
-
Lasers in Surgery and Medicine
Violet 405nm Light: A Novel Therapeutic Agent Againstb-Lactam-Resistant Escherichia coli
Nathaniel L.R. Rhodes, MS,1 Martin de la Presa, BA,2 Mitchell D. Barneck, BS,3 Ahrash Poursaid, BS,1
Matthew A. Firpo, PhD,2 and John T. Langell, MD, PhD, MBA1,21Department of Bioengineering, University of Utah, Salt Lake City, Utah 841122Department of General Surgery, University of Utah, Salt Lake City, Utah 841323School of Medicine, Oregon Health and Sciences University, Portland, Oregon 97239
Background and Objective: Approximately 1.7 millionpatients are affected by hospital-acquired infections everyyear in the United States. The increasing prevalence ofmultidrug-resistant bacteria associated with these infec-tions prompts the investigation of alternative sterilizationand antibacterial therapies. One method currently underinvestigation is the antibacterial properties of visible light.This study examines the effect of a visible light therapy(VLT) on b-lactam-resistant Escherichia coli, a commonnon-skin flora pathogen responsible for a large percentageof indwelling medical device-associated clinical infection.Materials and Methods: 405nm light-emitting diodeswere used to treat varying concentrations of a commonlaboratory E. coli K-12 strain transformed with the pCIGmammalian expression vector. This conferred ampicillinresistance via expression of the b-lactamase gene. Bacteriawere grown on sterile polystyrene Petri dishes plated withLuria-Bertani broth. Images of bacterial growth colonies onplates were processed and analyzed using ImageJ. Irradi-ance levels between 2.89 0.19 and 9.45 0.63mW cm2and radiant exposure levels between 5.60 0.39 and136.91 4.06 J cm2 were tested.Results: VLT with variable irradiance and constanttreatment time (120 minutes) demonstrated significantreduction (P< 0.001) in E. coli between an irradiance of2.89mW cm2 (81.70%) and 9.37mW cm2 (100.00%).Similar results were found with variable treatment timewith constant irradiance. Log10 reduction analysis pro-duced between 1.98 0.53 (60 minute treatment) and6.270.54 (250 minute treatment) log10 reduction inbacterial concentration (P
-
treatments are not always appropriate to stop HAIs andmore effective methods of sterilization should be imple-mented. Medical device manufacturers have attempted tosolve the issue of hardware-associated infections throughseveral novel approaches including coating at-risk surfaceswith bactericidal and bacteriostatic agents such as chlor-hexidine or silver compounds. These coatings are intendedto inhibit bacterial and fungal colonization of the device.
Unfortunately, these solutions have hadminimal efficacyin the clinical setting in reducing device-associatedinfections [6,7]. Given the magnitude of the problem ofindwelling medical device-associated infections, more effi-cacious solutionsmust be found. One novel approach underinvestigation is harnessing the potential of visible lighttherapy (VLT). VLT has shown substantial antimicrobialefficacy against pathogenic bacteria and has receivedclearance for clinical application for acne treatment bytheUnited States Food andDrugAdministration (FDA) [8].In addition, bacterial resistance to VLT has not beenobserved. This is thought to be due to a differentantimicrobial mechanism, compared to traditional phar-maceutical antibiotics, which avoids the method in whichbacteria become drug-resistant [9,10]. The most commonlyused classes of antibacterial drugs target cell wall biosyn-thesis, protein synthesis, or DNA replication and repair.However, once an antibiotic is introduced clinically, it willonly have a period of months to years until a statisticallysignificant efficacy reduction appears [11]. The mostcommon methods of antibiotic resistance seen in bacteriaare: chemical or enzymatic modification of the drug,transmembrane pumps which reduce intracellular drugconcentrations below therapeutic levels, and bacterialtarget structuremodification resulting in a reduced affinityfor the drug [10].
Althoughothershavedemonstratedthebactericidalefficacyof 405nm light on thedrug resistantGram-positive bacteriummethicillin-resistant S. aureus (MRSA) and non-resistantGram-negative bacteria, few studies have investigated itsefficacy against common drug-esistant Gram-negative organ-isms [1219]. In particular, Escherichia coli are Gram-negative bacilli commonly present in the gastrointestinaltract of humans. According to the United States Center forDisease Control, E.coli is one of the most common pathogensthat cause nosocomial infections in addition to S. aureus andPseudomonas aeruginosa [20]. Wavelength specific VLTagainst the spectrum of pathogens responsible for indwellingdevice-associate clinical infections may offer a novel, cost-effective, and sustainable agent against these life-threateninginfections. In this studywe explore the efficacy of 405nmVLTagainst E. coli, one of the most common isolates of HAIs andindwelling medical device-associated infections [21,22].
MATERIALS AND METHODS
Bacteria Preparation
The common laboratoryE. coliK-12 strain (fhuA2 lac(del)U169 phoA glnV44 F80 lacZ(del)M15 gyrA96 recA1 relA1endA1thi-1hsdR17) transformedwith thepCIGmammalianexpression vector was used for all experiments. The pCIG
plasmid confers ampicillin resistance to theE. coli strain viaexpression of the b-lactamase gene. The pCIG plasmid alsoconferred expression of green fluorescent protein, which wasused to verify strain selection. Sterile polystyrene10015mm2 Petri dishes were plated with Luria-Bertani(LB) broth (Lennox L3022). LB selective media contained0.1mg/ml ampicillin in all experiments. For consistency incounting colony forming units (CFUs) between experiments,dilution series were made from cultures inoculated with 34well-separated bacterial colonies and grown to saturation.Serial dilutions were prepared by taking 0.5ml of thesaturated bacterial solution and adding it to 4.5ml of theLB broth stock solution. Time and power trial plates werediluted in this fashion by a factor of 105 for each control andtreated plates. Log10 reductionplateswere diluted by a factorof 105 for control and between 101 and 103 for treated. Eachplate was seeded with 200ml aliquots and the liquid wasspreaduntil uniformlydistributed.Optimal platingdensitieswere determined in pilot experiments in order to yield 1015CFUscm2.
Experimental Setup
The 405nm light-emitting diodes (LEDs) were selected(Bivar#:UV5TZ-405-15) andwavelengthwasverifiedusinga visible light spectrometer (OceanOpticsUSB2000). LEDshad a peak wavelength at 404.63nm 1.74 and had aspectrum of 16.57nm 0.89 at 50% relative peak intensity.NineLEDswerewired inaparallel circuit andarranged ina3 3 grid pattern. This setup was placed onto a traycustomized for an incubator. Custom partitions werecreated to ensure no light transferred between treatmentareas (Supplementary Fig. S1).Light intensity from the LEDs were measured to
determine overall output power using a digital powermeter (PM100USB, Thorlabs, Newton, NJ) and sensor(S140C, Thorlabs, Newton, NJ). Diode intensity wasmeasured pre- and post-treatment to determine irradi-ance. Untreated and treated (exposure to 405nm light)areas within the same plate were measured for CFUs inorder to control for potential plate-to-plate differences inbacterial plating densities. A flexible opaque polyethylenesleevewas placed to cover half of the plate. The other half ofthe plate was left unobstructed and light sources wereplaced approximately 3.75 cm above the surface of theplate. Circular areas on both the control and treated sideswith a radius of 1.02 cmweremarked on the plate and usedto focus the light in a treated area. All measurements ofCFUs were done with respect to bacteria inside this1.02 cm radius circle. Radiant exposure levels are definedas the intensity of light in an area for a certain amount of
time giving it units of mWseccm2 orJ
cm2. Varying power levels of
light intensity as well as irradiation time led to severaldifferent radiant exposure levels tested.
Bacterial Growth Analysis
After 24 hours of growth, high-resolution images weretaken of each plate using a digital 18-megapixel camera(Canon T2i DLSR). The camera was mounted on a stand
2 RHODES ET AL.
-
with the lens 61 cm from the plate surface. Images wereprocessed and analyzed using ImageJ (National Insti-tute of Health). Supplementary Figure S2 shows variousstages of image processing including a whole Petri dishphotograph, a binary image, and individual colony countoutlines. Individual colonies were selected based on asize and circularity protocol. Size was determined bypixel count. A range of 2004000 pixel was determinedbased on the average isolated colony size [2]. Acircularity value range of 0.21.0 was selected. A valueof 1.0 indicates a perfect circle, whereas a valueapproaching 0.0 indicates an increasingly elongatedpolygon.The resulting CFUs counted at different radiant
exposures were plotted as survival fraction versusradiant exposure. The survival fraction values weregenerated based on a log10 normalization of the resultingCFUs.
Statistical Analysis
Continuous data of individual survival fractions weredefined as the quantity of colony forming units normal-ized by taking log10 of said value in treated and untreatedcontrol groups. Differences in continuous data wereassessed using a Wilcoxon signed-rank test using JMPsoftware (SAS, Cary, NC). Data was binned based onvariable component in each experimental setup. Forexample, in time variable testing, data groups werebinned by time, in log10 reduction testing, groups werebinned based on concentration and time. Differences inbinned data were assessed using a paired t-test usingMicrosoft Excel 2013. A P-value of less than 0.05 was setas the a priori level of significance.
RESULTS
Variable Irradiance With Constant Exposure TimeAnalysis
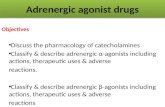
The bactericidal effect of the 405nm light on ampicillin-resistant bacteria was first determined using light ofvarying irradiance. Irradiance was modulated by control-ling the voltage and current applied to each diodedetermined as a percentage based on the manufacturerssuggested forward voltage and current (3.4 volts, 30mA).The values were 25%, 50%, 75%, and 100% of this voltage,which produced 9.43 0.72, 16.05 0.79, 26.15 2.30, and30.30 1.25 volts across each diode, respectively. Figure 1shows the results for the exposure of ampicillin-resistantE. coli to 405nm light delivered at increasing lightirradiance and with time being held constant at 120minutes. There was a significant reduction in E. colistarting at an irradiance of 2.89mWcm2 resulting in an81.70% reduction in bacterial growth (P< 0.001). Eachsubsequent increase in irradiance yielded a statisticallysignificant bacterial reduction (P< 0.001). Maximum bac-terial eradication (100.00%) was observed after an irradi-ance of 9.37mWcm2 for 120 minutes (65.90J cm2) wasapplied (P< 0.001). Table 1 lists the bacterial countsobserved at each treatment intensity.
Variable Exposure Time With Constant IrradianceAnalysis
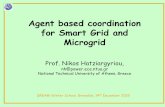
The antimicrobial effect of 405 nm light was alsodetermined by varying irradiation time. Voltage andcurrent levels of each diode were held at the manufac-turers suggested values (3.4 volts and 30mA, respec-tively). The average irradiation during the time protocolswas 9.24 0.44mWcm2. Figure 2 depicts the results forthe exposure of E. coli to 405nm light delivered atincreasing duration of time with irradiance being heldconstant. There was a significant reduction (P0.030,P
-
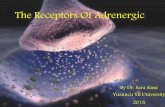
high confluent concentrations and irradiated with differ-ent exposure times (60, 120, and 250 minutes). Untreatedcontrol bacterial colony forming units averaged 2.16 0.17 103CFUs cm2, 2.12 0.16 104CFUs cm2, and1.56 0.13105CFUs cm2 for the 60, 120, and 250minute treatments, respectively. The resulting reductionsin bacterial concentration produced between 1.98 0.53(60 minute treatment) and 6.270.54 (250 minutetreatment) log10 reduction (Fig. 3). Statistically significantresults (P
-
An in vitro study by Maclean et al. demonstrated a 5 log10reduction of MRSA in a liquid suspension after irradiatingwith 630720J cm2 of >400nm light [32]. A followingstudy further showed that a 5 log10 reduction of MRSA canbe achieved with a significantly lower radiant exposure of45 J cm2 when light is delivered specifically at the 405nm
wavelength [13]. Another research study produced similarresults when irradiating both MRSA USA 300 and MRSAIS-853 at 55J cm2 with 405nm light, achieving areduction of 92.1% and 93.5%, respectively [16]. InGram-negative bacteria, Hamblin et al. tested VLT on astrain of H. pylori that was resistant to multipleantibiotics [19].
Though studies have demonstrated the use of violet lightto targetMRSAandH. pylori, data is lacking on the efficacyof 405nm light in the inactivation of b-lactam-resistantE. coli. b-lactam antibiotics act through inhibition ofbacterial cell wall biosynthesis. MRSA and other b-lactam-resistant bacteria produce b-lactamases that provideresistance to commonly used b-lactam antibiotics likepenicillin, cephamycin, and carbapenem. Hydrolysis ofthe b-lactam ring of the antibiotic will render itineffective [33].
This study has established the efficacy of using 405nmlight to inactivate a medically common drug-resistantbacterium. We have constructed dose-response curvesillustrating the irradiation necessary for the in vitroeradication of E. coli on plated growth media. Thisinformation may be useful for establishing the potentialfor clinical use. Due to the increasing numbers of HAIs andmedically relevant drug-resistant microbes, this technol-ogy could provide another option for the clinical treatmentof antibiotic-resistant bacterial infections.
Mechanism of Action
Although the antimicrobialmechanism of action of violetlight has not been completely elucidated, research over thepast decade has identified several critical areas of activity.It has been demonstrated that this process is oxygendependent. Studies have shown that bacteria exposed toviolet light under anaerobic conditions were able to resistthe phototoxic effects and that decreasing the amount ofreactive oxygen species (ROS) in an aerobic environmentalso reduced the phototoxic effect [34]. Conversely, othergroups have shown that increasing the amount of oxygensignificantly increased the rate of bacterial inactiva-tion [32]. It has also been demonstrated that violet lightillumination of endogenous porphyrins within bacteriaresults in their decreased proliferation [23]. Further,Hamblin et al. found that there is a strong positivecorrelation between amount of porphyrins contained
TABLE 2. Variable Treatment Time With Constant Irradiance
Irradiance
(mWcm2)Time
(minutes)
Radiant exposure
(J cm2)Treated
(CFU)
Control
(CFU)
Mean %
reduction P-values
9.32 0.51 10 05.590.31 18.947.71 27.42 13.42 26.40 0.0309.22 0.55 50 27.671.66 4.113.59 27.54 12.69 82.11
-
within bacteria and the cytotoxic effects of violet light [19].These studies support an oxygen dependent mechanismwhich allows violet light to excite endogenous porphyrinsto a high energy state. This energy is transferred to formROS that cause intracellular damage. Bacterial and fungalproteins, lipids, and nucleic acids are particularly suscep-tible to these ROS [35].
Themechanism of action of 405nmVLT is relevant whenassessing the potential for microbe resistance. Althoughresistance to 405nm light specifically has not beeninvestigated, the potential development of microbial resis-tance to photodynamic inactivation has been studied. Afterrepeated cycles of partial inactivation followed by regrowth,different bacterial species failed to develop resistance to thephotodynamic process after 10 and 20 cycles [36,37].
It is possible that due to the multifactorial mechanism ofaction viable bacteria are less likely or unable to develop aresistance toVLT.Further studies are necessary to determinethe extent to which bacteria are able to develop resistance.However, this study was able to illustrate that drug-resistantbacteria are susceptible to 405nm VLT. The significantbacterial toxicity demonstrated makes VLT a potentialalternative treatment for associated clinical infections.
Equivalent Radiant Exposure Dose
An in vitro study by Murdoch et al. showed significantdifferences in the bactericidal effect on Listeriamonocytogenes at equivalent radiant exposure levels butvarying irradiance and exposure time [18]. We performedsimilar preliminary testing on E. coli by reducing powerlevels and increased treatment time. The results supportedthe findings of Murdoch et al. in that we demonstrated asignificant reduction of bacteria in treatedplates evenat 25%power and fourfold longer treatment times. However, due tothe radiant exposure tested, both treatments in this studyresulted in a 100% reduction in bacterial CFUs. Because ofthis, we cannot ascertain if one method is more efficaciousthan the other given equivalent radiant exposure. Additionaltestingwill be performed in subsequent studies to determineefficacy trends at equivalent radiant exposure and varyingirradiance and time levels.
Log10 Reduction
This study has also established the potential log10reduction of 405nm light on drug-resistant E. coli. TheFDA requires that a minimum of a four-log10 reduction beachieved in order to be considered an antibacterial
solution [38]. In order to be considered for approval, theFDA recommends following ASTM E2315-03 StandardGuide for Assessment of Antimicrobial Activity Using aTime-Kill Procedure or an equivalent method.Using this ASTM protocol, we have demonstrated a
greater than 6 log10 reduction. This is 100 times thereduction necessary to be defined as bactericidal by theFDA. The results from this study also illustrate the timeand dose dependence of light technology. These resultssuggest that VLT using 405nm light could be a suitableclinical option for sterilization in drug-resistant species ofbacteria. The log10 reduction information provided mayhelp direct future applications of VLT in a clinical setting.
CONCLUSIONS
We, along with other researcher groups, have successfullydemonstrated a high efficacy at bacterial reduction usinghigh intensity 405nm light. Illustrating the efficacy of thistechnology against a b-lactam-resistant E. coli is especiallyrelevant given the great need for novel methods of steriliza-tion in healthcare settings. This information is also valuablein the context of the increasing occurrence of drug-resistantbacteria in HAIs and device-associated infections. Theincreasing incidence of these infections illustrate thatcurrent antimicrobial technologies are inadequate. Furtherresearch directives will focus on other common nosocomialinfection causing agents, such as P. aeruginosa, S. aureus,and other drug resistant bacteria.
ACKNOWLEDGMENTS
The authors would like to thank the University of Utahand Center forMedical Innovation who assisted in fundingthis research. The authors would like to thank theUniversity of Utah Department Of Surgery staff ElaineHillas, Patti Larrabee, and Dr. Jill Shay, as well as SamiBarneck and the microbiology laboratories at Weber StateUniversity. Also, they would like to thank the NationalInstitute of Health for allowing open access to ImageJ.
REFERENCES
1. Magill SS, Edwards JR, BambergW, Beldavs ZG, Dumyati G,Kainer MA, Lynfield R, Maloney M, McAllister-Hollod L,Nadle J, Ray SM, Thompson DL, Wilson LE, Fridkin SK.Team emerging infections program healthcare-associatedinfections and antimicrobial use prevalence survey. Multi-state point-prevalence survey of health care-associatedinfections. N Engl J Med 2014;370(13):11981208.
2. Klevens RM, Edwards JR, Richards CL, Horan TC, GaynesRP, PollockDA,CardoDM.Estimatinghealth care-associated
TABLE 3. Log10 Reduction
Irradiance
(mWcm2)Time
(minutes)
Radiant exposure
(J cm2)Treated
(CFU)
Control
(CFU)
Mean log
reduction P-values
8.800.79 60 34.032.28 105.6771.11 70.60 7.75 1.980.53
-
infections and deaths in U.S. hospitals, 2002. Public HealthRep 2007;122(2):160166.
3. Shah H, BoschW, Thompson KM, Hellinger WC. Intravascu-lar catheter-related bloodstream infection. Neurohospitalist2013;3(3):144151.
4. Sievert DM, Ricks P, Edwards JR, Schneider A, Patel J,Srinivasan A, Kallen A, Limbago B, Fridkin S. FacilitiesNational Healthcare Safety Network (NHSN) Team andParticipating NHSN. Antimicrobial-resistant pathogensassociated with healthcare-associated infections: Summaryof data reported to theNationalHealthcare SafetyNetwork atthe Centers for Disease Control and Prevention, 20092010.Infect Control Hosp Epidemiol 2013;34(1):114.
5. Elder M. Hospital-Acquired Infection Control Market Kalor-ama Information, 2013.
6. Rupp ME, Lisco SJ, Lipsett PA, Perl TM, Keating K, CivettaJM, Mermel LA, Lee D, Dellinger EP, Donahoe M, Giles D,Pfaller MA, Maki DG, Sherertz R. Effect of a second-generation venous catheter impregnated with chlorhexidineand silver sulfadiazine on central catheter-related infections:A randomized, controlled trial. Ann Intern Med2005;143(8):570580.
7. Darouiche RO, Raad II, Heard SO, Thornby JI, Wenker OC,Gabrielli A, Berg J, Khardori N, Hanna H, Hachem R, HarrisRL, Mayhall G. A comparison of two antimicrobial-impreg-nated central venous catheters. Catheter Study Group.N Engl J Med 1999;340(1):18.
8. Sigurdsson V, Knulst AC, van Weelden H. Phototherapy ofacne vulgaris with visible light. Dermatology 1997;194(3):256260.
9. Tenover FC. Mechanisms of antimicrobial resistance inbacteria. Am J Med 2006;119(6 Suppl 1):S310. discussionS6270.
10. Walsh C. Molecular mechanisms that confer antibacterialdrug resistance. Nature 2000;406(6797):775781.
11. Davies J. Bacteria on the rampage. Nature 1996;383(6597):219220.
12. EnwemekaCS,WilliamsD, Enwemeka SK,Hollosi S, YensD.Blue 470-nm light kills methicillin-resistant Staphylococcusaureus (MRSA) in vitro. Photomed Laser Surg 2009;27(2):221226.
13. Maclean M, MacGregor SJ, Anderson JG, Woolsey G.Inactivation of bacterial pathogens following exposure tolight from a 405-nanometer light-emitting diode array. ApplEnviron Microbiol 2009;75(7):19321937.
14. Bumah VV, Masson-Meyers DS, Cashin SE, Enwemeka CS.Wavelength and bacterial density influence the bactericidaleffect of blue light on methicillin-resistant Staphylococcusaureus (MRSA). Photomed Laser Surg 2013;31(11):547553.
15. Ganz RA, Viveiros J, Ahmad A, Ahmadi A, Khalil A, TolkoffMJ, Nishioka NS, Hamblin MR. Helicobacter pylori inpatients can be killed by visible light. Lasers Surg Med2005;36(4):260265.
16. EnwemekaCS,WilliamsD,Hollosi S, YensD, Enwemeka SK.Visible 405nm SLD light photo-destroys methicillin-resistantStaphylococcus aureus (MRSA) in vitro. Lasers Surg Med2008;40(10):734737.
17. Vermeulen N, Keeler WJ, Nandakumar K, Leung KT. Thebactericidal effect of ultraviolet and visible light on Escher-ichia coli. Biotechnol Bioeng 2008;99(3):550556.
18. Murdoch LE, Maclean M, Endarko E, MacGregor SJ,Anderson JG. Bactericidal effects of 405nm light exposuredemonstrated by inactivation of Escherichia, Salmonella,Shigella, Listeria, and Mycobacterium species in liquidsuspensions and on exposed surfaces. ScientificWorldJournal2012;2012:137805.
19. HamblinMR,Viveiros J, YangC, AhmadiA, GanzRA, TolkoffMJ. Helicobacter pylori accumulates photoactive porphyrinsand is killed by visible light. Antimicrob Agents Chemother2005;49(7):28222827.
20. Weinstein RA. Nosocomial infection update. Emerg Infect Dis1998;4(3):416420.
21. Hidron AI, Edwards JR, Patel J, Horan TC, Sievert DM,Pollock DA, Fridkin SK. Team National Healthcare SafetyNetwork, Facilities Participating National Healthcare SafetyNetwork. NHSN annual update: Antimicrobial-resistant
pathogens associated with healthcare-associated infections:Annual summary of data reported to the National HealthcareSafety Network at the Centers for Disease Control andPrevention, 20062007. Infect Control Hosp Epidemiol2008;29(11):9961011.
22. Crivaro V, Bogdanovic L, Bagattini M, Iula VD, Catania M,Raimondi F, Triassi M, Zarrilli R. Surveillance of healthcare-associated infections in a neonatal intensive care unit in Italyduring 20062010. BMC Infect Dis 2015;15:152.
23. Ashkenazi H, Malik Z, Harth Y, Nitzan Y. Eradication ofPropionibacterium acnes by its endogenic porphyrins afterillumination with high intensity blue light. FEMS ImmunolMed Microbiol 2003;35(1):1724.
24. Papageorgiou P, Katsambas A, Chu A. Phototherapy withblue (415nm) and red (660nm) light in the treatment of acnevulgaris. Br J Dermatol 2000;142(5):973978.
25. Kawada A, Aragane Y, Kameyama H, Sangen Y, Tezuka T.Acne phototherapy with a high-intensity, enhanced, narrow-band, blue light source: An open study and in vitroinvestigation. J Dermatol Sci 2002;30(2):129135.
26. Noborio R, Nishida E, KurokawaM,Morita A. A new targetedblue light phototherapy for the treatment of acne. Photo-dermatol Photoimmunol Photomed 2007;23(1):3234.
27. Omi T, Bjerring P, Sato S, Kawana S, Hankins RW,HondaM.420nm intense continuous light therapy for acne. J CosmetLaser Ther 2004;6(3):156562.
28. Wheeland RG, Dhawan S. Evaluation of self-treatment ofmild-to-moderate facial acne with a blue light treatmentsystem. J Drugs Dermatol 2011;10(6):596602.
29. Lembo AJ, Ganz RA, Sheth S, Cave D, Kelly C, Levin P,Kazlas PT, Baldwin PC, Lindmark WR, McGrath JR,Hamblin MR. Treatment of Helicobacter pylori infectionwith intra-gastric violet light phototherapy: A pilot clinicaltrial. Lasers Surg Med 2009;41(5):337344.
30. Guffey JS,Wilborn J. Effects of combined 405-nmand 880-nmlight on Staphylococcus aureus and Pseudomonas aeruginosain vitro. Photomed Laser Surg 2006;24(6):680683.
31. Lipovsky A, Nitzan Y, Gedanken A, Lubart R. Visible light-inducedkillingofbacteriaasafunctionofwavelength:Implicationforwoundhealing. Lasers SurgMed 2010;42(6):467472.
32. Maclean M, Macgregor SJ, Anderson JG, Woolsey GA. Therole of oxygen in the visible-light inactivation of Staphylococ-cus aureus. J Photochem Photobiol B 2008;92(3):180184.
33. Drawz SM, Bonomo RA. Three decades of beta-lactamaseinhibitors. Clin Microbiol Rev 2010;23(1):160201.
34. Feuerstein O, Ginsburg I, Dayan E, Veler D, Weiss EI.Mechanism of visible light phototoxicity on Porphyromonasgingivalis and Fusobacterium nucleatum. Photochem Photo-biol 2005;81(5):11861189.
35. Redmond R. Photophysics and photochemistry in photody-namic therapy. Advances in photodynamic therapy: Basic,translational, and clinical. BostonMass.: ArtechHouse; 2008.pp 4158.
36. Tavares A, Carvalho CM, Faustino MA, Neves MG, Tome JP,Tome AC, Cavaleiro JA, Cunha A, Gomes NC, Alves E,Almeida A. Antimicrobial photodynamic therapy: Study ofbacterial recovery viability and potential development ofresistance after treatment. Mar Drugs 2010;8(1):91105.
37. Giuliani F, Martinelli M, Cocchi A, Arbia D, Fantetti L,RoncucciG. In vitro resistance selection studies of RLP068/Cl,a new Zn(II) phthalocyanine suitable for antimicrobialphotodynamic therapy. Antimicrob Agents Chemother2010;54(2):637642.
38. FDAU.Guidance for Industry and FDAStaff: Class II SpecialControls Guidance Document: Wound Dressing with Poly-(diallyl dimethyl ammonium chloride) (pDADMAC)Additive. U.S. Department of Health and Human ServicesFood and Drug Administration Center for Devices andRadiological Health; 2009;111.
SUPPORTING INFORMATION
Additional supporting information may be found in theonline version of this article at the publishers web-site.
VISIBLE LIGHT TREATMENT ON A b-LACTAM-RESISTANT E. COLI 7