ueda2011 pathophysiology of dm-d.adel
6
Review Of The Pathophysiology Of Type 2 Diabetes And The Key Role Of Incretin Hormones
-
Upload
ueda2015 -
Category
Health & Medicine
-
view
14 -
download
0
Transcript of ueda2011 pathophysiology of dm-d.adel

Review Of The Pathophysiology Of Type 2 Diabetes And The Key
Role Of Incretin Hormones

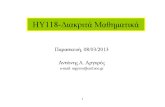
Major Pathophysiologic Defects in Type 2 Diabetes
Kahn CR, Saltiel AR. In: Kahn CR et al, eds. Joslin’s Diabetes Mellitus. 14th ed. Lippincott Williams & Wilkins; 2005:145–168.
Hepatic glucoseoutput
Insulin resistance
Glucose uptake
Glucagon(α cell)
Insulin(β cell)
LiverLiver
Hyperglycemia
Islet-Cell Dysfunction
MuscleMuscle
Adipose Adipose tissuetissue
PancreasPancreas
LiverLiver

Reprinted from Primary Care, 26, Ramlo-Halsted BA, Edelman SV, The natural history of type 2 diabetes. Implications for clinical practice, 771–789, © 1999, with permission from Elsevier.
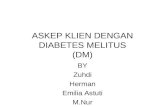
Development and Progression of Type 2 Diabetes and Related Complicationsa
aConceptual representation.
Insulin levelInsulin level
Insulin resistanceInsulin resistance
Hepatic glucose Hepatic glucose productionproduction
PostprandialPostprandial glucoseglucose
Fasting plasma Fasting plasma glucoseglucose
BBetaeta-cell function-cell function
Progression of Type 2 Diabetes Mellitus
Impaired Glucose Tolerance
Diabetes Diagnosis
Frank Diabetes
4–7 years
Development of Macrovascular Complications
Development of Microvascular Complications

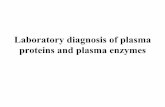
Relative Contribution of FPG and PPG to Overall Hyperglycemia Depending on HbA1c Quintiles
n = 58 n = 58 n = 58 n = 58n = 58
0
20
40
60
80
100
<7.3 7.3–8.4 8.5–9.2 9.3–10.2 >10.2
Postprandial glucose Fasting glucose
HbA1c
Co
ntr
ibu
tio
n, %
Monnier L et al. Diabetes Care. 2003;26:881–885. Copyright 2003 American Diabetes Association from Diabetes Care, Vol. 26, 2003; 881-885.Reprinted with permission from The American Diabetes Association.

Incretins Modulate Insulin and Glucagon to Decrease Blood Glucose During Hyperglycemia
GLP-1=glucagon-like peptide-1; GIP=glucose-dependent insulinotropic polypeptide.Brubaker PL et al. Endocrinology 2004;145:2653–2659; Zander M et al. Lancet 2002;359:824–930; Ahren B. Curr Diab Rep 2003;3:365–372; Buse JB et al. In: Williams Textbook of Endocrinology,11th ed. Philadelphia: Saunders; 2008:1329–1389; Drucker DJ. Diabetes Care 2003;26:2929–2940.
Incretin hormones GLP-1 and GIP are released by the intestine throughout the day; their levels increase in response to a meal.
Release ofactive incretinsGLP-1 and GIPa
Blood glucose in fasting and
postprandial states
Ingestion of food
Glucagonfrom alpha cells
(GLP-1)
Hepatic glucose
production
GI tract
DPP-4 enzyme
InactiveGLP-1
Insulin from beta cells
(GLP-1 and GIP)
Glucose-dependent
Glucose-dependent
Pancreas
InactiveGIP
Beta cellsBeta cellsAlpha cellsAlpha cells
Peripheral glucose uptake

THANK YOU