ueda2011 ealier insulinization-d.abbas
43
Earlier Insulinization >> Better Outcomes Prof. Abbas Oraby,MD Prof. of Internal Medicine and Diabetes. Faculty of Medicine –Zagazig University.
-
Upload
ueda2015 -
Category
Health & Medicine
-
view
12 -
download
0
Transcript of ueda2011 ealier insulinization-d.abbas

Earlier Insulinization >> Better Outcomes
Prof. Abbas Oraby,MDProf. of Internal Medicine and Diabetes.
Faculty of Medicine –Zagazig University.

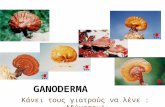
Normal Glucose Homeostasis Involves Pancreatic Islet Cells in Normal Subjects
Insulin from β-cells
Blood glucose homeostasis
Ingestion of food
Pancreas
-cells -cells
Glucagon from α-cells
Glucose production by
liver
Glucose uptake by
adipose and muscle tissue
Release of gut hormones
GI tract
Glucose dependent
Glucose dependent

Glycemic control mechanisms
Coordinated Functioning Of Pancreatic Beta Cells And Alpha Cells Is An Essential Component Of Normal Glycemic Control10

It involves 3 main steps :
Insulin release :
1. Translocation of insulin granules.
2. Docking of insulin granules.
3. Fusion of insulin granules.

Two essential components of the
cytoskeletal elements :
Translocation of insulin granules :
1. Microtubules (formed of tubulin
subunits).
2. Microfilaments (Actin + Myosin).

Microtubules form a network radiating from the perinuclear region outwords.
It gives the way but not the force
The framework provides the mechanical pathway along which secretory granules move toward the exocytic sites close to the plasma membrane.

The motive force to propel granules along the
microtubules is provided by the interaction
between :
It gives the force but not the way
ATP Ca+
Granule transport
Filamentous actin +
Phosphorylated myosin

Ca+ is essential for almost all steps
involved in insulin release, thus factors
increasing intracellular Ca+ will augment
insulin release.
Mechanisms involved in increasing intra-
cytoplasmic Ca+ :
Ca-influx from outside.
Inhibition of Ca-reuptake by intracellulas stores.
Increased Ca-sensitivity.
xCa++ Store
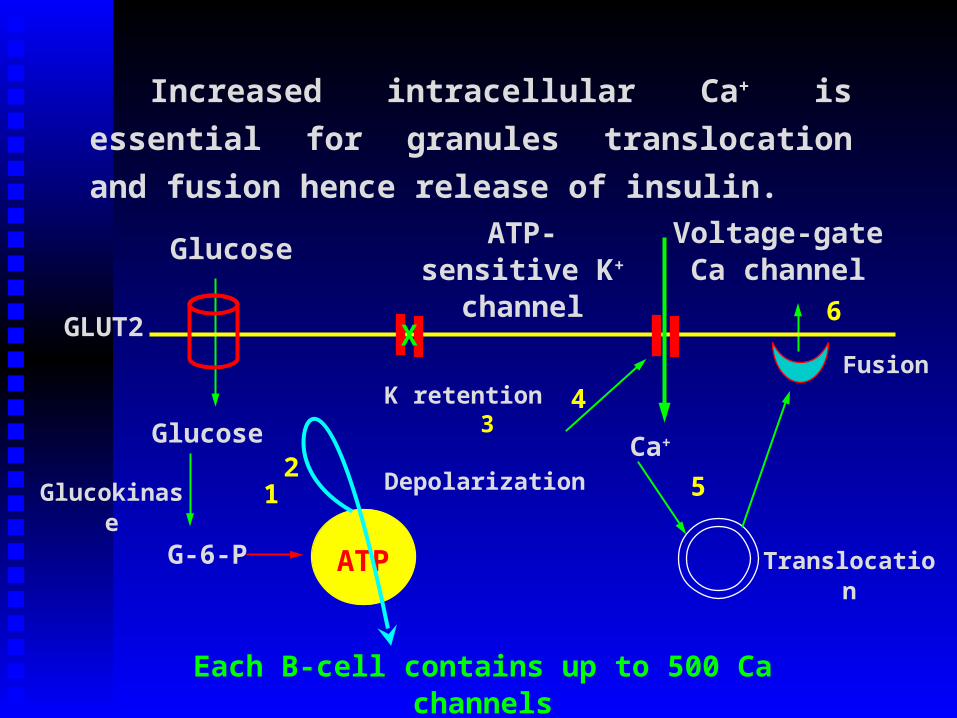
Increased intracellular Ca+ is essential for
granules translocation and fusion hence release
of insulin.
Each B-cell contains up to 500 Ca channels
Glucose ATP-sensitive K+ channel
K retention3
Depolarization
4
Glucokinase
TranslocationATP
Voltage-gate Ca channel
Fusion
Ca+
5
6
Glucose
1
G-6-P
2
GLUT2 X

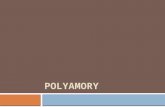
Normal IGT Type 2
INSULINRESISTANCE
INSULINSECRETION
FPG/PPGHbA1c↑
Type 2 Diabetes is a Dual Problem
Adapted from Type 2 Diabetes BASICS. Minneapolis, MN: International Diabetes Center; 2000
Schematic Representation of the Natural Progression of Type 2 Diabetes

The defect of insulin secretion in DM2 is
related to 2 compenents:
1- Insulin deficiency
2- Disturbed kinetics of insulin secretion.

Disturbed Kinetics:-
1- Loss of the 1st phase of insulin
secretion.
2- Decreased 2nd phase.

Non-diabetic
T2DM

-ce
ll m
ass
(%)
~65%
-cell deficit in T2DM
Modified from Butler AE, et al. Diabetes 2003;52:102–10.

-cell apoptosis in T2DM
Butler AE, et al. Diabetes 2003;52:102–10.
Lean(non-diabetic)
Obese(non-diabetic)
ObeseT2DM
0.00
0.25
0.50
0.25 *
*p<0.05 vs obese non-diabetic

Non-diabetic
T2DM

Pool-hypothesis
ATPADP
Modified from Rorsman P, et al. News Physiol Sci 2000;15:72–7.
I. Defective mobilisation
II. insulin requirements
RR-Pool
Reserve-Pool
Depletion of insulin stores

Insulin Deficiency:
1- mature insulin.
2- C-peptide.
3- Pro-insulin.
Immune- reactive
insulin.
PI/IRI

Factors for progressive loss of B-cell
function & mass:
- Glucotoxicity.
- Lipotoxicity.
- Inflammatory cytokines and leptin.
- Islet cell amyloid.
- Reduced B-cell mass and dysfunction.

Glucotoxicity
Nonphysiological and potentially
irreversible B-cell damage caused by
chronic exposure to supra-physiological
glucose concentration with characteristic
decreases in insulin synthesis and
secretion caused by decreases insulin
gene expression.
Glucotoxicity is irreversible

B-cell exhaustion
- A physical depletion of B-cell insulin
stores secondary to prolonged chronic
stimulation with glucose on non-
glucose secretagogues.
- No defect in insulin synthesis.
- The B-cell function fully recovers as it
rests.
Exhaustion is reversible

B-cells Gluose-induced apoptosis
Physiological Increase(100-200 mg%)
Longer & higher increase
Insulin Secretion Proinsulin synthesis
Long-term increase of cystosolic Ca+
Excess protein influx through ER
ER stress Apoptosis

ER Stress
-cell dysfunctionInsulin resistance
-cell apoptosis
Chronic inflammation
Obesity
Atherosclerosis
Endoplasmic reticulum stress

Hyperglycemia
Reactive oxygen species (ROS)
Oxidative stress
Apoptosis

Interplay between B-cell exhaustion & glucotoxicity
Excess insulin secreation
Prolonged hyperglycemia
Insulin depletion from B-cell (Exhausion)
Hyperglycemia
More, prolonged hyperglycemia
ER Stress ROS Ca++ Cytokines
Irreversible B-cell damge& apoptosis (Glucotoxicity)
Beta-cellRest

• The concept of B-cell rest was first
introduced 30 years before.
• The K channel opener diazoxide was
used to inhibit insulin secretion in DM2
patients receiving insulin.
• Re-accumulation of insulin stores in B-
cell restored the insulin response to a
combined stimulation with glucagon
plus tolbutamide.

K-channels opener(Diazoxide & NN414)
B-cell rest
Better functions
(B-cell preserve)
Cytosolic Ca++
Re-accumulationof insulin stores
Apoptosis

Diazoxide induces B-cell preserve by:
1-Blocking insulin screation (rest)
2-Reducing cytosolic Ca++ (anti-apoptosis)

The hypothesis
Induction of B-cell rest early in type 2
diabetes restore B-cell functions and
delay further B-cell destruction.

The approach
- Intensive insulin therapy
- Early in type 2 diabetes.

(The Evidence)
Many reports in the last few years
proved the beneficial effects of short term
intensive insulin therapy (2-3 weeks), early
in DM2 with remission extended up to 2
years and maintained better metabolic
profile after 4 years follow up.
- Alvarsson et al., 2003
- Ryan et al., 2004
- Orabi A, 2006
- Xu Wen et al., 2009

(The recommendation)
Early Insulinzation
ADA & CASD consensus 2008.

Current ADA / EASD guidelines
Lifestyle + metformin
Add basal insulin or SU
Intensify therapy e.g. ‘basal plus’
1
2
3
Nathan DM, et al. Diabetes Care 2009;32:193–203.

Blicklé JF, et al. Diabetes Obes Metab 2009;11(4):379–386
TULIP: initiating Insulin Glargine improves glycaemic control more than intensifying lifestyle management in Type 2 diabetes
Randomized study in 211 insulin-naïve subjects with T2DM, who initiated Insulin Glargine in combination with OADs or intensification of lifestyle management + OADs for 9 months

ADA/EASD Target
6.0
7.0
8.0
9.0
10.0
Baseline
Time (weeks)
12
Hb
A1
c (
%)
Insulin glargine
Pioglitazone
186 24 4830 36 42 Endpoint
6.8%
7.6%
Meneghini LF, et al. ADA 2005 (abstract).
48-week randomised trial in 173 patients with uncontrolled T2DM on MET or SU for ≥3 months and HbA1c 8–12%
4020 study: Insulin glargine provides better HbA1c control than TZD after OHA failure
Incidence of hypoglycaemia was similar for both treatment groups

Risk of severe hypoglycaemia and severe nocturnal hypoglycaemia reducedby 46% (p = 0.04) and 59% (p = 0.02), respectively, with insulin glargine
0.931 (0.771, 1.123); p = 0.455
0.591 (0.486, 0.718); p < 0.001
0.711 (0.586, 0.862); p = 0.001
Odds ratio
0 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8 2.0
Overall
Nocturnal
Daytime
Symptomatic hypoglycaemic events
Increased riskReduced risk
Risk reduction mainlyobserved at night
Rosenstock J, et al. Diabetes Care 2005;28:950−5.
Mean (CI)
Insulin glargine reduces hypoglycaemic risk versus NPH in T2DM: Meta analysis

Hyp
og
lyca
emia
NPH
Glargine
A1c
~ ~ 0.4–0.6% ? ?
The impact of hypoglycaemia on A1c
A “qualified A1c” by hypoglycaemiaThe quest for a better basal insulin…

RANDOMISATION
Insulin-naive patients with T2DM on 1 to 2 OHAs for ≥4 months
HbA1c 7.5–10%(n = 582)
Insulin glargine once daily in evenings + OHAs (n = 291)
Detemir once daily in evenings* + OHAs (n = 291)
Treatment phase
52 weeks
Insulin glargine versus detemir added to an OHA regimen
Rosenstock J, et al. Diabetologia 2008;51:408–16.
*An additional morning detemir dose was permitted if pre-dinner plasma glucose was >7.0 mmol/L afterachieving FPG <7.0 mmol/L. No second glargine dose was allowed.

−1.5% −1.5%
Similar rates of hypoglycaemia with insulin glargine and insulin detemir
Rosenstock J, et al. Diabetologia 2008;51:408–16.
Similar improvements in glycaemic control with insulin glargine and detemir

Dosing frequency and daily dose are lower with insulin glargine vs detemir: 1-year data
Once-daily dosing Daily insulin dose
Pa
tie
nts
(%
)
Rosenstock J, et al. Diabetologia 2008;51:408–16.
At
stu
dy
en
d (
U/k
g/d
ay)
*103 of the 104 patients who required twice-daily dosing were switched within 12 weeksChanges in HbA1c were similar

12,612
>6,000 standard step-therapy>6,000 standard step-therapy>6,000 early glargine>6,000 early glargine
FPG goal: <95 mg/dL (<5.3 mmol/L)
HbA1C goal: <7%
Start: 2003 Follow-up: Extended to 7 years Final results: 2011
ORIGIN trial: Study design
• Prediabetes and early T2DM with CVD
If positive…insulin replacement can be considered right from If positive…insulin replacement can be considered right from the outset ! the outset !
• CV event-reduction outcome study• Opportunity to assess -cell preservation
Gerstein HC, et al. Am Heart J 2008;155:26–32.

ACCORD VADT ADVANCE ORIGIN
Number of patients 10,251 1,792 11,140 12,612
Age (years) 62 60 66 64
Diabetes duration (years)
10 11.5 8 5
Macrovascular complications (%)
35 40 32 66
Baseline HbA1c (%) 8.3 9.4 7.5 6.5
Intensive Rx target A1c < 6% A1c < 6% A1c ≤ 6.5 % FBG ≤ 5.3 mmol/L
Intervention Multiple drugs Multiple drugs Gliclazide ± others
Glargine ± others
ORIGIN trial: Comparison with other CV outcome studies