ΠΛΗΡΩΣ ΑΡΘΡΟΣΚΟΠΙΚΗ ΑΠΟΚΑΤΑΣΤΑΣΗ ΧΟΝΔΡΙΝΩΝ ΚΑΙ ΟΣΤΕΟΧΟΝΔΡΙΝΩΝ ΒΛΑΒΩΝ ΓΟΝΑΤΟΣ
Upload
bioorthopedikiCategory
view
841download
0description

ANATOMIC APPROACH FOR REVISION ACL RECONSTRUCTION
MR ALEVROGIANNIS STAVROS, MD,PhDORTHOPAEDIC SURGEON
S. CONSULTANT IN SPORTS INJURIES.ATHENS/GREECE

ACL EPIDEMIOLOGY
• Annual incidence of ~200,000 ACL ruptures per year with an estimated 1 in 3,000 pts, in USA • 150,000 result in operations costing around two billion dollars a year• Females are injured with a higher frequency than males due to many factors including slightly different and disadvantageous joint anatomy, hormonal factors and less muscle mass• Incidence highest in population aged 15-45 years old with 1 in 1750 persons
(Brown, 2004)• Most common injury in football and basketball in younger patients- skiing in
older patients- • Substantial anterior tibial shear forces stress ACL from quads contraction(esp.
0 – 30 degrees contraction) (Sakane, ‘97) • Typically torn in non-contact deceleration results in valgus twisting injury• Athlete lands on legand pivots in opposite direction • Average return to full activity is ~ 6 to 8 months

INCREASE OF PRIMARY ACLRECONSTRUCTION
1. increased level of sports activities
2. increase of high risk associated activities (contact sports)
3. increased awareness
4. tendency towards operative treatment

FAILURE PRIMARY ACL SURGERY
3-10 % fail• arthritis and recurrent
pain• arthrofibrosis or loss of
motion• extensor mechanism
dysfunction• recurrent patholaxity(Johnson DL, Fu FH. Anterior cruciate ligamnet
reconstruction: why do failures occur? Instr Course Lect 1995: 44: 391-406)

CAUSES OF FAILURE
• traumatic re-injury
• returning to sports too soon after surgery
• inappropriate or overaggressive rehabilitation
• technical failures

TECHNICAL FAILURES(70% OF CASES)
• Improper graft placement• Graft impingement due to
inadequate notchplasty • Improper graft tensioning• Inadequate graft fixation due
to the fixation device or deficient bone stock
• Use of a graft of diminished tensile strength or size
• Failure to correct associated ligament instabilities

INDICATIONS FOR ACL-R1. Subjective feeling of instability during the normal daily and sports activities
2. Functional instability with or without pain under weight bearing
3. Objective anterior laxity (during the clinical examination) with positive Noulis-Lachman test and significant KT-1000 side-to-side difference

TYPICAL PATTERNS OF ACL GRAFT RUPTURE

ACL- REVISION ALGORITHM

TIPS & PEARLS FOR ACL REVISION SURGERY
• ACL ANATOMY• CLASSIFICATION • SURGICAL METHOD• REMOVAL HARDWARE• BONE GRAFTS• GRAFT CHOICE• FIXATION CHOICE• DRILLING TUNNELS

ANATOMIC ACL-R
CRITICAL QUESTIONS:
• WHAT IS ANATOMIC APPROACH IN ACL-R?
(be familiar with anatomical landmarks and footprints)
• WHY WE NEED ANATOMIC APPROACH?
(24-30% re-rupture of the graft)

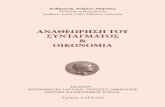
ACL ANATOMIC FOOTPRINTS
FEMUR TIBIA

• The intact AM and PL bundles of the ACL are shown in (A), and the soft tissue remnant of torn ACL on the femoral side is shown in (B). When the knee is in 90 degrees of flexion, the femoral insertion sites of the AM and PL are horizontally aligned. The white circles on the cadaveric specimen picture (A) and the arthroscopic surgery picture (B) show potential area that the femoral tunnels can be incorrectly placed when a trans-tibial approach and the clock face concept is used, which is seen in most of revision cases. Laser scan (C) and arthroscopic picture (D) show the two bony landmarks on the femoral insertion sites of the AM and PL bundles when knee is in 90° of flexion

Clinical Results after S.B ACLR
• Greatly improved over the last years
• However, there are many issues which should be improved in the future:
-the normal rate ( 2mm) is only 70%
-rotatory control is insufficient -normal athletic abilities are not
restored even in the “normal” knee
Renstrom P.ESSKA 2004)

A.M S.B ACLR

CONVENTIONAL D.B ACLR

ANATOMIC D.B ACLR

FEMORAL TUNNELS IN D.B TECHNIQUE


ANATOMIC APPROACH S.B TECHNIQUE - FEMORAL DRILLING

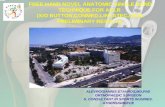
FEMORAL TUNNEL IN ANATOMIC S.B TECHNIQUE
The femoral tunnel is low and overlaps both the AM and PL anatomical sites

TIBIAL DRILLING IN ANATOMIC S.B ACLR

ACL GRAFT LENGTH

FEMORAL TUNNEL POSITION: AN X-RAY COMPARISON OF DRILLING THROUGH THE TIBIAL TUNNEL vs DRILLING
THROUGH THE MEDIAL PORTALChao D,Pallia C,Young S et al
• 40 ACL recon pts• Results- Statistical significance
superior (TT technique) vs inferior (AM technique) alignment of femoral tunnel placement
- TT technique produces a more anterior femoral tunnel and a more vertical ACL graft orientation

ACL SAGITTAL ANGLE ACCOUNTS FOR FEMORAL & TIBIAL INSERTION
Normal MRI Anteromedial Technique

MRI MEASUREMENT TECHNIQUES
• ACL angle
- Anterior edge of ACL
- Lateral tibial plateau

MRI MEASUREMENT TECHNIQUES
AT angle
-Anterior edge of ACL-Medial tibial plateau

MRI COMPARISON-RESULTS
NORMAL AM TECHNIQUE TT TECHNIQUE

ARTHOSCOPIC PORTALS
LP : (lateral portal = incision towards the outside of the knee) MP :(medial portal = incision towards the inside of the knee) AMP : (accessory medial portal = incision even further on the
inside of the knee) and CP :(central portal= incision towards medial one third of patellar
ligament)

ACL-REVISION GRAFTS
• AUTOGRAFTS-BPTB Ipsilateral contralateral-QUADRICERS-QUADRAPLED ST (indirect fixation recommended)-DOUBLED STG (more fixation options, internal rotation weakness)• ALLOGRAFTS Achilles tendon Posterior tibialis• XENOGRAFTS (new generation) JewelAcl (NeoLigaments)

JEWEL-ACLFeatures and benefits
• Is a specialized textile scaffold which is rendered versatile for ACL reconstruction by various structural features. The scaffold is treated with a proprietary gas plasma treatment process that increases its surface energy and renders it hydrophilic • The continuous tubular form can accommodate a
hamstring tendon• The open weave sections have appropriate spacing to
encourage tissue ingrowth into the scaffold. • The densely woven sections have superior handling
properties. • The JewelACL is a bio-enhanced prosthesis for the ACL
reconstruction. • The JewelACL can be secured to the bone with currently
available fixation devices.

• Can be implanted as a total tissue sparing device, or with a single hamstring tendon • Manufactured from Polyethylene Terephthalate (polyester) • Allows early rehabilitation (parallel longitudinal polyester fibres
provide high strength of 3000N) • Implanted using standard modern ACL guide-wire systems • Stiffness is matched to the semitendinosus tendon to permit load
transfer and encourage cell growth due to plasma-spray.
more than four times as many cells were found on the plasma-treated ligament surfaces after 14 days incubation compared to non plasma-treated polyester surfaces.
BENEFITS

ACLR (JewelAcl-X/O BUTTON) +in elite 25 y. male athlete.

ACLR (JewelAcl-X/O BUTTON) +CHONDROPLASTY MFC(Chondromimetic) in a
non-competitive 41 y.female athlete.

MATERIAL(AUG. 2010- FEB.2011)
8
2238
20
10
20
30
40
report activity prior to ACL re-rupture
PRE-OP EVALUATION• Sex ratio : 48 males, 22 females
• Side : 41 left, 29 right Mean age : 29 years (range 16-48)
no sportsport from time to timefrequent sportcompetition

CLASSIFICATION SYSTEM FOR ACL R.(H.H. Paessler et al, Wiosna 2002,48-60 New Techniques for ACL
revision surgery)
• GRADE I : a) Narrow femoral and tibial
tunnels in correct position b) Femoral ± tibial tunnel far
away from correct position• GRADE II: Large tibial
tunnel + small femoral tunnel or previous tunnel closed by bone block of initial graft
• GRADE III : Large femoral + tibial tunnel
• GRADE IV : GRADE III+additional lesions of secondary restraints osteoarthritis ± PCL

METHOD• Mean time between re-rupture of ACL graft and revision surgery 29m ( 9- 39m)• All cases were type I or II according to H.H Paessler Classification system • All cases performed by one senior surgeon in one stage procedure• Diagnostic arthroscopy first• All ACL graft remnants were removed• 29 meniscal tears ( 18 part.debrided-11 repaired)• 22 cartilage lesions ( 15/III,7/IV),16 debrided, 4 Chondromimetic, 2 ACT3D ( 2 procedures)• 52 cases using the anatomical approach, remaining 18 the modified one• No notchplasty!!!!• 2 had an OWHTO due to varus mal-alignment prior to ACLR (single varus)• 3 had reconstruction of the posterolateral ligament structures• Interference screw was not removed in misplaced femoral tunnel• ST tendon ( ipsilateral or contralateral) with JewelAcl augmentation was used in all cases• 3 doses of gentamycin was given i.v• Prophylactic anti-coagulants for 20 d.p.o• Functional brace

POST-OP REGIMEN• Immediate knee motion and muscle-strengthening exercises on the 1st d.p.o• Functional knee brace for 6 w.p.o• Full R.O.M from the 1st d.p.o• P.w.b from the 2nd w.p.o f.w.b 6th w.p.o• Physio- protocol was modified if concomitant procedure was performed• Running program 6th m.p.o• Pivoting+ contact sports 9th-12 m.p.o

COMPLICATIONS• No major complications were found• No joint effusion 2m.p.o • 1 DVT, 15d.p.o was solved uneventfully• 1 superficial infection ( oral antibiotics)• 2 arthrofibrosis ( 1 required MUA 7w.p.o- the other arthroscopic lysis of adhesions and scar tissue 10w.p.o)• No re-re-rupture of the graft (JewelAcl?)

MODIFIED CINCINATTI SCORE (0-100)
Excellent (>80), Good (55 to 79), Fair (30 to 54) or Poor(<30)
Pain
Swelling
Giving way
Overall activity level
Walking
Stairs
Running activity
Jumping or twisting activities
41,5
68,2 72,5
0
10
20
30
40
50
60
70
80
PRE.OP
6M.P.O
1Y.P.O

VISUAL ANALOGUE SCORE (0 = good, 10=poor)
0
2
4
6
8
10
0 6 12
months
po
ints

81%
1%18%
BETTER SAME WORSE
PATIENT OUTCOME FUNCTION SCORE

PAIN & ACTIVITY
4%
38%
45%
13%
0%6%
25%
69%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Severe with DailyActivities
Moderate withDaily Activities
Daily Activities Only None with SportsActivities
Pain Symptoms Related to Activity
Per
cent
of K
nees
Pre-Op
Post-Op

KNEE PERCEPRION
46%
35%
15%
0%2%
6%
15%
33%
37%
9%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Poor Fair Good VeryGood
Normal
Patient Perception of the Knee Condition
Per
cen
t of K
nee
s
Pre-Op
Post-Op

ACTIVITIES OF DAILY LIVING
17%
8%
40%35%
2% 2%
21%
75%
0%
10%
20%
30%
40%
50%
60%
70%
80%
0 20 30 40
Stair Climbing
Per
cen
t o
f K
nee
s
Pre-Op
Post-Op
15%10%
31%
44%
2% 2%6%
90%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 20 30 40
Walking
Pe
rce
nt
of
Kn
ee
s
Pre-Op
Post-Op

SPORTS ACTIVITIES
67%
10% 10%13%
29%
11%
29% 31%
0%
10%
20%
30%
40%
50%
60%
70%
80%
40 60 80 100
Running
Per
cent
of K
nees
Pre-Op
Post-Op
75%
10%13%
2%
33%
13%
37%
17%
0%
10%
20%
30%
40%
50%
60%
70%
80%
40 60 80 100
Twisting/ Turning
Perc
ent o
f Kne
es
Pre-Op
Post-Op

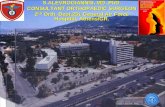
LACHMANN-NOULIS TEST
0% 2%
98%
64%
15%21%
0%
20%
40%
60%
80%
100%
120%
< 3 3-5.5 > 5.5
Antero-posterior Displacement
Per
cen
t o
f K
nees
Pre-Op
Post-Op

3,411,1 14,4
71,1
0
1020
3040
5060
7080
A B C D
C + D > 85%
PRE-OP IKDC SCORE (%)KT 1000 LAXITY

0
11
52
7
0
10
20
30
40
50
60
equal +glide ++ clunk +++ gross
PRE-OP PIVOT SHIFT

2
21
42
5
0
5
10
15
20
25
30
35
40
45
no sportsport fromtime totime
frequentsport
competition
1 year follow-up sport activity
POST-OP EVALUATION
no sport
sport from time to time
frequent sport
competition

1
45
18
51
0
5
10
15
20
25
30
35
40
45
-3 to -1 mm -1 to 2 mm 3 to 5 mm 6 to 10 mm > 10 mm
RESULTS KT 1000 LIGAMENT EVALUATION
manual maximum and Telos

84%
13%
3 0
0
10
20
30
40
50
60
70
80n
A equal B glide C clunk D gross
p = 0.001
RESULTS: Pivot Shift
Preop
Postop

61
72 00
10
20
30
40
50
60
70
equal +glide ++ clunk +++ gross
RESULTS
PIVOT SHIFT

2
32
8
24
1012
50
2
0
5
10
15
20
25
30
35
40
45
50
A B C D
GLOBAL SCORE IKDC at F.U.
pre-op
F-U

CONCLUSIONS
• Surgical error is the main cause of failure of a primary reconstruction
• Pre-operative planning is crucial to carefully access the factors that may have been related to the prior failure
• Revision ACL surgery is technically demanding- requires theoretical and clinical experience
• Anatomic approach for revision ACL is a very attractive surgical method
• No re-failure of the graft yet! (24-30% in the literature) • Primary results of ACL-R graft augmentation with JewelAcl,
seems to be more than encouraging• Further mid-term results are needed• Patients should be well informed about the less favorable
outcome of a revision (unrealistic expectations !!!!)