Two Populations of MS Patients Treatment of Multiple Sclerosis · Ocrelizumab(OCR) Phase II Updated...
8
Click here to load reader
Transcript of Two Populations of MS Patients Treatment of Multiple Sclerosis · Ocrelizumab(OCR) Phase II Updated...

2/16/2012
1
Multiple Sclerosis 2012Lessons From the Bench and Bedside
Recent Advances in Neurology
Stephen L. Hauser, MDDepartment of Neurology, University of California, San Francisco
Conflicts of Interest: BioMarin, Receptos
February 15, 2012
Sir Augustus d’Este (1794-1848)Victoria and Albert Museum, London
The Origins of Multiple Sclerosis
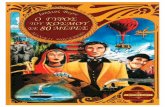
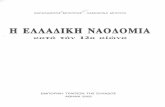
Two Populations of MS Patients
Relapsing and Progressive
0
10
20
0 1.5 2.5 3.5 4.5 5.5 6.5 7.5 8.5
Disability (EDSS)
BenignSymptoms
MinimalDisability
Gait Disturbance
Cane Crutches
NonambulatoryRelapsing Remitting MS Progressive MS
Treatment of Multiple SclerosisHarrison’s Principles of Internal Medicine 3rd Ed, 1958
The most that can be done is to reassure and encourage the patient through moderate exercise
and supportive measures…during an acute episode it is surely preferable to assure the patient that he will recover and to preserve
silence on the subject of relapse.
John N. Walton

2/16/2012
2
Marketed
Phase III
Phase II
Phase I
The Therapeutic Landscape in MS (2011)
Anti-proliferationagents
Interferons
Vaccine, tolerization
Targeted mAbs/Fc-Ab Symptomatic Tx
Targeted Immuneregulation
Lymphocyte trafficking
Oral administration
Injection
Fingolimod
Firategrast
AJM-300
TBC4746
R1295
TysabriATL-1102
MLN-0002
Laquinimod
Cladribine
BG-12
Riluzole
683699(T-0047)Daclizumab
MM-093
Sativex
DalfampridineSR
Nerispirdine
OcrelizumabCampath
Rituximab
AtaciceptLY-2127399
Ofatumumab
Copaxone
Tovaxin
ATX-MS-1467
PI2301
NovantronePixantrone Azathioprine
Teriflunomide
BetaseronAvonex
Rebif
Peg IFNß(BIIB017)
Interferon Tau
Fc-IFß
Interferon Omega
Courtesy of G. Giovannoni (modified)
Vesicular Demyelination in MSA Pattern of Humoral Immune Pathology
Rituximab in Relapsing Remitting MSGadolinium-Enhancing Lesions from Baseline to Week 48
Weeks
Mea
n N
umbe
r of G
dLe
sion
s
0
0.5
1
1.5
2
2.5
0 4 8 12 16 20 24 28 32 4036 44 48
* Missing values imputed by average of available data
P = 0.78
P = 0.003
P = 0.001
P < 0.001
Rituximab (N=66)
Placebo (N=35)
Hauser SL, Waubant E, Arnold DL, Vollmer T, Antel J, Fox RJ, Bar-Or A,..Smith CH. N Engl J Med: 358:676, 2008
Rituximab in Primary Progressive MSTime to Confirmed Disease Progression
Hawker et al, Ann Neurol 66:460, 2009
All Intent-to-Treat Patients (N=439)
Time to Confirmed Disease Progression (weeks)
Pro
porti
on o
f Pat
ient
s
0 12 24 36 48 60 72 84 108
HR: 0.77 (95% Cl: 0.55 – 1.09)p-value=0.1442
0
10
20
30
40
50
60
70
96
Rituximab
Placebo

2/16/2012
3
Rituximab in Primary Progressive MSTime to Confirmed Disease ProgressionSubgroup Analysis
HR: 0.63 (95% CI: 0.34-1.18)p=0.1427
HR: 0.33 (95% CI: 0.14-0.79)p=0.0088
Age <51Gd (+) at Baselinen=72
Age <51Gd (-) at Baselinen=143
Rituximab
Placebo
0 12 24 36 48 60 72 84 1080
10
20
30
40
50
60
70
96
Pro
porti
on o
f Pat
ient
s
0 12 24 36 48 60 72 84 1080
10
20
30
40
50
60
70
96
Time to Confirmed Disease Progression (weeks)
The Development of Anti-CD20 TherapyRituximab and Ocrelizumab
1995 Co-development
2003 Merger
2009 Merger
1986 Synthesis
Technological change moves faster than the pace of clinical experiments
SSSSSS
Constant region
Variable domains
CH1
SS
CH2
CH3
VH
V k
Ck
Fc
Heavy chain
Light chain
N-terminus
C-terminus
C
B B
PVP158
FCγRIIIa
PV
NK
ANP INIYNCEPANP
xx
X = mutation
V (ADCC) > P (ADCC)
Overlapping epitope
2 mutations in RTX reduce affinity for NK cells
Chimeric vs humanised VH/ VL
Ocrelizumab binds more strongly both forms of the Fc γRIIIa on NK cells
NK: natural killer cell
Ocrelizumab
Study Design for Ocrelizumab Phase II Trial
Design Randomized, double-blind, placebo-controlled ocrelizumab; blinded rater AvonexTM; 1:1:1:1 randomization stratified by geographical region
Sample Size / No. sites N = 200 planned (220 actual); ~100 sites European Union, United States, & Rest of World
PopulationRRMS, Expanded Disability Status Scale (EDSS) of 1.0–6.0, inclusive, At least two
documented relapses within last 3 years, at least one of which occurred within last year prior to screening, MRI evidence of disease burden
Schedule and dose
Placebo × 2 for Cycle 1 only �600 mg open-label ocrelizumab300 mg × 2 � by 600 mg q24 wks1000 mg × 2 �1000 mg q24 and 48 wks �600 mg q72 wksAvonexTM 30 µg IM qwk × 24 wks �600 mg open-label ocrelizumab
1°Endpoint Total number of Gd-enhancing lesions at Wks 12, 16, 20, and 24
2°Endpoint Annual relapse rate (ARR) by Wk 24; Proportion of patients relapse-free by Wk 24; total # new gadolinium (Gd)-enhancing lesions; change in total volume T2 lesions
Study duration 144 wks total = 96-week treatment period + 48 wks for follow-up
Double blind
Rater blinded
Screen (4 wks)
Treatment period (96 wks)
MRI
OCR / Pbo Infusion
-4 2 4 12 16 20 24 72 1440 8 9648

2/16/2012
4
Ocrelizumab in Relapsing Remitting MSPrimary Endpoint: Mean Gad+ Lesions Week 12 to Week 24
Weeks
Mea
n N
o. T
1 G
d-en
hanc
ing
Lesi
ons
0
1.0
2.0
3.0
4.0
0 4 8 12 16 20 24
*IFN beta-1a arm was open label, all efficacy comparisons were exploratory
Placebo (N=54)Ocrelizumab 600mg (N=51)Ocrelizumab 2000mg (N=52)IFN beta-1a (N=52)
Primary end point
P<0.0001 for both Ocrelizumab doses vs placebo
Lesions on MRI by week (ITT): average imputation
Kappos, Li, Calabresi, O’Connor, Bar-Or, Barkof,Yin, Leppert, Glanzman, Tinbergen, Hauser. Lancet 378:1779, 2011
A Fatality in the Ocrelizumab RRMS Trial!• 41 year old woman, disease duration 10 years, prior Rx IFN beta
• Randomized to OCR 2000 mg group
• At week 12, on day of routine blood and MRI follow-up studies (all unremarkable), developed delirium, thrombocytopenia and status epilepticus, then fever, and over the next 48 hrs a Systemic Inflammatory Response Syndrome (SIRS) with multiorgan dysfunction, brain edema
• Had sustained a bee sting on face 5 days earlier
• Multiple blood, CSF cultures (including viral PCR) negative for infection
• Treatment with platelets, IVIg, antibiotics to no avail; death on day 15• Pathology: severe cerebral ischemia with herniation; several
perivascular CNS hemorrhages; several septic emboli; multi-organ dysfunction; no evidence for TTP, DIC, or primary infection in brain or hepatic tissue
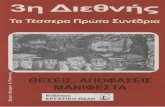
Ocrelizumab (OCR) Phase II Updated Results 96-Week ARR
Weeks 0-24 Placebo OCR 600 mg OCR 2000 mg IFN β-1a 30 mcg IMWeeks 24-48 OCR 600 mg OCR 600 mg OCR 1000 mg OCR 600 mg Weeks 48-72 OCR 600 mg OCR 600 mg OCR 1000 mg OCR 600 m gWeeks 72-96 OCR 600 mg OCR 600 mg OCR 600 mg OCR 600 mg
Ocrelizumab: 96 Week Data• There were 7 serious AEs in phase 2 RRMS trial: 1 in placebo; 1 in 600
mg; 3 in 2000 mg; 2 in IFNβ1a; no imbalance or increase over time
• Two serious AEs were thought to be infection-related: 1 in placebo; 1 in 2000 mg OCR
• No opportunistic infections were noted; no dropouts due to adverse events; no imbalance in infection rate during weeks 48-96
• Infusion-related reactions occurred after initial infusion (30-44%) and decreased on subsequent infusions; led to withdrawal in only 3 pts
• Through 96 weeks, with open-label Ocrelizumab 600 mg treatment:- No loss of efficacy; most patients had no clinical disease activity- No patient experienced a new or enlarging T2 lesion from Week 24 to Week 96- At the Week 96 MRI scan, no patient on Ocrelizumab experienced a Gd
enhancing TI lesion

2/16/2012
5
Ocrelizumab: The Path Forward
• Rheumatoid Arthritis (RA) phase 3 OCR program halted in May 2010 due to cases of serious/fatal opportunistic infections; dose, chronic GC use, co-morbid illness, Asian ancestry implicated as risk factors
• RA phase 3 trials: no increase in risk of opportunistic infections at 200 mg x2 dosing of OCR (>1500 pt/yrs)
• No cases of PML with OCR; with Rituxan (2 million Rx), PML noted in 6 RA (118,000 pts treated); 8 SLE; 6 other AID; 137 oncology; 0 MS cases
• Phase 3 OCR trials in MS launched in 2011: 2 in RRMS; 1 in PPMS
The Phase 3 Orchestra Trials of OcrelizumabORATORIO: Randomized, Double-Blind, Placebo-controlled Study in Primary Progressive MS`
OPERA I & II: Randomized, Double-Blind, Double-dummy Studies in Relapsing MS`vsIFN beta-1a (Rebif®)
B Cells and the brain
Bone marrow
Stem cell
pro-B
pre-B Immature B cell
CNS
Mature naïve B cell
SpleenSpleen
ActivatedB cell
Plasma cell(long lived)
Plasmablast
Plasma cell(long lived)
Plasmablast
Memory B cell
Potential sites of antigen recognition
Follicle-like aggregates
Bystander activation
Secondary lymphoid tissues
Lymph folliclewith germinal center
T
Courtesy of Christian vonBuedingen
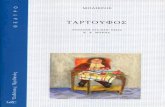
Anti CD20 ameliorates MOG protein-induced EAE
0
10
20
30
B c
ells
per
sq.
mm
Isotypeα-hCD20
0
10
20
30
40
50
0
4
8
12
16
20Isotypeα-hCD20
parenchymalmeningeal
Isotypeα-hCD20
B c
ells
per
sq.
mm
total
0
1
2
3
4
5
0 2 4 6 8 10 13 15 17 22 25 27 29 36 39 41 43 49 51 56
Treatment starting at EAE > 2
Isotypeα-hCD20
Days after immunization
0
1
2
3
4
5
0 2 4 6 8 10 12 13 14 15 17 18 20 24 27 33 39 43 48 52 57 63
EA
E s
core
Treatment starting at day -21
Days after immunization
*
* * **
* **
*
**
Isotype
α-hCD20
MOG protein
0
1
2
3
4
5
0 2 4 6 8 10 11 12 13 15 16 19 21 23 26 28 30 33 35 37 41 42 49
EA
E s
core
Isotype
α-hCD20
Treatment starting at day -21
Days after immunization
*
* * * ** *
*
0
0.5
1
1.5
2
2.5
3
0 2 4 6 8 10 11 12 13 15 17 19 25 28 31 33 35 38
Treatment starting at EAE > 2
Isotype
α-hCD20
Days after immunization
**
0
0.5
1
1.5
2
2.5
Inflammation Demyelination
isotype
α-hCD20
0
10
20
30
B c
ells
per
sq.
mm
isotype
α-hCD20
MOG peptide
but exacerbates MOG peptide-induced EAE
Weber, MS et al. Ann Neurol 68:369, 2010

2/16/2012
6
BLyS and APRIL are B cell maturation & survival factors
Bone-marrowenvironment
Tumour environment
B celldifferentiation
APRIL
T cell divisionAntibody-producingplasma cell
ActivatedB cell
RestingB cell
Class switch to IgA or IgGBLyS
Dillon S, et al. Nat Rev Drug Discov 2006;5:235–246
MalignantB cell survival
(Enhanced antigen presentation)
B cellsurvival
B cell division
BLyS and APRIL bind to B cell-expressed receptors
BAFF-R
BCMA TACI
Proteoglycans
B cell
Ligands
Receptors
BLyS APRILBLyS/APRILheterotrimer
ATAMS: Atacicept in MS
� Atacicept: Recombinant fusion protein with immunomodulatory effects on B cells
� ATAMS: 36-week phase II RCT of atacicept25, 75, 150 mg vs placebo (PBO) in relapsing MS
� Mean ARRs were greater in atacicept vsPBO arms (Figure)
� Significantly more T1 Gd+ lesions were observed in atacicept 75 mg (2.64) vs PBO (1.14; P = 0.017) arm
� Effects reversed after atacicept cessation in safety follow-up
� Conclusion: Atacicept was associated with worse outcomes
� Study stopped
P = 0.042
P = 0.015
Statistically significant results for 25 mg and 150 mg groups compared with placebo
Lessons From the B -Cell Experience in MS
• The anti-CD20 trials have revealed that B-cells are central players in the pathogenesis of focal lesions in MS
• The MOA is likely to involve interference with activation of pathogenic T-cells promoted by B-cells via APC or cytokine functions, but many questions remain
• The attractiveness of B cell therapies for MS will likely be determined by their safety profile in phase 3 trials and beyond
• These trials also set the stage for testing more selective therapies that target subsets of B-cells, B-cell growth/survival factors, or germinal center interactions
• More than 15 years will have passed from the initia l proposal to employ anti-CD20 therapy in MS to completion of the pivotal phase 3 trials!

2/16/2012
7
Will the Clinical Landscape of MS Look Different in 2016?
• Many available therapies for RRMS
• Aggressive early treatment is the norm
• Still no antigen-specific therapy on the horizon
• Strategies for primary prevention available
• Exquisite imaging capabilities of the entire neuraxis
• Biomarkers stratify patients for prognosis and treatment
• Fewer patients with progressive MS
• Promising prospects for remyelination (anti-LINGO; Wnt pathway; retinoid X receptor [RXR-γ] signaling)
• Treatment for the neurodegenerative component of MS remains a challenge
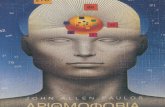
Gene Discovery in MS
A/A
G/G
A/G
First reportedassociation betweenMS and HLA
STUDIES
GENES1972
Separation from common ancestry
HLA
Meta-analysisof GWAS
2009
CD226CD6IRF8TNFRSF1ATYK2
Homo erectusupright man
First generationGWAS (1000 patients)
2007
IL2RAIL7RRPL5CD58CLEC16AEVI5
Homo ergastercommunities
Homo sapiens
VCAMPLEKMERTSP140EOMESCD86IL12BBACH2THEMISMYBIL22RA2TAGAPZNF767MYCPVT1HHEX
CLECL1ZFP36L1BATFGALCMALT1TNFSF14MPV17L2DKKL1MAPK1SCO2NFKB2CXCR5SOX8RPS6KB1TNFRSF6CYP27B1CYP24A1
Whole genomesequencingof MS twins
2010
Second generationGWAS (10,000 patients)
AustralopithecusWalking apes
First generation genome-wide linkage studies (400 markers)
1996
Second generation genome-wide linkage study (5000 markers)
2005
Homo habilisstone tools
MS Susceptibility Genes in T Cell Activation Pathwa ys
International Multiple Sclerosis Genetics Consortium Nature 476:214, 2011
Functional Studies of MS Variants

2/16/2012
8
A Disease-Focused Neuroscience Center at Mission Bay
Thank you!