Ceftazidime–Αvibactam combination: clinical trial data30/3.M... · Double-blind randomisation...
43
M. Antonelli Dept of Anesthesiology and Intensive Care Universita’ Cattolica del Sacro Cuore Fondazione Policlinico Universitario A. Gemelli Ceftazidime–Αvibactam combination: clinical trial data and…a bit more
Transcript of Ceftazidime–Αvibactam combination: clinical trial data30/3.M... · Double-blind randomisation...

M. AntonelliDept of Anesthesiology and Intensive Care
Universita’ Cattolica del Sacro CuoreFondazione Policlinico Universitario A. Gemelli
Ceftazidime–Αvibactam combination: clinical trial data and…a bit more

DisclosuresDisclosures
•
Research grants : Toray, Pfizer, Maquet, Orion, GE, Fisher and Paykel
•
Advisor/consultant: Orion, MSD, Bayer, Basileah
Speaker/chairman: Fisher and Paykel, Orion, Maquet,
Pfizer
The opinions expressed in this presentation belong to the presenter and do not necessarily reflect the views of the company.
For all medicinal products mentioned, please refer to the approved Summaries of Product Characteristics

Ceftazidime–avibactam Phase III clinical trial programme
Seven prospective, international, multicentre, randomised Phase III studies
•
Double-blind randomisation (1:1)
–
CAZ 2000 mg + AVI 500
mg + metronidazole 500 mg IV q8h or
–
MER 1000 mg IV + placebo q8h
•
Primary objective –
RECLAIM 1 and 2:–
Assess non-inferiority of CAZ–AVI re: clinical cure at TOC visit in patients with ≥1 identified pathogen (mMITT populations)
–
RECLAIM 3:–
Proportion of patients with clinical cure at TOC visit (CE populations)
•
Open-label randomisation (1:1)
–
CAZ 2000 mg + AVI 500 mg + metronidazole 500 mg q8h IV or
–
Best available therapy•
Primary objective–
Estimate per-patient clinical response to CAZ–AVI and best available therapy at TOC visit in cUTI and cIAI caused by CAZ-resistant Gram-negative pathogens
•
Double-blind randomisation (1:1)
–
CAZ 2000 mg + AVI 500 mg q8h IV or
–
DOR 500 mg + placebo q8h IV
•
Primary objective –
Assess non-inferiority of CAZ–AVI on co-primary endpoints in mMITT analysis set:
–
Resolution of UTI-
specific symptoms
–
Resolution/improvement of flank pain
–
Per-patient microbiological eradication and symptomatic resolution
•
Double-blind randomisation (1:1)
–
CAZ 2000 mg + AVI 500 mg q8h IV or
–
MER 1000 mg + placebo q8h IV
–
Plus open-label empiric linezolid + aminoglycoside
•
Primary objective–
Assess non-inferiority of CAZ–AVI on clinical cure rate at TOC visit in cMITT and CE populations
RECLAIM 1, 2 and 3: Adults with cIAI
REPRISE Adults with CAZ-resistant
pathogens
REPROVE Adults with nosocomial
pneumonia (including VAP)
RECAPTURE 1 and 2: Adults with cUTI (including acute
pyelonephritis)
AVI, avibactam; CAZ, ceftazidime; CE, clinically evaluable; cIAI, complicated intra-abdominal infection; cUTI, complicated urinary tract infection; DOR, doripenem; IV, intravenous; MER, meropenem; mMITT, microbiological modified intent-to-treat; TOC, test of cure; VAP, ventilator-associated pneumonia.
Presenter
Presentation Notes
Abbreviations AVI, avibactam; CAZ, ceftazidime; CE, clinically evaluable; cIAI, complicated intra-abdominal infection; cMMIT, clinically modified intent-to-treat; cUTI, complicated urinary tract infection; DOR, doripenem; IV, intravenous; MER, meropenem; mMITT, microbiological modified intent-to-treat; q8h, every 8 h; TOC, test of cure; UTI, urinary tract infection; VAP, ventilator-associated pneumonia.

RECAPTURE 1 & 2 Phase III studies in cUTI
Study design
•
Two identically designed, double-blind, double-dummy, randomized, multicenter, parallel-group, non inferiority trials comparing the efficacy and safety of ceftazidime–avibactam with doripenem
•
All data collected from the two trials were combined and analysed as a single pooled dataset EOT
(within 24 h last IV
infusion & before oral)
Doripenem 500mg, 30 min IV infusion, q8h
+ optional oral switch
CAZ–AVI(2000–500 mg, q8h)
+ optional oral switchHospitalized patients aged ≥18
years with cUTI or acute pyelonephritis (min 5 days IV, 10–14*
days IV + oral therapy)
1:1 randomization
Late Follow Up45–52 days
after randomization
21–25 days
after
randomization
Test Of Cure
*Therapy could be extended up to 14 days for bacteremic patients.
cUTI,
complicated urinary tract infection; CAZ–AVI, ceftazidime–avibactam; q8h, every 8 h; EOT, end of treatment; IV, intravenous; TOC, test of cure; LFU, late follow-up. Wagenlehner F, et al. Clin Infect Dis 2016;63:754-62.
Presenter
Presentation Notes
Abbreviations

RECAPTURE 1 & 2 Study endpoints
Primary endpoints–
FDA co-primary endpoints •
The proportion of patients with symptomatic resolution†
(or return to premorbid state) at Day 5 visit (based on PSAQ)
•
The proportion of patients with both a favorable microbiological response and symptomatic
resolution (or return to premorbid state) at TOC
in the mMITT population –
EMA primary endpoint•
The proportion of patients with a favourable per-patient microbiological response (i.e. eradication) at TOC in the mMITT population
•
The sponsor pre-specified non-inferiority margin was –12.5%. The FDA required a non-
inferiority margin of –10%
Key secondary endpoints–
Per-patient microbiological response at EOT (IV) and LFU–
Per-patient and per-pathogen microbiological
response at TOC
and LFU in patients with ≥1 ceftazidime-non-susceptible or only ceftazidime-susceptible pathogens isolated at baseline
–
Investigator-determined clinical cure
at EOT (IV), TOC and LFU –
Sustained clinical cure at LFU–
Safety
assessed by monitoring AEs†
Symptomatic resolution of UTI-specific symptoms, except flank pain, with resolution or improvement in flank pain from baseline at Day 5 visit.
AEs, adverse events; EMA, European Medicines Agency; EOT, end of
treatment; FDA, Food and Drug Administration; IV, intravenous; LFU, late follow-up; mMITT, microbiologically modified intent-to-treat; PSAQ, patient-reported symptom assessment questionnaire; TOC, test of cure.Wagenlehner F, et al. Clin Infect Dis 2016;63:754-62.
Presenter
Presentation Notes
Abbreviations PSAQ, patient-reported symptom assessment questionnaire; TOC, test of cure; mMITT, microbiologically modified intent-to-treat; AEs, adverse events; EOT, end of treatment; LFU, late follow-up; AEs, adverse events.

RECAPTURE 1 & 2 Study design and participants
•
Diagnosis based on +ve urine cultures within 48 h of enrollment showing 1–2 Gram-positive uropathogens and pyuria
•
cUTI without pyelonephritis was defined as presence of >2 symptoms with one UTI-specific symptom as well as one complicating factor
•
Patients were enroled before cultures were obtained if–
Positive results were expected
–
Appropriate antibiotic was considered–
Urine Gram stain showed Gram-negative bacilli
•
Indwelling catheters for >24 h were removed or replaced before baseline urine collection
cUTI,
complicated urinary tract infection; UTI,
urinary tract infection.Wagenlehner F, et al. Clin Infect Dis 2016;63:754–62.

RECAPTURE 1 & 2 Study flow
Patients randomized
n=1033
CAZ–AVI n=516
Doripenem n=517
Safety population n=511 (did not receive
treatment n=5)
mMITT population n=393
Safety population n=509(did not receive
treatment n=8)
mMITT population n=417
Completed TOC visit n=490Completed study n=473
Discontinued n=43 (subject decision n=12, eligibility criteria not fulfilled n=1, lost to follow-up
n=20, other reason=10)
Completed TOC visit n=492 Completed study n=476
Discontinued n=41 (subject decision n=12, eligibility criteria not fulfilled n=6 lost to follow-up
n=20, other reason 3)
CAZ–AVI, ceftazidime–avibactam; mMITT, microbiological modified intent to treat; TOC,
test of cure.Wagenlehner F, et al. Clin Infect Dis 2016;63:754–62.
Presenter
Presentation Notes
Abbreviations CAZ-AVI, ceftazidime-avibactam; mMITT, microbiological modified intent to treat; TOC, test of cure.

RECAPTURE 1 & 2 Baseline characteristics (mMITT)
ParameterCAZ–AVI
(n=393)
Doripenem
(n=417)
Age, years, mean (SD) 54.1 (20.2) 53.3 (18.6)Gender, male, n (%) 121 (30.8) 124 (29.7)Body mass index kg/m2, mean (SD) 26.2 (5.9) 26.3 (5.6)Renal status, n (%)
•
Normal renal function/mild impairment (CrCL >50
mL/min) 350 (89.1) 379 (90.9)•
Moderate impairment (CrCL >31 to ≤50
mL/min) 42 (10.7) 35 (8.4)•
Severe impairment (CrCL <31
mL/min) 1 (0.3) 3 (0.7)White blood cell count, 109/mL, median (range) 8.5 (3.3, 27.8) 7.9 (3.1, 35.4)Bacteremia, n (%) 38 (9.7) 33 (7.9)Diagnosis, n (%)•
cUTI without pyelonephritis 106 (27.0) 121 (29.0)•
Pyelonephritis 287 (73.0) 296 (71.0)–
With ≥1 complicating factor 41 (10.4) 39 (9.4)–
Meeting symptom criteria for cUTI 33 (8.4) 31 (7.4)Baseline pathogen in urine, n(%)1
•
Enterobacteriaceae 376 (95.7) 396 (95.0)–
Escherichia coli 292 (74.3) 306 (73.4)–
Klebsiella pneumoniae 44 (11.2) 56 (13.4)–
Proteus mirabilis 17 (4.3) 13 (3.1)•
Other Gram-negative bacteria 18 (4.6) 21 (5.0)–
Pseudomonas aeruginosa 18 (4.6) 20 (4.8)Prior systemic antibiotic use, n (%) 28 (7.1) 27 (6.5)
19.6% of all baseline pathogens were ceftazidime-non-susceptible 1. Includes pathogens reported with a combined frequency of ≥10 patients. Patients could have >1 pathogen. Multiple isolates of the same species from the same patient are counted only once.
CAZ–AVI, ceftazidime–avibactam; CrCL,
creatinine clearance; cUTI, complicated urinary tract infection;
mMITT,
microbiological modified intent-to-treat; SD, standard deviation.Wagenlehner F, et al. Clin Infect Dis 2016;63:754–62.
Presenter
Presentation Notes
Abbreviations mMITT, microbiological modified intent-to-treat; SD, standard deviation; CrCL, creatinine clearance; cUTI, complicated urinary tract infection.

RECAPTURE 1 & 2 Primary efficacy results (mMITT)
Patients, N (%)
CAZ–AVI
(n=393)
Doripenem
(n=417)
Difference, %
(95% CI)
FDA co-primary endpoints
•
Patient-assessed symptomatic resolution at Day 5 276 (70.2) 276 (66.2) 4.0 (–2.39, 10.42)
•
Combined patient-assessed symptomatic resolution and favourable per-patient microbiological response at TOC
280 (71.2) 269 (64.5) 6.7 (0.30, 13.12)
–
Per-patient favourable microbiological response at TOC 304 (77.4) 296 (71.0) 6.4 (0.33, 12.36)
–
Patient-reported symptomatic resolution at TOC 332 (84.5) 360 (86.3) –1.9 (–6.78, 3.02)
EMA primary endpoint
•
Per-patient favourable microbiological response at TOC 304 (77.4) 296 (71.0) 6.4 (0.33, 12.36)
The sponsor concluded non-inferiority if the lower limit if the 95% at TOC was greater than –12.5%. The FDA inferiority margin was a lower limit of the 95% CI greater than –10.0%. The mMITT population was all randomised patients with a minimum disease criteria and eligible baseline pathogen(s).
CAZ–AVI, ceftazidime–avibactam; CI, confidence interval; EMA, European Medicines Agency; EOT, end of treatment; FDA, Food and Drug Administration; mMITT, microbiological modified intent-to-treat; TOC, test of cure.Wagenlehner F, et al. Clin Infect Dis 2016;63:754–62.

RECAPTURE 1 & 2 Secondary efficacy results (mMITT)
Patients, N (%)CAZ–AVI
(n=393)
Doripenem
(n=417)
Difference, %
(95% CI)
Microbiological
•
Per-patient favourable microbiological response at EOT (IV)
374 (95.2) 395 (94.7) 0.4 (–2.7, 3.56)
•
Per-patient favourable microbiological response at LFU 268 (68.2) 254 (60.9) 7.3 (0.68, 13.81)
•
Per-patient favourable microbiological response at TOC in patients with a ceftazidime-non-susceptible pathogen*
47/75 (62.7) 51/84**
(60.7) 2.0 (–13.18, 16.89)
•
Per-patient favourable microbiological response at LFU in patients with a ceftazidime-non-susceptible pathogen*
46/75 (61.3) 38/84 (45.2) 16.1 (0.50, 30.89)
•
Per-patient favourable microbiological response at TOC in patients with a ceftazidime-susceptible pathogen*
256/316 (81.0) 238/326 (73.0)
8.0 (1.50, 14.48)
•
Per-patient favourable microbiological response at LFU in patients with a ceftazidime-susceptible pathogen*
221/316 (69.9) 209/326 (64.1)
5.8 (–1.46, 13.05)
*Ceftazidime resistance non-susceptibility was defined as a central microbiology reference laboratory MIC ≥8 μg/mL for Enterobacteriaceae or ≥16 μg/mL for P. aeruginosa, or local laboratory disk diffusion diameter (from a 30 μg ceftazidime disk) of ≤20 mm for Enterobacteriaceae and ≤17 mm for P. aeruginosa. Nine patients were not included in either subset (ceftazidime-non-susceptible or ceftazidime-susceptible) because no susceptibility tests were performed (6 patients) or baseline blood or urine susceptibility results were missing (3 bacteraemic patients).**One patient in the doripenem group had 2 ceftazidime-nonsusceptible pathogens isolated at baseline.CAZ–AVI, ceftazidime–avibactam; CI, confidence interval; EOT, end of treatment; IV, intravenous; LFU, late follow-up; mMITT, microbiological modified intent-to-treat; TOC, test of cure.Wagenlehner F, et al. Clin Infect Dis 2016;63:754–62.
Microbiological response rates were higher in CAZ–AVI at all study visits

Favourable response rate, n/N (%)
Secondary endpointCAZ–AVI
(n=393)
Doripenem
(n=417)
Difference, %
(95% CI)
All baseline pathogens
Overall 311/400 (77.8) 297/419 (70.9) 6.9 (0.88, 12.81)
•
Enterobacteriaceae 299/382 (78.3) 281/398 (70.6) 7.7 (1.054, 13.75)
•
P. aeruginosa 12/18 (66.7) 15/20 (75.0) –8.3 (–36.77, 20.66)
Ceftazidime-non-susceptible pathogens
Overall 48/75 (64.0) 51/85 (60.0)* 4.0 (–11.11, 18.81)
•
Enterobacteriaceae 43/68 (63.2) 46/79 (58.2) 5.0 (–10.87, 20.50)
•
P. aeruginosa 5/7 (71.4) 5/6 (83.3) –11.9 (–54.78, 37.60)
Ceftazidime-susceptible pathogens
Overall 254/311 (81.7) 228/312 (73.1) 8.6 (2.03, 15.14)
•
Enterobacteriaceae 247/301 (82.1) 217/297 (73.1) 9.0 (2.32, 16.66)
•
P. aeruginosa 7/10 (70.0) 10/14 (71.4) –1.4 (–38.84, 33.69)
RECAPTURE 1 & 2 Per‐pathogen favourable microbiological response rates at TOC (mMITT)
The sponsor concluded non-inferiority if the lower limit if the 95% at TOC was greater than –12.5%. The FDA inferiority margin was a lower limit of the 95% CI greater than –10.0%.
*One patient in the doripenem group had 2 ceftazidime-nonsusceptible pathogens isolated at baseline
CAZ–AVI, ceftazidime–avibactam; CI, confidence interval; mMITT, microbiological modified intent-to-treat; TOC, test of cure.Wagenlehner F, et al. Clin Infect Dis 2016;63:754–62.
Presenter
Presentation Notes
Abbreviations TOC, test of cure; mMITT, microbiological modified intent-to-treat; CAZ-AVI, ceftazidime-avibactam.

RECAPTURE 1 & 2 Summary of AEs up to LFU (safety
population)
n (%)CAZ–AVI
(n=511)Doripenem
(n=509)Any AE 185 (36.2) 158 (31.0)Any AE leading to death 0 (0.0) 0 (0.0)Any serious AE 21 (4.1) 12 (2.4)Any AE leading to discontinuation 7 (1.4) 6 (1.2)Any AE of severe intensity 10 (2.0) 7 (1.4)
•
Headache was the most frequently reported AE with both ceftazidime–avibactam (7.4%) and doripenem (7.9%)
•
No new safety concerns were identified
AE, adverse event; CAZ–AVI, ceftazidime–avibactam; LFU, late follow-up.Wagenlehner F, et al. Clin Infect Dis 2016;63:754–62.
Presenter
Presentation Notes
Abbreviations AE, adverse effects; CAZ-AVI, ceftazidime-avibactam; LFU, late follow-up.

RECAPTURE 1 & 2 Summary and conclusions
•
Non-inferiority of ceftazidime–avibactam versus doripenem for the treatment of hospitalized patients with cUTI, including acute pyelonephritis
•
Investigator-determined clinical cure rates were 90% across groups, and similar for patients with ceftazidime-non-susceptible and ceftazidime-susceptible pathogens
•
Per-pathogen eradication rates at TOC numerically favored ceftazidime–avibactam over doripenem for all Enterobacteriaceae including the most common ones such as E. coli, Klebsiella and Proteus
•
Ceftazidime–avibactam was generally well-tolerated, and demonstrated a safety profile consistent with that of ceftazidime alone
cUTI, complicated urinary tract infection; TOC, test of cure.Wagenlehner F, et al. Clin Infect Dis 2016;63:754–62.
Presenter
Presentation Notes

RECLAIM studies Phase III studies in cIAI
•
RECLAIM 1* (NCT01499290) –
performed in various countries in Asia, Europe, South America, India, Israel, South Africa and USA1
•
RECLAIM 2* (NCT01500239) –
performed in various countries in Europe, South America, Canada, India, Israel, Thailand and USA1
•
RECLAIM 3 (NCT01726023) –
performed in China, Republic of Korea and
Vietnam2
Study designs and objectives of the three RECLAIM studies were similar
*Because of similar timelines, designs and country enrolment, data from RECLAIM 1 and 2 were combined to form a single publication.
cIAI, complicated intra-abdominal infection.
1. Mazuski JE, et al. Clin Infect Dis. 2016;62:1380–9. 2. Qin X, et al. Int J Antimicrob Agents. 2017;49:579-588.
Presenter
Presentation Notes
Abbreviations NCT, national clinical trial.

RECLAIM 1 & 2 Study design
•
Two identically designed, prospective, randomised, multicentre, double-blind studies comparing the efficacy and safety of ceftazidime–avibactam + metronidazole with meropenem
•
It was pre-specified, with agreement from the FDA and the EMA, for data from the two studies to be combined and analysed as a single pooled dataset
EOT
within 24 h last IV infusion
Meropenem
1000 mg, 30 min IV infusion, q8h
Ceftazidime–avibactam(2000–500 mg, 2 h IV infusion)
+ metronidazole
(500 mg, 60 min IV infusion)
q8hHospitalised patients aged ≥18
years with cIAI requiring hospitalisation (5–14 days of therapy)
1:1 randomisation
42–49 days
after randomisation
28–35 days
after
randomisation
12.5% NI margin(powered for 10.0% NI margin as
required by FDA)
cIAI, complicated intra-abdominal infection; EMA, European Medicines Agency; EOT, end-of-treatment; FDA, Food and Drug Administration; IV, intravenous; LFU, late follow-up; NI, non-inferiority; TOC, test-of-cure.
Mazuski JE, et al. Clin Infect Dis. 2016;62:1380–9.
Late Follow UpTest Of Cure
Presenter
Presentation Notes
Abbreviations

RECLAIM 1 & 2 Study objectives
•
Primary objective–
To assess non-inferiority of ceftazidime–avibactam + metronidazole compared with meropenem
on clinical cure* rate at TOC visit (28–35 days after randomisation) in the mMITT primary analysis population, as required by the FDA, and in the MITT and Clinically evaluabe co-primary analysis populations, as required by the EMA
•
The sponsor pre-specified non-inferiority margin was –12.5%. The FDA required a non-
inferiority margin of –10% for the mMITT population
•
Key secondary objectives–
Clinical response at EOT (up to 24 h after last infusion) and LFU
(42–49 days after randomisation) visits; microbiological responses at each
time point; and efficacy of ceftazidime–avibactam + metronidazole or meropenem against ceftazidime-resistant pathogens
–
Safety and tolerability assessed by monitoring AEs and laboratory
parameters
*Complete resolution or significant improvement of signs and symptoms (no further antimicrobial therapy, drainage or surgical intervention necessary)AE, adverse event; CE, clinically evaluable; EMA, European Medicines Agency; EOT, end-of-treatment; FDA, Food and Drug Administration; LFU, late follow-up; MITT, modified intent-to-treat; mMITT, microbiologically modified intent-to-treat; TOC, test-of-cure.
Mazuski JE, et al. Clin Infect Dis. 2016;62:1380–9.
Presenter
Presentation Notes
Definitions in the trial Clinical cure: complete resolution or significant improvement of signs and symptoms (no further antimicrobial therapy, drainage or surgical intervention necessary). Clinical failure: death related to cIAI; persisting or recurring abdominal infection; post-surgical wound infection requiring antibiotics; any previously met criteria for failure. Indeterminate: patients with inadequate source control, or patients in the mMITT and MITT population who were lost to follow-up or in the case of death where cIAI was non-contributory. Abbreviations

RECLAIM 1 & 2 Analysis populations
1066 patients randomised
Safety population1058 patients
mMITT population Met clinical disease criteria and
≥1 pathogen identified at study entry
823 patientsCeftazidime–avibactam + metronidazole n=413
Meropenem n=410
MITT populationMet clinical disease criteria and received study drug
1043 patientsCeftazidime–avibactam + metronidazole n=520
Meropenem n=523
CE at TOC population Met all evaluability criteria*
826 patientsCeftazidime–avibactam + metronidazole n=410
Meropenem n=416
Primary analysis set required by the FDA
Co-primary analysis sets required by the EMA
Mazuski JE, et al. Clin Infect Dis. 2016;62:1380‐9CE, clinically evaluable; EMA, European Medicines Agency; FDA, Food and Drug Administration; MITT, modified intention-to-treat; mMITT, microbiologically modified intention-to-treat; TOC, test-of-cure.
Mazuski JE, et al. Clin Infect Dis. 2016;62:1380–9.
Presenter
Presentation Notes
Abbreviations

RECLAIM 1 & 2 Baseline patient and disease characteristicsParameter CAZ–AVI + MTZ MER
Patient characteristics (mMITT population) n=520 n=523Age, years, mean (SD) 49.8 (17.5) 50.3 (18.3)
Gender, male, n (%) 326 (62.7) 332 (63.5)Renal status, moderate impairment (CrCL >30–≤50
mL/min), n (%)41 (7.9) 43 (8.2)
APACHE II score, n (%)≤10 437 (84.0) 434 (83.0)>10–≤30 78 (15.0) 80 (15.3)>30 1 (0.2) 0Primary diagnosis, n (%)Cholecystitis 87 (16.7) 77 (14.7)Diverticular disease 35 (6.7) 52 (9.9)Appendiceal perforation or peri-appendiceal abscess 218 (41.9) 213 (40.7)Acute gastric and duodenal perforations 96 (18.5) 99 (18.9)Traumatic perforations 9 (1.7) 8 (1.5)Secondary peritonitis 36 (6.9) 33 (6.3)Intra-abdominal abscess 39 (7.5) 41 (7.8)Single abscess 32 (6.2) 35 (6.7)Bacteraemia, n (%) 22 (4.2) 14 (2.7)Disease characteristics (mMITT population) n=413 n=410CAZ-resistant, n (%) 47 (11.4) 64 (15.6)
APACHE, Acute Physiology and Chronic Health Evaluation; AVI, avibactam; CAZ, ceftazidime; CrCL, creatinine clearance; MER, meropenem; mMITT, microbiological modified intent-to-treat; MTZ, metronidazole; SD, standard deviation.
Mazuski JE, et al. Clin Infect Dis. 2016;62:1380–9.
Presenter
Presentation Notes
Abbreviations APACHE, Acute Physiology and Chronic Health Evaluation; AVI, avibactam; CAZ, ceftazidime; CrCL, creatinine clearance; MER, meropenem; mMITT, microbiological modified intent-to-treat; MTZ, metronidazole; SD, standard deviation.

RECLAIM 1 & 2 Primary efficacy results: Clinical cure at TOC
Analysis population n
Clinical cure rate n/N (%) Between group difference, %
(95% CI)CAZ–AVI
+ MTZ MER
MITT(EMA co-primary analysis population)
1043 429/520 (82.5) 444/523 (84.9) –2.4 (–6.90, 2.10)
CE at TOC(EMA co-primary
analysis population)
826 376/410 (91.7) 385/416 (92.5) –0.8 (–4.61, 2.89)
mMITT(FDA primary
analysis population)
823 337/413 (81.6) 349/410 (85.1) –3.5 (–8.64, 1.58)
% difference in clinical cure rate (95% CI)
Primary efficacy endpoints: CAZ–AVI was non-inferior to MER in all populations
Solid line represents sponsor pre-specified NI margin of –12.5% for the lower limit of the 95% CI. Dashed line represents FDA requirement of –10%AVI, avibactam; CAZ, ceftazidime; CE, clinically evaluable; CI, confidence interval; EMA, European Medicines Agency; EOT, end of
treatment; FDA, Food and Drug Administration; LFU, late follow-up; MER, meropenem; MITT, modified intent-to-treat; mMITT, microbiological modified intent-to-treat; MTZ,
metronidazole; NI, non-inferiority; TOC, test of cure.
Mazuski JE, et al. Clin Infect Dis. 2016;62:1380–9.
Presenter
Presentation Notes
Abbreviations AVI, avibactam; CAZ, ceftazidime; CE, clinically evaluable; CI, confidence interval; EMA, European Medicines Agency; EOT, end of treatment; FDA, Food and Drug Administration; LFU, late follow-up; MER, meropenem; MITT, modified intent-to-treat; mMITT, microbiological modified intent-to-treat; MTZ, metronidazole; NI, non-inferiority; TOC, test of cure.

RECLAIM 1 & 2 Clinical cure at TOC by pathogen (mMITT)CAZ–AVI + MTZ
(n=413)MER
(n=410) Comparison
Pathogen nClinical cure
n (%) n
Clinical cure
n (%)
Difference, %
(95% CI)
All CAZ-R 47 39 (83.0) 64 55 (85.9) –3.0 (–17.89, 10.60)
All CAZ-S 289 237 (82.0) 292 256 (87.7) –5.7 (–11.57, 0.17)
Enterobacteriaceae (CAZ-R) 44 36 (81.8) 62 53 (85.5) –3.7 (–19.31, 10.44)
Enterobacteriaceae (CAZ-S) 279 229 (82.1) 280 245 (87.5) –5.4 (–11.45, 0.54)
Escherichia coli (CAZ-R) 24 19 (79.2) 37 31 (83.8) –4.6 (–26.77, 14.86)
Escherichia coli (CAZ-S) 236 192 (81.4) 239 210 (87.9) –6.5 (–13.09, –0.02)
Klebsiella pneumoniae (CAZ-R) 13 10 (76.9) 13 9 (69.2) 7.7 (–27.10, 40.96)
Klebsiella pneumoniae (CAZ-S) 34 28 (82.4) 35 27 (77.1) 5.5 (–14.43, 24.56)
Non-Enterobacteriaceae
(CAZ-R) 4 4 (100.0) 4 4 (100.0) 0.0 (–52.33, 52.33)
Non-Enterobacteriaceae (CAZ-S) 35 31 (88.6) 43 41 (95.3) –6.8 (–22.10, 5.99)
Pseudomonas aeruginosa (CAZ-R) 2 2 (100.0) 4 4 (100.0) 0.0 (–69.74, 53.54)
Pseudomonas aeruginosa (CAZ-S) 30 27 (90.0) 32 30 (93.8) –3.8 (–20.55, 11.90)
These data suggest AVI restores the efficacy of CAZ against CAZ-resistant pathogens
AVI, avibactam; CAZ, ceftazidime; CAZ-R, ceftazidime-resistant; CAZ-S, ceftazidime-susceptible; CI, confidence interval; MER, meropenem; mMITT, microbiological modified intent-to-treat; MTZ,
metronidazole; TOC, test of cure.
Mazuski JE, et al. Clin Infect Dis. 2016;62:1380–9.
Presenter
Presentation Notes
Abbreviations AVI, avibactam; CAZ, ceftazidime; CAZ-R, ceftazidime-resistant; CAZ-S, ceftazidime-susceptible; CI, confidence interval; MER, meropenem; mMITT, microbiological modified intent-to-treat; MTZ, metronidazole; TOC, test of cure.

RECLAIM 1 & 2 Summary of AEs (safety population)
n (%) CAZ–AVI + MTZ (n=529)
MER (n=529)
Any AE 243 (45.9) 227 (42.9)Any AE leading to death 13 (2.5) 8 (1.5)Any SAE 42 (7.9) 40 (7.6)Any AE leading to discontinuation 14 (2.6) 7 (1.3)
Any AE of severe intensity 30 (5.7) 36 (6.8)
There were no new safety signals and the safety profile of CAZ–AVI + MTZ was comparable with that of CAZ, MTZ and MER alone
AE, adverse event; AVI, avibactam; CAZ, ceftazidime; LFU, late follow-up; MER, meropenem; MTZ,
metronidazole; SAE, serious adverse event.
Mazuski JE, et al. Clin Infect Dis. 2016;62:1380–9.
Presenter
Presentation Notes
Abbreviations

RECLAIM 1 & 2 Conclusions
•
The primary endpoint was met; ceftazidime–avibactam + metronidazole was non-
inferior to meropenem in hospitalized adults with cIAIs
•
Ceftazidime–avibactam + metronidazole was effective against ceftazidime-resistant pathogens
•
The safety and tolerability profile of ceftazidime–avibactam + metronidazole was broadly similar to the known profiles of ceftazidime and metronidazole alone
•
These results support the utilization of ceftazidime–avibactam + metronidazole as a potential alternative to carbapenems in the treatment of cIAI
cIAI, complicated intra-abdominal infection.
Mazuski JE, et al. Clin Infect Dis. 2016;62:1380–9.
Presenter
Presentation Notes
Abbreviations cIAI, complicated intra-abdominal infection.

REPROVE study Phase III study in HAP/VAP
•
Background: The randomised, double-blind, multicenter, Phase III REPROVE study (NCT01808092) compared the efficacy, safety and tolerability of ceftazidime–avibactam versus meropenem in the treatment of adults with nosocomial pneumonia (NP), including ventilator-associated pneumonia (VAP)
•
Material/methods: Adults (18–90 years) with NP, including VAP, were randomised 1:1 to receive ceftazidime–avibactam 2000–500 mg 2-h intravenous (IV) infusions every 8 h (q8h) or meropenem 1000 mg 30-min IV infusions q8h for 7–14 days (doses adjusted for renal function)
NP, nosocomial pneumonia; VAP, ventilator-associated pneumonia. Torres A, et al. OS0603: abstract presented at ECCMID 2017. Vienna, Austria. 22–25 April 2017.
Presenter
Presentation Notes
Slide ID: JE Abbreviations AVI, avibactam; CAZ, ceftazidime; cIAI, complicated intra-abdominal infection; cUTI, complicated urinary tract infection; NCT, national clinical trial; VAP, ventilator-associated pneumonia. References Lucasti C et al. Comparative study of the efficacy and safety of ceftazidime/avibactam plus metronidazole versus meropenem in the treatment of complicated intra-abdominal infections in hospitalized adults: results of a randomized, double-blind, Phase II trial. Antimicrob Chemother. 2013;68:1183–1192. Vazquez JA et al. Efficacy and safety of ceftazidime-avibactam versus imipenem-cilastatin in the treatment of complicated urinary tract infections, including acute pyelonephritis, in hospitalized adults: results of a prospective, investigator-blinded, randomized study. Curr Med Res Opin. 2012;28:1921–1931. Nicolau DP et al. Concentration of avibactam (AVI) and ceftazidime (CAZ) in plasma and epithelial lining fluid (ELF) in healthy volunteers. Poster A-1027 presented at ICAAC 2013, Denver, USA. NCT01808092. Highlighted references: Bullet 1: Cerexa FDA Briefing Package. NDA 206494. December 2014. Accessed January 2015 [www.fda.gov Cerexa_CAZ-AVI for Injection]. p10. paragraph 2. �Bullet 2: Lucasti C et al. J Antimicrob Chemother. 2013;68:1183–1192. p1. (abstract); Vazquez JA et al. Curr Med Res Opin. 2012;28:1921–1931. p1. (abstract).�Bullet 2 (sub-bullet): Nicolau D et al. ICAAC 2013 Poster A-1027. Abstract. �Bullet 3: NCT01808092 p1.�Bullet 3 (sub-bullet): NCT01808092 p2, p3.

REPROVE study Endpoints
•
The primary endpoint was assessment of non‐inferiority of ceftazidime–avibactam compared with meropenem in clinical cure at
TOC visit, 21–25 days from randomisation, in the clinically modified intent‐to‐treat (cMITT) population (minimal disease criteria excluding
patients with only non‐target pathogens) and the clinically evaluable (CE) subset of the cMITT, based on a 12.5% non‐inferiority margin
•
Secondary endpoints included clinical cure at TOC by ceftazidime susceptibility of baseline isolates (mMITT and CE populations), per‐ pathogen favourable microbiological response at TOC (mMITT and eME populations) and
all‐cause mortality at Day 28 (cMITT and CE populations)
CE, clinically evaluable; cMITT, clinically modified intention to treat; eME, extended microbiologically evaluable; EOT, end of treatment; MDR, multi-drug resistant; TOC, test of cure; VAP, ventilator-associated pneumonia. mMITT microbiologically modified intention
to treat; Torres A, et al. OS0603: abstract presented at ECCMID 2017. Vienna, Austria. 22–25 April 2017.
Presenter
Presentation Notes
Slide ID: LE PK will also be assessed as a secondary objective. Additional exploratory objectives include: To explore the timing of the resolution of signs and symptoms for patients receiving CAZ-AVI versus MER. To assess the consequence of first-line treatment failure in the treatment of patients with nosocomial pneumonia, as defined by clinical outcomes and resource utilisation. To understand the relationship between the lack of response/improvement in patients’ signs and symptoms, and their changes in clinical care. MITT analysis set All randomised patients who met minimum disease requirements and received any amount of IV study therapy. mMITT analysis set This is a subset of the MITT analysis set. Patients who had a properly obtained respiratory culture demonstrating Gram-negative pathogens, excluding patients not expected to respond to either study drug (i.e. patients with only the following monomicrobial Gram-negative infections: any of the Acinetobacter species; or any Legionella species; or S. maltophilia; or E. meningoseptica). (If baseline respiratory cultures were not available or did not identify a respiratory pathogen, but a Gram-negative organism known to cause pneumonia was identified from baseline blood cultures, the patient would qualify for the mMITT population.) cMITT analysis set This is a subset of the MITT analysis set. Patients whose baseline respiratory cultures demonstrated Gram-negative respiratory pathogens with or without concomitant Gram-positive pathogens (excluding patients with Gram-negative pathogens not expected to respond to either study drug [i.e. patients with only the following monomicrobial Gram-negative infections: any of the Acinetobacter species; or any Legionella species; or S. maltophilia; or E. meningoseptica]); or patients in whom no aetiologic pathogens were identified. CE analysis set This is a subset of the cMITT analysis set and is defined separately for each of the EOT and TOC visits. Patients who received an adequate course of treatment defined as either: Received therapy for ≥48 h, with ≥80% of the scheduled drug administered over the number of days administered, or Received therapy <48 h before discontinuing treatment due to an AE. Patients who were found to have a clinical response of success or failure (i.e. excluding indeterminates) within the protocolled visit window, for the respective EOT and TOC visits. Patients with no important protocol deviations that would affect assessment of efficacy. Patients who did not receive prior antibiotics other than those outlined as acceptable in the protocol between the time of randomisation and the time of the respective EOT and TOC visits. Patients who did not receive concomitant antibiotic therapy with potential activity against the baseline pathogen, except for protocol allowed antibiotics. If no baseline pathogen was identified, receipt of any concomitant antibiotic other than those outlined in the protocol would exclude the patient from the CE analysis set. ME analysis set This is a subset of the CE analysis set and is defined separately for each of the EOT and TOC visits. Patients who had at least one aetiologic pathogen from an adequate baseline culture that is susceptible to both study agents (CAZ-AVI and MER). Abbreviations AEs, adverse effects; AVI, avibactam; CAZ, ceftazidime; CE, clinically evaluable; cMMIT, clinically modified intent-to-treat; E. meningoseptica, Elizabethkingia meningoseptica; ECG, electrocardiogram; EOT, end of treatment; ME, microbiologically evaluable; MER, meropenem; MITT, microbiological modified intent-to-treat; mMITT, microbiological modified intent-to-treat; IV, intravenous; PK, pharmacokinetic; S. maltophilia, Stenotrophomonas maltophilia; SAEs, serious adverse effects; TOC, test of cure; VAP, ventilator-associated pneumonia. Highlighted references: Bullet 1: NCT01808092. p1. (purpose).�Bullet 2–6: NCT01808092. p1–2. (purpose).�Bullet 7: NCT01808092. p2. (purpose) .

REPROVE study Baseline characteristics
•
April 2013 ‐December 2015, 879 patients randomised in 23 countries, excluding 62 patients with moderate/severe renal impairment (CrCL 16–50
mL/min) recruited prior to a protocol amendment to the dose regimen for patients with moderate/severe renal impairment
•
405 patients received ceftazidime–avibactam and 403 meropenem (9 patients received no study treatment)
•
Baseline characteristics were well‐matched between treatment arms •
107/808 (13.2%) patients had an APACHE score ≥20 and 280/808
(34.7%) had VAP•
Predominant Gram‐negative pathogens isolated at baseline in the
microbiologically MITT population were Klebsiella pneumoniae (36.6%) and Pseudomonas aeruginosa (29.6%): 100/355 (28.2%)
patients had ≥1 ceftazidime non‐susceptible isolate
APACHE, Acute Physiology and Chronic Health Evaluation; CrCL, creatinine clearance level; VAP, ventilator-associated pneumonia.
Torres A, et al. OS0603: abstract presented at ECCMID 2017. Vienna, Austria. 22–25 April 2017.

REPROVE study Primary efficacy endpoint*
Patients, n/N (%)Ceftazidime–
avibactam Meropenem Difference, %
(95% CI)Clinical cure at TOCcMITT population 245/356 (68.8) 270/370 (73.0) –4.2 (–10.76,2.46)
VAP 83/118 (70.3) 95/128 (74.2) –3.9 (–15.11,7.31)Non-VAP 162/238 (68.1) 175/242 (72.3) –4.2 (–12.41,3.95)
CE population 199/257 (77.4) 211/270 (78.1) –0.7 (–7.86,6.39)VAP 62/80 (77.5) 63/83 (75.9) 1.6 (–11.55,14.63)Non-VAP 131/177 (77.4) 148/187 (79.1) –1.7 (–10.30,6.75)
*No formal statistical analysis was performed on subgroups or secondary endpoints CE, clinically evaluable; CI, confidence interval; cMITT, clinically modified intention to treat; TOC, test of cure; VAP, ventilator-associated pneumonia. Torres A, et al. OS0603: abstract presented at ECCMID 2017. Vienna, Austria. 22–25 April 2017.
Presenter
Presentation Notes
Slide ID: LE PK will also be assessed as a secondary objective. Additional exploratory objectives include: To explore the timing of the resolution of signs and symptoms for patients receiving CAZ-AVI versus MER. To assess the consequence of first-line treatment failure in the treatment of patients with nosocomial pneumonia, as defined by clinical outcomes and resource utilisation. To understand the relationship between the lack of response/improvement in patients’ signs and symptoms, and their changes in clinical care. MITT analysis set All randomised patients who met minimum disease requirements and received any amount of IV study therapy. mMITT analysis set This is a subset of the MITT analysis set. Patients who had a properly obtained respiratory culture demonstrating Gram-negative pathogens, excluding patients not expected to respond to either study drug (i.e. patients with only the following monomicrobial Gram-negative infections: any of the Acinetobacter species; or any Legionella species; or S. maltophilia; or E. meningoseptica). (If baseline respiratory cultures were not available or did not identify a respiratory pathogen, but a Gram-negative organism known to cause pneumonia was identified from baseline blood cultures, the patient would qualify for the mMITT population.) cMITT analysis set This is a subset of the MITT analysis set. Patients whose baseline respiratory cultures demonstrated Gram-negative respiratory pathogens with or without concomitant Gram-positive pathogens (excluding patients with Gram-negative pathogens not expected to respond to either study drug [i.e. patients with only the following monomicrobial Gram-negative infections: any of the Acinetobacter species; or any Legionella species; or S. maltophilia; or E. meningoseptica]); or patients in whom no aetiologic pathogens were identified. CE analysis set This is a subset of the cMITT analysis set and is defined separately for each of the EOT and TOC visits. Patients who received an adequate course of treatment defined as either: Received therapy for ≥48 h, with ≥80% of the scheduled drug administered over the number of days administered, or Received therapy <48 h before discontinuing treatment due to an AE. Patients who were found to have a clinical response of success or failure (i.e. excluding indeterminates) within the protocolled visit window, for the respective EOT and TOC visits. Patients with no important protocol deviations that would affect assessment of efficacy. Patients who did not receive prior antibiotics other than those outlined as acceptable in the protocol between the time of randomisation and the time of the respective EOT and TOC visits. Patients who did not receive concomitant antibiotic therapy with potential activity against the baseline pathogen, except for protocol allowed antibiotics. If no baseline pathogen was identified, receipt of any concomitant antibiotic other than those outlined in the protocol would exclude the patient from the CE analysis set. ME analysis set This is a subset of the CE analysis set and is defined separately for each of the EOT and TOC visits. Patients who had at least one aetiologic pathogen from an adequate baseline culture that is susceptible to both study agents (CAZ-AVI and MER). Abbreviations AEs, adverse effects; AVI, avibactam; CAZ, ceftazidime; CE, clinically evaluable; cMMIT, clinically modified intent-to-treat; E. meningoseptica, Elizabethkingia meningoseptica; ECG, electrocardiogram; EOT, end of treatment; ME, microbiologically evaluable; MER, meropenem; MITT, microbiological modified intent-to-treat; mMITT, microbiological modified intent-to-treat; IV, intravenous; PK, pharmacokinetic; S. maltophilia, Stenotrophomonas maltophilia; SAEs, serious adverse effects; TOC, test of cure; VAP, ventilator-associated pneumonia. Highlighted references: Bullet 1: NCT01808092. p1. (purpose).�Bullet 2–6: NCT01808092. p1–2. (purpose).�Bullet 7: NCT01808092. p2. (purpose) .

REPROVE study Secondary efficacy endpoints*
Patients, n/N (%)Ceftazidime–avibactam Meropenem Difference, % (95% CI)
Clinical cure at TOC by ceftazidime susceptibility of baseline isolates**
mMITT population
Ceftazidime-non-susceptible 35/45 (77.8) 40/54 (74.1) 3.7 (–13.73,20.38)
Ceftazidime-susceptible 80/119 (67.2) 96/126 (76.2) –9.0 (–20.17,2.33)
CE population
Ceftazidime-non-susceptible 29/36 (80.6) 32/41 (78.0) 2.5 (–16.42,20.74)
Ceftazidime-susceptible 63/84 (75.0) 69/88 (78.4) –3.4 (–16.18,9.30)
Per-pathogen favourable microbiological response at TOCmMITT population
K. pneumoniae 37/59 (62.7) 53/71 (74.6) –11.9 (–27.76,4.03)
P. aeruginosa 22/58 (37.9) 18/47 (38.3) –0.4 (–19.01,17.98)
eME population
K. pneumoniae 29/37 (78.4) 39/49 (79.6) –1.2 (–19.60,15.96)
P. aeruginosa 18/42 (42.9) 14/35 (40.0) 2.9 (–19.13, 24.32)
All-cause mortality at Day 28
cMITT population 30/356 (8.4) 27/370 (7.3) 1.1 (–2.84,5.18)
CE population 12/257 (4.7) 9/270 (3.3) 1.3 (–2.14,5.04)
*No formal statistical analysis was performed on subgroups or secondary endpoints. **Ceftazidime-non-susceptible includes both the CLSI-breakpoint-defined ceftazidime resistant and intermediate categories (i.e., MIC ≥8 mg/L for Enterobacteriaceae and ≥16 mg/L for P. aeruginosa or disk diffusion diameters ≤20 mm for Enterobacteriaceae and ≤17 mm for P. aeruginosa from local laboratory )
CE, clinically evaluable; CI, confidence interval; eME, extended
microbiologically evaluable; cMITT, clinically modified intention to treat; mMITT, microbiologically modified intention to treat; MIC, minimal inhibitory concentration; TOC, test of cure.
Torres A, et al. OS0603: abstract presented at ECCMID 2017. Vienna, Austria. 22–25 April 2017.

REPROVE study Results
•
Ceftazidime–avibactam was non-inferior to meropenem for the primary endpoint of clinical cure at test-of-cure in the cMITT (p=0.007) and CE (p<0.001) populations
•
Subgroup analyses in non-VAP and VAP patients were consistent with the primary analysis
•
Efficacy of ceftazidime-avibactam against ceftazidime-non- susceptible pathogens was similar to that against ceftazidime- susceptible pathogens and was also comparable
to meropenem•
The adverse event rate with ceftazidime-avibactam was 74.6%
versus 74.2% with meropenem; serious adverse event rates were 18.5% and 13.4%, respectively. The most frequent adverse event in both treatment arms was diarrhea
CE, clinically evaluable; cMITT, clinically modified intention to treat; EOT, end of treatment; MDR, multi-drug resistant; mMITT, microbiologically modified intention to treat; TOC, test of cure; VAP, ventilator-associated pneumonia.
Torres A, et al. OS0603: abstract presented at ECCMID 2017. Vienna, Austria. 22–25 April 2017.

REPROVE Conclusions
•
Ceftazidime–avibactam was effective in the treatment of NP, including VAP, as demonstrated by non-inferiority to meropenem in both co-primary cMITT and CE populations
•
Safety and tolerability observations were consistent with the known profile of ceftazidime–avibactam
CE, clinically evaluable; cMITT, clinically modified intention to treat; NP, nosocomial pneumonia; VAP, ventilator-associated pneumonia. Torres A, et al. OS0603: abstract presented at ECCMID 2017. Vienna, Austria. 22–25 April 2017.

REPRISE
Phase III study in ceftazidime-resistant pathogen infections Study design
•
Pathogen-directed, prospective, open-label, randomized, multicenter study•
333 patients ≥18 years of age with a definitive diagnosis of cUTI or cIAI caused by a ceftazidime-resistant, Gram-negative pathogen
•
Patients randomized 1:1 (stratified by entry diagnosis [cIAI or cUTI] and region) to receive either:–
Ceftazidime 2000 mg + avibactam 500 mg (+ metronidazole 500 mg for cIAI) IV q8h, or–
BAT (meropenem, imipenem, doripenem, tigecycline or colistin) based on the investigator’s standard of care and local resistance panel
EOT
(within 24 h of last IV infusion)
Best Available Therapy(as specified and
documented
beforerandomization)
Ceftazidime–avibactam (+ metronidazole if cIAI)
(2000 mg ceftazidime–500 mg avibactam)Hospitalized patients
aged ≥18 years with cIAI or cUTI caused by a
ceftazidime-resistant Gram-negative pathogen
(5–21 days of IV therapy)
1:1 randomization
Test Of Cure
28–35 days
7–10 days
after last infusion
Follow-up 1
cUTI:
cIAI:
Follow-up 1
21–25 days
after randomized28–32 days
Follow-up 2
Choice of BAT documented
by investigator
BAT, best available therapy; cIAI, complicated intra-abdominal infection; cUTI, complicated urinary tract infection; EOT, end of treatment.Carmeli Y, et al. Lancet Infect Dis. 2016;16:661–73.
Presenter
Presentation Notes
Abbreviations BAT, best available therapy; cIAI, complicated intra-abdominal infection; cUTI, complicated urinary tract infection; EOT, end of treatment; IV, intravenous; q8h, every 8 h; TOC, test of cure.

REPRISE Baseline characteristics (mMITT)
cUTI cIAI
Ceftazidime–
avibactam (n=144)
BAT
(n=137)
Ceftazidime–
avibactam
+ metronidazole
(n=10)
BAT
(n=11)
Age, years; mean (SD) 64.3 (14.6) 61.3 (15.3) 49.9 (16.1) 68.4 (11.1)
Female, n (%) 64 (44.4) 63 (46.0) 6 (60.0) 4 (36.4)
Race, n (%)
•
White 136 (94.4) 131 (95.6) 9 (90.0) 11 (100)
•
Other* 8 (5.6) 6 (4.4) 1 (10.0) 0
Body mass index, kg/m2; mean
(SD) 28.1 (5.5) 28.0 (5.8) 25.2 (6.3) 28.6 (4.6)
Renal status, CrCL; mL/min, n (%)
•
>50 118 (81.9) 113 (82.5) 10 (100) 6 (54.5)
•
31–50 19 (13.2) 18 (13.1) 0 3 (27.3)
•
16–30 4 (2.8) 5 (3.6) 0 2 (18.2)
•
6–15 3 (2.1) 1 (0.7) 0 0
*Black or African American, Asian, or other.
BAT, best available therapy; cIAI, complicated intra-abdominal infection; CrCL,
creatinine clearance; cUTI, complicated urinary tract infection;
mMITT,
microbiological modified intent-to-treat; SD, standard deviation.Carmeli Y, et al. Lancet Infect Dis. 2016;16:661–73.
Presenter
Presentation Notes
Abbreviations BAT, best available therapy; cIAI, complicated intra-abdominal infection; CrCL, creatinine clearance; cUTI, complicated urinary tract infection; mMITT, microbiological modified intent-to-treat; SD, standard deviation.

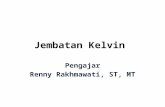
Susceptibilities of 314 Enterobacteriaceae isolates from the REPRISE study
MIC, minimum inhibitory concentration.
Stone GG, et al. Antimicrob Agents Chemother. 2017;61.pii: e01820-16.

cUTI diagnosisOpen‐label Phase III study of ceftazidime–avibactam and best ‐available‐therapy
(97% carbapenems) in patients with cIAI or cUTI caused by ceftazidime‐resistant Gram‐negative pathogens
BAT, best available therapy; cIAI, complicated intra-abdominal infection; cUTI,
complicated urinary tract infection; SD, standard deviation. Carmeli Y, et al. Lancet Infect Dis. 2016;16:661–73.
cUTI
Ceftazidime–avibactam (n=144)
BAT
(n=137)
Age, years; mean (SD) 64.3 (14.6) 61.3 (15.3)
Female, n (%) 64 (44.4) 63 (46.0)
cUTI diagnosis
Acute pyelonephritis 57 (40) 70 (51)
cUTI without pyelonephritis 87 (60) 67 (49)
Complicating factors
Partial obstructive uropathy 45 (31) 21 (15)
Abnormality of urogenital tract 39 (27) 38 (28)
Male with urinary retention 33 (23) 24 (18)
Catheterization 30 (21) 25 (18)
Urogenital procedure within 7 days 27 (19) 21 (15)

REPRISE: ceftazidime-resistant pathogens study
Open‐label Phase III study of ceftazidime–avibactam and best ‐
available‐therapy (97% carbapenems)
in
patients
with
cIAI
or
cUTI
caused
by
ceftazidime‐resistant
Gram‐
negative pathogens
Microbiological response rate (%)
126/154 (82%) 94/148
(64%)
118/144 (82%)
88/137 (64%)
cUTI+cIAI
cUTI
140/154 (91%)
135/148 (91%)
132/144 (92%)
129/137
(94%)
n/N (%) n/N (%)
cIAI
Clinical response rate (%)0 20 30 40 50 60 70 10080 9010
8/10 (80%)
6/11 (55%)
0 20 30 40 50 60 70 10080 9010
8/10 (80%) 6/11 (55%)
Clinical response rate (90% CI) at TOCPer-patient favourable microbiological response
rate* (95% CI) at TOC
Ceftazidime–avibactam BAT
*Presumed from clinical response.
BAT, best available therapy; CI, confidence interval; cIAI, complicated intra-abdominal infection; cUTI, complicated intra-abdominal infection; mMITT, microbiological modified intent-to-treat; TOC, test of cure.Carmeli Y, et al. Lancet Infect Dis. 2016;16:661–73.

REPRISE Per-pathogen microbiological response at TOC
(in cUTI in mMITT population)
Favourable microbiological response rate (%) with 95% CI0 20 10040 60 80
OverallEnterobacteriaceae
Citrobacter freundii complexEnterobacter aerogenes
Enterobacter cloacaeEscherichia coli
Klebsiella oxytocaKlebsiella ozaenae
Klebsiella pneumoniaeMorganella morganii
Proteus mirabilisProteus rettgeri
Providencia stuartiiRaoultella terrigena
Serratia marcescensOther than Enterobacteriaceae
Ochrobactrum anthropiPseudomonas aeruginosa
0 20 10040 60 80
(118/144) 82% vs (88/137) 64%
(2/3) 67% vs (0/2) 0%
(5/8) 63% vs (5/6) 83%(52/59) 88% vs (38/57) 67%(0/0) NC vs (1/2) 50% (0/0) NC vs (1/1) 100%(46/55) 84% vs (43/65) 66% (1/1) 100% vs (0/0) NC(2/5) 40% vs (0/1) 0%(0/0) NC vs (0/1) 0%(1/1) 100% vs (0/0) NC(0/0) NC vs (1/1) 100%(0/0) NC vs (1/2) 50%
(1/1) 100% vs (0/0) NC(11/14) 79% vs (3/5) 60%
CAZ–AVI BAT
(1/1) 100% vs (0/0) NC
CAZ–AVI: BAT
Favourable microbiological response rates for the most common pathogens isolated in cUTI patients were higher in the ceftazidime–avibactam group than in the best available
therapy group (88% vs 67%, respectively for E. coli, and 84% vs 66% for K. pneumoniae)
BAT, best available therapy; CAZ–AVI, ceftazidime–avibactam; cUTI, complicated intra-abdominal infection; mMITT, microbiological modified intent-to-treat; NC, not calculated; TOC, test of cure.
Carmeli Y, et al. Lancet Infect Dis. 2016;16:661–73.
Presenter
Presentation Notes
Abbreviations BAT, best available therapy; CAZ-AVI, ceftazidime-avibactam; cUTI, complicated intra-abdominal infection; mMITT, microbiological modified intent-to-treat; NC, not calculated.

REPRISE Summary of AEs up to the late follow-up visit (safety
population)
n (%) CAZ–AVI (n=164) BAT (n=168)Any AE 51 (31.1) 66 (39.3)Any AE considered related to study drug 14 (8.5) 11 (6.5)Any AE leading to death 3 (1.8) 4 (2.4)Deaths considered related to study drug 0 (0.0) 0 (0.0)Any SAE 9 (5.5) 10 (6.5)Any AE leading to discontinuation 1 (0.6) 2 (1.2)
•
Gastrointestinal disorders were the most frequently reported AEs
with both ceftazidime–avibactam (12.8%) and BAT (17.9%)
•
No new, significant or unexpected safety concerns were identified
AE, adverse events; BAT, best available therapy; CAZ–AVI, ceftazidime–avibactam; SAE, serious adverse event.
Carmeli Y, et al. Lancet Infect Dis. 2016;16:661–73.
Presenter
Presentation Notes
Abbreviations

REPRISE Summary and conclusions
•
Treatment of serious ceftazidime-resistant Gram-negative cUTI with ceftazidime–avibactam achieved
–
Similar clinical cure rates to treatment with BAT–
Numerically higher per-patient microbiological response rates than BAT
•
In cIAI, clinical and microbiological response rates were high for ceftazidime–avibactam and similar to BAT
–
Interpretation of the findings is limited by the small number of patients•
Safety and tolerability profile of ceftazidime–avibactam was broadly similar to ceftazidime alone
•
The REPRISE study is the first pathogen-directed clinical trial for ceftazidime–avibactam examining its efficacy against ceftazidime-resistant Gram-negative pathogens
•
These results support the use of ceftazidime–avibactam as a potential alternative to carbapenems in patients with resistant Gram-negative infections
BAT, best available therapy; cIAI, complicated intra-abdominal infection; cUTI,
complicated intra-abdominal infection.Carmeli Y, et al. Lancet Infect Dis. 2016;16:661–73.
Presenter
Presentation Notes
Abbreviations BAT, best available therapy; cIAI, complicated intra-abdominal infection; cUTI, complicated intra-abdominal infection.

A difficult case…
•
Male, Age 47•
Calculous cholecystitis
•
Necrotic haemorrhagic pancreatitis•
4 episodes of septic shock
•
Multiple vascular thrombosis•
Bleeding from multiple
pseudoaneurysm of left hepatic artery•
Multiple abdominal abscesses
•
KPC Klebsiella pneumoniae isolation from abdominal infected collections


Positive blood cultures
ID/ AST
Sub cultures
Gram staining
Direct MALDI-TOF MS
Eazyplex Amplex for resistance genes
detection
FilmArray if polymicrobial
Treating physician
Day
2
Microbiology Lab Blood cultures workflow
Day
1



Last episode of septic shock solved