Transitioning from conventional TBNA to EBUS-TBNA · Good for inferior mediastinum, station 5 and 6...
46
Transitioning from conventional TBNA to EBUS-TBNA Η μετάβαση από τη συμβατική στην υπερηχογραφικά καθοδηγούμενη ΤΒΝΑ Θ. Κοντακιώτης
Transcript of Transitioning from conventional TBNA to EBUS-TBNA · Good for inferior mediastinum, station 5 and 6...
Transitioning from conventionalTBNA to EBUS-TBNA
Η μετάβαση από τη συμβατική στην υπερηχογραφικά καθοδηγούμενη
ΤΒΝΑΘ Κοντακιώτης
SESSION II Invasive approach of the mediastinum Επεμβατική προσέγγιση του μεσοθωρακίου
Πρόεδροι Δ Χλωρός Ι Μπουκοβίνας Ι Άντζελbull 1030 - 1045 Video-assisted mediastinoscopy for mediastinal staging of lung cancer bull Η συμβολή της video-μεσοθωρακοσκόπησης στη σταδιοποίηση του καρκίνου του
πνεύμονα bull Χ Φορούλης
bull 1045 - 1100 Interesting cases presentation Παρουσίαση ενδιαφερόντων περιστατικών bull Δ Φιλίππου
bull 1100 - 1115 Transitioning from conventional TBNA to EBUS-TBNA bull Η μετάβαση από τη συμβατική στην υπερηχογραφικά καθοδηγούμενη ΤΒΝΑ bull Θ Κοντακιώτης
bull 1115 - 1130 EBUS-TBNA Practical tips EBUS-TBNA Πρακτικές συμβουλές bull Ν Παπανικολάου 1130 - 1145
bull 1145 - 1200 Comments Σχολιασμός bull Σχολιαστές Α Κλέωντας Δ Οικονόμου Ε Διαμαντίδουbull Question and Answer Session bull Ερωτήσεις amp Απαντήσεις
Conventional TBNA
bull Although the conventional TBNA technique has been available for almost three decades its use in routine clinical practice has only
been adopted by a minority (10-15) of pulmonologists for mediastinal nodal staging of patients with potentially resectablestage I-III lung cancer
bull Major reasons for its underuse are its dependency on nodal size (gt15-20 mm short axis on CT scan) and operator skills
bull Meta-analyses reported a sensitivity of 78 and a false negative rate of 28 for conventional TBNA in clinical N2 disease with high disease prevalence of 81 (1213) A conventional blind TBNA is useful if it leads to proof of N3 disease but too often does not exclude N3 disease in cases of proven N2 disease
Bronchoscopic findings in lung cancer diagnostic yield of specimen collection method compared to histological typeT Kontakiotis N Manolakoglou F Zoglopitis L Sakkas D Iakovidis A Mandali P Argyropoulou
Παρουσιάστηκε στο 15ο συνέδριο της European Respiratory Society 17-21 Σεπτεμβρίου 2005 Thematic Poster Session Diagnostic procedures staging of lung cancer and screening Δημοσιεύτηκε στον τόμο των πρακτικών Eur Respir J Suppl vol 26 suppl 49 Σελ P3458
bull Περίληψη From 111995 to 31122004 16816 bronchoscopies were performed in the General Hospital ldquoG Papanikolaourdquo 13779 (819) males (M) and 3037 (181) females (F)) According to histological (forceps biopsy) andor cytological analysis (Transbronchial needle aspiration (TBNA) andor brushing) 5684 (338) were proved to be positive for lung cancer (5192 (913) (M) and 492 (87) (F)) Most of these patients 2451 (431) had squamous cell carcinoma (SqCC) 1230 (216) had adenocarcinoma (AD) 1191 (21) had small cell carcinoma (SCLC) and 813 (143) subjects were sorted as ldquoother histological typesrdquo Best diagnostic yield for SqCC was observed in biopsy specimen (85) (p=0000) especially when the lesion was located in the left main bronchus (941) On the other hand best diagnostic yield for AD was observed for TBNA (754) (p=0001) especially when lesion was located in trachea (917) and for SCLC biopsy (854) (p=0000) especially for lesions in the left main bronchus (957) The percentage of the only one positive method when all the three methods of specimen collection were used was for biopsy 116 for TBNA 65 and for brushing 57 (p=0000) Conclusively SqCC is the most frequent histologic type of lung cancer followed by AD Bronchoscopic biopsy has the best yield followed by TBNA for the final diagnosis
J Thorac Dis 2014 May 6(5) 416ndash420
TBNA with and without EBUS a comparative efficacy study for the
diagnosis and staging of lung cancerJunhong Jiang1 Robert Browning2 Noah Lechtzin3 Jianan Huang1 Peter Terry3 and Ko Pen Wang 13
TBNA MethodDiagnosedtotal malignant cases
Percent yield ()
c-TBNA 6483 771
EBUS 6283 747
MethodsA total of 287 patients with mediastinal and hilar lymphadenopathy presenting for diagnosis andor staging of lung cancer at enrolling institutions were included Equal numbers of punctures were performed at the target lymph node stations using conventional TBNA techniques followed by EBUS-TBNA at the same sites Patients and puncture sites that were biopsied by both methods and were positive for lung cancer were compared to establish efficacy of each technique on the same patients
Conclusions
Recommendations for current practice depend on individual centers and bronchoscopist comfort level with TBNA (with or without EBUS) In our study no significant difference was seen between the techniques for the diagnosis and staging of individual patients
Indications for conventional transbronchial needle aspiration
bull Mediastinal andor hilar lymphadenopathybull Staging of lung cancer or suspect of lung cancer mainly to
prove unresectability Sarcoidosis lymphoma PTLDbull Extrinsic compression of the airway by a peribronchial
lesion or a lymphadenopathybull Submucosal diseasePeripheral nodules or masses negative
bronchus sign (Tsuboi type IV)bull Endobronchial tumors (necrotic or hemorrhagic tumors)bull Diagnosisdrainage of mediastinal cysts or abscesses
bull PTLD post transplant lymphoproliferative disorder
Elif Kuumlpeli Conventional transbronchial needle aspiration in community practice
J Thorac Dis 2015 Dec 7(Suppl 4) S256ndashS265
Assoc Prof FCCPAnkara Turkey Email mocoohayilepukfile
RESULTSOur analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90
lymph nodes were smaller than 100 mm The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929 The most common histological diagnosis was adenocarcinoma
Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Sebastiaacuten Fernaacutendez-Bussy Gonzalo Labarca Sofia Canals Ivaacuten Caviedes Erik Folch Adnan MajidJ Bras Pneumol 2015 May-Jun 41(3) 219ndash224
J Bronchology Interv Pulmonol 2012 Jul19(3)182-7 doi Comparative cost analysis of endobronchial ultrasound-guided and blind
TBNA in the evaluation of hilar and mediastinal lymphadenopathyGrove DA1 Bechara RI Josephs JS Berkowitz DM
bull BACKGROUND bull The superior accuracy of endobronchial ultrasound (EBUS) averts many diagnostic surgical procedures This
likely leads to significant cost savings despite an increased per procedure cost We sought to compare the true costs of endobronchial ultrasound-transbronchial needle aspiration (EBUS-TBNA) compared with blind fiberoptic bronchoscopy-transbronchial needle aspiration (FB-TBNA) factoring in the impact of diagnostic surgical procedures in the diagnosis of mediastinal lymphadenopathy
bull METHODS bull In this retrospective case study we selected 294 patients with thoracic lymphadenopathy as diagnosed by
computed tomography at a university hospital Information was extracted from the electronic record Costs were determined from the Centers for Medicare and Medicaid Services resource-based relative value scale We defined a positive diagnosis as one where benign or malignant disease was found A negative biopsy was one where lymph node sampling was confirmed but no pathology (benign or malignant) was seen A nondiagnosticbiopsy was one where no pathology was seen and lymph node sampling could not be confirmed The total cost of endoscopic and surgical diagnostic procedures was tallied for each patient to obtain mean costs per patient
bull RESULTS bull Thirty-seven patients underwent FB-TBNA and 257 underwent EBUS-TBNA A diagnosis was found in 90 of
patients in the EBUS group and 622 of patients in the FB-TBNA group (Plt0001) More patients in the FB-TBNA group underwent a diagnostic surgical procedure (HR= -01573 95 confidence interval -030 to -015 Plt0001) After accounting for all diagnostic procedures the mean savings with EBUS was $107109 (P=009) per patient
bull CONCLUSIONS bull EBUS-TBNA is less expensive than blind FB-TBNA in the
evaluation of thoracic lymphadenopathy when accounting for diagnostic surgical procedures
Trisolini Rocco MD Gasparini Stefano MDdagger Is It Time for Conventional TBNA to Die
Journalof Bronchology amp Interventional Pulmonology October 2013 - Volume 20 - Issue 4 - p 368ndash369
bull It is possible that the most cost-effective diagnostic approach is to use conventional TBNA for large (gt15 to 2 cm) and easy-to-sample (stations 4 R andor 7) lymph nodes and to reserve EBUS-TBNA for smaller or less accessible nodes or for situations when conventional TBNA has failed
bull Furthermore it seems at least questionable to conclude that EBUS-TBNA is less expensive than conventional TBNA on the basis of a retrospective comparison of merely 37 cases of conventional TBNA performed at the beginning of the study time (March 2006) with 257 of EBUS-TBNA performed during the following 4 years without considering the cost of the EBUS equipment the different needle costs the maintenance costs of EBUS and the potential cost of acquiring operator skills
nodeThrombus
vessel
21 or 22 gauge
Advantages and disadvantages of various mediastinal staging procedures in lung cancer
Procedure Advantages Disadvantages
Thoracotomy (surgical opening of the chest)Allows the most thorough inspection and sampling of lymph node stations may be followed by resection of tumor if feasible
Most invasive approach not indicated for staging alone significant risk of procedure-related morbidity
Extended cervical mediastinoscopy combined with a Chamberlain procedure which is also called a left parasternal mediastinotomy or anterior mediastinotomy
Permits evaluation of the aortopulmonary window lymph nodes
More invasive false-negative rate approximately 10
Chamberlain procedureAccess to station 5 (aortopulmonary windowlymph node)
Limited applications invasive
Cervical mediastinoscopyStill considered the gold standard (usual comparitor) by many excellent for 2RL 4RL
Does not cover all medastinal lymph node stations particularly subcarinal lymph nodes (station 7) paraesophageal and pulmonary ligament lymph nodes (stations 8 and 9) the aortopulmonary window lymph nodes (station 5) and the anterior mediastinal lymph nodes (station 6) false-negative rate approximately 20 invasive
Video-assisted thoracoscopyGood for inferior mediastinum station 5 and 6 lymph nodes
Invasive does not cover superior anterior mediastinum
Transthoracic percutaneous fine needle aspiration (FNA) under CT guidance
More widely available than some other methodsTraverses a lot of lung tissue therefore high pneumothorax risk some lymph node stations inaccessible
Bronchoscopy with blind transbronchial FNA (Wang needle)
Less invasive than above methodsRelatively low yield not widely practiced bleeding risk
Endobronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound (EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station 5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheallymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
bronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound(EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station
5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheal lymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
Endobronchial ultrasound (EBUS) mini radial probe image
A) The radial probe endobronchial ultrasound image demonstrates six distinct layers of the bronchial wall Layers 1 and 2 are the mucosa submucosa and muscle Layers 3 and 4 are the cartilage Layers 5 and 6 are the adventitia Layers 1 3 and 5 appear hyperechoic because they are interfaces B) Cross section of a normal bronchus
Endobronchial ultrasound (EBUS) peripheral nodule sampling II
Associate Prof of PulmonologyCo-director 5th Pulmonary DepartmentIzmir Dr Suat Seren Training amp Research Hospital for Thoracic Medicine amp Surgery35110 Yenisehir Izmir TurkeyTEL 90-532 661 45 22 FAX 90-232-362 28 31E-MAIL sbilaceroglu [AT] gmail [DOT] com
Semra Bilaceroglu Dr Suat Seren GoumlğuumlsHastalıkları Ve Cerrahisi Eğitim Ve Ara
How do you decide on whether to use conventional TBNA or EBUS-TBNA
I want to see views of bronchoscopists from different countries
TopicsInterventional Pulmonology Aug 11 2015 All
Answers (11)
Eman Sobh middot Al-Azhar University Hi Semra EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult
cases Aug 12 2015 middot Herveacute Dutau middot Assistance Publique Hocircpitaux de Marseille Semra I use TBNA- for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of ordercheersAug 12 2015 middot Suveer Singh middot Imperial College London Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cellsIt is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomybwSuveerAug 13 2015 middot Johannes M Daniels middot VU University Medical Center TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNAA problem is that there are so few cases that it becomes difficult to pass on the skillsAug 13 2015 middot Vicente Roig-Figueroa middot Hospital Cliacutenico Universitario de Valladolid In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11LAug 15 2015 middot Eman Sobh middot Al-Azhar University our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are
availableAug 15 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiI am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNAEBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm) For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA Aug 16 2015 middot Michel Febvre middot Hocircpital Tenon (Hocircpitaux Universitaires Est Parisien) Hello Semra interesting questionI was a hard defender of conventionnal TBNA for LN gt 20 mm in station 7 or 4R or tumors adjacent to the airways because it is quick and easyDespite that we have the chance of having 4 EBUS scopes in our department and it is now roughly as quick to do an EBUS so we use EBUS under local and premedication in 95 of the time The two other reasons of
using EBUS is teaching and sometimes doing EUS with the EBUS scopeNevertheless I continue to think that there is a place for conventionnal TBNA in centers for which EBUS is too expensive and indications less frequent for diagnosis of large mediastinal lymph nodes or tumors
Teaching conventionnal TBNA should be pursuedSincerelyAug 19 2015 middot Maria Majori middot University Hospital of Parma In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases)I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the
confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy
Otherwise it would be like driving a Ferrari just learned to driveBest regards to All of YouAug 21 2015 middot Mace M Schuurmans middot University of Zurich For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind
TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
Aug 22 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiThank you for all these answers Its important to have appropriate indications for conventional TBNA and EBUS-TBNATo be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for
conventional methodAug 23 2015 middot Can you help by adding an answerAdd your answer
Is conventional transbronchial needle aspiration (TBNA) obsolete απαρχαιωμένη Available from httpswwwresearchgatenetpost
[accessed Apr 17 2017]
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
SESSION II Invasive approach of the mediastinum Επεμβατική προσέγγιση του μεσοθωρακίου
Πρόεδροι Δ Χλωρός Ι Μπουκοβίνας Ι Άντζελbull 1030 - 1045 Video-assisted mediastinoscopy for mediastinal staging of lung cancer bull Η συμβολή της video-μεσοθωρακοσκόπησης στη σταδιοποίηση του καρκίνου του
πνεύμονα bull Χ Φορούλης
bull 1045 - 1100 Interesting cases presentation Παρουσίαση ενδιαφερόντων περιστατικών bull Δ Φιλίππου
bull 1100 - 1115 Transitioning from conventional TBNA to EBUS-TBNA bull Η μετάβαση από τη συμβατική στην υπερηχογραφικά καθοδηγούμενη ΤΒΝΑ bull Θ Κοντακιώτης
bull 1115 - 1130 EBUS-TBNA Practical tips EBUS-TBNA Πρακτικές συμβουλές bull Ν Παπανικολάου 1130 - 1145
bull 1145 - 1200 Comments Σχολιασμός bull Σχολιαστές Α Κλέωντας Δ Οικονόμου Ε Διαμαντίδουbull Question and Answer Session bull Ερωτήσεις amp Απαντήσεις
Conventional TBNA
bull Although the conventional TBNA technique has been available for almost three decades its use in routine clinical practice has only
been adopted by a minority (10-15) of pulmonologists for mediastinal nodal staging of patients with potentially resectablestage I-III lung cancer
bull Major reasons for its underuse are its dependency on nodal size (gt15-20 mm short axis on CT scan) and operator skills
bull Meta-analyses reported a sensitivity of 78 and a false negative rate of 28 for conventional TBNA in clinical N2 disease with high disease prevalence of 81 (1213) A conventional blind TBNA is useful if it leads to proof of N3 disease but too often does not exclude N3 disease in cases of proven N2 disease
Bronchoscopic findings in lung cancer diagnostic yield of specimen collection method compared to histological typeT Kontakiotis N Manolakoglou F Zoglopitis L Sakkas D Iakovidis A Mandali P Argyropoulou
Παρουσιάστηκε στο 15ο συνέδριο της European Respiratory Society 17-21 Σεπτεμβρίου 2005 Thematic Poster Session Diagnostic procedures staging of lung cancer and screening Δημοσιεύτηκε στον τόμο των πρακτικών Eur Respir J Suppl vol 26 suppl 49 Σελ P3458
bull Περίληψη From 111995 to 31122004 16816 bronchoscopies were performed in the General Hospital ldquoG Papanikolaourdquo 13779 (819) males (M) and 3037 (181) females (F)) According to histological (forceps biopsy) andor cytological analysis (Transbronchial needle aspiration (TBNA) andor brushing) 5684 (338) were proved to be positive for lung cancer (5192 (913) (M) and 492 (87) (F)) Most of these patients 2451 (431) had squamous cell carcinoma (SqCC) 1230 (216) had adenocarcinoma (AD) 1191 (21) had small cell carcinoma (SCLC) and 813 (143) subjects were sorted as ldquoother histological typesrdquo Best diagnostic yield for SqCC was observed in biopsy specimen (85) (p=0000) especially when the lesion was located in the left main bronchus (941) On the other hand best diagnostic yield for AD was observed for TBNA (754) (p=0001) especially when lesion was located in trachea (917) and for SCLC biopsy (854) (p=0000) especially for lesions in the left main bronchus (957) The percentage of the only one positive method when all the three methods of specimen collection were used was for biopsy 116 for TBNA 65 and for brushing 57 (p=0000) Conclusively SqCC is the most frequent histologic type of lung cancer followed by AD Bronchoscopic biopsy has the best yield followed by TBNA for the final diagnosis
J Thorac Dis 2014 May 6(5) 416ndash420
TBNA with and without EBUS a comparative efficacy study for the
diagnosis and staging of lung cancerJunhong Jiang1 Robert Browning2 Noah Lechtzin3 Jianan Huang1 Peter Terry3 and Ko Pen Wang 13
TBNA MethodDiagnosedtotal malignant cases
Percent yield ()
c-TBNA 6483 771
EBUS 6283 747
MethodsA total of 287 patients with mediastinal and hilar lymphadenopathy presenting for diagnosis andor staging of lung cancer at enrolling institutions were included Equal numbers of punctures were performed at the target lymph node stations using conventional TBNA techniques followed by EBUS-TBNA at the same sites Patients and puncture sites that were biopsied by both methods and were positive for lung cancer were compared to establish efficacy of each technique on the same patients
Conclusions
Recommendations for current practice depend on individual centers and bronchoscopist comfort level with TBNA (with or without EBUS) In our study no significant difference was seen between the techniques for the diagnosis and staging of individual patients
Indications for conventional transbronchial needle aspiration
bull Mediastinal andor hilar lymphadenopathybull Staging of lung cancer or suspect of lung cancer mainly to
prove unresectability Sarcoidosis lymphoma PTLDbull Extrinsic compression of the airway by a peribronchial
lesion or a lymphadenopathybull Submucosal diseasePeripheral nodules or masses negative
bronchus sign (Tsuboi type IV)bull Endobronchial tumors (necrotic or hemorrhagic tumors)bull Diagnosisdrainage of mediastinal cysts or abscesses
bull PTLD post transplant lymphoproliferative disorder
Elif Kuumlpeli Conventional transbronchial needle aspiration in community practice
J Thorac Dis 2015 Dec 7(Suppl 4) S256ndashS265
Assoc Prof FCCPAnkara Turkey Email mocoohayilepukfile
RESULTSOur analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90
lymph nodes were smaller than 100 mm The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929 The most common histological diagnosis was adenocarcinoma
Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Sebastiaacuten Fernaacutendez-Bussy Gonzalo Labarca Sofia Canals Ivaacuten Caviedes Erik Folch Adnan MajidJ Bras Pneumol 2015 May-Jun 41(3) 219ndash224
J Bronchology Interv Pulmonol 2012 Jul19(3)182-7 doi Comparative cost analysis of endobronchial ultrasound-guided and blind
TBNA in the evaluation of hilar and mediastinal lymphadenopathyGrove DA1 Bechara RI Josephs JS Berkowitz DM
bull BACKGROUND bull The superior accuracy of endobronchial ultrasound (EBUS) averts many diagnostic surgical procedures This
likely leads to significant cost savings despite an increased per procedure cost We sought to compare the true costs of endobronchial ultrasound-transbronchial needle aspiration (EBUS-TBNA) compared with blind fiberoptic bronchoscopy-transbronchial needle aspiration (FB-TBNA) factoring in the impact of diagnostic surgical procedures in the diagnosis of mediastinal lymphadenopathy
bull METHODS bull In this retrospective case study we selected 294 patients with thoracic lymphadenopathy as diagnosed by
computed tomography at a university hospital Information was extracted from the electronic record Costs were determined from the Centers for Medicare and Medicaid Services resource-based relative value scale We defined a positive diagnosis as one where benign or malignant disease was found A negative biopsy was one where lymph node sampling was confirmed but no pathology (benign or malignant) was seen A nondiagnosticbiopsy was one where no pathology was seen and lymph node sampling could not be confirmed The total cost of endoscopic and surgical diagnostic procedures was tallied for each patient to obtain mean costs per patient
bull RESULTS bull Thirty-seven patients underwent FB-TBNA and 257 underwent EBUS-TBNA A diagnosis was found in 90 of
patients in the EBUS group and 622 of patients in the FB-TBNA group (Plt0001) More patients in the FB-TBNA group underwent a diagnostic surgical procedure (HR= -01573 95 confidence interval -030 to -015 Plt0001) After accounting for all diagnostic procedures the mean savings with EBUS was $107109 (P=009) per patient
bull CONCLUSIONS bull EBUS-TBNA is less expensive than blind FB-TBNA in the
evaluation of thoracic lymphadenopathy when accounting for diagnostic surgical procedures
Trisolini Rocco MD Gasparini Stefano MDdagger Is It Time for Conventional TBNA to Die
Journalof Bronchology amp Interventional Pulmonology October 2013 - Volume 20 - Issue 4 - p 368ndash369
bull It is possible that the most cost-effective diagnostic approach is to use conventional TBNA for large (gt15 to 2 cm) and easy-to-sample (stations 4 R andor 7) lymph nodes and to reserve EBUS-TBNA for smaller or less accessible nodes or for situations when conventional TBNA has failed
bull Furthermore it seems at least questionable to conclude that EBUS-TBNA is less expensive than conventional TBNA on the basis of a retrospective comparison of merely 37 cases of conventional TBNA performed at the beginning of the study time (March 2006) with 257 of EBUS-TBNA performed during the following 4 years without considering the cost of the EBUS equipment the different needle costs the maintenance costs of EBUS and the potential cost of acquiring operator skills
nodeThrombus
vessel
21 or 22 gauge
Advantages and disadvantages of various mediastinal staging procedures in lung cancer
Procedure Advantages Disadvantages
Thoracotomy (surgical opening of the chest)Allows the most thorough inspection and sampling of lymph node stations may be followed by resection of tumor if feasible
Most invasive approach not indicated for staging alone significant risk of procedure-related morbidity
Extended cervical mediastinoscopy combined with a Chamberlain procedure which is also called a left parasternal mediastinotomy or anterior mediastinotomy
Permits evaluation of the aortopulmonary window lymph nodes
More invasive false-negative rate approximately 10
Chamberlain procedureAccess to station 5 (aortopulmonary windowlymph node)
Limited applications invasive
Cervical mediastinoscopyStill considered the gold standard (usual comparitor) by many excellent for 2RL 4RL
Does not cover all medastinal lymph node stations particularly subcarinal lymph nodes (station 7) paraesophageal and pulmonary ligament lymph nodes (stations 8 and 9) the aortopulmonary window lymph nodes (station 5) and the anterior mediastinal lymph nodes (station 6) false-negative rate approximately 20 invasive
Video-assisted thoracoscopyGood for inferior mediastinum station 5 and 6 lymph nodes
Invasive does not cover superior anterior mediastinum
Transthoracic percutaneous fine needle aspiration (FNA) under CT guidance
More widely available than some other methodsTraverses a lot of lung tissue therefore high pneumothorax risk some lymph node stations inaccessible
Bronchoscopy with blind transbronchial FNA (Wang needle)
Less invasive than above methodsRelatively low yield not widely practiced bleeding risk
Endobronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound (EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station 5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheallymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
bronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound(EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station
5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheal lymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
Endobronchial ultrasound (EBUS) mini radial probe image
A) The radial probe endobronchial ultrasound image demonstrates six distinct layers of the bronchial wall Layers 1 and 2 are the mucosa submucosa and muscle Layers 3 and 4 are the cartilage Layers 5 and 6 are the adventitia Layers 1 3 and 5 appear hyperechoic because they are interfaces B) Cross section of a normal bronchus
Endobronchial ultrasound (EBUS) peripheral nodule sampling II
Associate Prof of PulmonologyCo-director 5th Pulmonary DepartmentIzmir Dr Suat Seren Training amp Research Hospital for Thoracic Medicine amp Surgery35110 Yenisehir Izmir TurkeyTEL 90-532 661 45 22 FAX 90-232-362 28 31E-MAIL sbilaceroglu [AT] gmail [DOT] com
Semra Bilaceroglu Dr Suat Seren GoumlğuumlsHastalıkları Ve Cerrahisi Eğitim Ve Ara
How do you decide on whether to use conventional TBNA or EBUS-TBNA
I want to see views of bronchoscopists from different countries
TopicsInterventional Pulmonology Aug 11 2015 All
Answers (11)
Eman Sobh middot Al-Azhar University Hi Semra EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult
cases Aug 12 2015 middot Herveacute Dutau middot Assistance Publique Hocircpitaux de Marseille Semra I use TBNA- for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of ordercheersAug 12 2015 middot Suveer Singh middot Imperial College London Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cellsIt is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomybwSuveerAug 13 2015 middot Johannes M Daniels middot VU University Medical Center TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNAA problem is that there are so few cases that it becomes difficult to pass on the skillsAug 13 2015 middot Vicente Roig-Figueroa middot Hospital Cliacutenico Universitario de Valladolid In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11LAug 15 2015 middot Eman Sobh middot Al-Azhar University our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are
availableAug 15 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiI am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNAEBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm) For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA Aug 16 2015 middot Michel Febvre middot Hocircpital Tenon (Hocircpitaux Universitaires Est Parisien) Hello Semra interesting questionI was a hard defender of conventionnal TBNA for LN gt 20 mm in station 7 or 4R or tumors adjacent to the airways because it is quick and easyDespite that we have the chance of having 4 EBUS scopes in our department and it is now roughly as quick to do an EBUS so we use EBUS under local and premedication in 95 of the time The two other reasons of
using EBUS is teaching and sometimes doing EUS with the EBUS scopeNevertheless I continue to think that there is a place for conventionnal TBNA in centers for which EBUS is too expensive and indications less frequent for diagnosis of large mediastinal lymph nodes or tumors
Teaching conventionnal TBNA should be pursuedSincerelyAug 19 2015 middot Maria Majori middot University Hospital of Parma In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases)I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the
confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy
Otherwise it would be like driving a Ferrari just learned to driveBest regards to All of YouAug 21 2015 middot Mace M Schuurmans middot University of Zurich For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind
TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
Aug 22 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiThank you for all these answers Its important to have appropriate indications for conventional TBNA and EBUS-TBNATo be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for
conventional methodAug 23 2015 middot Can you help by adding an answerAdd your answer
Is conventional transbronchial needle aspiration (TBNA) obsolete απαρχαιωμένη Available from httpswwwresearchgatenetpost
[accessed Apr 17 2017]
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
Conventional TBNA
bull Although the conventional TBNA technique has been available for almost three decades its use in routine clinical practice has only
been adopted by a minority (10-15) of pulmonologists for mediastinal nodal staging of patients with potentially resectablestage I-III lung cancer
bull Major reasons for its underuse are its dependency on nodal size (gt15-20 mm short axis on CT scan) and operator skills
bull Meta-analyses reported a sensitivity of 78 and a false negative rate of 28 for conventional TBNA in clinical N2 disease with high disease prevalence of 81 (1213) A conventional blind TBNA is useful if it leads to proof of N3 disease but too often does not exclude N3 disease in cases of proven N2 disease
Bronchoscopic findings in lung cancer diagnostic yield of specimen collection method compared to histological typeT Kontakiotis N Manolakoglou F Zoglopitis L Sakkas D Iakovidis A Mandali P Argyropoulou
Παρουσιάστηκε στο 15ο συνέδριο της European Respiratory Society 17-21 Σεπτεμβρίου 2005 Thematic Poster Session Diagnostic procedures staging of lung cancer and screening Δημοσιεύτηκε στον τόμο των πρακτικών Eur Respir J Suppl vol 26 suppl 49 Σελ P3458
bull Περίληψη From 111995 to 31122004 16816 bronchoscopies were performed in the General Hospital ldquoG Papanikolaourdquo 13779 (819) males (M) and 3037 (181) females (F)) According to histological (forceps biopsy) andor cytological analysis (Transbronchial needle aspiration (TBNA) andor brushing) 5684 (338) were proved to be positive for lung cancer (5192 (913) (M) and 492 (87) (F)) Most of these patients 2451 (431) had squamous cell carcinoma (SqCC) 1230 (216) had adenocarcinoma (AD) 1191 (21) had small cell carcinoma (SCLC) and 813 (143) subjects were sorted as ldquoother histological typesrdquo Best diagnostic yield for SqCC was observed in biopsy specimen (85) (p=0000) especially when the lesion was located in the left main bronchus (941) On the other hand best diagnostic yield for AD was observed for TBNA (754) (p=0001) especially when lesion was located in trachea (917) and for SCLC biopsy (854) (p=0000) especially for lesions in the left main bronchus (957) The percentage of the only one positive method when all the three methods of specimen collection were used was for biopsy 116 for TBNA 65 and for brushing 57 (p=0000) Conclusively SqCC is the most frequent histologic type of lung cancer followed by AD Bronchoscopic biopsy has the best yield followed by TBNA for the final diagnosis
J Thorac Dis 2014 May 6(5) 416ndash420
TBNA with and without EBUS a comparative efficacy study for the
diagnosis and staging of lung cancerJunhong Jiang1 Robert Browning2 Noah Lechtzin3 Jianan Huang1 Peter Terry3 and Ko Pen Wang 13
TBNA MethodDiagnosedtotal malignant cases
Percent yield ()
c-TBNA 6483 771
EBUS 6283 747
MethodsA total of 287 patients with mediastinal and hilar lymphadenopathy presenting for diagnosis andor staging of lung cancer at enrolling institutions were included Equal numbers of punctures were performed at the target lymph node stations using conventional TBNA techniques followed by EBUS-TBNA at the same sites Patients and puncture sites that were biopsied by both methods and were positive for lung cancer were compared to establish efficacy of each technique on the same patients
Conclusions
Recommendations for current practice depend on individual centers and bronchoscopist comfort level with TBNA (with or without EBUS) In our study no significant difference was seen between the techniques for the diagnosis and staging of individual patients
Indications for conventional transbronchial needle aspiration
bull Mediastinal andor hilar lymphadenopathybull Staging of lung cancer or suspect of lung cancer mainly to
prove unresectability Sarcoidosis lymphoma PTLDbull Extrinsic compression of the airway by a peribronchial
lesion or a lymphadenopathybull Submucosal diseasePeripheral nodules or masses negative
bronchus sign (Tsuboi type IV)bull Endobronchial tumors (necrotic or hemorrhagic tumors)bull Diagnosisdrainage of mediastinal cysts or abscesses
bull PTLD post transplant lymphoproliferative disorder
Elif Kuumlpeli Conventional transbronchial needle aspiration in community practice
J Thorac Dis 2015 Dec 7(Suppl 4) S256ndashS265
Assoc Prof FCCPAnkara Turkey Email mocoohayilepukfile
RESULTSOur analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90
lymph nodes were smaller than 100 mm The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929 The most common histological diagnosis was adenocarcinoma
Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Sebastiaacuten Fernaacutendez-Bussy Gonzalo Labarca Sofia Canals Ivaacuten Caviedes Erik Folch Adnan MajidJ Bras Pneumol 2015 May-Jun 41(3) 219ndash224
J Bronchology Interv Pulmonol 2012 Jul19(3)182-7 doi Comparative cost analysis of endobronchial ultrasound-guided and blind
TBNA in the evaluation of hilar and mediastinal lymphadenopathyGrove DA1 Bechara RI Josephs JS Berkowitz DM
bull BACKGROUND bull The superior accuracy of endobronchial ultrasound (EBUS) averts many diagnostic surgical procedures This
likely leads to significant cost savings despite an increased per procedure cost We sought to compare the true costs of endobronchial ultrasound-transbronchial needle aspiration (EBUS-TBNA) compared with blind fiberoptic bronchoscopy-transbronchial needle aspiration (FB-TBNA) factoring in the impact of diagnostic surgical procedures in the diagnosis of mediastinal lymphadenopathy
bull METHODS bull In this retrospective case study we selected 294 patients with thoracic lymphadenopathy as diagnosed by
computed tomography at a university hospital Information was extracted from the electronic record Costs were determined from the Centers for Medicare and Medicaid Services resource-based relative value scale We defined a positive diagnosis as one where benign or malignant disease was found A negative biopsy was one where lymph node sampling was confirmed but no pathology (benign or malignant) was seen A nondiagnosticbiopsy was one where no pathology was seen and lymph node sampling could not be confirmed The total cost of endoscopic and surgical diagnostic procedures was tallied for each patient to obtain mean costs per patient
bull RESULTS bull Thirty-seven patients underwent FB-TBNA and 257 underwent EBUS-TBNA A diagnosis was found in 90 of
patients in the EBUS group and 622 of patients in the FB-TBNA group (Plt0001) More patients in the FB-TBNA group underwent a diagnostic surgical procedure (HR= -01573 95 confidence interval -030 to -015 Plt0001) After accounting for all diagnostic procedures the mean savings with EBUS was $107109 (P=009) per patient
bull CONCLUSIONS bull EBUS-TBNA is less expensive than blind FB-TBNA in the
evaluation of thoracic lymphadenopathy when accounting for diagnostic surgical procedures
Trisolini Rocco MD Gasparini Stefano MDdagger Is It Time for Conventional TBNA to Die
Journalof Bronchology amp Interventional Pulmonology October 2013 - Volume 20 - Issue 4 - p 368ndash369
bull It is possible that the most cost-effective diagnostic approach is to use conventional TBNA for large (gt15 to 2 cm) and easy-to-sample (stations 4 R andor 7) lymph nodes and to reserve EBUS-TBNA for smaller or less accessible nodes or for situations when conventional TBNA has failed
bull Furthermore it seems at least questionable to conclude that EBUS-TBNA is less expensive than conventional TBNA on the basis of a retrospective comparison of merely 37 cases of conventional TBNA performed at the beginning of the study time (March 2006) with 257 of EBUS-TBNA performed during the following 4 years without considering the cost of the EBUS equipment the different needle costs the maintenance costs of EBUS and the potential cost of acquiring operator skills
nodeThrombus
vessel
21 or 22 gauge
Advantages and disadvantages of various mediastinal staging procedures in lung cancer
Procedure Advantages Disadvantages
Thoracotomy (surgical opening of the chest)Allows the most thorough inspection and sampling of lymph node stations may be followed by resection of tumor if feasible
Most invasive approach not indicated for staging alone significant risk of procedure-related morbidity
Extended cervical mediastinoscopy combined with a Chamberlain procedure which is also called a left parasternal mediastinotomy or anterior mediastinotomy
Permits evaluation of the aortopulmonary window lymph nodes
More invasive false-negative rate approximately 10
Chamberlain procedureAccess to station 5 (aortopulmonary windowlymph node)
Limited applications invasive
Cervical mediastinoscopyStill considered the gold standard (usual comparitor) by many excellent for 2RL 4RL
Does not cover all medastinal lymph node stations particularly subcarinal lymph nodes (station 7) paraesophageal and pulmonary ligament lymph nodes (stations 8 and 9) the aortopulmonary window lymph nodes (station 5) and the anterior mediastinal lymph nodes (station 6) false-negative rate approximately 20 invasive
Video-assisted thoracoscopyGood for inferior mediastinum station 5 and 6 lymph nodes
Invasive does not cover superior anterior mediastinum
Transthoracic percutaneous fine needle aspiration (FNA) under CT guidance
More widely available than some other methodsTraverses a lot of lung tissue therefore high pneumothorax risk some lymph node stations inaccessible
Bronchoscopy with blind transbronchial FNA (Wang needle)
Less invasive than above methodsRelatively low yield not widely practiced bleeding risk
Endobronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound (EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station 5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheallymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
bronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound(EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station
5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheal lymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
Endobronchial ultrasound (EBUS) mini radial probe image
A) The radial probe endobronchial ultrasound image demonstrates six distinct layers of the bronchial wall Layers 1 and 2 are the mucosa submucosa and muscle Layers 3 and 4 are the cartilage Layers 5 and 6 are the adventitia Layers 1 3 and 5 appear hyperechoic because they are interfaces B) Cross section of a normal bronchus
Endobronchial ultrasound (EBUS) peripheral nodule sampling II
Associate Prof of PulmonologyCo-director 5th Pulmonary DepartmentIzmir Dr Suat Seren Training amp Research Hospital for Thoracic Medicine amp Surgery35110 Yenisehir Izmir TurkeyTEL 90-532 661 45 22 FAX 90-232-362 28 31E-MAIL sbilaceroglu [AT] gmail [DOT] com
Semra Bilaceroglu Dr Suat Seren GoumlğuumlsHastalıkları Ve Cerrahisi Eğitim Ve Ara
How do you decide on whether to use conventional TBNA or EBUS-TBNA
I want to see views of bronchoscopists from different countries
TopicsInterventional Pulmonology Aug 11 2015 All
Answers (11)
Eman Sobh middot Al-Azhar University Hi Semra EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult
cases Aug 12 2015 middot Herveacute Dutau middot Assistance Publique Hocircpitaux de Marseille Semra I use TBNA- for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of ordercheersAug 12 2015 middot Suveer Singh middot Imperial College London Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cellsIt is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomybwSuveerAug 13 2015 middot Johannes M Daniels middot VU University Medical Center TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNAA problem is that there are so few cases that it becomes difficult to pass on the skillsAug 13 2015 middot Vicente Roig-Figueroa middot Hospital Cliacutenico Universitario de Valladolid In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11LAug 15 2015 middot Eman Sobh middot Al-Azhar University our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are
availableAug 15 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiI am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNAEBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm) For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA Aug 16 2015 middot Michel Febvre middot Hocircpital Tenon (Hocircpitaux Universitaires Est Parisien) Hello Semra interesting questionI was a hard defender of conventionnal TBNA for LN gt 20 mm in station 7 or 4R or tumors adjacent to the airways because it is quick and easyDespite that we have the chance of having 4 EBUS scopes in our department and it is now roughly as quick to do an EBUS so we use EBUS under local and premedication in 95 of the time The two other reasons of
using EBUS is teaching and sometimes doing EUS with the EBUS scopeNevertheless I continue to think that there is a place for conventionnal TBNA in centers for which EBUS is too expensive and indications less frequent for diagnosis of large mediastinal lymph nodes or tumors
Teaching conventionnal TBNA should be pursuedSincerelyAug 19 2015 middot Maria Majori middot University Hospital of Parma In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases)I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the
confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy
Otherwise it would be like driving a Ferrari just learned to driveBest regards to All of YouAug 21 2015 middot Mace M Schuurmans middot University of Zurich For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind
TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
Aug 22 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiThank you for all these answers Its important to have appropriate indications for conventional TBNA and EBUS-TBNATo be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for
conventional methodAug 23 2015 middot Can you help by adding an answerAdd your answer
Is conventional transbronchial needle aspiration (TBNA) obsolete απαρχαιωμένη Available from httpswwwresearchgatenetpost
[accessed Apr 17 2017]
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
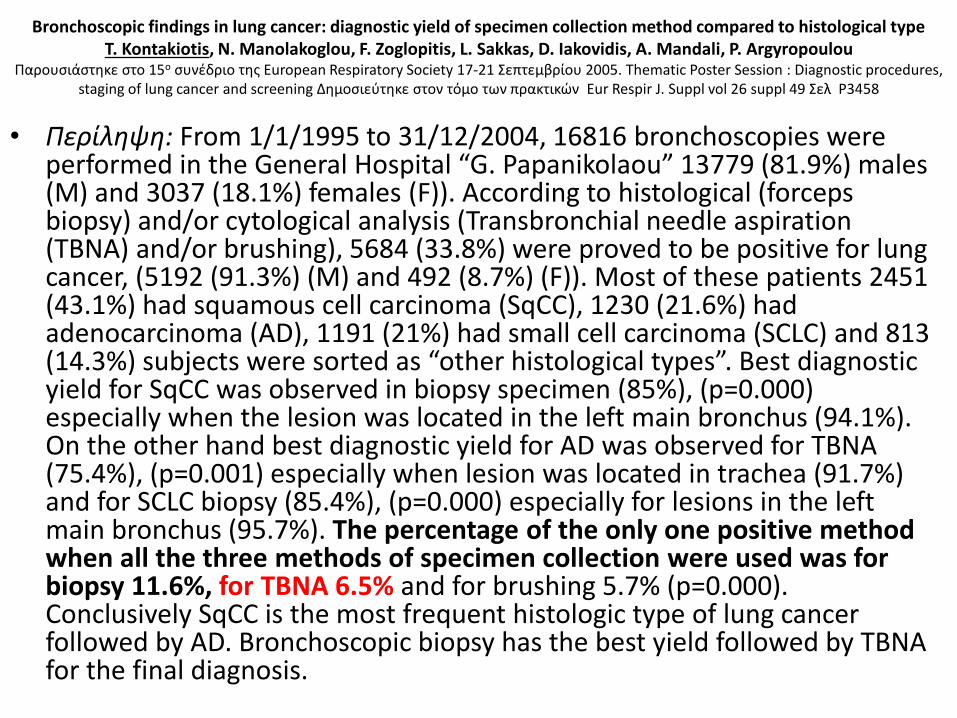
Bronchoscopic findings in lung cancer diagnostic yield of specimen collection method compared to histological typeT Kontakiotis N Manolakoglou F Zoglopitis L Sakkas D Iakovidis A Mandali P Argyropoulou
Παρουσιάστηκε στο 15ο συνέδριο της European Respiratory Society 17-21 Σεπτεμβρίου 2005 Thematic Poster Session Diagnostic procedures staging of lung cancer and screening Δημοσιεύτηκε στον τόμο των πρακτικών Eur Respir J Suppl vol 26 suppl 49 Σελ P3458
bull Περίληψη From 111995 to 31122004 16816 bronchoscopies were performed in the General Hospital ldquoG Papanikolaourdquo 13779 (819) males (M) and 3037 (181) females (F)) According to histological (forceps biopsy) andor cytological analysis (Transbronchial needle aspiration (TBNA) andor brushing) 5684 (338) were proved to be positive for lung cancer (5192 (913) (M) and 492 (87) (F)) Most of these patients 2451 (431) had squamous cell carcinoma (SqCC) 1230 (216) had adenocarcinoma (AD) 1191 (21) had small cell carcinoma (SCLC) and 813 (143) subjects were sorted as ldquoother histological typesrdquo Best diagnostic yield for SqCC was observed in biopsy specimen (85) (p=0000) especially when the lesion was located in the left main bronchus (941) On the other hand best diagnostic yield for AD was observed for TBNA (754) (p=0001) especially when lesion was located in trachea (917) and for SCLC biopsy (854) (p=0000) especially for lesions in the left main bronchus (957) The percentage of the only one positive method when all the three methods of specimen collection were used was for biopsy 116 for TBNA 65 and for brushing 57 (p=0000) Conclusively SqCC is the most frequent histologic type of lung cancer followed by AD Bronchoscopic biopsy has the best yield followed by TBNA for the final diagnosis
J Thorac Dis 2014 May 6(5) 416ndash420
TBNA with and without EBUS a comparative efficacy study for the
diagnosis and staging of lung cancerJunhong Jiang1 Robert Browning2 Noah Lechtzin3 Jianan Huang1 Peter Terry3 and Ko Pen Wang 13
TBNA MethodDiagnosedtotal malignant cases
Percent yield ()
c-TBNA 6483 771
EBUS 6283 747
MethodsA total of 287 patients with mediastinal and hilar lymphadenopathy presenting for diagnosis andor staging of lung cancer at enrolling institutions were included Equal numbers of punctures were performed at the target lymph node stations using conventional TBNA techniques followed by EBUS-TBNA at the same sites Patients and puncture sites that were biopsied by both methods and were positive for lung cancer were compared to establish efficacy of each technique on the same patients
Conclusions
Recommendations for current practice depend on individual centers and bronchoscopist comfort level with TBNA (with or without EBUS) In our study no significant difference was seen between the techniques for the diagnosis and staging of individual patients
Indications for conventional transbronchial needle aspiration
bull Mediastinal andor hilar lymphadenopathybull Staging of lung cancer or suspect of lung cancer mainly to
prove unresectability Sarcoidosis lymphoma PTLDbull Extrinsic compression of the airway by a peribronchial
lesion or a lymphadenopathybull Submucosal diseasePeripheral nodules or masses negative
bronchus sign (Tsuboi type IV)bull Endobronchial tumors (necrotic or hemorrhagic tumors)bull Diagnosisdrainage of mediastinal cysts or abscesses
bull PTLD post transplant lymphoproliferative disorder
Elif Kuumlpeli Conventional transbronchial needle aspiration in community practice
J Thorac Dis 2015 Dec 7(Suppl 4) S256ndashS265
Assoc Prof FCCPAnkara Turkey Email mocoohayilepukfile
RESULTSOur analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90
lymph nodes were smaller than 100 mm The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929 The most common histological diagnosis was adenocarcinoma
Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Sebastiaacuten Fernaacutendez-Bussy Gonzalo Labarca Sofia Canals Ivaacuten Caviedes Erik Folch Adnan MajidJ Bras Pneumol 2015 May-Jun 41(3) 219ndash224
J Bronchology Interv Pulmonol 2012 Jul19(3)182-7 doi Comparative cost analysis of endobronchial ultrasound-guided and blind
TBNA in the evaluation of hilar and mediastinal lymphadenopathyGrove DA1 Bechara RI Josephs JS Berkowitz DM
bull BACKGROUND bull The superior accuracy of endobronchial ultrasound (EBUS) averts many diagnostic surgical procedures This
likely leads to significant cost savings despite an increased per procedure cost We sought to compare the true costs of endobronchial ultrasound-transbronchial needle aspiration (EBUS-TBNA) compared with blind fiberoptic bronchoscopy-transbronchial needle aspiration (FB-TBNA) factoring in the impact of diagnostic surgical procedures in the diagnosis of mediastinal lymphadenopathy
bull METHODS bull In this retrospective case study we selected 294 patients with thoracic lymphadenopathy as diagnosed by
computed tomography at a university hospital Information was extracted from the electronic record Costs were determined from the Centers for Medicare and Medicaid Services resource-based relative value scale We defined a positive diagnosis as one where benign or malignant disease was found A negative biopsy was one where lymph node sampling was confirmed but no pathology (benign or malignant) was seen A nondiagnosticbiopsy was one where no pathology was seen and lymph node sampling could not be confirmed The total cost of endoscopic and surgical diagnostic procedures was tallied for each patient to obtain mean costs per patient
bull RESULTS bull Thirty-seven patients underwent FB-TBNA and 257 underwent EBUS-TBNA A diagnosis was found in 90 of
patients in the EBUS group and 622 of patients in the FB-TBNA group (Plt0001) More patients in the FB-TBNA group underwent a diagnostic surgical procedure (HR= -01573 95 confidence interval -030 to -015 Plt0001) After accounting for all diagnostic procedures the mean savings with EBUS was $107109 (P=009) per patient
bull CONCLUSIONS bull EBUS-TBNA is less expensive than blind FB-TBNA in the
evaluation of thoracic lymphadenopathy when accounting for diagnostic surgical procedures
Trisolini Rocco MD Gasparini Stefano MDdagger Is It Time for Conventional TBNA to Die
Journalof Bronchology amp Interventional Pulmonology October 2013 - Volume 20 - Issue 4 - p 368ndash369
bull It is possible that the most cost-effective diagnostic approach is to use conventional TBNA for large (gt15 to 2 cm) and easy-to-sample (stations 4 R andor 7) lymph nodes and to reserve EBUS-TBNA for smaller or less accessible nodes or for situations when conventional TBNA has failed
bull Furthermore it seems at least questionable to conclude that EBUS-TBNA is less expensive than conventional TBNA on the basis of a retrospective comparison of merely 37 cases of conventional TBNA performed at the beginning of the study time (March 2006) with 257 of EBUS-TBNA performed during the following 4 years without considering the cost of the EBUS equipment the different needle costs the maintenance costs of EBUS and the potential cost of acquiring operator skills
nodeThrombus
vessel
21 or 22 gauge
Advantages and disadvantages of various mediastinal staging procedures in lung cancer
Procedure Advantages Disadvantages
Thoracotomy (surgical opening of the chest)Allows the most thorough inspection and sampling of lymph node stations may be followed by resection of tumor if feasible
Most invasive approach not indicated for staging alone significant risk of procedure-related morbidity
Extended cervical mediastinoscopy combined with a Chamberlain procedure which is also called a left parasternal mediastinotomy or anterior mediastinotomy
Permits evaluation of the aortopulmonary window lymph nodes
More invasive false-negative rate approximately 10
Chamberlain procedureAccess to station 5 (aortopulmonary windowlymph node)
Limited applications invasive
Cervical mediastinoscopyStill considered the gold standard (usual comparitor) by many excellent for 2RL 4RL
Does not cover all medastinal lymph node stations particularly subcarinal lymph nodes (station 7) paraesophageal and pulmonary ligament lymph nodes (stations 8 and 9) the aortopulmonary window lymph nodes (station 5) and the anterior mediastinal lymph nodes (station 6) false-negative rate approximately 20 invasive
Video-assisted thoracoscopyGood for inferior mediastinum station 5 and 6 lymph nodes
Invasive does not cover superior anterior mediastinum
Transthoracic percutaneous fine needle aspiration (FNA) under CT guidance
More widely available than some other methodsTraverses a lot of lung tissue therefore high pneumothorax risk some lymph node stations inaccessible
Bronchoscopy with blind transbronchial FNA (Wang needle)
Less invasive than above methodsRelatively low yield not widely practiced bleeding risk
Endobronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound (EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station 5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheallymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
bronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound(EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station
5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheal lymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
Endobronchial ultrasound (EBUS) mini radial probe image
A) The radial probe endobronchial ultrasound image demonstrates six distinct layers of the bronchial wall Layers 1 and 2 are the mucosa submucosa and muscle Layers 3 and 4 are the cartilage Layers 5 and 6 are the adventitia Layers 1 3 and 5 appear hyperechoic because they are interfaces B) Cross section of a normal bronchus
Endobronchial ultrasound (EBUS) peripheral nodule sampling II
Associate Prof of PulmonologyCo-director 5th Pulmonary DepartmentIzmir Dr Suat Seren Training amp Research Hospital for Thoracic Medicine amp Surgery35110 Yenisehir Izmir TurkeyTEL 90-532 661 45 22 FAX 90-232-362 28 31E-MAIL sbilaceroglu [AT] gmail [DOT] com
Semra Bilaceroglu Dr Suat Seren GoumlğuumlsHastalıkları Ve Cerrahisi Eğitim Ve Ara
How do you decide on whether to use conventional TBNA or EBUS-TBNA
I want to see views of bronchoscopists from different countries
TopicsInterventional Pulmonology Aug 11 2015 All
Answers (11)
Eman Sobh middot Al-Azhar University Hi Semra EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult
cases Aug 12 2015 middot Herveacute Dutau middot Assistance Publique Hocircpitaux de Marseille Semra I use TBNA- for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of ordercheersAug 12 2015 middot Suveer Singh middot Imperial College London Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cellsIt is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomybwSuveerAug 13 2015 middot Johannes M Daniels middot VU University Medical Center TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNAA problem is that there are so few cases that it becomes difficult to pass on the skillsAug 13 2015 middot Vicente Roig-Figueroa middot Hospital Cliacutenico Universitario de Valladolid In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11LAug 15 2015 middot Eman Sobh middot Al-Azhar University our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are
availableAug 15 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiI am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNAEBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm) For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA Aug 16 2015 middot Michel Febvre middot Hocircpital Tenon (Hocircpitaux Universitaires Est Parisien) Hello Semra interesting questionI was a hard defender of conventionnal TBNA for LN gt 20 mm in station 7 or 4R or tumors adjacent to the airways because it is quick and easyDespite that we have the chance of having 4 EBUS scopes in our department and it is now roughly as quick to do an EBUS so we use EBUS under local and premedication in 95 of the time The two other reasons of
using EBUS is teaching and sometimes doing EUS with the EBUS scopeNevertheless I continue to think that there is a place for conventionnal TBNA in centers for which EBUS is too expensive and indications less frequent for diagnosis of large mediastinal lymph nodes or tumors
Teaching conventionnal TBNA should be pursuedSincerelyAug 19 2015 middot Maria Majori middot University Hospital of Parma In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases)I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the
confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy
Otherwise it would be like driving a Ferrari just learned to driveBest regards to All of YouAug 21 2015 middot Mace M Schuurmans middot University of Zurich For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind
TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
Aug 22 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiThank you for all these answers Its important to have appropriate indications for conventional TBNA and EBUS-TBNATo be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for
conventional methodAug 23 2015 middot Can you help by adding an answerAdd your answer
Is conventional transbronchial needle aspiration (TBNA) obsolete απαρχαιωμένη Available from httpswwwresearchgatenetpost
[accessed Apr 17 2017]
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
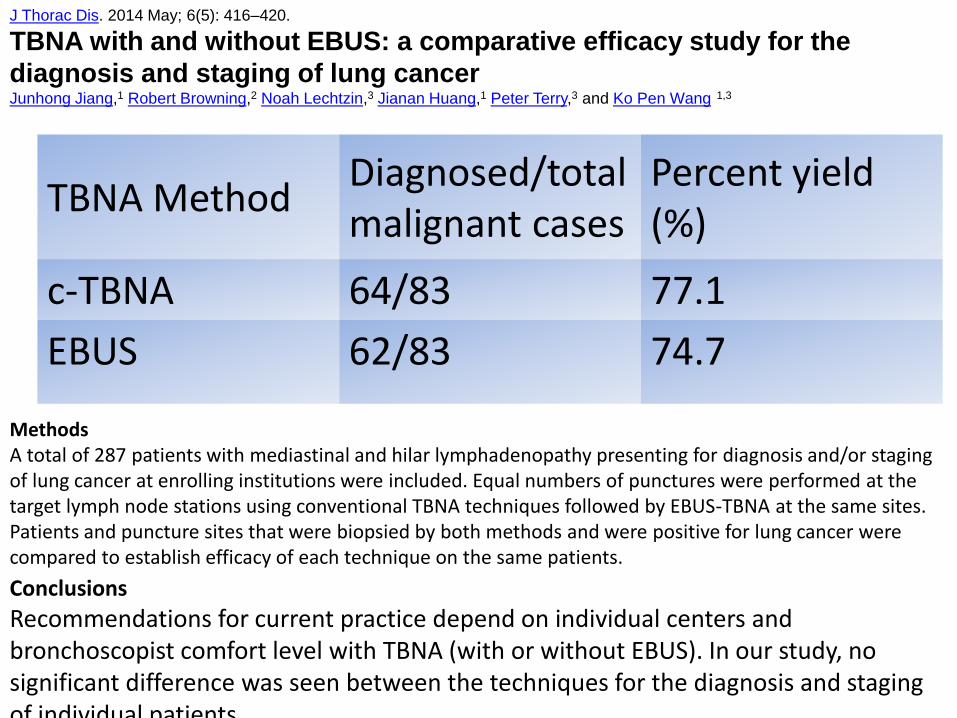
J Thorac Dis 2014 May 6(5) 416ndash420
TBNA with and without EBUS a comparative efficacy study for the
diagnosis and staging of lung cancerJunhong Jiang1 Robert Browning2 Noah Lechtzin3 Jianan Huang1 Peter Terry3 and Ko Pen Wang 13
TBNA MethodDiagnosedtotal malignant cases
Percent yield ()
c-TBNA 6483 771
EBUS 6283 747
MethodsA total of 287 patients with mediastinal and hilar lymphadenopathy presenting for diagnosis andor staging of lung cancer at enrolling institutions were included Equal numbers of punctures were performed at the target lymph node stations using conventional TBNA techniques followed by EBUS-TBNA at the same sites Patients and puncture sites that were biopsied by both methods and were positive for lung cancer were compared to establish efficacy of each technique on the same patients
Conclusions
Recommendations for current practice depend on individual centers and bronchoscopist comfort level with TBNA (with or without EBUS) In our study no significant difference was seen between the techniques for the diagnosis and staging of individual patients
Indications for conventional transbronchial needle aspiration
bull Mediastinal andor hilar lymphadenopathybull Staging of lung cancer or suspect of lung cancer mainly to
prove unresectability Sarcoidosis lymphoma PTLDbull Extrinsic compression of the airway by a peribronchial
lesion or a lymphadenopathybull Submucosal diseasePeripheral nodules or masses negative
bronchus sign (Tsuboi type IV)bull Endobronchial tumors (necrotic or hemorrhagic tumors)bull Diagnosisdrainage of mediastinal cysts or abscesses
bull PTLD post transplant lymphoproliferative disorder
Elif Kuumlpeli Conventional transbronchial needle aspiration in community practice
J Thorac Dis 2015 Dec 7(Suppl 4) S256ndashS265
Assoc Prof FCCPAnkara Turkey Email mocoohayilepukfile
RESULTSOur analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90
lymph nodes were smaller than 100 mm The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929 The most common histological diagnosis was adenocarcinoma
Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Sebastiaacuten Fernaacutendez-Bussy Gonzalo Labarca Sofia Canals Ivaacuten Caviedes Erik Folch Adnan MajidJ Bras Pneumol 2015 May-Jun 41(3) 219ndash224
J Bronchology Interv Pulmonol 2012 Jul19(3)182-7 doi Comparative cost analysis of endobronchial ultrasound-guided and blind
TBNA in the evaluation of hilar and mediastinal lymphadenopathyGrove DA1 Bechara RI Josephs JS Berkowitz DM
bull BACKGROUND bull The superior accuracy of endobronchial ultrasound (EBUS) averts many diagnostic surgical procedures This
likely leads to significant cost savings despite an increased per procedure cost We sought to compare the true costs of endobronchial ultrasound-transbronchial needle aspiration (EBUS-TBNA) compared with blind fiberoptic bronchoscopy-transbronchial needle aspiration (FB-TBNA) factoring in the impact of diagnostic surgical procedures in the diagnosis of mediastinal lymphadenopathy
bull METHODS bull In this retrospective case study we selected 294 patients with thoracic lymphadenopathy as diagnosed by
computed tomography at a university hospital Information was extracted from the electronic record Costs were determined from the Centers for Medicare and Medicaid Services resource-based relative value scale We defined a positive diagnosis as one where benign or malignant disease was found A negative biopsy was one where lymph node sampling was confirmed but no pathology (benign or malignant) was seen A nondiagnosticbiopsy was one where no pathology was seen and lymph node sampling could not be confirmed The total cost of endoscopic and surgical diagnostic procedures was tallied for each patient to obtain mean costs per patient
bull RESULTS bull Thirty-seven patients underwent FB-TBNA and 257 underwent EBUS-TBNA A diagnosis was found in 90 of
patients in the EBUS group and 622 of patients in the FB-TBNA group (Plt0001) More patients in the FB-TBNA group underwent a diagnostic surgical procedure (HR= -01573 95 confidence interval -030 to -015 Plt0001) After accounting for all diagnostic procedures the mean savings with EBUS was $107109 (P=009) per patient
bull CONCLUSIONS bull EBUS-TBNA is less expensive than blind FB-TBNA in the
evaluation of thoracic lymphadenopathy when accounting for diagnostic surgical procedures
Trisolini Rocco MD Gasparini Stefano MDdagger Is It Time for Conventional TBNA to Die
Journalof Bronchology amp Interventional Pulmonology October 2013 - Volume 20 - Issue 4 - p 368ndash369
bull It is possible that the most cost-effective diagnostic approach is to use conventional TBNA for large (gt15 to 2 cm) and easy-to-sample (stations 4 R andor 7) lymph nodes and to reserve EBUS-TBNA for smaller or less accessible nodes or for situations when conventional TBNA has failed
bull Furthermore it seems at least questionable to conclude that EBUS-TBNA is less expensive than conventional TBNA on the basis of a retrospective comparison of merely 37 cases of conventional TBNA performed at the beginning of the study time (March 2006) with 257 of EBUS-TBNA performed during the following 4 years without considering the cost of the EBUS equipment the different needle costs the maintenance costs of EBUS and the potential cost of acquiring operator skills
nodeThrombus
vessel
21 or 22 gauge
Advantages and disadvantages of various mediastinal staging procedures in lung cancer
Procedure Advantages Disadvantages
Thoracotomy (surgical opening of the chest)Allows the most thorough inspection and sampling of lymph node stations may be followed by resection of tumor if feasible
Most invasive approach not indicated for staging alone significant risk of procedure-related morbidity
Extended cervical mediastinoscopy combined with a Chamberlain procedure which is also called a left parasternal mediastinotomy or anterior mediastinotomy
Permits evaluation of the aortopulmonary window lymph nodes
More invasive false-negative rate approximately 10
Chamberlain procedureAccess to station 5 (aortopulmonary windowlymph node)
Limited applications invasive
Cervical mediastinoscopyStill considered the gold standard (usual comparitor) by many excellent for 2RL 4RL
Does not cover all medastinal lymph node stations particularly subcarinal lymph nodes (station 7) paraesophageal and pulmonary ligament lymph nodes (stations 8 and 9) the aortopulmonary window lymph nodes (station 5) and the anterior mediastinal lymph nodes (station 6) false-negative rate approximately 20 invasive
Video-assisted thoracoscopyGood for inferior mediastinum station 5 and 6 lymph nodes
Invasive does not cover superior anterior mediastinum
Transthoracic percutaneous fine needle aspiration (FNA) under CT guidance
More widely available than some other methodsTraverses a lot of lung tissue therefore high pneumothorax risk some lymph node stations inaccessible
Bronchoscopy with blind transbronchial FNA (Wang needle)
Less invasive than above methodsRelatively low yield not widely practiced bleeding risk
Endobronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound (EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station 5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheallymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
bronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound(EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station
5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheal lymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
Endobronchial ultrasound (EBUS) mini radial probe image
A) The radial probe endobronchial ultrasound image demonstrates six distinct layers of the bronchial wall Layers 1 and 2 are the mucosa submucosa and muscle Layers 3 and 4 are the cartilage Layers 5 and 6 are the adventitia Layers 1 3 and 5 appear hyperechoic because they are interfaces B) Cross section of a normal bronchus
Endobronchial ultrasound (EBUS) peripheral nodule sampling II
Associate Prof of PulmonologyCo-director 5th Pulmonary DepartmentIzmir Dr Suat Seren Training amp Research Hospital for Thoracic Medicine amp Surgery35110 Yenisehir Izmir TurkeyTEL 90-532 661 45 22 FAX 90-232-362 28 31E-MAIL sbilaceroglu [AT] gmail [DOT] com
Semra Bilaceroglu Dr Suat Seren GoumlğuumlsHastalıkları Ve Cerrahisi Eğitim Ve Ara
How do you decide on whether to use conventional TBNA or EBUS-TBNA
I want to see views of bronchoscopists from different countries
TopicsInterventional Pulmonology Aug 11 2015 All
Answers (11)
Eman Sobh middot Al-Azhar University Hi Semra EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult
cases Aug 12 2015 middot Herveacute Dutau middot Assistance Publique Hocircpitaux de Marseille Semra I use TBNA- for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of ordercheersAug 12 2015 middot Suveer Singh middot Imperial College London Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cellsIt is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomybwSuveerAug 13 2015 middot Johannes M Daniels middot VU University Medical Center TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNAA problem is that there are so few cases that it becomes difficult to pass on the skillsAug 13 2015 middot Vicente Roig-Figueroa middot Hospital Cliacutenico Universitario de Valladolid In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11LAug 15 2015 middot Eman Sobh middot Al-Azhar University our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are
availableAug 15 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiI am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNAEBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm) For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA Aug 16 2015 middot Michel Febvre middot Hocircpital Tenon (Hocircpitaux Universitaires Est Parisien) Hello Semra interesting questionI was a hard defender of conventionnal TBNA for LN gt 20 mm in station 7 or 4R or tumors adjacent to the airways because it is quick and easyDespite that we have the chance of having 4 EBUS scopes in our department and it is now roughly as quick to do an EBUS so we use EBUS under local and premedication in 95 of the time The two other reasons of
using EBUS is teaching and sometimes doing EUS with the EBUS scopeNevertheless I continue to think that there is a place for conventionnal TBNA in centers for which EBUS is too expensive and indications less frequent for diagnosis of large mediastinal lymph nodes or tumors
Teaching conventionnal TBNA should be pursuedSincerelyAug 19 2015 middot Maria Majori middot University Hospital of Parma In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases)I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the
confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy
Otherwise it would be like driving a Ferrari just learned to driveBest regards to All of YouAug 21 2015 middot Mace M Schuurmans middot University of Zurich For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind
TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
Aug 22 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiThank you for all these answers Its important to have appropriate indications for conventional TBNA and EBUS-TBNATo be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for
conventional methodAug 23 2015 middot Can you help by adding an answerAdd your answer
Is conventional transbronchial needle aspiration (TBNA) obsolete απαρχαιωμένη Available from httpswwwresearchgatenetpost
[accessed Apr 17 2017]
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
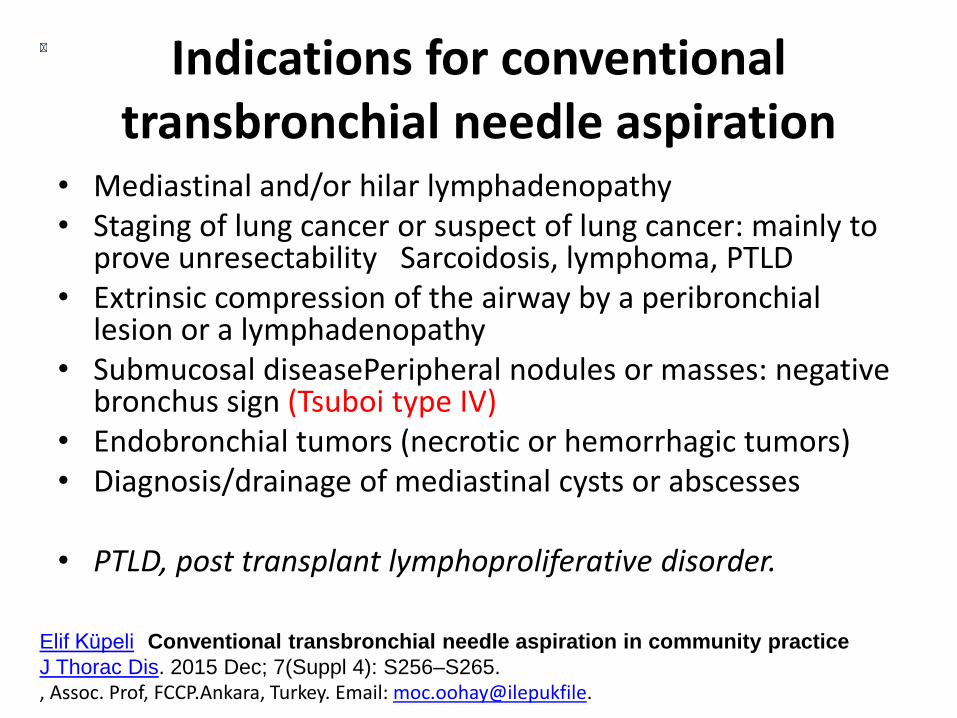
Indications for conventional transbronchial needle aspiration
bull Mediastinal andor hilar lymphadenopathybull Staging of lung cancer or suspect of lung cancer mainly to
prove unresectability Sarcoidosis lymphoma PTLDbull Extrinsic compression of the airway by a peribronchial
lesion or a lymphadenopathybull Submucosal diseasePeripheral nodules or masses negative
bronchus sign (Tsuboi type IV)bull Endobronchial tumors (necrotic or hemorrhagic tumors)bull Diagnosisdrainage of mediastinal cysts or abscesses
bull PTLD post transplant lymphoproliferative disorder
Elif Kuumlpeli Conventional transbronchial needle aspiration in community practice
J Thorac Dis 2015 Dec 7(Suppl 4) S256ndashS265
Assoc Prof FCCPAnkara Turkey Email mocoohayilepukfile
RESULTSOur analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90
lymph nodes were smaller than 100 mm The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929 The most common histological diagnosis was adenocarcinoma
Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Sebastiaacuten Fernaacutendez-Bussy Gonzalo Labarca Sofia Canals Ivaacuten Caviedes Erik Folch Adnan MajidJ Bras Pneumol 2015 May-Jun 41(3) 219ndash224
J Bronchology Interv Pulmonol 2012 Jul19(3)182-7 doi Comparative cost analysis of endobronchial ultrasound-guided and blind
TBNA in the evaluation of hilar and mediastinal lymphadenopathyGrove DA1 Bechara RI Josephs JS Berkowitz DM
bull BACKGROUND bull The superior accuracy of endobronchial ultrasound (EBUS) averts many diagnostic surgical procedures This
likely leads to significant cost savings despite an increased per procedure cost We sought to compare the true costs of endobronchial ultrasound-transbronchial needle aspiration (EBUS-TBNA) compared with blind fiberoptic bronchoscopy-transbronchial needle aspiration (FB-TBNA) factoring in the impact of diagnostic surgical procedures in the diagnosis of mediastinal lymphadenopathy
bull METHODS bull In this retrospective case study we selected 294 patients with thoracic lymphadenopathy as diagnosed by
computed tomography at a university hospital Information was extracted from the electronic record Costs were determined from the Centers for Medicare and Medicaid Services resource-based relative value scale We defined a positive diagnosis as one where benign or malignant disease was found A negative biopsy was one where lymph node sampling was confirmed but no pathology (benign or malignant) was seen A nondiagnosticbiopsy was one where no pathology was seen and lymph node sampling could not be confirmed The total cost of endoscopic and surgical diagnostic procedures was tallied for each patient to obtain mean costs per patient
bull RESULTS bull Thirty-seven patients underwent FB-TBNA and 257 underwent EBUS-TBNA A diagnosis was found in 90 of
patients in the EBUS group and 622 of patients in the FB-TBNA group (Plt0001) More patients in the FB-TBNA group underwent a diagnostic surgical procedure (HR= -01573 95 confidence interval -030 to -015 Plt0001) After accounting for all diagnostic procedures the mean savings with EBUS was $107109 (P=009) per patient
bull CONCLUSIONS bull EBUS-TBNA is less expensive than blind FB-TBNA in the
evaluation of thoracic lymphadenopathy when accounting for diagnostic surgical procedures
Trisolini Rocco MD Gasparini Stefano MDdagger Is It Time for Conventional TBNA to Die
Journalof Bronchology amp Interventional Pulmonology October 2013 - Volume 20 - Issue 4 - p 368ndash369
bull It is possible that the most cost-effective diagnostic approach is to use conventional TBNA for large (gt15 to 2 cm) and easy-to-sample (stations 4 R andor 7) lymph nodes and to reserve EBUS-TBNA for smaller or less accessible nodes or for situations when conventional TBNA has failed
bull Furthermore it seems at least questionable to conclude that EBUS-TBNA is less expensive than conventional TBNA on the basis of a retrospective comparison of merely 37 cases of conventional TBNA performed at the beginning of the study time (March 2006) with 257 of EBUS-TBNA performed during the following 4 years without considering the cost of the EBUS equipment the different needle costs the maintenance costs of EBUS and the potential cost of acquiring operator skills
nodeThrombus
vessel
21 or 22 gauge
Advantages and disadvantages of various mediastinal staging procedures in lung cancer
Procedure Advantages Disadvantages
Thoracotomy (surgical opening of the chest)Allows the most thorough inspection and sampling of lymph node stations may be followed by resection of tumor if feasible
Most invasive approach not indicated for staging alone significant risk of procedure-related morbidity
Extended cervical mediastinoscopy combined with a Chamberlain procedure which is also called a left parasternal mediastinotomy or anterior mediastinotomy
Permits evaluation of the aortopulmonary window lymph nodes
More invasive false-negative rate approximately 10
Chamberlain procedureAccess to station 5 (aortopulmonary windowlymph node)
Limited applications invasive
Cervical mediastinoscopyStill considered the gold standard (usual comparitor) by many excellent for 2RL 4RL
Does not cover all medastinal lymph node stations particularly subcarinal lymph nodes (station 7) paraesophageal and pulmonary ligament lymph nodes (stations 8 and 9) the aortopulmonary window lymph nodes (station 5) and the anterior mediastinal lymph nodes (station 6) false-negative rate approximately 20 invasive
Video-assisted thoracoscopyGood for inferior mediastinum station 5 and 6 lymph nodes
Invasive does not cover superior anterior mediastinum
Transthoracic percutaneous fine needle aspiration (FNA) under CT guidance
More widely available than some other methodsTraverses a lot of lung tissue therefore high pneumothorax risk some lymph node stations inaccessible
Bronchoscopy with blind transbronchial FNA (Wang needle)
Less invasive than above methodsRelatively low yield not widely practiced bleeding risk
Endobronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound (EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station 5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheallymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
bronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound(EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station
5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheal lymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
Endobronchial ultrasound (EBUS) mini radial probe image
A) The radial probe endobronchial ultrasound image demonstrates six distinct layers of the bronchial wall Layers 1 and 2 are the mucosa submucosa and muscle Layers 3 and 4 are the cartilage Layers 5 and 6 are the adventitia Layers 1 3 and 5 appear hyperechoic because they are interfaces B) Cross section of a normal bronchus
Endobronchial ultrasound (EBUS) peripheral nodule sampling II
Associate Prof of PulmonologyCo-director 5th Pulmonary DepartmentIzmir Dr Suat Seren Training amp Research Hospital for Thoracic Medicine amp Surgery35110 Yenisehir Izmir TurkeyTEL 90-532 661 45 22 FAX 90-232-362 28 31E-MAIL sbilaceroglu [AT] gmail [DOT] com
Semra Bilaceroglu Dr Suat Seren GoumlğuumlsHastalıkları Ve Cerrahisi Eğitim Ve Ara
How do you decide on whether to use conventional TBNA or EBUS-TBNA
I want to see views of bronchoscopists from different countries
TopicsInterventional Pulmonology Aug 11 2015 All
Answers (11)
Eman Sobh middot Al-Azhar University Hi Semra EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult
cases Aug 12 2015 middot Herveacute Dutau middot Assistance Publique Hocircpitaux de Marseille Semra I use TBNA- for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of ordercheersAug 12 2015 middot Suveer Singh middot Imperial College London Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cellsIt is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomybwSuveerAug 13 2015 middot Johannes M Daniels middot VU University Medical Center TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNAA problem is that there are so few cases that it becomes difficult to pass on the skillsAug 13 2015 middot Vicente Roig-Figueroa middot Hospital Cliacutenico Universitario de Valladolid In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11LAug 15 2015 middot Eman Sobh middot Al-Azhar University our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are
availableAug 15 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiI am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNAEBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm) For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA Aug 16 2015 middot Michel Febvre middot Hocircpital Tenon (Hocircpitaux Universitaires Est Parisien) Hello Semra interesting questionI was a hard defender of conventionnal TBNA for LN gt 20 mm in station 7 or 4R or tumors adjacent to the airways because it is quick and easyDespite that we have the chance of having 4 EBUS scopes in our department and it is now roughly as quick to do an EBUS so we use EBUS under local and premedication in 95 of the time The two other reasons of
using EBUS is teaching and sometimes doing EUS with the EBUS scopeNevertheless I continue to think that there is a place for conventionnal TBNA in centers for which EBUS is too expensive and indications less frequent for diagnosis of large mediastinal lymph nodes or tumors
Teaching conventionnal TBNA should be pursuedSincerelyAug 19 2015 middot Maria Majori middot University Hospital of Parma In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases)I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the
confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy
Otherwise it would be like driving a Ferrari just learned to driveBest regards to All of YouAug 21 2015 middot Mace M Schuurmans middot University of Zurich For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind
TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
Aug 22 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiThank you for all these answers Its important to have appropriate indications for conventional TBNA and EBUS-TBNATo be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for
conventional methodAug 23 2015 middot Can you help by adding an answerAdd your answer
Is conventional transbronchial needle aspiration (TBNA) obsolete απαρχαιωμένη Available from httpswwwresearchgatenetpost
[accessed Apr 17 2017]
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
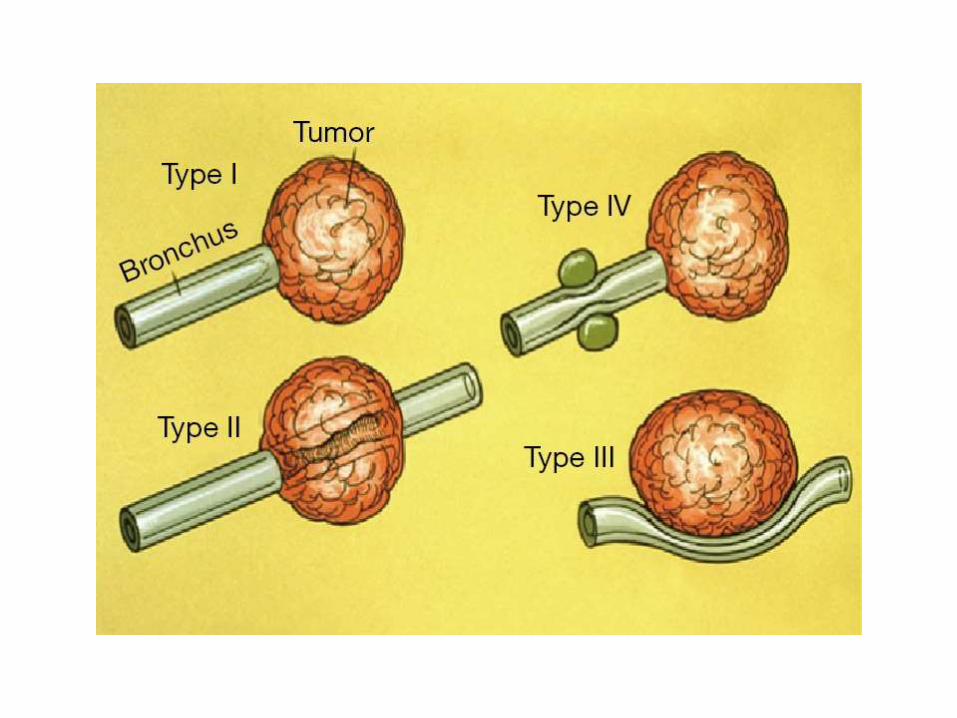
RESULTSOur analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90
lymph nodes were smaller than 100 mm The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929 The most common histological diagnosis was adenocarcinoma
Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Sebastiaacuten Fernaacutendez-Bussy Gonzalo Labarca Sofia Canals Ivaacuten Caviedes Erik Folch Adnan MajidJ Bras Pneumol 2015 May-Jun 41(3) 219ndash224
J Bronchology Interv Pulmonol 2012 Jul19(3)182-7 doi Comparative cost analysis of endobronchial ultrasound-guided and blind
TBNA in the evaluation of hilar and mediastinal lymphadenopathyGrove DA1 Bechara RI Josephs JS Berkowitz DM
bull BACKGROUND bull The superior accuracy of endobronchial ultrasound (EBUS) averts many diagnostic surgical procedures This
likely leads to significant cost savings despite an increased per procedure cost We sought to compare the true costs of endobronchial ultrasound-transbronchial needle aspiration (EBUS-TBNA) compared with blind fiberoptic bronchoscopy-transbronchial needle aspiration (FB-TBNA) factoring in the impact of diagnostic surgical procedures in the diagnosis of mediastinal lymphadenopathy
bull METHODS bull In this retrospective case study we selected 294 patients with thoracic lymphadenopathy as diagnosed by
computed tomography at a university hospital Information was extracted from the electronic record Costs were determined from the Centers for Medicare and Medicaid Services resource-based relative value scale We defined a positive diagnosis as one where benign or malignant disease was found A negative biopsy was one where lymph node sampling was confirmed but no pathology (benign or malignant) was seen A nondiagnosticbiopsy was one where no pathology was seen and lymph node sampling could not be confirmed The total cost of endoscopic and surgical diagnostic procedures was tallied for each patient to obtain mean costs per patient
bull RESULTS bull Thirty-seven patients underwent FB-TBNA and 257 underwent EBUS-TBNA A diagnosis was found in 90 of
patients in the EBUS group and 622 of patients in the FB-TBNA group (Plt0001) More patients in the FB-TBNA group underwent a diagnostic surgical procedure (HR= -01573 95 confidence interval -030 to -015 Plt0001) After accounting for all diagnostic procedures the mean savings with EBUS was $107109 (P=009) per patient
bull CONCLUSIONS bull EBUS-TBNA is less expensive than blind FB-TBNA in the
evaluation of thoracic lymphadenopathy when accounting for diagnostic surgical procedures
Trisolini Rocco MD Gasparini Stefano MDdagger Is It Time for Conventional TBNA to Die
Journalof Bronchology amp Interventional Pulmonology October 2013 - Volume 20 - Issue 4 - p 368ndash369
bull It is possible that the most cost-effective diagnostic approach is to use conventional TBNA for large (gt15 to 2 cm) and easy-to-sample (stations 4 R andor 7) lymph nodes and to reserve EBUS-TBNA for smaller or less accessible nodes or for situations when conventional TBNA has failed
bull Furthermore it seems at least questionable to conclude that EBUS-TBNA is less expensive than conventional TBNA on the basis of a retrospective comparison of merely 37 cases of conventional TBNA performed at the beginning of the study time (March 2006) with 257 of EBUS-TBNA performed during the following 4 years without considering the cost of the EBUS equipment the different needle costs the maintenance costs of EBUS and the potential cost of acquiring operator skills
nodeThrombus
vessel
21 or 22 gauge
Advantages and disadvantages of various mediastinal staging procedures in lung cancer
Procedure Advantages Disadvantages
Thoracotomy (surgical opening of the chest)Allows the most thorough inspection and sampling of lymph node stations may be followed by resection of tumor if feasible
Most invasive approach not indicated for staging alone significant risk of procedure-related morbidity
Extended cervical mediastinoscopy combined with a Chamberlain procedure which is also called a left parasternal mediastinotomy or anterior mediastinotomy
Permits evaluation of the aortopulmonary window lymph nodes
More invasive false-negative rate approximately 10
Chamberlain procedureAccess to station 5 (aortopulmonary windowlymph node)
Limited applications invasive
Cervical mediastinoscopyStill considered the gold standard (usual comparitor) by many excellent for 2RL 4RL
Does not cover all medastinal lymph node stations particularly subcarinal lymph nodes (station 7) paraesophageal and pulmonary ligament lymph nodes (stations 8 and 9) the aortopulmonary window lymph nodes (station 5) and the anterior mediastinal lymph nodes (station 6) false-negative rate approximately 20 invasive
Video-assisted thoracoscopyGood for inferior mediastinum station 5 and 6 lymph nodes
Invasive does not cover superior anterior mediastinum
Transthoracic percutaneous fine needle aspiration (FNA) under CT guidance
More widely available than some other methodsTraverses a lot of lung tissue therefore high pneumothorax risk some lymph node stations inaccessible
Bronchoscopy with blind transbronchial FNA (Wang needle)
Less invasive than above methodsRelatively low yield not widely practiced bleeding risk
Endobronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound (EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station 5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheallymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
bronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound(EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station
5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheal lymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
Endobronchial ultrasound (EBUS) mini radial probe image
A) The radial probe endobronchial ultrasound image demonstrates six distinct layers of the bronchial wall Layers 1 and 2 are the mucosa submucosa and muscle Layers 3 and 4 are the cartilage Layers 5 and 6 are the adventitia Layers 1 3 and 5 appear hyperechoic because they are interfaces B) Cross section of a normal bronchus
Endobronchial ultrasound (EBUS) peripheral nodule sampling II
Associate Prof of PulmonologyCo-director 5th Pulmonary DepartmentIzmir Dr Suat Seren Training amp Research Hospital for Thoracic Medicine amp Surgery35110 Yenisehir Izmir TurkeyTEL 90-532 661 45 22 FAX 90-232-362 28 31E-MAIL sbilaceroglu [AT] gmail [DOT] com
Semra Bilaceroglu Dr Suat Seren GoumlğuumlsHastalıkları Ve Cerrahisi Eğitim Ve Ara
How do you decide on whether to use conventional TBNA or EBUS-TBNA
I want to see views of bronchoscopists from different countries
TopicsInterventional Pulmonology Aug 11 2015 All
Answers (11)
Eman Sobh middot Al-Azhar University Hi Semra EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult
cases Aug 12 2015 middot Herveacute Dutau middot Assistance Publique Hocircpitaux de Marseille Semra I use TBNA- for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of ordercheersAug 12 2015 middot Suveer Singh middot Imperial College London Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cellsIt is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomybwSuveerAug 13 2015 middot Johannes M Daniels middot VU University Medical Center TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNAA problem is that there are so few cases that it becomes difficult to pass on the skillsAug 13 2015 middot Vicente Roig-Figueroa middot Hospital Cliacutenico Universitario de Valladolid In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11LAug 15 2015 middot Eman Sobh middot Al-Azhar University our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are
availableAug 15 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiI am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNAEBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm) For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA Aug 16 2015 middot Michel Febvre middot Hocircpital Tenon (Hocircpitaux Universitaires Est Parisien) Hello Semra interesting questionI was a hard defender of conventionnal TBNA for LN gt 20 mm in station 7 or 4R or tumors adjacent to the airways because it is quick and easyDespite that we have the chance of having 4 EBUS scopes in our department and it is now roughly as quick to do an EBUS so we use EBUS under local and premedication in 95 of the time The two other reasons of
using EBUS is teaching and sometimes doing EUS with the EBUS scopeNevertheless I continue to think that there is a place for conventionnal TBNA in centers for which EBUS is too expensive and indications less frequent for diagnosis of large mediastinal lymph nodes or tumors
Teaching conventionnal TBNA should be pursuedSincerelyAug 19 2015 middot Maria Majori middot University Hospital of Parma In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases)I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the
confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy
Otherwise it would be like driving a Ferrari just learned to driveBest regards to All of YouAug 21 2015 middot Mace M Schuurmans middot University of Zurich For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind
TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
Aug 22 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiThank you for all these answers Its important to have appropriate indications for conventional TBNA and EBUS-TBNATo be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for
conventional methodAug 23 2015 middot Can you help by adding an answerAdd your answer
Is conventional transbronchial needle aspiration (TBNA) obsolete απαρχαιωμένη Available from httpswwwresearchgatenetpost
[accessed Apr 17 2017]
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
J Bronchology Interv Pulmonol 2012 Jul19(3)182-7 doi Comparative cost analysis of endobronchial ultrasound-guided and blind
TBNA in the evaluation of hilar and mediastinal lymphadenopathyGrove DA1 Bechara RI Josephs JS Berkowitz DM
bull BACKGROUND bull The superior accuracy of endobronchial ultrasound (EBUS) averts many diagnostic surgical procedures This
likely leads to significant cost savings despite an increased per procedure cost We sought to compare the true costs of endobronchial ultrasound-transbronchial needle aspiration (EBUS-TBNA) compared with blind fiberoptic bronchoscopy-transbronchial needle aspiration (FB-TBNA) factoring in the impact of diagnostic surgical procedures in the diagnosis of mediastinal lymphadenopathy
bull METHODS bull In this retrospective case study we selected 294 patients with thoracic lymphadenopathy as diagnosed by
computed tomography at a university hospital Information was extracted from the electronic record Costs were determined from the Centers for Medicare and Medicaid Services resource-based relative value scale We defined a positive diagnosis as one where benign or malignant disease was found A negative biopsy was one where lymph node sampling was confirmed but no pathology (benign or malignant) was seen A nondiagnosticbiopsy was one where no pathology was seen and lymph node sampling could not be confirmed The total cost of endoscopic and surgical diagnostic procedures was tallied for each patient to obtain mean costs per patient
bull RESULTS bull Thirty-seven patients underwent FB-TBNA and 257 underwent EBUS-TBNA A diagnosis was found in 90 of
patients in the EBUS group and 622 of patients in the FB-TBNA group (Plt0001) More patients in the FB-TBNA group underwent a diagnostic surgical procedure (HR= -01573 95 confidence interval -030 to -015 Plt0001) After accounting for all diagnostic procedures the mean savings with EBUS was $107109 (P=009) per patient
bull CONCLUSIONS bull EBUS-TBNA is less expensive than blind FB-TBNA in the
evaluation of thoracic lymphadenopathy when accounting for diagnostic surgical procedures
Trisolini Rocco MD Gasparini Stefano MDdagger Is It Time for Conventional TBNA to Die
Journalof Bronchology amp Interventional Pulmonology October 2013 - Volume 20 - Issue 4 - p 368ndash369
bull It is possible that the most cost-effective diagnostic approach is to use conventional TBNA for large (gt15 to 2 cm) and easy-to-sample (stations 4 R andor 7) lymph nodes and to reserve EBUS-TBNA for smaller or less accessible nodes or for situations when conventional TBNA has failed
bull Furthermore it seems at least questionable to conclude that EBUS-TBNA is less expensive than conventional TBNA on the basis of a retrospective comparison of merely 37 cases of conventional TBNA performed at the beginning of the study time (March 2006) with 257 of EBUS-TBNA performed during the following 4 years without considering the cost of the EBUS equipment the different needle costs the maintenance costs of EBUS and the potential cost of acquiring operator skills
nodeThrombus
vessel
21 or 22 gauge
Advantages and disadvantages of various mediastinal staging procedures in lung cancer
Procedure Advantages Disadvantages
Thoracotomy (surgical opening of the chest)Allows the most thorough inspection and sampling of lymph node stations may be followed by resection of tumor if feasible
Most invasive approach not indicated for staging alone significant risk of procedure-related morbidity
Extended cervical mediastinoscopy combined with a Chamberlain procedure which is also called a left parasternal mediastinotomy or anterior mediastinotomy
Permits evaluation of the aortopulmonary window lymph nodes
More invasive false-negative rate approximately 10
Chamberlain procedureAccess to station 5 (aortopulmonary windowlymph node)
Limited applications invasive
Cervical mediastinoscopyStill considered the gold standard (usual comparitor) by many excellent for 2RL 4RL
Does not cover all medastinal lymph node stations particularly subcarinal lymph nodes (station 7) paraesophageal and pulmonary ligament lymph nodes (stations 8 and 9) the aortopulmonary window lymph nodes (station 5) and the anterior mediastinal lymph nodes (station 6) false-negative rate approximately 20 invasive
Video-assisted thoracoscopyGood for inferior mediastinum station 5 and 6 lymph nodes
Invasive does not cover superior anterior mediastinum
Transthoracic percutaneous fine needle aspiration (FNA) under CT guidance
More widely available than some other methodsTraverses a lot of lung tissue therefore high pneumothorax risk some lymph node stations inaccessible
Bronchoscopy with blind transbronchial FNA (Wang needle)
Less invasive than above methodsRelatively low yield not widely practiced bleeding risk
Endobronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound (EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station 5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheallymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
bronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound(EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station
5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheal lymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
Endobronchial ultrasound (EBUS) mini radial probe image
A) The radial probe endobronchial ultrasound image demonstrates six distinct layers of the bronchial wall Layers 1 and 2 are the mucosa submucosa and muscle Layers 3 and 4 are the cartilage Layers 5 and 6 are the adventitia Layers 1 3 and 5 appear hyperechoic because they are interfaces B) Cross section of a normal bronchus
Endobronchial ultrasound (EBUS) peripheral nodule sampling II
Associate Prof of PulmonologyCo-director 5th Pulmonary DepartmentIzmir Dr Suat Seren Training amp Research Hospital for Thoracic Medicine amp Surgery35110 Yenisehir Izmir TurkeyTEL 90-532 661 45 22 FAX 90-232-362 28 31E-MAIL sbilaceroglu [AT] gmail [DOT] com
Semra Bilaceroglu Dr Suat Seren GoumlğuumlsHastalıkları Ve Cerrahisi Eğitim Ve Ara
How do you decide on whether to use conventional TBNA or EBUS-TBNA
I want to see views of bronchoscopists from different countries
TopicsInterventional Pulmonology Aug 11 2015 All
Answers (11)
Eman Sobh middot Al-Azhar University Hi Semra EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult
cases Aug 12 2015 middot Herveacute Dutau middot Assistance Publique Hocircpitaux de Marseille Semra I use TBNA- for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of ordercheersAug 12 2015 middot Suveer Singh middot Imperial College London Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cellsIt is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomybwSuveerAug 13 2015 middot Johannes M Daniels middot VU University Medical Center TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNAA problem is that there are so few cases that it becomes difficult to pass on the skillsAug 13 2015 middot Vicente Roig-Figueroa middot Hospital Cliacutenico Universitario de Valladolid In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11LAug 15 2015 middot Eman Sobh middot Al-Azhar University our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are
availableAug 15 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiI am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNAEBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm) For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA Aug 16 2015 middot Michel Febvre middot Hocircpital Tenon (Hocircpitaux Universitaires Est Parisien) Hello Semra interesting questionI was a hard defender of conventionnal TBNA for LN gt 20 mm in station 7 or 4R or tumors adjacent to the airways because it is quick and easyDespite that we have the chance of having 4 EBUS scopes in our department and it is now roughly as quick to do an EBUS so we use EBUS under local and premedication in 95 of the time The two other reasons of
using EBUS is teaching and sometimes doing EUS with the EBUS scopeNevertheless I continue to think that there is a place for conventionnal TBNA in centers for which EBUS is too expensive and indications less frequent for diagnosis of large mediastinal lymph nodes or tumors
Teaching conventionnal TBNA should be pursuedSincerelyAug 19 2015 middot Maria Majori middot University Hospital of Parma In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases)I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the
confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy
Otherwise it would be like driving a Ferrari just learned to driveBest regards to All of YouAug 21 2015 middot Mace M Schuurmans middot University of Zurich For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind
TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
Aug 22 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiThank you for all these answers Its important to have appropriate indications for conventional TBNA and EBUS-TBNATo be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for
conventional methodAug 23 2015 middot Can you help by adding an answerAdd your answer
Is conventional transbronchial needle aspiration (TBNA) obsolete απαρχαιωμένη Available from httpswwwresearchgatenetpost
[accessed Apr 17 2017]
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
Trisolini Rocco MD Gasparini Stefano MDdagger Is It Time for Conventional TBNA to Die
Journalof Bronchology amp Interventional Pulmonology October 2013 - Volume 20 - Issue 4 - p 368ndash369
bull It is possible that the most cost-effective diagnostic approach is to use conventional TBNA for large (gt15 to 2 cm) and easy-to-sample (stations 4 R andor 7) lymph nodes and to reserve EBUS-TBNA for smaller or less accessible nodes or for situations when conventional TBNA has failed
bull Furthermore it seems at least questionable to conclude that EBUS-TBNA is less expensive than conventional TBNA on the basis of a retrospective comparison of merely 37 cases of conventional TBNA performed at the beginning of the study time (March 2006) with 257 of EBUS-TBNA performed during the following 4 years without considering the cost of the EBUS equipment the different needle costs the maintenance costs of EBUS and the potential cost of acquiring operator skills
nodeThrombus
vessel
21 or 22 gauge
Advantages and disadvantages of various mediastinal staging procedures in lung cancer
Procedure Advantages Disadvantages
Thoracotomy (surgical opening of the chest)Allows the most thorough inspection and sampling of lymph node stations may be followed by resection of tumor if feasible
Most invasive approach not indicated for staging alone significant risk of procedure-related morbidity
Extended cervical mediastinoscopy combined with a Chamberlain procedure which is also called a left parasternal mediastinotomy or anterior mediastinotomy
Permits evaluation of the aortopulmonary window lymph nodes
More invasive false-negative rate approximately 10
Chamberlain procedureAccess to station 5 (aortopulmonary windowlymph node)
Limited applications invasive
Cervical mediastinoscopyStill considered the gold standard (usual comparitor) by many excellent for 2RL 4RL
Does not cover all medastinal lymph node stations particularly subcarinal lymph nodes (station 7) paraesophageal and pulmonary ligament lymph nodes (stations 8 and 9) the aortopulmonary window lymph nodes (station 5) and the anterior mediastinal lymph nodes (station 6) false-negative rate approximately 20 invasive
Video-assisted thoracoscopyGood for inferior mediastinum station 5 and 6 lymph nodes
Invasive does not cover superior anterior mediastinum
Transthoracic percutaneous fine needle aspiration (FNA) under CT guidance
More widely available than some other methodsTraverses a lot of lung tissue therefore high pneumothorax risk some lymph node stations inaccessible
Bronchoscopy with blind transbronchial FNA (Wang needle)
Less invasive than above methodsRelatively low yield not widely practiced bleeding risk
Endobronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound (EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station 5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheallymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
bronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound(EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station
5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheal lymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
Endobronchial ultrasound (EBUS) mini radial probe image
A) The radial probe endobronchial ultrasound image demonstrates six distinct layers of the bronchial wall Layers 1 and 2 are the mucosa submucosa and muscle Layers 3 and 4 are the cartilage Layers 5 and 6 are the adventitia Layers 1 3 and 5 appear hyperechoic because they are interfaces B) Cross section of a normal bronchus
Endobronchial ultrasound (EBUS) peripheral nodule sampling II
Associate Prof of PulmonologyCo-director 5th Pulmonary DepartmentIzmir Dr Suat Seren Training amp Research Hospital for Thoracic Medicine amp Surgery35110 Yenisehir Izmir TurkeyTEL 90-532 661 45 22 FAX 90-232-362 28 31E-MAIL sbilaceroglu [AT] gmail [DOT] com
Semra Bilaceroglu Dr Suat Seren GoumlğuumlsHastalıkları Ve Cerrahisi Eğitim Ve Ara
How do you decide on whether to use conventional TBNA or EBUS-TBNA
I want to see views of bronchoscopists from different countries
TopicsInterventional Pulmonology Aug 11 2015 All
Answers (11)
Eman Sobh middot Al-Azhar University Hi Semra EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult
cases Aug 12 2015 middot Herveacute Dutau middot Assistance Publique Hocircpitaux de Marseille Semra I use TBNA- for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of ordercheersAug 12 2015 middot Suveer Singh middot Imperial College London Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cellsIt is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomybwSuveerAug 13 2015 middot Johannes M Daniels middot VU University Medical Center TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNAA problem is that there are so few cases that it becomes difficult to pass on the skillsAug 13 2015 middot Vicente Roig-Figueroa middot Hospital Cliacutenico Universitario de Valladolid In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11LAug 15 2015 middot Eman Sobh middot Al-Azhar University our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are
availableAug 15 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiI am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNAEBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm) For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA Aug 16 2015 middot Michel Febvre middot Hocircpital Tenon (Hocircpitaux Universitaires Est Parisien) Hello Semra interesting questionI was a hard defender of conventionnal TBNA for LN gt 20 mm in station 7 or 4R or tumors adjacent to the airways because it is quick and easyDespite that we have the chance of having 4 EBUS scopes in our department and it is now roughly as quick to do an EBUS so we use EBUS under local and premedication in 95 of the time The two other reasons of
using EBUS is teaching and sometimes doing EUS with the EBUS scopeNevertheless I continue to think that there is a place for conventionnal TBNA in centers for which EBUS is too expensive and indications less frequent for diagnosis of large mediastinal lymph nodes or tumors
Teaching conventionnal TBNA should be pursuedSincerelyAug 19 2015 middot Maria Majori middot University Hospital of Parma In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases)I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the
confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy
Otherwise it would be like driving a Ferrari just learned to driveBest regards to All of YouAug 21 2015 middot Mace M Schuurmans middot University of Zurich For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind
TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
Aug 22 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiThank you for all these answers Its important to have appropriate indications for conventional TBNA and EBUS-TBNATo be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for
conventional methodAug 23 2015 middot Can you help by adding an answerAdd your answer
Is conventional transbronchial needle aspiration (TBNA) obsolete απαρχαιωμένη Available from httpswwwresearchgatenetpost
[accessed Apr 17 2017]
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
nodeThrombus
vessel
21 or 22 gauge
Advantages and disadvantages of various mediastinal staging procedures in lung cancer
Procedure Advantages Disadvantages
Thoracotomy (surgical opening of the chest)Allows the most thorough inspection and sampling of lymph node stations may be followed by resection of tumor if feasible
Most invasive approach not indicated for staging alone significant risk of procedure-related morbidity
Extended cervical mediastinoscopy combined with a Chamberlain procedure which is also called a left parasternal mediastinotomy or anterior mediastinotomy
Permits evaluation of the aortopulmonary window lymph nodes
More invasive false-negative rate approximately 10
Chamberlain procedureAccess to station 5 (aortopulmonary windowlymph node)
Limited applications invasive
Cervical mediastinoscopyStill considered the gold standard (usual comparitor) by many excellent for 2RL 4RL
Does not cover all medastinal lymph node stations particularly subcarinal lymph nodes (station 7) paraesophageal and pulmonary ligament lymph nodes (stations 8 and 9) the aortopulmonary window lymph nodes (station 5) and the anterior mediastinal lymph nodes (station 6) false-negative rate approximately 20 invasive
Video-assisted thoracoscopyGood for inferior mediastinum station 5 and 6 lymph nodes
Invasive does not cover superior anterior mediastinum
Transthoracic percutaneous fine needle aspiration (FNA) under CT guidance
More widely available than some other methodsTraverses a lot of lung tissue therefore high pneumothorax risk some lymph node stations inaccessible
Bronchoscopy with blind transbronchial FNA (Wang needle)
Less invasive than above methodsRelatively low yield not widely practiced bleeding risk
Endobronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound (EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station 5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheallymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
bronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound(EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station
5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheal lymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
Endobronchial ultrasound (EBUS) mini radial probe image
A) The radial probe endobronchial ultrasound image demonstrates six distinct layers of the bronchial wall Layers 1 and 2 are the mucosa submucosa and muscle Layers 3 and 4 are the cartilage Layers 5 and 6 are the adventitia Layers 1 3 and 5 appear hyperechoic because they are interfaces B) Cross section of a normal bronchus
Endobronchial ultrasound (EBUS) peripheral nodule sampling II
Associate Prof of PulmonologyCo-director 5th Pulmonary DepartmentIzmir Dr Suat Seren Training amp Research Hospital for Thoracic Medicine amp Surgery35110 Yenisehir Izmir TurkeyTEL 90-532 661 45 22 FAX 90-232-362 28 31E-MAIL sbilaceroglu [AT] gmail [DOT] com
Semra Bilaceroglu Dr Suat Seren GoumlğuumlsHastalıkları Ve Cerrahisi Eğitim Ve Ara
How do you decide on whether to use conventional TBNA or EBUS-TBNA
I want to see views of bronchoscopists from different countries
TopicsInterventional Pulmonology Aug 11 2015 All
Answers (11)
Eman Sobh middot Al-Azhar University Hi Semra EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult
cases Aug 12 2015 middot Herveacute Dutau middot Assistance Publique Hocircpitaux de Marseille Semra I use TBNA- for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of ordercheersAug 12 2015 middot Suveer Singh middot Imperial College London Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cellsIt is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomybwSuveerAug 13 2015 middot Johannes M Daniels middot VU University Medical Center TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNAA problem is that there are so few cases that it becomes difficult to pass on the skillsAug 13 2015 middot Vicente Roig-Figueroa middot Hospital Cliacutenico Universitario de Valladolid In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11LAug 15 2015 middot Eman Sobh middot Al-Azhar University our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are
availableAug 15 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiI am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNAEBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm) For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA Aug 16 2015 middot Michel Febvre middot Hocircpital Tenon (Hocircpitaux Universitaires Est Parisien) Hello Semra interesting questionI was a hard defender of conventionnal TBNA for LN gt 20 mm in station 7 or 4R or tumors adjacent to the airways because it is quick and easyDespite that we have the chance of having 4 EBUS scopes in our department and it is now roughly as quick to do an EBUS so we use EBUS under local and premedication in 95 of the time The two other reasons of
using EBUS is teaching and sometimes doing EUS with the EBUS scopeNevertheless I continue to think that there is a place for conventionnal TBNA in centers for which EBUS is too expensive and indications less frequent for diagnosis of large mediastinal lymph nodes or tumors
Teaching conventionnal TBNA should be pursuedSincerelyAug 19 2015 middot Maria Majori middot University Hospital of Parma In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases)I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the
confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy
Otherwise it would be like driving a Ferrari just learned to driveBest regards to All of YouAug 21 2015 middot Mace M Schuurmans middot University of Zurich For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind
TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
Aug 22 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiThank you for all these answers Its important to have appropriate indications for conventional TBNA and EBUS-TBNATo be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for
conventional methodAug 23 2015 middot Can you help by adding an answerAdd your answer
Is conventional transbronchial needle aspiration (TBNA) obsolete απαρχαιωμένη Available from httpswwwresearchgatenetpost
[accessed Apr 17 2017]
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
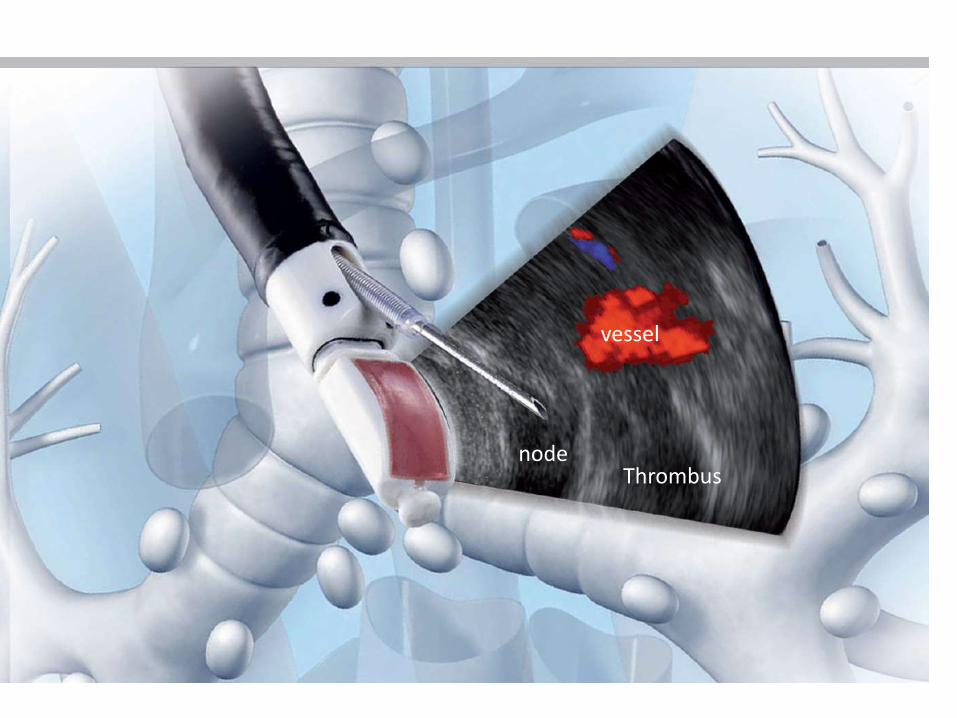
21 or 22 gauge
Advantages and disadvantages of various mediastinal staging procedures in lung cancer
Procedure Advantages Disadvantages
Thoracotomy (surgical opening of the chest)Allows the most thorough inspection and sampling of lymph node stations may be followed by resection of tumor if feasible
Most invasive approach not indicated for staging alone significant risk of procedure-related morbidity
Extended cervical mediastinoscopy combined with a Chamberlain procedure which is also called a left parasternal mediastinotomy or anterior mediastinotomy
Permits evaluation of the aortopulmonary window lymph nodes
More invasive false-negative rate approximately 10
Chamberlain procedureAccess to station 5 (aortopulmonary windowlymph node)
Limited applications invasive
Cervical mediastinoscopyStill considered the gold standard (usual comparitor) by many excellent for 2RL 4RL
Does not cover all medastinal lymph node stations particularly subcarinal lymph nodes (station 7) paraesophageal and pulmonary ligament lymph nodes (stations 8 and 9) the aortopulmonary window lymph nodes (station 5) and the anterior mediastinal lymph nodes (station 6) false-negative rate approximately 20 invasive
Video-assisted thoracoscopyGood for inferior mediastinum station 5 and 6 lymph nodes
Invasive does not cover superior anterior mediastinum
Transthoracic percutaneous fine needle aspiration (FNA) under CT guidance
More widely available than some other methodsTraverses a lot of lung tissue therefore high pneumothorax risk some lymph node stations inaccessible
Bronchoscopy with blind transbronchial FNA (Wang needle)
Less invasive than above methodsRelatively low yield not widely practiced bleeding risk
Endobronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound (EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station 5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheallymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
bronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound(EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station
5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheal lymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
Endobronchial ultrasound (EBUS) mini radial probe image
A) The radial probe endobronchial ultrasound image demonstrates six distinct layers of the bronchial wall Layers 1 and 2 are the mucosa submucosa and muscle Layers 3 and 4 are the cartilage Layers 5 and 6 are the adventitia Layers 1 3 and 5 appear hyperechoic because they are interfaces B) Cross section of a normal bronchus
Endobronchial ultrasound (EBUS) peripheral nodule sampling II
Associate Prof of PulmonologyCo-director 5th Pulmonary DepartmentIzmir Dr Suat Seren Training amp Research Hospital for Thoracic Medicine amp Surgery35110 Yenisehir Izmir TurkeyTEL 90-532 661 45 22 FAX 90-232-362 28 31E-MAIL sbilaceroglu [AT] gmail [DOT] com
Semra Bilaceroglu Dr Suat Seren GoumlğuumlsHastalıkları Ve Cerrahisi Eğitim Ve Ara
How do you decide on whether to use conventional TBNA or EBUS-TBNA
I want to see views of bronchoscopists from different countries
TopicsInterventional Pulmonology Aug 11 2015 All
Answers (11)
Eman Sobh middot Al-Azhar University Hi Semra EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult
cases Aug 12 2015 middot Herveacute Dutau middot Assistance Publique Hocircpitaux de Marseille Semra I use TBNA- for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of ordercheersAug 12 2015 middot Suveer Singh middot Imperial College London Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cellsIt is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomybwSuveerAug 13 2015 middot Johannes M Daniels middot VU University Medical Center TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNAA problem is that there are so few cases that it becomes difficult to pass on the skillsAug 13 2015 middot Vicente Roig-Figueroa middot Hospital Cliacutenico Universitario de Valladolid In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11LAug 15 2015 middot Eman Sobh middot Al-Azhar University our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are
availableAug 15 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiI am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNAEBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm) For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA Aug 16 2015 middot Michel Febvre middot Hocircpital Tenon (Hocircpitaux Universitaires Est Parisien) Hello Semra interesting questionI was a hard defender of conventionnal TBNA for LN gt 20 mm in station 7 or 4R or tumors adjacent to the airways because it is quick and easyDespite that we have the chance of having 4 EBUS scopes in our department and it is now roughly as quick to do an EBUS so we use EBUS under local and premedication in 95 of the time The two other reasons of
using EBUS is teaching and sometimes doing EUS with the EBUS scopeNevertheless I continue to think that there is a place for conventionnal TBNA in centers for which EBUS is too expensive and indications less frequent for diagnosis of large mediastinal lymph nodes or tumors
Teaching conventionnal TBNA should be pursuedSincerelyAug 19 2015 middot Maria Majori middot University Hospital of Parma In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases)I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the
confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy
Otherwise it would be like driving a Ferrari just learned to driveBest regards to All of YouAug 21 2015 middot Mace M Schuurmans middot University of Zurich For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind
TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
Aug 22 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiThank you for all these answers Its important to have appropriate indications for conventional TBNA and EBUS-TBNATo be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for
conventional methodAug 23 2015 middot Can you help by adding an answerAdd your answer
Is conventional transbronchial needle aspiration (TBNA) obsolete απαρχαιωμένη Available from httpswwwresearchgatenetpost
[accessed Apr 17 2017]
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
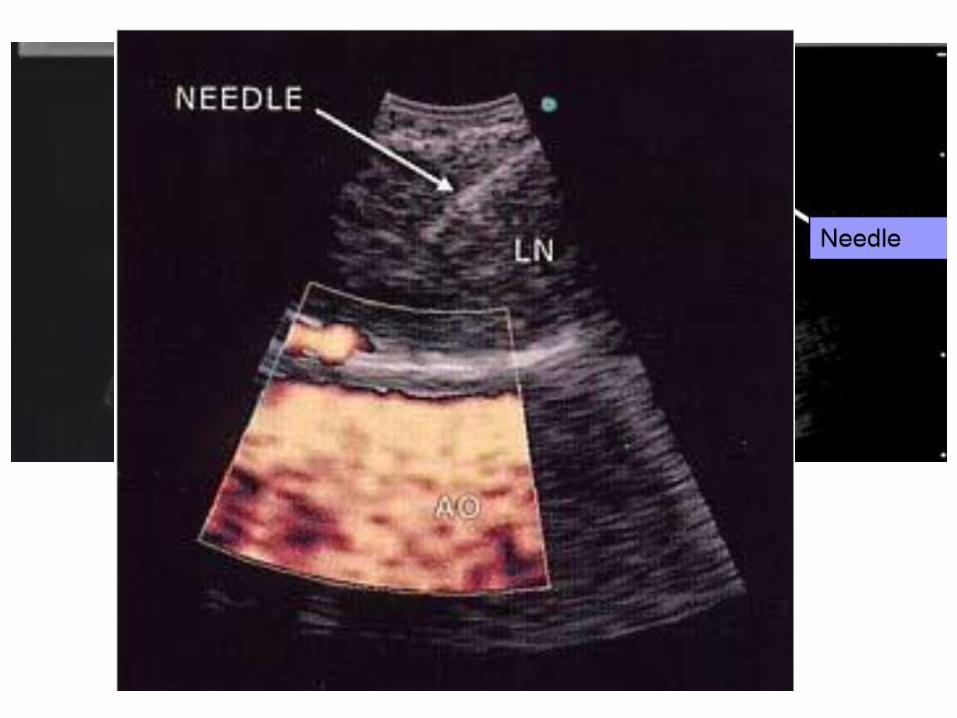
Advantages and disadvantages of various mediastinal staging procedures in lung cancer
Procedure Advantages Disadvantages
Thoracotomy (surgical opening of the chest)Allows the most thorough inspection and sampling of lymph node stations may be followed by resection of tumor if feasible
Most invasive approach not indicated for staging alone significant risk of procedure-related morbidity
Extended cervical mediastinoscopy combined with a Chamberlain procedure which is also called a left parasternal mediastinotomy or anterior mediastinotomy
Permits evaluation of the aortopulmonary window lymph nodes
More invasive false-negative rate approximately 10
Chamberlain procedureAccess to station 5 (aortopulmonary windowlymph node)
Limited applications invasive
Cervical mediastinoscopyStill considered the gold standard (usual comparitor) by many excellent for 2RL 4RL
Does not cover all medastinal lymph node stations particularly subcarinal lymph nodes (station 7) paraesophageal and pulmonary ligament lymph nodes (stations 8 and 9) the aortopulmonary window lymph nodes (station 5) and the anterior mediastinal lymph nodes (station 6) false-negative rate approximately 20 invasive
Video-assisted thoracoscopyGood for inferior mediastinum station 5 and 6 lymph nodes
Invasive does not cover superior anterior mediastinum
Transthoracic percutaneous fine needle aspiration (FNA) under CT guidance
More widely available than some other methodsTraverses a lot of lung tissue therefore high pneumothorax risk some lymph node stations inaccessible
Bronchoscopy with blind transbronchial FNA (Wang needle)
Less invasive than above methodsRelatively low yield not widely practiced bleeding risk
Endobronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound (EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station 5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheallymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
bronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound(EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station
5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheal lymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
Endobronchial ultrasound (EBUS) mini radial probe image
A) The radial probe endobronchial ultrasound image demonstrates six distinct layers of the bronchial wall Layers 1 and 2 are the mucosa submucosa and muscle Layers 3 and 4 are the cartilage Layers 5 and 6 are the adventitia Layers 1 3 and 5 appear hyperechoic because they are interfaces B) Cross section of a normal bronchus
Endobronchial ultrasound (EBUS) peripheral nodule sampling II
Associate Prof of PulmonologyCo-director 5th Pulmonary DepartmentIzmir Dr Suat Seren Training amp Research Hospital for Thoracic Medicine amp Surgery35110 Yenisehir Izmir TurkeyTEL 90-532 661 45 22 FAX 90-232-362 28 31E-MAIL sbilaceroglu [AT] gmail [DOT] com
Semra Bilaceroglu Dr Suat Seren GoumlğuumlsHastalıkları Ve Cerrahisi Eğitim Ve Ara
How do you decide on whether to use conventional TBNA or EBUS-TBNA
I want to see views of bronchoscopists from different countries
TopicsInterventional Pulmonology Aug 11 2015 All
Answers (11)
Eman Sobh middot Al-Azhar University Hi Semra EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult
cases Aug 12 2015 middot Herveacute Dutau middot Assistance Publique Hocircpitaux de Marseille Semra I use TBNA- for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of ordercheersAug 12 2015 middot Suveer Singh middot Imperial College London Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cellsIt is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomybwSuveerAug 13 2015 middot Johannes M Daniels middot VU University Medical Center TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNAA problem is that there are so few cases that it becomes difficult to pass on the skillsAug 13 2015 middot Vicente Roig-Figueroa middot Hospital Cliacutenico Universitario de Valladolid In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11LAug 15 2015 middot Eman Sobh middot Al-Azhar University our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are
availableAug 15 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiI am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNAEBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm) For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA Aug 16 2015 middot Michel Febvre middot Hocircpital Tenon (Hocircpitaux Universitaires Est Parisien) Hello Semra interesting questionI was a hard defender of conventionnal TBNA for LN gt 20 mm in station 7 or 4R or tumors adjacent to the airways because it is quick and easyDespite that we have the chance of having 4 EBUS scopes in our department and it is now roughly as quick to do an EBUS so we use EBUS under local and premedication in 95 of the time The two other reasons of
using EBUS is teaching and sometimes doing EUS with the EBUS scopeNevertheless I continue to think that there is a place for conventionnal TBNA in centers for which EBUS is too expensive and indications less frequent for diagnosis of large mediastinal lymph nodes or tumors
Teaching conventionnal TBNA should be pursuedSincerelyAug 19 2015 middot Maria Majori middot University Hospital of Parma In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases)I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the
confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy
Otherwise it would be like driving a Ferrari just learned to driveBest regards to All of YouAug 21 2015 middot Mace M Schuurmans middot University of Zurich For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind
TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
Aug 22 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiThank you for all these answers Its important to have appropriate indications for conventional TBNA and EBUS-TBNATo be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for
conventional methodAug 23 2015 middot Can you help by adding an answerAdd your answer
Is conventional transbronchial needle aspiration (TBNA) obsolete απαρχαιωμένη Available from httpswwwresearchgatenetpost
[accessed Apr 17 2017]
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8

bronchial ultrasound (EBUS)
Direct visualization of lymph node stations Complements EUS covers lymph node stations 2R and 4R which are difficult to access by EUS lower false-negative rate than with blind transbronchial FNA and fewer complications
More invasive than EUS few practitioners but rapidly growing in popularity
Endoscopic ultrasound(EUS)
Least invasive modality uses the esophagus to access mediastinal lymph nodes excellent for station
5 7 8 lymph nodes Useful for station 2L and 4L L adrenal celiac lymph node
Cannot reliably access right sided paratracheal lymph node stations 2 R and 4R accurate discrimination of primary hilar tumors and involved lymph nodes is important
Endobronchial ultrasound (EBUS) mini radial probe image
A) The radial probe endobronchial ultrasound image demonstrates six distinct layers of the bronchial wall Layers 1 and 2 are the mucosa submucosa and muscle Layers 3 and 4 are the cartilage Layers 5 and 6 are the adventitia Layers 1 3 and 5 appear hyperechoic because they are interfaces B) Cross section of a normal bronchus
Endobronchial ultrasound (EBUS) peripheral nodule sampling II
Associate Prof of PulmonologyCo-director 5th Pulmonary DepartmentIzmir Dr Suat Seren Training amp Research Hospital for Thoracic Medicine amp Surgery35110 Yenisehir Izmir TurkeyTEL 90-532 661 45 22 FAX 90-232-362 28 31E-MAIL sbilaceroglu [AT] gmail [DOT] com
Semra Bilaceroglu Dr Suat Seren GoumlğuumlsHastalıkları Ve Cerrahisi Eğitim Ve Ara
How do you decide on whether to use conventional TBNA or EBUS-TBNA
I want to see views of bronchoscopists from different countries
TopicsInterventional Pulmonology Aug 11 2015 All
Answers (11)
Eman Sobh middot Al-Azhar University Hi Semra EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult
cases Aug 12 2015 middot Herveacute Dutau middot Assistance Publique Hocircpitaux de Marseille Semra I use TBNA- for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of ordercheersAug 12 2015 middot Suveer Singh middot Imperial College London Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cellsIt is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomybwSuveerAug 13 2015 middot Johannes M Daniels middot VU University Medical Center TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNAA problem is that there are so few cases that it becomes difficult to pass on the skillsAug 13 2015 middot Vicente Roig-Figueroa middot Hospital Cliacutenico Universitario de Valladolid In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11LAug 15 2015 middot Eman Sobh middot Al-Azhar University our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are
availableAug 15 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiI am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNAEBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm) For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA Aug 16 2015 middot Michel Febvre middot Hocircpital Tenon (Hocircpitaux Universitaires Est Parisien) Hello Semra interesting questionI was a hard defender of conventionnal TBNA for LN gt 20 mm in station 7 or 4R or tumors adjacent to the airways because it is quick and easyDespite that we have the chance of having 4 EBUS scopes in our department and it is now roughly as quick to do an EBUS so we use EBUS under local and premedication in 95 of the time The two other reasons of
using EBUS is teaching and sometimes doing EUS with the EBUS scopeNevertheless I continue to think that there is a place for conventionnal TBNA in centers for which EBUS is too expensive and indications less frequent for diagnosis of large mediastinal lymph nodes or tumors
Teaching conventionnal TBNA should be pursuedSincerelyAug 19 2015 middot Maria Majori middot University Hospital of Parma In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases)I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the
confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy
Otherwise it would be like driving a Ferrari just learned to driveBest regards to All of YouAug 21 2015 middot Mace M Schuurmans middot University of Zurich For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind
TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
Aug 22 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiThank you for all these answers Its important to have appropriate indications for conventional TBNA and EBUS-TBNATo be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for
conventional methodAug 23 2015 middot Can you help by adding an answerAdd your answer
Is conventional transbronchial needle aspiration (TBNA) obsolete απαρχαιωμένη Available from httpswwwresearchgatenetpost
[accessed Apr 17 2017]
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
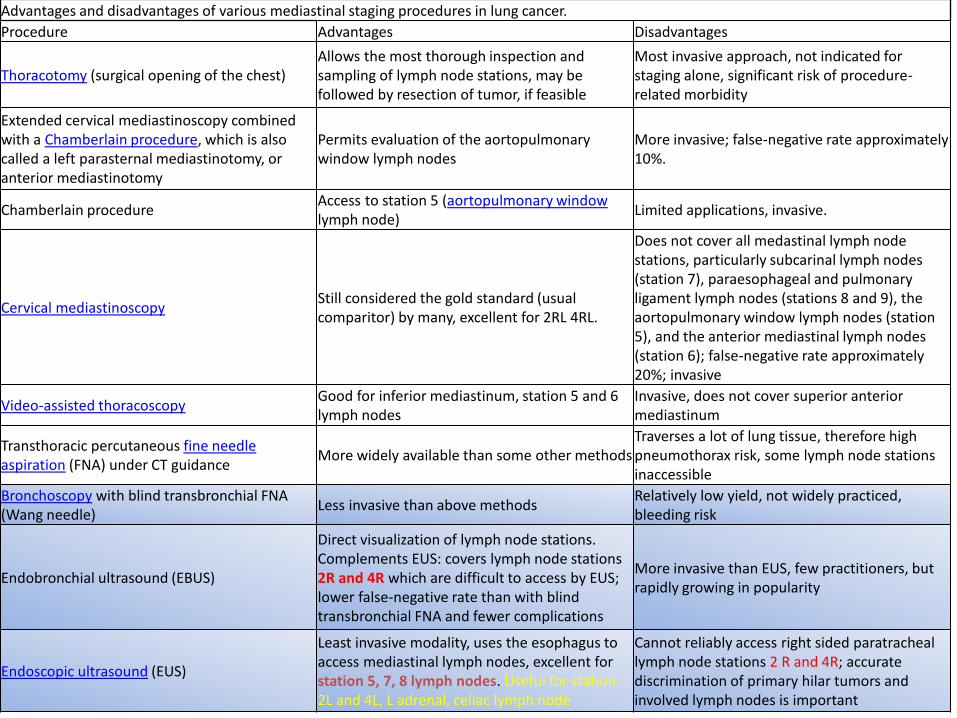
Endobronchial ultrasound (EBUS) mini radial probe image
A) The radial probe endobronchial ultrasound image demonstrates six distinct layers of the bronchial wall Layers 1 and 2 are the mucosa submucosa and muscle Layers 3 and 4 are the cartilage Layers 5 and 6 are the adventitia Layers 1 3 and 5 appear hyperechoic because they are interfaces B) Cross section of a normal bronchus
Endobronchial ultrasound (EBUS) peripheral nodule sampling II
Associate Prof of PulmonologyCo-director 5th Pulmonary DepartmentIzmir Dr Suat Seren Training amp Research Hospital for Thoracic Medicine amp Surgery35110 Yenisehir Izmir TurkeyTEL 90-532 661 45 22 FAX 90-232-362 28 31E-MAIL sbilaceroglu [AT] gmail [DOT] com
Semra Bilaceroglu Dr Suat Seren GoumlğuumlsHastalıkları Ve Cerrahisi Eğitim Ve Ara
How do you decide on whether to use conventional TBNA or EBUS-TBNA
I want to see views of bronchoscopists from different countries
TopicsInterventional Pulmonology Aug 11 2015 All
Answers (11)
Eman Sobh middot Al-Azhar University Hi Semra EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult
cases Aug 12 2015 middot Herveacute Dutau middot Assistance Publique Hocircpitaux de Marseille Semra I use TBNA- for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of ordercheersAug 12 2015 middot Suveer Singh middot Imperial College London Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cellsIt is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomybwSuveerAug 13 2015 middot Johannes M Daniels middot VU University Medical Center TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNAA problem is that there are so few cases that it becomes difficult to pass on the skillsAug 13 2015 middot Vicente Roig-Figueroa middot Hospital Cliacutenico Universitario de Valladolid In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11LAug 15 2015 middot Eman Sobh middot Al-Azhar University our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are
availableAug 15 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiI am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNAEBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm) For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA Aug 16 2015 middot Michel Febvre middot Hocircpital Tenon (Hocircpitaux Universitaires Est Parisien) Hello Semra interesting questionI was a hard defender of conventionnal TBNA for LN gt 20 mm in station 7 or 4R or tumors adjacent to the airways because it is quick and easyDespite that we have the chance of having 4 EBUS scopes in our department and it is now roughly as quick to do an EBUS so we use EBUS under local and premedication in 95 of the time The two other reasons of
using EBUS is teaching and sometimes doing EUS with the EBUS scopeNevertheless I continue to think that there is a place for conventionnal TBNA in centers for which EBUS is too expensive and indications less frequent for diagnosis of large mediastinal lymph nodes or tumors
Teaching conventionnal TBNA should be pursuedSincerelyAug 19 2015 middot Maria Majori middot University Hospital of Parma In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases)I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the
confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy
Otherwise it would be like driving a Ferrari just learned to driveBest regards to All of YouAug 21 2015 middot Mace M Schuurmans middot University of Zurich For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind
TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
Aug 22 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiThank you for all these answers Its important to have appropriate indications for conventional TBNA and EBUS-TBNATo be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for
conventional methodAug 23 2015 middot Can you help by adding an answerAdd your answer
Is conventional transbronchial needle aspiration (TBNA) obsolete απαρχαιωμένη Available from httpswwwresearchgatenetpost
[accessed Apr 17 2017]
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
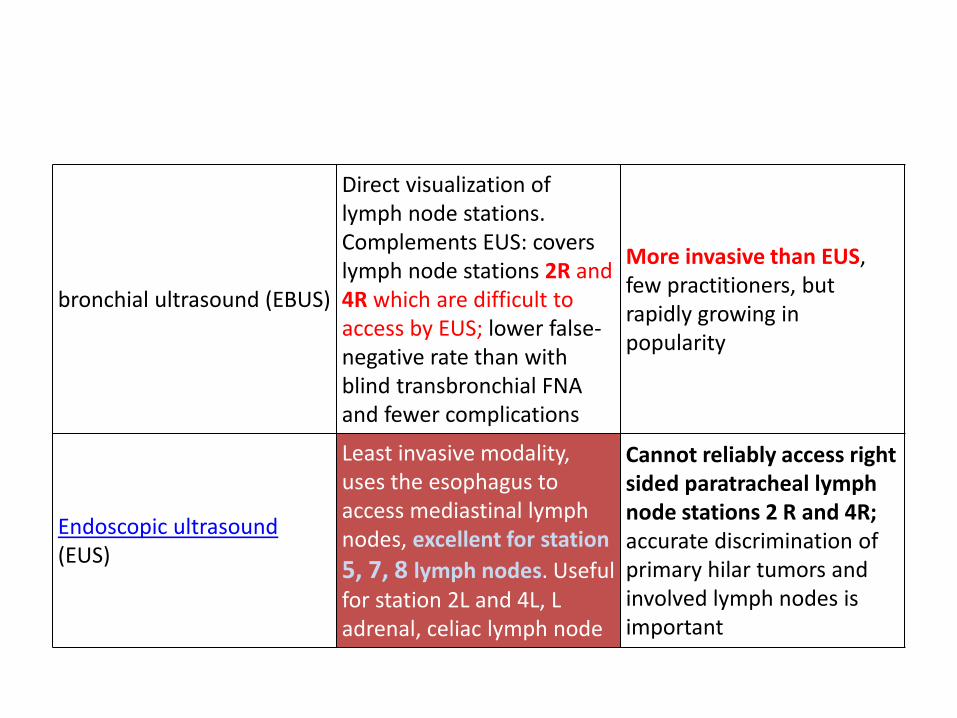
Endobronchial ultrasound (EBUS) peripheral nodule sampling II
Associate Prof of PulmonologyCo-director 5th Pulmonary DepartmentIzmir Dr Suat Seren Training amp Research Hospital for Thoracic Medicine amp Surgery35110 Yenisehir Izmir TurkeyTEL 90-532 661 45 22 FAX 90-232-362 28 31E-MAIL sbilaceroglu [AT] gmail [DOT] com
Semra Bilaceroglu Dr Suat Seren GoumlğuumlsHastalıkları Ve Cerrahisi Eğitim Ve Ara
How do you decide on whether to use conventional TBNA or EBUS-TBNA
I want to see views of bronchoscopists from different countries
TopicsInterventional Pulmonology Aug 11 2015 All
Answers (11)
Eman Sobh middot Al-Azhar University Hi Semra EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult
cases Aug 12 2015 middot Herveacute Dutau middot Assistance Publique Hocircpitaux de Marseille Semra I use TBNA- for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of ordercheersAug 12 2015 middot Suveer Singh middot Imperial College London Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cellsIt is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomybwSuveerAug 13 2015 middot Johannes M Daniels middot VU University Medical Center TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNAA problem is that there are so few cases that it becomes difficult to pass on the skillsAug 13 2015 middot Vicente Roig-Figueroa middot Hospital Cliacutenico Universitario de Valladolid In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11LAug 15 2015 middot Eman Sobh middot Al-Azhar University our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are
availableAug 15 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiI am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNAEBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm) For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA Aug 16 2015 middot Michel Febvre middot Hocircpital Tenon (Hocircpitaux Universitaires Est Parisien) Hello Semra interesting questionI was a hard defender of conventionnal TBNA for LN gt 20 mm in station 7 or 4R or tumors adjacent to the airways because it is quick and easyDespite that we have the chance of having 4 EBUS scopes in our department and it is now roughly as quick to do an EBUS so we use EBUS under local and premedication in 95 of the time The two other reasons of
using EBUS is teaching and sometimes doing EUS with the EBUS scopeNevertheless I continue to think that there is a place for conventionnal TBNA in centers for which EBUS is too expensive and indications less frequent for diagnosis of large mediastinal lymph nodes or tumors
Teaching conventionnal TBNA should be pursuedSincerelyAug 19 2015 middot Maria Majori middot University Hospital of Parma In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases)I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the
confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy
Otherwise it would be like driving a Ferrari just learned to driveBest regards to All of YouAug 21 2015 middot Mace M Schuurmans middot University of Zurich For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind
TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
Aug 22 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiThank you for all these answers Its important to have appropriate indications for conventional TBNA and EBUS-TBNATo be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for
conventional methodAug 23 2015 middot Can you help by adding an answerAdd your answer
Is conventional transbronchial needle aspiration (TBNA) obsolete απαρχαιωμένη Available from httpswwwresearchgatenetpost
[accessed Apr 17 2017]
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
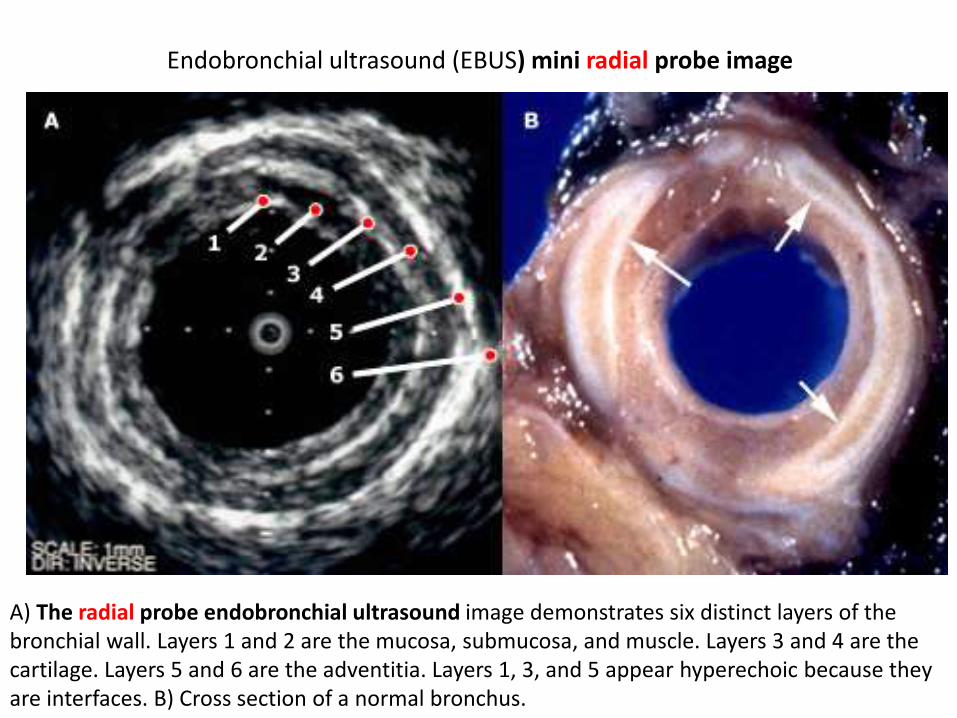
Associate Prof of PulmonologyCo-director 5th Pulmonary DepartmentIzmir Dr Suat Seren Training amp Research Hospital for Thoracic Medicine amp Surgery35110 Yenisehir Izmir TurkeyTEL 90-532 661 45 22 FAX 90-232-362 28 31E-MAIL sbilaceroglu [AT] gmail [DOT] com
Semra Bilaceroglu Dr Suat Seren GoumlğuumlsHastalıkları Ve Cerrahisi Eğitim Ve Ara
How do you decide on whether to use conventional TBNA or EBUS-TBNA
I want to see views of bronchoscopists from different countries
TopicsInterventional Pulmonology Aug 11 2015 All
Answers (11)
Eman Sobh middot Al-Azhar University Hi Semra EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult
cases Aug 12 2015 middot Herveacute Dutau middot Assistance Publique Hocircpitaux de Marseille Semra I use TBNA- for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of ordercheersAug 12 2015 middot Suveer Singh middot Imperial College London Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cellsIt is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomybwSuveerAug 13 2015 middot Johannes M Daniels middot VU University Medical Center TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNAA problem is that there are so few cases that it becomes difficult to pass on the skillsAug 13 2015 middot Vicente Roig-Figueroa middot Hospital Cliacutenico Universitario de Valladolid In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11LAug 15 2015 middot Eman Sobh middot Al-Azhar University our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are
availableAug 15 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiI am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNAEBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm) For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA Aug 16 2015 middot Michel Febvre middot Hocircpital Tenon (Hocircpitaux Universitaires Est Parisien) Hello Semra interesting questionI was a hard defender of conventionnal TBNA for LN gt 20 mm in station 7 or 4R or tumors adjacent to the airways because it is quick and easyDespite that we have the chance of having 4 EBUS scopes in our department and it is now roughly as quick to do an EBUS so we use EBUS under local and premedication in 95 of the time The two other reasons of
using EBUS is teaching and sometimes doing EUS with the EBUS scopeNevertheless I continue to think that there is a place for conventionnal TBNA in centers for which EBUS is too expensive and indications less frequent for diagnosis of large mediastinal lymph nodes or tumors
Teaching conventionnal TBNA should be pursuedSincerelyAug 19 2015 middot Maria Majori middot University Hospital of Parma In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases)I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the
confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy
Otherwise it would be like driving a Ferrari just learned to driveBest regards to All of YouAug 21 2015 middot Mace M Schuurmans middot University of Zurich For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind
TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
Aug 22 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiThank you for all these answers Its important to have appropriate indications for conventional TBNA and EBUS-TBNATo be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for
conventional methodAug 23 2015 middot Can you help by adding an answerAdd your answer
Is conventional transbronchial needle aspiration (TBNA) obsolete απαρχαιωμένη Available from httpswwwresearchgatenetpost
[accessed Apr 17 2017]
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
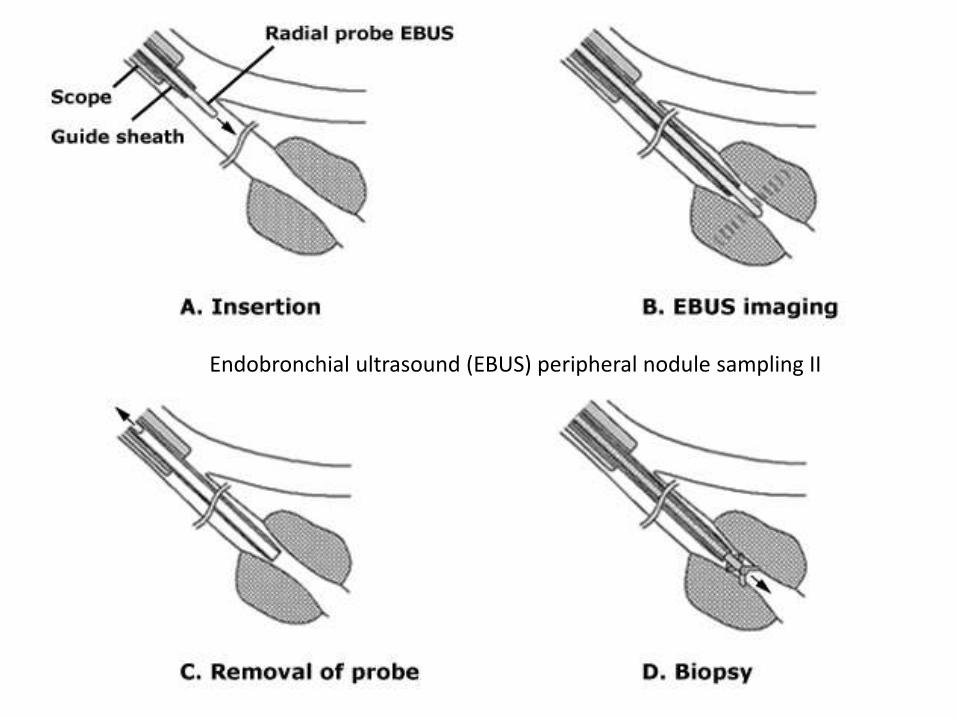
Eman Sobh middot Al-Azhar University Hi Semra EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult
cases Aug 12 2015 middot Herveacute Dutau middot Assistance Publique Hocircpitaux de Marseille Semra I use TBNA- for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of ordercheersAug 12 2015 middot Suveer Singh middot Imperial College London Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cellsIt is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomybwSuveerAug 13 2015 middot Johannes M Daniels middot VU University Medical Center TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNAA problem is that there are so few cases that it becomes difficult to pass on the skillsAug 13 2015 middot Vicente Roig-Figueroa middot Hospital Cliacutenico Universitario de Valladolid In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11LAug 15 2015 middot Eman Sobh middot Al-Azhar University our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are
availableAug 15 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiI am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNAEBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm) For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA Aug 16 2015 middot Michel Febvre middot Hocircpital Tenon (Hocircpitaux Universitaires Est Parisien) Hello Semra interesting questionI was a hard defender of conventionnal TBNA for LN gt 20 mm in station 7 or 4R or tumors adjacent to the airways because it is quick and easyDespite that we have the chance of having 4 EBUS scopes in our department and it is now roughly as quick to do an EBUS so we use EBUS under local and premedication in 95 of the time The two other reasons of
using EBUS is teaching and sometimes doing EUS with the EBUS scopeNevertheless I continue to think that there is a place for conventionnal TBNA in centers for which EBUS is too expensive and indications less frequent for diagnosis of large mediastinal lymph nodes or tumors
Teaching conventionnal TBNA should be pursuedSincerelyAug 19 2015 middot Maria Majori middot University Hospital of Parma In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases)I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the
confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy
Otherwise it would be like driving a Ferrari just learned to driveBest regards to All of YouAug 21 2015 middot Mace M Schuurmans middot University of Zurich For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind
TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
Aug 22 2015 middot Semra Bilaceroglu middot Dr Suat Seren Goumlğuumls Hastalıkları Ve Cerrahisi Eğitim Ve Araştırma HastanesiThank you for all these answers Its important to have appropriate indications for conventional TBNA and EBUS-TBNATo be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for
conventional methodAug 23 2015 middot Can you help by adding an answerAdd your answer
Is conventional transbronchial needle aspiration (TBNA) obsolete απαρχαιωμένη Available from httpswwwresearchgatenetpost
[accessed Apr 17 2017]
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
1 EBUS is preferred in cases not in reach for conventional TBNA and if lymph nodes are small or near vessels sometimes you have no choice because of high costs related to EBUS-TBNA so reserved for difficult cases
2 I use TBNA - for larges nodes (gt3 cm) mainly in stations 7 11R and 11L- when my two EBUS scopes are out of order
3 Less used now but no less important than it always was Like Herve we still use it (gt2cm) Important to have your cytologists give a clear statement regarding representative lymphoid cells
4 It is Important to have the technique of conventional TBNA as it also bundles in the skill of CT lymph node mapping and cognitively matching that to your endobronchial surface anatomy
5 TBNA is still alive although much less used For large lymph nodes or large central tumors it can still an effective tool And indeed when the EBUS scope breaks down it is nice if you can perform proper TBNA
6 In my opinion TBNA is an effective tool and the yield is high in nodes gt 25 cm in stations 4R 7 10R 11R and 11L
7 our EBUS is out of work for long time and we have to use conventional TBNA and results are satisfactory (stations 4R7 10R 11R 11L) but you still have to worry about yield every time till pathology results are available
8 I am happy to hear that conventional TBNA is considered to be not obsolete In stations 4R and 7 and in mediastinal lymph nodes gt15-2 cm the diagnostic yield is equal to that of EBUS-TBNA
9 EBUS-TBNA and EUS-FNA should be used- For smaller mediastinal lymph nodes (lt15-20 mm)For difficult amp less accessible lymph nodes (1 2 3p 4L 5 8 9) When lymph node mobility is a problem After failing conventional TBNA
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
In my opinion conventional TBNA should be the first approach in the case of lymph nodes with a diameter gt 2 cm in stations 4R 7 10R 11R and 11L (the most of the cases) I also believe that only through the knowledge of TBNA is possible to become experienced and able operator to best use EBUS when indicated Indeed the matter is not only of a technical nature to improve the confidence with the procedure are essential a good knowledge of mediastinal radiological anatomy the awareness of lymph node and carina displacement in relation to the tracheobronchial tree during respiration and the ability to integrate the radiologic information to the endoscopic anatomy Otherwise it would be like driving a Ferrari just learned to drive
For large (gt2cm) LN the experienced bronchoscopist will sample the nodes in a few minutes and if you have ROSE (rapid onsite cytological evaluation) you will likely be even quicker Conventional TBNA is not blind TBNA as many like to term it unless you admit not being able to read a CT scan or you are unsure about the correct puncture sites Learning to read a CT scan and knowing the landmarks in the bronchial tree and where to place your needle should continue to be part of the pulmonologists training Most LN locations can be safely and efficiently sampled by conventional TBNA with acceptable yield with the possible exception of high paratracheal LN where the EBUS certainly has its merits In these high paratracheal LN it is often quite difficult to estimate the correct distance from the main carina or the subglottic region and then obtain a good sample from these particular lesions The visualisation of the LN then is a great help
bull Semra Bilaceroglu middotbull Thank you for all these answers Its important to have appropriate indications for
conventional TBNA and EBUS-TBNAbull To be efficient in EBUS-TBNA one should learn conventional TBNA very well Indeed if one
is experienced in conventional TBNA learning curve for EBUS-TBNA is shorter And EBUS-TBNA increases the skills for conventional method
bull Aug 23 2015 middot
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
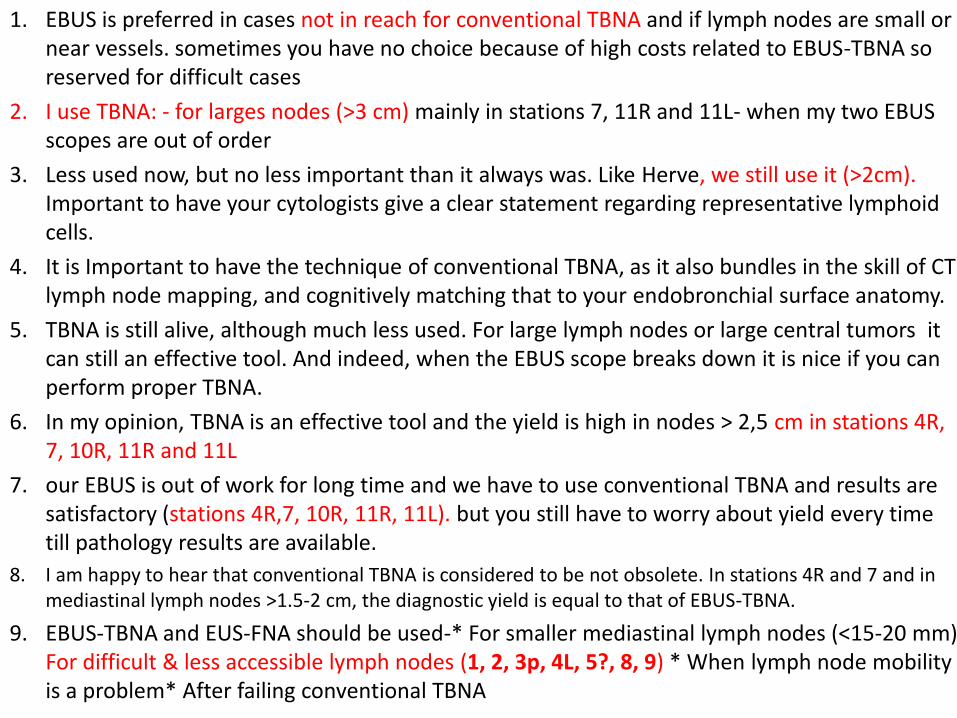
The most common indication for EBUS-TBNA would be
bull Staging the mediastinum for suspected non-small cell lung cancer (NSCLC) which is important in determining outcome and treatment
bull For diagnosis of both NSCLC and small cell lung cancer as often there is no endoluminal tumor at bronchoscopy and this avoids the need for either a CT guided lung biopsy or mediastinoscopy (which may not be appropriate especially if the patient is unlikely to be having surgical treatment)
bull For diagnosis of unexplained mediastinallymphadenopathy accessible to the major airway including benign conditions such as sarcoidosis or tuberculosis
bull As a research tool for tissue banking samples for later studies
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
Revised ESTS guideline for primary mediastinal staging (De Leyn et al European Journal of Cardiothoracic Surgery 201445787-798 with permission
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
bull (a) in tumours gt3 cm (mainly in adenocarcinoma with high FDG uptake) invasive staging should be considered
bull (b) depending on local expertise to adhere to minimal requirements for staging
bull (c) endoscopic techniques are minimally invasive and are the first choice if local expertise with EBUSEUS needle aspiration is available
bull (d) due to its higher NPV in case of PET positive or CT enlarged mediastinal LNrsquos videoassisted mediastinoscopy(VAM) with nodal dissection or biopsy remain indicated when endoscopic staging is negative Nodal dissection has an increased accuracy over biopsy
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
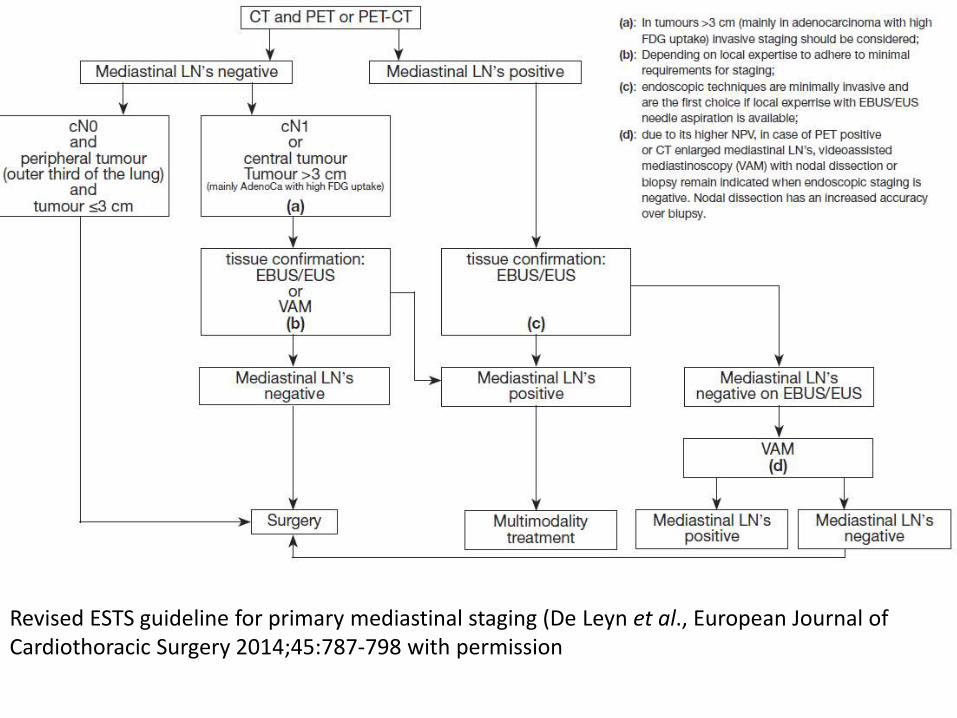
Ong P1 Grosu H Eapen GA Rodriguez M Lazarus D Ost D Jimenez CA Morice R Bandi V Tamara L Cornwell L Green L Zhu A Casal RF
Endobronchial ultrasound-guided transbronchial needle aspiration for systematic nodal staging of lung cancer in patients with N0 disease by computed tomography and integrated positron emission tomography-computed tomography Ann Am Thorac Soc 2015 Mar12(3)415-9 doi
bull CONCLUSIONS bull This is the largest report of EBUS-TBNA in patients with N0 disease by
integrated PET-CT The majority of false-negative EBUS results were in LN stations outside its reach In our study both sensitivity and NPV of EBUS-TBNA were lower than early reports despite more extensive LN sampling Given the high false-negative rate of imaging modalities EBUS-TBNA may still play an important role in patients with radiographic N0 disease particularly when nonsurgical ablative therapies are planned Prospective studies are needed to corroborate our findings in the nonsurgical population
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
bull NX Regional lymph nodes cannot be assessed bull N0 No regional lymph node metastases bull N1 Metastasis in ipsilateral peribronchial andor
ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateral mediastinal andor subcarinal lymph node(s)
bull N3 Metastasis in contralateral mediastinal contralateral hilar ipsilateral or contralateralscalene or supraclavicular lymph node(s)
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
bull NX Regional lymph nodes cannot be assessed
bull N0 No regional lymph node metastases
bull N1 Metastasis in ipsilateralperibronchial andor ipsilateralhilar lymph nodes and intrapulmonary nodes including involvement by direct extension
bull N2 Metastasis in ipsilateralmediastinal andor subcarinallymph node(s)
bull N3 Metastasis in contralateralmediastinal contralateral hilar ipsilateral or contralateral scalene or supraclavicular lymph node(s)
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
httpwwwradiologyassistantnlenp4646f1278c26fmediastinum-lymph-node-maphtml
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
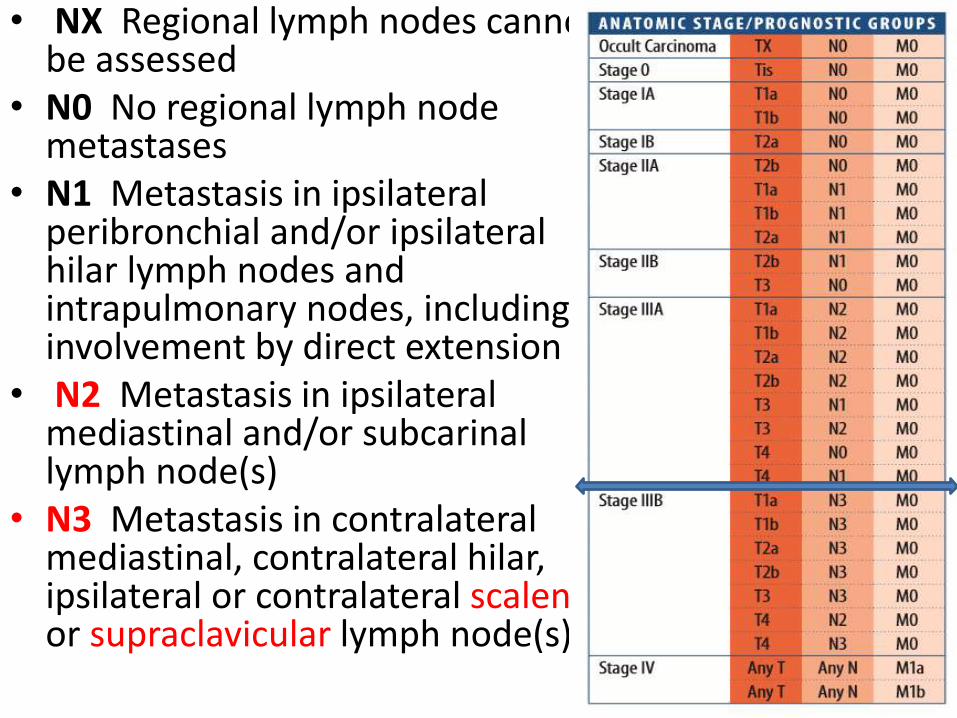
You can use conversional TBNA
bull nodes gt 25 cm
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
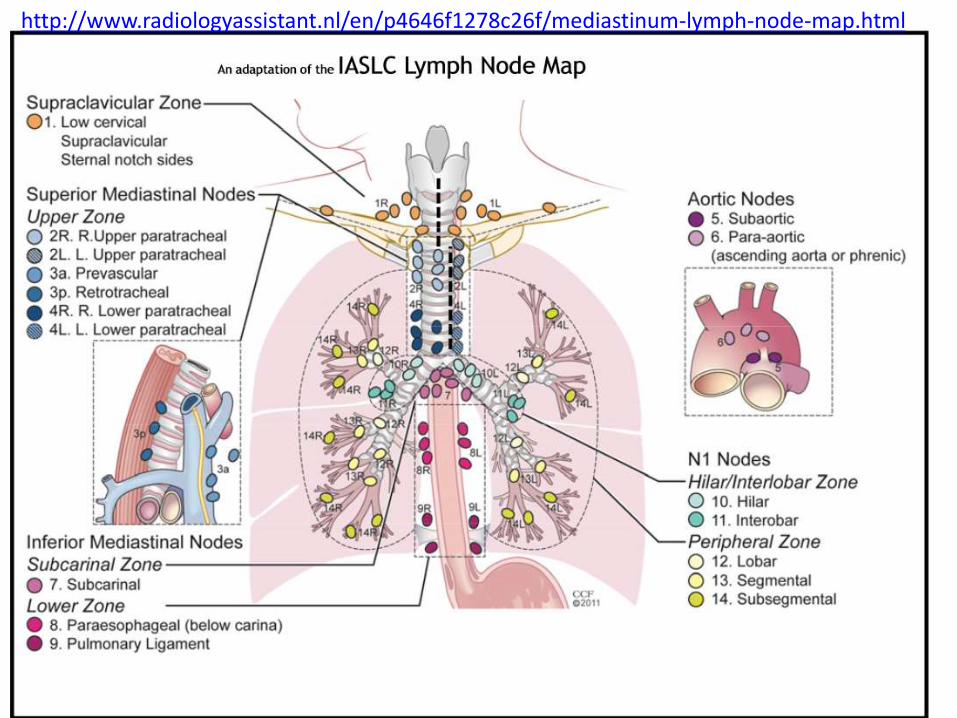
Θεση λήψης υλικού 2 και 4 δεξιά 12 cmSUV=4
Θεση λήψης υλικού 2 και 4 δεξιά Μπράχος
Κωννος
Peripheral
mass 3cm
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
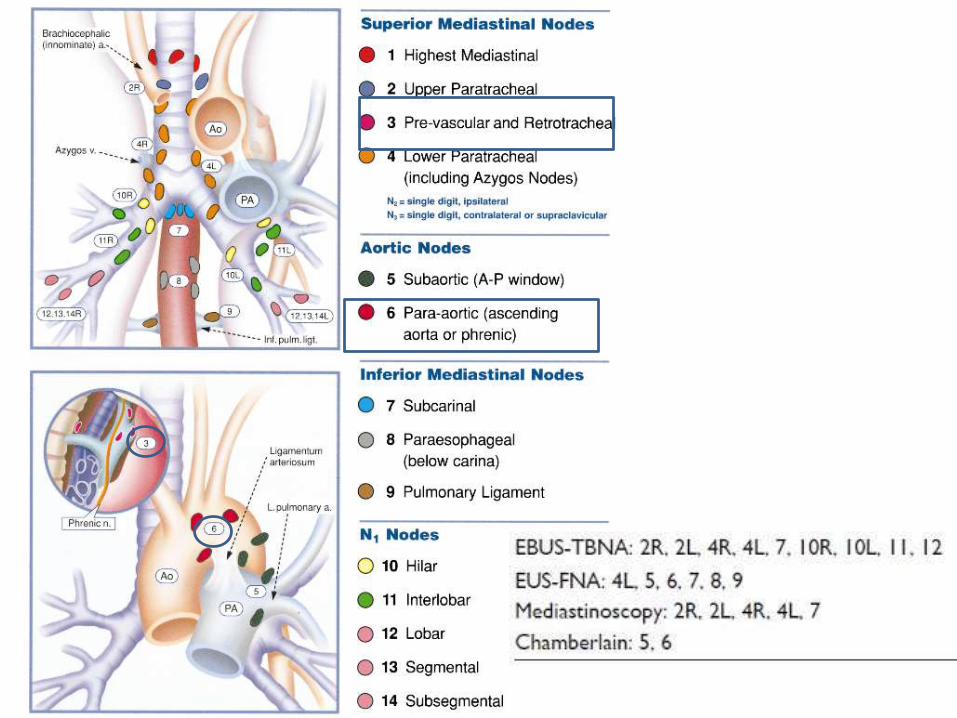
bull Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer European Society of Gastrointestinal Endoscopy (ESGE) Guideline in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS)Endoscopy 2015 47(06) c1-c1DOI 101055s-0034-1392453
This is an official guideline of the European Society of Gastrointestinal Endoscopy (ESGE) produced in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) It addresses the benefit and burden associated with combined endobronchial and esophageal mediastinal nodal staging of lung cancer The Scottish Intercollegiate Guidelines Network (SIGN) approach was adopted to define the strength of recommendations and the quality of evidenceThe article has been co-published with permission in the European Journal of Cardio-Thoracic Surgery and the European Respiratory Journal
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
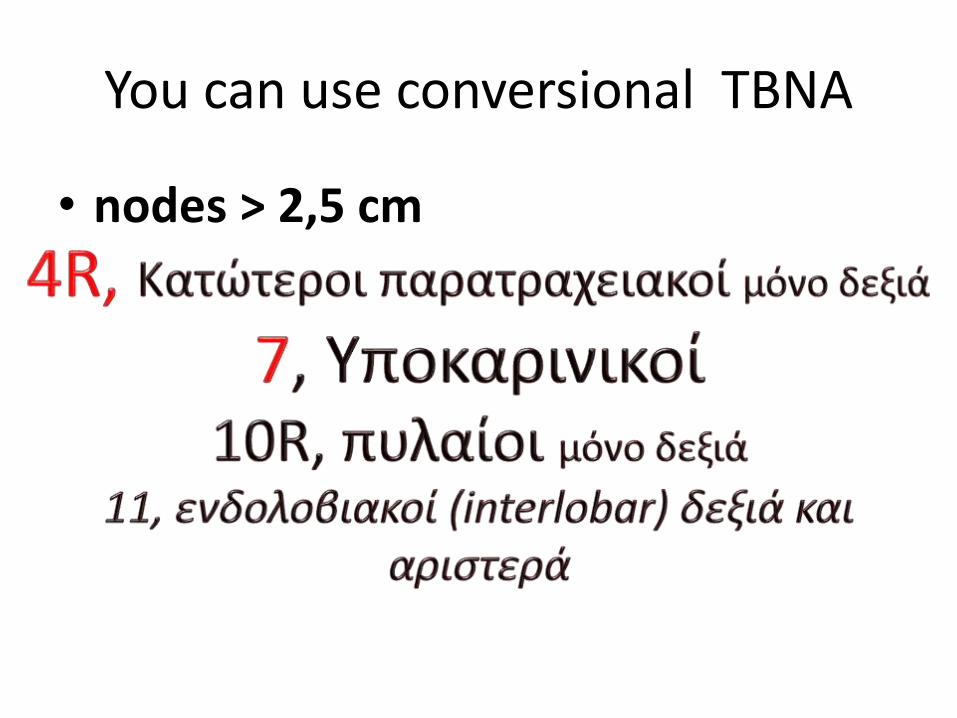
1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer (NSCLC) with abnormal mediastinal andor hilar nodes at computed tomography (CT) andor positron emission tomography (PET) endosonography is recommended over surgical staging as the initial procedure (Recommendation grade A)
2 The combination of endobronchial ultrasound with real-time guided transbronchial needle aspiration (EBUS-TBNA) and endoscopic (esophageal) ultrasound with fine needle aspiration with use of a gastrointestinal (EUS-FNA) or EBUS (EUS-B-FNA) scope is preferred over either test alone (Recommendation grade C) If the combination of EBUS and EUS-(B) is not available we suggest that EBUS alone is acceptable (Recommendation grade C)
3 Subsequent surgical staging is recommended when endosonography does not show malignant nodal involvement (Recommendation grade B)
4 For mediastinal nodal staging in patients with suspected or proven non-small-cell peripheral lung cancer without mediastinal involvement at CT or CT-PET we suggest that EBUS-TBNA andor EUS-(B)-FNA should be performed before therapy provided that one or more of the following conditions is present (i) enlarged or fluorodeoxyglucose (FDG)-PET-avid ipsilateralhilar nodes (ii) primary tumor without FDG uptake (iii) tumor size ge 3 cm (Recommendation grade C)
5 If endosonography does not show malignant nodal involvement we suggest that mediastinoscopy is considered especially in suspected N1 disease (Recommendation grade C)
6 If PET is not available and CT does not reveal enlarged hilar or mediastinal lymph nodes we suggest performance of EBUS-TBNA andor EUS-(B)-FNA andor surgical staging (Recommendation grade C)
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
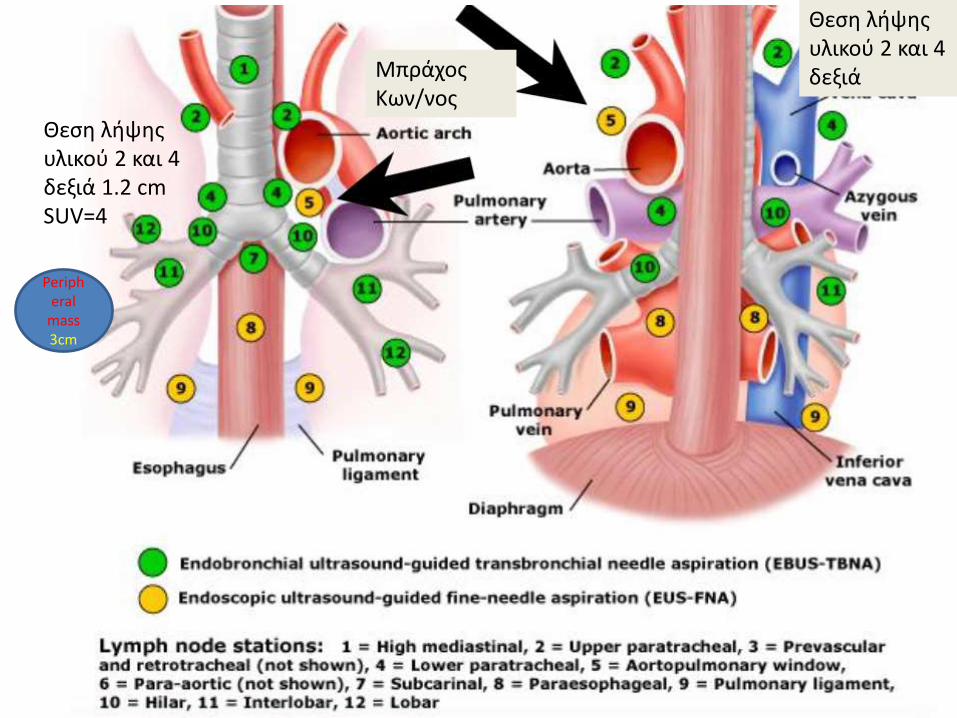
1 in patients with suspected or proven lt 3 cm peripheral NSCLC with normal mediastinal and hilar nodes at CT andor PET we suggest initiation of therapy without further mediastinal staging (Recommendation grade C)
2 For mediastinal staging in patients with centrally located suspected or proven NSCLC without mediastinal or hilar involvement at CT andor CT-PET we suggest performance of EBUS-TBNA with or without EUS-(B)-FNA in preference to surgical staging (Recommendation grade D)
3 If endosonography does not show malignant nodal involvement mediastinoscopy may be considered (Recommendation grade D)
4 For mediastinal nodal restaging following neoadjuvant therapy EBUS-TBNA andor EUS-(B)-FNA is suggested for detection of persistent nodal disease but if this is negative subsequent surgical staging is indicated (Recommendation grade C)
5 A complete assessment of mediastinal and hilar nodal stations and sampling of at least three different mediastinal nodal stations (4 R 4 L 7) is suggested in patients with NSCLC and an abnormal mediastinumby CT or CT-PET (Recommendation grade D)
6 For diagnostic purposes in patients with a centrally located lung tumor that is not visible at conventional bronchoscopy endosonography is suggested provided the tumor is located immediately adjacent to the larger airways (EBUS) or esophagus (EUS-(B)) (Recommendation grade D)
7 In patients with a left adrenal gland suspected for distant metastasis we suggest performance of endoscopic ultrasound fine needle aspiration (EUS-FNA) (Recommendation grade C) while the use of EUS-B with a transgastric approach is at present experimental (Recommendation grade D)
8 For optimal endosonographic staging of lung cancer we suggest that individual endoscopists should be trained in both EBUS and EUS-B in order to perform complete endoscopic staging in one session (Recommendation grade D)
9 We suggest that new trainees in endosonography should follow a structured training curriculum consisting of simulation-based training followed by supervised practice on patients (Recommendation grade D)
10 We suggest that competency in EBUS-TBNA and EUS-(B)-FNA for staging lung cancer be assessed using available validated assessment tools (Recommendation Grade D)
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
bull Our analysis included 354 biopsies from 145 patients Of those 145 patients 5448 were male The mean age was 6375 years The mean lymph node size was 1503 mm and 90 lymph nodes were smaller than 100 mm
bull The EBUS-TBNA method showed a sensitivity of 9117 a specificity of 1000 and a negative predictive value of 929
bull The most common histological diagnosis was adenocarcinoma
Fernaacutendez-Bussy S Labarca G Canals S Caviedes I Folch E Majid A Diagnostic yield of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal staging in lung cancer Jornal Brasileiro de Pneumologia 201541(3)219-224 doi101590S1806-37132015000004466
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
bull A total of 91 patients consisting of 35 females (385 ) and 56 males (615 ) were included in the study The mean age of the patients was 605 (plusmn114) Malignancy was not observed in 54 (593 ) patients primary malignancy metastasis was detected in 33 (363 ) patients and primary lung cancer was detected in 4 (44 ) patients with EBUS-TBNA
bull The sensitivity of EBUS-TBNA in extrathoracic malignancies was determined as 902
bull its specificity was determined as 100 bull its negative predictive value as 925 bull its positive predictive value as 100 bull its diagnostic accuracy as 956 bull The highest rate was determined in the left lower paratracheal
lymph node when they were examined in terms of malignancy detection rate in lymph node stations
Surg Endosc 2016 Oct 21 [Epub ahead of print]The role of endobronchial ultrasonography for mediastinal lymphadenopathy in cases with extrathoracic malignancyTertemiz KC1 Alpaydin AO2 Karacam V3
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
Preoperative mediastinal lymph node staging for non-small cell lung cancer 2014 update of the 2007 ESTS guidelines Transl Lung Cancer Res 2014 Aug 3(4) 225ndash233
negative likelihood ratio
False-negative samples occur at variable rates and depend on factors such as operator and cytologist experience Even in the most experienced hands false-negative rates of up to 15-20 can be seenTo minimize false-negative results both the largest and the second largest node at each station should be sampled especially in adenocarcinoma
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
Radial endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions A systematic review and meta‐analysis
RespirologyVolume 22 Issue 3 pages 443-453 8 FEB 2017 DOI 101111resp12980httponlinelibrarywileycomdoi101111resp12980fullresp12980-fig-0003
Respirology8 FEB 2017
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
EBUS-TBNA guided 125I implantation (A) EBUS-TBNA (Subcarinal lymph node) (B) 125I ultrasound form (C) 125I implantation CT scan image 125I iodine-125 EBUS-TBNA endobronchial ultrasound-guided transbronchial needle aspiration
Jun-Hong Jiang1 J Francis Turner Jr 2 and Jian-An Huang Endobronchial ultrasound elastography a new method in
endobronchial ultrasound-guided transbronchial needle aspiration
J Thorac Dis 2015 Dec 7(Suppl 4) S272ndashS278 1
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
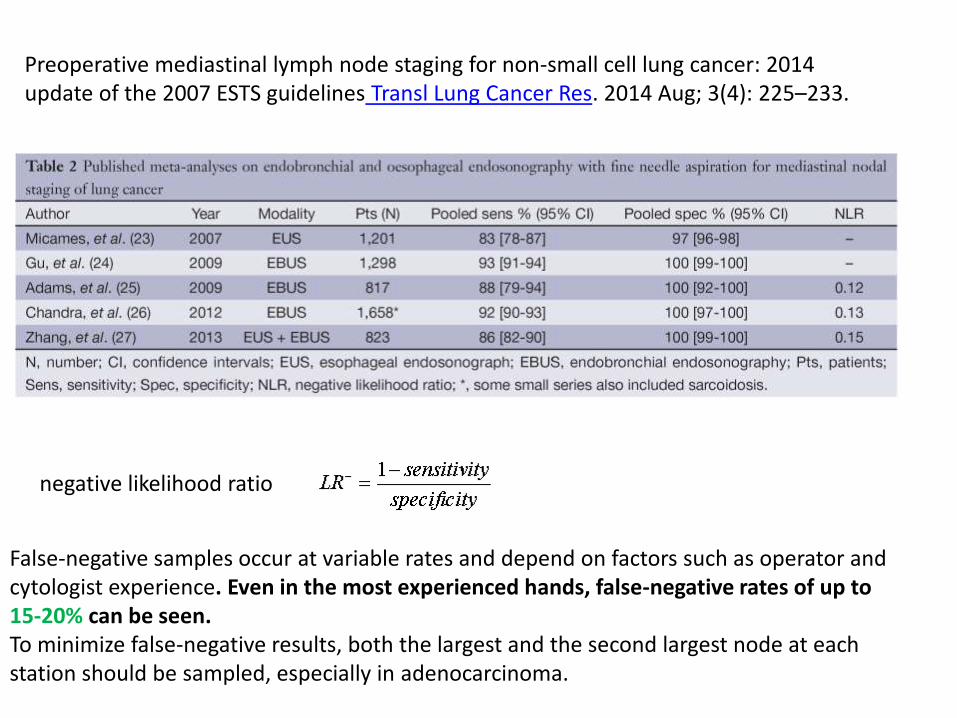
Representative lymph nodes on endobronchial ultrasound elastography (a) Representative images showing that the lymph node had a distinct
boundary low echo and homogeneous echo The elastography grading score in this figure was 1 point Histopathological specimen from endobronchial ultrasound-guided transbronchial needle aspiration demonstrated the existence of inflammation
(b) Representative images showing that the lymph node was round the boundary was clear and the internal echo was low The herein elastography grading score was 2 points The pathological result confirmed the existence of granuloma lesion
(c) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The elastography grading score in this figure was 3 points The pathological result showed the diagnosis of small cell lung cancer
(d) Representative images showing that the lymph node had a distinct boundary medium echo and uneven echo The herein elastographygrading score was 4 points The pathological result showed the diagnosis of poorly differentiated adenocarcinoma
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
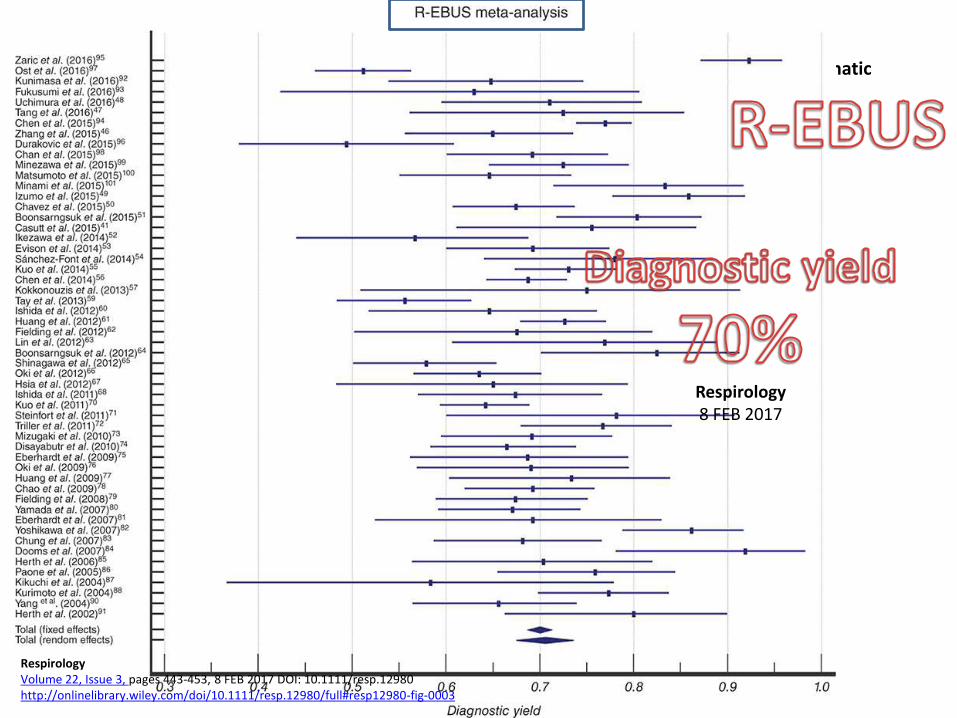
EB-530US
Viewing direction 10deg forward oblique
Observation range 3 - 100mm
Field of view 120deg
Distal end diameter 67mm
Flexible portion diameter 63mm
Bending capability
Up 130deg
Down 90deg
Forceps channel diameter 20mm
Working length 610mm
Total length 880mm
Scanning modeColor Doppler Power Doppler Pulse wave B-Mode M-Mode
Scanning method Convex
Scanning angle 65deg
Frequency 5MHz 75MHz 10MHz 12MHz
Compatible SystemsEPX-4440HD EPX-4400HD EPX-4400 SU-1 Ultrasonic Processors
With a distal end outer diameter of 67mm this scope reduces patient discomfort improves maneuverability insertion capability and physician efficiency The EBUS Systems is to be used in conjunction with the SU-1 Ultrasonic Processors
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
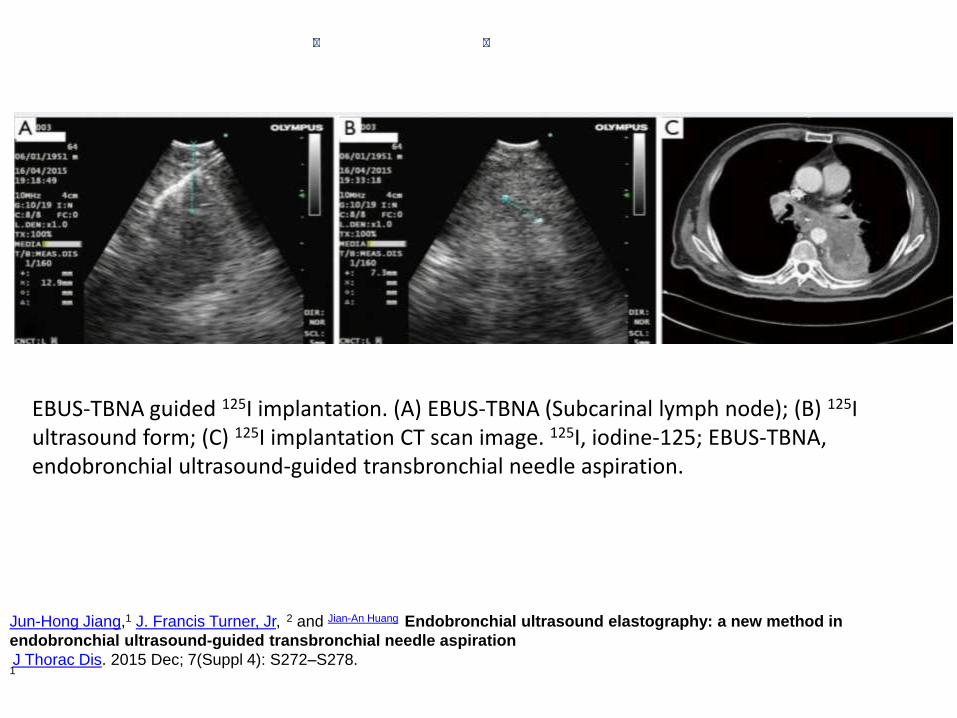
BF-UC180FUltrasound Bronchoscope
Endoscopic functions Optical system Field of view 80deg
Direction of view 35deg forward oblique
Depth of field 2 to 50 mm
Insertion tube Distal end outer diameter 69 mm
Insertion tube outer diameter
63 mm
Working length 600 mm
Instrument channel Channel inner diameter 22 mm
Bending section Angulation range Up 120deg Down 90deg
Total length 890 mm
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8
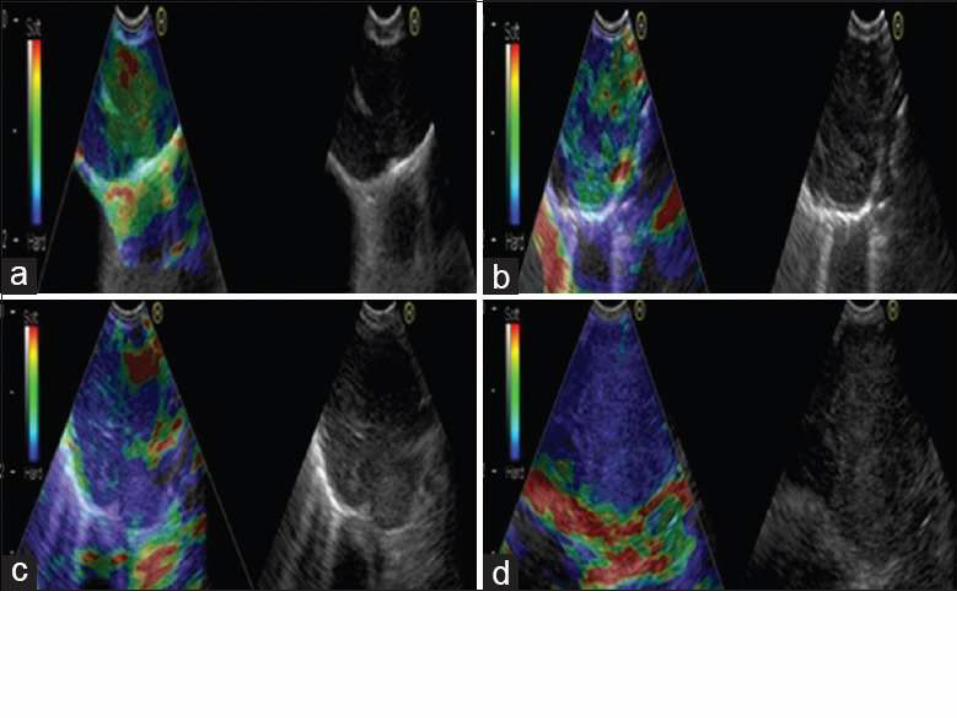
Δεν ξέρω τι να παίξω στα παιδιά στην αγορά στο Λαύριο είμαι μεγάλος με τιράντες και γυαλιά κι όλο φοβάμαι το αύριο Πώς να κρυφτείς απ τα παιδιά έτσι κι αλλιώς τα ξέρουν όλακαι μας κοιτάζουν με μάτια σαν κι αυτά όταν ξυπνούν στις δύο η ώρα
TransitioningEBUS
Transitioningconversional
TransitioningR EBUS
bull Elastographybull Viewing direction
1 Navigation bronchoscopy(with EBUS)
2 The ultra miniature radial probe
3 Confocal bronchoscopy4 Fluorescence
bronchoscopy
Im so old with braces and glasses - and Im afraid of tomorrow How can you hide from children Anyway they know everything
httpswwwyoutubecomwatchv=9U1VR_ADUA8