Macrofollicular Variant of Papillary Thyroid Carcinoma ... · sule. (Fig. 4) Lymph node metastasis...
6
Endocrine Journal 2009, 56 (3), 503-508 posed predominantly or exclusively of macrofollicles (>50% of a cross-sectional area) larger than 200μm that morphologically resembles benign nodular goiter [1, 3]. Although some studies, including case reports, describing the pathological characteristics of macro- follicular variant have been published to date [2, 4-8], its prevalence and clinical outcomes on long-term fol- low-up have not been studied in depth. We previously reported that 5 (0.3%) of 1521 papillary carcinoma were diagnosed as the macrofollicular variant [1]. In this study, we investigated their preoperative findings and biological characteristics, including their clinical outcomes, in detail. Received: November 27, 2008 Accepted: February 18, 2009 Correspondence to: Yasuhiro ITO, M.D., Ph.D., Department of Surgery, Kuma Hospital, 8-2-35, Shimoyamate-dori, Chuo-ku, Kobe 650-0011, Japan Macrofollicular Variant of Papillary Thyroid Carcinoma: Its Clinicopathological Features and Long-Term Prognosis MITSUHIRO FUKUSHIMA*, YASUHIRO ITO*, MITSUYOSHI HIROKAWA**, KAORU KOBAYASHI*, AKIHIRO MIYA*, YUUKI TAKAMURA*, HARUKI AKASU***, KAZUO SHIMIZU***, AKIRA MIYAUCHI* *Department of Surgery, Kuma Hospital, 8-2-35, Shimoyamate-dori, Chuo-ku, Kobe 650-0011, Japan **Department of Pathology, Kuma Hospital, 8-2-35, Shimoyamate-dori, Chuo-ku, Kobe 650-0011, Japan ***Department of Surgery, Nippon Medical School, 1-1-5, Sendagi, Bunkyo-ku, Tokyo 113-8603, Japan Abstract. Macrofollicular variant is a rare entity of papillary carcinoma. We previously demonstrated that this variant accounts for 0.3% of papillary carcinoma in Japan. In this study, we investigated the biological characteristics of 5 cases of macrofollicular variant. We reviewed the diagnosis and clinical course of 5 patients with macrofollicular variant. On preoperative ultrasonographic study, 2 cases were diagnosed as having benign nodule and the remaining 3 suspected of having papillary carcinoma, although they lacked typical ultrasonographic findings of papillary carcinoma. Cytological findings suggested papillary carcinoma for 3 cases and the remaining 2 were diagnosed as indeterminate. Based on both examinations, 4 of 5 patients were diagnosed as having or suspected of having papillary carcinoma. All patients underwent thyroidectomy with lymph node dissection. Three patients underwent central node dissection and the remaining 2 underwent modified radical neck dissection. None of these patients showed clinically apparent node metastasis or massive extrathyroid extension, although 3 of these patients had latent node metastasis confirmed by pathological examination. All patients survived with no evidence of carcinoma recurrence during follow-up (145-235 months). It is therefore suggested that patients with macrofollicular variant can be diagnosed as having or suspected of having papillary carcinoma if ultrasonographic and cytological examinations are appropriately performed and show an excellent prognosis possibly because this variant lacks the aggressive characteristics of papillary carcinoma. Key words: Macrofollicular variant, Papillary carcinoma, Thyroid, Diagnosis, Prognosis (Endocrine Journal 56: 503-508, 2009) PAPILLARY carcinoma, the most common malig- nant tumor originating from thyroid follicular cells, demonstrates numerous variants. On pathological examination, not only the diagnosis of papillary carci- noma but also classification of the variant is important because patient outcomes of some variants differ from conventional papillary carcinoma [1]. The macrofol- licular variant is one of these variants, which was first reported by Albores-Saavedra et al. in 1991 [2] and was adopted as a specific variant in the WHO clas- sification [3]. This variant is defined as a form com-
Transcript of Macrofollicular Variant of Papillary Thyroid Carcinoma ... · sule. (Fig. 4) Lymph node metastasis...

Endocrine Journal 2009, 56 (3), 503-508
posed predominantly or exclusively of macrofollicles (>50% of a cross-sectional area) larger than 200μm that morphologically resembles benign nodular goiter [1, 3]. Although some studies, including case reports, describing the pathological characteristics of macro-follicular variant have been published to date [2, 4-8], its prevalence and clinical outcomes on long-term fol-low-up have not been studied in depth. We previously reported that 5 (0.3%) of 1521 papillary carcinoma were diagnosed as the macrofollicular variant [1]. In this study, we investigated their preoperative findings and biological characteristics, including their clinical outcomes, in detail.
Received: November 27, 2008Accepted: February 18, 2009Correspondence to: Yasuhiro Ito, M.D., Ph.D., Department of Surgery, Kuma Hospital, 8-2-35, Shimoyamate-dori, Chuo-ku, Kobe 650-0011, Japan
Macrofollicular Variant of Papillary Thyroid Carcinoma: Its Clinicopathological Features and Long-Term Prognosis
Mitsuhiro FuKuSHIMA*, Yasuhiro Ito*, MitsuYoshi HIRoKAWA**, Kaoru KobAYASHI*, aKihiro MIYA*, YuuKi tAKAMuRA*, haruKi AKASu***, Kazuo SHIMIzu***, aKira MIYAuCHI*
*Department of Surgery, Kuma Hospital, 8-2-35, Shimoyamate-dori, Chuo-ku, Kobe 650-0011, Japan**Department of Pathology, Kuma Hospital, 8-2-35, Shimoyamate-dori, Chuo-ku, Kobe 650-0011, Japan
***Department of Surgery, Nippon Medical School, 1-1-5, Sendagi, Bunkyo-ku, Tokyo 113-8603, Japan
Abstract. Macrofollicular variant is a rare entity of papillary carcinoma. We previously demonstrated that this variant accounts for 0.3% of papillary carcinoma in Japan. In this study, we investigated the biological characteristics of 5 cases of macrofollicular variant. We reviewed the diagnosis and clinical course of 5 patients with macrofollicular variant. on preoperative ultrasonographic study, 2 cases were diagnosed as having benign nodule and the remaining 3 suspected of having papillary carcinoma, although they lacked typical ultrasonographic findings of papillary carcinoma. Cytological findings suggested papillary carcinoma for 3 cases and the remaining 2 were diagnosed as indeterminate. Based on both examinations, 4 of 5 patients were diagnosed as having or suspected of having papillary carcinoma. All patients underwent thyroidectomy with lymph node dissection. three patients underwent central node dissection and the remaining 2 underwent modified radical neck dissection. None of these patients showed clinically apparent node metastasis or massive extrathyroid extension, although 3 of these patients had latent node metastasis confirmed by pathological examination. All patients survived with no evidence of carcinoma recurrence during follow-up (145-235 months). It is therefore suggested that patients with macrofollicular variant can be diagnosed as having or suspected of having papillary carcinoma if ultrasonographic and cytological examinations are appropriately performed and show an excellent prognosis possibly because this variant lacks the aggressive characteristics of papillary carcinoma. Key words: Macrofollicular variant, Papillary carcinoma, thyroid, Diagnosis, Prognosis
(Endocrine Journal 56: 503-508, 2009)
PAPillAry carcinoma, the most common malig-nant tumor originating from thyroid follicular cells, demonstrates numerous variants. on pathological examination, not only the diagnosis of papillary carci-noma but also classification of the variant is important because patient outcomes of some variants differ from conventional papillary carcinoma [1]. the macrofol-licular variant is one of these variants, which was first reported by Albores-Saavedra et al. in 1991 [2] and was adopted as a specific variant in the WHo clas-sification [3]. This variant is defined as a form com-

504 FuKuSHIMA et al.
190.2 months. Serum thyroglobulin was also exam-ined as a marker of recurrence or persistent disease in patients who had undergone total thyroidectomy. Radioiodine ablation therapy was not performed for any patient in this series.
results
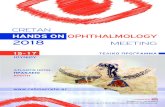
In our series, 5 cases were diagnosed as having macrofollicular variant. table 1 summarizes their backgrounds and clinicopathological features. on preoperative ultrasonographic examination, 2 patients (patients 1 and 2) were diagnosed as having benign nodule because tumors had a regular shape with well-defined and smooth border and their internal echoes were isodense and homogenous (Fig. 1-a). the re-maining three were suspected of papillary carcinoma, because they showed slightly rough border and/or a small amount of fine strong echoes [9], but were not clearly diagnosed as papillary carcinoma (Fig. 1-b). None of the patients showed clinically apparent lymph node metastasis (N1b or N1a on UICC/TNM classifi-cation [10]) on ultrasonography. On cytological find-
Patients and Methods
between 1987 and 1995, 1707 patients underwent an initial surgical treatment of papillary carcinoma. All these specimens were re-reviewed by a coauthor (M.H.) and after excluding 186 cases of poorly dif-ferentiated carcinoma, 5 (0.3%) of 1521 papillary car-cinoma were diagnosed as the macrofollicular vari-ant according to the WHO classification as described previously [1]. these 5 patients were enrolled in this study. they consisted of 4 females and 1 male and pa-tient ages ranged from 31 to 78 years. All these pa-tients underwent ultrasonography preoperatively to examine the size and location of primary tumors and determine whether they had clinically apparent node metastasis. Fine needle aspiration biopsy (FNAb) by palpation or guided by ultrasonography was performed for all patients. Patients who had been diagnosed as having or suspected of having papillary carcinoma also underwent chest Ct scan preoperatively and there were no lung metastases detected in those patients.
We normally follow patients by ultrasonography with chest roentogenography and/or Ct scan once or twice per year. the average follow-up period was
Table 1. backgrounds and clinicopathological features of 5 patients with macrofollicular variants
Patient number 1 2 3 4 5 Age(yrs)/Gender(M/F) 38/F 31/F 49/M 78/F 62/F
Suspect of papillarycarcinoma
Suspect of papillarycarcinoma
Suspect ofpapillary
carcinomaUltrasonographic findings benign benign
Maximal diameter (mm) 25 35 31 40 10#N classification N0 N0 N0 N0 N0
Cytological findings Indeterminate Papillarycarcinoma Indeterminate Papillary
carcinomaPapillary
carcinoma
thyroidectomy *Lo **tt Lo tt Lo
Lymph node dissection ^CND ^^MND CND MND CND
Extrathyroid extension None None None Minimal None
#pN classification pN1a pN1b pN0 pN1b pN0
Follow-up periods (mos) 235 145 222 192 157 *lobectomy, **total thyroidectomy, ^central node dissection^^modified radical neck dissection, # according to UICC/TNM classification (10)

505MACRoFoLLICuLAR vARIANt oF PAPILLARY CARCINoMA
Patient 1 underwent lobectomy based on preopera-tive diagnosis as follicular tumor, but the central com-partment was also dissected because swollen lymph nodes in this compartment were detected during sur-gery. Patient 3 also underwent lobectomy but the cen-tral compartment was prophylactically dissected based on preoperative ultrasonographic findings suggesting papillary carcinoma. Patients 2 and 4 underwent total thyroidectomy with modified radical neck dissection (MND) based on cytological findings of papillary car-cinoma. Patient 5 underwent only lobectomy and cen-tral node dissection because maximal tumor diameter was only 10 mm, although this patient was also cyto-logically diagnosed as having papillary carcinoma.
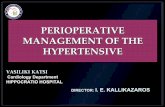
Figure 2 shows the macroscopic finding of the tu-mor. As shown in Figure 2, cut sections of the tumor appeared solid and succulent, implying abundant col-loid. Figure 3 shows the microscopic findings of the tumor. Microscopically, the tumors were composed mainly of macrofollicles. these follicles measured >200μm in diameter and were lined with flat or cuboi-dal cells. Small papillary projections were observed in some of the macrofollicles. the macrofollicles con-tained more eosinophilic colloid than that seen in adja-cent normal follicles. Peripheral scalloping of colloid was prominent (Fig. 3-a). the nuclei of almost all tu-mor cells showed ground-glass appearance and nucle-ar grooves (Fig. 3-b). the patients were diagnosed as having papillary carcinoma, macrofollicular variant
ings, 2 patients (patients 1 and 3) were diagnosed as indeterminate. the cytological specimen of patient 1 showed only a small number of cells having enlarged nuclei with mild atypia, and that of patient 3 showed nuclear grooves in some cells but lacked inclusion bodies and papillary structures. the remaining 3 pa-tients were diagnosed as having papillary carcinoma. therefore, although only one patient (patient 1) was diagnosed as having follicular tumor, the remaining 4 patients were diagnosed as having or suspected of papillary carcinoma, by preoperative imaging and cy-tological studies.
Fig. 1. Ultrasonographic profile of macrofollicular variant. (Arrows: outline of tumor, TR: trachea). 1-a Ultrasonographic appearance of the tumor presents a regular shape with well-defined and a smooth border, and the internal
echo is isodense and homogenous. (Patient No.1) 1-b ultrasonographic appearance of the tumor presents a regular shape and a slightly rough border, and the internal echo is
isodense with a few strong echoes. (Patient No.3)
Fig. 2. Macroscopic profile of macrofollicular variant. Tumor is solid and succulent, implying abundant colloid. (Patient No.4) (Arrows: outline of tumor)
a b

506 FuKuSHIMA et al.
regarding this variant showed that it is often misdiag-nosed as benign nodules [2]. Indeed, surgical speci-mens from patients that had previously been diagnosed as having adenoma or nodular goiter diagnosed 6 of 17 cases in that series. this is probably because most of their cases were treated before the era of routine ultrasonography and only 6 cases underwent FNAb. on ultrasonography, 3 of 5 cases were suspected of papillary carcinoma. In addition, on cytological ex-amination, 3 of these patients were diagnosed as hav-ing papillary carcinoma. In total, 4 (80%) of 5 cases were diagnosed as or suspected of papillary carcinoma based on the findings of imaging and cytological stud-ies. there is only one patient that failed to be preop-eratively diagnosed as papillary carcinoma (patient 1), which is because the FNAb specimen was poor for di-agnosis. It is possible that some macrofollicular vari-ant cases have been followed-up based on the misdi-agnosis as benign nodules. However, FNAb should be able to improve the ability for diagnosis of macro-follicular variant dramatically if properly performed, because the nuclei of the macrofollicular variant usu-ally show typical findings of nuclei in papillary car-cinoma. It is therefore suggested that a high percent-age of the macrofollicular variant can be diagnosed as or, at least, suspected of papillary carcinoma, if ultra-sonography and FNAb are appropriately performed and evaluated. on pathological examination, all cases in our series showed typical nuclear characteristics of papillary carcinoma, although they did not show pap-illary growth pattern. therefore, pathologists should
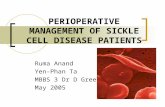
based on these findings. None of these patients showed massive extrathy-
roid extension, although the tumor of patient 4 showed capsular invasion and minimal extrathyroid exten-sion to the anterior connective tissue beyond the cap-sule. (Fig. 4) Lymph node metastasis was observed in 3 patients (patients 1, 2 and 4) on postoperative patho-logical examination. A macrofollicular variant struc-ture was seen also in the metastatic nodes in patients 1 and 2, but in those in patient 4, only the structure of conventional papillary carcinoma was observed. Although swollen lymph nodes in the central compart-ment were perioperatively detected in patient 1, this patient involved only one metastasis in the delphian node. Patient 2 had 4 metastatic nodes, 3 in the cen-tral and 1 in the lateral compartment. Patient 4 had 4 metastatic nodes only in the lateral compartment.
Serum thyroglobulin decreased to below the mea-surement sensitivity and was not elevated during fol-low-up for two patients who underwent total thyroi-dectomy. All patients survived with no evidence of carcinoma recurrence for 145 to 235 months (average 190.2 months).
Discussion
This is the first study investigating the prevalence, preoperative diagnosis and biological characteris-tics, including long-term prognosis, of macrofollicular variant at a single institute in Japan. the first study
Fig. 3. Typical H & E staining profile of macrofollicular variant. (Patient No.2) 3-a Follicles measured >200μm in diameter, and were lined with flat or cuboidal cells. (x100) 3-b the nuclei of tumor cells showed a ground-glass appearance and nuclear grooves. (x400)
a b

507MACRoFoLLICuLAR vARIANt oF PAPILLARY CARCINoMA
tients [14]. All 5 patients survived with no evidence of carcinoma recurrence on long-term follow-up (145-225 months), which is thought to be because this vari-ant lacks the prominent clinicopathological features that adversely affect prognosis. Previous studies from Western countries have also shown a good progno-sis for this variant [2, 4-8]. However, cases demon-strating palpable lymph node metastasis, recurrence to the lung and locoregional recurrence with anaplastic transformation have also been reported [2, 4, 5], indi-cating that the macrofollicular variant in Japan is pos-sibly more indolent than that in Western countries.
Although 80% of cases in our series could be diag-nosed as having or suspected of having papillary car-cinoma, some patients with macrofollicular variant may undergo limited thyroidectomy without lymph node dissection after being preoperatively misdiag-nosed as benign nodule or follicular tumor. We previ-ously demonstrated that papillary carcinomas that had been resected as benign nodules showed an excellent prognosis even if they did not undergo immediate ad-ditional surgery such as completion total thyroidecto-my and lymph node dissection, indicating that papil-lary carcinoma misdiagnosed as benign nodule even on imaging and cytological studies has a mild charac-ter [15]. therefore, no additional surgery may be nec-essary if this variant is resected under the preoperative misdiagnosis as benign nodule. At present, it is diffi-cult to diagnose macrofollicular variant on preopera-tive examinations, but if it becomes possible in the fu-ture, limited thyroidectomy and lymph node dissection could be considered because this variant shows a mild character.
In summary, patients with macrofollicular vari-ant can be diagnosed as having or suspected of hav-ing papillary carcinoma in high incidence if ultrasono-graphic and cytological examinations are appropriately performed. this variant, at least in Japan, has a very mild character and long-term survival without recur-rence can be expected.
take notice of the presence of the nuclear pattern of the papillary carcinoma when they examine thyroid nod-ules lacking papillary growth pattern in order to avoid misdiagnosis. our institution encountered 5 cases that were diagnosed as benign goiter but showed metastasis to the lymph nodes and/or distant organs after initial surgery [11]. those cases were diagnosed as benign goiter on pathological examination because, unlike the macrofollicular variant, they did not show any typical findings of nuclei in papillary carcinoma. Therefore, we can conclude that macrofollicular variant is an en-tirely different entity from those cases.
there are several prognostic factors related to pap-illary carcinoma. We demonstrated that, among these, massive extrathyroid extension (pt4 [10]) and clini-cally apparent lateral node metastasis (N1b [10]) inde-pendently affect both disease-free survival and cause-specific survival of patients [12-14]. the 5 cases in our series did not show either of these features. three cases showed lymph node metastasis detected on path-ological examination, but we have also shown that latent metastasis found only on pathological exami-nation does not affect cause-specific survival of pa-
Fig. 4. Capsular invasion is shown in Patient No.4. (Arrows: capsular invasion, C: capsule) (H&E staining x40)
references
1. Ito Y, Hirokawa M, uruno t, Kihara M, Higashiyama t, takamura Y, Miya A, Kobayashi K, Matsuzuka F, Miyauchi A. (2008) Prevalence and biological behav-ior of variants of papillary thyroid carcinoma; experi-
ence at a single hospital. Pathology in press. 2. Albores-Saavedra J, Gould E, vardaman C, vuitch F.
(1991) the macrofollicular of papillary thyroid carci-noma: A study of 17 cases. Hum Pathol 22: 1195-1205.

508 FuKuSHIMA et al.
10. Sobin LH, Wittekind CH., eds. (2002) UICC/TNM classification of malignant tumors. 6th ed. New York: Wiley-Liss.
11. Ito Y, Yabuta t, Hirokawa M, Fukushima M, Inoue H, uruno t, Kihara M, Higashiyama t, takamura Y, Miya A, Kobayashi K, Matsuzuka F, Amino N, Miyauchi A. (2008) Distant and lymph node metastases of thyroid nodules with no pathological evidence of malignance; a limitation of pathological examination. Endocrine J 55: 889-894.
12. Ito Y, tomoda C, uruno t, takamura Y, Miya A, Kobayashi K, Matsuzuka F, Kuma K, Miyauchi A. (2005) ultrasonographically and anatomopathologi-cally detectable node metastases in the lateral compart-ment as indicators of worse relapse-free survival in pa-tients with papillary thyroid carcinoma. World J Surg 29: 917-920.
13. Ito Y, tomoda C, uruno t, takamura Y, Miya A, Kobayashi K, Matsuzuka F, Kuma K, Miyauchi A. (2006) Prognostic significance of extrathyroid exten-sion of papillary thyroid carcinoma: massive but not minimal extension affects the relapse-free survival. World J Surg 30: 780-788.
14. Ito Y, Miyauchi A, Jikuzono t, Higashiyama t, takamura t, Miya A, Kobayashi K, Matsuzuka F, Ichihara K, Kuma K. (2007) Risk factors contribut-ing to a poor prognosis of papillary thyroid carcinoma: validity of UICC/AJCC TNM classification and stage grouping. World J Surg 31: 838-848.
15. Ito Y, Higashiyama t, takamura Y, Miya A, Kobayashi K, Matsuzuka F, Kuma K, Miyauchi A. (2007) Long-term follow-up for patients with papillary thyroid car-cinoma treated as benign nodules. Anticancer Res 27: 2243-2246.
3. Livolsi vA, Mazzaferri EL, Albores-Saavedra J. (2004) Papillary carcinoma. In DeLeillils RA, Lloyd Rv, Heitz Pu, eds. Pathology and genetics of tumors of endo-crine organs. Lyon, IARC Press, 57-66.
4. Lugli A, terracciano LM, oberholzer M, bubendorf L, tormillo L. (2004) Macrofollicular variant of papillary carcinoma of the thyroid. Arch Pathol Lab Med 128: 54-58.
5. Albores-Saavedra J, Houosini I, vuitch F, Snyder WH 3rd. (1997) Macrofollicular variant of papillary thyroid carcinoma with minor insular component. Cancer 80: 1110-1116.
6. Hirokawa M, Shimizu M, terayama K, Kanahara t, Sonoo H, Manabe t. (1998) Macrofollicular variant of papillary thyroid carcinoma; Report of a case with fine needle aspiration biopsy findings. Acta Cytol 42: 1441-1443.
7. Fadda G, Fiorino MC, Mule A, Livolsi vA. (2002) Macrofollicular encapsulated variant of papillary thy-roid carcinoma as a potential pitfall in histologic and cytologic diagnosis. Acta Cytol 46: 555-559.
8. Mesonero CE, Jugle JE, Wilbur DC, Nayar R. (1998) Fine-needle aspiration of the macrofollicular and mi-crofollicular subtypes of the follicular variant of papil-lary carcinoma of the thyroid. Cancer Cytopathol 44: 235-244.
9. Shimura H, Haraguchi K, Hiejima Y, Fukunari N, Fujimoto Y, Katagiri M, Koyanagi N, Kurita t, Miyakawa M, Miyamoto Y, Suzuki N, Suzuki S, Kanbe M, Kato Y, Murakami t, tohno E, tsunoda-Shimizu H, Yamada K, ueno E, Kobayashi K, Kobayashi t, Yokozawa t, Kitaoka M. 2005 Distinct diagnostic cri-teria for ultrasonographic examination of papillary thy-roid carcinoma: a multicenter study. Thyroid 15: 251-258.