The Shoulder Medial Rotation Test: An Intertester and Intratester Reliability Study in Overhead...
8
THE SHOULDER MEDIAL ROTATION TEST:AN INTERTESTER AND INTRATESTER RELIABILITY STUDY IN OVERHEAD ATHLETES WITH CHRONIC SHOULDER PAIN Enrique Lluch, PT, a,b Josep Benítez, PT, PhD, a,b Lirios Dueñas, PT, PhD, a José Casaña, PT, a Yasser Alakhdar, PT, PhD, a Jo Nijs, PT, PhD, b,c and Filip Struyf, PT, PhD b,d ABSTRACT Objective: The purpose of this study was to examine intertester and intratester reliability of the shoulder medial rotation test (MRT) and reliability differences depending on examiner expertise. Methods: Seventeen athletes with chronic shoulder pain participated in the study. Four independent observers with different experience levels simultaneously rated MRT performance as “correct” or “incorrect,” after a standardized assessment protocol, the same day (for intertester reliability) and in a 7-day interval (for intratester reliability). Results: The intrarater reliability was admissible for 2 experts and one novice, with κ values ranging between 0.32 to 0.76 and poor for one novice (κ b 0). Interrater agreement for all 4 assessors demonstrated slight agreement (κ = 0.06; 95% confidence interval: 0.06-0.47), increasing to fair agreement (κ = 0.33; 95% confidence interval: 0.21-0.69) when comparing the MRT findings between the 2 experienced assessors. Practice with the MRT in novices only marginally improved their level of agreement. Conclusions: Reliability of the MRT for detecting movement control of the shoulder girdle was fair at best for experienced examiners and poor overall. Dexterity and repetitive performance of the test is necessary for correct interpretation of the MRT. (J Manipulative Physiol Ther 2014;37:198-205) Key Indexing Terms: Shoulder Joint; Physical Examination; Reproducibility of Results S houlder disorders are the third most common musculoskeletal condition presenting in general practice after neck and low-back pain, with an estimated lifetime prevalence of 42% in people performing highly repetitive overhead motions. 1 Shoulder symptoms are often persistent and recurrent, with 40% to 50% of patients reporting persistent symptoms after 6 to 12 months 2 and 14% of patients continuing care after 2 years. 3 Altered dynamic control of the shoulder complex (ie, scapular dyskinesis) appears to be a significant factor contributing to shoulder dysfunction. 4-7 Consequently, evaluation of such control and treatment directed to its improvement forms currently an integral part of diagnosis and management of all shoulder disorders. Classification of movement control faults have been proposed to guide diagnosis and treatment of patients with shoulder pain. 8-10 For example, Caldwell et al 10 illustrated how an impaired movement system aids diagnosis in a patient with shoulder pain guiding the clinician in prescribing treatment. Several movement pattern alterations have been detected at both the glenohumeral and scapulothoracic joints in people with shoulder pathology. 4,6,7,11,12 Specifically, lesser upward rotation, lesser posterior tilting, and greater internal rotation of the scapula have been consistently shown in subjects with shoulder pain of different etiologies. 6 Studies demonstrating differences in movement patterns for symptomatic shoulders usually applied expensive and specialized equipment (ie, full 3-dimensional motion tracking a Professor, Department of Physical Therapy, University of Valencia, Valencia, Spain. b Researcher, Pain in Motion Research Group, Departments of Human Physiology and Physiotherapy, Faculty of Physical Education & Rehabilitation, Vrije Universiteit, Brussel, Belgium. c Professor, Department of Physical Medicine and Physiother- apy, University Hospital Brussels, Brussels, Belgium. d Professor, Division of Musculoskeletal Physiotherapy, Depart- ment of Health Sciences, Artesis University College Antwerp, Antwerp, Belgium. Submit requests for reprints to: Enrique Lluch, PT, Department of Physical Therapy, University of Valencia, Gascó Oliag 5, 46010 Valencia, Spain. (e-mail: [email protected]). Paper submitted October 3, 2013; in revised form December 26, 2013; accepted December 26, 2013. 0161-4754/$36.00 Copyright © 2014 by National University of Health Sciences. http://dx.doi.org/10.1016/j.jmpt.2013.12.012 198
Transcript of The Shoulder Medial Rotation Test: An Intertester and Intratester Reliability Study in Overhead...

THE SHOULDER MEDIAL ROTATION TEST: AN INTERTESTER
AND INTRATESTER RELIABILITY STUDY IN OVERHEAD
ATHLETES WITH CHRONIC SHOULDER PAIN
Enrique Lluch, PT, a, b Josep Benítez, PT, PhD,a, b Lirios Dueñas, PT, PhD,a José Casaña, PT, a
Yasser Alakhdar, PT, PhD,a Jo Nijs, PT, PhD,b, c and Filip Struyf, PT, PhDb, d
a Professor, DValencia, Valenc
b Researcher, PHuman PhysioloEducation & Reh
c Professor, Deapy, University H
d Professor, Diment of HealthAntwerp, Belgium
Submit requesof Physical The46010 Valencia,
Paper submitt26, 2013; accepte
0161-4754/$3Copyright ©http://dx.doi.o
198
ABSTRACT
Objective: The purpose of this study was to examine intertester and intratester reliability of the shoulder medialrotation test (MRT) and reliability differences depending on examiner expertise.Methods: Seventeen athletes with chronic shoulder pain participated in the study. Four independent observers withdifferent experience levels simultaneously rated MRT performance as “correct” or “incorrect,” after a standardizedassessment protocol, the same day (for intertester reliability) and in a 7-day interval (for intratester reliability).Results: The intrarater reliability was admissible for 2 experts and one novice, with κ values ranging between 0.32 to0.76 and poor for one novice (κ b0). Interrater agreement for all 4 assessors demonstrated slight agreement (κ = 0.06;95% confidence interval: 0.06-0.47), increasing to fair agreement (κ = 0.33; 95% confidence interval: 0.21-0.69) whencomparing the MRT findings between the 2 experienced assessors. Practice with the MRT in novices only marginallyimproved their level of agreement.Conclusions: Reliability of the MRT for detecting movement control of the shoulder girdle was fair at best forexperienced examiners and poor overall. Dexterity and repetitive performance of the test is necessary for correctinterpretation of the MRT. (J Manipulative Physiol Ther 2014;37:198-205)
Key Indexing Terms: Shoulder Joint; Physical Examination; Reproducibility of ResultsShoulder disorders are the third most commonmusculoskeletal condition presenting in generalpractice after neck and low-back pain, with an
estimated lifetime prevalence of 42% in people performinghighly repetitive overhead motions.1 Shoulder symptoms
epartment of Physical Therapy, University ofia, Spain.ain in Motion Research Group, Departments ofgy and Physiotherapy, Faculty of Physicalabilitation, Vrije Universiteit, Brussel, Belgium.partment of Physical Medicine and Physiother-ospital Brussels, Brussels, Belgium.vision of Musculoskeletal Physiotherapy, Depart-Sciences, Artesis University College Antwerp,.ts for reprints to: Enrique Lluch, PT, Departmentrapy, University of Valencia, Gascó Oliag 5,Spain. (e-mail: [email protected]).ed October 3, 2013; in revised form Decemberd December 26, 2013.6.002014 by National University of Health Sciences.rg/10.1016/j.jmpt.2013.12.012
are often persistent and recurrent, with 40% to 50% ofpatients reporting persistent symptoms after 6 to 12 months2
and 14% of patients continuing care after 2 years.3
Altered dynamic control of the shoulder complex (ie,scapular dyskinesis) appears to be a significant factorcontributing to shoulder dysfunction.4-7 Consequently,evaluation of such control and treatment directed to itsimprovement forms currently an integral part of diagnosisand management of all shoulder disorders. Classification ofmovement control faults have been proposed to guidediagnosis and treatment of patients with shoulder pain.8-10
For example, Caldwell et al10 illustrated how an impairedmovement system aids diagnosis in a patient with shoulderpain guiding the clinician in prescribing treatment.
Several movement pattern alterations have been detectedat both the glenohumeral and scapulothoracic joints inpeople with shoulder pathology.4,6,7,11,12 Specifically,lesser upward rotation, lesser posterior tilting, and greaterinternal rotation of the scapula have been consistentlyshown in subjects with shoulder pain of different etiologies.6
Studies demonstrating differences in movement patterns forsymptomatic shoulders usually applied expensive andspecialized equipment (ie, full 3-dimensional motion tracking

199Lluch et alJournal of Manipulative and Physiological TherapeuticsShoulder Medial Rotation TestVolume 37, Number 3
systems)13-15, making its application difficult in a clinicalsetting.12 Therefore, feasible and reliable test maneuvers thathave strong clinical utility to detect shoulder movementabnormalities are required.16 Without them, clinicians cannotidentify whether patients need interventions that are focusedon retraining motor control at the shoulder region.
Movement control tests specifically designed toidentify movement faults at the shoulder complex havebeen proposed, such as the dynamic rotary stability testor the dynamic relocation test17,18, but their reliability orvalidity remains to be established. Adequate levels ofreliability have been reported for other tests such as thescapular dyskinesis test.19 However, a recent systematicreview questioned the validity of methods used toidentify alterations in position and motion of thescapula, mostly due to their lack of correlation withsymptoms.20 One test suggested to evaluate optimalmovement control and function of the shoulder girdle isthe shoulder medial rotation test (MRT). The MRT is adissociation or motor control test firstly described byMorrisey et al21, which assesses the patients’ ability toactively dissociate and control scapular movement andglenohumeral translation during active glenohumeralinternal/medial rotation.8 The ideal pattern for theMRT has been described as a completion of 60º ofmedial rotation of the humerus, starting with theshoulder in 90º of abduction and in the plane of thescapula (30º anterior to the coronal plane), without anysignificant scapulothoracic movement (N6 mm) orglenohumeral anterior translation (N4 mm)21. Uncon-trolled or excessive movement at the scapula orglenohumeral joint is considered a positive test. Themost common movement faults identified during the testare uncontrolled forward tilt, downward rotation, orelevation of the scapula and excessive anterior transla-tion of the humeral head. Uncontrolled scapularmovement during active shoulder internal rotation isidentified through excessive movement of the therapistmiddle finger placed on the coracoid process toward theceiling (forward tilt), patient feet (downward rotation),or patient head (elevation), with the patient in supine.Excessive anterior humeral head translation is ascer-tained when the therapist index finger located at thehumeral head moves excessively toward the ceilingduring shoulder internal rotation. Moreover, presence ofexcessive movement at the scapula has been linked withrisk of impingement, whereas uncontrolled anteriortranslation of the humeral head has been related withglenohumeral instability risk.21 However, the validity ofthese assertions is unknown, as no study has evaluatedpossible correlations between positive results on theMRT and the prevalence or future incidence of thosepathologies. In addition, as the scapula is stabilized bythe weight of the body during the MRT, its assumedability of dissociating scapular movement and gleno-
humeral translation during active shoulder medialrotation may be questioned.
Although accuracy of examiner palpation during theMRT was explored by Morrissey et al21 with 3-dimensionalultrasound and motion analysis measures, agreementbetween different examiners when interpreting the test hasnot been previously examined. Nonetheless, some studieshave used the MRT as part of their clinical assessmentprotocol of the shoulder girdle.22,23
The aim of this study was therefore to examine theintertester and intratester reliability of MRT in a populationof overhead athletes with chronic shoulder pain. In addition,the possible influence of the therapists’ clinical experienceon the reliability of the MRT was also explored.
METHODS
SubjectsSeventeen athletes (11 men, 6 women), ages of 18 to 60
years (mean ± standard deviation [SD], 30 ± 7.27 years),height of 175.29 ± 6.78 cm, weight of 70.64 ± 9.23 kg, and 5months of average shoulder pain duration, were included inthis study. Table 1 shows the descriptive characteristics of theathletes. Recruitment was performed via notices distributed inthe sports medicine sections of the Valencia Technical Collegeand the University of Valencia. Besides presenting with ahistory of chronic shoulder pain (ie, shoulder pain lasting ≥3months), athletes were required to play overhead sport (ie,volleyball, handball, and tennis) regularly (at least once perweek), in an organized way and have at least 60º of passiveshoulder medial rotation, measured in supine position with thescapula in the coronal plane and 90º of shoulder abduction.
Subjects were excluded if they had a history of surgeryto the shoulder complex, upper thorax, upper back, orhumerus in the past year or cervical radiculopathy.24
Subjects were told to avoid any medication intake duringthe week before the study commencement.
All participants received an information leaflet and gavewritten informed consent before the study beginning. Thestudy was approved by the Ethics and Research Committeeof the University of Valencia (Spain), and the procedureswere conducted according to the Declaration of Helsinki.
Study DesignAn interobserver and intraobserver reliability study of
the MRT was conducted. Four assessors with differentexperience levels rated the MRT performance the same day(for intertester reliability) and at interval of 7 days (forintratester reliability). The 7-day interval was chosen as weconsidered that movement faults at the shoulder girdle, ifpresent, should be revealed at 2 different points in time (day1 and day 7). Subjects were told to continue with normalactivity during the 7-day interval between the 2 measure-ment points. Two raters were clinical specialists in the field

Table 2. Operational Definitions for the MRT
List A (score = 1) List B (score = 1 for each item)
- The patient showed anteriortranslation of the scapula(displacement of examinermiddle finger placed at thecoracoid process towardthe ceiling), before 60°of active medial rotation.
- Alteration on respiratory pattern(ie, patient held his breath duringthe test).- Patient difficulty to performthe test.- Patient could not perform60° active shoulderinternal rotation.- Anterior humeral head translationbefore 60° of shoulder internalrotation, through examiner indexfinger located at the anteriorhumeral head.- Fatigue: the first repetition ofthe test was negative but withsuccessive repetitions, the patientstarted trembling duringperformance of the test.- Patient needed external feedbackduring the test (verbal feedbackfrom the assessor, ie, “holdyour scapular fixed to the table”).- Patient needed external supportduring the test (ie, the assessorsupported the arm).
The MRT was considered positive if (1) scored 1 in List A, (2) scored morethan 3 in List B, or (3) both criteria (1) and (2) were accomplished.
Table 1. Descriptive Characteristics of the Athletes (N = 17)
Variable Value
Age (y)Mean 30SD 7.27
SexMale 11Female 6
Weight (kg)Mean 70.64SD 9.23
Height (cm)Mean 175.29SD 6.78
Duration of contiguous overhead activities (y)Mean 9.23SD 7.46
Duration of shoulder pain (mo)Mean 6.29SD 7.06
200 Journal of Manipulative and Physiological TherapeuticsLluch et alMarch/April 2014Shoulder Medial Rotation Test
with 15 years of working experience. Each had apostgraduate degree in manual therapy and was experiencedwith the use of MRT. The other 2 raters were novice, withonly 1 year of working experience, and neither of them hada postgraduate degree nor had used before the MRT.Assessors were blinded to each other’s test results, andpatients did not receive any information about the testresults to avoid bias. Medial rotation test was evaluatedonly on the painful shoulder. In case bilateral shoulder painwas present, both shoulders were assessed.
ProcedurePatients were initially examined by an independent
researcher who assessed their compliance with the inclusionand exclusion criteria. The researcher was blinded to theresults obtained by the examiners for the MRT. In addition,relevant demographic information of each patient (age, sex,height, weight, dominant arm, type of sport activity,duration of pain, and mode of pain onset), pain intensityrated in the last 24 hours on a visual analogue scale (VAS), 25
and ROM of passive shoulder internal rotation in the painfulshoulder (in supine, with the scapula in the coronal plane and90º of shoulder abduction), were collected. The VAS isrepresented by a 100 mm horizontal line, where “0”corresponds to “no pain” and “100” is “pain as bad aspossible”. It is a valid and reliable tool to record the amount ofpain experienced.26
Subjects who met the study requirements carried out theMRT in a separate room, where they were ratedindependently by each assessor. The clinical assessmentwas performed in a random order using a computer-generated sequence of numbers. The MRT was rated aseither negative or positive by the assessors, according tooperational definitions previously established for the testand detailed elsewhere8,23 (Table 2). A familiarization
period with the MRT preceded the study initiation. Four 1-hour training sessions were undertaken, including pilottesting on healthy athletes, where experts instructed novicesabout use and interpretation of the MRT. Consensus aboutscoring system and operational definition was reached.
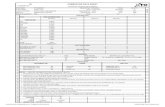
All the subjects received standardized instructionsregarding the performance of the MRT. They were initiallypositioned in supine, with the humerus abducted 90° (handto the ceiling) and supported in the plane of the scapula.Instructions were given as follows: “From this startingposition, internally rotate your shoulder with your scapulastill, as far as you can in a comfortable way.” The examinersplaced their index finger on the anterior humeral head andthe middle finger on the coracoid process during theprocedure, to evaluate humeral head and scapular move-ment, respectively (Fig 1). The test lasted 6 seconds in total;3 seconds for the active shoulder internal rotation and 3seconds for returning to the initial position. After receivingexplanation from the therapist, patients underwent onerepetition as a rehearsal before the formal test wasconducted. The formal test consisted of 3 repetitions ofthe test and straight afterward; the assessors had to interpretand score it, taking the second repetition for the analysis.
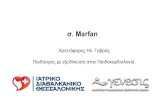
As 60° of shoulder active internal rotation has beenestablished as the reference standard range of movement forthe MRT,21 a home-made device consisting of a plinth with2 wedges joined with Velcro (Velcro, Barcelona, Spain) strapwas designed, to guarantee repeatability of the test (Fig 2).

Fig 1. A, Medial rotation test starting position. B, Medial rotationtest final position.
Fig 2. A big wedge supplied with a 30º angle (right) ensured thathe humerus remained in the scapular plane. A small wedge, alsosupplied with a 30º angle (left) and coupled to the big wedgeallowed for a maximum of 60º of active internal rotation with eachMRT repetition.
201Lluch et alJournal of Manipulative and Physiological TherapeuticsShoulder Medial Rotation TestVolume 37, Number 3
The big wedge supplied with a 30° angle ensured that thehumerus remained in the scapular plane. The plane of thescapula was considered 30° anterior to the coronal plane forall the participants following the description of the test byMorrissey et al,21 although it is known that scapular planecan vary, for instance, depending on the amount of thoracickyphosis.27 The small wedge, also supplied with a 30° angleand coupled to the big wedge, allowed for a maximum of 60°of active internal rotation with each repetition.
Statistical AnalysisDescriptive statistics were used to define the demographic
characteristics of the sample. A categorical scale with eitherpositive or negative was applied to rate the result from theMRT. Percentage agreement between assessors and κcoefficient with 95% confidence interval (CI) were used toestimate the intrarater reliability. In addition, Fleiss κ wasused, only with binary or nominal scale ratings, forcalculating interrater agreement. A κ coefficient less than0 was considered to reflect poor agreement, 0.01 to 0.20
t
,
slight agreement, 0.21 to 0.40 fair agreement, 0.41 to 0.60moderate agreement, 0.61 to 0.80 substantial agreement, and0.81 to 1.00 almost perfect agreement.28 Data were analyzedusing Minitab, version 15 (Minitab Inc, Paris, France).
RESULTS
A total of 17 overhead athletes, 59% (10) with rightshoulder pain, 35% (6) with left shoulder pain, and 6% (1)with bilateral shoulder pain, agreed to participate. There-fore, a total of 18 shoulders were evaluated. Most ofparticipants (94%) were right hand dominant (n = 16), witha mean VAS value for their current pain of 28.35 mm.Table 3 show the results of MRT scores in all subjects. Thepercentages for a positive MRT at the first (day 1) vs secondassessment (day 7) were 44.4% vs 44.4% (assessor 1,expert), 44.4% vs 38.8% (assessor 2, expert), 11.1% vs5.5%, (assessor 3, novice), and 16.6% vs 11.1% (assessor 4,novice), respectively. The intrarater reliability was fair forexaminer 1 (expert), substantial for examiner 2 (expert),poor for examiner 3 (novice), and substantial for examiner 4(novice), with κ values of 0.32, 0.65, −0.09, and 0.76,respectively. The results of the intrarater reliability studysuggest that the measurement reliability for the MRT isacceptable (percentage agreement, Table 4).
Interrater agreement for all 4 examiners demonstratedslight agreement (κ = 0.06; 95% CI: 0.06-0.47) andremained unchanged if we included in the analysis onlythe 2 more experienced (examiners 1 and 2) and the lessnovel assessor (examiner 4) (κ = 0.11; 95% CI: 0.06-0.47).The κ agreement increased to fair agreement (κ = 0.33;95% CI: 0.21-0.69), when we compared the MRT findingsfrom the 2 experienced assessors (examiners 1 and 2). Toobserve the training process in novel assessors (examiner 3and 4), 2 examination sessions were performed. The results

Table 3. Medial Rotation Test Scoring for All the Subjects (N = 17) in the Total of 18 Shoulders (Subject 17 Was Measured Bilaterally
E1-1 E1-2 E2-1 E2-2 E3-1 E3-2 E4-1 E4-2
0 0 0 0 0 0 0 0 Subject 11 0 0 0 1 0 0 0 Subject 20 0 1 0 1 0 0 0 Subject 31 1 0 0 0 1 1 0 Subject 41 1 0 0 0 1 0 0 Subject 50 0 0 0 0 0 0 0 Subject 60 0 0 1 1 1 0 0 Subject 71 1 0 0 1 1 0 0 Subject 81 1 0 0 1 1 0 1 Subject 91 1 0 0 1 1 0 0 Subject 101 0 1 0 1 0 0 0 Subject 110 1 0 0 0 0 0 0 Subject 120 0 0 0 1 0 0 0 Subject 130 0 0 0 0 0 0 0 Subject 140 0 0 1 0 0 0 0 Subject 150 0 0 0 0 0 0 0 Subject 160 1 0 1 0 1 0 1 Subject 171 1 0 0 0 0 0 0 Subject 1710 10 10 11 16 17 15 16 Total negative8 8 8 7 2 1 3 2 Total positive55.6 55.6 55.6 61.2 88.9 94.5 83.4 88.9 Percentage negative results (%)44.4 44.4 44.4 38.8 11.1 5.5 16.6 11.1 Percentage positive results (%)
0 equals to negative result; 1 equals to positive result.E1-1, examiner 1 (expert), first assessment (day 1). E1-2, examiner 1 (expert), second assessment (day 7); E2-1, examiner 2 (expert), first assessment (day1); E2-2, examiner 2 (expert), second assessment (day 7); E3-1, examiner 3 (novice), first assessment (day 1); E3-2, examiner 3 (novice), secondassessment (day 7); E4-1, examiner 4 (novice), first assessment (day 1); E4-2, examiner 4, second assessment (day 7).
able 4. Intrarater Agreement and Percentage With 95%onfidence Interval (CI)
Assessor Sample Agreement Percentage (95% CI)
1 18 12 66.67 (40.99-86.66)2 18 15 83.33 (58.58-96.42)3 18 15 83.33 (58.58-96.42)4 18 17 94.44 (72,71-99.86)
202 Journal of Manipulative and Physiological TherapeuticsLluch et alMarch/April 2014Shoulder Medial Rotation Test
TC
for the first session (at day 1) demonstrated poor agreement(κ = −0.05; 95% CI: 0.39-0.97), whereas they slightlyimproved in the second one (at day 7) (κ = 0.14; 95% CI:0.34-0.96).
DISCUSSION
The MRT aims at observing movement faults orcompensation strategies both at the scapula and glenohum-eral joint, which are hypothetically associated with arestriction of glenohumeral joint medial rotation and alteredscapulothoracic dynamic muscle control.8 This test wasdeveloped by observation of patients together with researchresults relating shoulder girdle movement, and it issupposedly a clinically useful tool to identify movementcontrol dysfunction at the shoulder girdle.21,29 The factorsinfluencing the MRT rating system (ie, list A and B;Table 2), are relying on the therapist subjective interpre-tation, leading the authors to a priori uncertainty aboutreliability for this test.
)
The present study demonstrated that, although values ofintrarater reliability were admissible except for oneexaminer, only slight agreement was reached when resultsof the MRT were compared between all the 4 examiners.Interestingly, interrater reliability increased when compar-ison was made between the 2 more experienced assessors,which may indicate that familiarity and expertise with thetest may be crucial for achieving good accuracy. Even so,overall reliability values were still lower than desired.Curiously, the novice examiner 4 achieved better intraraterreliability results than examiner 1 (expert). More time spentby novices on training in MRT testing before studycommencement might be the reason. Ellenbecker et al30
also found low interrater reliability in all their analyses whentrying to evaluate subtle scapular abnormalities thoroughvisual observation of scapular plane elevation. Other authorslike McClure et al19 or Uhl et al31, who examined interraterreliability of movement impairments classification at theshoulder region (ie, scapular dyskinesis categorization),found higher values than us with κ coefficients of 0.48 to0.61 and 0.40, respectively. It must be keep in mind,however, that all the aforementioned studies used onlyvisual observation for evaluation of movement dysfunction,whereas the method used during the MRT relies mostly onaccurate scapular and humeral motion tracking throughpalpation. Results are therefore not directly comparable.
Low values for interrater reliability achieved in the currentstudy could be due to several reasons. Firstly, someexaminers reported difficulties on palpation, particularly

203Lluch et alJournal of Manipulative and Physiological TherapeuticsShoulder Medial Rotation TestVolume 37, Number 3
with the coracoids process of larger subjects with abundantmuscle tissue. This point, together with the movement of thegreater tuberosity under the palpating index finger during theMRT, may have occasionally complicated the interpretationof the test. In addition, determination of the kinematic centerof the humeral head for tracking motion was donesubjectively. All these issues therefore cannot be discardedas influencing the final scoring of the examiners and thusoverall results for reliability. However, it is important to notethat scapula and humeral head palpation is a highly accurateand valid manner for motion tracking during the MRT.21
Finally, the fact that the study of Morrisey et al21 wasperformed with healthy subjects, whereas subjects formingour sample had shoulder pain, may have affected theaccuracy of motion tracking (pain is known to affectmovement), and this is turn reliability results.
Our percentages for positive MRT within experiencedassessors (approximately 40%) were higher than previouslyfound by Struyf et al22,23 (approximately 20%-25%). Extrapositive scores in the current studymay have beenmotivatedby experts’ prejudgment of movement aberrations, as theywere not blinded to the patients’ condition as in Struyf et al22
Prejudice may also be a major problem when evaluating apainful shoulder with the MRT in a clinical setting.However, knowledge of patient condition (and thusinclusion only of subjects with pain) was consideredvaluable in our study as movement analysis-based diagnosisalone has been demonstrated to be insufficient.32 Theinclusion of control healthy subjects and therefore increas-ing the variability of the sample may have influenced ourresults through avoiding possible raters’ predisposition fortoo many positive results in the MRT.
Interestingly, overestimation of experts’ positive results(and thus presence of motor control dysfunction), comparedwith novices’ (6%-17% positive test) was also noticed. Lessaccurate bony landmark palpation or estimation of scapularand humeral movement during the test by the lessexperienced assessors (ie, they could need the motorcontrol dysfunction to be more obvious to be detected)may explain those findings. Considering that observationand palpation were the only tools clinicians had forinterpreting the test, future investigations should make aneffort to develop new clinical methods for quantitativeassessment of motor control at the shoulder complex, as, forexample, reported at the lumbar spine by Enoch et al33
Morrissey et al21related positive results on theMRTwithincreased risk of impingement and instability. To validatethis assertion, evaluation of the MRT should be conductedon subgroups of patients affected by those pathologies.However, lack of uniformity and suitability of diagnosticlabeling for shoulder pain have been highlighted by severalauthors.34-36 Accordingly, no intent to recruit subjects withspecific diagnosis labels for their shoulder pain was planned,and only subjects with chronic “general” shoulder pain wereconsidered in this study.
LIMITATIONS
Some limitations of the study should be acknowledged.Possible occurrence of pain during the MRT was notconsidered, as the main objective of the study was toevaluate reliability of the visible and palpable informationregistered during the test. The existing interaction betweennociception and motor control is widely recognized.37-39
Consequently, pain experienced during performance of thetest could have induced motor inhibition and in turn affectthe achievement of the task. The present study onlyevaluated MRT on subjects with shoulder pain and intheir painful shoulder, so no healthy control group orcontralateral (ie, pain-free shoulder) measurement wasmade for comparison. Future research should expand theapplication of the MRT bilaterally and to pain-freepopulation to further ascertain the utility of the test.
This study does not say anything about the validity of theMRT (ie, how do patients with shoulder pain perform MRTcompared with subjects without shoulder pain). Futurestudies should therefore assess the validity of the MRT. Asthere is no clear indication in the literature of which is thebest interval between measurements for assessing motorcontrol dysfunction in terms of intratester reliability, wedecided to choose the 7-day interval. However, changes inpain level, activity, injury, or treatment that may haveoccurred during those 7 days were not assessed (partici-pants were only told to continue with normal activity duringthe 7-day interval between the 2 measurement points). Suchchanges might have influenced the results of the currentstudy but more likely in a way that would underestimate thereliability of the test.
As mentioned above, no attempt to identify the tissue inlesion was made in this study what could be considered alimitation, especially if one recognizes that most practi-tioners working with overhead throwing athletes still usepathoanatomic diagnoses. In addition, redefinition ofdiagnostic labels using movement system diagnoses asproposed by some35,36 is a topic which needs moreinterdisciplinary discussion, to make this nomenclatureconsistent and useful across clinicians and researchers.Finally, the findings from this study can only be applicableto athletes who compete in overhead sports, with shoulderpain complaints and more than 60º of shoulder internalrotation. In addition, studies done with athletes usuallyconsider subjects younger than the age interval (ages of 18-60 years) used here. However, the mean age of our sample(age of 30 years) is more or less reflective of the athleticpopulation with chronic shoulder pain.
CONCLUSIONS
Our results suggest that MRT reliability for detectingmovement control of the shoulder girdle was fair at best forexperienced examiners and poor overall. A long-term

204 Journal of Manipulative and Physiological TherapeuticsLluch et alMarch/April 2014Shoulder Medial Rotation Test
process of training may be necessary to acquire expertisewith accurate interpretation of the test.
Practical Applications• Intrarater but not interrater reliability values wereacceptable for the shoulder MRT.
• Familiarity and expertise with the test may becrucial for achieving good accuracy, as interraterreliability increased with experienced assessors.
• Future studies should assess the validity of theshoulder MRT.
FUNDING SOURCES AND POTENTIAL CONFLICTS OF INTERESTNo funding sources or conflicts of interest were reported
for this study.
CONTRIBUTORSHIP INFORMATION
Concept development (provided idea for the research):ELL, JN, FS.Design (planned the methods to generate the results):ELL, JB, LD, JC, YA, JN, FS.
Supervision (provided oversight, responsible for orga-nization and implementation, writing of the manuscript):ELL, JB, LD, JC, YA, JN, FS.Data collection/processing (responsible for experiments,patient management, organization, or reporting data):ELL, JB, LD, JC, YA.Analysis/interpretation (responsible for statistical analy-sis, evaluation, and presentation of the results): ELL, JB,LD, JC, YA, JN, FS.Literature search (performed the literature search): ELL
Writing (responsible for writing a substantive part of themanuscript): ELL, JB, JN, FS.Critical review (revised manuscript for intellectualcontent; this does not relate to spelling and grammarchecking): ELL, JB, LD, JC, YA, JN, FS.
REFERENCES
1. Mohseni-Bandpei MA, Keshavarz R, Minoonejhad H,Mohsenifar H, Shakeri H. Shoulder pain in Iranian eliteathletes: the prevalence and risk factors. J ManipulativePhysiol Ther 2012;35:541-8.
2. Winters JC, Sobel JS, Groenier KH, Arendzen JH, Meyboom-de Jong B. The long-term course of shoulder complaints: aprospective study in general practice. Rheumatology 1999;38:160-3.
3. Linsell L, Dawson J, Zondervan K, et al. Prevalence andincidence of adults consulting for shoulder conditions in UKprimary care; patterns of diagnosis and referral. Rheumatol-ogy 2006;45:215-21.
4. Ludewig PM, Cook TM. Alterations in shoulder kinematicsand associated muscle activity in people with symptoms ofshoulder impingement. Phys Ther 2000;80:276-91 [Review].
5. Kibler WB, Ludewig PM, McClure P, Uhl TL, Sciascia A.Scapular Summit 2009: introduction. July 16, 2009,Lexington, Kentucky. J Orthop Sports Phys Ther 2009;39:A1-A13.
6. Ludewig PM, Reynolds JF. The association of scapularkinematics and glenohumeral joint pathologies. J OrthopSports Phys Ther 2009;39:90-104.
7. Kibler WB, Ludewig PM, McClure PW, Michener LA, BakK, Sciascia AD. Clinical implications of scapular dyskinesisin shoulder injury: the 2013 consensus statement from the“Scapular Summit”. Br J Sports Med 2013;47:877-85.
8. Commerford M, Mottram S. Kinetic control. The managementof uncontrolled movement. First Edition. Churchill Living-stone, Australia; 2012.
9. Sahrmann SA. Diagnosis and treatment of movement.Impairment syndromes. St. Louis, MO: Mosby; 2002.
10. Caldwell C, Sahrmann S, Van Dillen L. Use of a movementsystem impairment diagnosis for physical therapy in themanagement of a patient with shoulder pain. J Orthop SportsPhys Ther 2007;37:551-63.
11. Struyf F, Nijs J, Baeyens J P, Mottram S, Meeusen R.Scapular positioning and movement in unimpaired shoulders,shoulder impingement syndrome, and glenohumeral instabil-ity. Scand J Med Sci Sports 2011;21:352-8.
12. Struyf F, Nijs J, Mottram S, Roussel N A, Cools A M,Meeusen R. Clinical assessment of the scapula: a review of theliterature [published online ahead of print July 21, 2012]. Br JSports Med.
13. Hébert LJ, Moffet H, McFadyen BJ, St-Vincent G. A methodof measuring three-dimensional scapular attitudes using theoptotrak probing system. Clin Biomech (Bristol, Avon) 2000;15:1-8.
14. Ebaugh DD, McClure PW, Karduna AR. Three-dimensionalscapulothoracic motion during active and passive armelevation. Clin Biomech (Bristol, Avon) 2005;20:700-9.
15. Park JY, Hwang JT, Kim KM, Makkar D, Moon SG, HanKJ. How to assess scapular dyskinesis precisely: 3-dimensional wing computer tomography—a new diagnosticmodality. J Shoulder Elbow Surg 2013;22:1084-91.
16. Nijs J, Roussel N, Struyf F, Mottram S, Meeusen R. Clinicalassessment of scapular positioning in patients with shoulderpain: state of the art. J Manipulative Physiol Ther 2007;30:69-75.
17. Magarey ME, Jones MA. Dynamic evaluation and earlymanagement of altered motor control around the shouldercomplex. Man Ther 2003;8:195-206 [Review].
18. Magarey ME, Jones MA. Specific evaluation of the functionof force couples relevant for stabilization of the glenohumeraljoint. Man Ther 2003;8:247-53.
19. McClure P, Tate AR, Kareha S, Irwin D, Zlupko E. A clinicalmethod for identifying scapular dyskinesis, part 1: reliability.J Athl Train 2009;44:160-4.
20. Wright AA, Wassinger CA, Frank M, Michener LA, HegedusEJ. Diagnostic accuracy of scapular physical examinationtests for shoulder disorders: a systematic review. Br J SportsMed 2013;47:886-92.
21. Morrissey D, Morrissey MC, Driver W, King JB, WoledgeRC. Manual landmark identification and tracking during themedial rotation test of the shoulder: an accuracy study usingthree-dimensional ultrasound and motion analysis measures.Man Ther 2008;13:529-35.
22. Struyf F, Nijs J, De Graeve J, Mottram S, Meeusen R.Scapular positioning in overhead athletes with and without

205Lluch et alJournal of Manipulative and Physiological TherapeuticsShoulder Medial Rotation TestVolume 37, Number 3
shoulder pain: a case-control study. Scand J Med Sci Sports2011;21:809-18.
23. Struyf F, Nijs J, Horsten S, Mottram S, Truijen S, Meeusen R.Scapular positioning and motor control in children and adults:a laboratory study using clinical measures. Man Ther 2011;16:155-60.
24. Wainner RS, Fritz JM, Irrgang JJ, Boninger ML, Delitto A,Allison S. Reliability and diagnostic accuracy of the clinicalexamination and patient self-report measures for cervicalradiculopathy. Spine (Phila Pa 1976) 2003;28:52-62.
25. Jensen MP, Mardekian J, Lakshminarayanan M, Boye ME.Validity of 24-h recall ratings of pain severity: biasing effectsof “peak” and “end” pain. Pain 2008;137:422-7.
26. Kahl C, Cleland J. Visual analogue scale, Numerical PainRating Scale and the McGill Pain Questionnaire: an overviewof physometric properties. Phys Ther Rev 2005;10:123-8.
27. Finley MA, Lee RY. Effect of sitting posture on 3-dimensional scapular kinematics measured by skin-mountedelectromagnetic tracking sensors. Arch Phys Med Rehabil2003;84:563-8.
28. Landis JR, Koch GG. The measurement of observeragreement for categorical data. Biometrics 1977;33:159-74.
29. ComerfordMJ,MottramSL.Movement and stability dysfunctioncontemporary developments. Man Ther 2001;6:15-26 [Review].
30. Ellenbecker TS, Kibler WB, Bailie DS, Caplinger R, DaviesGJ, Riemann BL. Reliability of scapular classification inexamination of professional baseball players. Clin OrthopRelat Res 2012;470:1540-4.
31. Uhl TL, Kibler WB, Gecewich B, Tripp BL. Evaluation ofclinical assessment methods for scapular dyskinesis. Arthros-copy 2009;25:1240-8.
32. Hickey BW, Milosavljevic S, Bell ML, Milburn PD.Accuracy and reliability of observational motion analysis inidentifying shoulder symptoms. Man Ther 2007;12:263-70.
33. Enoch F, Kjaer P, Elkjaer A, Remvig L, Juul-Kristensen B.Inter-examiner reproducibility of tests for lumbar motorcontrol. BMC Musculoskelet Disord 2011;12:114.
34. Schellingerhout JM, Verhagen AP, Thomas S, Koes BW.Lack of uniformity in diagnostic labeling of shoulderpain: time for a different approach. Man Ther 2008;13:478-83.
35. Lewis JS. Rotator cuff tendinopathy/subacromial impinge-ment syndrome: is it time for a new method of assessment?Br J Sports Med 2009;43:259-64.
36. Ludewig PM, Lawrence RL, Braman JP. What’s in a name?Using movement system diagnoses versus pathoanatomicdiagnoses. J Orthop SportsPhys Ther 2013;43:280-3.
37. Hodges PW. Pain and motor control: from the laboratory torehabilitation. J Electromyogr Kinesiol 2011;21:220-8.
38. Hodges PW, Tucker K. Moving differently in pain: a newtheory to explain the adaptation to pain. Pain 2011;152(3Suppl):S90-8.
39. Nijs J, Daenen L, Cras P, Struyf F, Roussel N, OostendorpRA. Nociception affects motor output: a review on sensory-motor interaction with focus on clinical implications. Clin JPain 2012;28:175-81.