The dynamics of urinary N -acetyl-β- d -glucosaminidase (NAG), a marker of renal tubular...
7
163 CLINICAL NOTE e dynamics of urinary N-acetyl-β-d-glucosaminidase (NAG), a marker of renal tubular dysfunction, in patients with lupus nephritis undergoing oral prednisone therapy Cristina Gluhovschi 1 , Silvia Velciov 1 , Adriana Kaycsa 2 , Gheorghe Gluhovschi 1 , Ligia Petrica 1 , Roxana Marian 1 , Gheorghe Bozdog 1 , Florica Gadalean 1 , Flaviu Bob 1 , Daniel Cioca 3 , and Corina Vernic 4 1 Division of Nephrology, University of Medicine and Pharmacy “V. Babes” Timisoara, Romania, 2 Division of Biochemistry, University of Medicine and Pharmacy “V. Babes” Timisoara, Romania, 3 Department of Cellular and Molecular Biology, University of Medicine and Pharmacy “V. Babes” Timisoara, Romania, and 4 Department of Medical Informatics and Biostatistics, University of Medicine and Pharmacy “V. Babes” Timisoara, Romania Abstract Introduction and aims: N-Acetyl-β-D-glucosaminidase (NAG), a marker of renal tubular dysfunction, is increased in patients with lupus nephritis. In addition to the toxic effects of proteinuria, patients with lupus nephritis may exhibit other factors that contribute to tubular dysfunction, such as pathogenic antitubular basement membrane antibodies. The aim of our study was to assess urinary NAG, proteinuria, and glomerular filtration rate (GFR) before treatment and after 7 and 30 days of oral prednisone therapy in patients with lupus nephritis. Methods: Ten patients with lupus nephritis, all females, mean age: 29.4 ± 10.17 years, were enrolled into the study. All the patients received oral prednisone 1 mg/kg. Twenty healthy subjects served as controls. We measured urinary NAG before treatment and after 7 and 30 days of oral prednisone therapy. Proteinuria, GFR, blood pressure, and side effects of therapy were also followed up. Urinary NAG was measured using the colorimetrical method and expressed as units per gram of creatinine (U/gCr). Statistical analysis (Wilcoxon signed ranks test and Wilcoxon rank sum test) was performed using SPSS 17. Results: In the 10 patients with lupus nephritis, urinary NAG before treatment was 16.9 ± 13.39 U/gCr (P = 0.005 compared with controls). NAG in controls was 1.73 ± 0.51 U/gCr. Proteinuria before treatment was 3.84 ± 1.93 g/24 h. The GFR before treatment was 50.48 ± 11.98 mL/min/1.73 m 2 . After 7 days of prednisone, urinary NAG was 23.55 ± 25.25 U/gCr (P = 0.878 compared with baseline, and P = 0.02 compared with controls). Proteinuria was 2.94 ± 1.3 g/24 h (P = 0.005 compared with baseline), and the GFR was 58.11 ± 13.64 mL/min/1.73 m 2 (P = 0.005 compared with baseline). After 30 days of prednisone, urinary NAG was 11.77 ± 12.18 U/gCr (P = 0.203 compared with baseline, P = 0.022 compared with the value after 7 days of prednisone, and P = 0.01 compared with controls). Proteinuria was 1.73 ± 0.68 g/24 h (P = 0.005 compared with baseline, and P = 0.005 compared with the value after 7 days of prednisone), and the GFR was 67.49 ± 16.42 mL/ min/1.73 m 2 (P = 0.005 compared with baseline and P = 0.009 compared with the value after 7 days of prednisone). Blood pressure measurements did not show any significant changes. No major side effects of steroid therapy were noticed. Conclusions: Urinary NAG showed a significant reduction between 7 and 30 days of therapy. The reduction in urinary NAG set in later than the decline in proteinuria and the improvement in GFR. Further studies incorporating a longer follow-up are needed to observe whether the reduction in NAG persists upon continuation of prednisone therapy. Keywords: Lupus nephritis, NAG, proteinuria, GFR, prednisone Address for Correspondence: Cristina Gluhovschi, Calea Aradului No. 8 Ap. 16, 300088 Timisoara, Romania. Tel: +40-256-435950. E-mail: [email protected] (Received 26 February 2011; revised 25 April 2011; accepted 29 April 2011) Immunopharmacology and Immunotoxicology, 2012; 34(1): 163–169 © 2012 Informa Healthcare USA, Inc. ISSN 0892-3973 print/ISSN 1532-2513 online DOI: 10.3109/08923973.2011.585343 Immunopharmacology and Immunotoxicology Downloaded from informahealthcare.com by McMaster University on 11/21/14 For personal use only.
Transcript of The dynamics of urinary N -acetyl-β- d -glucosaminidase (NAG), a marker of renal tubular...

163
CLINICAL NOTE
The dynamics of urinary N-acetyl-β-d-glucosaminidase (NAG), a marker of renal tubular dysfunction, in patients with lupus nephritis undergoing oral prednisone therapy
Cristina Gluhovschi1, Silvia Velciov1, Adriana Kaycsa2, Gheorghe Gluhovschi1, Ligia Petrica1, Roxana Marian1, Gheorghe Bozdog1, Florica Gadalean1, Flaviu Bob1, Daniel Cioca3, and Corina Vernic4
1Division of Nephrology, University of Medicine and Pharmacy “V. Babes” Timisoara, Romania, 2Division of Biochemistry, University of Medicine and Pharmacy “V. Babes” Timisoara, Romania, 3Department of Cellular and Molecular Biology, University of Medicine and Pharmacy “V. Babes” Timisoara, Romania, and 4Department of Medical Informatics and Biostatistics, University of Medicine and Pharmacy “V. Babes” Timisoara, Romania
AbstractIntroduction and aims: N-Acetyl-β-d-glucosaminidase (NAG), a marker of renal tubular dysfunction, is increased in patients with lupus nephritis. In addition to the toxic effects of proteinuria, patients with lupus nephritis may exhibit other factors that contribute to tubular dysfunction, such as pathogenic antitubular basement membrane antibodies. The aim of our study was to assess urinary NAG, proteinuria, and glomerular filtration rate (GFR) before treatment and after 7 and 30 days of oral prednisone therapy in patients with lupus nephritis.
Methods: Ten patients with lupus nephritis, all females, mean age: 29.4 ± 10.17 years, were enrolled into the study. All the patients received oral prednisone 1 mg/kg. Twenty healthy subjects served as controls. We measured urinary NAG before treatment and after 7 and 30 days of oral prednisone therapy. Proteinuria, GFR, blood pressure, and side effects of therapy were also followed up. Urinary NAG was measured using the colorimetrical method and expressed as units per gram of creatinine (U/gCr). Statistical analysis (Wilcoxon signed ranks test and Wilcoxon rank sum test) was performed using SPSS 17.
Results: In the 10 patients with lupus nephritis, urinary NAG before treatment was 16.9 ± 13.39 U/gCr (P = 0.005 compared with controls). NAG in controls was 1.73 ± 0.51 U/gCr. Proteinuria before treatment was 3.84 ± 1.93 g/24 h. The GFR before treatment was 50.48 ± 11.98 mL/min/1.73 m2. After 7 days of prednisone, urinary NAG was 23.55 ± 25.25 U/gCr (P = 0.878 compared with baseline, and P = 0.02 compared with controls). Proteinuria was 2.94 ± 1.3 g/24 h (P = 0.005 compared with baseline), and the GFR was 58.11 ± 13.64 mL/min/1.73 m2 (P = 0.005 compared with baseline). After 30 days of prednisone, urinary NAG was 11.77 ± 12.18 U/gCr (P = 0.203 compared with baseline, P = 0.022 compared with the value after 7 days of prednisone, and P = 0.01 compared with controls). Proteinuria was 1.73 ± 0.68 g/24 h (P = 0.005 compared with baseline, and P = 0.005 compared with the value after 7 days of prednisone), and the GFR was 67.49 ± 16.42 mL/min/1.73 m2 (P = 0.005 compared with baseline and P = 0.009 compared with the value after 7 days of prednisone). Blood pressure measurements did not show any significant changes. No major side effects of steroid therapy were noticed.
Conclusions: Urinary NAG showed a significant reduction between 7 and 30 days of therapy. The reduction in urinary NAG set in later than the decline in proteinuria and the improvement in GFR. Further studies incorporating a longer follow-up are needed to observe whether the reduction in NAG persists upon continuation of prednisone therapy.
Keywords: Lupus nephritis, NAG, proteinuria, GFR, prednisone
Address for Correspondence: Cristina Gluhovschi, Calea Aradului No. 8 Ap. 16, 300088 Timisoara, Romania. Tel: +40-256-435950. E-mail: [email protected]
(Received 26 February 2011; revised 25 April 2011; accepted 29 April 2011)
Immunopharmacology and Immunotoxicology, 2012; 34(1): 163–169© 2012 Informa Healthcare USA, Inc.ISSN 0892-3973 print/ISSN 1532-2513 onlineDOI: 10.3109/08923973.2011.585343
Immunopharmacology and Immunotoxicology
2012
34
1
163
169
26 February 2011
25 April 2011
29 April 2011
0892-3973
1532-2513
© 2012 Informa Healthcare USA, Inc.
10.3109/08923973.2011.585343
LIPI
585343
Imm
unop
harm
acol
ogy
and
Imm
unot
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 11
/21/
14Fo
r pe
rson
al u
se o
nly.

164 C. Gluhovschi et al.
Immunopharmacology and Immunotoxicology
Introduction
Systemic lupus erythematosus (SLE) is a multiorgan system autoimmune disease that displays a broad spec-trum of immunological and clinical manifestations. Renal disease occurs in 40–75% of SLE patients, most often within 5 years of disease onset, and is one of the stron-gest predictors of a poor outcome.(1,2) Renal disease in the course of SLE consists of glomerular lesions, tubulointer-stitial lesions, and renal vascular lesions.
According to Ponticelli, severe and predominant tubulointerstitial nephritis in SLE may cause clinical manifestations of renal disease, such as tubular acidosis, salt-losing nephritis, Fanconi syndrome, and occasion-ally acute renal failure.(1) Most patients have a benign, steroid-responsive course, but in some cases a progres-sive decline in renal function is observed.(1)
Renal tubular function is not routinely assessed in lupus patients, despite the fact that SLE may be associated with a variety of tubular defects. However, tubulointerstitial disease has a serious bearing on renal outcome. According to Marks, tubular defects may pro-vide an earlier and more effective indication of renal disease than glomerular defects and disease activity scoring systems. Investigations of tubular function may reveal earlier evidence of renal involvement and have implications for immunosuppressive and other treat-ment modalities.(3)
N-Acetyl-β-d-glucosaminidase (NAG) is a urinary enzyme that has been proposed as a valuable marker for renal tubular dysfunction.(4) Urinary NAG activity is probably an indicator of the increased lysosomal turn-over that occurs when increased protein is presented to the tubular cells.(5)
An abnormally increased entry of proteins into the uri-nary space, subsequent to an alteration of the glomerular barrier, overwhelms the protein-reabsorptive capacity of the proximal tubular cells and leads to damage of these reabsorbing cells. This protein toxicity for the epithelial tubular cells can be documented in all types of glomeru-lar disease.(6) Patients with lupus nephritis may exhibit additional factors that contribute to tubular dysfunction, such as pathogenic antitubular basement membrane antibodies.
Treatment with prednisone is a mainstay of lupus nephritis. Although the effect of prednisone on glom-erular lesions is well-known, its effect on tubular lesions warrants investigation. We used urinary NAG excretion as a biomarker to assess the effects of prednisone on renal tubular dysfunction.
Objectives
The aim of our study was to assess urinary NAG, protei-nuria, and glomerular filtration rate (GFR) before therapy and after 7 and 30 days of oral prednisone in patients with lupus nephritis.
Methods
Ten female patients with lupus nephritis (mean age 29.4 ± 10.17 years) were enrolled into the study. All the patients received oral prednisone 1 mg/kg. Twenty healthy subjects served as controls. We measured uri-nary NAG before treatment and after 7 and 30 days of oral prednisone therapy. Proteinuria, GFR, blood pressure, and side effects of therapy were also followed up.
Urinary NAG was measured by means of the colori-metrical method and expressed as units per gram of creatinine (U/gCr).
Assay
Morning urine samples were collected in plain con-tainers and stored at −20°C until the analyses were performed. The urine samples were brought to room temperature and centrifuged for 10 min at 1000 g. The supernatant was used for analyzing creatinine content and NAG activity.
Since these were spot urine samples, the mean patient urinary NAG activity was adjusted for variability in urine flow by dividing by urinary creatinine values and was expressed as U/gCr.
The creatinine concentration was measured by the Jaffe reaction using alkaline picric reagent.
NAG was determined using a commercial colorimet-ric assay kit (Roche, Mannheim, Germany, Cat. No. 875-406). In brief, the reaction mixtures, which consisted of a 1 mL solution of 3-cresol-sulfonphtaleinyl-N-acetyl-β-d-glucosaminide in citrate buffer and 0.05 mL of the urine sample, were incubated for 60 min at 37°C. The reactions were stopped with the kit’s sodium carbonate reagent (2 mL).
The completed reaction mixtures were measured within 50 min at 580 nm on a UV–visible spectrophotom-eter model Spekol 1300 (Analytik Jena, Jena, Germany). The mean values for NAG activity were calculated using paired duplicate specimens of urine. Duplicate speci-mens that exceeded a variation from the mean of 10% were discarded and re-run. The results were expressed as U/gCr.
The GFR was estimated by the modified diet in renal disease-4 (MDRD-4) method.
Statistical analysis
The statistical analysis (Wilcoxon signed ranks test and Wilcoxon rank sum test) was performed using SPSS 17.
The Wilcoxon signed ranks test was used to com-pare NAG, proteinuria, and GFR after 7 and 30 days of therapy with the values of these parameters before treatment.
The Wilcoxon rank sum test was used to compare NAG values in the patients with lupus nephritis with NAG val-ues in controls.
Imm
unop
harm
acol
ogy
and
Imm
unot
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 11
/21/
14Fo
r pe
rson
al u
se o
nly.

Dynamics of urinary NAG in patients with lupus nephritis 165
© 2012 Informa Healthcare USA, Inc.
A P-value < 0.05 was considered statistically significant.
Results
In the 10 patients with lupus nephritis, urinary NAG before treatment was 16.9 ± 13.39 U/gCr (P = 0.005 com-pared with controls). NAG in controls was 1.73 ± 0.51 U/gCr. Proteinuria before treatment was 3.84 ± 1.93 g/24 h. The GFR before treatment was 50.48 ± 11.98 mL/min/1.73 m2.
After 7 days of prednisone, urinary NAG was 23.55 ± 25.25 U/gCr (P = 0.878 compared with baseline, and P = 0.02 compared with controls). Proteinuria was 2.94 ± 1.3 g/24 h (P = 0.005 compared with baseline), and the GFR was 58.11 ± 13.64 mL/min/1.73 m2 (P = 0.005 compared with baseline).
After 30 days of prednisone, urinary NAG was 11.77 ± 12.18 U/gCr (P = 0.203 compared with base-line, P = 0.022 compared with the value after 7 days of prednisone, and P = 0.01 compared with controls). Proteinuria was 1.73 ± 0.68 g/24 h (P = 0.005 com-pared with baseline, and P = 0.005 compared with the
value after 7 days of prednisone), and the GFR was 67.49 ± 16.42 mL/min/1.73 m2 (P = 0.005 compared with baseline and P = 0.009 compared with the value after 7 days of prednisone).
Blood pressure measurements did not show any sig-nificant changes, and no major side effects of steroid therapy were noticed, either.
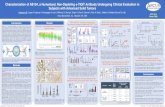
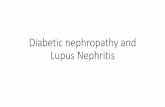
The dynamics of urinary NAG, proteinuria, and GFR are shown in Table 1. The dynamics of urinary NAG, pro-teinuria, and GFR for the individual cases are presented in Figures 1–10. An overview of the dynamics of NAG for all the 10 patients is shown in Figure 11.
Discussion
The most common presentation of lupus nephri-tis is glomerulonephritis. In some cases, however, the renal lesion is present in the tubulointerstitium. Tubulointerstitial involvement is a well-recognized but less frequently emphasized abnormality in lupus nephritis. Furthermore, tubulointerstitial damage due to increased protein traffic across the tubular cells is pres-ently considered to be the most important determinant
Figure 1. The dynamics of N-acetyl-β-d-glucosaminidase (NAG), proteinuria, and glomerular filtration rate (GFR) for patient 1.
Figure 2. The dynamics of N-acetyl-β-d-glucosaminidase (NAG), proteinuria, and glomerular filtration rate (GFR) for patient 2.
Imm
unop
harm
acol
ogy
and
Imm
unot
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 11
/21/
14Fo
r pe
rson
al u
se o
nly.

166 C. Gluhovschi et al.
Immunopharmacology and Immunotoxicology
of the progression to end-stage renal disease in patients with proteinuric glomerular disease.(5)
Proteinuria is actually regarded as the most crucial destructive factor for kidney structure, inducing an
inflammatory sequence within the nephron and renal parenchyma that initiates the progression to end-stage renal disease.(7) In addition to the toxic effects of proteinuria, patients with lupus nephritis may exhibit
Figure 3. The dynamics of N-acetyl-β-d-glucosaminidase (NAG), proteinuria, and glomerular filtration rate (GFR) for patient 3.
Figure 4. The dynamics of N-acetyl-β-d-glucosaminidase (NAG), proteinuria, and glomerular filtration rate (GFR) for patient 4.
Figure 5. The dynamics of N-acetyl-β-d-glucosaminidase (NAG), proteinuria, and glomerular filtration rate (GFR) for patient 5.
Imm
unop
harm
acol
ogy
and
Imm
unot
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 11
/21/
14Fo
r pe
rson
al u
se o
nly.

Dynamics of urinary NAG in patients with lupus nephritis 167
© 2012 Informa Healthcare USA, Inc.
other factors that contribute to tubular dysfunction, such as pathogenic antitubular basement membrane antibodies.
The central role of tubular damage in determining the progression to end-stage renal disease in proteinuric
glomerular diseases has prompted interest in finding reliable markers for tubular damage.
Urinary enzymes have been used as early markers of nephron toxicity, useful for detecting small changes in tubular epithelial cell function in many pathological
Figure 6. The dynamics of N-acetyl-β-d-glucosaminidase (NAG), proteinuria, and glomerular filtration rate (GFR) for patient 6.
Figure 7. The dynamics of N-acetyl-β-d-glucosaminidase (NAG), proteinuria, and glomerular filtration rate (GFR) for patient 7.
Figure 8. The dynamics of N-acetyl-β-d-glucosaminidase (NAG), proteinuria, and glomerular filtration rate (GFR) for patient 8.
Imm
unop
harm
acol
ogy
and
Imm
unot
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 11
/21/
14Fo
r pe
rson
al u
se o
nly.

168 C. Gluhovschi et al.
Immunopharmacology and Immunotoxicology
conditions.(8) NAG is a lysosomal enzyme found mostly in the proximal tubules. It is a valuable marker for detecting tubular dysfunction and for monitoring nephrotoxicity.(9)
Since both the quantity and quality of proteinuria predict the clinical course and the response to therapy
in glomerular diseases,(5,10) an assessment of the quali-tative aspect of proteinuria (e.g. tubular proteinuria) by means of urinary NAG may be a useful supplement to the routine urinary biochemical analysis performed in SLE cases.(6)
Figure 11. The dynamics of N-acetyl-β-d-glucosaminidase (NAG) for all the 10 patients.
Figure 10. The dynamics of N-acetyl-β-d-glucosaminidase (NAG), proteinuria, and glomerular filtration rate (GFR) for patient 10.
Figure 9. The dynamics of N-acetyl-β-d-glucosaminidase (NAG), proteinuria, and glomerular filtration rate (GFR) for patient 9.
Imm
unop
harm
acol
ogy
and
Imm
unot
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 11
/21/
14Fo
r pe
rson
al u
se o
nly.

Dynamics of urinary NAG in patients with lupus nephritis 169
© 2012 Informa Healthcare USA, Inc.
Our study sought to assess urinary NAG, proteinuria and GFR before therapy and after 7 and 30 days of oral prednisone in patients with lupus nephritis.
Before treatment, urinary NAG values were signifi-cantly higher than in controls (P = 0.005), indicating the presence of renal tubular dysfunction. This finding is con-sistent with the results reported by Marks and Erdener.(3,6)
After 7 days of oral prednisone therapy, urinary NAG did not change significantly. Proteinuria declined signifi-cantly and GFR increased significantly.
After 30 days of oral prednisone, urinary NAG declined significantly compared with the value after 7 days of oral prednisone. The decline in urinary NAG between 7 and 30 days of oral prednisone suggests that the reduction in urinary NAG sets in after the reduction in proteinuria and the improvement in GFR. Further studies incorpo-rating a longer follow-up are needed to observe whether the reduction in NAG persists upon continuation of pred-nisone therapy.
The dynamics of urinary NAG, proteinuria, and GFR for the individual cases were extremely variable.
Although previous studies(3,6) have shown increases in the urinary excretion of NAG in patients with lupus nephritis, the changes in this urinary parameter during the clinical course of lupus nephritis have not yet been fully clarified.
Proximal tubule dysfunction may be a sign of active lupus nephritis.(11) The reduction in urinary NAG between 7 and 30 days of therapy may be a more subtle indicator than proteinuria that active lupus nephritis begins to recede.
Conclusions
Urinary NAG showed a significant reduction between 7 and 30 days of therapy. The reduction in urinary NAG set in later than the decline in proteinuria and the improvement in GFR. Further studies incorporating a longer follow-up are needed to observe whether the reduction in NAG persists upon continuation of predni-sone therapy.
Declaration of interest
The authors declare no conflicts of interest.
References 1. Ponticelli, C., Banfi, G., Moroni, G. Systemic lupus erythematosus.
In: Oxford Textbook of Clinical Nephrology, 3rd edition. Edited by Davison, A., Cameron, J.S., Gruenfeld, J.P., Ponticelli, C., Ritz, E., Winearls, C., van Ypersele, C. Oxford University Press, Oxford, 2005, pp. 824–842.
2. Mason, L.J., Isenberg, D.A. The patient with systemic lupus erythematosus. In: Oxford Textbook of Clinical Nephrology, 3rd edition. Edited by Davison, A., Cameron, J.S., Gruenfeld, J.P., Ponticelli, C., Ritz, E., Winearls, C., van Ypersele, C. Oxford University Press, Oxford, 2005, pp. 809–824.
3. Marks, S.D., Shah, V., Pilkington, C., Woo, P., Dillon, M.J. Renal tubular dysfunction in children with systemic lupus erythematosus. Pediatr Nephrol 2005, 20, 141–148.
4. Bosomworth, M.P., Aparicio, S.R., Hay, A.W. Urine N-acetyl-beta-d-glucosaminidase—a marker of tubular damage? Nephrol Dial Transplant 1999, 14, 620–626.
5. Bazzi, C., Petrini, C., Rizza, V., Arrigo, G., Napodano, P., Paparella, M., D’Amico, G. Urinary N-acetyl-beta-glucosaminidase excretion is a marker of tubular cell dysfunction and a predictor of outcome in primary glomerulonephritis. Nephrol Dial Transplant 2002, 17, 1890–1896.
6. Erdener, D., Aksu, K., Biçer, I., Doganavsargil, E., Kutay, F.Z. Urinary N-acetyl-beta-d-glucosaminidase (NAG) in lupus nephritis and rheumatoid arthritis. J Clin Lab Anal 2005, 19, 172–176.
7. Hallan, S.I., Ritz, E., Lydersen, S., Romundstad, S., Kvenild, K., Orth, S.R. Combining GFR and albuminuria to classify CKD improves prediction of ESRD. J Am Soc Nephrol 2009, 20, 1069–1077.
8. D’Amico, G., Bazzi, C. Urinary protein and enzyme excretion as markers of tubular damage. Curr Opin Nephrol Hypertens 2003, 12, 639–643.
9. Price, R.G. The role of NAG (N-acetyl-beta-d-glucosaminidase) in the diagnosis of kidney disease including the monitoring of nephrotoxicity. Clin Nephrol 1992, 38 (Suppl 1), S14–S19.
10. D’Amico, G., Bazzi, C. Pathophysiology of proteinuria. Kidney Int 2003, 63, 809–825.
11. Tsai, C.Y., Wu, T.H., Yu, C.L., Lu, J.Y., Tsai, Y.Y. Increased excretions of beta2-microglobulin, IL-6, and IL-8 and decreased excretion of Tamm-Horsfall glycoprotein in urine of patients with active lupus nephritis. Nephron 2000, 85, 207–214.
Table 1. The dynamics of urinary N-acetyl-β-d-glucosaminidase (NAG), proteinuria, and glomerular filtration rate (GFR).
Parameter Before treatment After 7 days of oral prednisoneAfter 30 days of oral prednisone
Urinary NAG (U/gCr) 16.9 ± 13.39 23.55 ± 25.25 11.77 ± 12.18Proteinuria (g/24 h) 3.84 ± 1.93 2.94 ± 1.3 1.73 ± 0.68GFR (mL/min/1.73 m2) 50.48 ± 11.98 58.11 ± 13.64 67.49 ± 16.42
Imm
unop
harm
acol
ogy
and
Imm
unot
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
cMas
ter
Uni
vers
ity o
n 11
/21/
14Fo
r pe
rson
al u
se o
nly.