The clinical role of serum concentrations of selected cytokines: IL-1 β , TNF- α and IL-6 in...
7
http://informahealthcare.com/aut ISSN: 0891-6934 (print), 1607-842X (electronic) Autoimmunity, Early Online: 1–7 ! 2014 Informa UK Ltd. DOI: 10.3109/08916934.2014.914175 ORIGINAL ARTICLE The clinical role of serum concentrations of selected cytokines: IL-1b, TNF-a and IL-6 in diagnosis of autoimmune thyroid disease (AITD) in children Hanna Mikos 1,2 , Marcin Mikos 3 , Barbara Rabska-Pietrzak 1 , and Marek Niedziela 1,2 1 Department of Pediatric Endocrinology and Rheumatology, 2 Molecular Endocrinology Laboratory, and 3 Department of Pneumonology, Allergology and Clinical Immunology, Poznan University of Medical Sciences, Poznan, Poland Abstract Chronic autoimmune thyroiditis (cAIT) leads to hypothyroidism due to T cell-mediated cytotoxicity in most cases. By contrast, Graves’ disease (GD) with thyrotropin receptor stimulatory autoantibodies cause hyperthyroidism. Cytokines play a crucial role in modulating immune response in both disorders. The aim of study was to evaluate the concentrations of cytokines: IL-1b, TNF-a and IL-6 in these two opposite clinical and hormonal thyroid diseases. The study group consisted of 64 children, 44 newly diagnosed, untreated children with cAIT (n ¼ 22; with hypothyroidism) and GD (n ¼ 22; hyperthyroidism), and the control group of 20 healthy children. Cytokine concentrations were evaluated using the ELISA technique. The studied groups of children did not differ significantly in concentrations of IL-6 (p ¼ 0.48) and TNF-a (p ¼ 0.067). In children with hypothyroidism, we found significantly higher concentra- tions of IL-1b (median 2.16 pg/ml, IQR 0.87) compared to hyperthyroidism (median 1.39 pg/l, IQR 1.27) (p50.01) and the control group (median 1.88 pg/ml, IQR 1.04) (p50.05). The results of ROC curve analysis demonstrated the usefulness of IL-1b (AUC ¼ 0.77, p ¼ 0.003) and TNF-a (AUC ¼ 0.691, p ¼ 0.034) as diagnostic parameters in cAIT which enable discrimination of children with autoimmune thyroid disease from healthy individuals. Concentrations of these markers are increased in autoimmune hypothyroidism. We found no significant sex differences in the tested parameters. In conclusion, IL-1b and TNF-a may be considered as markers of hypothyroidism, and could efficiently discriminate between healthy and autoimmune hypothyroid children. Significantly higher concentrations of IL-1b in children with hypothy- roidism may be used to distinguish children with cAIT from GD patients. Keywords Autoimmunity, cytokines, children, serum, thyroid History Received 15 February 2014 Revised 22 March 2014 Accepted 8 April 2014 Published online 7 May 2014 Introduction Autoimmune thyroid disease (AITD) is the most common organ-specific autoimmune disease. It is characterized by infiltration of the gland by T- and B-lymphocytes, dendritic cells and macrophages. The presence of autoantibodies reacting against thyroid autoantigens and alterations in T cell subsets are also characteristic features of AITD [1]. Autoimmune thyroid dysfunction creates an image consisting of two opposing clinical and hormonal states of thyroid function: chronic autoimmune thyroiditis (cAIT) presenting as hypothyroidism and Graves’ disease (GD), characterized by hyperthyroidism. The thyroid gland of patients with auto- immune thyroid disease is morphologically characterized by massive infiltration of lymphoid cells. The interleukin-1 (IL-1), tumor necrosis factor-a (TNF-a) and interleukin-6 (IL-6) are involved in the intercellular communication required to initiate and control immune response. However, their role in the pathogenesis of AITD is unclear. Antigen determinants activate naive CD4+ T cells, which may differentiate into Th1 cells and contribute to the development of HT [2]. Reduced number of Tregs with CD4+CD25 and CD4+FoxP3 phenotype suggests their role in initiation of autoimmune process in thyroid disorders in children [3]. Both T helper 17 (Th17) and T regulatory cells might play a role in the pathogenesis of GD [4]. B cells have taken the center stage in tolerance and autoimmunity, mainly through polar- ization of T cell subsets (Tregs/Th1/Th2) and their ability to produce cytokines [5]. The pathogenesis of GD is complex and heterogeneous and hyperthyroidism is an example of antibody-mediated organ-specific autoimmunity. Since TSAb and B-cell proliferation is hallmark of GD, Th2 responses have been associated with its pathogenesis [6]. Cytokines, predominantly IL-1b, TNF-a and IL-6, have been implicated in the pathogenesis of AITD and are also considered to play important role in intrathyroidal inflammation and modulation of thyrocyte growth and function [7,8]. Correspondence: Prof. Marek Niedziela, MD, PhD, Department of Pediatric Endocrinology and Rheumatology, 2nd Chair of Pediatrics, Poznan University of Medical Sciences, 27/33, Szpitalna Street, 60-572 Poznan, Poland. Tel: +48 61 8491481. Fax: +48 61 8480291. E-mail: [email protected] Autoimmunity Downloaded from informahealthcare.com by Thammasat University on 10/08/14 For personal use only.
Transcript of The clinical role of serum concentrations of selected cytokines: IL-1 β , TNF- α and IL-6 in...

http://informahealthcare.com/autISSN: 0891-6934 (print), 1607-842X (electronic)
Autoimmunity, Early Online: 1–7! 2014 Informa UK Ltd. DOI: 10.3109/08916934.2014.914175
ORIGINAL ARTICLE
The clinical role of serum concentrations of selected cytokines: IL-1b,TNF-a and IL-6 in diagnosis of autoimmune thyroid disease (AITD) inchildren
Hanna Mikos1,2, Marcin Mikos3, Barbara Rabska-Pietrzak1, and Marek Niedziela1,2
1Department of Pediatric Endocrinology and Rheumatology, 2Molecular Endocrinology Laboratory, and 3Department of Pneumonology,
Allergology and Clinical Immunology, Poznan University of Medical Sciences, Poznan, Poland
Abstract
Chronic autoimmune thyroiditis (cAIT) leads to hypothyroidism due to T cell-mediatedcytotoxicity in most cases. By contrast, Graves’ disease (GD) with thyrotropin receptorstimulatory autoantibodies cause hyperthyroidism. Cytokines play a crucial role in modulatingimmune response in both disorders. The aim of study was to evaluate the concentrations ofcytokines: IL-1b, TNF-a and IL-6 in these two opposite clinical and hormonal thyroid diseases.The study group consisted of 64 children, 44 newly diagnosed, untreated children with cAIT(n¼ 22; with hypothyroidism) and GD (n¼ 22; hyperthyroidism), and the control group of 20healthy children. Cytokine concentrations were evaluated using the ELISA technique. Thestudied groups of children did not differ significantly in concentrations of IL-6 (p¼ 0.48) andTNF-a (p¼ 0.067). In children with hypothyroidism, we found significantly higher concentra-tions of IL-1b (median 2.16 pg/ml, IQR 0.87) compared to hyperthyroidism (median 1.39 pg/l,IQR 1.27) (p50.01) and the control group (median 1.88 pg/ml, IQR 1.04) (p50.05). The results ofROC curve analysis demonstrated the usefulness of IL-1b (AUC¼ 0.77, p¼ 0.003) and TNF-a(AUC¼ 0.691, p¼ 0.034) as diagnostic parameters in cAIT which enable discrimination ofchildren with autoimmune thyroid disease from healthy individuals. Concentrations of thesemarkers are increased in autoimmune hypothyroidism. We found no significant sex differencesin the tested parameters. In conclusion, IL-1b and TNF-a may be considered as markers ofhypothyroidism, and could efficiently discriminate between healthy and autoimmunehypothyroid children. Significantly higher concentrations of IL-1b in children with hypothy-roidism may be used to distinguish children with cAIT from GD patients.
Keywords
Autoimmunity, cytokines, children, serum,thyroid
History
Received 15 February 2014Revised 22 March 2014Accepted 8 April 2014Published online 7 May 2014
Introduction
Autoimmune thyroid disease (AITD) is the most common
organ-specific autoimmune disease. It is characterized by
infiltration of the gland by T- and B-lymphocytes, dendritic
cells and macrophages. The presence of autoantibodies
reacting against thyroid autoantigens and alterations in T
cell subsets are also characteristic features of AITD [1].
Autoimmune thyroid dysfunction creates an image consisting
of two opposing clinical and hormonal states of thyroid
function: chronic autoimmune thyroiditis (cAIT) presenting
as hypothyroidism and Graves’ disease (GD), characterized by
hyperthyroidism. The thyroid gland of patients with auto-
immune thyroid disease is morphologically characterized by
massive infiltration of lymphoid cells. The interleukin-1
(IL-1), tumor necrosis factor-a (TNF-a) and interleukin-6
(IL-6) are involved in the intercellular communication
required to initiate and control immune response. However,
their role in the pathogenesis of AITD is unclear. Antigen
determinants activate naive CD4+ T cells, which may
differentiate into Th1 cells and contribute to the development
of HT [2]. Reduced number of Tregs with CD4+CD25 and
CD4+FoxP3 phenotype suggests their role in initiation of
autoimmune process in thyroid disorders in children [3]. Both
T helper 17 (Th17) and T regulatory cells might play a role in
the pathogenesis of GD [4]. B cells have taken the center
stage in tolerance and autoimmunity, mainly through polar-
ization of T cell subsets (Tregs/Th1/Th2) and their ability to
produce cytokines [5]. The pathogenesis of GD is complex
and heterogeneous and hyperthyroidism is an example of
antibody-mediated organ-specific autoimmunity. Since TSAb
and B-cell proliferation is hallmark of GD, Th2 responses
have been associated with its pathogenesis [6]. Cytokines,
predominantly IL-1b, TNF-a and IL-6, have been implicated
in the pathogenesis of AITD and are also considered to play
important role in intrathyroidal inflammation and modulation
of thyrocyte growth and function [7,8].
Correspondence: Prof. Marek Niedziela, MD, PhD, Department ofPediatric Endocrinology and Rheumatology, 2nd Chair of Pediatrics,Poznan University of Medical Sciences, 27/33, Szpitalna Street, 60-572Poznan, Poland. Tel: +48 61 8491481. Fax: +48 61 8480291. E-mail:[email protected]
Aut
oim
mun
ity D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ham
mas
at U
nive
rsity
on
10/0
8/14
For
pers
onal
use
onl
y.

Materials and methods
Patients
The study group consisted of 64 children: 45 girls (70.3%) and
19 boys (23.7%). The study group was divided into three
subgroups: 22 newly diagnosed, untreated hypothyroid chil-
dren with cAIT, including 18 girls (81.8%) and 4 boys
(18.2%), with median age of 11.3 years (range: 6.7–15.9); 22
untreated hyperthyroid children with GD: including 16 girls
(72.7%) and 6 boys (27.3%), with median age of 14.7 years,
(range: 3.2–18.1) and a control group of 20 healthy children:
11 girls (55%) and 9 boys (45%), with median age of 12.7
years (range: 1.9–18.0). These groups were comparable in
terms of age and gender distribution (p¼ 0.31). Therefore, the
study included children with newly diagnosed autoimmune
thyroid disease. Patients were recruited from the Department
of Endocrinology and Rheumatology K. Jonscher’s Clinical
Hospital, Poznan University of Medical Sciences and pedi-
atric endocrinology outpatient clinic. All children underwent
full history, pediatric examination, laboratory tests and
thyroid ultrasound. The study was performed in accordance
with the Helsinki Declaration and good clinical practice and
was approved by the local Ethics Committee. The inclusion
criteria were: female and male subjects, age below 18 years of
age and confirmed diagnosis cAIT and GD (criteria: hormo-
nal, immunological profile and thyroid ultrasound).
Thyroid function
Serum samples were tested for serum concentrations of TSH
(reference range: 0.46–4.67 mIU/ml) and free T4 (reference
range: 0.71–1.85 ng/dl), free T3 (reference range: 1.45–
3.48 pg/ml) using Abbott AxSYM System (Abbott
Diagnostics, Germany). Antithyroid antibodies (ATG,
ATPO, TRAb) in all participants were examined by radio-
immunoassay, according to the manufacturers’ instructions
(BRAHMS, Berlin, Germany). The reference values for
ATPO and ATG were below 60 IU/ml and for TRAb below
1 U/l. The tests were conducted in the Laboratory of the K.
Jonscher’s Clinical Hospital of Poznan University of Medical
Sciences. Anthropometrical measurements (weight and
height) were performed in all participants of the study and
were used to calculate BMI, BMI-SDS and Cole index.
Reference percentile charts for Polish children were used for
the analysis of the obtained data [9] (Table 1).
Cytokine assays
Peripheral blood samples were collected before treatment
introduction. Sera were collected after centrifugation imme-
diately after blood was drawn and stored at �70 �C until
assayed. Serum concentrations of IL-1b, TNF-a and IL-6
were evaluated using ELISA kits (Bender MedSystems
GmbH, Vienna, Austria) according to manufacturer’s instruc-
tions. The limit of detection for IL-1b was 0.32 pg/ml (intra-
and interassay CV: 8.6% and 5.1%, respectively); for TNF-a:
5.0 pg/ml (intra- and interassay CV: 8.1%, 7.7%); for IL-6:
0.92 pg/ml (intra- and interassay CV: 5.2%, 3.2%). The
analyses were conducted in the Molecular Endocrinology
Laboratory of the Department of Pediatric Endocrinology and
Rheumatology of Poznan University of Medical Sciences
(Table 2).
Statistical analyses
A Shapiro–Wilk test was used to verify the normality of
subsets of data. Descriptive statistics including mean with
standard deviation for normally distributed variables was
reported, otherwise median with interquartile range was
reported. The differences between the two groups were
analyzed for significance either with t-test or Mann–Whitney
non-parametric test. The significance of differences between
all three groups was either tested with ANOVA with
Newman–Keuls post-test or with a Kruskal–Wallis test
with Dunn’s post-test. Nominal variables were tested with
Pearson’s chi-square. The correlations between variables were
evaluated by Spearman rank correlation test. To determine the
diagnostic value of cytokines, we calculated the area under
the curve (AUC) of the receiver operating characteristic
(ROC) curve. Cut-off values for ROC curves were calculated
with J-Youden statistic. SPSS 17.0 for Windows (SPSS,
Chicago, IL) was used in the analysis. A p value less than 0.05
was considered statistically significant.
Results
Relationships between metabolic and thyroidfunction
We found no significant differences in the tested parameters
between boys and girls in groups of children with cAIT and
GD (age, BMI, BMI-SDS, Cole index, TSH, fT4, fT3, ATG,
ATPO, TRAb, IL-1b, TNF-a and IL-6). There were no
Table 1. Demographic and clinical characteristics of groups.
HypothyroidismMean ± SD median (IQR)
HyperthyroidismMean ± SD median (IQR)
Control groupMean ± SD median (IQR) s
n n¼ 22 n¼ 22 n¼ 20
Sex 18 girls/4 boys 16 girls/6 boys 11 girls/9 boys nsAge (years) 11.39 ± 2.68 14.75 (7.09) 11.57 ± 4.86 nsBMI (kg/m2) 18.69 (5.45) 18.25 ± 3.42 18.17 ± 3.50 nsBMI-SDS 0.3 (2.04) �0.38 ± 1.05 �0.55 (1.29) nsCole index 1.05 ± 0.22 0.95 ± 0.13 0.9 ± 70.14 nsTSH (0.5–5.0mIU/ml) 37.34 (17.69)" 0 (0.01)# 2.42 (1.52) p50.001 (K–W)fT4 (0.7–1.85 ng/dl) 0.54 ± 0.31# 4.24 ± 1.06" 1.03 ± 0.12 p50.001 (ANOVA)fT3 (1.7–3.5 pg/ml) 2.10 ± 0.97 19.01 ± 5.30" 2.70 ± 0.56 p50.001 (ANOVA)ATG (560 IU/ml) 124 (589)" 101 (552)" 20 (4.5) p50.001 (K–W)ATPO (560 IU/ml) 3000 (111)" 3000 (1536)" 10 (29) p50.001 (K–W)TRAb (51 IU/l) 0.7 ± 0.3 16.75 (24.6)" 0.5 ± 0.3 p50.001 (K–W)
#: below reference range; ": above reference range.
2 H. Mikos et al. Autoimmunity, Early Online: 1–7
Aut
oim
mun
ity D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ham
mas
at U
nive
rsity
on
10/0
8/14
For
pers
onal
use
onl
y.

significant differences in age and nutritional status param-
eters: BMI, BMI-SDS and Cole index between the groups
with cAIT, GD and control (p¼ 0.31, p¼ 0.8, p¼ 0.31,
p¼ 0.15). The study identified statistically significant differ-
ences (p50.001) of parameters of thyroid hormonal function
(TSH, fT4 and fT3) and immune markers: (ATG, ATPO and
TRAb) between the analyzed groups of children. All of these
observed differences are directly related to the opposing states
of hormonal hyperthyroidism and hypothyroidism compared
to the control group.
Cytokine serum concentrations
Serum IL-6 levels did not differ significantly between all
groups: cAIT (median; IQR; range: 1.60 pg/ml; 0.07; 0.39–
11.10), GD (1.60 pg/ml; 0.04; 0.39–9.18) and control
(1.56 pg/ml; 0.37; 0.12–2.48) (p¼ 0.48). Likewise, no sig-
nificant differences in TNF-a concentration between the
groups of children were found: cAIT (median; IQR; range:
15.08 pg/ml; 21.94; 0.00–143.44), GD (13.63 pg/ml; 15.28;
0.00–28.51) and control (0.96 pg/ml; 12.81; 0.00–17.75)
(p¼ 0.067).
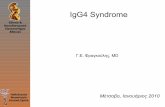
Significantly higher serum IL-1b concentration was found
in children with cAIT (median; IQR; range: 2.16 pg/ml; 0.87;
0.11–9.53), compared to control (1.88 pg/ml; 1.04; 0.01–2.38)
(p50.05) and cAIT compared to GD (1.39 pg/ml; 1.27; 0.26–
2.68) (p50.01) (Figure 1). There was no difference in IL-1bconcentration between children with hyperthyroidism and
control group (p40.05).
Correlations of cytokine concentrations
Significant positive correlations between cytokines were
identified; in cAIT: IL-1b and TNF-a (r¼ 0.45, p50.05)
and in GD: IL-6 and TNF-a (r¼ 0.62, p50.01). TNF-apositively correlated with ATPO in cAIT (r¼ 0.54, p50.01)
as well as IL-1b and ATPO in GD (r¼ 0.47; p50.05). In the
control group, we found negative correlation of IL-1b and
TNF-a (r¼�0.58, p50.01).
ROC analysis
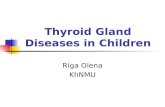
The results of ROC curve analysis enabled determination of
usefulness of monitoring cytokine concentrations in order to
discriminate children with autoimmune thyroid disease from
healthy individuals. Cytokines IL-1b (AUC¼ 0.77,
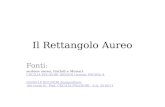
p¼ 0.003) (Table 3 and Figure 2) and TNF-a(AUC¼ 0.691, p¼ 0.034) (Table 3 and Figure 3) discrimi-
nated healthy and autoimmune-hypothyroid (cAIT) children
Table 2. Comparison of serum cytokines concentrations between groups.
HypothyroidismMean ± SD median (IQR)
HyperthyroidismMean ± SD median (IQR)
Control groupMean ± SD median (IQR)
n n¼ 22 n¼ 22 n¼ 20 s
TNF-a (pg/ml) 19.57 ± 31.95 10.44 ± 8.31 6.43 ± 7.26 ns15.80 (21.94) 13.63 (15.28) 0.96 (12.81) p¼ 0.067 (K–W)
IL-6 (pg/ml) 2.09 ± 2.13 1.96 ± 1.76 1.40 ± 0.53 ns2.60 (0.07) 1.60 (0.04) 1.56 (0.37) p¼ 0.48 (K–W)
IL-1b (pg/ml) 2.58 ± 1.80 1.45 ± 0.67 1.48 ± 0.702.16 (0.87) 1.39 (1.27) 1.88 (1.04) p¼ 0.002 (K–W)
Figure 1. Boxplot of IL-1b serum concentra-tions in the hypothyroid, hyperthyroid andcontrol groups. [*]: outlier.
DOI: 10.3109/08916934.2014.914175 IL-1�, TNF-� and IL-6 in AITD in children 3
Aut
oim
mun
ity D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ham
mas
at U
nive
rsity
on
10/0
8/14
For
pers
onal
use
onl
y.

with low sensitivity of 59.1% and 54.5%, respectively, but
high specificity of 95% and 85% at cut-off points of 2.1 pg/ml
for IL-1b and 14.7 pg/ml for TNF-a. The concentration of
these markers increased in hypothyroidism. Moreover, the
ROC curve for IL-1b showed good sensitivity and specificity
for discriminating between the cAIT and GD groups:
AUC¼ 0.773; p¼ 0.002 (sensitivity 72.7%, specificity
86.4%) at cut-off point of 1.7 pg/ml (Table 4 and Figure 4).
None of the studied cytokines IL-1b, TNF-a and IL-6
effectively discriminated between GD and control (AUC did
not differ significantly from 0.5: p¼ 0.801, p¼ 0.092 and
p¼ 0.435, respectively) (Table 5).
Discussion
In AITD, the occurrence of both Th1 and Th2 cell-mediated
immune response is documented, but the specific role of
cytokines in both opposing clinical states of disease is not
clearly defined. cAIT is characterized by destruction of
thyroid cells and dominance of Th1 type immune response
with secretion of the following cytokines: IL-1b, IL-2, TNF-aand IFN-g. In contrast, GD is characterized by stimulation of
the gland through TSAb with Th2 cytokine pattern dominated
by secretion of IL-4, IL-5, IL-6, IL-9, IL-10 and IL-13. Th1
and Th2 cells are responsible for specific cytokine profiles in
Table 3. Area under the curve: cAIT versus control.
Asymptotic 95%confidence interval
Variable AreaStandard
errorAsymptoticsignificance
Lowerbound
Upperbound
IL-6 (pg/ml) 0.601 0.088 p¼ 0.262 (ns) 0.428 0.774IL-1b (pg/ml) 0.770 0.073 p¼ 0.003 0.627 0.914TNF-a (pg/ml) 0.691 0.082 p¼ 0.034 0.529 0.852
Figure 2. ROC curve of IL-1b: cAIT versus control group (AUC¼ 0.77,p¼ 0.003, cut-off¼ 2.1 pg/ml; sensitivity: 59.1%, specificity: 95%).
Table 4. Area under the curve: cAIT versus GD.
Asymptotic 95%confidence interval
Variable AreaStandard
errorAsymptoticsignificance
Lowerbound
Upperbound
IL-6 (pg/ml) 0.536 0.088 p¼ 0.681 (ns) 0.363 0.709TNF-a (pg/ml) 0.572 0.089 p¼ 0.411 (ns) 0.397 0.748IL-1b (pg/ml) 0.773 0.073 p¼ 0.002 0.629 0.916
Figure 3. ROC curve of TNF-a: cAIT versus control group(AUC¼ 0.691, p¼ 0.034, cut-off¼ 14.7 pg/ml, sensitivity: 54.5%, spe-cificity: 85%).
Figure 4. ROC curve of IL-1b: cAIT versus GD (AUC¼ 0.773,p¼ 0.002, cut-off¼ 1.7 pg/ml, sensitivity: 72.7%, specificity: 86.4%).
4 H. Mikos et al. Autoimmunity, Early Online: 1–7
Aut
oim
mun
ity D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ham
mas
at U
nive
rsity
on
10/0
8/14
For
pers
onal
use
onl
y.

cAIT and GD. Th1 cells are involved in inflammatory
reactions and cellular immune responses. The corresponding
cytokines promote cytotoxic reactions and inflammatory
processes, participating in the delayed hypersensitivity reac-
tion in the tissue. Th2 cytokines stimulate production of
antibodies and are involved in the humoral immune response,
promoting immune and allergic reactions. The prevalence of
either Th1 or Th2 cytokine secretion varies from one disease
to another and leads to a different immune response.
Cytokines secreted by both T-cell populations exhibit an
inhibitory effect on each other and can shift the balance of
the immune response toward Th1 or Th2 cells [10].
In the present study we examined levels of of Th1
cytokines: IL-1b, TNF-a and Th2 cytokine: IL-6 in the serum
of children diagnosed with cAIT manifesting with hypothy-
roidism and in the serum of children with GD presenting
hyperthyroidism – prior to the introduction of treatment in
both diseases. The highest concentration of IL-1b was found
in children with cAIT (median of 2.16 pg/ml) and the lowest
in the GD group (median of 1.39 pg/ml), whereas in the
control group the median level of IL-1b was 1.88 pg/ml. The
concentration of IL-1b was significantly different between the
groups of children with cAIT and GD (p50.01) and in cAIT
versus control (p50.05). There was no difference in IL-1blevels between the group of children with GD and control
group (p40.05). The results confirm the important role of IL-
1b in the hypothyroid phase of chronic autoimmune
thyroiditis rather than in the severe phase of GD in children.
There were no significant differences of TNF-a and IL-6
levels between the studied groups of children (p¼ 0.067 and
p¼ 0.48, respectively).
Nanba and Watanabe [11] investigated the proportion of
peripheral Th1, Th2 and Th17 cells in patients with AITD.
The proportion of peripheral Th1 cells was higher in patients
with severe HT than in patients with mild HT (p50.05) and
the proportion of peripheral Th2 cells was lower in patients
with severe HT than in patients with mild HT (p50.001).
Therefore, the Th1/Th2 ratio was higher in severe HT in
comparison with mild HT (p50.001). The proportion of
peripheral Th17 cells in patients with AITD was higher than
in control subjects, and the proportion of these cells in
patients with intractable GD was higher than in patients with
GD in remission (p50.05). The authors concluded that the
peripheral Th1/Th2 cell ratio is related to the severity of HT,
and the proportion of Th17 cells is related to the intractability
of GD. They hypothesize that these patterns of peripheral Th
cell subsets may be expressed within the thyroid.
Rebuffat et al. [12] studied the effect of proinflammatory
cytokines IL-1b and TNF-a on the integrity of the epithe-
lium of thyrocytes in autoimmune thyroid diseases.
These cytokines stimulate secretion of IL-6 which may
modify epithelial integrity, transmembrane protein expression
and cell adhesion. High expression of these proteins in thyroid
follicular cells has been demonstrated in GD, in contrast to
the decreased expression of JAM-A and ZO-1 junction
proteins in cells derived from the thyroid gland of patients
suffering from HT. This is confirmed by the loss of the
integrity of the thyroid follicular cells, occurring as a result of
inflammatory processes in HT and apoptosis. It has been
shown that IL-1b modifies thyroid epithelial tightness –
altering the expression and localization of Claudin and ZO-1.
This confirms the important pathogenic role of IL-1b in
thyroid autoimmunity [1].
Our study confirmed a significant positive correlation of
IL-1b and TNF-a (r¼ 0.46, p50.05) in children with cAIT,
whereas in the control group the significant correlation of
IL-1b and TNF-a was negative (r¼ 0.58, p50.01). Both
elevated levels of IL-1b and a positive correlation profile
confirms the inflammatory nature of HT in children. ROC
analysis showed that IL-1b may aid in differentiation between
healthy children and patients with hypothyroidism in cAIT
(AUC¼ 0.77, p¼ 0.003) with low sensitivity (59.1%) but
very high specificity (95%) at a cut-off point of 2.1 pg/ml.
Thus, concentrations of IL-b below the cut-off point of 2.1 pg/
ml enable exclusion of cAIT in a given patient with high
probability. The ROC curve of cAIT versus GD for IL-1bshowed high sensitivity (72.7%) and high specificity (86.4%)
which demonstrates a similar ability to differentiate these
groups (AUC¼ 0.773, p¼ 0.002) at a lower cut-off point of
1.7 pg/ml compared to a ROC curve of cAIT versus control
(2.1 pg/ml). This result confirms that the serum level of IL-1bmay be an effective marker for hypothyroidism in chronic
autoimmune thyroiditis.
The presence of TNF-a in the serum of patients with
autoimmune thyroid disease may be an important stimulus for
the production of IL-6. Studies were conducted on the
cytokine profile of TNF-a and IL-6 in the serum of patients
with adult AITD in hypothyroidism and hyperthyroidism
before and after normalization of thyroid function [13]. The
data in the literature confirm the elevated levels of IL-6
and TNF-a observed in hyperthyroidism of Graves’ disease
[14–18] as well as in TAO [19].
Trials made by Pichler et al. [20] on 39 patients with newly
diagnosed Graves’ disease showed a higher IL-6 level only in
four cases compared to healthy controls.
Kiziltunc et al. [21] investigated a group of 27 adult
patients between 58 and 64 years of age with untreated
hyperthyroidism and 23 with untreated hypothyroidism. The
average concentrations of cytokines TNF-a and IL-6 were
comparable to a group of 18 healthy subjects. The concen-
tration of both cytokines was higher in patients with GD and
lower in patients with HT, compared to the control group
(p50.001). After treatment, the levels of cytokines TNF-aand IL-6 decreased in patients with GD (p50.01), but
increased in the group with HT (p50.05). In a similar study,
Akalin et al. [22] reported elevated levels of IL-6 in patients
with hyperthyroidism in the course of GD. The results of
these studies suggest that IL-6 may modulate the function of
the thyroid cells, because it plays an important role in B cell
differentiation and T cell activation. The release of IL-6 by
Table 5. Area under the curve: GD versus control group.
Asymptotic 95%confidence interval
Variable AreaStandard
errorAsymptoticsignificance
Lowerbound
Upperbound
IL-6 (pg/ml) 0.570 0.091 p¼ 0.435 (ns) 0.392 0.749TNF-a (pg/ml) 0.652 0.085 p¼ 0.092 (ns) 0.485 0.820IL-1b (pg/ml) 0.523 0.094 p¼ 0.801 (ns) 0.338 0.707
DOI: 10.3109/08916934.2014.914175 IL-1�, TNF-� and IL-6 in AITD in children 5
Aut
oim
mun
ity D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ham
mas
at U
nive
rsity
on
10/0
8/14
For
pers
onal
use
onl
y.

thyrocytes may increase the intrathyroidal immune response
in Graves’ disease.
In the present study we found a positive correlation of IL-6
and TNF-a in hyperthyroidism (r¼ 0.62, p50.01). This
aspect has also been observed in the other authors’ studies
[21]. The increased TNF-a concentration is related to the
increasing serum IL-6 level in the hyperthyroid children.
Jiskra et al. [23] determined concentrations of cytokine
panel including sIL-2R, IFN-g, TNF-a, IL-10, CD30 and Bcl-
2 in 28 untreated patients with GD and 24 with HT, compared
to 15 healthy subjects, finding elevated TNF-a, IL-10, sIL-2R
in patients with GD compared to patients with HT and the
control group.
Diez et al. [13] studied 20 untreated patients with
hyperthyroidism and 20 with untreated hypothyroidism and
reported elevated levels of TNF-a and sTNFR-1 before
introducing treatment. After treatment of hyperthyroidism,
the authors achieved a significant reduction in TNF-a and
reduced levels of sTNFR-1, while L-thyroxine therapy in
patients with hypothyroidism did not bring changes in the
concentrations of both parameters. In another study, Aust
et al. [24] showed high levels of TNF-a mRNA in tissues of
patients with HT in contrast with low levels in patients with
GD, suggesting that thyroid cells derived from patients with
hypothyroidism may potentially release TNF-a.
The concentrations of TNF-a in our study did not differ
significantly between the studied groups. However, ROC
curve analysis showed that TNF-a may differentiate healthy
children and children with hypothyroidism (AUC¼ 0.691,
p¼ 0.034) with low sensitivity (54.5%) and high specificity
(85%) at a designated cut-off point of 14.7 pg/ml. Therefore,
TNF-a can be considered as a marker for hypothyroidism
in cAIT and its concentrations below a cut-off point of
14.7 pg/ml may be helpful in ruling-out cAIT in a given
patient. Moreover, children with hypothyroidism showed a
significant positive correlation between TNF-a and ATPO
(r¼ 0.54, p50.01). A similar correlation between ATPO and
secretion of cytokines TNF-a and IFN-g was presented in the
work of Karanikas et al. [25]. The hypothesis was recently
confirmed by demonstrating that ATPO antibodies may
promote thyroid peroxidase – dependent on the production
of cytokines, including IFN-g, TNF-a and IL-6 [26].
The role of cytokines in the pathogenesis of AITD is still
unclear, and the data in the literature on the clinical effects of
cytokines within the thyroid gland are controversial. To date,
only a few studies have demonstrated a relationship between
IL-6 and HT. In animal experiments, IL-6 plays a minor role
in the development of autoimmune thyroiditis [27]. In a recent
study, Rugerri et al. [28] found elevated levels of IL-6 in
patients with HT. Similar results were obtained by Sieminska
et al. [29]. The main findings of the study included
demonstration of high levels of IL-6 in the serum of patients
with HT, suggesting that IL-6 is involved in the development
of the disease in postmenopausal women.
In our study, no significant difference in IL-6 concentra-
tions between groups was found, which may indicate that IL-6
does not play a significant pathological role in the group of
young patients with AITD. Nonetheless, further studies are
needed to clarify this issue and to determine the potential
implications of serum IL-6 for diagnosis of AITD in children.
In conclusion, we demonstrated increased IL-1b levels in
children with cAIT. Our findings indicate that both IL-1b and
TNF-a in serum could be used as markers for differentiation
of children with cAIT from healthy children. Moreover,
significantly higher concentrations of IL-1b in children with
hypothyroidism may be used to distinguish between children
with cAIT and GD. Our results suggest that serum assays of
selected cytokines: IL-1b and TNF-a may provide valuable
clinical information relevant for the diagnosis and follow-up
of AITD in children.
Declaration of interest
The authors state that they have no conflicts of interest.
The study was funded from the research grant of the
Department (UM 502-01-01104118-06037).
References
1. Rasmussen, A. K., K. Bendtzen, and U. Feldt-Rasmussen. 2000.Thyrocyte-interleukin-1 interactions. Exp. Clin. Endocrinol.Diabetes. 108: 67–71.
2. Shi, Y., H. Wang, Z. Su, et al. 2010. Differentiation imbalance ofTh1/Th17 in peripheral blood mononuclear cells might contributeto pathogenesis of Hashimoto’s thyroiditis. Scand. J. Immunol. 72:250–255.
3. Bossowski, A., M. Moniuszko, M. Dabrowska, et al. 2013. Lowerproportions of CD4+CD25(high) and CD4+FoxP3, but notCD4+CD25+CD127(low) FoxP3+ T cell levels in children withautoimmune thyroid diseases. Autoimmunity. 46: 222–230.
4. Klatka, M., E. Grywalska, M. Partyka, et al. 2014. Th17 and Tregcells in adolescents with Graves’ disease. Impact of treatment withmethimazole on these cell subsets. Autoimmunity. 47: 201–211.
5. Luu, V. P., M. I. Vazquez, and A. Zlotnik. 2014. B cells participatein tolerance and autoimmunity through cytokine production.Autoimmunity. 47: 1–12.
6. Peng, D., B. Xu, Y. Wang, et al. 2013. A high frequency ofcirculating th22 and th17 cells in patients with new onset Graves’disease. PLoS One. 8: e68446.
7. Gianoukakis, A. G., and T. J. Smith. 2004. The role of cytokines inthe pathogenesis of endocrine disease. Can. J. Diabetes. 28: 30–42.
8. Rasmussen, A. K. 2000. Cytokine actions on the thyroid gland.Dan. Med. Bull. 47: 94–114.
9. Palczewska, I., and Z. Niedzwiedzka. 2001. Somatic developmentindices in children and youth of Warsaw. Med. Wieku. Rozwoj. 5:18–118.
10. Phenekos, C., A. Vryonidou, A. D. Gritzapis, et al. 2004. Th1and Th2 serum cytokine profiles characterize patients withHashimoto’s thyroiditis (Th1) and Graves’ disease (Th2).Neuroimmunomodulation. 11: 209–213.
11. Nanba, T., M. Watanabe, N. Inoue, and Y. Iwatani. 2009. Increasesof the Th1/Th2 cell ratio in severe Hashimoto’s disease and in theproportion of Th17 cells in intractable Graves’ disease. Thyroid. 19:495–501.
12. Rebuffat, S. A., M. Kammoun-Krichen, I. Charfeddine, et al. 2013.IL-1beta and TSH disturb thyroid epithelium integrity in auto-immune thyroid diseases. Immunobiology. 218: 285–291.
13. Diez, J. J., A. Hernanz, S. Medina, et al. 2002. Serum concentra-tions of tumour necrosis factor-alpha (TNF-alpha) and solubleTNF-alpha receptor p55 in patients with hypothyroidism andhyperthyroidism before and after normalization of thyroid function.Clin. Endocrinol. (Oxf). 57: 515–521.
14. Pedro, A. B., J. H. Romaldini, and K. Takei. 2011. Changesof serum cytokines in hyperthyroid Graves’ disease patientsat diagnosis and during methimazole treatment.Neuroimmunomodulation. 18: 45–51.
15. Salvi, M., M. Pedrazzoni, G. Girasole, et al. 2000. Serumconcentrations of proinflammatory cytokines in Graves’ disease:effect of treatment, thyroid function, ophthalmopathy and cigarettesmoking. Eur. J. Endocrinol. 143: 197–202.
6 H. Mikos et al. Autoimmunity, Early Online: 1–7
Aut
oim
mun
ity D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ham
mas
at U
nive
rsity
on
10/0
8/14
For
pers
onal
use
onl
y.

16. Lakatos, P., J. Foldes, C. Horvath, et al. 1997. Serum interleukin-6and bone metabolism in patients with thyroid function disorders.J. Clin. Endocrinol. Metab. 82: 78–81.
17. Celik, I., S. Akalin, and T. Erbas. 1995. Serum levels of interleukin6 and tumor necrosis factor-alpha in hyperthyroid patients beforeand after propylthiouracil treatment. Eur. J. Endocrinol. 132:668–672.
18. Siddiqi, A., J. P. Monson, D. F. Wood, et al. 1999. Serum cytokinesin thyrotoxicosis. J. Clin. Endocrinol. Metab. 84: 435–439.
19. Wakelkamp, I. M., M. N. Gerding, J. W. Van Der Meer, et al.2000. Both Th1- and Th2-derived cytokines in serum areelevated in Graves’ ophthalmopathy. Clin. Exp. Immunol. 121:453–457.
20. Pichler, R., W. Maschek, M. Hatzl-Griesenhofer, et al. 2003.Soluble tumour necrosis factor-alpha receptor I and interleukin-6 asmarkers of activity in thyrotoxic Graves’ disease. Horm. Metab.Res. 35: 427–433.
21. Kiziltunc, A., M. Basoglu, B. Avci, and I. Capoglu. 1999. SerumIL-6 and TNF-a in patients with thyroid disorders. Turk. J. Med.Sci. 29: 25–30.
22. Akalin, A., O. Colak, O. Alatas, and B. Efe. 2002. Boneremodelling markers and serum cytokines in patients with hyper-thyroidism. Clin. Endocrinol. (Oxf). 57: 125–129.
23. Jiskra, J., M. Antosova, Z. Limanova, et al. 2009. The relationshipbetween thyroid function, serum monokine induced by interferon
gamma and soluble interleukin-2 receptor in thyroid autoimmunediseases. Clin. Exp. Immunol. 156: 211–216.
24. Aust, G., and W. A. Scherbaum. 1996. Expression of cytokines inthe thyroid: thyrocytes as potential cytokine producers. Exp. Clin.Endocrinol. Diabetes. 104: 64–67.
25. Karanikas, G., M. Schuetz, K. Wahl, et al. 2005. Relation of anti-TPO autoantibody titre and T-lymphocyte cytokine productionpatterns in Hashimoto’s thyroiditis. Clin. Endocrinol. (Oxf). 63:191–196.
26. Nielsen, C. H., T. H. Brix, R. G. Leslie, and L. Hegedus. 2009. Arole for autoantibodies in enhancement of pro-inflammatorycytokine responses to a self-antigen, thyroid peroxidase. Clin.Immunol. 133: 218–227.
27. Mori, K., K. Yoshida, M. Mihara, et al. 2009. Effects of interleukin-6 blockade on the development of autoimmune thyroiditis innonobese diabetic mice. Autoimmunity. 42: 228–234.
28. Ruggeri, R. M., S. Sciacchitano, A. Vitale, et al. 2009. Serumhepatocyte growth factor is increased in Hashimoto’s thyroiditiswhether or not it is associated with nodular goiter as compared withhealthy non-goitrous individuals. J. Endocrinol. Invest. 32:465–469.
29. Sieminska, L., C. Wojciechowska, B. Kos-Kudla, et al. 2010.Serum concentrations of leptin, adiponectin, and interleukin-6 inpostmenopausal women with Hashimoto’s thyroiditis. Endokrynol.Pol. 61: 112–116.
DOI: 10.3109/08916934.2014.914175 IL-1�, TNF-� and IL-6 in AITD in children 7
Aut
oim
mun
ity D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ham
mas
at U
nive
rsity
on
10/0
8/14
For
pers
onal
use
onl
y.