
IgG4 Syndrome - rheumatology.gr · IgG4 Syndrome Γ.Ε ... Pathophysiology Is it an autoimmune ......
27
IgG4 Syndrome Γ.Ε. Φραγκούλης, MD Μέτσοβο, Ιανουάριος 2010 Παθολογική Φυσιολογία Ιατρική Σχολή Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών
-
Upload
trinhkhuong -
Category
Documents
-
view
238 -
download
4
Transcript of IgG4 Syndrome - rheumatology.gr · IgG4 Syndrome Γ.Ε ... Pathophysiology Is it an autoimmune ......
IgG4 Syndrome
Γ.Ε. Φραγκούλης, MD
Μέτσοβο, Ιανουάριος 2010Παθολογική Φυσιολογία
Ιατρική Σχολή
Εθνικό & Καποδιστριακό Πανεπιστήμιο
Αθηνών
Outline
Definitions
Pathophysiology
Clinical manifestations
Treatment
Conclusions
Definitions
Firstly described: 2001 in a patient with autoimmune pancreatitis
Other names “IgG4-related systemic sclerosing disease”
“IgG4-related autoimmune disease”
“IgG4-related systemic disease”
“IgG4-positive multiorgan lymphoproliferative
syndrome”
N Engl J Med. 2001 Mar
Definitions
Tissue
Infiltrates by IgG4 (+) plasmatocytes
Fibrosis
Serum
IgG4
> 135 or 140 mg/dl
Not disease activity marker
Response to Glucocorticosteroids
Not always high
Pathophysiology
Is it an autoimmune
condition ? Correlation with
HLA DRB1*0405
HLA DQB1*0401
Immuner-complexes
deposition in tissues
Possible autoantigens
Allergic reaction?
Τh2 cytokines
From PBMCs
In tissues
IgE
Allergies
Ota et al, Immunogenetics 2007Zen et al. Hepatology 2007Bateman et al Histopathology 2009
Pathophysiology
Potential autoantigens Antibodies against
Lactoferin (73% of AIP patients)
CA I, II and IV (50%)
Pancreatic Secretory Trypsin Inhibitor (35%)
Plasminogen binding protein of H. pylori (90%)
Their role is debatable…

Pathophysiology
Role of T regulatory cells (Tregs) In tissues and in peripheral blood
IL-10 and TGF-b αριθμός Tregs
IgG4 antibodies Τh2 cytokines, Tregs, IL-10
Differentiation of B lymphocytes into IgG4 plasmatocytes IgG4 antibodies in other diseases
multicentric Castleman’s disease idiopathic plasmacytic lympadenopathy, Wegener’s granulomatosis, Pemphigus vulgaris Pemphigus foliaceus
Jeannin et al. Blood 1998
Clinical manifestations
Pancreatitis
Sclerosing Cholangitis
Sclerosing Sialadenitis
Tubulointerstitial nephritis
Riedel or Hashimoto’s
thyroiditis (?)
Lymphadenopathy
Retroperitoneal fibrosis
Hypophisitis
Mastitis
Prostatitis
Lung involvement
Skin involvement
Autoimmune pancreatitis
The most common clinical manifestation Usually accompanied with extrapancreatic manifestations US/CT
Diffuse or segmental enlargement of pancreas (sausage like appearance)
Hypoechogenic with hyperehcogenic spots Pseudocysts and calcifications are rare
ERCP Usually diffuse narrowing of pancreatic duct
Kamisawa et al. Am. J. Gastroenterol, 2001
Zhang et al. Mod Pathol, 2007
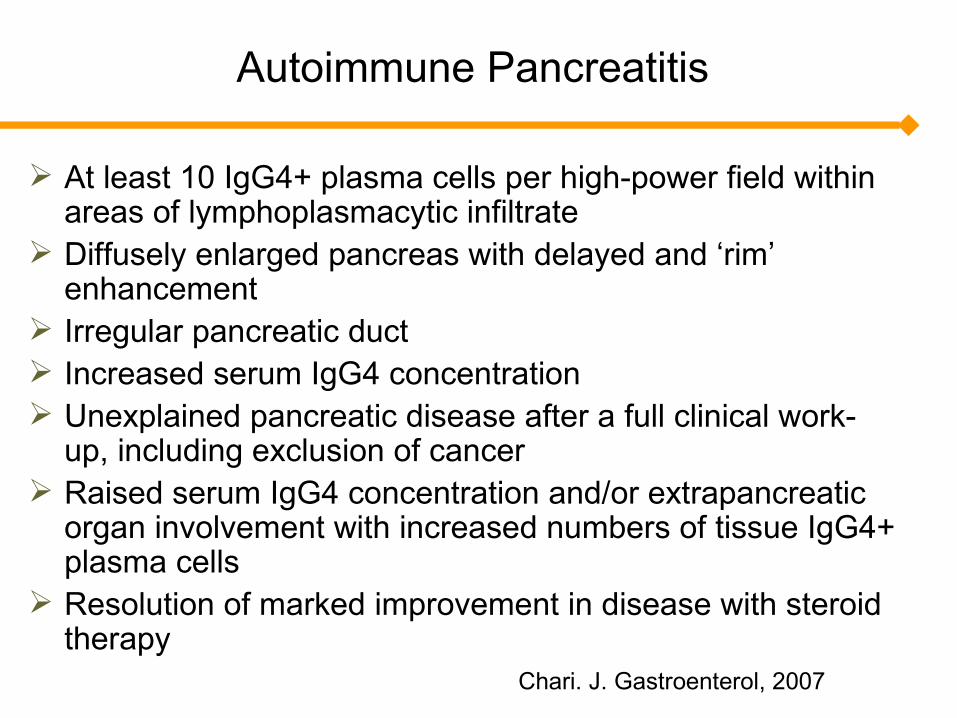
Autoimmune Pancreatitis
At least 10 IgG4+ plasma cells per high-power field within areas of lymphoplasmacytic infiltrate
Diffusely enlarged pancreas with delayed and ‘rim’ enhancement
Irregular pancreatic duct Increased serum IgG4 concentration Unexplained pancreatic disease after a full clinical work-
up, including exclusion of cancer Raised serum IgG4 concentration and/or extrapancreatic
organ involvement with increased numbers of tissue IgG4+ plasma cells
Resolution of marked improvement in disease with steroid therapy
Chari. J. Gastroenterol, 2007
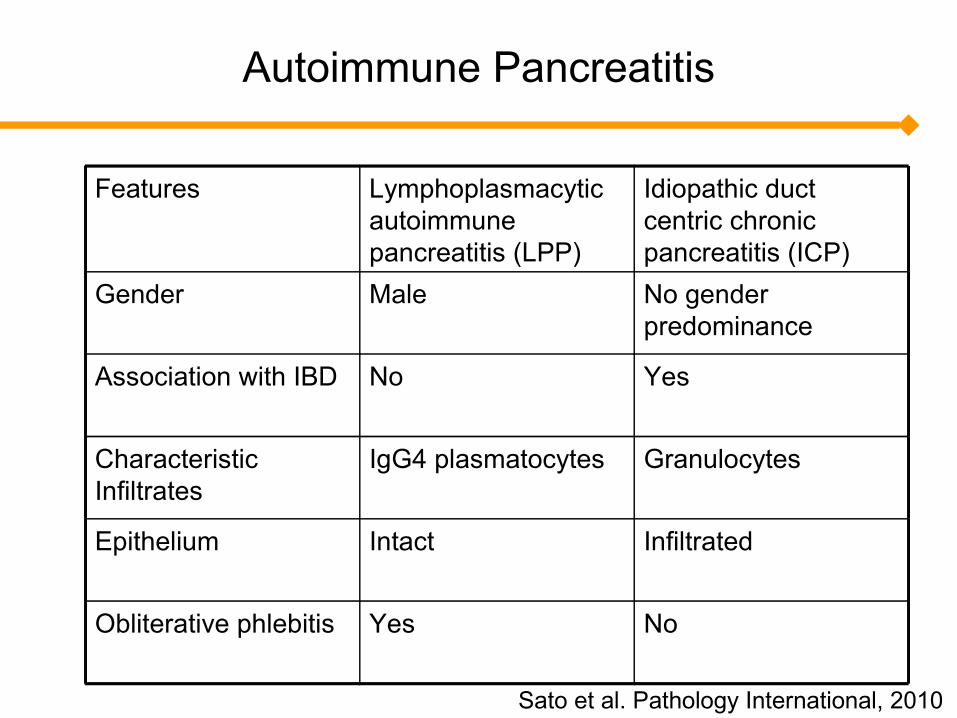
Autoimmune Pancreatitis
Features Lymphoplasmacytic autoimmune pancreatitis (LPP)
Idiopathic duct centric chronic pancreatitis (ICP)
Gender Male No gender predominance
Association with IBD No Yes
Characteristic Infiltrates
IgG4 plasmatocytes Granulocytes
Epithelium Intact Infiltrated
Obliterative phlebitis Yes No
Sato et al. Pathology International, 2010
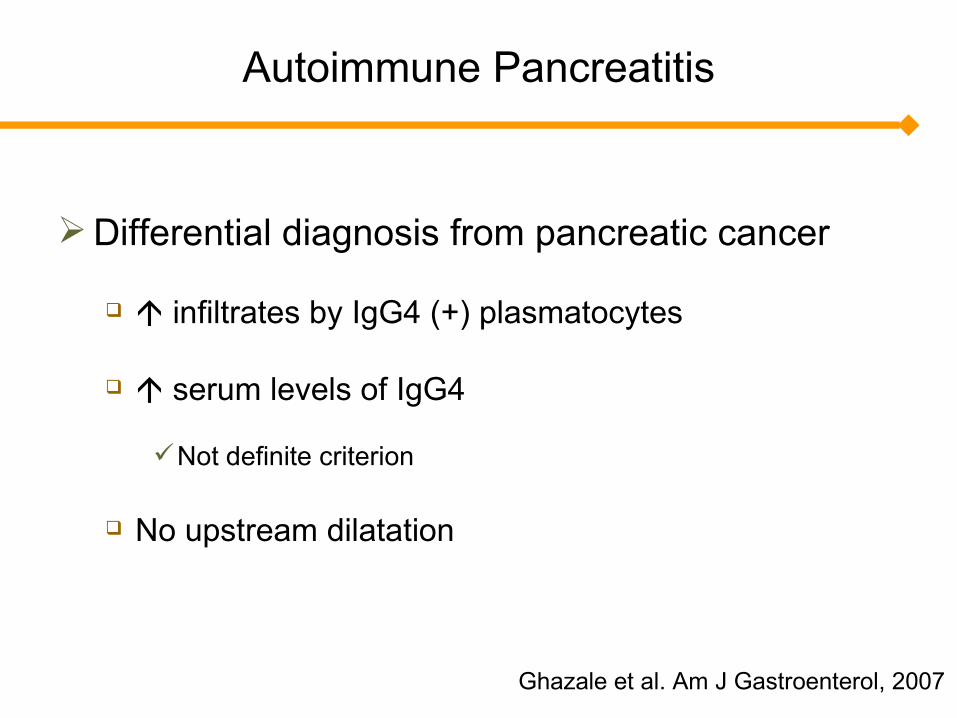
Autoimmune Pancreatitis
Differential diagnosis from pancreatic cancer
infiltrates by IgG4 (+) plasmatocytes
serum levels of IgG4
Not definite criterion
No upstream dilatation
Ghazale et al. Am J Gastroenterol, 2007
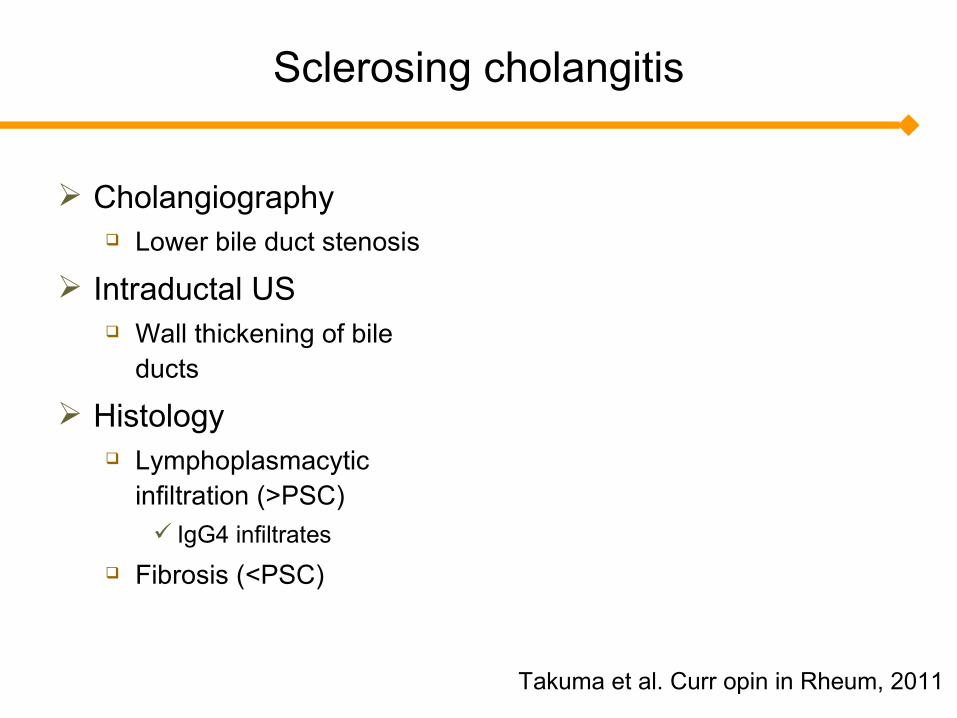
Sclerosing cholangitis
Cholangiography Lower bile duct stenosis
Intraductal US Wall thickening of bile
ducts
Histology Lymphoplasmacytic
infiltration (>PSC) IgG4 infiltrates
Fibrosis (<PSC)
Takuma et al. Curr opin in Rheum, 2011
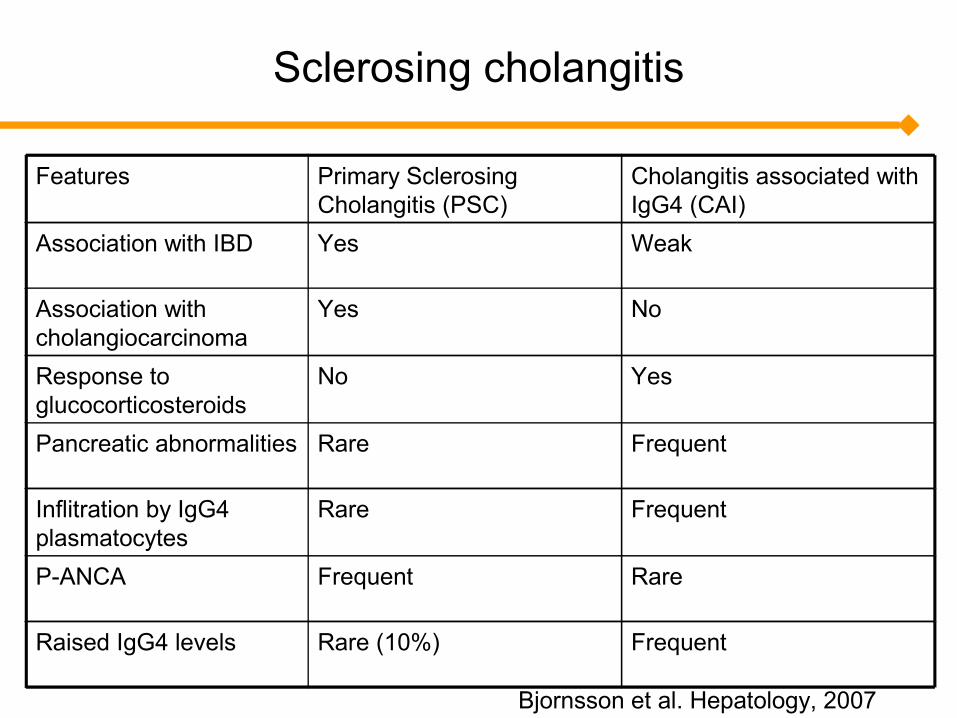
Sclerosing cholangitis
Features Primary Sclerosing Cholangitis (PSC)
Cholangitis associated with IgG4 (CAI)
Association with IBD Yes Weak
Association with cholangiocarcinoma
Yes No
Response to glucocorticosteroids
No Yes
Pancreatic abnormalities Rare Frequent
Inflitration by IgG4 plasmatocytes
Rare Frequent
P-ANCA Frequent Rare
Raised IgG4 levels Rare (10%) Frequent
Bjornsson et al. Hepatology, 2007
Salivary Gland Enlargement
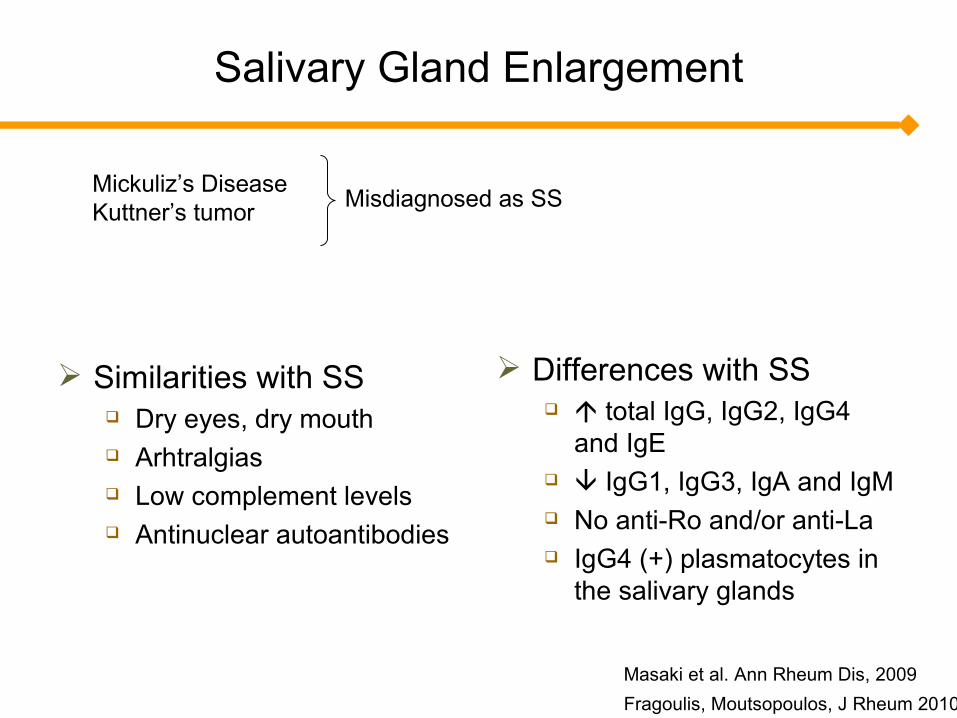
Similarities with SS Dry eyes, dry mouth Arhtralgias Low complement levels Antinuclear autoantibodies
Differences with SS total IgG, IgG2, IgG4
and IgE IgG1, IgG3, IgA and IgM No anti-Ro and/or anti-La IgG4 (+) plasmatocytes in
the salivary glands
Misdiagnosed as SS
Masaki et al. Ann Rheum Dis, 2009Fragoulis, Moutsopoulos, J Rheum 2010
Mickuliz’s DiseaseKuttner’s tumor
Salivary Gland Enlargement
Histological Differences with SS Large lymphoid follicles Germinal centers Obliterative plebitis Interlobular fibrosis
Geyer et al. Curr Opin Rheum, 2011
Lymphadenopathy
Lymph nodes Regional or distal Size: 1-5 cm (usually 2cm) 3 histological types have been recognized but all of
them> 60% of infiltrating plasma cells are IgG4 (+) in the majority eosinophilic infiltration
In these patients ESR, IgG, IgE and IL-2r IL-6, CRP No B symptoms
Sato et al. Mod Pathol, 2009
Lymphomas
Only few NHLs have been described till nowMost of them
MALT type Various organs (not necessarily in that infiltrated by
IgG4 (+) plasmatocytes One case of IgG4 producing MZ lymphoma in the
lymph node
Takahashi et al. Pancreas, 2009
Tubulointerstitial nephritis
Few cases of renal involvement Tubulointerstitial nephritis
(mainly) Some cases of IgG4-
related nodular lesions DD from renal cell
carcinoma
Murashima et al. Am J Kidney Dis, 2007
Skin
Erythematous papules or plaques Face/head/scalp SC lymphoplasmacytic infiltrate
IgG4 Eosinophils Histiocytes
Follicle formation Stromal fibrosis
Cheuk et al. Am J Surg Pathol 2009
Hashimoto’s Thyroiditis
In a large scale study 27% of Hashimoto thyroiditis
patients identified as IgG4 thyroiditis based on > 20 IgG4 plasmatocytes / HPF IgG4/IgG ratio > 30% Higher grades of lymphoplasmacytic
proliferation Stromal fibrosis Follicular cells degeneration High IgG4 serum levels
IgG4 thyroiditis Higher titers of anti-TPO & anti-TG
compared to non-IgG4 thyroiditis Diffuse low echogenicity
Li et al. Curr Opin in Rheum, 2011
Riedel thyroiditis
Riedel thyroiditis
Few cases have been described
Difficult differential diagnosis from fibrous variant of
Hashimoto’s thyroiditis
IgG4 related inflammatory abdominal aneurysm
IgG4 IAAA 50% of total IAAA 5% of total AAAs
Characteristics Similar clinicopathological with IgG4 disease (allergies, IgE,
IgG4 levels etc) Less rupture than non IgG4 No difference in diameter or location Histological
Eosinohpils Obliterative phlebitis Perineural infiltration Lyphoid follicle formation IgG4 plasmatocytes
Kamisawa et al. Curr Opin in Rheum, 2011
Thoracic aortic aneurysms and other atreries
Some cases and only few studies
9% of nonifectious aoritis may be IgG4 related
Mesenteric and right coronary arteries has been
found to be involved
Matsumoto et al Hum Pathol, 2008
Treatment
GC: 30-40 mg qd for 4w tapering by 5mg every 1-2 w for 1-2 mo 2.5-5mg qd for 3y
IgG4 levelsnormalization of liver function tests resolution of the strictures
less effective in the later stages fibrosis & atrophy
some cases improve without any treatment while others relapse after tapering the GCs
32% after 6mo, 56% after 12mo, 96% after 3yRetreat with high GCs.
Erkelens et al. Lancet, 1999Ghazale et al. Curr. Gastroenterol Repr, 2008

Treatment
AZA: 2-2.5mg/kg/day
MMF: 750mg twice daily
In GC refractory cases
RTX only small studies have been published
Ghazale et al. Gastroenterolgy, 2008
Ghazale et al Gut, 2007
Conclusions
Is it an autoimmune disorder ?
Is this a real entity or disease subgroups ?
Genetic make-up?
Prevalence among racial or ethnic groups?















![Exploring the Involvement of NLRP3 and IL-1β in …downloads.hindawi.com/journals/mi/2019/2363460.pdfhand osteoarthritis [26] were recruited in the Rheumatol-ogy Unit of Siena Hospital](https://static.fdocument.org/doc/165x107/5f93c90a1258491ec9221a4a/exploring-the-involvement-of-nlrp3-and-il-1-in-hand-osteoarthritis-26-were-recruited.jpg)

