Small Bowel Obstruction in Pregnancy A case report and review of the literature
1
A 29 year old primigravida presented at 31 weeks of gestation with severe epigastric pain, nausea and lack of appetite. She reported no vomiting or obstipation. She never had similar symptoms in the past. She had undergone sigmoid colectomy for volvulus 18 years ago and an appendicectomy a couple of years previously. On clinical examination, she was apyrexial and had a normal blood pressure. She had mild epigastric tenderness with no abdominal guarding or rigidity. Her obstetric examination was normal. She was reviewed by a general surgeon on admission, who suspected faecal impaction and gave her a trial with laxatives to which she responded. Her urine examination, blood investigations and ECG revealed no obvious abnormality. She had an abdominal ultrasound scan which showed no intra-abdominal pathology. She was managed conservatively with fluid support, analgesia, thromboprophylaxis and given prophylactic steroids for fetal lung maturation. She had vomiting on day 2, which was treated with anti-emetic and omeprazole. On day 3, the patient developed feculent vomiting and had to have continuous nasogastric aspiration for suspected bowel obstruction due to adhesions. She then improved and her pain settled. Later she became unwell once again, when the oral intake was commenced. A repeat ultrasound scan on day 5 revealed multiple dilated loops of bowel, highly suggestive of a small bowel obstruction (figure 1). At this stage, a joint decision was made with the surgeons for an emergency laparotomy. At laparotomy, she had an uneventful caesarean section to facilitate access to the bowel. The preterm baby was transferred to the special care baby unit in good condition. Intraoperative findings included multiple dilated loops of small bowel with bands of adhesions around proximal and mid-ileum causing complete obstruction. During adhesiolysis, she had an ileal perforation which was then repaired. She had a stormy and protracted post-operative course which required high dependency care. She developed multiple pulmonary emboli postoperatively and received therapeutic anticoagulation. She had a wound dehiscence on day 10 of her surgery, which was treated M Andrikopoulou 1 , A N Sridhar 1 , S Nausheen 2 1.Foundation Year 2; 2. Consultant Obstetrician and Gynaecologist, Macclesfield District General Hospital The incidence of acute abdomen during pregnancy is 1 in 500–635 pregnancies (1) . Small bowel obstruction accounts for around 15% of the cases (2) with an incidence of 1:17,000 pregnancies (3) Predisposing conditions include previous abdominal surgery resulting in adhesions such as following a gastric bypass, previous ruptured uterus, enlarged uterus (4) as in multiple pregnancies and co-existent fibroids; also hernia and appendicitis. Clinical diagnosis can be difficult; hence any abdominal pain accompanied by nausea and vomiting in the mid and last trimester of pregnancy should alert the clinician to the possibility of bowel obstruction in differential diagnosis. Ultrasound is ideal for initial evaluation but further plain films or MRI may help to confirm the diagnosis in equivocal cases (5) . A repeat ultrasound could be helpful in clinching the diagnosis, as shown in our patient, however, in hindsight, this could have been done earlier since there is no risk of radiation to the fetus as observed with X-rays. Prompt diagnosis and early surgical management is the cornerstone for a good outcome. Supportive management has a role only whilst awaiting definitive surgical intervention as it would otherwise cause unnecessary delay, which could be detrimental for both the mother and the fetus. Our case highlights a rare and potentially serious entity of small bowel obstruction during the last trimester of pregnancy, when the diagnosis is not straightforward as the bowel is pushed up due to gravid uterus. However, an early recourse to active management, including better imaging in selected situations should be considered in symptomatic women with previous surgery in order to optimize the outcome for the mother and the baby, thereby avoiding morbidity with its sequelae. 2. Case History 4. Discussion References Small bowel obstruction is rare during pregnancy. Diagnosis is challenging as the clinical picture may mimic pregnancy symptoms. It is often associated with high maternal and fetal morbidity and occasionally mortality due to delay in diagnosis. Here we illustrate a case of small bowel obstruction complicating pregnancy which we encountered in our unit. 1. Long SS et al - Imaging strategies for right lower quadrant pain in pregnancy. Am J Roentgenol 2011;196:4–12 2. Unal A et al - Acute abdomen in pregnancy requiring surgical management: a 20-case series. Eur J Obstet Gynecol Reprod Biol. 2011 Nov;159(1):87-90 3. Myerson S et al - Small bowel obstruction in pregnancy. Am J Gastroenterol 1995;90(2):299–302. 4. Ludmir J et al - Spontaneous small bowel obstruction associated with a spontaneous triplet gestation. A case report. J Reprod Med. 1989 Dec;34(12):985-7. 5. (2010) Suspected small-bowel obstruction. American College of Radiology Appropriateness Criteria. Figure 1. Ultrasound scan of the abdomen demonstrating dilated small bowel loops on day 5. 3. Management 1. Background
description
Small Bowel Obstruction in Pregnancy A case report and review of the literature. M Andrikopoulou 1 , A N Sridhar 1 , S Nausheen 2 Foundation Year 2; 2 . Consultant Obstetrician and Gynaecologist , Macclesfield District General Hospital. 4. Discussion . References . - PowerPoint PPT Presentation
Transcript of Small Bowel Obstruction in Pregnancy A case report and review of the literature

A 29 year old primigravida presented at 31 weeks of gestation with severe epigastric pain, nausea and lack of appetite. She reported no vomiting or obstipation. She never had similar symptoms in the past. She had undergone sigmoid colectomy for volvulus 18 years ago and an appendicectomy a couple of years previously. On clinical examination, she was apyrexial and had a normal blood pressure. She had mild epigastric tenderness with no abdominal guarding or rigidity. Her obstetric examination was normal.
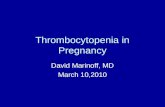
She was reviewed by a general surgeon on admission, who suspected faecal impaction and gave her a trial with laxatives to which she responded. Her urine examination, blood investigations and ECG revealed no obvious abnormality. She had an abdominal ultrasound scan which showed no intra-abdominal pathology. She was managed conservatively with fluid support, analgesia, thromboprophylaxis and given prophylactic steroids for fetal lung maturation. She had vomiting on day 2, which was treated with anti-emetic and omeprazole. On day 3, the patient developed feculent vomiting and had to have continuous nasogastric aspiration for suspected bowel obstruction due to adhesions. She then improved and her pain settled. Later she became unwell once again, when the oral intake was commenced. A repeat ultrasound scan on day 5 revealed multiple dilated loops of bowel, highly suggestive of a small bowel obstruction (figure 1). At this stage, a joint decision was made with the surgeons for an emergency laparotomy.
At laparotomy, she had an uneventful caesarean section to facilitate access to the
bowel. The preterm baby was transferred to the special care baby unit in good condition. Intraoperative findings included multiple dilated loops of small bowel with bands of adhesions around proximal and mid-ileum causing complete obstruction. During adhesiolysis, she had an ileal perforation which was then repaired.
She had a stormy and protracted post-operative course which required high
dependency care. She developed multiple pulmonary emboli postoperatively and received therapeutic anticoagulation. She had a wound dehiscence on day 10 of her surgery, which was treated with vacuum assisted closure. Finally, she made a complete recovery and was discharged in a good condition, along with her baby.
M Andrikopoulou1, A N Sridhar 1, S Nausheen2
1. Foundation Year 2; 2. Consultant Obstetrician and Gynaecologist,
Macclesfield District General Hospital
The incidence of acute abdomen during pregnancy is 1 in 500–635 pregnancies (1).
Small bowel obstruction accounts for around 15% of the cases (2) with an incidence of
1:17,000 pregnancies(3)
Predisposing conditions include previous abdominal surgery resulting in adhesions such
as following a gastric bypass, previous ruptured uterus, enlarged uterus (4) as in multiple
pregnancies and co-existent fibroids; also hernia and appendicitis.
Clinical diagnosis can be difficult; hence any abdominal pain accompanied by nausea
and vomiting in the mid and last trimester of pregnancy should alert the clinician to the
possibility of bowel obstruction in differential diagnosis.
Ultrasound is ideal for initial evaluation but further plain films or MRI may help to confirm
the diagnosis in equivocal cases (5). A repeat ultrasound could be helpful in clinching the
diagnosis, as shown in our patient, however, in hindsight, this could have been done
earlier since there is no risk of radiation to the fetus as observed with X-rays.
Prompt diagnosis and early surgical management is the cornerstone for a good
outcome. Supportive management has a role only whilst awaiting definitive surgical
intervention as it would otherwise cause unnecessary delay, which could be detrimental
for both the mother and the fetus.
Our case highlights a rare and potentially serious entity of small bowel
obstruction during the last trimester of pregnancy, when the diagnosis is
not straightforward as the bowel is pushed up due to gravid uterus.
However, an early recourse to active management, including better imaging
in selected situations should be considered in symptomatic women with
previous surgery in order to optimize the outcome for the mother and the
baby, thereby avoiding morbidity with its sequelae.
2. Case History
4. Discussion
References
Small bowel obstruction is rare during pregnancy. Diagnosis is challenging as the
clinical picture may mimic pregnancy symptoms. It is often associated with high
maternal and fetal morbidity and occasionally mortality due to delay in diagnosis. Here
we illustrate a case of small bowel obstruction complicating pregnancy which we
encountered in our unit.
1. Long SS et al - Imaging strategies for right lower quadrant pain in pregnancy. Am J Roentgenol 2011;196:4–12
2. Unal A et al - Acute abdomen in pregnancy requiring surgical management: a 20-case series. Eur J Obstet Gynecol Reprod Biol. 2011 Nov;159(1):87-90
3. Myerson S et al - Small bowel obstruction in pregnancy. Am J Gastroenterol 1995;90(2):299–302.
4. Ludmir J et al - Spontaneous small bowel obstruction associated with a
spontaneous triplet gestation. A case report. J Reprod Med. 1989 Dec;34(12):985-7.
5. (2010) Suspected small-bowel obstruction. American College of Radiology Appropriateness Criteria.
Figure 1. Ultrasound scan of the abdomen
demonstrating dilated small bowel loops on
day 5.
3. Management
1. Background