Primary sclerosing cholangitis and bile acids
5
Correspondance. E-mail address: [email protected] (O. Chazouillères). © 2012 Elsevier Masson SAS. All rights reserved. Clinics and Research in Hepatology and Gastroenterology (2012) 36, S21—S25 Therapeutic approaches of hepatobiliary Therapeutic approaches of hepatobiliary disorders with ursodeoxycholic acid disorders with ursodeoxycholic acid and bile-acid derivatives and bile-acid derivatives Guest editor: L. Serfaty Guest editor: L. Serfaty Clinics and R d esearch in Hepatology and Gastroenterology SEPTEMBER 2012 Supplement 1 - Vol. 36 70364 Disponible en ligne sur www.sciencedirect.com Summary Primary sclerosing cholangitis (PSC) is a rare and complex chronic cholestatic liver di- sease, and its management is hindered by a very poor understanding of its pathogenesis. Endogenous bile acids are likely to play a role either directly or indirectly in the pathoge- nesis and/or progression of PSC (‘toxic-bile’hypothesis). At present, no medical therapies have been proven to delay disease progression. Ursodeoxycholic acid (UDCA) is the agent that has received the most attention. Based on large randomized studies, it appears that UDCA at doses from 13 to 23mg/kg/d has no proven beneÀt on survival, but is well tolerated and improves serum liver tests and surrogate markers of prognosis whereas, at higher doses (28–30mg/kg/d), it is associated with a worsened outcome. However, except at very high doses and despite the controversies, many hepatologists still consider UDCA a reasonable treatment choice. Indeed, its use at dosages of 15–20mg/kg/d has recently been approved for the treatment of PSC by the French National Health Authority. In ad- dition, 24- nor- ursodeoxycholic acid, a side-chain-modiÀed UDCA derivative, has shown promising results in animal models of PSC and is currently under investigation in humans. © 2012 Elsevier Masson SAS. All rights reserved. Primary sclerosing cholangitis and bile acids Olivier Chazouillères Service d’Hépatologie, Hôpital Saint-Antoine, AP-HP, 184, rue du Faubourg Saint Antoine, 75571 Paris Cedex 12, France ; UPMC Univ Paris 06, UMR_S 938, F-75012 Paris, France ; INSERM UMR_S 938, Centre de Recherche Saint-Antoine, F-75012 Paris, France Introduction Primary sclerosing cholangitis (PSC) is a rare and chronic cholestatic liver disease of unknown cause that is commonly associated with inÁammatory bowel disease (IBD) and cha- racterized by progressive obliterative Àbrosis of the biliary tree [1]. Although the natural course of PSC may vary from one patient to another, PSC is often progressive, leading to biliary cirrhosis and its complications. In addition, PSC is a condition harboring considerable neoplastic potential, with increased susceptibility for the development of both biliary and colon cancers. Overall, median survival ranges from 11 to 18 years. Guidelines for the management of PSC have recently been published by both the European Association for the Study of the Liver (EASL) [2] and the American Association for the Study of Liver Diseases (AASLD) [3]. At present, there is no medical treatment with proven efÀcacy, although ursodeoxycholic acid (UDCA) is commonly given to patients with PSC. PSC: general features Diagnosis The prevalence rate of PSC in Northern Europeans is around 10/100,000 population. PSC is diagnosed at all ages, but most often at around the age of 40 years. In contrast to the usual autoimmune conditions, there is a male preponde- rance (approximately 2/3). A large majority of PSC patients, 60% in France [4], have concomitant inÁammatory bowel disease (IBD), while other autoimmune conditions, most
Transcript of Primary sclerosing cholangitis and bile acids

Correspondance.E- mail address: [email protected] (O. Chazouillères).
© 2012 Elsevier Masson SAS. All rights reserved.
Clinics and Research in Hepatology and Gastroenterology (2012) 36, S21—S25
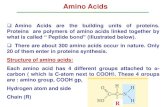
COOH
UDCA
H
OH
CH3
CH3
H3C
HO
H H
H
H COOH
CH3
CH3
H3C
OHHO
H
H
H
H
H
NorUDCA
COOHCH3
CH3
H3C
OHHO
H
H
H
H
H
6α-ECDCA
Therapeutic approaches of hepatobiliary Therapeutic approaches of hepatobiliary disorders with ursodeoxycholic aciddisorders with ursodeoxycholic acid
and bile-acid derivativesand bile-acid derivativesGuest editor: L. SerfatyGuest editor: L. Serfaty
C linics and Rd esearch in Hepatology
and Gastroenterology
SEPTEMBER
2012 Supplement 1 - Vol. 36
ISSN
221
0-74
01
7036
4
Disponible en ligne sur
www.sciencedirect.com
SummaryPrimary sclerosing cholangitis (PSC) is a rare and complex chronic cholestatic liver di-sease, and its management is hindered by a very poor understanding of its pathogenesis. Endogenous bile acids are likely to play a role either directly or indirectly in the pathoge-nesis and/or progression of PSC (‘toxic- bile’hypothesis). At present, no medical therapies have been proven to delay disease progression. Ursodeoxycholic acid (UDCA) is the agent that has received the most attention. Based on large randomized studies, it appears that UDCA at doses from 13 to 23mg/kg/d has no proven bene t on survival, but is well tolerated and improves serum liver tests and surrogate markers of prognosis whereas, at higher doses (28–30mg/kg/d), it is associated with a worsened outcome. However, except at very high doses and despite the controversies, many hepatologists still consider UDCA a reasonable treatment choice. Indeed, its use at dosages of 15–20mg/kg/d has recently been approved for the treatment of PSC by the French National Health Authority. In ad-dition, 24- nor- ursodeoxycholic acid, a side- chain- modi ed UDCA derivative, has shown promising results in animal models of PSC and is currently under investigation in humans.© 2012 Elsevier Masson SAS. All rights reserved.
Primary sclerosing cholangitis and bile acidsOlivier Chazouillères
Service d’Hépatologie, Hôpital Saint- Antoine, AP- HP, 184, rue du Faubourg Saint Antoine, 75571 Paris Cedex 12, France ; UPMC Univ Paris 06, UMR_S 938, F- 75012 Paris, France ; INSERM UMR_S 938, Centre de Recherche Saint- Antoine, F- 75012 Paris, France
Introduction
Primary sclerosing cholangitis (PSC) is a rare and chronic cholestatic liver disease of unknown cause that is commonly associated with in ammatory bowel disease (IBD) and cha-racterized by progressive obliterative brosis of the biliary tree [1]. Although the natural course of PSC may vary from one patient to another, PSC is often progressive, leading to biliary cirrhosis and its complications. In addition, PSC is a condition harboring considerable neoplastic potential, with increased susceptibility for the development of both biliary and colon cancers. Overall, median survival ranges from 11 to 18 years. Guidelines for the management of PSC have recently been published by both the European Association for the Study of the Liver (EASL) [2] and the American Association for the Study of Liver Diseases (AASLD) [3]. At
present, there is no medical treatment with proven ef cacy, although ursodeoxycholic acid (UDCA) is commonly given to patients with PSC.
PSC: general features
Diagnosis
The prevalence rate of PSC in Northern Europeans is around 10/100,000 population. PSC is diagnosed at all ages, but most often at around the age of 40 years. In contrast to the usual autoimmune conditions, there is a male preponde-rance (approximately 2/3). A large majority of PSC patients, 60% in France [4], have concomitant in ammatory bowel disease (IBD), while other autoimmune conditions, most
04-Chazoullieres.indd S21 25/09/2012 11:49:49

S22 O. Chazouillères
in advanced liver disease and in cases of severe recurrent cholangitis. It may also be considered in a highly selected group of patients with small CCA [6]. According to both the EASL and AASLD guidelines, dominant strictures with signi- cant cholestasis should be treated with balloon dilatation; however, as the long- term ef cacy of endoscopic treatment has yet to be proven, this application is presently performed based on individual patient assessments.
Development of effective medical therapy for PSC has been hindered by uncertainty as to its cause(s), the relative scarcity of PSC patients, the remarkable variability of its natural history and the fact that PSC may be a ‘mixed bag’ of disease entities. The agent that has received the most atten-tion is UDCA, but its precise role is still unclear (see below). A number of other drugs, including immunosuppressors ranging from corticosteroids to tumor necrosis factor (TNF)- alpha antagonists, anti brotics and other agents, have been tested in small randomized or pilot studies, but none has been shown to be ef cient in delaying disease progression in regular PSC patients. However, there is evidence to suggest that immunosuppressive therapy can bene t some patient subgroups and that corticosteroid treatment with or without adjuvant immunosuppressant therapy can be recommended in PSC patients with features of autoimmune hepatitis (as well as in those with IgG4- associated cholangitis) [2,3].
Bile acids and PSC pathogenesis
The pathogenesis of PSC remains largely unknown. Based on clinical features and experimental data, several hypotheses have been proposed, but it should be borne in mind that, because of the limited repertoire of the biliary tract in reacting to any insult, a number of pathogenetic mechanisms may result in a clinical picture of sclerosing cholangitis, so these hypotheses are not mutually exclu-sive [7]. There is strong evidence for genetic susceptibility, and PSC is likely to be caused by a complex interplay of multiple genetic variants and environmental factors. Besides various hypotheses (such as ‘autoimmunity’, ‘aberrant homing’, ‘leaky gut’and ‘ischemia’), several studies have elaborated on the toxic- bile hypothesis in PSC pathogenesis. As with any chronic cholestatic disease, accumulation of endogenous bile acids in affected segments of the liver may lead to liver cell injury, apoptosis, necrosis and brosis. However, more original and speci c to PSC is the hypothesis of bile- duct injury resulting from abnormal bile composi-tion. This hypothesis is based on the ndings of PSC- like changes in mice devoid of the canalicular transporter mdr2 (MDR3- ABCB4 in humans). This transporter mediates biliary excretion of phospholipids, which normally form mixed micelles with bile acids and cholesterol to protect biliary epithelium against the detergent properties of bile acids. Mdr2 knockout mice are unable to secrete phospholipids in bile and spontaneously develop bile- duct injury with macroscopic and microscopic features closely resembling human PSC [8]. However, no associations between ABCB4 variants and PSC have so far been reported [9], although its role in subgroups such as small- duct PSC or PSC with lithiasis cannot be excluded. Bile- acid toxicity towards biliary epithelium could also result from decreased biliary
often thyroid diseases and diabetes mellitus, are seen in up to 25% of cases. About 50% of patients are symptomatic at rst presentation, and typical symptoms include pruritus, jaundice, abdominal pain, and episodes of fever and chills. A diagnosis of PSC can be made in patients with biochemical cholestasis not otherwise explained when magnetic reso-nance cholangiopancreatography (MRCP) shows multifocal strictures and segmental dilatations, and when causes of secondary sclerosing cholangitis (especially IgG4- associated cholangitis) have been excluded. A number of autoantibo-dies have been described, but none are disease- speci c. A liver biopsy is not mandatory in typical cases, but should be performed when variant forms are suspected, particularly small- duct PSC (normal high- quality MRCP) and PSC with autoimmune features or ‘overlap syndrome’ (high tran-saminase levels, positive titers of autoantibodies and/or markedly elevated IgG levels) [2,3].
Disease course
Symptoms and liver tests may initially uctuate, with more steady progression only observed in advanced stages of cirrhosis. Several prognostic models, including clinical and biochemical parameters, have been developed. To what extent cholangiographic ndings may predict outcome, however, is disputed. Overall, it appears that these models are useful for predicting outcomes in patient cohorts, but cannot be used to reliably predict the outcome in any given patient [3].
Risk of hepatobiliary malignancies
Besides the usual risk of hepatocellular carcinoma in cir-rhotic patients, PSC is associated with an increased risk of biliary malignancies, particularly cholangiocarcinoma (CCA). Up to 50% of CCA are diagnosed within the rst year of diagnosis of PSC and, thereafter, the yearly incidence rate is 0.6–1.5%. Diagnosis of CCA in PSC is a challenge and there is currently no evidence- based biochemical marker or imaging modality that can be recommended for early detection of CCA, although current practices include annual testing for serum carbohydrate antigen 19- 9 [5]. Gallbladder carcinoma is seen in up to 2% of patients, and gallbladder polyps are associated with a substantial risk of malignancy. As a conse-quence, guidelines recommend annual non- invasive imaging follow- up and removal of any gallbladder lesions [2,3].
The risk of colorectal cancer or dysplasia in PSC patients with IBD is higher than that observed in patients with IBD alone. Colonoscopy with biopsy is therefore recommended in PSC patients with IBD at 1 – to 2- year intervals from the time of PSC diagnosis [2,3].
Management
Several therapeutic modalities (medical, endoscopic and surgical) have so far been investigated. Unfortunately, none except liver transplantation (LT) has been proven to signi cantly alter the course of the disease. LT is indicated
04-Chazoullieres.indd S22 25/09/2012 11:49:50

Primary sclerosis cholangitis and bile acids S23
population. The second study was the American multicenter study using doses of 28–30mg/kg/d in 150 PSC patients for 5 years [22]. However, this trial was terminated because of an enhanced risk in the UDCA group of reaching primary end-points such as liver transplantation and the development of varices despite overall biochemical improvement. Patients with the higher Mayo Clinic risk scores and more advanced histological stages at entry had poorer outcomes irrespective of their treatment group. Surprisingly, though, subsequent analysis showed that the increased risk of adverse outcomes in patients treated with UDCA was only apparent in patients with early- stage PSC [23]. The mechanism behind this unexpected detrimental effect of UDCA remains unclear, but the expansion and altered composition of the bile- acid pool may have been contributing factors, especially in patients with severe biliary obstruction [24]. Unfortunately, the results presented for the bile- acid changes in this study were far from clear and did not allow rm conclusions to be drawn [25].
The role of UDCA as a potential chemopreventive agent against colon carcinogenesis is speci cally addressed in this journal issue. Brie y, in PSC patients with IBD, a bene cial effects of UDCA on the risk of colorectal neoplasia have been determined from retrospective studies of patients treated with low- dose UDCA [26- 28], but not with UDCA at 18–23mg/kg/d [29]; and recently, an increased risk has even been described with the highest dosages (28- 30mg/ kg/d) [30]. However, it should be noted that all these studies were based on retrospective analyses with their inherent limitations and that prospective well- designed studies are lacking.
Evidence of a bene cial effect of UDCA on the risk of developing CCA is limited. Lack of UDCA treatment was an independent risk factor for developing CCA in a study of 255 PSC patients listed for liver transplantation [31], and there was a trend in some studies suggesting that PSC patients treated with UDCA may develop fewer CCA [4,16,32]. As CCA is a relatively rare event, further large and prolonged stu-dies are clearly needed to con rm this potential bene cial effect of UDCA.
From these data, it may be concluded that UDCA at 15- 20mg/kg/d is safe, and improves serum liver tests and surrogate markers of prognosis, but has no proven bene t on survival, whereas UDCA at 30mg/kg/d may be harmful. Moreover, the EASL and AASLD have provided different recommendations, thereby causing confusion in patients as well as in doctors. According to the EASL, “the limited data base does not yet allow a speci c recommendation for the general use of UDCA in PSC” [2]. In contrast, the authors of the AASLD guidelines “recommend against the use of UDCA in adult patients”, although surprisingly, this strong negative recommendation does not apply to pediatric patients [3]. So, the EASL guidelines allow for the possible use of UDCA, whereas the AASLD guidelines interpret its lack of ef cacy very (or perhaps too) strictly. Indeed, it should be remembered that the AASLD guidelines were devised through a less collective process than those of the EASL, and that the American opinion of UDCA in PSC was shifted somewhat suddenly from rather positive to strongly negative following the disappointing results of the very high- dose trial.
HCO3 – secretion (the so- called ‘HCO3 – umbrella’) [10]. The bile- salt- sensing receptor TGR5 plays a role in the complex regulation of HCO3 – secretion and, interestingly, TGR5 has been identi ed as a likely disease gene in a large genome- wide association study of PSC [11]. In addition, it has also been shown that bile acids control the antimicrobial peptide cathelicidin through nuclear receptors such as the Farnesoid X receptor (FXR) and vitamin D receptor (VDR) in human biliary epithelium [12]. Overall, bile acids are likely to play a role either directly or indirectly in the pathogenesis and/or progression of PSC, and the toxic- bile hypothesis points the way to new directions towards developing therapeutic strategies targeting bile toxicity via nuclear receptors regu-lating biliary phospholipid, bile acid and HCO3 – secretion.
Bile acids as therapeutic agents in PSC
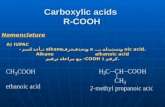
Ursodeoxycholic acid (UDCA)
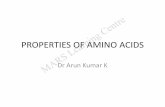
UDCA, a hydrophilic dihydroxy bile acid (see speci c paper in this issue), is an effective treatment of primary biliary cirrhosis (PBC) and has therefore been investigated as a potential candidate for the treatment of PSC. Small pilot trials using doses of 10–15mg/kg/d in the early 1990s demonstrated biochemical and, in some cases, histological improvement in PSC patients [13- 15]. A larger double- blind placebo- controlled study including 105 patients and using 13- 15mg/kg/d for 2 years con rmed improvements in serum liver tests, but not in symptoms, histological brosis or disease progression [16]. The study had some limitations (half the patients had extensive brosis or cirrhosis), and the results were profoundly disappointing to both patients and physicians. Subsequently, and on the grounds that larger doses might be necessary to provide suf cient enrichment of the bile pool in the context of cholestasis and that biliary enrichment of UDCA, a potential key factor for its clinical effect, increases with increasing dose [17], higher doses were then studied. A small well- designed placebo- controlled study (26 patients) using 20mg/kg/d for 2 years demonstra-ted improvement in histological brosis and even in cho-langiographic ndings, as well as the expected biochemical improvement [18]. Also encouraging were a small open- label trial using 25–30mg/kg/d showing signi cant improvement of predicted survival [19], and a 2- year dose- ranging pilot study of 30 patients in which the low (10mg/kg/d) and intermediate (20mg/kg/d) doses tended to improve, and the high dose (30mg/kg/d) signi cantly improved, the predicted survival [20].
However, two large placebo- controlled studies fell short of demonstrating improved transplant- free survival with intermediate and high UDCA doses [21,22]. The rst was a Scandinavian trial that recruited the largest group of PSC patients (n=219) for the longest treatment period (5 years) ever studied using doses of 17–23mg/kg/d [21]. Although a trend towards increased survival in the UDCA group was observed, the mortality rate was globally low and, despite the large number of patients, the trial was still insuf ciently powered to produce a statistically signi cant result. In addition, the unexpected poor biochemical response raised questions concerning adequate compliance among the study
04-Chazoullieres.indd S23 25/09/2012 11:49:50

S24 O. Chazouillères
Competing interests
The author has received research support from Aptalis and he has received compensation for providing consulting related to UDCA from Mayoly- Spindler.
References[1] Lee YM, Kaplan MM. Primary sclerosing cholangitis. N Engl J
Med 1995;332:924- 33.[2] European Association for the Study of the Liver. EASL Clinical
Practice Guidelines: management of cholestatic liver diseases. J Hepatol 2009;51:237- 67.
[3] Chapman R, Fevery J, Kalloo A, Nagorney DM, Boberg KM, Shneider B, et al. Diagnosis and management of primary sclerosing cholangitis. Hepatology 2010;51:660- 78.
[4] Garioud A, Seksik P, Chretien Y, Corpechot C, Poupon R, Poupon RE, et al. Characteristics and clinical course of primary sclerosing cholangitis in France: a prospective cohort study. Eur J Gastroenterol Hepatol 2010;22:842- 7.
[5] Razumilava N, Gores GJ, Lindor KD. Cancer surveillance in patients with primary sclerosing cholangitis. Hepatology 2011;54:1842- 52.
[6] Darwish Murad S, Kim WR, Harnois DM, Douglas DD, Burton J, Kulik LM, et al. Ef cacy of neoadjuvant chemoradiation, followed by liver transplantation, for perihilar cholangiocar-cinoma at 12 US centers. Gastroenterology 2012;143:88- 98.
[7] Karlsen TH, Schrumpf E, Boberg KM. Update on primary sclerosing cholangitis. Dig Liver Dis 2010;42:390- 400.
[8] Fickert P, Fuchsbichler A, Wagner M, Zollner G, Kaser A, Tilg H, et al. Regurgitation of bile acids from leaky bile ducts causes sclerosing cholangitis in Mdr2 (Abcb4) knockout mice. Gastroenterology 2004;127:261- 74.
[9] Rosmorduc O, Hermelin B, Boelle PY, Poupon RE, Poupon R, Chazouilleres O. ABCB4 gene mutations and primary sclerosing cholangitis. Gastroenterology 2004;126:1220- 2.
[10] Beuers U, Hohenester S, de Buy Wenniger LJ, Kremer AE, Jansen PL, Elferink RP. The biliary HCO(3)(- ) umbrella: a unifying hypothesis on pathogenetic and therapeutic aspects of brosing cholangiopathies. Hepatology 2010;52:1489- 96.
[11] Karlsen TH, Franke A, Melum E, Kaser A, Hov JR, Balschun T, et al. Genome- wide association analysis in primary sclerosing cholangitis. Gastroenterology 2010;138:1102- 11.
[12] D’Aldebert E, Biyeyeme Bi Mve MJ, Mergey M, Wendum D, Firrincieli D, Coilly A, et al. Bile salts control the antimicrobial peptide cathelicidin through nuclear receptors in the human biliary epithelium.
[13] Chazouillères O, Poupon R, Capron JP, Metman EH, Dhumeaux D, et al. Ursodeoxycholic acid for primary sclerosing cholan-gitis. J Hepatol 1990;11:120- 3.
[14] O’Brien CB, Senior JR, Arora- Mirchandani R, Batta AK, Salen G. Ursodeoxycholic acid for the treatment of primary sclerosing cholangitis: a 30- month pilot study. Hepatology 1991;14:838- 47.
[15] Beuers U, Spengler U, Kruis W, Aydemir U, Wiebecke B, Heldwein W, et al. Ursodeoxycholic acid for treatment of primary sclerosing cholangitis: a placebo- controlled trial. Hepatology 1992;16:707- 14.
[16] Lindor KD. Ursodiol for primary sclerosing cholangitis. Mayo Primary Sclerosing Cholangitis- Ursodeoxycholic Acid Study Group. N Engl J Med 1997;336:691- 5.
[17] Rost D, Rudolph G, Kloeters- Plachky P, Stiehl A. Effect of high- dose ursodeoxycholic acid on its biliary enrichment in primary sclerosing cholangitis. Hepatology 2004;40:693- 8.
[18] Mitchell SA, Bansi DS, Hunt N, Von Bergmann K, Fleming KA, Chapman RW. A preliminary trial of high- dose ursodeoxycholic
Since the release of these guidelines, two meta- analyses have been published based on eight randomized trials evaluating UDCA vs placebo or no intervention (567 patients) [33,34]. Unfortunately, these meta- analyses bring little to the table because of a high risk of bias. Durations of treatment (3 months to 6 years) and dosages (from 10 to 30mg/kg/d) were widely different and two of the studies had very poor- quality methodology. The Cochrane group concluded that there was not enough evidence to either support or refute the use of UDCA [33], and the London group found that neither standard nor “high- dose” (>15mg/kg/d) UDCA had any favourable in uence on the progression of PSC [34].
So, where do we stand with the use of UDCA in PSC? Clearly, UDCA is less effective in PSC than in PBC and the effect of UDCA on the survival of PSC patients is still unsett-led. However, for a number of European experts, this is not the time to « throw the Urso out with the bathwater » [35], and UDCA can still be used at low or intermediate doses. Also, a re- evaluation of doses of UDCA in better- selected patients and with the support of better surrogate markers of ef cacy has been suggested [35, 36]. In France, approval of UDCA for the treatment of PSC has recently been con rmed and a dose of 15–20mg/kg/d is recommended. At Saint- Antoine Hospital, our current policy is to use doses of around 20mg/kg/d except in patients with severe biliary stenosis (15mg/kg/d).
Other bile acids
24- norUrsodeoxycholic acid (24- norUDCA) is the C23 homo-log of UDCA with one fewer methylene group in its side chain. In experimental models, this side- chain structure determines unique physiological and pharmacological properties, including the ability to undergo cholehepatic shunting and to directly stimulate cholangiocyte secretion, both resulting in an HCO3- rich hypercholeresis [37]. When 24- norUDCA was used in Mdr2 knockout mice, sclerosing cholangitis improved dramatically [38]. The results of an ongoing phase- II clinical trial are now eagerly awaited and a large multicenter phase- III trial is likely to be planned soon.
The FXR agonist 6- ethyl- chenodeoxycholic acid, or obe-ticholic acid (see speci c paper in this issue), is also being evaluated for the treatment of PBC. However, at this time, there are as yet no reports of its effects in experimental models of sclerosing cholangitis and no planned clinical trials in PSC patients.
Conclusion
Despite new insights over the past few years, PSC remains a ‘black box’with many unresolved questions. Endogenous bile acids are likely to play a role either directly or indirectly in the pathogenesis and/or progression of PSC. Although the effect of UDCA on the survival of PSC patients is still unresolved and despite the controversies, at this time UDCA is still a reasonable treatment choice at doses not much higher than 20mg/kg/d. Another bile acid, 24- norUDCA, is currently under investigation and may prove to be a thera-peutic alternative in the future.
04-Chazoullieres.indd S24 25/09/2012 11:49:50

Primary sclerosis cholangitis and bile acids S25
with ulcerative colitis and primary sclerosing cholangitis. Gastroenterology 2003;124:889- 93.
[29] Lindstrom L, Boberg KM, Wikman O, Friis- Liby I, Hultcrantz R, Prytz H, et al. High dose ursodeoxycholic acid in primary sclerosing cholangitis does not prevent colorectal neoplasia. Aliment Pharmacol Ther 2012;35:451- 7.
[30] Eaton JE, Silveira MG, Pardi DS, Sinakos E, Kowdley KV, Luketic VA, et al. High- dose ursodeoxycholic acid is associated with the development of colorectal neoplasia in patients with ulcerative colitis and primary sclerosing cholangitis. Am J Gastroenterol 2011;106:1638- 45.
[31] Brandsaeter B, Isoniemi H, Broome U, Olausson M, Backman L, Hansen B, et al. Liver transplantation for primary sclerosing cholangitis; predictors and consequences of hepatobiliary malignancy. J Hepatol 2004;40:815- 22.
[32] Rudolph G, Kloeters- Plachky P, Rost D, Stiehl A. The incidence of cholangiocarcinoma in primary sclerosing cholangitis after long- time treatment with ursodeoxycholic acid. Eur J Gastroenterol Hepatol 2007;19:487- 91.
[33] Poropat G, Giljaca V, Stimac D, Gluud C. Bile acids for primary sclerosing cholangitis. Cochrane Database Syst Rev 2011;1:CD003626.
[34] Triantos CK, Koukias NM, Nikolopoulou VN, Burroughs AK. Meta- analysis: ursodeoxycholic acid for primary sclerosing cholangitis. Aliment Pharmacol Ther 2011;34:901- 10.
[35] Chapman RW. High- dose ursodeoxycholic acid in the treatment of primary sclerosing cholangitis: throwing the urso out with the bathwater? Hepatology 2009;50:671- 3.
[36] Paumgartner G. Biliary physiology and disease: re ections of a physician- scientist. Hepatology 2010;51:1095- 106.
[37] Halilbasic E, Fiorotto R, Fickert P, Marschall HU, Moustafa T, Spirli C, et al. Side chain structure determines unique physio-logic and therapeutic properties of norursodeoxycholic acid in Mdr2- /- mice. Hepatology 2009;49:1972- 81.
[38] Fickert P, Wagner M, Marschall HU, Fuchsbichler A, Zollner G, Tsybrovskyy O, et al. 24- norUrsodeoxycholic acid is supe-rior to ursodeoxycholic acid in the treatment of sclerosing cholangitis in Mdr2 (Abcb4) knockout mice. Gastroenterology 2006;130:465- 81.
acid in primary sclerosing cholangitis. Gastroenterology 2001;121:900- 7.
[19] Harnois DM, Angulo P, Jorgensen RA, Larusso NF, Lindor KD. High- dose ursodeoxycholic acid as a therapy for patients with primary sclerosing cholangitis. Am J Gastroenterol 2001;96:1558- 62.
[20] Cullen SN, Rust C, Fleming K, Edwards C, Beuers U, Chapman RW. High dose ursodeoxycholic acid for the treatment of primary sclerosing cholangitis is safe and effective. J Hepatol 2008;48:792- 800.
[21] Olsson R, Boberg KM, de Muckadell OS, Lindgren S, Hultcrantz R, Folvik G, et al. High- dose ursodeoxycholic acid in primary sclerosing cholangitis: a 5- year multicenter, randomized, controlled study. Gastroenterology 2005;129:1464- 72.
[22] Lindor KD, Kowdley KV, Luketic VA, Harrison ME, McCashland T, Befeler AS, et al. High- dose ursodeoxycholic acid for the treatment of primary sclerosing cholangitis. Hepatology 2009;50:808- 14.
[23] Imam MH, Sinakos E, Gossard AA, Kowdley KV, Luketic VA, Edwyn Harrison M, et al. High- dose ursodeoxycholic acid increases risk of adverse outcomes in patients with early stage primary scle-rosing cholangitis. Aliment Pharmacol Ther 2011;34:1185- 92.
[24] Fickert P, Zollner G, Fuchsbichler A, Stumptner C, Weiglein AH, Lammert F, et al. Ursodeoxycholic acid aggravates bile infarcts in bile duct- ligated and Mdr2 knockout mice via disruption of cholangioles. Gastroenterology 2002;123:1238- 51.
[25] Sinakos E, Marschall HU, Kowdley KV, Befeler A, Keach J, Lindor K. Bile acid changes after high- dose ursodeoxycholic acid treatment in primary sclerosing cholangitis: Relation to disease progression. Hepatology 2010;52:197- 203.
[26] Tung BY, Emond MJ, Haggitt RC, Bronner MP, Kimmey MB, Kowdley KV, et al. Ursodiol use is associated with lower preva-lence of colonic neoplasia in patients with ulcerative colitis and primary sclerosing cholangitis. Ann Intern Med 2001;134:89- 95.
[27] Wolf JM, Rybicki LA, Lashner BA. The impact of ursodeoxy-cholic acid on cancer, dysplasia and mortality in ulcerative colitis patients with primary sclerosing cholangitis. Aliment Pharmacol Ther 2005;22:783- 8.
[28] Pardi DS, Loftus EV Jr, Kremers WK, Keach J, Lindor KD. Ursodeoxycholic acid as a chemopreventive agent in patients
04-Chazoullieres.indd S25 25/09/2012 11:49:50