Ponecia realizada por el Dr. Peter Barnes.
24
CONTROVERSIES AROUND USE CONTROVERSIES AROUND USE OF CORTICOSTEROIDS IN COPD OF CORTICOSTEROIDS IN COPD Peter Barnes National Heart & Lung Institute Imperial College, London, UK Imperial College Royal Brompton Hospital Amsterdam: September 2011 Amsterdam: September 2011
-
Upload
ferrer-epocsite -
Category
Documents
-
view
248 -
download
3
description
Ponencia realizada por el Dr. Peter Barnes sobre la controversia en torno al uso de los corticoides en el tratamiento de la EPOC.Conferencia llevada a cabo en el Symposium "Hacia un tratamiento más personalizado de la EPOC". Organizado por el Grupo Ferrer.
Transcript of Ponecia realizada por el Dr. Peter Barnes.

CONTROVERSIES AROUND USE CONTROVERSIES AROUND USE OF CORTICOSTEROIDS IN COPDOF CORTICOSTEROIDS IN COPD
Peter BarnesNational Heart & Lung InstituteImperial College, London, UK
Imperial College Royal Brompton Hospital
Amsterdam: September 2011Amsterdam: September 2011

ASTHMA AND COPDASTHMA AND COPD
MacrophagesMacrophages
NeutrophilsNeutrophils
Tc1 cells Tc1 cells
Mast cellsMast cells
EosinophilsEosinophils
Th2 cellsTh2 cells
Airway InflammationAirway Inflammation
ASTHMAASTHMA COPDCOPD
Inflammatory geneInflammatory geneexpressionexpression
NF-NF-κκBBAP-1AP-1
Steroid sensitiveSteroid sensitive Steroid resistantSteroid resistant

TRIAL OF STEROIDSTRIAL OF STEROIDS
1 2 3 4 5 6 7 8 9 10 11 12 13 14
Pea
k fl
ow
(L
/min
)
Days
Prednisolone 30 mg o.m. x 14 daysPrednisolone 30 mg o.m. x 14 days
0
100
200
300
400
500
ASTHMAASTHMA
0
100
200
300
400
500
1 2 3 4 5 6 7 8 9 10 11 12 13 14
Pea
k fl
ow
(L
/min
)
Prednisolone 30 mg o.m. x 14 daysPrednisolone 30 mg o.m. x 14 days
COPDCOPD

OVERLAP BETWEEN COPD AND ASTHMAOVERLAP BETWEEN COPD AND ASTHMA
COPDCOPD
NeutrophilsNeutrophils
No AHRNo AHR
No steroid No steroid responseresponse
ASTHMAASTHMA
EosinophilsEosinophils
AHRAHR
Steroid Steroid responseresponse
““Wheezy Wheezy bronchitis”bronchitis”
~10%~10%

Papi A et al: AJRCCM 2000
EX NO & SPUTUM EOS IN “REVERSIBLE” COPDEX NO & SPUTUM EOS IN “REVERSIBLE” COPD
Reversible: >15%Reversible: >15% in FEV in FEV11 after b/d after b/d
Exhaled Exhaled NONO
Sputum Sputum eoseos

0
10
20
30
40
50
60
70
80
Ce
l l c
ou
nt
(% t
ota
l)
BaselineBaseline
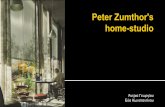
EFFECT OF ORAL STEROID ON INDUCED SPUTUM EFFECT OF ORAL STEROID ON INDUCED SPUTUM INFLAMMATORY CELL PROFILE IN COPDINFLAMMATORY CELL PROFILE IN COPD
COPD patients (n=8) 645.1yr; FEV1=48% predicted
FEV1=1.20L
MacrophagesMacrophages
NeutrophilsNeutrophils
EosinophilsEosinophils
PlaceboPlacebo PrednisolonePrednisolone(30mg daily x 14d)(30mg daily x 14d)
FEV1=1.27L FEV1=1.30L
Keatings V et al: AJRCCM 1997

Mild Moderate Severe Unknown
0
25
50
75
Exacerbations(%)
Paggiaro P et al, Lancet 1998
Fluticasone propionate(76/142)Placebo(111/139)
EFFECT OF ICS ON FREQUENCY AND EFFECT OF ICS ON FREQUENCY AND SEVERITY ON EXACERBATIONSSEVERITY ON EXACERBATIONS
*
NoNo overall reduction in exacerbations overall reduction in exacerbationsSmall reduction in patients with Small reduction in patients with
severesevere exacerbations exacerbations
ALTHOUGH STATISTICALLY SIGNIFICANTALTHOUGH STATISTICALLY SIGNIFICANTIS THIS CLINICALLY RELEVANT ?IS THIS CLINICALLY RELEVANT ?

ICS AND ACUTE EXACERBATIONSICS AND ACUTE EXACERBATIONS
• Several studies show a small reduction (25-25%) in exacerbations - hospital admissions, oral steroids, antibiotics
• Similar reduction is shown with long-acting bronchodilators esp tiotropium bromide (LAMA) N.B. tiotropium has no anti-inflammatory effect in COPD

TIOTROPIUM TIOTROPIUM vsvs SERETIDE: INSPIRE STUDY SERETIDE: INSPIRE STUDY
Wedzicha JA et al: AJRCCM 2007
0
0.5
1
1.5
Tiotropium (n=658)
Salmeterol/fluticasone (n=665)
Exa
cerb
atio
ns/
year
COPD patients: FEVCOPD patients: FEV11 ~40% predicted: 2 years ~40% predicted: 2 years
TotalN.S.
Oral steroids
Antibiotics
p<0.05
p<0.05

ICS AND ACUTE EXACERBATIONSICS AND ACUTE EXACERBATIONS
• Several studies show a small reduction (25-25%)Several studies show a small reduction (25-25%) in exacerbationsin exacerbations - hospital admissions, oral steroids, antibiotics- hospital admissions, oral steroids, antibiotics
• Similar reduction is shown with long-acting bronchodilatorsSimilar reduction is shown with long-acting bronchodilators esp tiotropium bromide (LAMA)esp tiotropium bromide (LAMA) N.B. tiotropium has no anti-inflammatory effect in COPDN.B. tiotropium has no anti-inflammatory effect in COPD
• No additive effect of LAMA and ICS in No additive effect of LAMA and ICS in ↓ exacerbations↓ exacerbations Choice should therefore be based on long-term safetyChoice should therefore be based on long-term safety

ICS AND COPD PROGRESSIONICS AND COPD PROGRESSION
TRIAL n DURATION SEVERITYTRIAL n DURATION SEVERITY
Copenhagen City 290Copenhagen City 290 3 yr mild 3 yr mild
EUROSCOP 1277 3 yr mildEUROSCOP 1277 3 yr mild
ISOLDE 751 3 yr moderateISOLDE 751 3 yr moderate
Lung Health 2 1116 3.5 yr moderateLung Health 2 1116 3.5 yr moderate11oo outcome = decline in lung function outcome = decline in lung function
OUTCOMEOUTCOME
no effectno effect
no effectno effect
no effectno effect
no effectno effect
Cochrane Database Systematic Review: Cochrane Database Systematic Review: >13,000 COPD patients- no >13,000 COPD patients- no ↓ FEV↓ FEV1 1 decline decline (Yang IM et al 2007)(Yang IM et al 2007)

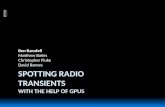
Calverley PA et al: NEJM 2007
18
16
14
12
10
8
6
4
2
0
Time to death (weeks)
Pro
bab
ilit
y o
f d
eath
(%
)
Placebo FP/Salm
0 12 24 36 48 60 72 84 96 108 120 132 144 156
TORCH STUDYTORCH STUDY
All cause mortalityAll cause mortality
17.5% ↓p=0.52
ICS AND COPD MORTALITYICS AND COPD MORTALITY
15.2%15.2%
12.6%12.6%
Salm FP
16.0%16.0%
13.5%13.5%
No effect on mortality: 9 studiesNo effect on mortality: 9 studies
OR 0.98 (0.83-1.16) n=8390OR 0.98 (0.83-1.16) n=8390Yang IM et al: Cochrane review 2007Yang IM et al: Cochrane review 2007

DOSE-RESPONSE TO INHALED STEROID IN ASTHMADOSE-RESPONSE TO INHALED STEROID IN ASTHMA
Adams NP & Jones PW: Resp Med 2006
Ch
an
ge
in F
EV
1 (
litre
)co
mp
ared
to
bas
elin
e
0.6
0.4
0.2
0.0
100 200 500 1000
n = 8N = 1219
n = 20N = 3527
n = 6N = 872
n = 3N = 414
Daily dose of fluticasone propionate (μg/day)
IT IS DIFFICULT TO SHOW A IT IS DIFFICULT TO SHOW A DOSE EFFECT WHEN THERE IS DOSE EFFECT WHEN THERE IS
NO RESPONSE !NO RESPONSE !
NO DOSE-RESPONSE TO INHALEDNO DOSE-RESPONSE TO INHALEDSTEROIDS HAS BEEN STEROIDS HAS BEEN
DEMONSTRATED IN COPDDEMONSTRATED IN COPD

INHALED CORTICOSTEROIDS IN COPD:INHALED CORTICOSTEROIDS IN COPD:SIDE EFFECTSSIDE EFFECTS
• High doses usually usedHigh doses usually used
• High risk of osteoporosis and fracturesHigh risk of osteoporosis and fractures low mobility, poor nutrition, smoking, elderly low mobility, poor nutrition, smoking, elderly
• Risk of cataractsRisk of cataracts
• Co-morbidity may be worsenedCo-morbidity may be worsened diabetes, hypertension, peptic ulceration]diabetes, hypertension, peptic ulceration]
• Increased risk of pneumonia, TBIncreased risk of pneumonia, TB

47 studies in 13,139 patients47 studies in 13,139 patients
• ↑ ↑ oropharyngeal candidiasis OR 2.49 (1.78-3.49) n=4380oropharyngeal candidiasis OR 2.49 (1.78-3.49) n=4380
• ↑ ↑ hoarsenesshoarseness
• NO major effect on fractures or BMD over 3 yearsNO major effect on fractures or BMD over 3 years
Yang IA et al, Cochrane review 2007
SIDE EFFECTS OF ICS IN COPDSIDE EFFECTS OF ICS IN COPD
16-44% ↑risk of 16-44% ↑risk of cataractscataracts with ICS exposure with ICS exposure dose-response, observational studydose-response, observational studyErnst P et al: ERJ 2006Ernst P et al: ERJ 2006
Longer term studies are neededLonger term studies are needed

Calverley PMA et al, NEJM 2007
25
20
15
10
5
0
0 12 24 36 48 60 72 84 96 108 120 132 144 156
Pro
bab
ility
of
ev
en
t (%
)
Time to event (weeks)
p < 0.001 vs placeboSALM/FP 19.6%SALM/FP 19.6%FP 18.3%FP 18.3%
SALM 13.3%SALM 13.3%Placebo 12.3%Placebo 12.3%
TORCH STUDY: PNEUMONIATORCH STUDY: PNEUMONIA

Nannini LJ et al: Cohrane Review 2007
OR 1.62 (1.35 to 1.94) OR 1.62 (1.35 to 1.94)
PNEUMONIA: ICS+LABA PNEUMONIA: ICS+LABA vsvs LABA LABA

Nested case control study within population cohortfrom Quebec Healthcare Database covering >7 million175,906 COPD patients (identified by Rx) - 7.1 y av. follow up 23,942 hospitalised for pneumonia (mean age 77yr)4 controls /case
Ernst P et al: AJRCCM 2007
RR on ICSRR on ICSPneumonia rate (all)Pneumonia rate (all) 1.7 (1.63-1.77)1.7 (1.63-1.77)FP FP >>1000 1000 μμg/dg/d 2.25 (2.07-2.44)2.25 (2.07-2.44)
Pneumonia deathPneumonia death 1.53 (1.30-1.80)1.53 (1.30-1.80)FP FP >>1000 1000 μμ/d/d 1.78 (1.33-2.37) 1.78 (1.33-2.37)
ICS AND PNEUMONIA IN COPDICS AND PNEUMONIA IN COPD

10
8
6
4
2
[TN
F-
(n
mo
l/mL
)]
0
TNF-TNF-
PlaceboPlacebo Budesonide (800 µg b.d.x 2 wk)Budesonide (800 µg b.d.x 2 wk)BaselineBaseline
COPD patients (n=14): age 65 1.1 yr; FEV1 = 35 1.3%
CYTOKINES IN INDUCED SPUTUM IN COPD:CYTOKINES IN INDUCED SPUTUM IN COPD:LACK OF EFFECT OF INHALED CORTICOSTEROIDLACK OF EFFECT OF INHALED CORTICOSTEROID
[IL
-8 (
nm
ol/m
L)]
0
2
4
6
8
IL-8IL-8
Keatings V et al: Am J Respir Crit Care Med 1997
N.SN.S.N.SN.S.
IS THERE AN ACTIVE STEROID IS THERE AN ACTIVE STEROID RESISTANCE MECHANISM IN COPD?RESISTANCE MECHANISM IN COPD?

00
100100
200200
MIP
-1M
IP-1
(
ng
/ml)
(n
g/m
l)
1010-10-10 10 10-8-8 10 10-6-6
Dexamethasone (M)Dexamethasone (M)
LPSLPSNSNS
Non-smokerNon-smoker
NS LPSNS LPS1010-8-8MM
DexDex
COPDCOPD
Bronchoalveolar lavage macrophagesBronchoalveolar lavage macrophagesREDUCED EFFECT OF CORTICOSTEROIDS IN COPDREDUCED EFFECT OF CORTICOSTEROIDS IN COPD
ALVEOLAR MACROPHAGES AREALVEOLAR MACROPHAGES ARESTEROID-RESISTANT IN COPDSTEROID-RESISTANT IN COPD
(SIMILAR RESULTS WITH IL-8, MMP-9)(SIMILAR RESULTS WITH IL-8, MMP-9)
Culpitt SV et al: Am J Respir Crit Care Med 2002

Cigarette smokeCigarette smoke
Oxidative stressOxidative stress
AMPLIFICATION AND STEROID RESISTANCEAMPLIFICATION AND STEROID RESISTANCE
NF-NF-κκBBGlucocorticoid Glucocorticoid receptorreceptor
HDAC2HDAC2
CorticosteroidsCorticosteroids
HistoneHistoneacetylationacetylation
InflammationInflammation
Inflammatory Inflammatory genes genes e.g. IL-8, MMP-9e.g. IL-8, MMP-9

Cigarette smokeCigarette smoke
Oxidative stressOxidative stress
AMPLIFICATION AND STEROID RESISTANCEAMPLIFICATION AND STEROID RESISTANCE
NF-NF-κκBB
HistoneHistoneacetylationacetylation
Inflammatory Inflammatory genes genes e.g. IL-8, MMP-9e.g. IL-8, MMP-9
HDAC2HDAC2
↑ ↑ InflammationInflammation
SteroidSteroidresistanceresistance
PI3K-δ
HD
AC
2 e
xp
res
sio
n(r
ati
o v
s h
ist o
ne-
1)
0
1
2
3
Non-smokers
***
Normalsmokers
COPD
HDAC2HDAC2
Peripheral lung
Ito K et al: N Engl J Med 2005
TheophyllineTheophylline NortriptylineNortriptyline

INHALED CORTICOSTEROIDS IN COPDINHALED CORTICOSTEROIDS IN COPD
• Treat associated asthmaTreat associated asthma (asthma and COPD may coexist in the same patient)(asthma and COPD may coexist in the same patient)
• No significant effect on inflammationNo significant effect on inflammation (c.f. asthma)(c.f. asthma)
• No effect on progression of diseaseNo effect on progression of disease
• Reduction in severe exacerbations (small effect)Reduction in severe exacerbations (small effect)
• Risk of adverse systemic effects (esp diabetes)Risk of adverse systemic effects (esp diabetes)
• Increased pneumonia, TBIncreased pneumonia, TB
• ExpensiveExpensive
Inhaled corticosteroids recommended forInhaled corticosteroids recommended forpatients with severe disease (FEVpatients with severe disease (FEV11<50% predicted)<50% predicted)
who have frequent exacerbations (>2/year) who have frequent exacerbations (>2/year) <10% of patients (high dose ICS currently in >80%)<10% of patients (high dose ICS currently in >80%)
The use of high dose inhaled steroids for COPDThe use of high dose inhaled steroids for COPDneeds to needs to markedlymarkedly reduced in the future reduced in the future• Can we make steroids more effective?Can we make steroids more effective?• Are there alternative anti-inflammatory treatments?Are there alternative anti-inflammatory treatments?

SO WHAT ABOUT INHALED STEROIDS IN COPD?SO WHAT ABOUT INHALED STEROIDS IN COPD?
• ~80% diagnosed COPD patients in UK on ICS/combination~80% diagnosed COPD patients in UK on ICS/combination GOLD recommendations 10-20%!GOLD recommendations 10-20%!
• Corticosteroids: NO anti-inflammatory effects in COPD Corticosteroids: NO anti-inflammatory effects in COPD in vitroin vitro or or in vivoin vivo (sputum, bronchial biopsies) (sputum, bronchial biopsies)
• High dose ICS: no effect on FEVHigh dose ICS: no effect on FEV11 decline or mortality decline or mortality
• Small Small ↓ exacerbations: but trials misinterpreted↓ exacerbations: but trials misinterpreted
• High dose ICS (FP): High dose ICS (FP): ↑ pneumonias↑ pneumonias• ↑ ↑ systemic side effects with timesystemic side effects with time - osteoporosis, diabetes, cataracts, etc- osteoporosis, diabetes, cataracts, etc
• Restrict use of ICS in the future?Restrict use of ICS in the future?