Pharmacokinetics and Monte Carlo Simulations of Doripenem in Patients with Febrile Neutropenia
6
F ever is a common complication in neutropenic patients with cancer. High-risk hospitalized patients are in danger of significant morbidity and mor- tality and require early initiation of broad-spectrum antibiotic therapy. Cur- rent guidelines suggest treatment with an antipseudomonal β-lactam agent such as a group 2 carbapenem. 1 Doripenem is a group 2 carbapenem that closely resembles meropenem. 2 It has enhanced in vitro activity against gram-negative bacteria including Pseu- domonas aeruginosa. 3 Furthermore, it is stable in infusion solutions, which al- lows for prolonged administration. 4 A longer, 4-hour infusion time (1-hour infu- sions being normal) has the potential for improving the pharmacodynamics of dori- penem against serious gram-negative bac- terial infections. 5 These longer infusions also appear to be safe and well tolerated even at high (1000-mg) doses. 6 It is well established that antibiotic pharmacokinetic parameters in patients with cancer are altered. 7 Studies have demonstrated that the volume of distri- bution (Vd) and clearance (Cl) of β-lac- tams, aminoglycosides, and vancomycin are frequently increased in febrile neutropenia. 8 Several studies have evaluated the pharmacokinetic parameters of carbapenems in this population. Two small studies in neu- tropenic patients receiving imipenem showed a high vari- ability in Vd and Cl, but comparable results to healthy vol- unteers. 9,10 In the only study to compare meropenem phar- macokinetic parameters in neutropenic patients with those in healthy controls, the volume of distribution and nonre- nal clearance were significantly increased in patients with neutropenia. 11 To date there are no published data regard- ing doripenem in neutropenic patients. These altered phar- macokinetic characteristics, combined with an increased likelihood of infections caused by organisms with higher The Annals of Pharmacotherapy ■ 2012 October, Volume 46 ■ 1281 Pharmacokinetics and Monte Carlo Simulations of Doripenem in Patients with Febrile Neutropenia Gary E Stein, Grace Kulhanek, Curtis L Smith, Joseph L Kuti, David P Nicolau, Amy Scharmen, Chris Farnum, MaryAnn Tran, Apoorv Kalra, and Daniel H Havlichek theannals.com Pharmacokinetics Author information provided at end of text. RESEARCH REPORTS BACKGROUND: Doripenem is a group 2 carbapenem with enhanced in vitro activity against gram-negative bacteria including Pseudomonas aeruginosa. There is a paucity of pharmacokinetic/pharmacodynamic data on doripenem in patients with febrile neutropenia. OBJECTIVE: To conduct a pharmacokinetic evaluation of 2 doses of doripenem in patients with febrile neutropenia and provide probability estimates of attaining effective drug exposure against common gram-negative pathogens. METHODS: We obtained multiple blood samples from 12 adults with febrile neutro- penia who were receiving either 500 mg or 1000 mg of intravenous doripenem over 4 hours every 8 hours. Following at least 2 doses, serum concentrations were measured in each subject at 1, 4, 6, and 8 hours after initiation of a dose by a validated high-performance liquid chromatography assay. The derived pharmaco- kinetic parameters from these serum levels were used to perform a 5000-patient Monte Carlo simulation against bacteria with minimal inhibitory concentrations (MICs) of 0.008-64 mg/L to determine probability estimates of the time in which unbound drug concentrations remain above the MIC ( f T >MIC ). RESULTS: The mean pharmacokinetic parameters in these patients were a volume of distribution of 43.9 L, an elimination rate constant of 0.37 h –1 , a total clearance of 14.4 L/h, and an area under the concentration-time curve of 57.6 mg•h/L. An optimal probability of target attainment (40% fT >MIC ) of 90% was obtained against bacteria with MICs ≤2 mg/L and ≤4 mg/L with 500-mg and 1000-mg doses, respectively. Adverse events associated with doripenem were not observed. CONCLUSIONS: The findings from this analysis of doripenem suggest that higher doses, as well as prolonged infusions, may be necessary to optimally treat selected gram-negative bacteria (eg, P. aeruginosa) in patients with febrile neutropenia. KEY WORDS: doripenem, neutropenia, pharmacokinetics. Ann Pharmacother 2012;46:1281-6. Published Online, 25 Sept 2012, theannals.com, doi: 10.1345/aph.1R097
Transcript of Pharmacokinetics and Monte Carlo Simulations of Doripenem in Patients with Febrile Neutropenia

Fever is a common complication inneutropenic patients with cancer.
High-risk hospitalized patients are indanger of significant morbidity and mor-tality and require early initiation ofbroad-spectrum antibiotic therapy. Cur-rent guidelines suggest treatment with anantipseudomonal β-lactam agent such asa group 2 carbapenem.1
Doripenem is a group 2 carbapenemthat closely resembles meropenem.2 Ithas enhanced in vitro activity againstgram-negative bacteria including Pseu-domonas aeruginosa.3 Furthermore, it isstable in infusion solutions, which al-lows for prolonged administration.4 Alonger, 4-hour infusion time (1-hour infu-sions being normal) has the potential forimproving the pharmacodynamics of dori-penem against serious gram-negative bac-terial infections.5 These longer infusionsalso appear to be safe and well toleratedeven at high (1000-mg) doses.6
It is well established that antibioticpharmacokinetic parameters in patientswith cancer are altered.7 Studies havedemonstrated that the volume of distri-bution (Vd) and clearance (Cl) of β-lac-tams, aminoglycosides, and vancomycinare frequently increased in febrile neutropenia.8 Severalstudies have evaluated the pharmacokinetic parameters ofcarbapenems in this population. Two small studies in neu-tropenic patients receiving imipenem showed a high vari-ability in Vd and Cl, but comparable results to healthy vol-
unteers.9,10 In the only study to compare meropenem phar-macokinetic parameters in neutropenic patients with thosein healthy controls, the volume of distribution and nonre-nal clearance were significantly increased in patients withneutropenia.11 To date there are no published data regard-ing doripenem in neutropenic patients. These altered phar-macokinetic characteristics, combined with an increasedlikelihood of infections caused by organisms with higher
The Annals of Pharmacotherapy n 2012 October, Volume 46 n 1281
Pharmacokinetics and Monte Carlo Simulations of Doripenem in
Patients with Febrile Neutropenia
Gary E Stein, Grace Kulhanek, Curtis L Smith, Joseph L Kuti, David P Nicolau, Amy Scharmen, Chris Farnum,
MaryAnn Tran, Apoorv Kalra, and Daniel H Havlichek
theannals.com
Pharmacokinetics
Author information provided at end of text.
RESEARCH REPORTS
BACKGROUND: Doripenem is a group 2 carbapenem with enhanced in vitroactivity against gram-negative bacteria including Pseudomonas aeruginosa.There is a paucity of pharmacokinetic/pharmacodynamic data on doripenem inpatients with febrile neutropenia.
OBJECTIVE: To conduct a pharmacokinetic evaluation of 2 doses of doripenem inpatients with febrile neutropenia and provide probability estimates of attainingeffective drug exposure against common gram-negative pathogens.
METHODS: We obtained multiple blood samples from 12 adults with febrile neutro-penia who were receiving either 500 mg or 1000 mg of intravenous doripenem over4 hours every 8 hours. Following at least 2 doses, serum concentrations weremeasured in each subject at 1, 4, 6, and 8 hours after initiation of a dose by avalidated high-performance liquid chromatography assay. The derived pharmaco-kinetic parameters from these serum levels were used to perform a 5000-patientMonte Carlo simulation against bacteria with minimal inhibitory concentrations(MICs) of 0.008-64 mg/L to determine probability estimates of the time in whichunbound drug concentrations remain above the MIC (fT>MIC).
RESULTS: The mean pharmacokinetic parameters in these patients were a volumeof distribution of 43.9 L, an elimination rate constant of 0.37 h–1, a total clearance of14.4 L/h, and an area under the concentration-time curve of 57.6 mg•h/L. An optimalprobability of target attainment (40% fT>MIC) of 90% was obtained against bacteriawith MICs ≤2 mg/L and ≤4 mg/L with 500-mg and 1000-mg doses, respectively.Adverse events associated with doripenem were not observed.
CONCLUSIONS: The findings from this analysis of doripenem suggest that higherdoses, as well as prolonged infusions, may be necessary to optimally treat selectedgram-negative bacteria (eg, P. aeruginosa) in patients with febrile neutropenia.
KEY WORDS: doripenem, neutropenia, pharmacokinetics.
Ann Pharmacother 2012;46:1281-6.
Published Online, 25 Sept 2012, theannals.com, doi: 10.1345/aph.1R097

inhibitory concentrations, demonstrate the importance ofstudying carbapenems in this population.
To enhance our knowledge of doripenem dosing in pa-tients with febrile neutropenia, we conducted a pharma-cokinetic evaluation of 2 different doses of doripenem in-fused over 4 hours. This research report also providesprobability estimates of attaining effective drug exposureof doripenem against common gram-negative pathogensusing Monte Carlo simulation techniques.12
Methods
Hospitalized adults with febrile (temperature ≥38.3 ˚C)neutropenia (absolute neutrophil count <1000 cells/µL)who were to be empirically treated with doripenem wereeligible to enroll in this study. Patients with renal failure(creatinine clearance ≤30 mL/min) or hepatic failure (inter-national normalized ratio ≥2) who were pregnant or whohad an allergy to β-lactam antibiotics were excluded fromthis investigation. Each patient gave written informed con-sent that was approved by the hospital research reviewcommittee.
Patients were equally randomized using a random num-ber table (blocks of 4) to receive a 4-hour intravenous infu-sion of 500 mg or 1000 mg of doripenem every 8 hours inan unblinded manner. Other antibiotics could be adminis-tered as deemed necessary by the attending physician. Pa-tients were monitored for adverse effects by the study in-vestigators.
Blood samples were obtained after at least 2 doses ofdoripenem at 1, 4, 6, and 8 hours after the initiation of the4-hour infusion. After centrifugation, serum samples werealiquoted and stored at –70 ˚C until time of analysis. Theconcentrations of doripenem were measured at the Centerfor Anti-Infective Research (Hartford, CT) by a validatedhigh-performance liquid chromatography assay.13 The as-say was linear over a range of 0.5 to 40 mg/L (R2 = 0.995).Intraday coefficients of variation for the low-quality (1-mg/L) and high-quality (30-mg/L) control samples were4.02% and 4.44%, respectively. Interday coefficients ofvariation for the quality control samples were 5.44% and5.93%, respectively.
Each patient’s concentration-time profile was fit to 1-and 2-compartment models using WinNonlin ProfessionalVersion 5.3 (Pharsight Corporation). Final model selectionwas based on visual inspection of the fit and correlation be-tween the observed and predicted concentration by log-likelihood and the Akaike information criterion. Based onthe above and the rule of parsimony, a 1-compartmentmodel best fit the data.
Mean (SD) estimates for the first-order elimination rateconstant (k) and Vd were extrapolated from the pharma-cokinetic analysis to perform a 5000-patient Monte Carlosimulation (Crystal Ball 2000 Professional Edition, Oracle
Corporation). A 1-compartment model was used to simu-late steady-state concentration-time profiles for 500-mgand 1000-mg doripenem doses every 8 hours as 1-hourand 4-hour infusions. The k and Vd parameters were as-sumed to follow log-normal distributions. The fraction un-bound was set at 0.92.2 The probability of attaining 40%time of unbound drug concentration above the minimal in-hibitory concentration (fT>MIC) was calculated for the popu-lation against MICs of 0.008-64 mg/L in doubling dilu-tions.14 An a priori threshold of 90% probability of targetattainment was considered optimal. The cumulative frac-tion of response (CFR) was estimated for populations ofgram-negative bacteria from the TRUST (Tracking Resis-tance in the United States Today) 13 surveillance program.3
The CFR was calculated as the summation of the probabil-ity of target attainment (PTA) at each MIC multiplied bythe fraction of isolates at that MIC.
Results
Of the 12 patients (4 females, 8 males) enrolled, 8 hadhematologic malignancies. None were in the intensive careunit. Mean age was 50 years (range 20-76) and mean totalbody weight was 90 kg (range 54-114). Their mean creati-nine clearance, estimated by the Cockcroft-Gault equation,was 114 mL/min (range 73-178).15 Demographic charac-teristics between the 2 groups were not statistically signifi-cant (p > 0.05; Wilcoxon rank-sum test). None of the pa-tients experienced an adverse event associated withdoripenem treatment.
The mean patient demographic characteristics for the 2study groups are shown in Table 1. A male patient in the500-mg group was excluded because serum concentrationsof doripenem could not be interpreted. The mean pharma-cokinetic parameters (Vd, k, half-life [t1/2], total Cl, andarea under the concentration-time curve [AUC]) for the to-
1282 n The Annals of Pharmacotherapy n 2012 October, Volume 46 theannals.com
GE Stein et al.
Table 1. Mean Patient Demographic Characteristics for theTwo Study Groups
Doripenem
Variable 500 mg 1000 mg p Value
Pts., n 5 6
Sex, n
male 2 6
female 3 0
Age, years 49 49 0.78
Weight, kg 78 100 0.07
Height, cm 171 173 0.93
BMI, kg/m2 27 33 0.14
CrCl, mL/min 114 112 0.85
BMI = body mass index; CrCl = creatinine clearance.

tal population and the 2 study groups, following multipledoses of doripenem, are presented in Table 2. The meanpharmacokinetic parameters in these 2 groups were notsignificantly different (p > 0.05; Wilcoxon rank-sum test).The increased Vd and Cl values in the 1000-mg groupwere likely due to the higher mean weight (100 kg vs 78kg) in these patients. This weight difference would also ex-plain the lack of dose proportionality in the AUC calcula-tion.
Because the pharmacokinetics were determined not tobe different between the 2 study groups, the total popula-tion estimates were applied in the Monte Carlo simula-tions. The PTA with 500-mg and 1000-mg doses ofdoripenem every 8 hours is shown in Figures 1 and 2. Anoptimal PTA of 90% was obtained against bacteria withMICs ≤2 mg/L and ≤4 mg/L with 500-mg and 1000-mgdoses, respectively.
Discussion
The pharmacokinetics and pharmacodynamics of car-bapenem antibiotics are important to evaluate because ofincreased resistance in gram-negative pathogens and thegreater use of these agents in the immunocompromisedhost.16 Carbapenems exhibit time-dependent killing, and invivo efficacy is correlated to the length of time unbounddrug concentrations exceed the MIC (%fT>MIC).8 For theseantimicrobial agents, bactericidal effects are observed whenT>MIC exceeds 40% of the dosing interval.17 One method toincrease the exposure of these antibiotics is to lengthen theirduration of infusion. Extensions in the infusion time havenot only been well tolerated, but have been shown to im-prove the T>MIC for carbapenems.6,18 To determine whetherprolonged infusions for these agents are clinically justified, astudy comparing target attainment rates of different dosageregimens against recent bacterial isolates is warranted.19
Monte Carlo simulation has been shown to be an ac-ceptable method to evaluate the probability of differentdosage regimens in attaining pharmacodynamic targetsagainst specific bacterial pathogens.17,19 The results fromthese simulations can provide clinicians with reasonableconfidence concerning which dosage regimens have thehighest probabilities of in vivo efficacy. The principal re-quirements to perform Monte Carlo simulations are robustpharmacokinetic parameters and a defined interrelationshipbetween the pharmacokinetics, pharmacodynamics, and mi-crobial susceptibility data for a given antibiotic.12 Althoughthis investigation had a small sample size, the pharmacoki-netic parameters obtained were similar to those from anotherstudy of doripenem treatment in critically ill patients and canprovide a suitable basis for modeling.20 Of note, these criti-
cally ill patients with ventilator-associated pneu-monia were found to have an increased volumeof distribution and elimination half-life ofdoripenem compared to healthy volunteers.20,21
We also found these pharmacokinetic parame-ters to be increased in our patient population.
Our Monte Carlo simulations discoveredthat the predetermined pharmacodynamic tar-gets (fT>MIC for 40% of the dosing interval)could be obtained for bacteria with MICs ≤2mg/L and ≤4 mg/L with 500-mg and 1000-mgdoses of doripenem, respectively (Figures 1and 2). This observation is similar to a study ofmeropenem in patients with febrile neutrope-nia.18 A recent survey of carbapenem resis-tance in the US (TRUST 13) of commongram-negative pathogens found that doripen-em had an MIC90 (MIC for 90% of strains) lessthan or equal to 0.5 mg/L for common Enter-obacteriaceae (eg, Escherichia coli, Klebsiellapneumoniae, Proteus mirabilis, Enterobacter
Pharmacokinetics of Doripenem in Febrile Neutropenia
The Annals of Pharmacotherapy n 2012 October, Volume 46 n 1283theannals.com
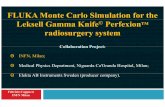
Figure 1. The probability of target attainment (PTA) for a range of MICs for a 500-mgdose of doripenem. fT>MIC = fraction of time above minimal inhibitory concentration.
Table 2. Doripenem Pharmacokinetic Parameters in Febrile Neutropenic Patientsa
Pt. Groups
Parameter 500 mg 1000 mg Combined p Value
Pts., n 5 6 11
Vd (L/kg) 0.49 (0.22) 0.50 (0.17) 0.49 (0.19) 0.72
k (hour-1) 0.36 (0.14) 0.38 (0.20) 0.37 (0.17) 0.93
t1/2 (hours) 2.2 (0.84) 2.4 (1.3) 2.3 (1.1) 0.93
Cl (L/h/kg) 0.16 (0.05) 0.18 (0.09) 0.17 (0.07) 0.85
AUC (mg•h/L) 47.1 (13.2) 66.4 (33.1) 57.6 (26.8) 0.46
AUC = area under the concentration-curve; Cl = total body clearance; k= elimination rate constant; t1/2 = half-life; Vd = volume of distribution.aMean (SD).

cloacae, and Serratia marcescens) and anMIC90 of 4 mg/L for P. aeruginosa.3 Based onthis surveillance study and our simulations,standard dosing of intravenous doripenem 500mg over 1 hour every 8 hours would be ade-quate to empirically treat common Enterobac-teriaceae, but a higher dose (1000 mg) andlonger infusion would be necessary for optimalcoverage of P. aeruginosa (Table 3).
In a retrospective analysis of febrile neu-tropenic patients with bacteremia, Ariano et al.discovered that an 80% clinical response ratewas evident when the %T>MIC for meropenemexceeded 75% of the dosing interval comparedto 59% T>MIC for nonresponders.22 We foundthat this target (80% fT>MIC) could be achievedfor bacteria with MICs ≤0.5 mg/L and ≤1mg/L with 500-mg and 1000-mg doses ofdoripenem infused over 4 hours, respectively(Table 4). None of the dosing regimens simu-lated in this investigation would provide 80%fT>MIC for isolates of P. aeruginosa at an MICof 4 mg/L.
A recent editorial highlighted pharmacoki-netic alterations in critically ill patients that canbe associated with antibiotic failure and includ-ed a synopsis of a prematurely terminatedstudy of doripenem treatment in patients withventilator-associated pneumonia.23 The interimdata analyses showed greater mortality andlower clinical cure rates in patients receivingdoripenem compared to imipenem. Althoughour patients were not critically ill, pharmacoki-netic parameters can be altered in febrile neu-tropenia.8 These changes can predispose thispopulation of patients to subtherapeutic antibi-otic concentrations and clinical failure as well.
In conclusion, the findings from this analy-sis of doripenem suggest that higher doses aswell as prolonged infusions may be necessaryto optimally treat selected gram-negative bac-teria associated with infections in patients withfebrile neutropenia.24 The MICs of key patho-gens, such as P. aeruginosa, in a given medicalcenter or unit will ultimately determine whichdoripenem dosing strategy has the greatestmerit.
Gary E Stein PharmD, Professor of Medicine and Phar-macology, Department of Medicine, Michigan State Uni-versity, East Lansing, MIGrace Kulhanek MD, Fellow in Infectious Diseases,Michigan State UniversityCurtis L Smith PharmD BCPS, Professor of Phar-macy, College of Pharmacy, Ferris State University,Big Rapids, MI
1284 n The Annals of Pharmacotherapy n 2012 October, Volume 46 theannals.com
GE Stein et al.
Table 3. Cumulative Fraction of Response (40% fT>MIC) Against VariousGram-Negative Pathogens
DoripenemDose and Infusion Times
MIC90500 mg 1000 mg
Organism (mg/L)a 1 hour 4 hours 1 hour 4 hours
Escherichia coli 0.06 1.00 1.00 1.00 1.00
Klebsiella pneumoniae 0.12 0.99 1.00 1.00 1.00
Proteus mirabilis 0.50 0.99 1.00 0.99 1.00
Enterobacter cloacae 0.25 0.99 1.00 0.99 1.00
Serratia marcescens 0.25 0.99 1.00 0.99 0.99
Pseudomonas aeruginosa 4.00 0.55 0.63 0.87 0.94
aTRUST 13 (2009) surveillance data.3
Table 4. Cumulative Fraction of Response (80% fT>MIC) Against Various Gram-Negative Pathogens
DoripenemDose and Infusion Times
MIC90500 mg 1000 mg
Organism (mg/L)a 1 hour 4 hours 1 hour 4 hours
Escherichia coli 0.06 0.98 0.99 0.99 0.99
Klebsiella pneumoniae 0.12 0.96 0.99 0.98 0.99
Proteus mirabilis 0.50 0.83 0.96 0.92 0.99
Enterobacter cloacae 0.25 0.92 0.99 0.96 0.99
Serratia marcescens 0.25 0.92 0.99 0.96 0.99
Pseudomonas aeruginosa 4.00 0.16 0.28 0.40 0.61
aTRUST 13 (2009) surveillance data.3
Figure 2. The probability of target attainment (PTA) for a range of MICs for a 1000-mg dose of doripenem. fT>MIC = fraction of time above minimal inhibitory concentration.

Joseph L Kuti PharmD, Associate Director, Clinical and Econom-ic Studies, Center for Anti-Infective Research, Hartford Hospital,Hartford, CTDavid P Nicolau PharmD, Director, Clinical and Economic Stud-ies, Center for Anti-Infective Research, Hartford HospitalAmy Scharmen BS, Research Associate, Department of Medicine,Michigan State UniversityChris Farnum MD, Staff Physician, McLaren-Greater Lansing Hospital,Lansing, MIMaryAnn Tran MD, Assistant Professor of Medicine, Department ofMedicine, Michigan State UniversityApoorv Kalra MD, Assistant Professor of Medicine, Departmentof Medicine, Michigan State UniversityDaniel H Havlichek MD, Professor of Medicine, Department ofMedicine, Michigan State UniversityCorrespondence: Dr. Stein, [email protected]/Online Access: www.theannals.com/cgi/reprint/aph.1R097
Conflict of interest: Dr. Stein received a grant from Ortho-McNeilPharmaceutical, Inc.
Funding: This study was supported by the Sparrow Hospital/Michi-gan State University Infectious Diseases Fellowship Program.
References
1. Freifeld AG, Bow EJ, Sepkowitz KA, et al. Executive summary: clinicalpractice guideline for the use of antimicrobial agents in neutropenic pa-tients with cancer: 2010 update by the Infectious Diseases Society ofAmerica. Clin Infect Dis 2011;52:427-31.
2. Paterson DL, DePestel DD. Doripenem. Clin Infect Dis 2009;49:291-8.3. Davies TA, Queenan AM, Morrow BJ, et al. Longitudinal survey of car-
bapenem resistance and resistance mechanisms in Enterobacteriaceaeand non-fermenters from the USA in 2007-9. J Antimicrob Chemother2011;66:2298-307.
4. Berthoin K, Le Duff CS, Marchand-Brynaert J, et al. Stability ofmeropenem and doripenem solutions for administration by continuousinfusion. J Antimicrob Chemother 2010;65:1073-5.
5. Samtani MN, Flamm R, Kaniga K, Nandy P. Pharmacokinetic-pharmaco-dynamic-model-guided doripenem dosing in critically ill patients. Anti-microb Agents Chemother 2010;54:2360-4.
6. Cirillo I, Vaccaro N, Turner K, et al. Pharmacokinetics, safety, and tolera-bility of doripenem after 0.5-, 1-, and 4-hour infusions in healthy volun-teers. J Clin Pharmacol 2009;49:798-806.
7. Theuretzbacher U. Pharmacokinetic and pharmacodynamic issues forantimicrobial therapy in patients with cancer. Clin Infect Dis 2012;54:1785-92.
8. Lortholary O, Lefort A, Tod M, et al. Pharmacodynamics and pharma-cokinetics of antibacterial drugs in the management of febrile neutrope-nia. Lancet Infect Dis 2008;8:612-20.
9. Drusano GL, Plaisance Kl, Forrest A, et al. Steady-state pharmacokinet-ics of imipenem in febrile neutropenic cancer patients. AntimicrobAgents Chemother 1987;31:1420-2.
10. Janmohamed RM, Leyland MJ, Farrell I. Pharmacokinetics of imipenem/cilastatin in neutropenic patients with haematological malignancies. JAntimicrob Chemother 1990;25:407-12.
11. Nhylen A, Ljungberg B, Nilsson-Ehle I. Pharmacokinetics of meropen-em in febrile neutropenic patients. Swedish study group. Eur J ClinMicrobiol Infect Dis 1997;16:797-802.
12. Roberts JA, Kirkpatrick CMJ, Lipman J. Monte carlo simulations: maxi-mizing antibiotic pharmacokinetic data to optimize clinical practice forcritically ill patients. J Antimicrob Agents 2011;66:227-31.
13. Sutherland C, Nicolau DP. Development of an HPLC method for the de-termination of doripenem in humans and mouse serum. J Chromatogr B2007;853:123-6.
14. Kim A, Banevicius MA, Nicolau DP. In vivo pharmacodynamic profil-ing of doripenem against Pseudomonas aeruginosa by simulating humanexposures. Antimicrob Agents Chemother 2008;52:2497-502.
15. Spinler SA, Nawarskas JJ, Boyce EG, et al. Predictive performance often equations for estimating creatinine clearance in cardiac patients. AnnPharmacother 1998;32:1275-83.
16. Rahal JJ. Antimicrobial resistance among and therapeutic options againstgram-negative pathogens. Clin Infect Dis 2009;49(suppl 1):S4-10.
17. Nicolau DP, Kuti JL. Optimizing antibiotic-related outcomes in the criti-cally ill patient. Infect Dis Clin Prac 2005;13:158-64.
18. Jaruratanasirikul S, Limapichat T, Jullangkoon M, et al. Pharmacody-namics of meropenem in critically ill patients with febrile neutropeniaand bacteraemia. Intern J Antimicrob Agents 2011;38:231-6.
19. Lodise TP, Lomaestro BM, Drusano GL. Application of antimicrobialpharmacodynamic concepts into clinical practice: focus on β-lactam an-tibiotics. Pharmacotherapy 2006;26:320-32.
20. Vaccaro N, Umeh O, Redman R, Cirillo I. Pharmacokinetics of doripen-em 1 g administered over 4 hours in patients with ventilator-associatedpneumonia (abstract A1-018.). In: Abstracts of the 47th InterscienceConference on Antimicrobial Agents and Chemotherapy. September 12-15, 2009, San Francisco, CA.
21. Nandy P, Samtani MN, Lin R. Population pharmacokinetics of doripen-em based on data from phase 1 studies with healthy volunteers and phase2 and 3 studies with critically ill patients. Antimicrob Agents Chemother2010;54:2354-9.
22. Ariano RE, Nyhlen A, Donnelly JP, Sitar DS, Harding GKM, ZelenitskySA. Pharmacokinetics and pharmacodynamics of meropenem in febrileneutropenic patients with bacteremia. Ann Pharmacother 2005;39:32-8.doi: 10.1345/aph.1E271
23. Udy AA, Roberts JA, De Waele JJ, et al. What’s behind the failure ofemerging antibiotics in the critically ill? Intern J Antimicrob Agents2012;39:455-7.
24. Safdar A, Armstrong D. Infections in patients with hematologic neo-plasms and hematopoietic stem cell transplantation: neutropenia, hu-moral and splenic defects. Clin Infect Dis 2011;53:798-806.
EXTRACTO
Farmacocinética y Simulaciones Monte Carlo de Doripenem enPacientes con Neutropenia Febril
GE Stein, G Kulhanek, CL Smith, JL Kuti, DP Nicolau, Amy Scharmen, CFarnum, MA Tran, A Kalra, y DH Havlichek
Ann Pharmacother 2012;46:1281-6.
TRASFONDO: Doripenem es un carbapenem del grupo 2 con actividadmejorada in vitro en contra de bacteria gram-negativa incluyendoPseudomonas aeruginosa. Actualmente, hay una carencia de datosfarmacocinéticos y farmacodinámicos de doripenem en pacientes conneutropenia febril.
OBJETIVOS: Llevar a cabo una evaluación farmacocinética de dos dosisde doripenem en pacientes neutropénicos febriles y proveer estimadosde la probabilidad de alcanzar exposición efectiva al fármaco contrapatógenos Gram-negativos comunes.
MÉTODOS: Obtuvimos múltiples muestras de sangre de 12 pacientesadultos con neutropenia febril que estaban recibiendo 500 mg o1000 mgde doripenem IV por 4 horas cada 8 horas. Después de por lo menos 2dosis, concentraciones séricas fueron obtenidas en cada sujeto a las 1, 4,6, y 8 horas después de la iniciación de una dosis usando un ensayovalidado de HPLC. Los parámetros farmacocinéticos (PK) derivados deestos niveles séricos fueron usados para llevar a cabo una simulaciónMonte Carlo de 5000 pacientes contra la bacteria con concentracionesmínimas inhibitorias (MICs) de 0.008 a 64 mg/L para determinarestimados de probabilidad del tiempo de concentraciones de fármacolibre > MIC (fT>MIC).
RESULTADOS: El promedio de los parámetros PK en estos pacientes fueun volumen de distribución (Vd) de 43.9L, una constante de eliminación(k) de 0.37 h -1, una depuración total (Cl) de14.4 L/h, y un área bajo lacurva de concentración contra tiempo (AUC) 57.6 mg•h/L. Unaprobabilidad óptima para alcanzar el objetivo (40% fT>MIC) de 90%fue obtenida en contra de bacteria con MICs ≤ 2 y ≤ 4 mg/L con dosis
Pharmacokinetics of Doripenem in Febrile Neutropenia
The Annals of Pharmacotherapy n 2012 October, Volume 46 n 1285theannals.com

de 500 mg y 1000 mg respectivamente. Eventos adversos asociados condoripenem no fueron observados en estos pacientes.
CONCLUSIONES: Los resultados de este análisis de doripenem sugierenque dosis más altas, además de infusiones prolongadas, pueden sernecesarias para tratar óptimamente bacterias gram-negativa selectas (eg.P. aeruginosa) en pacientes con neutropenia febril.
Traducido por Sonia I Lugo
RÉSUMÉ
La Pharmacocinétique et la Pharmacodynamie du Doripénème chezles Patients Neutropéniques Fébriles
GE Stein, G Kulhanek, CL Smith, JL Kuti, DP Nicolau, Amy Scharmen, CFarnum, MA Tran, A Kalra, et DH Havlichek
Ann Pharmacother 2012;46:1281-6.
OBJECTIF: Le doripénème est un antibiotique de la classe des carbapénèmesqui possède une activité in vitro contre les bacilles gram négatif, incluantle Pseudomonas aeruginosa. L’objectif de cette étude était d’évaluer lapharmacocinétique du doripénème chez les patients neutropéniques fébrileset de simuler, à partir de ces données pharmacocinétiques, les dosesoptimales de l’antibiotique pouvant permettre l’atteinte de concentrationsefficaces envers différents pathogènes gram négatif.
DEVIS EXPÉRIMENTAL: Des échantillons sanguins provenant de 12 patientsadultes neutropéniques fébriles ayant reçu un minimum de 2 dosesintraveineuses de 500 mg ou de 1000 mg de doripénème administrée surune période de 4 heures à des intervalles de 8 heures, ont été prélevés. Lesconcentrations sanguines de doripénème ont été mesurées par uneméthode validée de chromatographie en phase liquide à haute performanceaux temps 1, 4, 6, et 8 heures. Une simulation Monte-Carlo de 5000patients a utilisé les paramètres pharmacocinétiques pour déterminer lesprobabilités de pourcentage de temps où les concentrations libres de dori-pénème étaient supérieures aux concentrations minimales inhibitrices(CMI).
RÉSULTATS: Les paramètres pharmacocinétiques moyens du doripénèmeont été calculés: un volume de distribution de 43.9 L, une constanted’élimination de 0.37 heure-1, une clairance totale de 14.4 L/h et une airesous la courbe de 57.6 mg-h/L. Selon la simulation Monte-Carlo, laprobabilité qu’une dose de 500 mg et de 1000 mg de doripénème puisseatteindre 90% de la cible (soit 40% du temps où les concentrations libressont supérieures aux CMI) est possible pour les bactéries ayant respective-ment une CMI ≤2 mg/L et de ≤4 mg/L. Aucun effet indésirable associé àl’administration du doripénème n’a été observé.
CONCLUSIONS: Les résultats de cette étude suggèrent que des doses de1000 mg de doripénème administrées par perfusion sur une période dequelques heures seraient nécessaires pour traiter de façon optimale lesinfections à gram négatif chez les patients neutropéniques fébriles.
Traduit par Sylvie Robert
1286 n The Annals of Pharmacotherapy n 2012 October, Volume 46 theannals.com
GE Stein et al.
For Our PatientsSummaries to Enhance Patient Education
Articles published in The Annals are summarized in uncomplicated language to make medical infor-mation more accessible to patients. Written in an easy-to-follow format, For Our Patients provides ab-stracts of articles to increase the patient’s understanding and offer healthcare providers a tool to rein-force patient counseling.
For Our Patients is available online (ForOurPatients.info), with a complete listing and links to allavailable summaries. Individual copies may be reproduced for educational purposes for distribution topatients.