Πρόληψη κ xφαλικού σ ασθνίς μ κολπική μαρμαρή ......40 45 50 55...
41
Πρόληψη εγκεφαλικού σε ασθενείς με κολπική μαρμαρυγή και νεφρική ανεπάρκεια Δρ Στέργιος Ζ. Τζήκας 17.10.2019
Transcript of Πρόληψη κ xφαλικού σ ασθνίς μ κολπική μαρμαρή ......40 45 50 55...

Πρόληψη εγκεφαλικού σε ασθενείς μεκολπική μαρμαρυγή και νεφρική ανεπάρκεια
Δρ Στέργιος Ζ. Τζήκας17.10.2019

Σύγκρουση συμφερόντων
Έχω συμμετάσχει ως ερευνητής σε κλινικές μελέτες αντιαιμοπεταλιακών φαρμάκων (ΤRΙΤΟΝ-TIMI 38, PLATO, ACCOAST) και αντιπηκτικών φαρμάκων (RELY)
Έχω λάβει τιμητικές από φαρμακευτικές εταιρίες
Astra Zeneca, Novartis, Boehringer-Ingelheim

Steffel J et al. Eur Heart J. 2018;39(16):1330-1393.
CKD Classification

Prevalence of CVD in patients with/without CKD
AFIB, atrial fibrillation; AMI, acute myocardial infarction; ASHD, atherosclerotic heart disease; CHF, congestive heart failure; CKD, chronic kidney disease; CVA/TIA, cerebrovascular accident/transient ischemic attack; CVD, cardiovascular disease; PAD, peripheral arterial disease; SCA/VA, sudden cardiac arrest and ventricular arrhythmias; VHD, valvular heart disease; VTE/PE, venous thromboembolism and pulmonary embolism.2016 Annual Data Report, Vol 1, CKD, Ch 4

Why do the Kidneys Matter in AF?
• Diabetes in the primary cause of kidney failure for 45% of patients receiving dialysis
• Patients with diabetes have a much higher risk of:
• Stroke, stroke-related dementia, recurrent stroke, stroke-related mortality
• Diabetes may increase the risk of thromboembolism in patients with AF
◆ Anticoagulant-related nephropathy (ARN) is a newly
recognized form of AKI
◆ Over-anticoagulation causes profuse glomerular
haemorrhage
• In renal biopsy, this manifests as numerous renal tubules
filled with red cells and red cell casts
◆ ARN is not a rare occurrence in the anticoagulated
patient with AF
◆ An age-associated decline in renal function has been
shown in epidemiological studies and surveys, including
both longitudinal and cross-sectional studies
◆ The rate of renal function decline varied substantially
among individuals
Kidney
function
◆ Having CKD is associated with an increased risk of
subsequently developing AF and vice versa
◆ AF has been shown to accelerate CKD progression
◆ Multiple risk factors are shared for AF and CKD:
suggesting common underlying pathogenic mechanisms:
• Obesity, hypertension, diabetes, CV disease, metabolic
syndrome
AF, atrial fibrillation; AKI, acute kidney injury; ARN, anticoagulant-related nephropathy; CV, cardiovascular; GFR, glomerular filtration rate
1. Shang W et al, PLoS One 2016;11:e155581; 2. Kiuchi M G Kidney Res Clin Pract 2018;37:103–105; 3. Soliman EZ et al, Am Heart J 2010;159:1102–1107;
4. Cavanaugh KL Clinical Diabetes 2007;25:90–97; 5. Aguiar C et al, Rev Port Cardiol 2019;38:53–63; 6. Surawan J et al, Neurol Int, 2017;9:63–69;
7. Shou J et al, J Stroke Cerebrovasc Dis, 2015;24:1961–1968; 8. Chen R et al, Am J Med Sci, 2016;351:380–386; 9. Ashburner JM et al, J Am Coll Cardiol 2016;67:239–47;
10. Brodsky S et al, J Am Soc Nephrol 2018;29:2787–2793

Survival of patients with AFib, by CKD status
2016 Annual Data Report, Vol 1, CKD, Ch 4
6

Orbit-AF Study

Orbit-AF Study

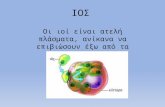
CKD & Afib increase the Risk of CV Events
◆ Patients with AF and renal
impairment:
• Higher risk of stroke/SE and
bleeding vs patients with AF
and normal renal function1
• Undertreated with warfarin vs
patients with AF and normal
renal function2,3
3.61 3.54
6.44
8.77
0
2
4
6
8
10
12
Stroke/systemicthromboembolism
Bleeding
Eve
nt
rate
pe
r 1
00
pa
tie
nt-
ye
ars
Danish registry1 (N=132,372 with NVAF; 1997–2008)
(~28% of patients received warfarin)
Without renal disease (n=127,884)
Non-end-stage CKD* (n=3587)HR=2.24
(95% CI 2.10–2.38)
p<0.001
*Defined as patients with CKD who did not require renal replacement therapy
AF, atrial fibrillation; CI, confidence interval; CKD, chronic kidney disease; HR, hazard ratio; NVAF, non-valvular AF; SE, systemic embolism
1. Olesen JB et al, N Engl J Med 2012;367:625–635; 2. Capodanno D et al, Circulation 2012;125:2649–2661; 3. Friberg L et al, Eur Heart J 2015;36:297–306
HR=1.49
(95% CI 1.38–1.59)
p<0.001

Θεραπευτικό δίλλημα
10
ΘρομβοεμβολήΑιμορραγία

Prevention of Stroke
• Diet and lifestyle changes
• Blood pressure control
• Caution against NSAIDs
• Smoking cessation
• Adjust medication
• Anticoagulation

40
45
50
55
0 1 2 3 4 5
eG
FR
(m
l/m
in/1
.73
m2)
Follow-up (years)
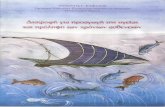
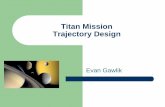
eGFR trajectory: Absolute scale*
No VKA exposure (n=7023) VKA exposure (n=7409)
VKA Exposure Accelerates Progression of CKD
Renal function decline over 5 years in patients with AF and CKD (stage 3/4)
– outcomes from a prospective, real-world database analysis
80
85
90
95
100
0 1 2 3 4 5
eG
FR
(%
)
Follow-up (years)
eGFR trajectory: Relative scale*
No VKA exposure (n=7023) VKA exposure (n=7409)
*Kidney function trajectory over time is defined as the annualized change in eGFR
AF, atrial fibrillation; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; VKA, vitamin K antagonist
Posch F et al, presented at ÖGIM 2017

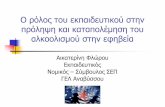
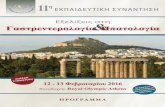
Renal Function Better Preserved in Patients Taking NOACsARISTOTLE (n=14,913)3
eGFR* changes over 12 months
eGFR at baseline: NR
ROCKET AF (n=12,612)1
CrCl changes over 21 months2
Median CrCl at baseline:1 68 ml/min
RE-LY (n=16,490)4
eGFR* changes over 30 months
Mean eGFR at baseline:4 66 ml/min
-2.57-2.46
-3.68
-5
-4.5
-4
-3.5
-3
-2.5
-2
-1.5
-1
-0.5
0
Ad
juste
d m
ean
declin
e i
n e
GF
R
(ml/m
in)
Dabigatran 110 mg
Dabigatran 150 mg
Warfarin
p<0.005
-1.42
-0.92
-5
-4.5
-4
-3.5
-3
-2.5
-2
-1.5
-1
-0.5
0
Mean
declin
e i
n e
GF
R (
ml/m
in)
Apixaban
Warfarin
-3.5
-4.3
-5
-4.5
-4
-3.5
-3
-2.5
-2
-1.5
-1
-0.5
0
Mean
ch
an
ge i
n C
rCl
sin
ce
scre
en
ing
(m
l/m
in)
Rivaroxaban
Warfarin p<0.005
p=0.01
Not intended for direct comparison.
*Calculated with CKD-EPI formula.
CrCl, creatinine clearance; eGFR, estimated glomerular filtration rate; NR, not reported; RCT, randomised controlled trial
1. Fordyce CB et al. Circulation 2016;134:37–47; 2. Fordyce CB et al. Circulation 2016;134:e532–533; 3. Hijazi Z et al. JAMA Cardiol 2016;1(4):451–460; 4. Böhm M et al. J Am Coll
Cardiol 2015;65:2481–2493.

New entity

Arteria Calcification

Arteria Calcification
Warfarin and Vascular Calcification. Poterucha TJ, Goldhaber SZ. Am J Med. 2016;129(6):635 e631-634.

Arteria Calcification
Role of different imaging modalities of vascular calcification in predicting outcomes in chronic kidney disease. Disthabanchong S, Boongird S. World J Nephrol. 2017;6(3):100-110.

No Evidence
9974 hemodialysis patients with atrial fibrillation

No Evidence
Ischemic stroke Hemorrhagic stroke

Μηχανισμός πήξης

Safety and Efficacy of NOACs in Moderate Renal Impairment
ROCKET AF1
(n=14,264)
ARISTOTLE2–4
(n=18,201)
ENGAGE AF5,6
(n=21,105)
RE-LY7,8
(n=18,113)
Specific renal dose studied
to support safety (i.e.
dosing based on renal
function only)
✓
Proportion of patients with
moderate renal impairment21%* 17%# 19%‡ 20%§
Number of patients studied
with low dose
15 mg od:
1474
2.5 mg bid:
428
30 mg od¶:
1784
110 mg bid:
6015
Number of patients on low
dose with moderate renal
impairment (% of NOAC
arm of study)
1474
(20.7%)
149ǁ
(1.6%ǁ)
1379¶
(19.6%¶)
1196
(9.9%)
NOT INTENDED FOR DIRECT COMPARISONbid, twice daily; CrCl, creatinine clearance; eGFR, estimated glomerular filtration rate; NOAC, non-vitamin K antagonist oral anticoagulant; od, once daily
*CrCl 30–49 ml/min; #eGFR ≤50 ml/min (Cockcroft–Gault); ‡CrCl ≤50 ml/min; §eGFR <50 ml/min; ǁrenal impairment defined as serum creatine levels ≥1.5 mg/dl; ¶data given for dose
adjusted arm of ‘high-dose’ (60/30) group
1. Fox KAA et al, Eur Heart J 2011;32:2387–2394; 2. Granger GB et al, N Engl J Med 2011;365:981–992; 3. Hohnloser SH et al, Eur Heart J 2012;33:2821–2830;
4. Apixaban FDA medical review; 5. Giugliano RP et al, N Engl J Med 2013;369:2093–2104; 6. Bohula et al, Circulation 2016;134:24–36;
7. Connolly SJ et al, N Engl J Med 2009;361:1139–1151; 8. Hijazi Z et al, Circulation 2014;129:961–970

Absorption and metabolism of the different NOACs
Steffel J et al. Eur Heart J. 2018;39(16):1330-1393.

Steffel J et al. Eur Heart J.2018;39(16):1330-1393.
Use of NOACs according to renal function

Apixaban in ESRD
2351 patients on apixaban and 23172 patients on warfarin

Outcomes Associated With Apixaban Use in Patients With End-Stage Kidney Disease and Atrial Fibrillation in the United States. Siontis KC et al. Circulation. 2018;138(15):1519-1529
Apixaban in ESRD

Outcomes Associated With Apixaban Use in Patients With End-Stage Kidney Disease and Atrial Fibrillation in the United States. Siontis KC et al. Circulation. 2018;138(15):1519-1529
Apixaban in ESRD

Rivaroxaban & ESRD

Permissive US labeling

Algorithm - decision making
Antithrombotic Therapy for Atrial Fibrillation: CHEST Guideline and Expert Panel Report. Lip GYH et al. Chest. 2018;154(5):1121-1201.

Last NOAC intake before elective intervention
Low risk: with a low frequency of bleeding and/or minor impact of a bleeding; high risk: with a high frequency of bleeding and/or important clinical impact.
The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur Heart J, 2018. 39(16): p. 1330-1393.

Θεραπευτικό δίλλημα
31
ΘρομβοεμβολήΑιμορραγία

LAA Occlusion

LAA Occlusion

LAA Occlusion

LAA Occlusion

Συμπεράσματα

Συμπεράσματα
• Αμφίδρομη συσχέτιση Κολπικής μαρμαρυγής & Νεφρικής ανεπάρκειας
• Προβληματική η χορήγηση NOACs σε GFR<30ml/min
• Αντικρουόμενα δεδομένα για ανταγωνιστές Vit K
• Νέα δεδομένα για Apixaban σε GFR<15ml/min
• LAA Occlusion ως εναλλακτική θεραπεία

Ευχαριστώ για την προσοχή σας!Δρ Στέργιος Ζ. Τζήκας

CV comorbidities & by CKD status, age, race, & sex
2016 Annual Data Report, Vol 1, CKD, Ch 4
39
(a) Cardiovascular comorbidities
# Patients
% Patients
Overall 66-69 70-74 75-84 85+ WhiteBlk/Af
AmOther Male Female
Cerebrovascular accident/transient ischemic attack (CVA/TIA)
Without CKD 1,102,843 7.1 3.8 5.7 9.0 11.8 7.1 7.7 5.4 7.1 7.1
Any CKD 138,176 18.2 13.8 15.4 19.0 21.3 18.1 20.4 15.5 18.5 17.9
Peripheral artery disease (PAD)
Without CKD 1,102,843 8.8 4.2 6.4 10.5 18.6 8.9 9.6 6.6 8.9 8.8
Any CKD 138,176 25.3 18.6 21.6 25.6 31.2 25.6 24.7 22.2 26.7 24.1
Atrial fibrillation (AFIB)
Without CKD 1,102,843 9.5 4.0 6.7 12.3 19.1 10.2 4.8 5.1 10.7 8.6
Any CKD 138,176 24.5 14.1 17.8 25.6 33.1 26.3 15.0 16.0 27.0 22.2
Cardiac arrest and ventricular arrhythmias (SCA/VA)
Without CKD 1,102,843 1.3 0.9 1.2 1.6 1.6 1.4 1.1 0.8 1.8 1.0
Any CKD 138,176 4.2 3.6 4.1 4.6 4.1 4.3 4.4 3.0 5.8 2.8
Venous thromboembolism and pulmonary embolism (VTE/PE)
Without CKD 1,102,843 1.2 0.8 1.0 1.5 1.9 1.3 1.5 0.7 1.2 1.3
Any CKD 138,176 4.2 3.9 3.8 4.2 4.5 4.1 5.4 3.0 4.0 4.3

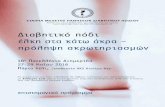
CKD is prevalent in CVD
Ix, et al., 2003; Anavekar, et al., 2004; Shlipak, et al., 2004.
0
20
40
60
CAD
CrCl ≤60 mL/min
AMI
GFR <60 mL/min
CHF
GFR ≤60 mL/min
23%
46%
33%P
ati
en
ts W
ith
CK
D (
%)

Incidence and Prevalence of End-Stage RD in the US