NUTRITION and IMMUNONUTRITION in the ICU Marcia McDougall October 2007.
69
NUTRITION and NUTRITION and IMMUNONUTRITION in the IMMUNONUTRITION in the ICU ICU Marcia McDougall Marcia McDougall October 2007 October 2007
-
Upload
richard-anderson -
Category
Documents
-
view
225 -
download
5
Transcript of NUTRITION and IMMUNONUTRITION in the ICU Marcia McDougall October 2007.

NUTRITION and NUTRITION and IMMUNONUTRITION in the ICUIMMUNONUTRITION in the ICU
Marcia McDougallMarcia McDougall
October 2007October 2007

‘‘A slender and restricted diet is A slender and restricted diet is always dangerous in chronic and in always dangerous in chronic and in
acute diseases’acute diseases’
Hippocrates 400 B.C.Hippocrates 400 B.C.


Critical IllnessCritical Illness
Heterogeneous patients Extreme physiological stress/organ
failure Acute phase response: TNF, IL-6, IL-1β Immuno-suppression: monocytes, MØ,
NK cells, T and B lymphocytes Insulin resistance: hyperglycaemia Protein loss and fat gain in muscle Impaired gut function

Consequences of malnutrition
Increased morbidity and mortality Prolonged hospital stay Impaired tissue function and wound
healing Defective muscle function, reduced
respiratory and cardiac function Immuno-suppression, increased risk
of infection CIPs lose around 2%/day muscle
protein

Scale of the problem Scale of the problem
McWhirter and Pennington 1994:McWhirter and Pennington 1994: >40% of hospital patients >40% of hospital patients
malnourished on admissionmalnourished on admission Recent Scottish data 35% Recent Scottish data 35% Estimated cost to hospitals: Estimated cost to hospitals:
£3.8bn/yr£3.8bn/yr Many ICU patients malnourished or Many ICU patients malnourished or
at risk on ICU admissionat risk on ICU admission

ICU Nutrition in the 1970s

ICU Nutrition through the ages
Overfeeding1980s

1970s: TPN - separate CH, AAs and Lipids1970s: TPN - separate CH, AAs and Lipids 2500-3000kcals/day: Lactic acidosis, 2500-3000kcals/day: Lactic acidosis,
high glucose loads, fatty livers, high high glucose loads, fatty livers, high insulin reqtinsulin reqt
Single lumen C/Lines, no pumpsSingle lumen C/Lines, no pumps Urinary urea measured, N calculatedUrinary urea measured, N calculated 1980s: Scientific studies of metabolism: 1980s: Scientific studies of metabolism:
recognition of overfeeding recognition of overfeeding 1990s: nitrogen limitation: 0.2g/kg/24hr, 1990s: nitrogen limitation: 0.2g/kg/24hr,
start of immunonutrition trialsstart of immunonutrition trials 2000s: glucose control, specific nutrients2000s: glucose control, specific nutrients

Nutrition trials in ICUNutrition trials in ICU
Small, underpoweredSmall, underpowered Heterogeneous and complex patientsHeterogeneous and complex patients Mixed nutritional statusMixed nutritional status Different feeding regimensDifferent feeding regimens Underfeeding – failure to deliver Underfeeding – failure to deliver
nutrients nutrients Overfeeding – adverse metabolic effectsOverfeeding – adverse metabolic effects HyperglycaemiaHyperglycaemia Scientific basis essentialScientific basis essential

What is the evidence in ICU?What is the evidence in ICU?
Early enteral feeding is best Early enteral feeding is best Hyperglycaemia/overfeeding are badHyperglycaemia/overfeeding are bad PN meta-analyses controversial PN meta-analyses controversial Nutritional deficit a/w worse outcomeNutritional deficit a/w worse outcome EN a/w aspiration and VAP, PN infection EN a/w aspiration and VAP, PN infection EN and PN can be used to achieve goalsEN and PN can be used to achieve goals Protocols improve delivery of feedProtocols improve delivery of feed Some nutrients show promising resultsSome nutrients show promising results

Unanswered questionsUnanswered questions
Should we aim for full calorific delivery Should we aim for full calorific delivery ASAP using EN + PN?ASAP using EN + PN?
What are the best lipids to use in PN?What are the best lipids to use in PN? What is the role of small bowel feeding?What is the role of small bowel feeding? Are probiotics helpful?Are probiotics helpful? Which patients will benefit from Which patients will benefit from
immuno-nutrition?immuno-nutrition? The future: targeted Nutrition Therapy?The future: targeted Nutrition Therapy?

Current practice - ScotlandCurrent practice - Scotland
SICS Nutrition Survey 2005-2006SICS Nutrition Survey 2005-2006 Wide variation in PN and NJ feeding useWide variation in PN and NJ feeding use Wide variation in opinions about nutritionWide variation in opinions about nutrition Lack of education about nutritionLack of education about nutrition Lack of interest from cliniciansLack of interest from clinicians Nutrition teams in 11/24 hospitals (QIS)Nutrition teams in 11/24 hospitals (QIS) Discussion between dietitians and Discussion between dietitians and
doctors limiteddoctors limited

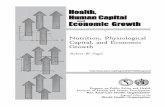
% patients receiving PN/year% patients receiving PN/year
0
5
10
15
20
25
30
E WD I F V M X A K N Q G S P H B C R
Unit

NJ feed: patient use per yearNJ feed: patient use per year
6-10/year3 units
>10/year12 units
None3 units
1-5/year6 units

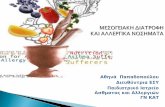
What is the maximum amount of What is the maximum amount of time an ICU patient should go time an ICU patient should go
without nutrition?without nutrition?
0123456789
10
Units
0.5-1d
1-2d
2d 3d 2-5d
5d 5-7d
Days

Nutrition QI StudyNutrition QI Study
Canadian Critical Care NetworkCanadian Critical Care Network 156 units cf CCCN guidelines156 units cf CCCN guidelines 8 Scotland, 22 UK8 Scotland, 22 UK Adequacy of ENAdequacy of EN Use of PNUse of PN Use of ImmunonutritionUse of Immunonutrition Protocols/Glycaemic control/Bed Protocols/Glycaemic control/Bed
elevationelevation


GuidelinesGuidelines

“systematically developed statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances”
U.S. Institute of Medicine
“EBM - the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients”
Sackett DL et al. BMJ 1996

What Guidelines are available?What Guidelines are available?
Canadian Critical Care Network Canadian Critical Care Network 2003/2007: Clinical Practice 2003/2007: Clinical Practice Guidelines Guidelines
ICS: Practical Management of ICS: Practical Management of Parenteral Nutrition in Critically Ill Parenteral Nutrition in Critically Ill Patients 2005Patients 2005
ESPEN: Enteral Nutrition 2006ESPEN: Enteral Nutrition 2006 NICE: Nutrition Support in Adults 2006NICE: Nutrition Support in Adults 2006

Organisation of Nutrition SupportOrganisation of Nutrition Support
3. NICE Guidelines for Nutrition Support in Adults 2006
Screen
Recognise
Treat
Oral Enteral Parenteral
Monitor & Review

ScreenScreen
Various nutritional screening toolsVarious nutritional screening tools NRS 2002, SGA, MNA Malnutrition Universal Screening Tool
from the Malnutrition Advisory Group of BAPEN
Low risk: routine clinical care, Medium risk: observe High risk: treat- ‘refer to dietitian/local
protocols’

Screening in ICUScreening in ICU
MUST not very helpful in guiding MUST not very helpful in guiding decisionsdecisions
Almost all patients require artificial Almost all patients require artificial nutrition- cannot ‘observe’nutrition- cannot ‘observe’
What about refeeding syndrome?What about refeeding syndrome? Needs adaptation using NICE GuidelinesNeeds adaptation using NICE Guidelines Adapted MUST for ICU: Uses BMI/weight Adapted MUST for ICU: Uses BMI/weight
loss/food intake + refeeding risk loss/food intake + refeeding risk assessment; linked to feeding flowchartassessment; linked to feeding flowchart

Step 3 Treat: EnteralStep 3 Treat: Enteral
use the most appropriate route of access and mode of delivery
has a functional and accessible gastrointestinal tract
if patient malnourished/at risk of malnutritiondespite the use of oral interventions and
3. NICE Guidelines for Nutrition Support in Adults 2006

Step 3 Treat: PNStep 3 Treat: PN
and has either
introduce progressively and monitor closely
if patient malnourished/at risk of malnutrition
a non-functional, inaccessible or perforated
gastrointestinal tract
inadequate or unsafe oral or enteral nutritional intake
use the most appropriate route of access and mode of delivery
3. NICE Guidelines for Nutrition Support in Adults 2006

RoutesOf feeding

REDUCED ENTERAL STIMULATION
DECREASED: Peyer’s patch leukotrienes + MAdCAM-1 T & B cells in Peyer’s patches, Lamina
propria & epithelium Reduced secretory IgA and altered
cytokines Mucosal atrophy Altered flora Decreased gastric acid Bacterial translocation

Enteral
Preserves intestinal mucosal structure and function
More physiological Relatively non-invasive Reduced risk of infectious
complications cf PN (?) Relatively cheap

NG problemsNG problems
Risk of microaspiration in ICU Risk of microaspiration in ICU Risk of displacement Risk of displacement High gastric aspirates with opioids, High gastric aspirates with opioids,
sepsis, electrolyte imbalancessepsis, electrolyte imbalances Reaching goals uncommon Reaching goals uncommon PEG/gastrostomy feeding for long-PEG/gastrostomy feeding for long-
term >4 weeksterm >4 weeks

Jejunal FeedingJejunal Feeding
Insertion Surgical jejunostomy: at
laparotomy May reduce incidence of aspiration Sometimes increases dose of EN
given over NG Indications

Parenteral NutritionParenteral Nutrition
GI tract not functional GI tract not functional GI tract cannot be accessed GI tract cannot be accessed Inadequate enteral nutrition <80% 3 Inadequate enteral nutrition <80% 3
daysdays Do not delay nutrition in Do not delay nutrition in
malnourishedmalnourished Keep 10ml/hr EN if possibleKeep 10ml/hr EN if possible

Supplemental PNSupplemental PN
Optimize EN first if possible (??) Optimize EN first if possible (??) Villet: Villet: Clin NutrClin Nutr 24, 2005: Caloric debt 24, 2005: Caloric debt
a/w increased LOS, vent days and a/w increased LOS, vent days and complications complications
Need trial to compare early supplemental Need trial to compare early supplemental PN and early EN with early EN onlyPN and early EN with early EN only
North America/Europe split over use of PNNorth America/Europe split over use of PN Unanswered questionsUnanswered questions

How much to give in ICU?How much to give in ICU? Schofield equation/Harris Benedict Schofield equation/Harris Benedict e.g. for 65 year old woman: BMR = (9.2x e.g. for 65 year old woman: BMR = (9.2x
weight in kg) + 687, = requirement in weight in kg) + 687, = requirement in Kcal/24hr Kcal/24hr
Add Activity and Stress factors e.g. 10% Add Activity and Stress factors e.g. 10% for bedbound + 20-60% for sepsis/burnsfor bedbound + 20-60% for sepsis/burns
For 65kg woman ventilated woman with For 65kg woman ventilated woman with sepsis: 1670 Kcal = approx 25 sepsis: 1670 Kcal = approx 25 Kcal/kg/24hrKcal/kg/24hr
No dietitian? Rough guide: 25 Kcal/kg/day No dietitian? Rough guide: 25 Kcal/kg/day total energy. Increase to 30 as patient total energy. Increase to 30 as patient improvesimproves

How much to give?How much to give?
0.2g/Kg/day of Nitrogen (1.25g/kg/day protein)0.2g/Kg/day of Nitrogen (1.25g/kg/day protein) 30 – 35ml fluid/kg/24 hours baseline 30 – 35ml fluid/kg/24 hours baseline Add 2-2.5ml/kg/day of fluid for each degree of Add 2-2.5ml/kg/day of fluid for each degree of
temperature temperature Account for excess fluid lossesAccount for excess fluid losses Adequate electrolytes, micronutrients, Adequate electrolytes, micronutrients,
vitaminsvitamins Avoid overfeeding Avoid overfeeding Obesity: feed to BMR, add stress factor only if Obesity: feed to BMR, add stress factor only if
severe i.e. burns/traumasevere i.e. burns/trauma

Refeeding SyndromeRefeeding Syndrome
Prisoners of war 1944-5, 1944: Prisoners of war 1944-5, 1944: conscientious objectors in USA studiedconscientious objectors in USA studied
Starvation: early use of glycogen stores Starvation: early use of glycogen stores for AAs - gluconeogenesis; 72 hrs: FFA for AAs - gluconeogenesis; 72 hrs: FFA oxidation; use of FFAs and ketones for oxidation; use of FFAs and ketones for energy source, low insulinenergy source, low insulin
Atrophy of organs, reduced lean body Atrophy of organs, reduced lean body massmass

Refeeding syndromeRefeeding syndrome CH Feeding: shift to CH metabolism: insulin releaseCH Feeding: shift to CH metabolism: insulin release Stimulates POStimulates PO44
2-2- and K and K++ shift into cells. PO shift into cells. PO442-2- drops drops
lower (ATP, 2-3DPG). Mglower (ATP, 2-3DPG). Mg2+2+ loss in urine 2 loss in urine 2o o lowlow POPO442-2-
(Na+K(Na+K++ATPase)ATPase) May get Lactic acidosis 2May get Lactic acidosis 2o o conversion of pyruvate to
lactate NaNa++ and H and H22O shift out of cells – oedema; ECF O shift out of cells – oedema; ECF
expansion 2expansion 2oo reduced excretion of Na reduced excretion of Na++ and H and H22O;O; Hyperinsulinaemia is antinatriuretic Hyperinsulinaemia is antinatriuretic Protein synthesis increases cellr demand for POProtein synthesis increases cellr demand for PO44
2-2- and and KK++
Thiamine deficiency occurs (co-factor in CH Thiamine deficiency occurs (co-factor in CH metabolism): encephalopathymetabolism): encephalopathy

Refeeding Syndrome in ICURefeeding Syndrome in ICU
Unlikely to be a clear diagnosisUnlikely to be a clear diagnosis Many deleterious effects: oedema, Many deleterious effects: oedema,
arrhythmias, pulmonary oedema, cardiac arrhythmias, pulmonary oedema, cardiac decompensation, respiratory weakness, decompensation, respiratory weakness, fits, hypotension, leukocyte dysfunction, fits, hypotension, leukocyte dysfunction, diarrhoea, coma, rhabdomyolysis, sudden diarrhoea, coma, rhabdomyolysis, sudden deathdeath
Screen: nutritional history and electrolytesScreen: nutritional history and electrolytes Remember in HDU patients/malnourished Remember in HDU patients/malnourished
ward patientsward patients Poor awareness among doctors!Poor awareness among doctors!

Risk of re-feeding syndromeRisk of re-feeding syndrome
TwoTwo or more of the following: or more of the following: BMI less than 18.5 kg/mBMI less than 18.5 kg/m2 2 (<16)(<16) unintentional weight loss greater than unintentional weight loss greater than
10% within the last 3-6 months (>15%)10% within the last 3-6 months (>15%) little or no nutritional intake for more than little or no nutritional intake for more than
5 days (>10)5 days (>10) Hx alcohol abuse or drugs including Hx alcohol abuse or drugs including
insulin, chemotherapy, antacids or insulin, chemotherapy, antacids or diureticsdiuretics
(Critically low levels of PO(Critically low levels of PO442-2-, K, K++ and Mg and Mg2+)2+)

Managing refeeding problemsManaging refeeding problems
provide Thiamine/multivitamin/trace provide Thiamine/multivitamin/trace element supplementationelement supplementation
start nutrition support at 5-10 start nutrition support at 5-10 kcal/kg/day kcal/kg/day
increase levels slowlyincrease levels slowly restore circulatory volume restore circulatory volume monitor fluid balance and clinical monitor fluid balance and clinical
statusstatus replace POreplace PO44
2-2-, K, K++ and Mg and Mg2+2+
ReduceReduce feeding rate if problems arisefeeding rate if problems ariseNICE Guidelines for Nutrition Support in Adults 2006

IMMUNONUTRITIONIMMUNONUTRITIONHuman EvolutionHuman Evolution
No ambulances/hospitals First 72 hours after severe illness or
injury crucial Little hope of survival past this; not
desirable Significant stores of stress substrates
not necessary e.g. glutamine

The Immune SystemThe Immune System
A complex and interactive biological system A complex and interactive biological system that coordinates the detection, destruction that coordinates the detection, destruction and elimination of any foreign material or and elimination of any foreign material or organism entering the body.organism entering the body.
Oxidants: cytokines, NFkB, genes, inflamOxidants: cytokines, NFkB, genes, inflamnn
Nutrients: glutamine, FFAs, proteinNutrients: glutamine, FFAs, protein Glutathione: oxidant defenceGlutathione: oxidant defence Anti-inflammatory molecules: attenuationAnti-inflammatory molecules: attenuation

Critical IllnessCritical Illness
Sepsis: Battle between inflammatory Sepsis: Battle between inflammatory response and microbes/toxinsresponse and microbes/toxins
Trauma: SIRS to non-infectious insultTrauma: SIRS to non-infectious insult Minor insult: inflammatory response winsMinor insult: inflammatory response wins Major insult: with support (antibiotics, Major insult: with support (antibiotics,
fluids) body may be able to fight insult fluids) body may be able to fight insult but in severe insult inflammatory but in severe insult inflammatory response continues and causes organ response continues and causes organ damage, f/b immune paresis and 2damage, f/b immune paresis and 2°° infection; deathinfection; death

Inflammation, organ failure
Inflammationand resolution
THE ICU GAMBLETHE ICU GAMBLEHow to tip the scales?How to tip the scales?
DEATH
LIFE
DISABILITY

Critical IllnessCritical Illness
Small reductions in mortality over yearsSmall reductions in mortality over years Increasing problems with infectionIncreasing problems with infection Advances in treatment have limited Advances in treatment have limited
effectseffects Pathophysiology complexPathophysiology complex The future: replacement of the body’s
own ‘stress substrates’ Could immunonutrition be the most Could immunonutrition be the most
important area in critical care important area in critical care development?development?

Failed ICU strategiesFailed ICU strategies
Anti-TNF antibodiesAnti-TNF antibodies Steroids in sepsis – recent work Steroids in sepsis – recent work
suggests little effectsuggests little effect NO synthetase inhibitor: increased NO synthetase inhibitor: increased
mortalitymortality ??? Activated protein C - ??? Activated protein C -
controversialcontroversial

Immuno/PharmaconutritionImmuno/Pharmaconutrition
‘Disease-modulating’ nutrients Attenuate metabolic response Prevent oxidant stress Favourably modulate immune
response Probiotics to alter gut environment Glycaemic control: keep blood
glucose <8mmol/l: reduces infections and organ failures

GlutamineGlutamine
Non-essential amino acid – ‘conditionally Non-essential amino acid – ‘conditionally essential’ in sepsis/major traumaessential’ in sepsis/major trauma
Vital to gut, immune cells, and kidney Serves as metabolic fuel; precursor to DNA
synthesis BUT Levels drop after injury, exercise and BUT Levels drop after injury, exercise and
stress. Very low in critical illness first 72 hoursstress. Very low in critical illness first 72 hours Glutamine deficiency at onset of critical
illness/sepsis correlated with increased mortality

Potential Beneficial Effects of Glutamine
Fuel forFuel forEnterocytesEnterocytes
Fuel forFuel forLymphocytesLymphocytes
Nuclotide Nuclotide SynthesisSynthesis
Maintenance ofMaintenance ofIntestinalIntestinalMucosal BarrierMucosal Barrier
Maintenance ofMaintenance ofLymphocyteLymphocyteFunctionFunction
Preservation Preservation of TCA Functionof TCA Function
Decreased FreeRadical availability (Anti-inflammatory action)
GlutathioneGlutathioneSynthesisSynthesis
GLNGLNpoolpool
GlutamineTherapy
Enhanced HeatEnhanced Heat Shock ProteinShock Protein
Anti-cataboliceffect
Preservation of Muscle mass
Reduced Reduced TranslocationTranslocationEnteric BacteriaEnteric Bacteriaor Endotoxinsor Endotoxins
Reduction ofReduction ofInfectious Infectious complicationscomplications
Inflammatory Cytokine Inflammatory Cytokine AttenuationAttenuation
NF-kBNF-kB??
Preserved CellularEnergetics- ATP content
GLNGLNPoolPool
Critical IllnessCritical Illness
Enhanced insulin sensitivity
Wischmeyer PE, Curr Opin Clin Nutr MetabCare 6: 217-222, 2003

Glutamine trialsGlutamine trials
Modest reduction in mortality/infections Modest reduction in mortality/infections in 9 studies of glutamine-supplemented in 9 studies of glutamine-supplemented PNPN
Improvement in morbidity and Improvement in morbidity and mortality in 2 studies of enteral mortality in 2 studies of enteral glutamine in burns and trauma patientsglutamine in burns and trauma patients
CCCN recommend enteral glutamine CCCN recommend enteral glutamine for burns and trauma and IV glutamine for burns and trauma and IV glutamine to be given with parenteral nutritionto be given with parenteral nutrition
SIGNET and REDOXs awaitedSIGNET and REDOXs awaited

PROBIOTICS
Live micro-organisms which when administered in adequate amounts confer a health benefit on the host
Bioecological control: Supply viable Bioecological control: Supply viable beneficial bacteria, or a substrate beneficial bacteria, or a substrate which enhances specific beneficial which enhances specific beneficial bacteria, instead of trying to eliminate bacteria, instead of trying to eliminate the pathogenthe pathogen

ProbioticsProbiotics Critical illness causes virulence of gut Critical illness causes virulence of gut
bacteria; treatment worsens gut bacteria; treatment worsens gut function function
Probiotics inhibit growth of pathogenic Probiotics inhibit growth of pathogenic enteric bacteria enteric bacteria
block epithelial invasion by pathogensblock epithelial invasion by pathogens eliminate pathogenic toxins eliminate pathogenic toxins improve mucosal barrier function improve mucosal barrier function enhance T-cell and macrophage enhance T-cell and macrophage
functionfunction reduce production of TNF and NFkBreduce production of TNF and NFkB

ProbioticsProbiotics
Potential to cut VAP and C. diffPotential to cut VAP and C. diff BUT: safety concernsBUT: safety concerns dosagedosage which bacteria to use which bacteria to use viability in the gutviability in the gut storage issuesstorage issues unforeseen effectsunforeseen effects More research requiredMore research required

ArginineArginine
‘‘Conditionally essential’ amino acid Conditionally essential’ amino acid derived from glutamine and citrulline derived from glutamine and citrulline
For protein synthesis, cell division, NO, For protein synthesis, cell division, NO, urea cycle, creatine phosphate (ATP)urea cycle, creatine phosphate (ATP)
Stimulates hormone releaseStimulates hormone release Deficiency:Deficiency: Immune suppression, ↓TH2
cell function, free radical formation Abnormal microperfusion Abnormal wound healing

SepsisSepsis
Sepsis: iNOS, dendritic cells, IL-1, IL-6Sepsis: iNOS, dendritic cells, IL-1, IL-6 TH1 cytokine profile: IL-TH1 cytokine profile: IL-
2,TNF,interferon-2,TNF,interferon-үү Arginine deficiency not severe in
sepsis Little drop in plasma arginine levels CCCN: not recommended (harm?)

TraumaTrauma
Trauma: IL-10, poor antigen presentation, Trauma: IL-10, poor antigen presentation, TH2 cytokine profile: IL-4, IL-13TH2 cytokine profile: IL-4, IL-13
Pathologic release of arginase from myeloid Pathologic release of arginase from myeloid suppressor cells, hepatocytes, RBCssuppressor cells, hepatocytes, RBCs
Significant drop in arginine levels in trauma CCCN: not recommended – future role? Pre-operative patients, cancer, sickle cell,
haemolytic anaemia, PIH

PUFAsPUFAs
Arachidonic Acid: COX and LOX precursor: Omega-
6 ү-Linoleic acid (GLA) – borage oil Fish oils: Eicosapentanoic acid
(EPA) and Docosahexanoic acid (DHA): Omega-3 FAs

Dietary LipidsDietary Lipids
Ratios in paleolithic diet Ratios in paleolithic diet ωω-6:-6:ωω-3 1:1-3 1:1 Current Western diet 16.7:1Current Western diet 16.7:1 Current UK PN Soybean oil base 7:1 (LCT)Current UK PN Soybean oil base 7:1 (LCT) New PN (‘SMOF’) 2.5:1 (LCT/MCT)New PN (‘SMOF’) 2.5:1 (LCT/MCT) Membrane composition depends on dietMembrane composition depends on diet AA arises from GLAAA arises from GLA AA, DHA and EPA are present in AA, DHA and EPA are present in
inflammatory cell membrane phospholipidsinflammatory cell membrane phospholipids Hydrolysis of FAs by phospholipase to Hydrolysis of FAs by phospholipase to
mediatorsmediators

Mechanisms of ActionMechanisms of Action
ωω-3s -3s EPA/DHA are incorporated quickly into EPA/DHA are incorporated quickly into cell membrane: inhibit cell membrane: inhibit ωω-6 activity -6 activity
Promote synthesis of low activity PGs and LTsPromote synthesis of low activity PGs and LTs Decrease expression of adhesion moleculesDecrease expression of adhesion molecules Inhibits monocyte prodInhibits monocyte prodnn of pro-inflamm of pro-inflamm
cytokinescytokines Decreases NFkB, increases lymphocyte Decreases NFkB, increases lymphocyte
apoptosisapoptosis Decreases pro-inflammatory gene expressionDecreases pro-inflammatory gene expression Lipoxins, resolvins and protectinsLipoxins, resolvins and protectins

3 Studies: OXEPA3 Studies: OXEPA
Patients with ARDS fed with GLA, EPA and antioxidants had a reduction in pulmonary neutrophils
Improvement in oxygenation Decrease in ventilator days Decrease in ICU and hospital days Gadek, Singer, Pontes-Arruda
(sepsis)

Omega-3 Fatty AcidsOmega-3 Fatty Acids
BUTBUT Control group had high fat diet – bad?Control group had high fat diet – bad? Was it the FAs or the antioxidants or both?Was it the FAs or the antioxidants or both? CCCN – consider in ARDS i.e. OXEPA mixCCCN – consider in ARDS i.e. OXEPA mix Other researchers: not enough evidence Other researchers: not enough evidence Science makes sense; works in IHD, PVD Science makes sense; works in IHD, PVD

Anti-oxidantsAnti-oxidants
Normal state: reduction > oxidation Normal state: reduction > oxidation Acute stress: injury/sepsis causes acute Acute stress: injury/sepsis causes acute
dysregulation: ROS/RNOS formed dysregulation: ROS/RNOS formed Mitochondria are both sources and Mitochondria are both sources and
targetstargets Observational studies: anti-oxidant Observational studies: anti-oxidant
capacity inversely correlated with capacity inversely correlated with disease severity due to depletion disease severity due to depletion during oxidative stressduring oxidative stress
REDUCTION
OXIDATION

Reactive Oxygen Species OReactive Oxygen Species O--, NO, NO--
Positive actions: Bactericidal Regulation of
vascular tone Cell signalling
But mostly detrimental:
Cell injury (ischaemia /reperfusion)
DNA, Lipids, ProteinsOrgan dysfunction Lungs, Heart, Kidney Liver, Blood, Brain
OXIDATION
REDUCTION

ACUTE INSULTACUTE INSULT
Exacerbation Exacerbation of cell and of cell and
tissue injurytissue injury
Inflammatory mediators
ROS/RNOS
Healing/repair/defence

AntioxidantsAntioxidants
Glutathione, Vitamins A, C and EGlutathione, Vitamins A, C and E Zinc, copper, manganese, iron, Zinc, copper, manganese, iron,
seleniumselenium Already added to feedsAlready added to feeds Should we give extra CCCN – ‘consider’Should we give extra CCCN – ‘consider’ Results of SIGNET and REDOXs awaitedResults of SIGNET and REDOXs awaited Oxidative stress in critically ill patients
contributes to organ damage / malignant inflammation

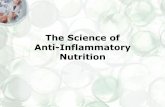
Elective
SurgeryCritically Ill
General Septic Trauma Burns Acute Lung Injury
Arginine Benefit No benefit Harm(?)
(Possible benefit)
No benefit
No benefit
Glutamine Possible Benefit
PN Beneficial
Recom-mend
… EN Possibly
Beneficial:
Consider
EN Possibly
Beneficial:
Consider
…
Omega 3 FFA
… … … … … Recom-mend
Anti-oxidants
… Consider … … … …
Which Nutrient for Which Population?
Canadian Clinical Practice Guidelines JPEN 2003;27:355

Immunonutrition- the future?Immunonutrition- the future?
The right nutrient or combination Correct dose The appropriate timing The right patient and circumstance The appropriate assessment of
efficacy Balance between harm and benefit of
the immune response ?? Nutrient-gene interactions

NowNow
More & better trials of ImmunonutritionMore & better trials of Immunonutrition Early PN supplementation trialEarly PN supplementation trial Meanwhile: the basics- screening, Meanwhile: the basics- screening,
reaching goals, protocols, refeedingreaching goals, protocols, refeeding HDU feeding HDU feeding Profile of Nutrition: Education, dialogueProfile of Nutrition: Education, dialogue FundingFunding

MaintainsMaintainsStimulates Stimulates the environmentthe environmentdefencesdefences
FEEDINGFEEDING
Provides Provides energyenergy