Acute fatty liver versus HELLP syndrome in obstetric ICU: why and how to differentiate? BY...
44
Acute fatty liver versus Acute fatty liver versus HELLP syndrome in HELLP syndrome in obstetric ICU: obstetric ICU: why and how to why and how to differentiate? differentiate? BY BY Bahaa-El-Din Ewees MD Bahaa-El-Din Ewees MD
-
Upload
layne-flowers -
Category
Documents
-
view
217 -
download
1
Transcript of Acute fatty liver versus HELLP syndrome in obstetric ICU: why and how to differentiate? BY...
Acute fatty liver versus Acute fatty liver versus HELLP syndrome in HELLP syndrome in
obstetric ICU:obstetric ICU: why and how to why and how to
differentiate?differentiate?
BYBY
Bahaa-El-Din Ewees MDBahaa-El-Din Ewees MD
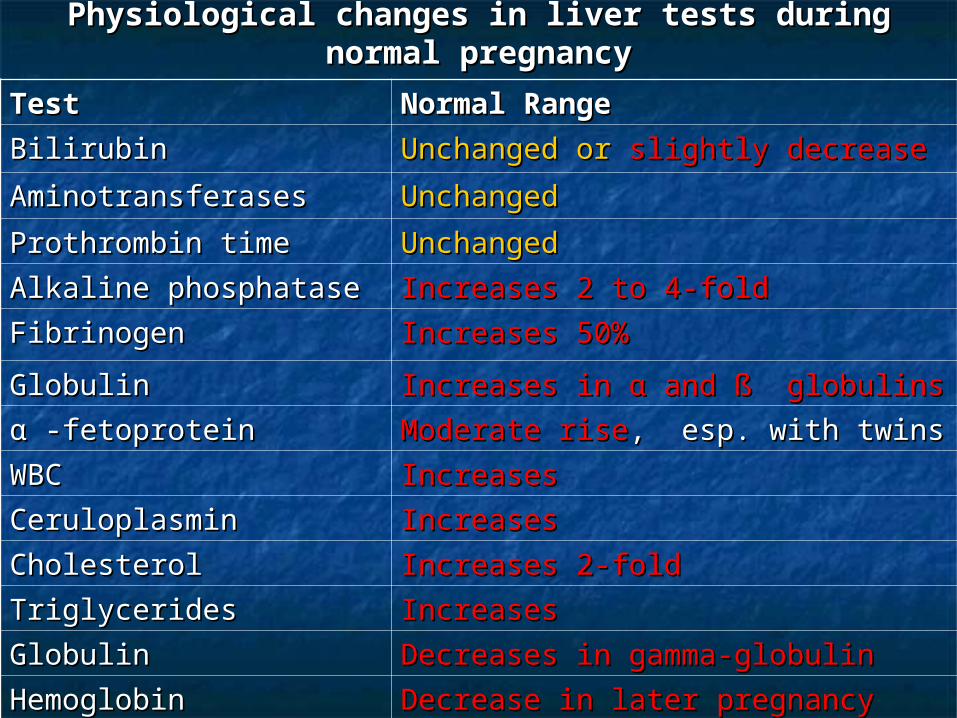
Physiological changes in liver tests during normal Physiological changes in liver tests during normal pregnancypregnancy
TestTest Normal RangeNormal Range
BilirubinBilirubin Unchanged or Unchanged or slightly decreaseslightly decrease
AminotransferasesAminotransferases UnchangedUnchanged
Prothrombin timeProthrombin time UnchangedUnchanged
Alkaline phosphataseAlkaline phosphatase Increases 2 to 4-foldIncreases 2 to 4-fold
FibrinogenFibrinogen Increases 50%Increases 50%
GlobulinGlobulin Increases in α and ß globulinsIncreases in α and ß globulins
α -fetoproteinα -fetoprotein Moderate riseModerate rise, esp. with twins, esp. with twins
WBCWBC IncreasesIncreases
CeruloplasminCeruloplasmin IncreasesIncreases
CholesterolCholesterol Increases 2-foldIncreases 2-fold
TriglyceridesTriglycerides IncreasesIncreases
GlobulinGlobulin Decreases in gamma-globulinDecreases in gamma-globulin
HemoglobinHemoglobin Decrease in later pregnancyDecrease in later pregnancy
Abnormal liver function tests Abnormal liver function tests occur inoccur in 3 - 5%3 - 5% of pregnancies for of pregnancies for different reasonsdifferent reasons
Liver diseases in pregnancyLiver diseases in pregnancy
liver disorders that occur liver disorders that occur only inonly in the the setting of setting of pregnancypregnancy
liver disorders that occur liver disorders that occur coincidentallycoincidentally with pregnancywith pregnancy
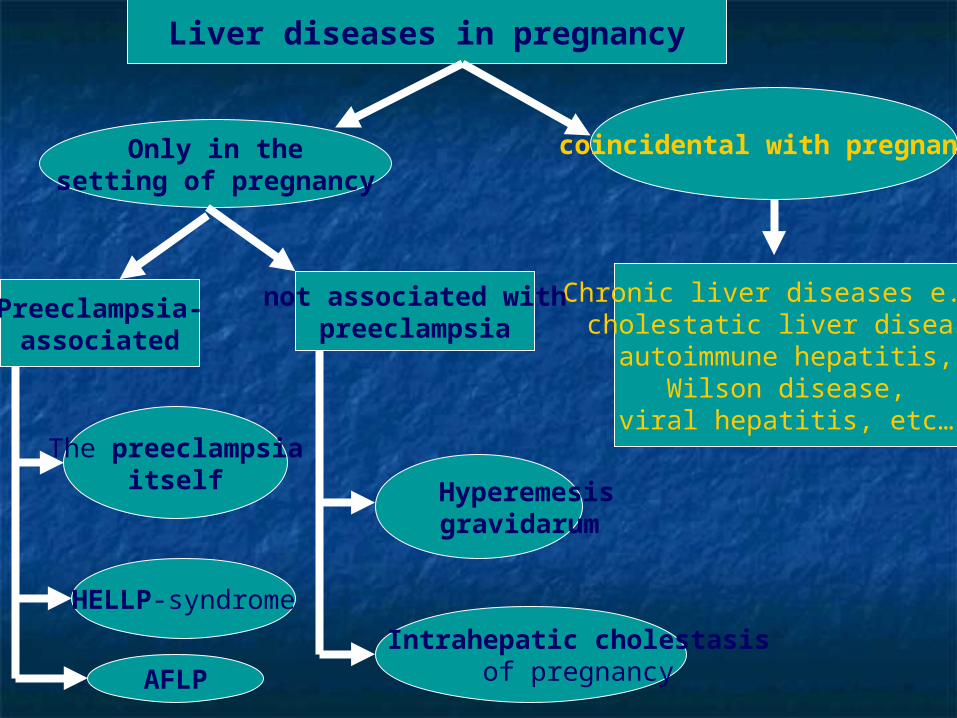
Liver diseases in pregnancy
Only in thesetting of pregnancy
coincidental with pregnancy
Preeclampsia-associated
Chronic liver diseases e.g.: cholestatic liver disease,
autoimmune hepatitis,Wilson disease,
viral hepatitis, etc…
not associated withpreeclampsia
The preeclampsiaitself
HELLP-syndrome
AFLP
Hyperemesisgravidarum
Intrahepatic cholestasisof pregnancy
HELLP syndromeHELLP syndrome
Severe preeclampsia is complicated in Severe preeclampsia is complicated in 2-12% of cases (0.2-0.6% of all 2-12% of cases (0.2-0.6% of all pregnancies) by hemolysis (pregnancies) by hemolysis (HH), ), elevated liver tests (elevated liver tests (ELEL), and low ), and low platelet count (platelet count (LPLP), the ), the HELLP HELLP syndromesyndrome..
Etiology:Etiology: microangiopathic hemolytic microangiopathic hemolytic anemia anemia ++ vascular endothelial injury vascular endothelial injury fibrin deposition in blood vessels fibrin deposition in blood vessels ++ platelet activation & consumption, platelet activation & consumption, small to diffuse areas of small to diffuse areas of hemorrhage and necrosis hemorrhage and necrosis large hematomas large hematomas ++ capsular tears capsular tears ++ intraperitoneal bleeding.intraperitoneal bleeding.
Clinical Features and Clinical Features and DiagnosisDiagnosis
Most patients: 27 - 36 weeks’ Most patients: 27 - 36 weeks’ gestation,gestation,
butbut 25% in postpartum period. 25% in postpartum period.
Can occur with any parity and age Can occur with any parity and age butbut commoner in white, multiparous commoner in white, multiparous & older pts.& older pts.
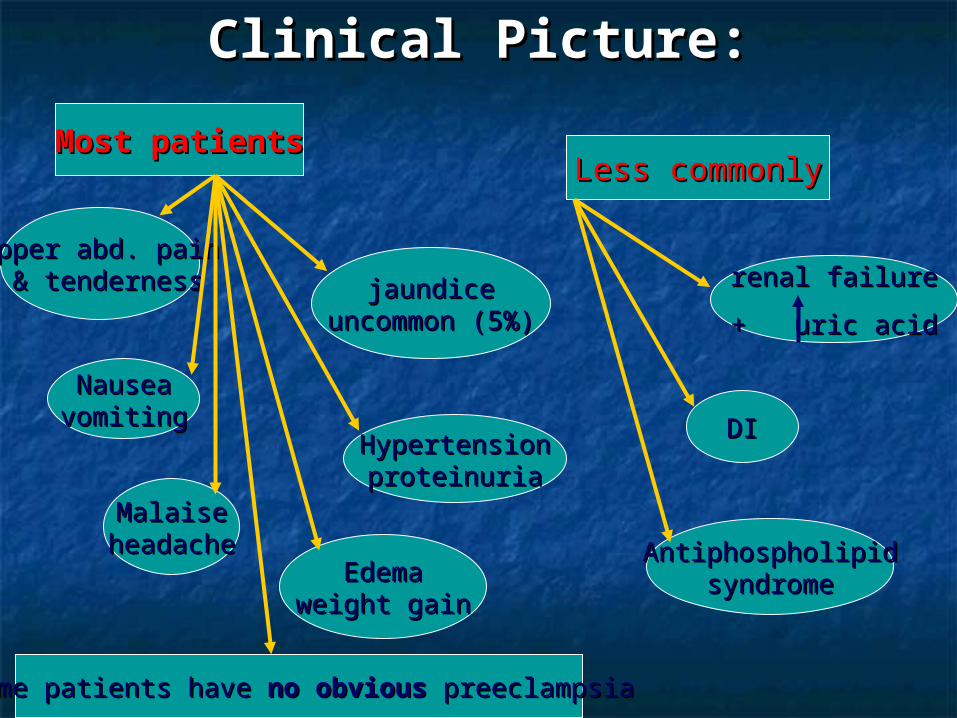
Clinical Picture:Clinical Picture:
Most patientsMost patientsLess commonlyLess commonly
upper abd. painupper abd. pain & tenderness& tenderness
NauseaNauseavomitingvomiting
MalaiseMalaiseheadacheheadache
EdemaEdemaweight gainweight gain
jaundicejaundiceuncommon (5%)uncommon (5%)
HypertensionHypertensionproteinuriaproteinuria
renal failurerenal failure
+ uric acid+ uric acid
DIDI
AntiphospholipidAntiphospholipidsyndromesyndrome
some patients have some patients have no obviousno obvious preeclampsia preeclampsia
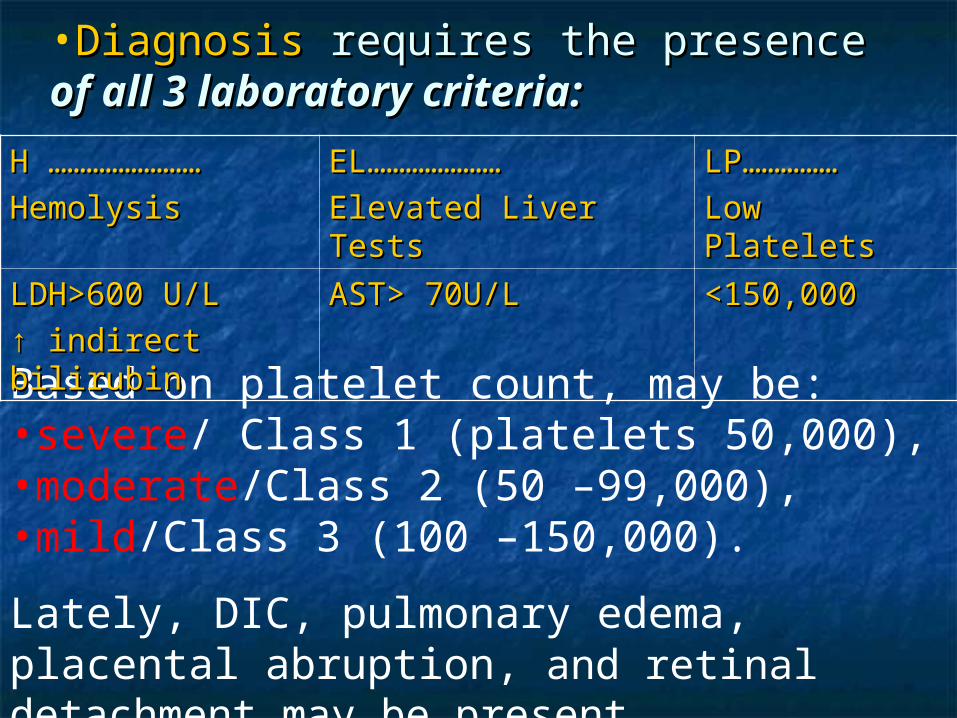
•DiagnosisDiagnosis requires the presence requires the presence of of all 3 laboratory criteria:all 3 laboratory criteria:
Based on platelet count, may be:•severe/ Class 1 (platelets 50,000),•moderate/Class 2 (50 –99,000),•mild/Class 3 (100 –150,000).
Lately, DIC, pulmonary edema, placental abruption, and retinal detachment may be present.
H ……………………H ……………………
Hemolysis Hemolysis EL…………………EL…………………
Elevated Liver Tests Elevated Liver Tests LP……………LP……………
Low Platelets Low Platelets
LDH>600 U/LLDH>600 U/L
↑ ↑ indirect bilirubin indirect bilirubin AST> 70U/L AST> 70U/L <150,000 <150,000
AminotransferaseAminotransferase: variable, from mild to : variable, from mild to 10 – 20 fold,10 – 20 fold,
BilirubinBilirubin: usually < 5 mg/dL.: usually < 5 mg/dL.
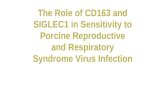
Liver CTLiver CT: : subcapsular hematomas,subcapsular hematomas, intra-parenchymal hemorrhage, or infarctionintra-parenchymal hemorrhage, or infarction hepatic rupture.hepatic rupture.
HistologicallyHistologically: focal hepatocyte necrosis, : focal hepatocyte necrosis, periportal hemorrhage, and fibrin deposits.periportal hemorrhage, and fibrin deposits.
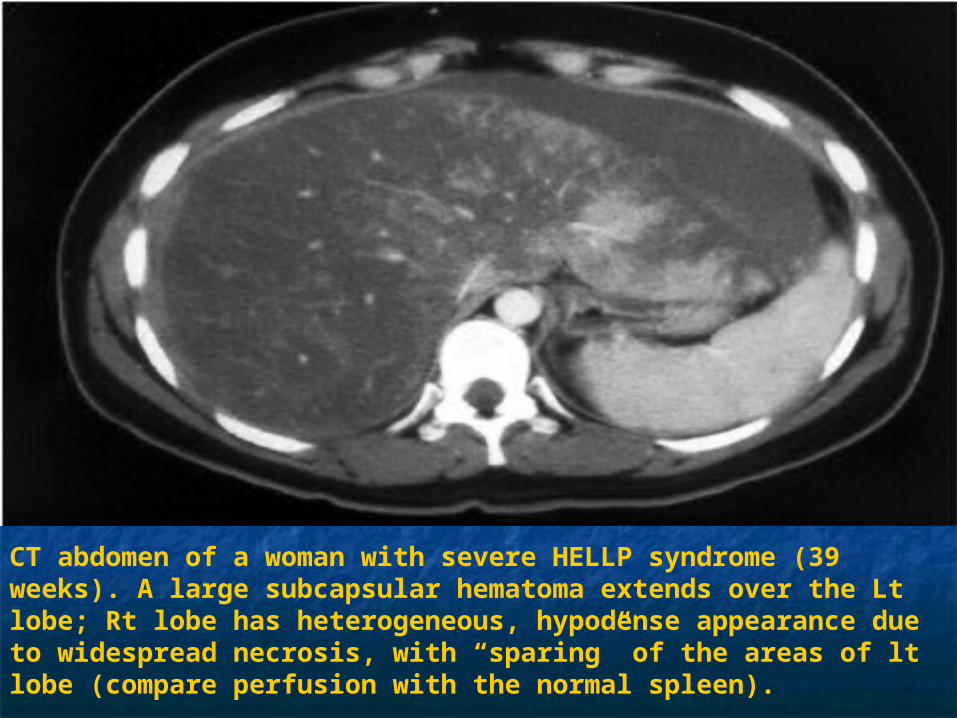
CT abdomen of a woman with severe HELLP syndrome (39 weeks). A large subcapsular hematoma extends over the Lt lobe; Rt lobe has heterogeneous, hypodense appearance due to widespread necrosis, with “sparing” of the areas of lt lobe (compare perfusion with the normal spleen).

TreatmentTreatment

Hospitalization & ICU careHospitalization & ICU care for: for:o antepartum stabilization of BP and DIC,antepartum stabilization of BP and DIC,o seizure prophylaxis,seizure prophylaxis,o fetal monitoring.fetal monitoring.
pregnancy is > 34 wk gestational age
24-34 wk
immediate induction
corticosteroids for 48 h(fetal lung maturity)
delivery
The only definitive treatment is deliveryThe only definitive treatment is delivery
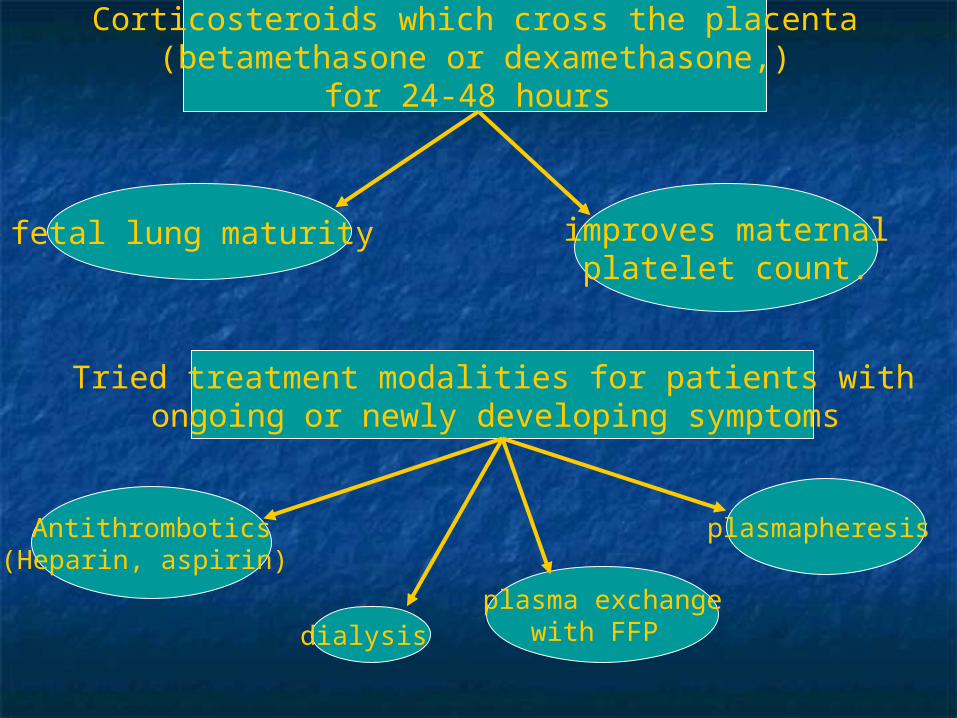
Corticosteroids which cross the placenta(betamethasone or dexamethasone,)
for 24-48 hours
fetal lung maturity improves maternalplatelet count.
Tried treatment modalities for patients with ongoing or newly developing symptoms
Antithrombotics(Heparin, aspirin)
plasmapheresis
plasma exchangewith FFP dialysis
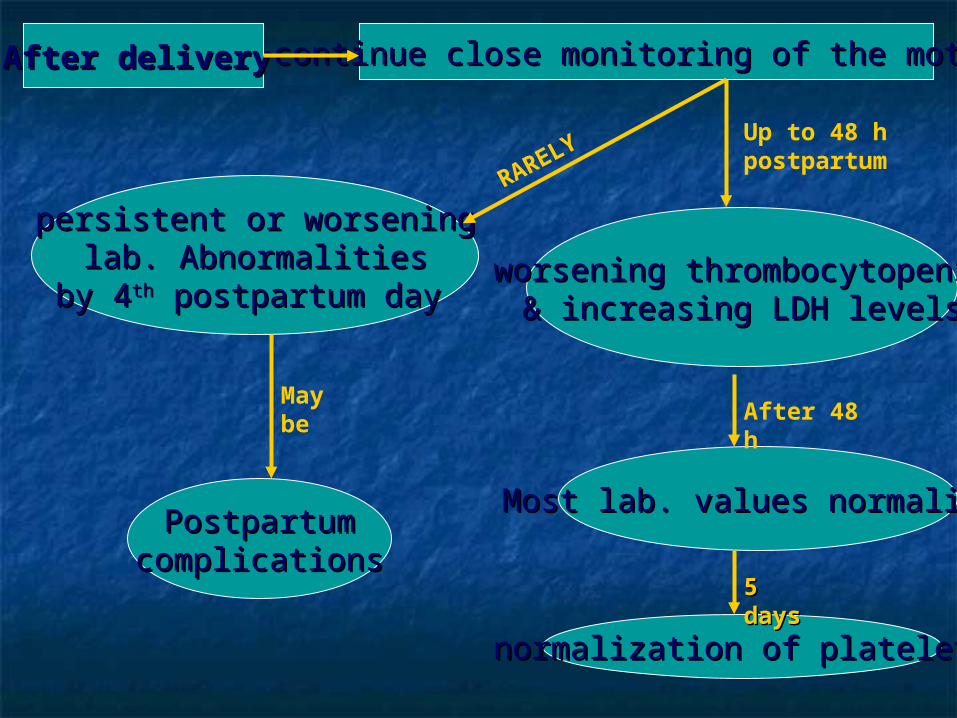
After deliveryAfter delivery continue close monitoring of the mothercontinue close monitoring of the mother
Up to 48 h postpartum
worsening thrombocytopeniaworsening thrombocytopenia& increasing LDH levels& increasing LDH levels
Most lab. values normalizeMost lab. values normalize
After 48 h
persistent or worseningpersistent or worseninglab. Abnormalitieslab. Abnormalities
by 4by 4thth postpartum day postpartum day
PostpartumPostpartumcomplicationscomplications
May be
normalization of plateletsnormalization of platelets
5 5 daysdays
RARELY

Fate & complicationsFate & complications
ReportedReported maternal mortalitymaternal mortality isis 1%1%
Perinatal mortalityPerinatal mortality rate ranges rate ranges fromfrom 7%-22%7%-22% and may be due to:and may be due to:• premature detachment of placenta,premature detachment of placenta,• intrauterine asphyxia,intrauterine asphyxia,• prematurity.prematurity.

Other complicationsOther complications::
No long-term effect on renal No long-term effect on renal function noted.function noted.
•abruptio abruptio placentaeplacentae•DICDIC•ARFARF•ARDSARDS
•pulmonary pulmonary edemaedema
•strokestroke•liver failureliver failure•hepatic hepatic infarctioninfarction
Recurrence Recurrence : : Subsequent Subsequent pregnancies carry a high risk of pregnancies carry a high risk of complications complications • pre-eclampsia, pre-eclampsia, • recurrence, recurrence, • prematurity, prematurity, • IUGR, IUGR, • abruptio placentae, abruptio placentae, • perinatal mortality. perinatal mortality.
Acute fatty liverAcute fatty liver
Acute fatty liver of pregnancy (Acute fatty liver of pregnancy (AFLPAFLP) is a) is a rarerare butbut seriousserious maternal illness that maternal illness that occurs in theoccurs in the third trimesterthird trimester of of pregnancy.pregnancy.
Incidence:Incidence: 1/10 000 to 1/15 0001/10 000 to 1/15 000 pregnancies.pregnancies.
Maternal mortality:Maternal mortality: 18%18%
Fetal mortality:Fetal mortality: 23%23%..
More common inMore common in nulliparous womennulliparous women and and withwith multiple gestationmultiple gestation..
PathophysiologyPathophysiology Defects in intramitochondrial fatty acid beta-Defects in intramitochondrial fatty acid beta-
oxidation (enzymatic mutations in fatty acid oxidation (enzymatic mutations in fatty acid oxidation).oxidation).
Heterozygous woman gets a homozygous Heterozygous woman gets a homozygous fetus fetal fatty acids accumulatefetus fetal fatty acids accumulate
return to the mother’s circulationreturn to the mother’s circulation extra load of long-chain fatty acidsextra load of long-chain fatty acids triglyceride accumulation triglyceride accumulation
hepatic fat deposition & impaired hepatic fat deposition & impaired maternal hepatic function.maternal hepatic function.
Clinical Features and Clinical Features and DiagnosisDiagnosis
Typical presentation:Typical presentation:
a 1 - 2 wk history of nausea, a 1 - 2 wk history of nausea, vomiting, abdominal pain & fatigue,vomiting, abdominal pain & fatigue,
Jaundice (frequent),Jaundice (frequent), moderate to severe hypoglycemia,moderate to severe hypoglycemia, hepatic encephalopathy,hepatic encephalopathy, coagulopathy.coagulopathy.
Laboratory Laboratory findingsfindings aminotransferase levels (from mild aminotransferase levels (from mild
elevation to 1000 IU/L, usually elevation to 1000 IU/L, usually 300 - 300 - 500500).).
Bilirubin: frequently Bilirubin: frequently > 5mg/dL> 5mg/dL.. Commonly: leukocytosis, anemia.Commonly: leukocytosis, anemia. With progress: thrombocytopenia (With progress: thrombocytopenia (±±
DIC) & hypoalbuminemia.DIC) & hypoalbuminemia. May be: rising uric acid, renal May be: rising uric acid, renal
impairment, metabolic acidosis, impairment, metabolic acidosis, ammonia & biochemical pancreatitis.ammonia & biochemical pancreatitis.
Laboratory findings (Cont.)Laboratory findings (Cont.)
liver biopsy
most definitive test
often not doned. t. coagulopathy
swollen, pale hepatocytesin the central zones
microvesicular fatty infiltration(frozen section with oil red staining)
findings
Imaging studies (US & CT)
Inconsistent
So, diagnosis
is
usually
based on
clinica
l & la
b. findings
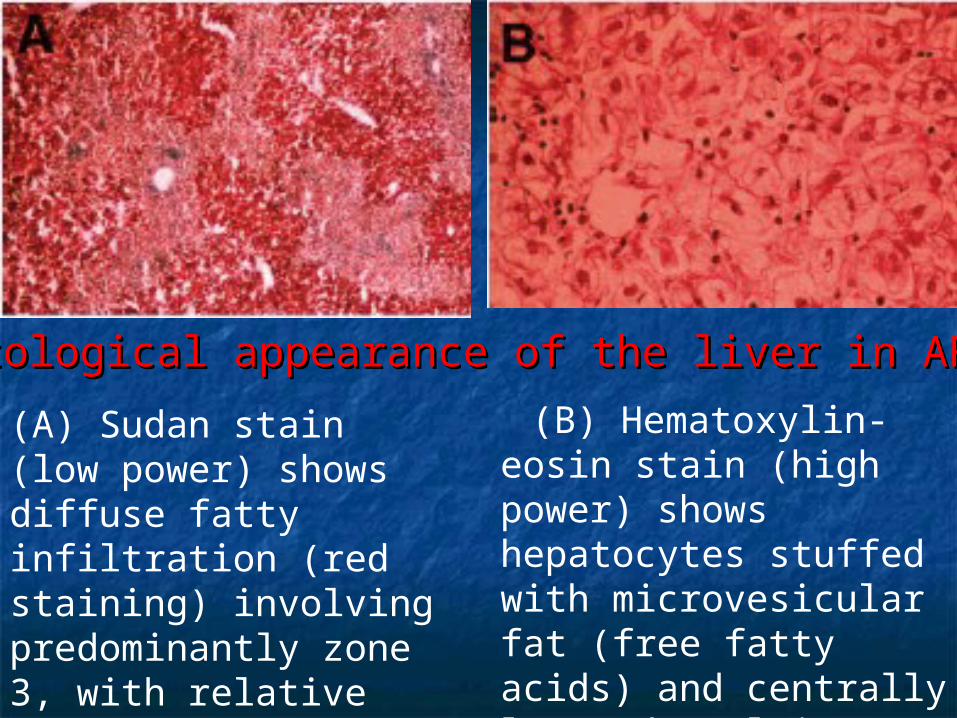
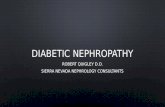
(B) Hematoxylin-eosin stain (high power) shows hepatocytes stuffed with microvesicular fat (free fatty acids) and centrally located nuclei.
Histological appearance of the liver in AFLPHistological appearance of the liver in AFLP.
(A) Sudan stain (low power) shows diffuse fatty infiltration (red staining) involving predominantly zone 3, with relative sparing of periportal areas.

TreatmentTreatment
If no obstetric indication, normal delivery is If no obstetric indication, normal delivery is preferred to CS ( % of major intra-preferred to CS ( % of major intra-abdominal bleeding)abdominal bleeding)
Careful attention to the infant: risk ofCareful attention to the infant: risk of cardiomyopathycardiomyopathy, , neuropathyneuropathy, , myopathymyopathy, , nonketotic hypoglycemianonketotic hypoglycemia, , hepatic failurehepatic failure, , and and death.death.
Treatment involves
early recognition & diagnosis immediate terminationof pregnancy +

Fate & complicationsFate & complications
Usually By 2 - 3 dayspostpartum
liver enzymes & encephalopathy
improve
Sometimeslaboratory abnormalities
persist after delivery& may initially worsen during
first postpartum week
Rarelypatients progress to fulminant hepatic failure
with need for liver transplantation.
Most patients improve in 1 to 4 weeks postpart
With advances in supportive With advances in supportive management, the maternal mortality management, the maternal mortality is now 7%-18% and fetal mortality is now 7%-18% and fetal mortality 9%-23%.9%-23%.
Complications:Complications:• Infectious and bleeding remain the Infectious and bleeding remain the
most life threatening.most life threatening.
Liver transplantation has a very Liver transplantation has a very limited role because of the great limited role because of the great potential for recovery with delivery.potential for recovery with delivery.

HOW TO HOW TO DIFFERENTIATEDIFFERENTIATE
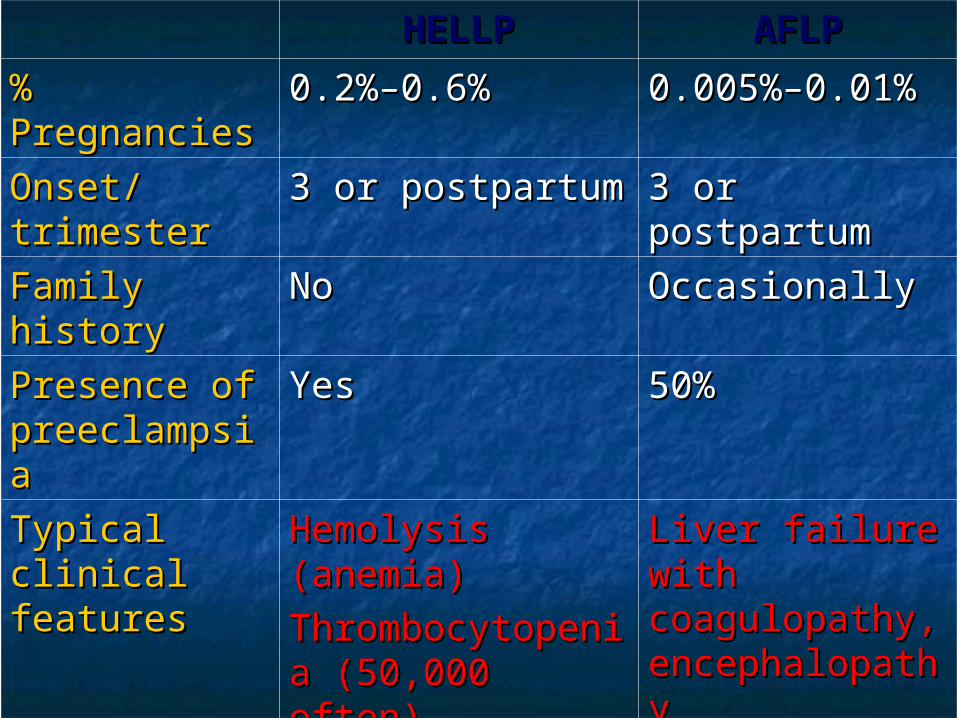
HELLPHELLP AFLPAFLP
% % PregnanciesPregnancies
0.2%–0.6%0.2%–0.6% 0.005%–0.01%0.005%–0.01%
Onset/Onset/trimestertrimester
3 or postpartum3 or postpartum 3 or 3 or postpartumpostpartum
Family Family historyhistory
NoNo OccasionallyOccasionally
Presence of Presence of preeclampsiapreeclampsia
YesYes 50%50%
Typical Typical clinical clinical featuresfeatures
Hemolysis Hemolysis (anemia)(anemia)
ThrombocytopeniThrombocytopenia (50,000 often)a (50,000 often)
Liver failure Liver failure with with coagulopathy, coagulopathy, encephalopathyencephalopathy
hypoglycemia, hypoglycemia, DICDIC
AminotransfeAminotransfer-asesr-ases
MildMild, but may be , but may be up to 10-20-fold up to 10-20-fold riserise
300-500 typical300-500 typical but variablebut variable

HELLPHELLP AFLPAFLP
BilirubinBilirubin <5<5 mg/dL unless mg/dL unless massive necrosismassive necrosis
often often >5>5 mg/dL, higher mg/dL, higher if severeif severe
Hepatic Hepatic imagingimaging
Hepatic infarctsHepatic infarcts
Hematomas, Hematomas, rupturerupture
Fatty infiltrationFatty infiltration
HistologyHistology Patchy/extensivePatchy/extensive
necrosis, necrosis, periportal hge, periportal hge, fibrin depositsfibrin deposits
Microvesicular fat in Microvesicular fat in zone 3zone 3
Maternal Maternal mortalitymortality
1%–25%1%–25% 7%–18%7%–18%
Fetal/Fetal/perinatal perinatal mortalitymortality
11%11% 9%–23%9%–23%
Recurrence in Recurrence in subsequentsubsequent
PregnanciesPregnancies
4%–19%4%–19% fatty acid oxidation defect fatty acid oxidation defect 25%25%
No fatty acid oxidation defect No fatty acid oxidation defect rare rare
WHY TO WHY TO DIFFERENTIATEDIFFERENTIATE
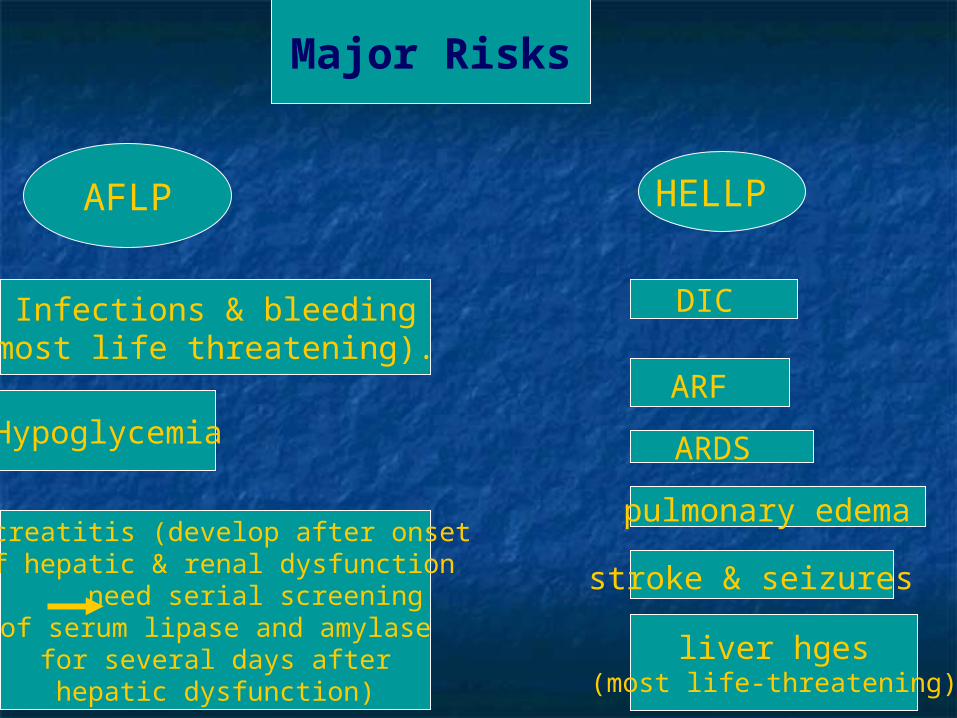
Major Risks
Infections & bleeding(most life threatening).
Hypoglycemia
AFLP HELLP
Pancreatitis (develop after onset of hepatic & renal dysfunction
need serial screeningof serum lipase and amylase
for several days afterhepatic dysfunction)
DIC
ARF
ARDS
pulmonary edema
stroke & seizures
liver hges(most life-threatening)

Therapeutic Options
AFLP HELLP
FFP
glucose
Liver transplant(limited role)
Antithrombotics:(heparin, antithrombin,
low dose aspirin)
Steroids: rapid clinical &lab. improvement
Blood transfusion
Early Late
Plasmapheresis
Liver transplantMore definite role role
Follow-up Precautions:Follow-up Precautions:A deficiency in long chain 3-hydroxyacyl-A deficiency in long chain 3-hydroxyacyl-
CoA dehydrogenase (LCHAD) is thought CoA dehydrogenase (LCHAD) is thought to be associated with the development to be associated with the development of AFLP.of AFLP.
Under normal circumstances, an Under normal circumstances, an individual that is heterozygous for individual that is heterozygous for enzymatic mutations in fatty acid enzymatic mutations in fatty acid oxidation will not have abnormal fatty oxidation will not have abnormal fatty oxidation.oxidation.
Affected patients should be screened Affected patients should be screened for defects in fatty acid oxidation as for defects in fatty acid oxidation as recurrence in subsequent children is recurrence in subsequent children is 25%, and recurrence of AFLP in 25%, and recurrence of AFLP in mothers is also possible.mothers is also possible.
Presymptomatic diagnosis of FAOD Presymptomatic diagnosis of FAOD withwith The application of tandem mass The application of tandem mass spectrometry to newborn screening spectrometry to newborn screening is an effective way to identify most is an effective way to identify most FAOD patients presymptomaticallyFAOD patients presymptomatically
reduce morbidity and avoid mortalityreduce morbidity and avoid mortality
Current management of pts with Current management of pts with FAOD includes long-term dietary FAOD includes long-term dietary therapy of:therapy of: fasting avoidance,fasting avoidance, low-fat/high-carbohydrate dietlow-fat/high-carbohydrate diet restriction of long-chain fatty acid restriction of long-chain fatty acid
intake and substitution with medium-intake and substitution with medium-chain fatty acids.chain fatty acids.
These dietary approaches appear These dietary approaches appear promising in the short-term, but not promising in the short-term, but not the long-term outcome.the long-term outcome.
In conclusionIn conclusion
Important to diff. AFLP from HELLPImportant to diff. AFLP from HELLP Diff. mainly based on lab. + imaging Diff. mainly based on lab. + imaging
(CT-MRI)(CT-MRI) Diff. because AFLP needs:Diff. because AFLP needs:
o Maternal follow-up for recurrenceMaternal follow-up for recurrenceo Baby follow-up for FAOD needing Baby follow-up for FAOD needing
dietary controldietary controlo Next pregnancies for presymptomatic Next pregnancies for presymptomatic
diagnosisdiagnosis