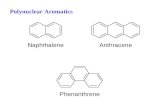
Nomenclature The Common Phakomatoses
8
The Common Phakomatoses Birgit Ertl-Wagner ECPNR, 10 th Cycle, Rome Nomenclature • From Greek φακός, phakos – spot, lens • Named by Jan van der Hoewe in 1920 (Dutch ophtalmologist): “lens- like” changes on fundoscopy in a tuberous sclerosis patient • Newer nomenclature: neurocutaneous syndromes neuro-oculo-cutaneous syndromes https://de.wikipedia.org/wiki/Jan_van_d er_Hoeve Many more diagnoses encompassed now • Neurofibromatosis type 1 • Neurofibromatosis type 2 • Tuberous sclerosis • Sturge-Weber syndrome • von Hippel-Lindau disease • Ataxia telangiectasia • Incontinentia pigmenti • Nevoid basal cell carcinoma syndrome • Wyburn-Mason syndrome (Bonnet– Dechaume–Blanc syndrome) • And many more… “The Big Five” • Neurofibromatosis type 1 • Neurofibromatosis type 2 • Tuberous sclerosis • Sturge-Weber syndrome • von Hippel-Lindau disease 3-year old boy with seizures and developmental delay Tuberous Sclerosis Complex • aka M. Bourneville-Pringle • Autosomal dominant • 70% sporadic (de novo mutations) • 2 genes: TSC1 on chromosome 9q34 TSC2 on chromosome 16p13.3 • Incidence: 1:8000 live births • Developmental tauopathy (tau abnormally expressed) 9 16 Van Eeghen et al., 2013 Jansen et al., 2008 Tuberous Sclerosis Complex - Background • Original „Vogt triad “: • cognitive impairment • epilepsy • adenoma sebaceum • 18 to 55% do not suffer from mental retardation • Adenoma sebaceum usually only in later childhood / adolescence Rayer „Traites des maladies de la peau“ 1835 Umeoka et al., 2008 Tuberous Sclerosis Complex - Skin • Ash Leaf spots – hypomelanotic lesions • Adenoma sebaceum - angiofibromas in the face • Koenen tumours of the fingernails • Dental enamel pits www.webmd.com ; www.ourdermatology.blogspot.com
Transcript of Nomenclature The Common Phakomatoses

The Common Phakomatoses
Birgit Ertl-Wagner
ECPNR, 10th Cycle, Rome
Nomenclature
• From Greek φακός, phakos – spot,lens
• Named by Jan van der Hoewe in 1920 (Dutch ophtalmologist): “lens-like” changes on fundoscopy in a tuberous sclerosis patient
• Newer nomenclature: neurocutaneous syndromes neuro-oculo-cutaneous syndromes
https://de.wikipedia.org/wiki/Jan_van_der_Hoeve
Many more diagnoses encompassed now • Neurofibromatosis type 1 • Neurofibromatosis type 2 • Tuberous sclerosis • Sturge-Weber syndrome • von Hippel-Lindau disease • Ataxia telangiectasia • Incontinentia pigmenti • Nevoid basal cell carcinoma
syndrome • Wyburn-Mason syndrome (Bonnet–
Dechaume–Blanc syndrome) • And many more…
“The Big Five”
• Neurofibromatosis type 1
• Neurofibromatosis type 2
• Tuberous sclerosis
• Sturge-Weber syndrome
• von Hippel-Lindau disease
3-year old boy with seizures and developmental delay Tuberous Sclerosis Complex • aka M. Bourneville-Pringle • Autosomal dominant • 70% sporadic (de novo
mutations) • 2 genes:
TSC1 on chromosome 9q34 TSC2 on chromosome 16p13.3
• Incidence: 1:8000 live births • Developmental tauopathy (tau
abnormally expressed)
9
16
Van Eeghen et al., 2013 Jansen et al., 2008
Tuberous Sclerosis Complex - Background
• Original „Vogt triad“: • cognitive impairment
• epilepsy
• adenoma sebaceum • 18 to 55% do not suffer from
mental retardation • Adenoma sebaceum usually
only in later childhood / adolescence
Rayer „Traites des maladies de la peau“ 1835
Umeoka et al., 2008
Tuberous Sclerosis Complex - Skin
• Ash Leaf spots –hypomelanotic lesions
• Adenoma sebaceum - angiofibromas in the face
• Koenen tumours of the fingernails
• Dental enamel pits
www.webmd.com;www.ourdermatology.blogspot.com

Tuberous Sclerosis Complex - Extracranial
• Angiomyolipomas • Renal cysts • Rhabdomyomas of the
heart – usually spontaneously regress postnatally
• Lymphangioleiomyo-matosis (LAM) of the lung
• Cystic bone lesions • Giant drusen on
fundoscopy
Tuberous Sclerosis Complex - Tubers • Tuber = swelling; in plants: for
storage of nutrients
• Contain balloon cells large, eosinophilic
• Can be heterotopic or transhemispheric
• Number and location of tubers may play a role in neurocognitive outcome
Kassiri et al., 2011
Tuberous Sclerosis Complex - Tubers • Frontal > parietal > occipital >
temporal > cerebellum
• 50% are calcified by age 10 y
• Signal variable relative to myelin maturation
• FLAIR hyperintense in older children
• 3-4% enhance
• Higher ADC values in more epileptogenic tubers
• AMT (α-11C-methyl-L-tryptophan) PET may identify epileptogenictubers
Manoukian et al., 2015
Cystic Appearing Tubers
• Tubers may appear cyst-like
• High signal intensity T2w, low signal intensity T1w
• More aggressive type of seizures?
Kassiri et al., 2011
Tuber vs. FCD Type IIb
• Focal cortical dysplasia type IIb histologically identical to tuber
• May also have a funnel-shaped migration part
• FCD IIb do not calcify • If in doubt:
• Skin examination with Wood´s light
• Renal ultrasound • Echocardiography
Kassiri et al., 2011
White Matter Radial Migration Lines
• Heterotopic glia with neurons along migration pathways
• Linear to curvilinear • Radial migration
abnormalities correlate with outcome
• Cyst-like structures in white matter possible as well (origin unknown)
Kassiri et al., 2011
Subependymal Nodules
• Subependymal hamartomas • Usually calcify in the course of
time (after one year of age) • Irregularly shaped nodules • Main axis perpendicular to
ventricular wall • Protrude into the ventricles • May enhance • Are NOT isointense to cortex
Subependymal Nodules

Subependymal Giant Cell Astrocytoma - SEGA
• WHO grade I • At Foramen Monroi • In 15-20% of patients with TSC • Round configuration,
pronounced enhancement • May lead to ipsilateral dilatation
of lateral ventricle
Diagnosis based on size and growth
Enlarging, enhancing mass >1.3 cm near foramen Monroi
Subependymal Giant Cell Astrocytoma - SEGA
• CT: may have calcification • T2WI / FLAIR: iso- to
hyperintense, heterogeneous • T1WI: hypo- to isointense • T2* may have low SI from
calcifications • Contrast-enhancement • (Asymmetric) hydrocephalus
SEGA - Treatment
• Mammalian target of rapamycin (mTOR) inhibitors (e.g.Sirolimus, Everolimus)
• normalize the mTOR pathway also in other TSC manifestations(angiomyolipomas,lymphangioleiomyomatosis,epilepsy)
• consider treatment effects when evaluating SEGAs
Jozwiak et al., 2013; Krueger et al., 2013; Lam et al., 2010
Tuberous Sclerosis Complex – Imaging Patterns
Cortical tuber, subependymal nodules, giant cell astrocytomas
6-year old boy with developmental delay Neurofibromatosis Type 1
• Autosomal dominant • Long arm of chromosome 17
(17q11.2) • NF-1 gene (neurofibromin 1)
probably a tumor-suppressor gene
• Incidence: 1:2500 to 1:3300 live births
• About 50% de novo mutations • Neurofibromin inactivated
(negative regulator of RAS protooncogene)
Gutmann et al., 2012
Neurofibromatosis Type 1
• Café-au-lait spots(>5, >25mm, + symptoms)
• Axillary freckling
• Lisch-nodules (hamartomas of the iris)
• Cutaneous / subcutaneous neurofibromas
Gutmann et al., 2012 Pictures: www.de.wikipedia.org
NF-1 – Diagnostic Criteria: 2 or more
• First degree relative with NF-1 • Six or more Cafe-au-lait spots• Axillary or inguinal freckling • Two or more Lisch nodules (iris hamartomas) • Two or more neurofibromas or one or more plexiform
neurofibroma • Optic pathway glioma
• Distinctive bone lesion (e.g. dysplasia of the sphenoid)
Gutmann et al., 2012

NF-1 – FASI (Focal Areas of Signal Intensity) • Also called “UBOs” (unidentified
bright objects) • Transient intramyelin edema • Start in childhood, tend to
disappear in adulthood • 80-90% in pre-teen children with
NF-1 • No mass effect • In cerebral white matter / internal
capsule / corpus callosum, may also involve thalamus, pallidum,cerebellum, brainstem
Ferraz-Filho et al., 2013; Barbier et al., 2011; Chabernaud et al., 2009
NF-1 – FASI (Focal Areas of Signal Intensity)
• Hyperintense on T2WI, isointense on T1WI
• No edema, no swelling • DTI decreased FA • MRS decreased NAA/Cr &
NAA/Cho (thalamic)
Ferraz-Filho et al., 2013; Barbier et al., 2011; Chabernaud et al., 2009
NF-1 – Location of Tumors NF 1 Location of Tumors Optic Pathway Gliomas (OPGs) • 15% of NF1 patients • Peak age 4-5 yrs • Asymptomatic or reduced visual
acuity • Mostly pilocytic astrocytomas (WHO
grade I), but highly malignant subtypes
• Enhancing lesion • Optic nerve, uni (50%)- or bilateral
(20%) and / or chiasma • Can be extensive • May regress spontaneously
Ferraz-Filho et al., 2013; Barbier et al., 2011; Chabernaud et al., 2009
OPGs – Are GBCAs Necessary in Surveillance?
• GBCAs may not be needed for follow-up
• GBCA enhancement does not necessarily correlate with biological behavior
Maloney et al., 2018
NF-1 – Gliomas (Outside Optic Pathway)
• Incidence of gliomas increased
• Any WHO grade possible
• 5x higher risk of high grade gliomas
• Mortality higher in symptomatic and adult patients
Rasmussen et al, 2001 Guillamo et al., 2003 Rodriguez et al, 2008
NF-1 – Brainstem Gliomas
• May be diffuse or focal
• 68% medullary, 52% pontine,44% midbrain
• 56% multiple locations
• Diffuse brainstem gliomasgenerally slower progression in NF-1
• Beware of hydrocephalus Rasmussen et al, 2001 Guillamo et al., 2003 Rodriguez et al, 2008
NF-1 – Spine
• Kyphoscoliosis common
• Dural ectasia – dysplasia of meninges, vulnerable to CSF pulsation, vertebral scalloping
• Lateral meningoceles

NF-1 – Neurofibromas
• Tumors of the nerve sheaths • Degree of connective tissue • Intraspinal, paraspinal,
peripheral • Variable signal intensity on
T2w• Enhancement with GBCA
17-year old girl with lower back pain
NF-1 – Malignant Peripheral Nerve Sheath Tumors
• Malignant peripheral nerve sheath tumors (MPNST) in 5-13% of NF-1 patients
• FDG-PET may predict malignant transformation
Tsai et al., 2013
NF-1 – Plexiform Neurofibromas
• Characteristic for NF-1 • Locally aggressive • Transspatial lesion • No metastases • Diffuse growth along a nerve • Can be disfiguring • May transform to MPNST
(10%)
Tsai et al., 2013
NF-1 – Vascular Abnormalities
• Moyamoya pattern • Arterial ectasias • Aneurysms• Renal artery stenosis • Aortic stenosis
NF-1 – Imaging Patterns
FASIs, gliomas – optic nerve / chiasma, neurofibromas
14-year old boy with bilateral hearing loss Neurofibromatosis Type 2
• „Neurofibromatosis with bilateral acoustic schwannomas“
• autosomal dominant • NF2 gene (neurofibromin 2 –
merlin): long arm of chromosome 22 (22q12.2)
• Est. incidence: 1:60.000 • About 50% de novo
mutations
Evans, 2009

Neurofibromatosis Type 2
• Often becomes symptomatic in early adulthood
• Café au lait spots and cutaneous neurofibromas less common than in NF-1
• May lead to cataracts (subcapsular, posterior)
Bosch et al, Eye (2005) 19, 705–706
NF-2 – Vestibular Schwannomas
• Uni- or bilateral • Mostly superior branch of
vestibular nerve • Faster growth rate than
spontaneous forms • Clinical trials for medical
treatments (lapatinib,bevacizumab)
Karajannis et al., 2012; Plotkin et al., 2012
NF-2 – Diagnostic Criteria Bilateral vestibular schwannomas (disease-defining) ORRelative with NF-1 PLUS Unilateral vestibular schwannoma < 30y/oAny 2 of the following: Meningioma, ependymoma,
schwannoma, glioma, cataract
In a child / adolescent even unilateral vestibular schwannoma or solitary meningioma suspicious for NF-2
Beware: 25% of pts. > 50 years and 50% of pts > 70 years with bilateral vestibular schwanomas do NOT have NF2 mutations
Evans et al., 2015
NF-2 - Schwannomas May also affect other cranial
nerves, e.g. • Trigeminal nerve • Oculomotor nerve • Facial nerve NF2-related schwannomas
have higher proliferative activity than sporadic schwannomas
Look into the corners…
NF-2 - Meningeomas
• Multiple meningeomas possible
• Intraventricular location possible
Goutagny et al., 2012
Meningeoma(s) at a young age – consider NF-2
NF-2 – Ependymomas
Incidence of brain stem andspinal ependymomas increased
6% of NF-2 patients develop ependymomas
Goutagny et al., 2012
Beware of intraaxial brain stem and spinal cord
ependymomas in patients with NF2
NF-2 – Spinal Tumors
Look at the entire neuro-axis! Intra- or paraspinal Spinal schwannomas Meningiomas Ependymomas Beware of: myelopathy,
syringohydromyelia Spinal tumours associated with
higher number of intracranial meningiomas,schwannomas, frameshiftmutations
Goutagny et al., 2012
NF-2 – Imaging Patterns
Vestibular schwannomas, other cranial nerve and / orspinal schwannomas, meningeomas, ependymomas

22-year old woman with progressive back pain (and known visual problems)
Von Hippel-Lindau Syndrome • Retino-cerebellar
angiomatosis • Autosomal dominant • Short arm of chromosome 3
(3p26-p25); VHL tumour suppressor gene
• Rate of spontaneous mutations about 50%
• Incidence:1:35,000 live births • Often becomes symptomatic
in adolescence with visual symptoms Bader et al., 2012
Kim et al., 2010
VHL – Diagnostic Criteria / Subtypes Two or more CNS hemangioblastomas OROne CNS hemangioblastoma plus visceral lesion or retinal
hemorrhage
Subtypes of VHL•Type 1: Low risk of pheochromocytoma •Type 2: High risk of pheochromocytoma
•Type 2A: low risk of renal cell carcinoma •Type 2B: high risk of renal cell carcinoma •Type 2C: familial pheochromocytoma without renal cell cancer or hemangioblastoma
Binderup et al., 2015
VHL – Extracranial Manifestations
• Retinal haemangioblastomas
• Clear cell renal carcinomas – most common cause ofpremature death in VHL
• Pheochromocytomas • Papillary cystadenoma of
the epididymis andmesosalpinx
• Polycythemia National Eye Institute http://www.nei.nih.gov/photo/eyedis/index.asp Kim et al., 2010
VHL – NIH Screening Recommendations
• Contrast-enhanced MRI of the brain and spinal cord every 2 years from age 11 years
• Yearly ultrasonography of the abdomen from age 11 years
• Abdominal CT from age 20 years, yearly to every other year
• MRI of the temporal bone if hearing loss or tinnitus or vertigo
Bamps et al., 2013
VHL – Cerebellar Hemangioblastomas
• 60% of haemangioblastomas are cerebellar
• Commonly lead to hydrocephalus
• Can produce erythropoietin • Often cyst with enhancing
mural nodule • However: 1/3 solid
Maher et al., 2012
VHL – Spinal Hemangioblastomas
• Look at the entire neuro-axis • 30% of hemangioblastomas
are spinal • Give GBCA to increase
sensitivity • Syringohydromyelia may be
indirect sign – 95% have syrinx
Beitner et al., 2011
VHL – Endolymphatic Sac Tumors (ELST)
• Posteromedial surface of the temporal bone
• May invade the labyrinth • About 4% prevalence in
VHL • Symptoms: vertigo, tinnitus,
sensorineural hearing loss • Ca be large • May recur after resection
Kim et al., 2013 Bastier et al., 2013 Bausch et al., 2015

VHL – Imaging Patterns
Cerebellar and spinal hemangioblastomas– cyst with mural nodule or solid; endolymphatic sac tumours
17-year old girl with seizures
Sturge-Weber Syndrome • Encephalotrigeminal
angiomatosis • Somatic mutation of GNAQ • Incidence < 1:50.000 • Facial naevus flammeus
(trigeminal area(s)) • Can be bilateral (20%) • Persistent fetal vasculature,
deep venous stasis • Glaucoma
Lo et al., 2012 Shirley et al., 2013
www.apotheken-umschau.de
Sturge-Weber Syndrome – X-Ray (historical) 1922: description of tram-
track calcifications in radiographs of the skull
Often hyperpneumatisation of the frontal sinus
Toronto
Sturge-Weber Syndrome
• Absence of normal cortical venous drainage
• Venous stasis • Flow redirection to the
deep vessels • Enlarged medullary and
basal veins • Contrast-enhanced
FLAIR sequence most sensitive
Alkonyi et al., 2012
Sturge-Weber Syndrome
• Early swelling and „accelerated“ myelination
• Venous stasis • Regional perfusion and
cortical metabolic alterations • Ensuing focal atrophy in the
affected area • Calcifications • Hypertrophy of the choroid
plexus • Increased leptomeningeal
enhancement
Sturge-Weber Syndrome – Imaging Patterns
Calcifications, atrophy, leptomeningeal enhancement, hypertrophy ofthe choroid plexus (early: accelerated myelination, swelling)
THANK YOU FOR YOUR ATTENTION





![NOMENCLATURE OF LIGNANS AND NEOLIGNANS · PDF filepling. The term lignan was introduced by Haworth [2] for the structures where the two units are β,β'-linked](https://static.fdocument.org/doc/165x107/5a79d56a7f8b9ae67b8c611f/nomenclature-of-lignans-and-neolignans-the-term-lignan-was-introduced-by-haworth.jpg)