NF-κB Activation and Severity of Gastritis in Helicobacter pylori ...
11
NF-jB Activation and Severity of Gastritis in Helicobacter pylori-Infected Children and Adults Patrick Bontems,* ,† Ezra Aksoy, †,‡ Alain Burette, § Val erie Segers, ¶ Carine Deprez, ¶ Franc ßoise Mascart †, ** and Samy Cadranel* *Paediatric Gastroenterology-Hepatology, Queen Fabiola Children’s University Hospital, Universit e Libre de Bruxelles, Av JJ Crocq 15, 1020 Brussels, Belgium, † Laboratory of Vaccinology and Mucosal Immunity, Universit e Libre de Bruxelles, Route de Lennik 808, 1070 Brussels, Belgium, ‡ Centre for Cell Signalling, Barts Cancer Institute, Queen Mary University of London, Charterhouse Square, London EC1M 6BQ, UK, § Department of Gastroenterology, Nouvelle Clinique de la Basilique, Rue Pangaert 37, 1083 Brussels, Belgium, ¶ Department of Pathology, University Hospital Brugmann, Universit e Libre de Bruxelles, Place Van Gehuchten 4, 1020 Brussels, Belgium, **Immunobiology Clinic, Academic Hospital Erasme, Universit e Libre de Bruxelles, Route de Lennik 808, Brussels, Belgium Keywords Helicobacter pylori, NF-jB activation, gastroduodenal ulcer, children, gastritis. Reprint requests to: Patrick Bontems, Paediatric Gastroenterology-Hepatology, Queen Fabiola Children’s University Hospital, Universit e Libre de Bruxelles, Av JJ Crocq 15, 1020 Brussels, Belgium. E-mail: [email protected] Abstract Background: In contrast to adults, Helicobacter pylori gastritis in children is reported as milder and ulcer disease as uncommon, but unequivocal data are lacking. Objectives: To compare the frequency of gastro-duodenal ulcers in children and adults as well as the proportion of Helicobacter pylori infection in these patients and to study the effect of chronological age on NF-jB activation and on severity of gastritis. Design: Patients referred in one pediatric and one adult facility for upper GI endoscopy were included. Gastric biopsies were obtained in consecutive Heli- cobacter pylori-infected patients and age-matched negative controls for immu- nohistochemistry and electrophoresis mobility shift assay. Three age groups were defined: younger than 8 years, 8–17 years, and adults. Results: Peptic ulcer disease was less frequent in children and less fre- quently associated with Helicobacter pylori infection. When comparing infected subjects to controls, densities of neutrophils and CD20 cells in the lamina propria increased in all age groups, CD3 cells increasing only in patients older than 8 years and CD8 cells only in adults. NF-jB-p65-positive cells were also increased only in infected adults as well as NF-jB-binding activity. A positive correlation was found between age and densities of neu- trophils and CD3, but not of CD8 or CD20 cells. Conclusion: Peptic ulcer disease was less frequent in children and less fre- quently caused by Helicobacter pylori infection. The different clinical outcome of the infection in children can be the consequence of the lower mucosal immune response. Helicobacter pylori (H. pylori) is a gram-negative microor- ganism that colonizes the mucus coat overlying the gastric epithelium and causes chronic/active gastritis, peptic ulcer disease (PUD), gastric mucosal atrophy, intestinal metapla- sia, gastric adenocarcinoma, and gastric lymphoma [1]. Although the prevalence of infection varies geographically and is declining over time in developed countries, the organism still infects approximately one half of the world’s population [2]. Progression from gastritis toward more severe disease states appears to be influenced by both bac- terial determinants and host immune response [3,4]. Immune response against H. pylori involves innate components represented mainly by neutrophils and adaptive immunity involving systemic and mucosal H. pylori-specific antibody production as well as a com- plex mix of Th1, Th17, and Treg immune responses [5–9]. Interactions of H. pylori strains and bacterial compounds with diverse host epithelial and cytoplasmic signaling pathways such as Toll-like receptors (TLRs) or nucleotide-binding oligomerization domain (NLRs) is followed by the activation of NF-jB, a transcription factor regulating activation of genes responding to © 2014 John Wiley & Sons Ltd, Helicobacter 19: 157–167 157 Helicobacter ISSN 1523-5378 doi: 10.1111/hel.12118
Transcript of NF-κB Activation and Severity of Gastritis in Helicobacter pylori ...

NF-jB Activation and Severity of Gastritis in Helicobacterpylori-Infected Children and AdultsPatrick Bontems,*,† Ezra Aksoy,†,‡ Alain Burette,§ Val�erie Segers,¶ Carine Deprez,¶ Franc�oise Mascart†,**and Samy Cadranel*
*Paediatric Gastroenterology-Hepatology, Queen Fabiola Children’s University Hospital, Universit�e Libre de Bruxelles, Av JJ Crocq 15, 1020
Brussels, Belgium, †Laboratory of Vaccinology and Mucosal Immunity, Universit�e Libre de Bruxelles, Route de Lennik 808, 1070 Brussels, Belgium,‡Centre for Cell Signalling, Barts Cancer Institute, Queen Mary University of London, Charterhouse Square, London EC1M 6BQ, UK, §Department of
Gastroenterology, Nouvelle Clinique de la Basilique, Rue Pangaert 37, 1083 Brussels, Belgium, ¶Department of Pathology, University Hospital
Brugmann, Universit�e Libre de Bruxelles, Place Van Gehuchten 4, 1020 Brussels, Belgium, **Immunobiology Clinic, Academic Hospital Erasme,
Universit�e Libre de Bruxelles, Route de Lennik 808, Brussels, Belgium
Keywords
Helicobacter pylori, NF-jB activation,
gastroduodenal ulcer, children, gastritis.
Reprint requests to: Patrick Bontems, Paediatric
Gastroenterology-Hepatology, Queen Fabiola
Children’s University Hospital, Universit�e Libre de
Bruxelles, Av JJ Crocq 15, 1020 Brussels,
Belgium. E-mail: [email protected]
Abstract
Background: In contrast to adults, Helicobacter pylori gastritis in children is
reported as milder and ulcer disease as uncommon, but unequivocal data
are lacking.
Objectives: To compare the frequency of gastro-duodenal ulcers in children
and adults as well as the proportion of Helicobacter pylori infection in these
patients and to study the effect of chronological age on NF-jB activation
and on severity of gastritis.
Design: Patients referred in one pediatric and one adult facility for upper GI
endoscopy were included. Gastric biopsies were obtained in consecutive Heli-
cobacter pylori-infected patients and age-matched negative controls for immu-
nohistochemistry and electrophoresis mobility shift assay. Three age groups
were defined: younger than 8 years, 8–17 years, and adults.
Results: Peptic ulcer disease was less frequent in children and less fre-
quently associated with Helicobacter pylori infection. When comparing
infected subjects to controls, densities of neutrophils and CD20 cells in the
lamina propria increased in all age groups, CD3 cells increasing only in
patients older than 8 years and CD8 cells only in adults. NF-jB-p65-positivecells were also increased only in infected adults as well as NF-jB-bindingactivity. A positive correlation was found between age and densities of neu-
trophils and CD3, but not of CD8 or CD20 cells.
Conclusion: Peptic ulcer disease was less frequent in children and less fre-
quently caused by Helicobacter pylori infection. The different clinical outcome
of the infection in children can be the consequence of the lower mucosal
immune response.
Helicobacter pylori (H. pylori) is a gram-negative microor-
ganism that colonizes the mucus coat overlying the gastric
epithelium and causes chronic/active gastritis, peptic ulcer
disease (PUD), gastric mucosal atrophy, intestinal metapla-
sia, gastric adenocarcinoma, and gastric lymphoma [1].
Although the prevalence of infection varies geographically
and is declining over time in developed countries, the
organism still infects approximately one half of the world’s
population [2]. Progression from gastritis toward more
severe disease states appears to be influenced by both bac-
terial determinants and host immune response [3,4].
Immune response against H. pylori involves innate
components represented mainly by neutrophils and
adaptive immunity involving systemic and mucosal
H. pylori-specific antibody production as well as a com-
plex mix of Th1, Th17, and Treg immune responses
[5–9]. Interactions of H. pylori strains and bacterial
compounds with diverse host epithelial and cytoplasmic
signaling pathways such as Toll-like receptors (TLRs) or
nucleotide-binding oligomerization domain (NLRs) is
followed by the activation of NF-jB, a transcription
factor regulating activation of genes responding to
© 2014 John Wiley & Sons Ltd, Helicobacter 19: 157–167 157
Helicobacter ISSN 1523-5378
doi: 10.1111/hel.12118

immune or inflammatory signals [8–16]. These immune
responses fail to eradicate H. pylori infection and cer-
tainly contribute to disease pathogenesis, in part due to
tissue remodeling trough inflammation and activation
of matrix metalloproteinase [17–22]. Although NF-jBhas a key role in mediating gastric mucosal inflamma-
tion caused by H. pylori, its activation has not been
studied yet in infected children.
The systemic humoral response to H. pylori infec-
tion is weaker and variable in children [23,24]. In
addition, a lower IFN-c secretion in the stomach and a
lower infiltration by IFN-c-secreting cells characterize
the mucosal immune response to H. pylori in children
compared with infected adults [6,7]. Moreover, regula-
tory T-cell response to H. pylori infection also predomi-
nates in children instead of Th17 cell [25–27]. These
evidences suggest that a weaker immune response
could protect the child from more severe gastroduode-
nal damages due to the infection. A lesser inflamma-
tory cell mucosal infiltration has been reported in
children, but there are still controversies especially
concerning the lack or reduced infiltration of the gas-
tric mucosa by polymorphonuclear cells in H. pylori-
infected children [28]. Indeed, most studies are not
really comparative because adult patients were not
included (the reference to adult patients is only histor-
ical). Moreover, three comparative studies that used a
semiquantitative scoring of gastritis (the Update Syd-
ney system [29]) give conflicting results [25,30,31].
Using the same score in a pilot study, we also failed to
demonstrate a difference in the severity of gastritis
between children and adults (P. Bontems, A. Neuman-
Ova, P. Heimann, J.M. Devaster, V. Segers, C. Deprez,
S. Cadranel, unpublished observations).
In the present study, we compared the frequency of
gastric and duodenal ulcer disease between children
and adults and the proportion of lesions related to
H. pylori infection as well as the cellular density of
immune cells in the gastric mucosa using immunohisto-
chemical staining and a morphometric method and the
activation of NF-jB by the same method and by
electrophoresis mobility shift assay (EMSA).
Patients and Methods
Frequency of Gastric and Duodenal Ulcers
The source of data was two different endoscopy facili-
ties, one for children and one for adults, located very
closely in Brussels. In our routine practice, gastric biop-
sies for histologic analysis and microbiologic culture
were systematically taken from children and adults
whenever not contraindicated. All patients undergoing
an upper GI endoscopy between January 2007 and
December 2008 were enrolled to compare the frequency
of gastric and duodenal ulcers and the proportion of
ulcers associated with H. pylori infection. Only ulcers
with a diameter of 5 mm or larger were considered. The
following items were recorded: the presence of gastric or
duodenal ulcers, H. pylori status, age, and gender.
At least two biopsies were taken from the antrum
and two more from the fundus for histology and for
microbiologic culture. The biopsies were processed
according to the previously described methods [32].
Briefly, sections from formalin-fixed, paraffin-embed-
ded biopsies were stained with hematoxylin/eosin to
detect histologic features of inflammation (in accor-
dance with the Updated Sydney system [29]) and with
Giemsa to detect H. pylori-like microorganisms. Biopsy
specimens for culture were dipped with sterile cotton in
a semisolid agar transport medium (Cultiplast, LP Itali-
ana SPA, Milan, Italy). Less than 4 hours later, the
samples were grounded at 10000 rpm for 15 second
with an electric homogenizer (Ultraturrax, Staufen,
Germany) and then inoculated onto selective Columbia
blood agar and incubated under microaerophilic (5%
O2 – 10% CO2 – 85% N2) conditions at 37 °C for up to
7 days. H. pylori infection was confirmed when culture
and histology were both positives. Discrepancies
between histology and culture were resolved using an
additional diagnostic test (urease test or 13C-urea breath
test). H. pylori culture in our departments was concor-
dant with histology in 98% [32].
Cellular Density of Immune Cells in the Antral
Mucosa
Another database was constructed with all the patients
undergoing an upper GI endoscopy during 1 year except
those presenting with erosive esophagitis, gastric, or duo-
denal ulcers. Those with inflammatory bowel disease,
celiac disease, immunologic disorders as well as those
treated during the preceding 4 weeks with antibiotics,
proton-pump inhibitors, nonsteroidal anti-inflammatory
drugs, steroids, or under immunosuppressive drugs were
also excluded. From this database, 30 consecutive
H. pylori-infected patients and 30 negative controls were
selected in the proportion of 10 in each age group
(<8 years, 8–17 years and adults). Age groups were arbi-
trarily defined because the humoral response was found
weaker in children younger than 8 years, whereas it was
comparable with adults in older children [23].
Polymorphonuclear cells were counted on hematoxy-
lin- or eosin-stained sections and neutrophils differenti-
ated using morphologic criteria. B cells (anti-CD20),
T cells (anti-CD3), and T cells subsets (anti-CD8) were
© 2014 John Wiley & Sons Ltd, Helicobacter 19: 157–167158
NF-jB and severity of H. pylori gastritis Bontems et al.

counted on sections using an indirect immunoperoxidase
technique. Formalin-fixated tissue sections (causing
inter- and intramolecular cross-linking masking
antigenic epitopes) from the antrum were submitted to
microwave oven treatment. Deparaffinized and rehy-
drated tissue sections, placed in a 0.01 mol/L citrate buf-
fer at pH 6, were heated twice during 5 minute and then
rinsed in Tris-buffered saline at pH 7.4. Sequential
sections were then pre-incubated with rabbit antiserum
to reduce nonspecific staining and with 0.2% H2O2 to
inhibit endogenous peroxidases. Optimal dilution of the
primary antibody layer was added and incubated for
1 hour at room temperature, followed by optimal
dilution of the secondary (biotinylated) antibody layer,
the streptavidin-biotin complex, and the 3,30-Diam-
inobenzidine tetrahydrochloride (DAB) which develops
the peroxidase. The sections were counterstained with
hematoxylin. Monoclonal mouse anti-human antibodies
were used as primary antibody and biotinylated rabbit
anti-mouse antibody as secondary antibody (Dako Ltd,
Glostrup, Denmark). In place of the primary antibody, a
nonimmune serum from the same species was used as
negative control staining, whereas human tonsil sections
were used for positive control staining.
Cellular densities were counted at 4009 magnifica-
tion in the lamina propria using a calibrated eyepiece
graticule (Leitz, Wetzlar, Germany) defining a limited
area (four different areas on two different sections) and
in the epithelium on a 500 epithelial cells surface.
Slides were counted by two independent observers.
Activation of the Transcription Factor NF-jB in
the Antral Mucosa
The number of cells expressing activated NF-jB was
determined using the same indirect immunoperoxidase
technique described above using an anti-a-p65 subunit
antibody (Biognost, Heule, Belgium) that recognizes only
the activated form of NF-jB. The densities of cells express-ing the activated form of NF-jBwere then determined.
Additionally, DNA-binding activity of NF-jB was
determined in protein extracts obtained from consecu-
tive patients with nonulcer dyspepsia (six consecutive
children: three of them being infected by H. pylori and
the three others serving as controls; eight consecutive
adults: three infected by H. pylori and five controls) by
EMSA. Biopsies were immediately snap-frozen in liquid
nitrogen after sampling and stored at �70 °C until
assayed. To prepare total protein extracts, biopsies were
suspended in 400 lL of buffer 10 mmol/L HEPES (pH
7.8), 10 mmol/L KCl, 0.1 mmol/L EDTA, 0.5 mmol/L
DTT, 19 protease inhibitor cocktail (Sigma-Aldrich,
Bornem, Belgium), 0.2 mmol/L PMSF (Roche Diagnos-
tics, Basel, Switzerland), and 0.5% Triton X-100
(Sigma-Aldrich) for 10 minute on ice after mechanical
homogenization. Suspensions were then centrifuged at
4 °C for 5 minute, and the cytoplasmic proteins in the
supernatants carefully removed. Protein concentrations
were determined by BioRad Protein Assay Reagent
(Bio-Rad Labs., Hercules, CA, USA). The double-
stranded binding oligonucleotides for consensus NF-jB50 – AGT TGA GGG GAC TTT CCC AGG C – 30 were
obtained from Santa CruzBiotechnology. 50 – AGT TGA
GGG GAC TTT CCC AGG C – 30-NF-jB mutant oligos
were created with a “G’’?”C’’ substitution (Santa Cruz
Biotechnology, Dallas, TX, USA). Oligonucleotides were
end-labeled with [c-32P] ATP (Amersham, Little
Chalfont, UK) using T4 polynucleotide kinase (Roche
Diagnostics). For the binding reaction, 30 lg of each of
the extract was added to a reaction mixture containing
2 lg poly(dI-dC) (Pharmacia, San Diego, CA, USA),
4 lL of 59 binding buffer (10 mmol/L HEPES, (pH
7.8), 50 mmol/L KCl, 1 mmol/L EDTA, 5 mmol/L
MgCl2, 10% glycerol), and 30,000 cpm of [32P]-labeled
oligonucleotide in a final volume of 20 lL and was
incubated at room temperature for 15 minute. The free
and protein-bound oligonucleotides were resolved by
electrophoresis on a 5% polyacrylamide gel in a 0.59
Tris-borate EDTA buffer. After electrophoresis, the gel
was dried and exposed to autoradiography film (East-
man Kodak Co., Rochester, NY, USA). The images were
processed with Adobe Photoshop CS3 extended (Adobe
Systems Inc, San Jos�e, CA, USA) and the densitometric
analyses of the NF-jB-binding bands were analyzed
using ImageJ software. (Rasband WS, National Insti-
tutes of Health, Bethesda, MD, USA).
CagA Strains
The cagA gene encodes a cytotoxin-associated gene A
antigen (CagA) protein, an important bacterial viru-
lence factor. Genomic DNA from the bacterial strains
was PCR-amplified using two sets of synthetic oligonu-
cleotide primers as described elsewhere [33]. The
amplified PCR products were resolved in 1% agarose
gels containing Tris/borate/EDTA using 100 bp (Gibco
BRL; Gaithersburg, MD, USA) as a molecular weight
marker. The agarose gels were stained with ethidium
bromide and viewed under short-wavelength UV light.
The strains were considered to be CagA positive when
at least one of the reactions was positive.
Ethics
This study was approved by the Research Ethical Com-
mittee of the Medical Faculty of the Universit�e Libre de
© 2014 John Wiley & Sons Ltd, Helicobacter 19: 157–167 159
Bontems et al. NF-jB and severity of H. pylori gastritis

Bruxelles, and informed consent was obtained from the
patients or their parents.
Data Analysis
The statistical analysis was performed using Statistical
Package for Social Sciences (SPSS; IBM, Armonk, NY,
USA), version 21. The medians and the ranges were
calculated for all continuous variables as well as reparti-
tion for qualitative parameters. The performance of the
Pearson chi-square test was calculated for unpaired
qualitative variables. The distributions of non-Gaussian
continuous variable between two groups were com-
pared using the nonparametric Mann–Whitney U-test
and the Kruskal–Wallis test for more than two groups.
Spearman’s rank correlation was used to measure the
statistical dependence between two continuous vari-
ables. Statistical significance was set up at the p < .05
level, and all p values were two-tailed.
Results
Frequency of Gastric and Duodenal Ulcers
Through 2007–2008, 1484 upper GI endoscopies were
performed in 1279 pediatric patients and 1046 endos-
copies in 1010 adult patients. Gastric or duodenal ulcers
with a diameter of at least 5 mm were found less fre-
quently in children than in adults (20/1279 children –
1.6% vs 58/1010 adults – 5.7%, OR 0.30, 95% CI
0.10–0.86, p = .02). Ulcers were also less frequently
associated with H. pylori infection in children than in
adults (8/20 vs 40/58, OR 0.26, 95% CI 0.16–0.78,
p < .0001). The median age for children with ulcer was
14.5 years (range 1.7–16.1) and 7.0 years (range 0.1–
17.9) for those without ulcer.
Cellular Density of Immune Cells in the Antral
Mucosa
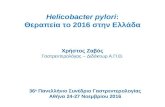
Neutrophils
Neutrophil densities were compared in the antrum and
in the fundus (Fig. 1) in the different age groups.
Among the controls, there was virtually no neutrophil
within the lamina propria and the epithelium of the
antral and fundic mucosa. Among the H. pylori-infected
patients, the median neutrophil count per field
increased significantly in all age groups in the lamina
propria of the antrum and the fundus. In the epithe-
lium, the neutrophil count increased only in adults in
the antrum. When considering the effect of age, we
found a significant correlation with neutrophil density
in the antrum of infected patients (Spearman’s rank
correlation: lamina propria r = .456, p = .003 – epithe-
lium r = .500, p = .001), but not in the fundus of these
patients or in uninfected controls.
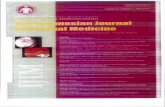
CD20, CD3, and CD8 cells
Among the controls (Fig. 2), there was virtually no
CD20-positive cell in the lamina propria and in the epi-
thelium except a very low density found in the lamina
propria of adults.
Among the H. pylori-infected patients, there was a
significant increase in the densities of CD20-positive
cells in all age groups in the lamina propria, but not in
the epithelium. When considering the effect of age, no
correlation found with CD20 density in the lamina pro-
pria or in the epithelium of infected patients or in
uninfected controls.
Among the controls, CD3-positive cells were found
in the lamina propria and in the epithelium. The den-
sity was slightly higher in the lamina propria of the
younger children compared with older ones and to
adults, whereas in the epithelium, the densities were
comparable in all age groups.
Among the H. pylori-infected patients, the CD3
densities in the lamina propria and in the epithelium
remained comparable with controls in children younger
than 8 years and increased significantly in older chil-
dren and in adults. When considering the effect of age,
a positive correlation was found with CD3 density in
the lamina propria of infected patients (r = .516,
p = .001), but not in the epithelium or in uninfected
controls.
Among the controls, there were some CD8-positive
cells in the lamina propria and in the epithelium, the
densities being lower than those of CD3 cells. There
was no difference between age groups.
Among the H. pylori-infected patients, we only
observed an increased density of CD8 cells in the lam-
ina propria of adult patients. However, there was no
correlation between age and density of CD8 cells in the
lamina propria or in the epithelium of infected patients
or uninfected controls.
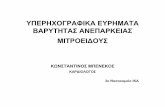
Activation of the Transcription Factor NF-jB
Density of cells expressing activated NF-jB
The number of cells expressing activated NF-jB in the
lamina propria and in the epithelium of the antral
mucosa was increased in infected adults, whereas it is
similar to controls in infected children (Fig. 3). The lack
of activation of NF-jB correlates with the lower
© 2014 John Wiley & Sons Ltd, Helicobacter 19: 157–167160
NF-jB and severity of H. pylori gastritis Bontems et al.

recruitment of neutrophils in children compared with
adults (r = .672, p < 10�4).
Electrophoresis Mobility Shift Assay
DNA-binding activity of NF-jB is similar in infected
children and in controls, but largely increased in
infected adults (Fig. 4).
Helicobacter pylori Density and CagA-Positive
Strains
Helicobacter pylori density
The densities of H. pylori in the antral and the fundic
mucosa were evaluated using the Sydney system, a
semiquantitative score. Although there is a tendency to
have a higher bacterial load between the pediatric age
groups, the differences were not significant (Fig. 5).
Moreover, the severity of the recruitment of immune
cells in the mucosa was not correlated with the bacterial
load.
Frequency of CagA-positive strains
Infection with a CagA-positive strain was found in 5 of
10 children younger than 8 years, 4 of 10 in the 8–17
years age group, and in 5 of 10 adults (NS). Densities of
immune cell in patients with a CagA-positive strain were
generally slightly higher in each age group, but a statisti-
cal significance was only observed for the number of
neutrophils in the epithelium of adults (p = .02).
Figure 1 Comparison of the densities of neutrophils in the lamina propria and in the epithelium of uninfected and H. pylori-infected children
(below 8 years of age and 8–17 years) and adults with nonulcer dyspepsia. There are 10 patients in each group. Neutrophil densities are
expressed as number of cells per surface unit, defined using a calibrated eyepiece graticule at 4009 magnification, in the lamina propria and as
number of cells per 100 epithelial cells surface in the epithelium. Data are compared between groups using the Mann–Whitney U-test (NS, not
significant). In this boxplot representation, ends of the whiskers represent �1.5 interquartile range; outliers are indicated by a circle and extreme
outliers (outside �3 interquartile range) by a star.
© 2014 John Wiley & Sons Ltd, Helicobacter 19: 157–167 161
Bontems et al. NF-jB and severity of H. pylori gastritis

Figure 2 Comparison of the densities of CD20-stained cells (B cells), CD3-stained cells (T cells), and CD8-stained cells (cytotoxic T cells) cells in
the lamina propria and in the epithelium of uninfected and H. pylori-infected children (below 8 years of age and 8–17 years) and adults with non-
ulcer dyspepsia. There are 10 patients in each group. Neutrophil densities are expressed as number of cells per surface unit, defined using a cali-
brated eyepiece graticule at 4009 magnification, in the lamina propria and as number of cells per 100 epithelial cells surface in the epithelium.
Data are compared between groups using the Mann–Whitney U-test (NS, not significant). In this boxplot representation, ends of the whiskers rep-
resent �1.5 interquartile range; outliers are indicated by a circle and extreme outliers (outside �3 interquartile range) by a star.
© 2014 John Wiley & Sons Ltd, Helicobacter 19: 157–167162
NF-jB and severity of H. pylori gastritis Bontems et al.

Figure 3 Comparison of the densities of cells stained using an anti-p65 NF-jB antibody that binds to the active form of NF-jB in the lamina pro-
pria and in the epithelium of uninfected and H. pylori-infected children (below 8 years of age and 8–17 years) and adults with nonulcer dyspepsia.
There are 10 patients in each group. Neutrophil densities are expressed as number of cells per surface unit, defined using a calibrated eyepiece
graticule at 4009 magnification, in the lamina propria and as number of cells per 100 epithelial cells surface in the epithelium. Data are compared
between groups using the Mann–Whitney U-test (NS, not significant). In this boxplot representation, ends of the whiskers represent �1.5 inter-
quartile range; outliers are indicated by a circle and extreme outliers (outside �3 interquartile range) by a star.
A
B
Figure 4 Cell extracts were prepared from antral biopsies of consec-
utive patients with nonulcer dyspepsia. The interaction between NF-
jB and consensus radioactively labeled DNA probes was detected by
gel electrophoresis (Eight consecutive adults, five uninfected controls,
nos. 1–4 and three adults infected with H. pylori nos 5–7 followed by
six children; three uninfected controls nos. 8–10 and three infected
with H. pylori nos 11–13). The double arrows indicate NF-jB-binding
activity while single arrow represents nonspecific binding (ns). Pr,
probe alone.
A
B
Figure 5 Comparison of the H. pylori densities in the antrum (A) and
in the fundus (B) between the infected children (below 8 years of age
and 8–17 years) and the adults with nonulcer dyspepsia. There are 10
patients in each group. H. pylori densities are evaluated using the
Sydney system, a semiquantitative score. Although there is a ten-
dency to have a higher bacterial load between the pediatric age
groups, the differences are not significant.
© 2014 John Wiley & Sons Ltd, Helicobacter 19: 157–167 163
Bontems et al. NF-jB and severity of H. pylori gastritis

Discussion
Although it is generally established that PUD is a rare
pathology in pediatrics, there were no data comparing its
frequency in children and in adults. Ulcers and erosions
in the stomach and in the duodenum also occur in chil-
dren as previously shown by several studies [34–36].
PUD is, however, more frequent in older children than
in very young ones [36]. A preliminary study performed
in our center showed that PUD in H. pylori-infected
patients appears after the age of 8 years and that the
frequency of PUD gradually increases up to adulthood
(P. Bontems, S. Cadranel, unpublished data). In this
paper, we showed clearly that the frequency of PUD was
lower in children than in adults and, more interestingly,
that PUD was less frequently associated with H. pylori
infection in children than in adults.
The other question we tried to elucidate was the
possible underlying reasons explaining that ulcers in
children occur more rarely in the course of an H. pylori
infection. As the clinical outcome of the infection
depends to a large degree on the relative balance of the
immune responses, we compared innate and adaptive
mucosal response between children and adults. The
response in children is generally claimed to correspond
to an early immune response and in adults to a more
chronic response to H. pylori infection. Humoral
response was first investigated by several research
teams, who have found that this response was weaker
and that the antigens recognized in children were
different [23,24]. The Th1 type mucosal cytokine secre-
tion was also less intense [6,7,37]. The results concern-
ing the severity of gastritis were more conflicting.
Indeed, some previous studies did not show differences
in the severity of gastritis in children compared with
adults nor differences in bacterial density, atrophy, and
intestinal metaplasia being the only parameter that
showed a linear tendency to increase with age [30]. We
found the same results in a pilot study (P. Bontems,
A. Neuman-Ova, P. Heimann, J.M. Devaster, V. Segers,
C. Deprez, S. Cadranel, unpublished data). On the
contrary, Whitney et al. [31] found that in children,
the bacterial density was higher with a milder density
of neutrophils, plasma cells, and eosinophil compared
with adults. Harris et al. [25] found similar results.
Due to these inconsistent results between past stud-
ies, we decided to conduct a comparative study where
the cellular densities of immune cells were counted
manually. We found that, in the lamina propria, the
densities of neutrophils and of CD20 cells were
increased compared with the controls in all age groups.
The density of CD3 cells also increased except in chil-
dren younger than 8 years, whereas CD8 cells
increased only in adults. In the epithelium, the density
of neutrophils increased only in adults and CD3 cells
only in children of at least 8 years of age. There was no
increase in CD20 or CD8 cells. A correlation was found
between age and densities of neutrophils and of CD3
cells in the lamina propria. A correlation was also
found between age and the activation status of NF-jB.Some previous studies suggested that the recruit-
ment of neutrophils is lower or inconstant. Indeed, in
these noncomparative studies, the presence of neu-
trophils in the gastric mucosa was observed more fre-
quently than in controls but only in 35–75% of
infected children [38,39]. When comparing children
from population with high or low risk of cancer, Be-
doya et al. [40] observed that all of the components of
the inflammatory response to H. pylori infection
described in adults are present in children, but that
older children display higher degrees of neutrophil and
lymphocyte infiltrates and of H. pylori colonization than
younger ones. In our study, we only observed an
absence of neutrophils in some areas delimited by the
eyepiece graticule in children younger than 8 years (5/
10), while neutrophils were always present in older
children and in adults.
Our study has some limitations. Indeed, we mainly
studied the antral mucosa because the severity of the
gastritis using the Sydney system score always showed
more severe features in this area of the stomach. The
children were arbitrarily separated into two subgroups
using a cutoff of 8 years of age. This cutoff was decided
after a ROC curve was performed when evaluating the
accuracy of serology in children (clearly lower before
the age of 8 years) [23]. Several studies have ascribed
an increased risk of peptic ulcer and/or gastric cancer
with bacterial genes encoding virulence factors (such as
vacA genes, the cag PAI, or homB) [8,41]. In this study,
CagA-positive strains were equally distributed and
could not explain the differences observed in the densi-
ties of immune cells. However, other virulence factors
were not determined.
Interleukin-8 (IL-8) and IL-17 have been shown to
be the cytokines mainly implicated in the mucosal
recruitment of neutrophils and their secretion related
to NF-jB activation. As we were not able to measure
these cytokines, we cannot provide evidence that a
lower secretion of these cytokines due to a lower acti-
vation of NF-jB causes the failure of neutrophil recruit-
ment. One study suggested that lower neutrophil
recruitment might be due to lack of IL-8 secretion [42]
while others have shown that IL-8 protein levels were
significantly higher in the gastric mucosa of infected
children compared with uninfected ones, but the secre-
tion of IL-8 was not compared with the level observed
© 2014 John Wiley & Sons Ltd, Helicobacter 19: 157–167164
NF-jB and severity of H. pylori gastritis Bontems et al.

in adults [5,37,43–45]. Interestingly, IL-17 mRNA was
found increased in the mucosa of infected children
compared with uninfected ones [5], but IL-17 level was
found lower in infected children than in adults [27].
The activation of NF-jB in H. pylori infection was
first described by Sharma et al. [10] in vitro. Since
then, several studies have shown in vivo that the
NF-jB activity is higher in the gastric mucosa of
H. pylori-infected adults, activated NF-jB being present
in different cells in the epithelium and in the lamina
propria. NF-jB activation correlates with mucosal IL-8
secretion [46], activity of gastritis [12,13,16] (a semi-
quantitative score of neutrophil influx), and H. pylori
density [13]. In another study, however, the correlation
with bacterial density was not observed [16]. In this
study, we showed that the activation of NF-jB in
H. pylori-infected children is weaker than in adults and
correlated with neutrophil recruitment and CagA sta-
tus, but not with bacterial density. Many pathways can
be implicated in the activation of NF-jB during the
infection, and there are conflicting results to determine
the major ones in vivo [47]. Some are CagA dependent
and others CagA independent. No study so far has com-
pared the stimulation of the upstream signaling path-
ways implicated in the activation of NF-jB, such as
those mediated by TLRs and NOD-like receptors in dif-
ferent age groups. It is highly tempting to compare the
immune response of children and adults to H. pylori
infection in terms of qualitative and quantitative innate
immune signaling induced by this bacterium. One pos-
sibility is that induced inflammasome-mediated inflam-
matory pathways might be intrinsically different in
children in comparison with the adults due to the
immaturity of the innate defenses in children’s under
8 years [48]. Indeed, a recent study has shown that, in
comparison with adults, infants from birth onwards
exhibit a steady decline in IL-8 and IL-1-beta produc-
tion induced by alum, an unrelated inflammasome
activator commonly used as vaccine adjuvant [49].
In conclusion, PUD was less frequent in children
and less frequently caused by H. pylori infection. The
different clinical outcomes observed from the infection
in children, especially under the age of 8 years, can be
the consequence of the lower mucosal immune
response. We showed additional evidences that the gas-
tric mucosal recruitment of neutrophils, of CD3+, and
of CD8+ cells is lower in infected children in compari-
son with infected adults. The lower activation status of
NF-jB transcription factor in children may be either a
direct consequence of the lesser mucosal recruitment of
neutrophils, of CD3+, and of CD8+ cells or, more proba-
bly, of the existence of an overall more subtle inflam-
matory innate host defense in children.
Acknowledgements and Disclosures
We are thankful to Anouk Neuman-Ova for assistance in read-
ing the histologic sections, Nathalie Vennist for the numerous
immunohistochemical staining, and Pierre Heiman for instruct-
ing how to read sections and participation in the development
of the immunohistochemical methods. This study was
supported by grants of The Belgian Kids Foundation and the
Belgian Helicobacter study group.
Author Contributions
All authors have participated in the concept and design
of the study, interpretation of the data, drafting and
revising of the manuscript and have approved the man-
uscript as submitted. Data collection and data encoding
were performed by P Bontems and A Burette. EMSA
was performed by E Aksoy. Histologic analysis was per-
formed by P Bontems, V Segers, and C Deprez. Statisti-
cal analysis was performed by P Bontems.
References
1 Malfertheiner P, M�egraud F, O’Morain CA, et al. Management
of Helicobacter pylori infection–the maastricht IV/florence con-
sensus report. Gut 2012;61:646–64.
2 Miendje Deyi VY, Vanderpas J, Bontems P, Van Den Borre C,
De Koster E, Cadranel S, Burette A. Marching cohort of Helicob-
acter pylori infection over two decades (1988-2007): combined
effects of secular trend and population migration. Epidemiol
Infect 2010;139:572–80.
3 Ernst PB, Gold BD. The disease spectrum of Helicobacter pylori:
the immunopathogenesis of gastroduodenal ulcer and gastric
cancer. Annu Rev Microbiol 2000;54:615–40.
4 Allison CC, Ferrero RL. Role of virulence factors and host
cell signaling in the recognition of Helicobacter pylori and the
generation of immune responses. Future Microbiol
2010;5:1233–55.
5 Luzza F, Parrello T, Sebkova L, Pensabene L, Imeneo M,
Mancuso M, La Vecchia AM, Monteleone G, Strisciuglio P,
Pallone F. Expression of proinflammatory and Th1 but not Th2
cytokines is enhanced in gastric mucosa of Helicobacter pylori
infected children. Dig Liver Dis 2001;33:14–20.
6 Bontems P, Robert F, Van Gossum A, Cadranel S, Mascart F.
Helicobacter pylori modulation of gastric and duodenal mucosal T
cell cytokine secretions in children compared with adults. Heli-
cobacter 2003;8:216–26.
7 Lopes AI, Quiding-Jarbrink M, Palha A, Ruivo J, Monteiro L,
Oleastro M, Santos A, Fernandes A. Cytokine Expression in
Pediatric Helicobacter pylori Infection. Clin Vaccine Immunol
2005;12:994–1002.
8 Wroblewski LE, Peek RM, Wilson KT. Helicobacter pylori and
gastric cancer: factors that modulate disease risk. Clin Microbiol
Rev 2010;23:713–39.
9 M€uller A, Solnick JV. Inflammation, immunity, and vaccine
development for Helicobacter pylori. Helicobacter 2011;16(Suppl
1):26–32.
10 Sharma SA, Tummuru MK, Blaser MJ, Kerr LD. Activation of
IL-8 gene expression by Helicobacter pylori is regulated by
transcription factor nuclear factor-kappa B in gastric epithelial
cells. J Immunol 1998;160:2401–7.
© 2014 John Wiley & Sons Ltd, Helicobacter 19: 157–167 165
Bontems et al. NF-jB and severity of H. pylori gastritis

11 Isomoto H, Mizuta Y, Miyazaki M, Takeshima F, Omagari K,
Murase K, Nishiyama T, Inoue K, Murata I, Khono S. Implica-
tion of NF-kappaB in Helicobacter pylori-associated gastritis.
Am J Gastroenterol 2000;95:2768–76.
12 van Den Brink GR, ten Kate FJ, Ponsioen CY, Rive MM, Tytgat
GN, van Deventer SJ, Peppelenbosh MP. Expression and activa-
tion of NF-kappa B in the antrum of the human stomach. J
Immunol 2000;164:3353–9.
13 Doger FK, Meteoglu I, Ozkara E, Erkul ZK, Okyay P, Y€ukselen
V. Expression of NF-kappaB in Helicobacter pylori infection. Dig
Dis Sci 2006;51:2306–9.
14 Bartels M, Schweda AT, Dreikhausen U, Frank R, Resch K, Beil
W, Nourbakhsh M. Peptide-mediated disruption of NFkappaB/
NRF interaction inhibits IL-8 gene activation by IL-1 or
Helicobacter pylori. J Immunol 2007;179:7605–13.
15 Atherton JC, Blaser MJ. Coadaptation of Helicobacter pylori and
humans: ancient history, modern implications. J Clin Invest
2009;119:2475–87.
16 Moorchung N, Srivastava AN, Sharma AK, Achyut BR, Mittal
B. Nuclear factor kappa-B and histopathology of chronic
gastritis. Indian J Pathol Microbiol 2010;53:418–21.
17 Pender SL, Tickle SP, Docherty AJ, Howie D, Wathen NC,
MacDonald TT. A major role for matrix metalloproteinases in T
cell injury in the gut. J Immunol 1997;158:1582–90.
18 Yokoyama T, Otani Y, Kurihara N, et al. Matrix
metalloproteinase expression in cultured human gastric
wall fibroblasts–
interactions with Helicobacter pylori isolated from patients
with ulcers. Aliment Pharmacol Ther 2000;14(Suppl 1):193–8.
19 G€o~oz M, G€o~oz P, Smolka AJ. Epithelial and bacterial metallo-
proteinases and their inhibitors in H. pylori infection of human
gastric cells. Am J Physiol Gastrointest Liver Physiol 2001;281:
G823–32.
20 Mori N, Sato H, Hayashibara T, SenbaM, Geleziunas R,Wada A,
Hirayama T, Yamamoto N.Helicobacter pylori induces matrix
metalloproteinase-9 through activation of nuclear factor kappaB.
Gastroenterology 2003;124:983–92.
21 Bergin PJ, Anders E, Sicheng W, Erik J, Jennie A, Hans L,
Michetti P, Pan-Hammarstr€om Q, Quiding-J€arbrink M.
Increased production of matrix metalloproteinases in Helicobact-
er pylori-associated human gastritis. Helicobacter 2004;9:201–10.
22 Pillinger MH, Marjanovic N, Kim S-Y, et al. Helicobacter pylori
stimulates gastric epithelial cell MMP-1 secretion via CagA-
dependent and -independent ERK activation. J Biol Chem
2007;282:18722–31.
23 Corvaglia L, Bontems P, Devaster JM, Heimann P, Glupczynski
Y, Keppens E, Cadranel S. Accuracy of serology and 13C-urea
breath test for detection of Helicobacter pylori in children. Pediatr
Infect Dis J 1999;18:976–9.
24 OkudaM,Miyashiro E, KoikeM, Tanaka T, BouokaM, Okuda S,
Yoshikawa N. Serodiagnosis of Helicobacter pylori infection is
not accurate for children aged below 10. Pediatr Int 2002;44:
387–90.
25 Harris PR, Wright SW, Serrano C, et al. Helicobacter pylori
Gastritis in Children Is Associated With a Regulatory T-Cell
Response. Gastroenterology 2008;134:491–9.
26 Cho KY, Cho MS, Seo JW. FOXP3+ regulatory T cells in
children with Helicobacter pylori infection. Pediatr Dev Pathol
2012;15:118–26.
27 Freire de Melo F, Rocha AMC, Rocha GA, et al. A regulatory
instead of an IL-17 T response predominates in Helicobacter
pylori-associated gastritis in children. Microbes Infect
2012;14:341–7.
28 Ernst PB, Gold BD. Helicobacter pylori in childhood: new insights
into the immunopathogenesis of gastric disease and implica-
tions for managing infection in children. J Pediatr Gastroenterol
Nutr 1999;28:462–73.
29 Dixon MF, Genta RM, Yardley JH, Correa P. Classification and
grading of gastritis. The updated Sydney System. International
Workshop on the Histopathology of Gastritis, Houston 1994.
Am J Surg Pathol 1996;20:1161–81.
30 Meining A, Behrens R, Lehn N, Bayerd€orffer E, Stolte M. Dif-
ferent expression of Helicobacter pylori gastritis in children: evi-
dence for a specific pediatric disease? Helicobacter 1996;1:92–7.
31 Whitney AE, Guarner J, Hutwagner L, Gold BD. Helicobacter
pylori gastritis in children and adults: comparative histopatho-
logic study. Ann Diagn Pathol 2000;4:279–85.
32 Miendje Deyi VY, Bontems P, Vanderpas J, De Koster E, Nto-
unda R, Van Den Borre C, Cadranel S, Burette A. Multicenter
survey of routine determinations of resistance of Helicobacter
pylori to antimicrobials over the last 20 years (1990 to 2009) in
Belgium. J Clin Microbiol 2011;49:2200–9.
33 Queiroz DM, Mendes EN, Carvalho AS, Rocha GA, Oliveira
AM, Soares TF, Santos A, Cabral M, Nogueira A. Factors associ-
ated with Helicobacter pylori infection by a cagA-positive strain
in children. J Infect Dis 2000;181:626–30.
34 Egbaria R, Levine A, Tamir A, Shaoul R. Peptic ulcers and ero-
sions are common in Israeli children undergoing upper endos-
copy. Helicobacter 2008;13:62–8.
35 Tam YH, Lee KH, To KF, Chan KW, Cheung ST. Helicobacter
pylori-positive versus Helicobacter pylori-negative idiopathic
peptic ulcers in children with their long-term outcomes.
J Pediatr Gastroenterol Nutr 2009;48:299–305.
36 Kalach N, Bontems P, Koletzko S, et al. Frequency and risk
factors of gastric and duodenal ulcers or erosions in children: a
prospective 1-month European multicenter study. Eur J
Gastroenterol Hepatol 2010;22:1174–81.
37 Shimizu T, Haruna H, Ohtsuka Y, Kaneko K, Gupta R,
Yamashiro Y. Cytokines in the gastric mucosa of children with
Helicobacter pylori infection. Acta Paediatr 2004;93:322–6.
38 De Giacomo C, Fiocca R, Villani L, Lisato L, Licardi G, Diegoli N,
Donadini A, Maggiore G.Helicobacter pylori infection and chronic
gastritis: clinical, serological, and histologic correlations in chil-
dren treated with amoxicillin and colloidal bismuth subcitrate.
J Pediatr Gastroenterol Nutr 1990;11:310–6.
39 Mu~noz L, Camorlinga M, Hern�andez R, Giono S, Ram�on G,
Mu~noz O, Torres J. Immune and proliferative cellular
responses to Helicobacter pylori infection in the gastric mucosa of
Mexican children. Helicobacter 2007;12:224–30.
40 Bedoya A, Garay J, Sanzon F, Bravo LE, Bravo JC, Correa H,
Craver R, Fontham E, Du J, Correa P. Histopathology of gastri-
tis in Helicobacter pylori-infected children from populations at
high and low gastric cancer risk. Hum Pathol 2003;34:206–13.
41 Oleastro M, Cordeiro R, Ferrand J, et al. Evaluation of the clin-
ical significance of homB, a novel candidate marker of Helicob-
acter pylori strains associated with peptic ulcer disease. J Infect
Dis 2008;198:1379–87.
42 Whitney AE, Emory TS, Marty AM, O’Shea PA, Newman GW,
Gold BD. Increased macrophage infiltration of gastric mucosa
in Helicobacter pylori infected children. Dig Dis Sci 2000;45:
1337–42.
43 Guiraldes E, Duarte I, Pe~na A, Godoy A, EspinosaMN, Bravo R,
Larrain F, Schultz M, Harris P. Proinflammatory cytokine
expression in gastric tissue from children with Helicobacter
pylori-associated gastritis. J Pediatr Gastroenterol Nutr
2001;33:127–32.
© 2014 John Wiley & Sons Ltd, Helicobacter 19: 157–167166
NF-jB and severity of H. pylori gastritis Bontems et al.

44 Camorlinga-Ponce M, Aviles-Jimenez F, Cabrera L, Hern�andez-
Pando R, Mu~noz O, Soza J, Torres J. Intensity of inflammation,
density of colonization and interleukin-8 response in the gastric
mucosa of children infected with Helicobacter pylori. Helicobacter
2003;8:554–60.
45 Dzierzanowska-Fangrat K, Michalkiewicz J, Cielecka-Kuszyk J,
Nowak M, Celinska-Cedro D, Rozynek E, Dzierzanowska D,
Crabtree J. Enhanced gastric IL-18 mRNA expression in Helicob-
acter pylori-infected children is associated with macrophage
infiltration, IL-8, and IL-1b mRNA expression. Eur J Gastroenter-
ol Hepatol 2008;20:314–9.
46 Isomoto H, Miyazaki M, Mizuta Y, Takeshima F, Murase K,
Inoue K, Yamasaki K, Murata I, Koji T, Kohno S. Expression of
nuclear factor-kappaB in Helicobacter pylori-infected gastric
mucosa detected with southwestern histochemistry. Scand J
Gastroenterol 2000;35:247–54.
47 Lamb A, Chen L-F. The many roads traveled by Helicobacter
pylori to NFjB activation. Gut Microbes 2010;1:109–13.
48 Kollmann TR, Levy O, Montgomery RR, Goriely S.
Innate immune function by Toll-like receptors: distinct
responses in newborns and the elderly. Immunity 2012;37:
771–83.
49 Lisciandro JG, Prescott SL, Nadal-Sims MG, Devitt CJ, Pomat
W, Siba PM, Tulic MC, Holt PG, Strickland D, van den Big-
gelaar AH. Ontogeny of Toll-like and NOD-like receptor-medi-
ated innate immune responses in Papua New Guinean infants.
PLoS One 2012;7:e36793.
© 2014 John Wiley & Sons Ltd, Helicobacter 19: 157–167 167
Bontems et al. NF-jB and severity of H. pylori gastritis