Name Occupation Age D.O.B. / / Date / /20 Address City ... Occupation_____ Age_____...
1
Click here to load reader
Transcript of Name Occupation Age D.O.B. / / Date / /20 Address City ... Occupation_____ Age_____...

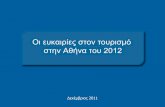
Name__________________ Occupation__________________ Age_____ D.O.B.___/___/___ Date___/___/20___
Address_________________ City/State_______________ Phone (home/work/cell)__________ Email_____________
VAs 1
Far (no Rx)
Far (w/ Rx)
Near (no Rx)
Near (w/ Rx)
Old
Rx Sph. Cyl. Axis Add Prism OCs
Lens
Tint
Lens
Type
OD 20/ 20/ 20/ 20/
Right . . ° + . Δ
/
OS 20/ 20/ 20/ 20/
Left . . ° + . Δ
/
OU 20/ 20/ 20/ 20/
IPD / Other Information:
2
R
/ @
Problems/Complaints: (ٱ routine exam)
L
/ @
3 Δ 13A Δ
4
R . – . × ° 20/ General Health: (ٱ good)
20/
L . – . × ° 20/
Medications: (ٱ none)
5 R + . (dynamic add over #4 @ 20") L + . (dynamic add over #4 @ 20")
7
R . – . × ° 20/ Medical Allergies: (ٱ none)
20/
L . – . × ° 20/ Eye History: (ٱ n.p.)
8 Δ 9 / Family History: (ٱ n.p.) diabetes_____________ hypertension_____________ cancer_____________
10 / 11 / glaucoma_____________ cataracts_____________ armd_____________ other_________________
12A,B Δ R R sup / R inf / ___________________________________________________________________________________
13B Δ [– Δ / +1.00D gradient] Right Anterior Left
14A R + . add
15A Δ Lids/Adnexa Pupils (ٱ PERRLA) Lids/Adnexa
L + . add Cornea Iris Lens Cornea Iris Lens
14B + . add 15B Δ
16 / / / 17 / / /
18A,B Δ R R sup / R inf /
19 ____in. or ____cm. ( . D) Right Posterior Left
20 + . D 21 – . D A/V: / Fundus
C/D: . V / . H
A/V: / Fundus
C/D: . V / . H
Tono: ____________
R ______ mm Hg
L ______ mm Hg
Anes.: ____________ Time: ____________
Cover Test (___unaided ___#7 ___present Rx): Analysis:
PR Δ PP Δ Pursuits: Saccades: Stereopsis: " of arc other: test: _____________________________________ Plan:
Color Perception: test: _____________________________________
Worth 4-Dot: _____red _____green _____white
Return:_____________
http://www.tedmontgomery.com/the_eye