Measurement of β-tryptase in postmortem serum, pericardial fluid, urine and vitreous humor in the...
6
Measurement of b-tryptase in postmortem serum, pericardial fluid, urine and vitreous humor in the forensic setting Lionel Comment a , Luca Reggiani Bonetti b , Patrice Mangin a , Cristian Palmiere a, * a University Center of Legal Medicine, Lausanne University Hospital, 21 rue du Bugnon, 1011 Lausanne, VD, Switzerland b Department of Diagnostic Services, Pathology and Legal Medicine, Section of Pathology, University of Modena and Reggio Emilia, Modena, Italy 1. Introduction Acute mast cell activation occurs in a number of pathologic conditions and is commonly observed in patients with allergic reactions. In living subjects, measurements of histamine and histamine metabolites in plasma and urine may be as accurate as b-tryptase in confirming mast cell activation and serve as diagnostic markers [1,2]. Conversely, determinations of b-tryptase in urine for diagnostic purposes have only been occasionally performed in the clinical field and with contradictory results [3,4]. Postmortem serum from femoral blood represents the ideal biological sample for b-tryptase measurement in the forensic setting [5–11]. However, it may be partially or completely unavailable in some specific situations when limited quantities of sampled blood are usually allotted to toxicological investiga- tions as a priority. In these cases, the collection of alternative biological fluids to analyze is of utmost importance. In this study, we investigated b-tryptase levels in postmortem serum from femoral blood, urine, vitreous humor and pericardial fluid in a series of cases that underwent medico-legal investiga- tions. The aim of our analyses was to characterize b-tryptase distribution in tested biological samples and therefore evaluate their usefulness for diagnostic purposes in the forensic setting. 2. Material and methods 2.1. Subjects A total of 94 subjects (72 males and 22 females) with a mean age of 45.2 years (range 19–68 years) were selected. Case inclusion criteria consisted of postmortem interval (not exceeding 48 h) and availability of postmortem serum from femoral blood, urine, vitreous humor and pericardial fluid during autopsy. Forensic Science International 240 (2014) 29–34 A R T I C L E I N F O Article history: Received 7 August 2013 Received in revised form 11 February 2014 Accepted 1 April 2014 Available online 13 April 2014 Keywords: Beta-tryptase Mast cells Anaphylaxis Postmortem biochemistry Pericardial fluid Forensic pathology A B S T R A C T In the realm of forensic pathology, b-tryptase measurement for diagnostic purposes is performed in postmortem serum obtained from femoral blood. This may be partially or completely unavailable in some specific cases, such as infant autopsies and severely damaged bodies. The aim of this study was to investigate the usefulness of determining b-tryptase levels for diagnostic purposes in alternative biological samples. Urine, vitreous humor and pericardial fluid were selected and measured in 94 subjects including: fatal anaphylaxis following contrast material administration (6 cases), hypothermia (10 cases), diabetic ketoacidosis (10 cases), gunshot suicide (10 cases), heroin injection-related deaths (18 cases), trauma (10 cases), sudden death with minimal coronary atherosclerosis (10 cases), severe coronary atherosclerosis without myocardial infarction (10 cases) and severe coronary atherosclerosis with myocardial infarction (10 cases). Postmortem serum and pericardial fluid b-tryptase levels higher than the clinical reference value (11.4 ng/ml) were systematically identified in fatal anaphylaxis following contrast material administration and 6 cases unrelated to anaphylaxis. b-tryptase concentrations in urine and vitreous humor were lower than the clinical reference value in all cases included in this study. Determination of b-tryptase in pericardial fluid appears to be a possible alternative to postmortem serum in the early postmortem period when femoral blood cannot be collected during autopsy and biochemical investigations are required to objectify increased b-tryptase levels. ß 2014 Elsevier Ireland Ltd. All rights reserved. * Corresponding author. Tel.: +41 21 314 49 61/+41 79 556 69 89; fax: +41 21 314 70 90. E-mail addresses: [email protected], [email protected] (C. Palmiere). Contents lists available at ScienceDirect Forensic Science International jou r nal h o mep age: w ww.els evier .co m/lo c ate/fo r sc iin t http://dx.doi.org/10.1016/j.forsciint.2014.04.006 0379-0738/ß 2014 Elsevier Ireland Ltd. All rights reserved.
Transcript of Measurement of β-tryptase in postmortem serum, pericardial fluid, urine and vitreous humor in the...

Forensic Science International 240 (2014) 29–34
Measurement of b-tryptase in postmortem serum, pericardial fluid,urine and vitreous humor in the forensic setting
Lionel Comment a, Luca Reggiani Bonetti b, Patrice Mangin a, Cristian Palmiere a,*a University Center of Legal Medicine, Lausanne University Hospital, 21 rue du Bugnon, 1011 Lausanne, VD, Switzerlandb Department of Diagnostic Services, Pathology and Legal Medicine, Section of Pathology, University of Modena and Reggio Emilia, Modena, Italy
A R T I C L E I N F O
Article history:
Received 7 August 2013
Received in revised form 11 February 2014
Accepted 1 April 2014
Available online 13 April 2014
Keywords:
Beta-tryptase
Mast cells
Anaphylaxis
Postmortem biochemistry
Pericardial fluid
Forensic pathology
A B S T R A C T
In the realm of forensic pathology, b-tryptase measurement for diagnostic purposes is performed in
postmortem serum obtained from femoral blood. This may be partially or completely unavailable in
some specific cases, such as infant autopsies and severely damaged bodies. The aim of this study was to
investigate the usefulness of determining b-tryptase levels for diagnostic purposes in alternative
biological samples. Urine, vitreous humor and pericardial fluid were selected and measured in 94
subjects including: fatal anaphylaxis following contrast material administration (6 cases), hypothermia
(10 cases), diabetic ketoacidosis (10 cases), gunshot suicide (10 cases), heroin injection-related deaths
(18 cases), trauma (10 cases), sudden death with minimal coronary atherosclerosis (10 cases), severe
coronary atherosclerosis without myocardial infarction (10 cases) and severe coronary atherosclerosis
with myocardial infarction (10 cases). Postmortem serum and pericardial fluid b-tryptase levels higher
than the clinical reference value (11.4 ng/ml) were systematically identified in fatal anaphylaxis
following contrast material administration and 6 cases unrelated to anaphylaxis. b-tryptase
concentrations in urine and vitreous humor were lower than the clinical reference value in all cases
included in this study. Determination of b-tryptase in pericardial fluid appears to be a possible
alternative to postmortem serum in the early postmortem period when femoral blood cannot be
collected during autopsy and biochemical investigations are required to objectify increased b-tryptase
levels.
� 2014 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at ScienceDirect
Forensic Science International
jou r nal h o mep age: w ww.els evier . co m/lo c ate / fo r sc i in t
1. Introduction
Acute mast cell activation occurs in a number of pathologicconditions and is commonly observed in patients with allergicreactions. In living subjects, measurements of histamine andhistamine metabolites in plasma and urine may be as accurate asb-tryptase in confirming mast cell activation and serve asdiagnostic markers [1,2]. Conversely, determinations of b-tryptasein urine for diagnostic purposes have only been occasionallyperformed in the clinical field and with contradictory results [3,4].
Postmortem serum from femoral blood represents the idealbiological sample for b-tryptase measurement in the forensicsetting [5–11]. However, it may be partially or completelyunavailable in some specific situations when limited quantities
* Corresponding author. Tel.: +41 21 314 49 61/+41 79 556 69 89;
fax: +41 21 314 70 90.
E-mail addresses: [email protected], [email protected]
(C. Palmiere).
http://dx.doi.org/10.1016/j.forsciint.2014.04.006
0379-0738/� 2014 Elsevier Ireland Ltd. All rights reserved.
of sampled blood are usually allotted to toxicological investiga-tions as a priority. In these cases, the collection of alternativebiological fluids to analyze is of utmost importance.
In this study, we investigated b-tryptase levels in postmortemserum from femoral blood, urine, vitreous humor and pericardialfluid in a series of cases that underwent medico-legal investiga-tions. The aim of our analyses was to characterize b-tryptasedistribution in tested biological samples and therefore evaluatetheir usefulness for diagnostic purposes in the forensic setting.
2. Material and methods
2.1. Subjects
A total of 94 subjects (72 males and 22 females) with a meanage of 45.2 years (range 19–68 years) were selected. Case inclusioncriteria consisted of postmortem interval (not exceeding 48 h) andavailability of postmortem serum from femoral blood, urine,vitreous humor and pericardial fluid during autopsy.

L. Comment et al. / Forensic Science International 240 (2014) 29–3430
Of these, 6 cases (5 males, 1 female) concerned individualsadmitted to local hospitals where they underwent diagnosticprocedures with contrast material administration. None of thesecases had experienced general anesthesia prior to investigation.Arterial pressure markedly decreased approximately 3–10 minafter contrast material administration in all cases. Patients lostconsciousness, became unresponsive, collapsed and were imme-diately transferred to the intensive care units. Electromechanicaldissociation arrest was evident on electrocardiogram and patientsdied between 45 and 90 min after having lost consciousnessdespite cardiopulmonary resuscitation attempts. Acute systemichypersensitivity reactions to contrast material were suspected inall these cases.
The bodies were transferred from the local hospitals to themedico-legal center by request of the inquiring authorities (publicprosecutor) for postmortem investigations and reconstruction ofthe sequence of events responsible for death.
10 cases (7 males, 3 females) were hypothermia fatalitiesselected according to circumstantial elements that suggestedexposure to cold, autopsy findings consistent with the hypothesisof hypothermia (frost erythema of the outer hip areas, elbows andknees as well as Wischnewsky spots in the gastric mucosa),biochemical investigation results consistent with the hypothesis ofhypothermia (increased blood acetone and b-hydroxybutyratelevels, increased cortisol concentrations in postmortem serum,increased cortisol and adrenaline values in urine) as well as theexclusion of other causes of death based on all postmortem findings.
10 cases (all males) were diabetic ketoacidosis deaths selectedaccording to postmortem biochemical findings (vitreous glucoseconcentrations higher than 10 mmol/l, corresponding to 104 mg/dl, femoral or cardiac b-hydroxybutyrate levels higher than2.5 mmol/l, corresponding to 26 mg/dl) as well as the exclusionof other causes of death based on all postmortem investigationresults.
10 cases (all males) concerned individuals who committedsuicide and had a gunshot wound to the head.
18 cases (15 males, 3 females) concerned heroin addictedindividuals who died shortly after heroin injection. These caseswere selected according to toxicology results confirming heroinoverdose as well as the exclusion of other causes of death based onall postmortem findings.
10 cases (6 males, 4 females) were individuals who hadsuddenly died in the presence of witnesses, with minimal coronaryatherosclerosis at postmortem examination. Based on the resultsof all investigations, the cause of death was attributed to cardiacarrhythmia and cardiac arrest in the absence of macroscopic ormicroscopic abnormalities other than minimal coronary athero-sclerosis.
10 cases (7 males, 3 females) were individuals with severecoronary artery atherosclerosis, coronary artery calcifications andmyocardial fibrosis at autopsy, without acute coronary thrombosisor myocardial infarction. Based on the results of all investigations,the cause of death was determined to be cardiac arrhythmia andcardiac arrest in the presence of severe coronary artery athero-sclerosis and myocardial fibrosis.
10 cases (7 males, 3 females) were individuals with severecoronary artery atherosclerosis, acute coronary thrombosis andacute myocardial infarction at postmortem examination. Based onthe results of all postmortem investigations, the cause of death wasdetermined to be myocardial infarction in the presence of acutecoronary thrombosis.
Lastly, 10 cases (5 males, 5 females) were crash-involvedcyclists or pedestrians with rib fractures, pulmonary and cardiaccontusions as well as thoracic and abdominal hemorrhages. Basedon the results of all investigations, the cause of death wasdetermined to be multiple traumas.
In order to investigate the effect of decompositional changes onpericardial fluid b-tryptase levels, 10 autopsy cases with causes ofdeath unrelated to anaphylaxis, severe postmortem changes andavailable pericardial fluid at postmortem examination wereretrospectively selected. These cases exclusively underwentpericardial fluid b-tryptase determination.
2.2. Postmortem investigations
Complete conventional autopsy, histology, neuropathology andtoxicology were performed on all subjects after unenhancedcomputed tomography-scan (CT-scan). Conventional autopsieswere performed within 24 h after death (for hypothermia fatalitiesand bodies presenting severe postmortem changes autopsies wereperformed 24 h after body discovery).
Conventional histology included hematoxylin-eosin (HE) stainof the brain, heart, lung, liver, kidney and spleen. Eosinophils anddegranulated mast cells were specifically sought out with PagodaRed (PR) stain [12]. HE and PR stains were performed after tissuefixation in formaldehyde.
Immunohistochemistry using anti-tryptase antibodies was alsoperformed on spleen tissue samples. Biochemical investigationsincluded measurements of b-tryptase in postmortem serum,pericardial fluid, urine and vitreous humor.
2.3. Biological sample collection
Biological samples for toxicological and biochemical investiga-tions were collected as soon as possible on arrival of the bodies atthe morgue (vitreous humor) and during postmortem examination(femoral blood, pericardial fluid and urine).
Undiluted vitreous humor samples (between 1 and 3 ml) wereobtained by aspiration using a sterile needle and syringe. Right andleft vitreous samples were collected through a scleral puncture atthe lateral canthus, aspirated from the center of each eye, pooled inthe same syringe and mixed together. After collection, vitreoussamples were immediately centrifuged at 3000 � g for 15 min. Theseparated supernatant was collected and stored in preservative-free tubes. No specimens were excluded due to insufficient samplevolume. All samples were transferred to the laboratories immedi-ately post collection. When analyses were delayed, samples werestored at �20 8C.
Femoral blood samples were collected by aspiration with asterile needle and a syringe from the femoral vein(s) afterunenhanced CT-scan and before autopsy. Blood samples weredrawn after clamping the vein(s) at the proximal end and liftingthe lower limb(s) for several minutes. Blood was stored in tubescontaining sodium fluoride and tubes containing gel serumseparator. These latter were centrifuged immediately post collec-tion at 3000 � g for 15 min. After centrifugation, the separatedsupernatant (postmortem serum) was collected and stored inpreservative-free tubes. Whole femoral blood and postmortemserum samples were transferred to the laboratories immediatelyafter collection. When analyses were delayed, samples were storedat �20 8C.
Undiluted pericardial fluid samples (between 5 and 10 ml)were collected immediately post pericardium incision duringpostmortem examination. All samples were immediately cen-trifuged at 3000 � g for 15 min. After centrifugation, theseparated supernatant was collected and stored in preserva-tive-free tubes. When analyses were delayed, samples werestored at �20 8C.
Urine samples were collected by bladder aspiration duringautopsy and stored in preservative-free tubes. All samples weretransferred to the laboratories immediately post collection. Whenanalyses were delayed, samples were stored at �20 8C.

L. Comment et al. / Forensic Science International 240 (2014) 29–34 31
2.4. Analytical techniques
Mast cell b-tryptase was measured in postmortem serum fromfemoral blood, urine, pericardial fluid and vitreous humor with acommercial fluoroenzyme immunoassay (FEIA) method (Pharma-cia & Upjohn, Freiburg, Germany) with a detection limit below2 ng/ml.
2.5. Ethical issues
All relevant ethical issues were identified and discussed withthe local Ethical Committee. All cases collected for this studyunderwent medicolegal autopsies as requested by the publicprosecutor. Toxicology, histology and biochemistry, including b-tryptase measurements, were performed as part of the medicolegalinvestigations. All biological samples were anonymized prior toanalysis. No further ethical approval was necessary to performbiochemical investigations in the selected cases.
2.6. Reference values
The serum b-tryptase reference value in living subjects is11.4 ng/ml. The concentration of 45 ng/ml in postmortem serumfrom femoral blood was chosen as the reference value todiscriminate anaphylactic from nonanaphylactic deaths basedon the observations of Mayer et al. [8] and Edston et al. [10].
3. Results
Table 1 summarizes the main clinical information andpostmortem investigation findings in the group of individualswho underwent diagnostic procedures with contrast materialinjection. Table 2 summarizes biochemical results concerning allstudied groups.
In all the cases included in the group who had contrast materialadministered, postmortem examination revealed pulmonarycongestion and edema as well as generalized visceral congestion.
Table 1Summarizes the main clinical information and postmortem investigation findings in
contrast material injection.
Subject,
gender,
age
Clinical information Main MPCTA and
autopsy findings
M
Male 63 Noniodinate contrast material
administration (gadobutrol)
Pulmonary congestion and edema.
Cerebral edema. Coronary artery
atherosclerosis
Sp
an
Female 53 Iodinate contrast material
administration (iomeprol)
Pulmonary congestion and edema.
Cerebral edema
Sp
an
Male 74 Iodinate contrast material
administration (iohexol)
Pulmonary congestion and edema.
Cerebral edema. Coronary artery
atherosclerosis
Sp
an
Male 79 Iodinate contrast material
administration (iomeprol)
Pulmonary congestion and edema.
Cerebral edema. Laryngeal edema
Coronary artery atherosclerosis
Sp
an
Male 54 Iodinate contrast material
administration (iohexol)
Pulmonary congestion and edema.
Cerebral edema
Sp
an
Male 65 Iodinate contrast material
administration (iomeprol)
Pulmonary congestion and edema.
Cerebral edema
Sp
an
S: postmortem serum, PF: pericardial fluid, U: urine, VH: vitreous humor.
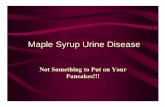
Brain swelling was also systematically observed. Mild to severecoronary artery atherosclerosis was identified in three cases.Histologically, PR stain showed the presence of typical histologicalpatterns of splenic and pulmonary eosinophilia and degranulatedmast cells. Immunohistochemistry confirmed the presence ofdegranulated mast cells in spleen samples (Fig. 1A and B).Toxicology did not provide any evidence of drug intoxication. Inall the cases included in this group, toxicological analyses didconfirmed however the presence of contrast media in peripheralblood in correspondence with their administration shortly beforeloss of patient consciousness and collapse. Moreover, contrastmaterial concentrations in blood were not only consistent with thedoses usually administered for diagnostic purposes but also withthose that were documented in medical records in each case.Biochemical results showed increased postmortem serum b-tryptase levels suggesting anaphylaxis (range 146–979 ng/ml).
Postmortem investigations did not provide any evidence forother possible causes of death. Hence, the cause of death wasdetermined to be anaphylaxis to contrast material administrationin all 6 cases of this group.
In all the cases included in this group, pericardial fluid b-tryptase levels were higher than the clinical reference value of11.4 ng/ml and even higher than the postmortem serum referencevalue of 45 ng/ml. The highest pericardial fluid concentration(119 ng/ml) was observed in the case that had the most elevatedpostmortem serum b-tryptase value (979 ng/ml).
Vitreous and urine b-tryptase levels were systematically lowerthan the clinical reference value of 11.4 ng/ml.
Postmortem serum and pericardial fluid b-tryptase levelshigher than the reference value of 11.4 ng/ml were observed indiabetic ketoacidosis deaths (one case), heroin injection-relateddeaths (two cases), severe coronary artery atherosclerosis (onecase), myocardial infarction (one case) and traumatic deaths (onecase, which had the most elevated tryptase concentration amongthe deaths unrelated to allergic reactions). b-tryptase concentra-tions were below the reference value of 11.4 ng/ml in vitreoushumor and urine in all studied groups.
the group of individuals who underwent diagnostic radiological procedures with
ain histology findings b-Tryptase levels
(S, PF, U, VH)
(ng/ml)
Final diagnosis
lenic and pulmonary eosinophilia
d degranulated mast cells
S 181
PF 56
U <11.4
VH <11.4
Anaphylaxis to contrast
material
lenic and pulmonary eosinophilia
d degranulated mast cells
S 146
PF 46
U <11.4
VH <11.4
Anaphylaxis to contrast
material
lenic and pulmonary eosinophilia
d degranulated mast cells
S 170
PF 52
U <11.4
VH <11.4
Anaphylaxis to contrast
material
lenic and pulmonary eosinophilia
d degranulated mast cells
S 979
PF 119
U <11.4
VH <11.4
Anaphylaxis to contrast
material
lenic and pulmonary eosinophilia
d degranulated mast cells
S 282
PF 81
U <11.4
VH <11.4
Anaphylaxis to contrast
material
lenic and pulmonary eosinophilia
d degranulated mast cells
S 151
PF 47
U <11.4
VH <11.4
Anaphylaxis to contrast
material

Table 2Summarizes biochemical results concerning all the studied groups.
Group of subjects Number of subject S b-tryptase (ng/ml) PF b-tryptase (ng/ml) VH b-tryptase (ng/ml) U b-tryptase (ng/ml)
Contrast material injection 6 181 56 <11.4 <11.4
146 46 <11.4 <11.4
170 52 <11.4 <11.4
979 119 <11.4 <11.4
282 81 <11.4 <11.4
151 47 <11.4 <11.4
Hypothermia 10 <11.4 <11.4 <11.4 <11.4
Diabetic ketoacidosis 10 24 (1 case out of 10) 19 <11.4 <11.4
Gunshot suicides 10 <11.4 <11.4 <11.4 <11.4
Heroin injection-related deaths 18 19 15 <11.4 <11.4
16 (2 cases out of 18) 14 <11.4 <11.4
Minimal coronary artery atherosclerosis 10 <11.4 <11.4 <11.4 <11.4
Severe coronary artery atherosclerosis 10 21 (1 case out of 10) 16 <11.4 <11.4
Myocardial infarction 10 29 (1 case out of 10) 20 <11.4 <11.4
Trauma 10 48 (1 case out of 10) 32 <11.4 <11.4
S: postmortem serum, PF: pericardial fluid, U: urine, VH: vitreous humor.
L. Comment et al. / Forensic Science International 240 (2014) 29–3432
Hypothermia fatalities, gunshot wound suicides and suddenunexpected deaths with minimal coronary artery atherosclerosisrevealed b-tryptase levels lower than the cut off value of 11.4 ng/ml in all tested fluids.
Fig. 1. (A) Immunohistochemical stain of paraffin-embedded, formalin-fixed spleen
tissue, using anti-tryptase antibodies. Tryptase-positive cells (mast cells) can be
identified (red dots) [20�]. (B) Immunohistochemical stain of paraffin-embedded,
formalin-fixed spleen tissue, using anti-tryptase antibodies. Tryptase-positive cells
(mast cells) and granules can be identified (red dots and arrows) [40�].
Lastly, pericardial fluid b-tryptase concentrations in bodieswith causes of death unrelated to allergic reactions (five gunshotsuicides and five hangings) and advanced decomposition rangedbetween 250 ng/ml and 5150 ng/ml, suggesting that severepostmortem changes are associated with massive b-tryptaseleaking in the pericardial space.
4. Discussion
To our knowledge, this is the first study focusing on b-tryptaselevels in biological samples other than postmortem serumcollected during autopsy.
The results of our investigations suggest that b-tryptasedetermination in pericardial fluid might be an alternative topostmortem serum, especially in the early postmortem period, inthose situations in which biochemistry is required and bloodsamples collected during autopsy prove insufficient.
Indeed, in both anaphylactic and nonanaphylactic deaths,increased postmortem serum b-tryptase levels (>11.4 ng/mg)were systematically associated with increased pericardial fluid b-tryptase concentrations (>11.4 ng/mg).
No case was identified that had exclusively increased pericar-dial fluid b-tryptase levels and normal postmortem serum b-tryptase concentrations. Conversely, vitreous and urine b-tryptaselevels were always lower than the reference value.
Moreover, our analysis suggests that severe decompositionalchanges are associated with high pericardial fluid b-tryptaseconcentrations even when the cause of death is unrelated toanaphylaxis.
Lastly, our findings concur with those reported in formerclinical and forensic investigations and confirm that highpostmortem serum b-tryptase levels may be identified in severalsituations unrelated to anaphylactic shock.
Anaphylaxis is an acute, life-threatening systemic reactionresulting from the release of mast cell and basophil mediators.Currently, histamine and b-tryptase are the laboratory parametersused in routine analyses for diagnostic purposes [13,14].
Although b-tryptase is released from mast cells at the sametime with histamine, it diffuses through tissues more slowly thanhistamine. The practical consequence of these different timecourses is that plasma samples for histamine measurements mustbe obtained within minutes of the onset of the episode. Conversely,samples for b-tryptase determination can be obtained up toseveral hours after the reaction begins, depending on its severity[8,9,14–18].
Besides situations of hypersensitivity, elevated b-tryptaselevels have been identified in both the clinical and forensic setting

L. Comment et al. / Forensic Science International 240 (2014) 29–34 33
in cases of trauma, drug injection (mostly heroin) related-deathsand sudden infant death syndrome (SIDS) [8–11,19–22].
Edston and van Hage-Hamsten [9,22] described elevated b-tryptase values in postmortem femoral blood in traumatic deathspossibly caused by direct mechanical injury to tissue mast cellswith subsequent degranulation and/or to mast cell lysis.
b-tryptase concentrations were measured in SIDS cases byseveral authors with results often indicating IgE-independent mastcell activation in a portion of these deaths, suggesting that allergicanaphylaxis is an unlikely etiology for SIDS [9,17,23–29].
Edston and van Hage-Hamsten [30] and by Fineschi et al. [31]observed increased blood tryptase levels in heroin related-deathscompared to control subjects. According to Edston and van Hage-Hamsten [30], the absence of correlations between total IgE andtryptase was consistent with the hypothesis that opiates likemorphine and heroin may stimulate mast cell degranulationwithout specific IgE antibody involvement.
Perskvist et al. [32,33] found that several cases of heroininjection-related deaths had high a + b-tryptase concentrationsand a degree of cardiac mast cell infiltration similar to thatobserved in anaphylactic deaths. These results suggested that mastcell degranulation into the myocardium could be involved in thepathogenesis of death following drug injection.
In the clinical field, Rook et al. [34] investigated b-tryptaseserum levels after the inhalation or intravenous administration ofhigh doses of pharmaceutically prepared heroin and observed thatb-tryptase levels increased after intravenous administration butnot following inhalation.
In addition to macrophages and other inflammatory cells, mastcells also reside in the arterial adventitia and intima. Locallyactivated mast cells have been postulated to participate in both thedevelopment and weakening of atherosclerotic plaques [35–39].Significant mast cell accumulation at the site of atheromatouserosion or rupture has been described in clinical studies. Based onthese findings, associations between blood tryptase levels andatherosclerotic plaque instability have been suggested by someauthors, though with diverging results [40–43].
In the realm of forensic pathology, Edston and van Hage-Hamsten [44] did not observe systematically increased postmor-tem serum b-tryptase and IgE values in coronary arterythrombosis deaths compared to control cases.
Lastly, as far as metabolic diseases are concerned, no clinicalstudies have established direct correlations between diabeticketoacidosis and mast cell activation as of yet. However, increasedmast cell degranulation was found in the kidneys of patients atdifferent clinical stages of diabetic nephropathy. Though themechanism of mast cell involvement in diabetic nephropathy isnot completely understood, numerous mast cell mediators couldtheoretically contribute to the progression of the disease [45,46].
In conclusion, though further studies are required to confirmthese preliminary observations, our findings suggest that elevatedpericardial fluid b-tryptase levels in the early postmortem periodcan be the consequence of b-tryptase elevation in systemiccirculation. Hence, measurements of b-tryptase in pericardial fluidin the early postmortem period might be used for diagnosticpurposes should postmortem serum prove unavailable duringautopsy. However, since higher b-tryptase levels can be observedin deaths unrelated to anaphylaxis and severe decomposition canbe accompanied by extremely elevated pericardial fluid b-tryptaseconcentrations, high pericardial fluid b-tryptase levels, individu-ally considered, must be interpreted carefully and after havingevaluated all potentially relevant data. Pathologists should neveryield to the temptation of univocally linking biochemical results tospecific causes of death and always remember that biochemicalresults must be integrated and interpreted in the context of globalfindings.
Conflict of interest statement
The authors have no conflict of interest to declare.
References
[1] P. Valent, H.P. Horny, M. Triggiani, M. Arock, Clinical and laboratory parameters ofmast cell activation as basis for the formulation of diagnostic criteria, Int. Arch.Allergy Immunol. 156 (2011) 119–127.
[2] K.D. Stone, C. Prussin, D.D. Metcalfe, IgE, mast cells, basophils, and eosinophils, J.Allergy Clin. Immunol. 125 (2 (Suppl. 2)) (2010) S73–S80.
[3] W. Boucher, M. el-Mansoury, X. Pang, G.R. Sant, Elevated mast cell tryptase in theurine of patients with interstitial cystitis, Br. J. Urol. 76 (1995) 94–100.
[4] M.R. Simon, M. Jan, J. Yee, U.S. Nori, J. Hu, C. Akin, L.B. Schwartz, Tryptase isnot cleared by the kidneys into the urine, Int. Arch. Allergy Immunol. 152 (2010)28–31.
[5] R.S. Pumphrey, I.S. Roberts, Postmortem findings after fatal anaphylactic reac-tions, J. Clin. Pathol. 53 (2000) 273–276.
[6] S. Luongo, C. Frontalini, M. Pesaresi, M. Valsecchi, A. Tagliabracci, Histopatho-logical markers for the diagnosis of anaphylactic death, Med. Sci. Law 51 (2011)30–36.
[7] U. Da Broi, C. Moreschi, Post-mortem diagnosis of anaphylaxis: a difficult task inforensic medicine, Forensic Sci. Int. 204 (2011) 1–5.
[8] D.E. Mayer, A. Krauskopf, W. Hemmer, K. Moritz, R. Jarisch, C. Reiter, Usefulness ofpost mortem determination of serum tryptase, histamine and diamine oxydase inthe diagnosis of fatal anaphylaxis, Forensic Sci. Int. 212 (2011) 96–101.
[9] E. Edston, M. van Hage-Hamsten, b-Tryptase measurements post-mortem inanaphylactic deaths and in controls, Forensic Sci. Int. 93 (1998) 135–142.
[10] E. Edston, O. Eriksson, M. van Hage, Mast cell tryptase in postmortem serum—reference values and confounders, Int. J. Legal Med. 121 (2007) 275–280.
[11] C. Palmiere, L. Comment, P. Mangin, Allergic reactions following contrast materialadministration: nomenclature, classification, and mechanisms, Int. J. Legal Med.128 (2014) 95–103, http://dx.doi.org/10.1007/s00414-013-0912-x.
[12] N. Trani, L.R. Bonetti, G. Gualandri, G. Barbolini, Immediate anaphylactic deathfollowing antibiotic injection: splenic eosinophilia easily revealed by pagoda redstain, Forensic Sci. Int. 181 (2008) 21–25.
[13] P. Lieberman, R.A. Nicklas, J. Oppenheimer, S.F. Kemp, D.M. Lang, D.I. Bernstein,J.A. Bernstein, A.W. Burks, A.M. Feldweg, J.N. Fink, P.A. Greenberger, D.B. Golden,J.M. James, S.F. Kemp, D.K. Ledford, P. Lieberman, A.L. Sheffer, D.I. Bernstein, J.Blessing-Moore, L. Cox, D.A. Khan, D. Lang, R.A. Nicklas, J. Oppenheimer, J.M.Portnoy, C. Randolph, D.E. Schuller, S.L. Spector, S. Tilles, D. Wallace, The diagnosisand management of anaphylaxis practice parameter: 2010 update, J. Allergy Clin.Immunol. 126 (2010) 477–480, e1-42.
[14] A. Sala-Cunill, V. Cardona, M. Labrador-Horrillo, O. Luengo, O. Esteso, T. Garriga,M. Vicario, M. Guilarte, Usefulness and limitations of sequential serum tryptasefor the diagnosis of anaphylaxis in 102 patients, Int. Arch. Allergy Immunol. 160(2013) 192–199.
[15] J.W. Yunginger, D.R. Nelson, D.L. Squillace, R.T. Jones, K.E. Holley, B.A. Hyma, L.Biedrzycki, K.G. Sweeney, W.Q. Sturner, L.B. Schwartz, Laboratory investigation ofdeaths due to anaphylaxis, J. Forensic Sci. 36 (1991) 857–865.
[16] Y. Ogawa, J.A. Grant, Mediators of anaphylaxis, Immunol. Allergy Clin. North Am.27 (2007) 249–260.
[17] L.B. Schwartz, J.W. Yunginger, J. Miller, R. Bokhari, D. Dull, Time course ofappearance and disappearance of human mast cell tryptase in the circulationafter anaphylaxis, J. Clin. Invest. 83 (1989) 1551–1555.
[18] P.W. van der Linden, C.E. Hack, J. Poortman, Y.C. Vivie-Kipp, A. Struyvenberg, J.K.van der Zwan, Insect-sting challenge in 138 patients: relation between clinicalseverity of anaphylaxis and mast cell activation, J. Allergy Clin. Immunol. 90(1992) 110–118.
[19] B. Randall, J. Butts, J.F. Halsey, Elevated postmortem tryptase in the absence ofanaphylaxis, J. Forensic Sci. 40 (1995) 208–211.
[20] H. Nishio, S. Takai, M. Miyazaki, H. Horiuchi, M. Osawa, K. Uemura, K. Yoshida, M.Mukaida, Y. Ueno, K. Suzuki, Usefulness of serum mast cell-specific chymaselevels for postmortem diagnosis of anaphylaxis, Int. J. Legal Med. 119 (2005) 331–334.
[21] K.D. Horn, J.F. Halsey, R.E. Zumwalt, Utilization of serum tryptase and immuno-globulin E assay in the postmortem diagnosis of anaphylaxis, Am. J. Forensic Med.Pathol. 25 (2004) 37–43.
[22] E. Edston, M. van Hage-Hamsten, Mast cell tryptase and hemolysis after trauma,Forensic Sci. Int. 131 (2003) 8–13.
[23] M.S. Platt, J.W. Yunginger, A. Sekula-Perlman, A.M. Irani, J. Smialek, H.G. Mirch-andani, L.B. Schwartz, Involvement of mast cells in sudden infant death syn-drome, J. Allergy Clin. Immunol. 94 (1994) 250–256.
[24] S.T. Holgate, C. Walters, A.F. Walls, S. Lawrence, D.J. Shell, S. Variend, P.J. Fleming,P.J. Berry, R.E. Gilbert, C. Robinson, The anaphylaxis hypothesis of sudden infantdeath syndrome (SIDS): mast cell degranulation in cot death revealed by elevatedconcentrations of tryptase in serum, Clin. Exp. Allergy 24 (1994) 1115–1122.
[25] L.L. Hagan, D.W. Goetz, C.H. Revercomb, J. Garriott, Sudden infant death syn-drome: a search for allergen hypersensitivity, Ann. Allergy Asthma Immunol. 80(1998) 227–231.
[26] E. Edston, E. Gidlund, M. Wickman, H. Ribbing, M. Van Hage-Hamsten, Increasedmast cell tryptase in sudden infant death—anaphylaxis hypoxia or artefact? Clin.Exp. Allergy 29 (1999) 1648–1654.
[27] M.G. Buckley, S. Variend, A.F. Walls, Elevated serum concentrations of beta-tryptase, but not alpha-tryptase, in Sudden Infant Death Syndrome (SIDS). An

L. Comment et al. / Forensic Science International 240 (2014) 29–3434
investigation of anaphylactic mechanisms, Clin. Exp. Allergy 31 (2001) 1696–1704.
[28] H. Nishio, K. Suzuki, Serum tryptase levels in sudden infant death syndrome inforensic autopsy cases, Forensic Sci. Int. 139 (2004) 57–60.
[29] S. D’Errico, M. Neri, I. Riezzo, G. Rossi, C. Pomara, E. Turillazzi, V. Fineschi, Beta-tryptase and quantitative mast-cell increase in a sudden infant death followinghexavalent immunization, Forensic Sci. Int. 179 (2008) 25–29.
[30] E. Edston, M. van Hage-Hamsten, Anaphylactoid shock—a common cause of deathin heroin addicts, Allergy 52 (1997) 950–954.
[31] V. Fineschi, R. Cecchi, F. Centini, L.P. Reattelli, E. Turillazzi, Immunohistochemicalquantification of pulmonary mast-cells and post-mortem blood dosages of tryp-tase and eosinophil cationic protein in 48 heroin-related deaths, Forensic Sci. Int.120 (2001) 189–194.
[32] N. Perskvist, E. Edston, Differential accumulation of pulmonary and cardiac mastcell-subsets and eosinophils between fatal anaphylaxis and asthma death, Fo-rensic Sci. Int. 169 (2007) 43–49.
[33] N. Perskvist, C. Soderberg, M. van Hage, E. Edston, Pathogenic role of cardiac mastcell activation/degranulation, TNF-alpha, and cell death in acute drug-relatedfatalities, Vasc. Health Risk Manage. 3 (2007) 1053–1062.
[34] E.J. Rook, A.P. van Zanten, W. Van den Brink, J.M. van Ree, J.H. Beijnen, Mast cellmediator tryptase levels after inhalation or intravenous administration ofhigh doses pharmaceutically prepared heroin, Drug Alcohol Depend. 85(2006) 185–190.
[35] P. Laine, M. Kaartinen, A. Penttila, P. Panula, T. Paavonen, P.T. Kovanen, Associa-tion between myocardial infarction and the mast cells in the adventitia of theinfarct-related coronary artery, Circulation 99 (1999) 361–369.
[36] P.T. Kovanen, M. Kaartinen, T. Paavonen, Infiltrates of activated mast cells at thesite of coronary atheromatous erosion or rupture in myocardial infarction,Circulation 92 (1995) 1084–1088.
[37] K.A. Lindstedt, P.T. Kovanen, Mast cells in vulnerable coronary plaques: potentialmechanisms linking mast cell activation to plaque erosion and rupture, Curr.Opin. Lipidol. 15 (2004) 567–573.
[38] J.L. Kelley, D.S. Chi, W. Abou-Auda, J.K. Smith, G. Krishnaswamy, The molecularrole of mast cells in atherosclerotic cardiovascular disease, Mol. Med. Today 6(2000) 304–308.
[39] H. Kervinen, M. Kaartinen, H. Makynen, T. Palosuo, M. Manttari, P.T. Kovanen,Serum tryptase levels in acute coronary syndromes, Int. J. Cardiol. 104 (2005)138–143.
[40] E.N. Deliargyris, B. Upadhya, D.C. Sane, G.J. Dehmer, J. Pye, S.C. Smith Jr., W.S.Boucher, T.C. Theoharides, Mast cell tryptase: a new biomarker in patients withstable coronary artery disease, Atherosclerosis 178 (2005) 381–386.
[41] M. Xiang, J. Sun, Y. Lin, J. Zhang, H. Chen, D. Yang, J. Wang, G.P. Shi, Usefulness ofserum tryptase level as an independent biomarker for coronary plaque instabilityin a Chinese population, Atherosclerosis 215 (2011) 494–499.
[42] P.L. van Haelst, J.R. Timmer, H.J. Crijns, H.F. Kauffman, R.O. Gans, J.J. van Doormaal,No long-lasting or intermittent mast cell activation in acute coronary syndromes,Int. J. Cardiol. 78 (2001) 75–80.
[43] K.J. Filipiak, B. Tarchalska-Krynska, G. Opolski, A. Rdzanek, J. Kochman, D.A. Kosior,A. Czlonkowski, Tryptase levels in patients after acute coronary syndromes: thepotential new marker of an unstable plaque? Clin. Cardiol. 26 (2003) 366–372.
[44] E. Edston, M. van Hage-Hamsten, Immunoglobulin E, mast cell-specific tryptaseand the complement system in sudden death from coronary artery thrombosis,Int. J. Cardiol. 52 (1995) 77–81.
[45] A. He, G.P. Shi, Mast cell chymase and tryptase as targets for cardiovascular andmetabolic diseases, Curr. Pharm. Des. 19 (2013) 1114–1125.
[46] J.M. Zheng, G.H. Yao, Z. Cheng, R. Wang, Z.H. Liu, Pathogenic role of mast cells inthe development of diabetic nephropathy: a study of patients at different stagesof the disease, Diabetologia 55 (2012) 801–811.