Diagnostic testing for nephrology casesSmall Animal Clinic University of Giessen, Germany Urology...
9
1 Prof. Dr. Reto Neiger Small Animal Clinic University of Giessen, Germany Urology y from Greek οὖρον ‐ oûron, "urine" and ‐λογία, ‐logia "study of" is the medical and surgical specialty that focuses on the urinary tracts of males and females Testing for urology cases y Urine (± urine culture) y Routine blood tests y GFR measurement y Diagnostic imaging y Radiographs (± contrast) y Ultrasound y Endoscopy y MRI / CT y Biopsy Urine collection y Mid‐stream voiding (cats: non‐absorbable litter) y Contamination from urethra etc. y Not advised for culture y Good to test for haematuria y Manual bladder expression y Use mainly in anaesthetised patients y Catheterisation y Male dog: pre‐measure length, no force; good for all purposes including urine culture y Female dog: dorsal recumbency, use speculum y Tomcats: extend penis caudally y Female cats: anaesthesia required, ventral recumbency Urine collection y Cystocentesis y Under palpation, blind, under ultrasound control y Advantage: no contamination, easy to perform, well tollerated y Disadvantage: may introduce micro‐ haematuria, puncture other organs, dissemination of transitional cell carcinoma (?) y Contraindication: <20‘000 PLT/μl Urinalysis y Perform as quickly as possible after collection (< 30 min) y Use minimum of 3 ml urine y If refrigerated – warm before analysis y Record type of collection y Colour and transparency y Specific gravity (refractometer) y Dip‐stick analysis y Sediment y Bacterial culture y Others
Transcript of Diagnostic testing for nephrology casesSmall Animal Clinic University of Giessen, Germany Urology...
1
Prof. Dr. Reto NeigerSmall Animal Clinic
University of Giessen, Germany
Urologyfrom Greek οὖρον ‐ oûron, "urine" and ‐λογία, ‐logia"study of" is the medical and surgical specialty that focuses on the urinary tracts of males and females
Testing for urology casesUrine (± urine culture)Routine blood testsGFR measurementDiagnostic imaging
Radiographs (± contrast)UltrasoundEndoscopyMRI / CT
Biopsy
Urine collectionMid‐stream voiding (cats: non‐absorbable litter)
Contamination from urethra etc.Not advised for cultureGood to test for haematuria
Manual bladder expressionUse mainly in anaesthetised patients
CatheterisationMale dog: pre‐measure length, no force; good for all purposes including urine cultureFemale dog: dorsal recumbency, use speculumTomcats: extend penis caudallyFemale cats: anaesthesia required, ventral recumbency
Urine collectionCystocentesis
Under palpation, blind, underultrasound controlAdvantage: no contamination, easyto perform, well tolleratedDisadvantage: may introduce micro‐haematuria, puncture other organs, dissemination of transitional cellcarcinoma (?)Contraindication: <20‘000 PLT/µl
UrinalysisPerform as quickly as possible after collection (< 30 min)Use minimum of 3 ml urineIf refrigerated – warm before analysisRecord type of collection
Colour and transparencySpecific gravity (refractometer) Dip‐stick analysisSedimentBacterial cultureOthers
2
Physical propertiesUrine colour
Derived fromurochromes
TransparencyNormally clearCloudy: mostlyWBC, casts, crystalls
OdorAmmonia odordue to bacteria
Urine specific gravity: 3 methods
Urine specific gravityOnly refractometer gives accurate results (never usedipstick value)Measures total number of solutes and their weight
1000 mg/dl (55 mmol/l) glucose increases USG by 0.0041000 mg/dl protein increased USH by 0.003
Measure USG BEFORE any fluid or drugs are given
1.000 1.008 1.0121.030 dog1.035 cat
>1.050
isohypo normal In dehydratedanimasthenuric
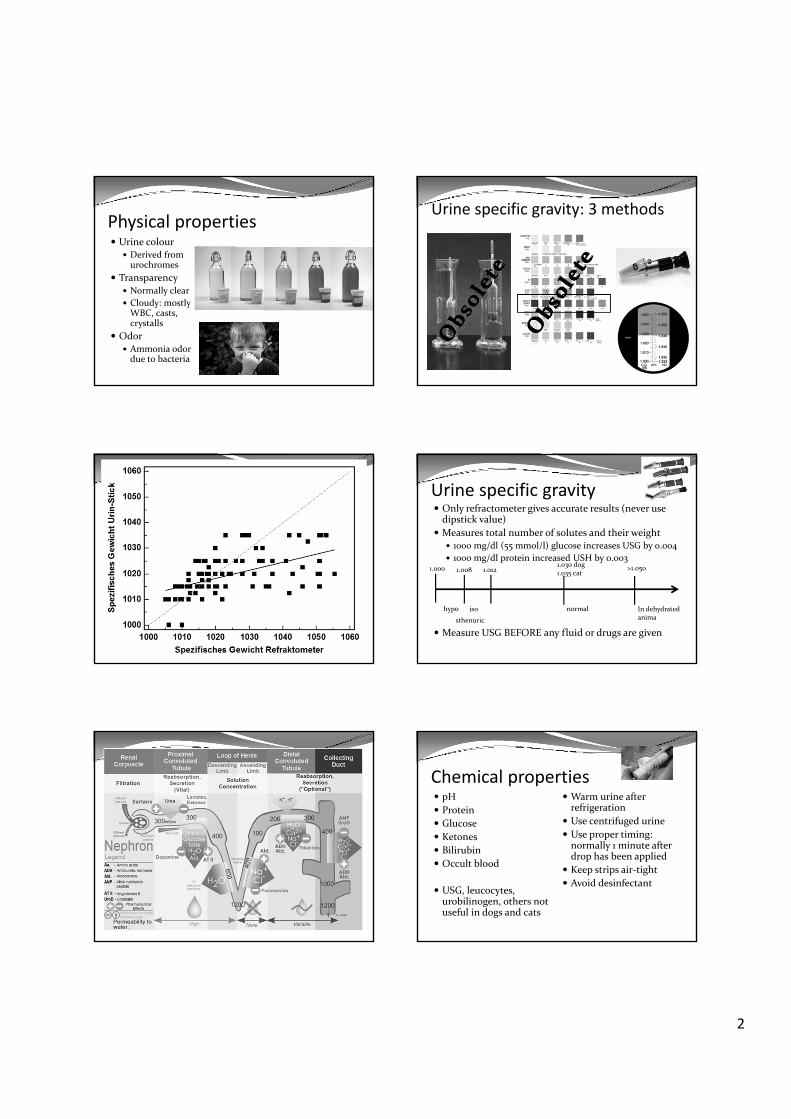
Chemical propertiespHProteinGlucoseKetonesBilirubinOccult blood
USG, leucocytes, urobilinogen, others not useful in dogs and cats
Warm urine after refrigerationUse centrifuged urineUse proper timing: normally 1 minute after drop has been appliedKeep strips air‐tightAvoid desinfectant
3
Urine pHNormally measured on dip‐stick but ok with any pH‐meterNormal: 5‐7.5Varies based on diet and acid‐base statusPlant based diet causes more alkaline urineCats have post‐prandial alkaline tideUTI with urease producing bacteria have alkaline urine
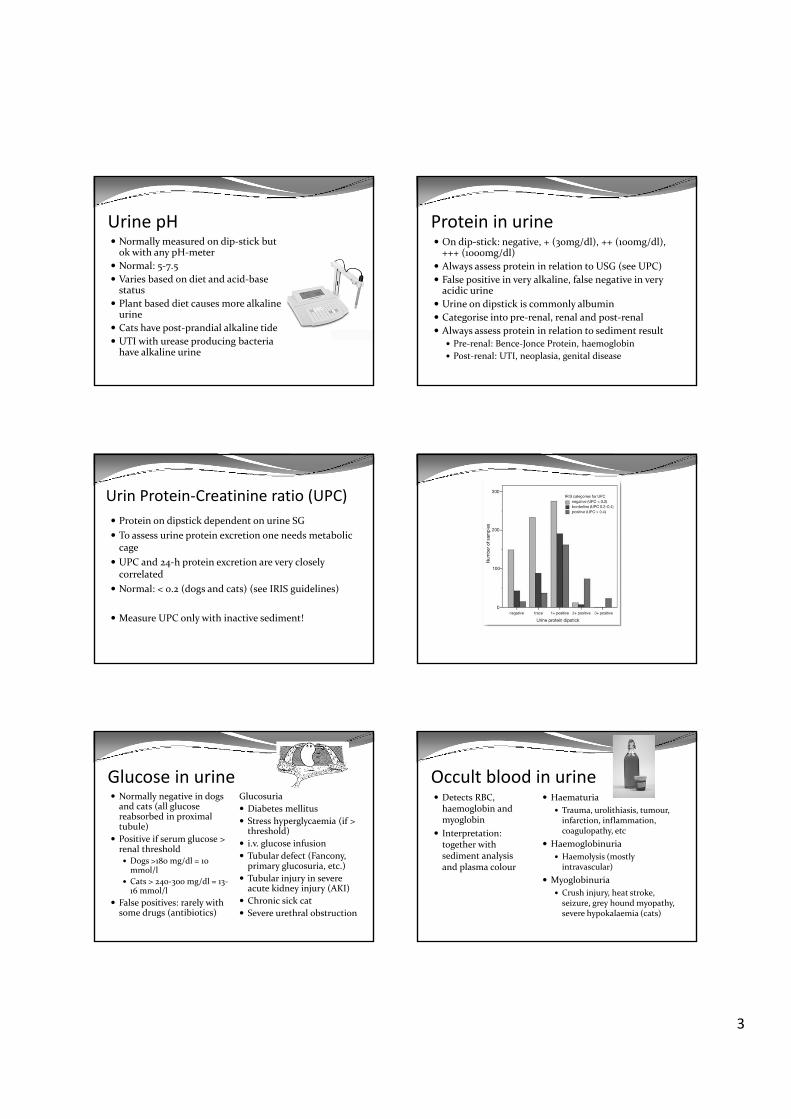
Protein in urineOn dip‐stick: negative, + (30mg/dl), ++ (100mg/dl), +++ (1000mg/dl)Always assess protein in relation to USG (see UPC)False positive in very alkaline, false negative in very acidic urineUrine on dipstick is commonly albuminCategorise into pre‐renal, renal and post‐renalAlways assess protein in relation to sediment result
Pre‐renal: Bence‐Jonce Protein, haemoglobinPost‐renal: UTI, neoplasia, genital disease
Urin Protein‐Creatinine ratio (UPC)Protein on dipstick dependent on urine SGTo assess urine protein excretion one needs metabolic cageUPC and 24‐h protein excretion are very closely correlated Normal: < 0.2 (dogs and cats) (see IRIS guidelines)
Measure UPC only with inactive sediment!
Glucose in urineNormally negative in dogs and cats (all glucose reabsorbed in proximal tubule)Positive if serum glucose > renal threshold
Dogs >180 mg/dl = 10 mmol/lCats > 240‐300 mg/dl = 13‐16 mmol/l
False positives: rarely with some drugs (antibiotics)
GlucosuriaDiabetes mellitusStress hyperglycaemia (if > threshold)i.v. glucose infusionTubular defect (Fancony, primary glucosuria, etc.)Tubular injury in severe acute kidney injury (AKI)Chronic sick catSevere urethral obstruction
Occult blood in urineDetects RBC, haemoglobin and myoglobinInterpretation: together with sediment analysis and plasma colour
HaematuriaTrauma, urolithiasis, tumour, infarction, inflammation, coagulopathy, etc
HaemoglobinuriaHaemolysis (mostly intravascular)
MyoglobinuriaCrush injury, heat stroke, seizure, grey hound myopathy, severe hypokalaemia (cats)
4
OthersKetones
Acetoacetate, acetone in urine give positive results, ß‐Hydroxybuturate (other breakdown of fatty oxidation) does notMost commonly in diabetic ketoacidosis or diabetic ketosis
BilirubinFrom breakdown of excessive haemoglobin (only conjugated bilirubin in urine)In dogs + (to ++ in males) of bilirubin can be normalIn cats bilirubin is always abnormalCases: haemolysis, liver disease, post‐hepatic disease, fever, starvation
SedimentMust be done on fresh urine samples (casts and crystals might otherwise disappear)Centrifugation: 1000‐1500 rpm for 5 minutesInterpretation: knowledge of USG and way of collectionRecord all findings and amount (neg, +, ++, +++)
Casts on 10x (LPF)Cells and bacteria on 40x (HPF)Crystals (type)Others (fat droplet, sperm, artefacts and contaminants)
Cells Red blood cells:
Numbers depend on collection technique (commonly < 5RBC / HPF)Can come from entire urogenital tractCauses: see lecture abnormal urine colour
White blood cells:Numbers depend on collection (more in voided samples) (commonly < 5WBC / HPF)Increased numbers = pyuriaIndication of inflammation in urinary or genital tract (localisation unclear). Most often UTI
CellsSquamous epithelial cells:
Common in voided and catheter samplesNo significance
Transitional epithelial cells:Arise from renal pelvis to urethraSeen in normal (few, during sampling) and abnormal samples(inflammation, trauma, FLUTD, etc.) May becomemalignant diagnosis of TCC
Renal epithelial cells:Are always abnormal (ischemia, inflammation, AKI, etc.)
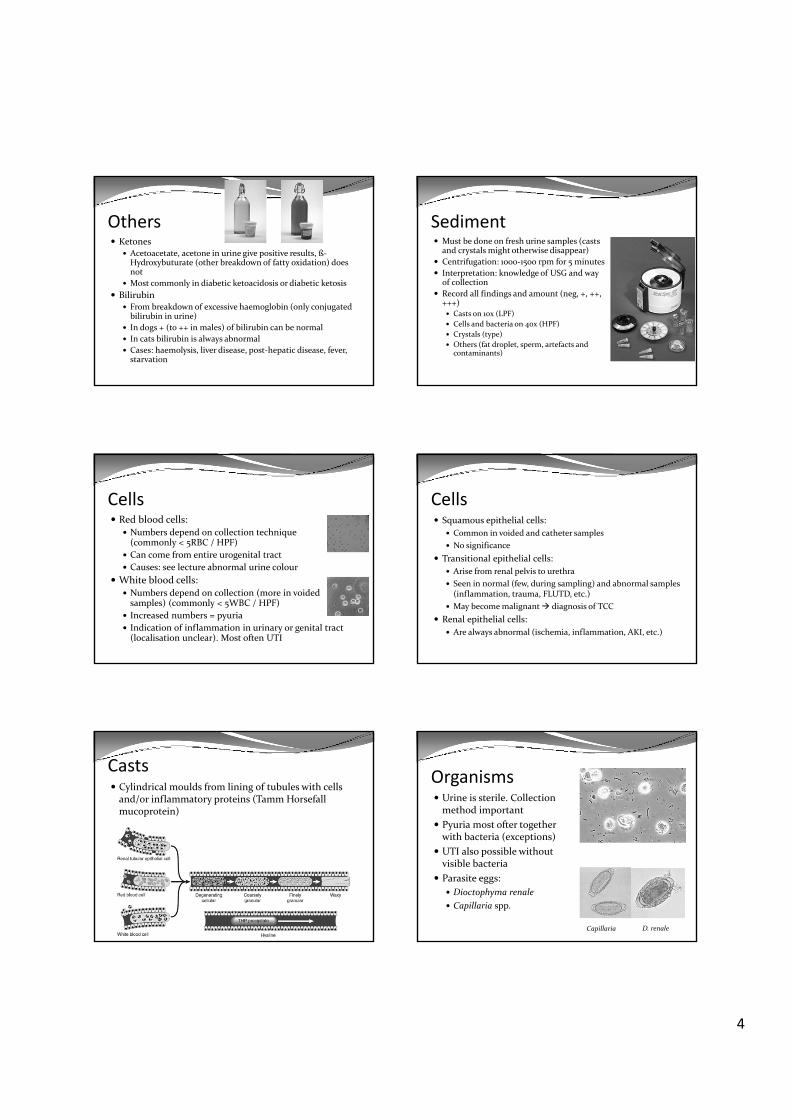
CastsCylindrical moulds from lining of tubules with cellsand/or inflammatory proteins (Tamm Horsefallmucoprotein)
OrganismsUrine is sterile. Collectionmethod importantPyuria most ofter togetherwith bacteria (exceptions)UTI also possible withoutvisible bacteriaParasite eggs:
Dioctophyma renaleCapillaria spp.
Capillaria D. renale
5
CrystalsMany crystals are normal in dogs and cats (struvite, calcium‐oxalate)!Crystalluria ≠ Urolithiasis!!Crystals may dissolve or form de novo (especially during refrigeration)Crystal formation depends on pH, temperatur und osmolality
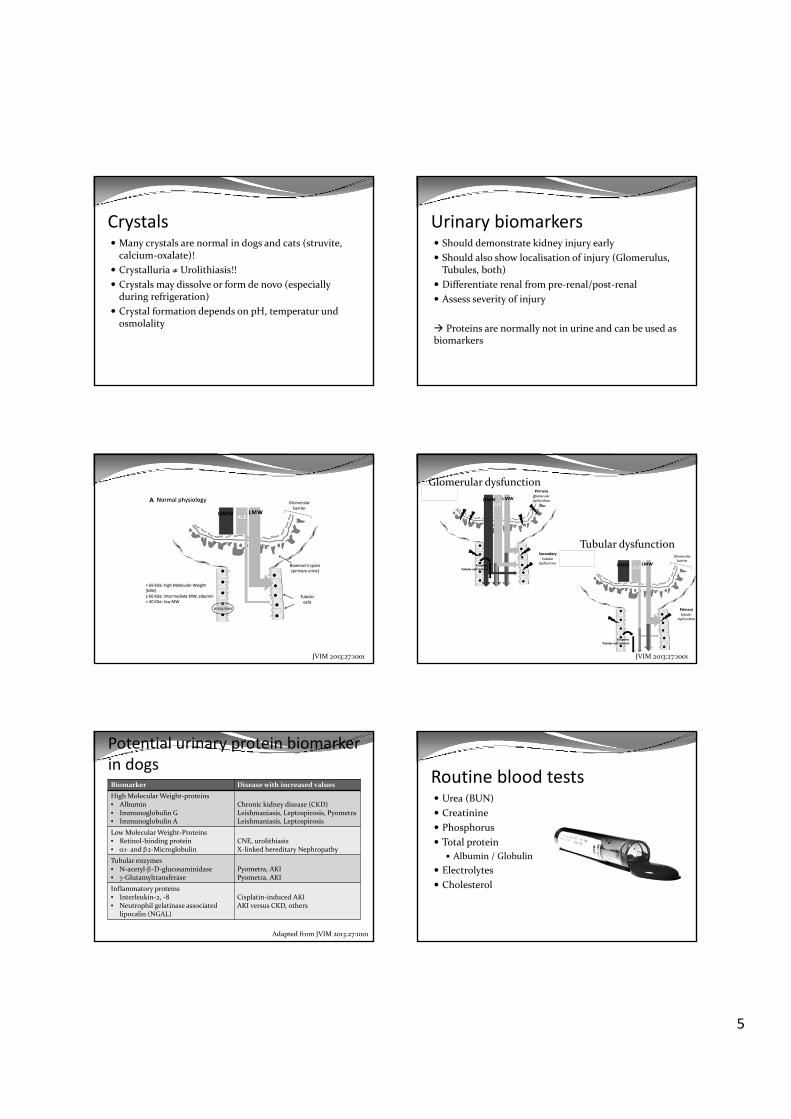
Urinary biomarkersShould demonstrate kidney injury earlyShould also show localisation of injury (Glomerulus, Tubules, both)Differentiate renal from pre‐renal/post‐renalAssess severity of injury
Proteins are normally not in urine and can be used as biomarkers
JVIM 2013:27:1001
Tubular dysfunction
Glomerular dysfunction
JVIM 2013:27:1001
Potential urinary protein biomarkerin dogsBiomarker Disease with increased valuesHigh Molecular Weight‐proteins• Albumin• Immunoglobulin G• Immunoglobulin A
Chronic kidney disease (CKD)Leishmaniasis, Leptospirosis, PyometraLeishmaniasis, Leptospirosis
LowMolecular Weight‐Proteins• Retinol‐binding protein• α1‐ and β2‐Microglobulin
CNE, urolithiasisX‐linked hereditary Nephropathy
Tubular enzymes• N‐acetyl‐β‐D‐glucosaminidase• γ‐Glutamyltransferase
Pyometra, AKIPyometra, AKI
Inflammatory proteins• Interleukin‐2, ‐8• Neutrophil gelatinase associated
lipocalin (NGAL)
Cisplatin‐induced AKIAKI versus CKD, others
Adapted from JVIM 2013:27:1001
Routine blood testsUrea (BUN)CreatininePhosphorusTotal protein
Albumin / GlobulinElectrolytesCholesterol
6
Azotaemia etc.Azotaemia = Increase in urea and creatinin
Pre‐renal azotaemia (decreased perfusion ofkideny; hypovolaemia, anaemia, heart failure, etc.)Renal azotaemia (intrinsic kidney diseasePost‐renal azotaemia (obstruction of urine flowirrespective where)
Uraemia = syndom of azotaemia with clinicalsigns (anorexia, vomiting, ulcers, bad breath, etc.)
USG
↑↑↑
↓↓↓
AzotaemiaUrea und Creatinine
Pre‐renal Renal Post‐renal
Urea:creatinin‐ratio does not differentiate
USG USG
Liver
NH3Ureacycle
Urea
Urea
Urea
FoodProteins
NH3
Colon
Body proteins
Amino acids
KidneyUrea
Urea
Urine75%
Faeces25%
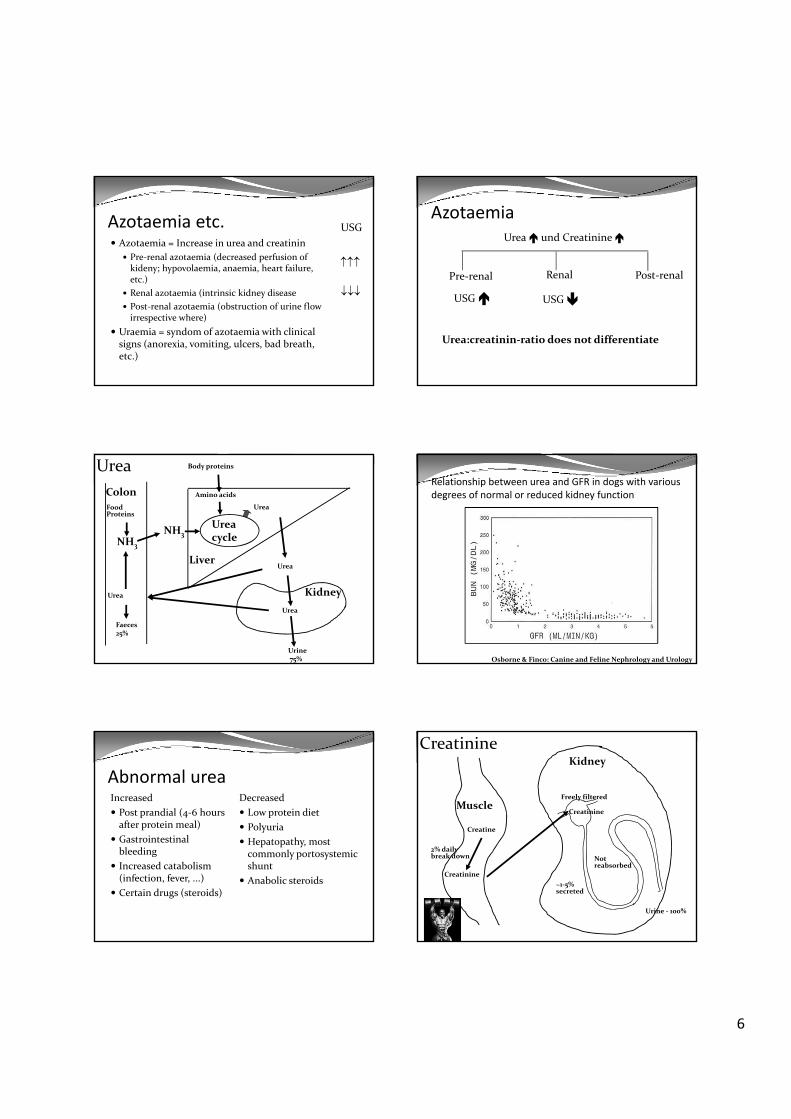
Relationship between urea and GFR in dogs with various degrees of normal or reduced kidney function
Osborne & Finco: Canine and Feline Nephrology and Urology
Abnormal ureaIncreasedPost prandial (4‐6 hoursafter protein meal)Gastrointestinal bleedingIncreased catabolism(infection, fever, ...)Certain drugs (steroids)
Decreased Low protein dietPolyuriaHepatopathy, most commonly portosystemicshuntAnabolic steroids
Kidney
Muscle
Creatine
Creatinine
2% dailybreak down
Creatinine
Freely filtered
~1‐5% secreted
Not reabsorbed
Creatinine
Urine ‐ 100%
7
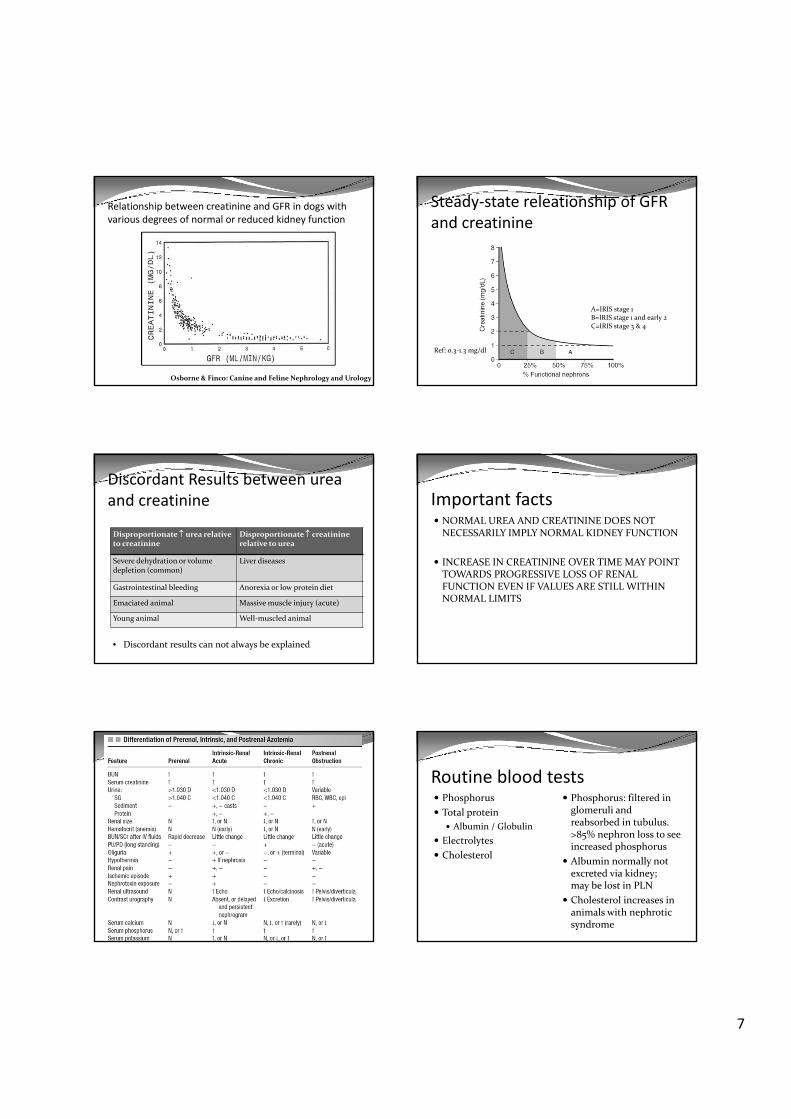
Osborne & Finco: Canine and Feline Nephrology and Urology
Relationship between creatinine and GFR in dogs with various degrees of normal or reduced kidney function
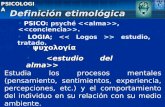
Steady‐state releationship of GFR and creatinine
A=IRIS stage 1B=IRIS stage 1 and early 2C=IRIS stage 3 & 4
Ref: 0.3‐1.3 mg/dl
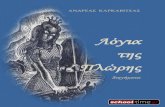
Discordant Results between ureaand creatinine
Disproportionate ↑ urea relative to creatinine
Disproportionate ↑ creatininerelative to urea
Severe dehydration or volume depletion (common)
Liver diseases
Gastrointestinal bleeding Anorexia or low protein diet
Emaciated animal Massive muscle injury (acute)
Young animal Well‐muscled animal
• Discordant results can not always be explained
Important factsNORMAL UREA AND CREATININE DOES NOT NECESSARILY IMPLY NORMAL KIDNEY FUNCTION
INCREASE IN CREATININE OVER TIME MAY POINT TOWARDS PROGRESSIVE LOSS OF RENAL FUNCTION EVEN IF VALUES ARE STILL WITHIN NORMAL LIMITS
Routine blood testsPhosphorusTotal protein
Albumin / GlobulinElectrolytesCholesterol
Phosphorus: filtered in glomeruli andreabsorbed in tubulus. >85% nephron loss to seeincreased phosphorusAlbumin normally not excreted via kidney;may be lost in PLNCholesterol increases in animals with nephroticsyndrome

8
Serum renal biomarkersCystatin C
NGALHomocysteinBig‐endothelin‐1
Glomerular filtration rate (GFR)Definition:
Estimated clearance, defined as volume of plasma cleared of a given substance over time
Influenced by many non‐renal factors (protein intake, hydration status, sodium balance, gender, age, breed, day‐to‐day variation, etc.)
Wide reference interval of normal GFR in healthy animals
Heiene R, Moe L: Pharmacokineatic Aspects of Measurement of Glomerular Filtration Rate in the Dog: A Review. JVIM 1998Lefebvre HP, Craig AJ, Braun JP. GFR in the dog: Breed effect. Proceedings of the 16th ECVIM–CA Congress, Amsterdam, 2006
GFR measurementGFR can not be measured directlyRenal clearance of substance (x) that is neither reabsorbed nor secreted by tubules = GFRGFR = V • C(U) / t • C (P) = ml/min
C(U) = concentration in urine (mg/ml)V= volume of urine (ml)t = specific amount of time (min)C(P) = concentration in plasma (mg/ml)
Heiene R, Moe L: Pharmacokineatic Aspects of Measurement of Glomerular Filtration Rate in the Dog: A Review. JVIM 1998Lefebvre HP: Renal Function testing In: Nephrology and Urology of Small Animals
Ideal substance to measure GFRFreely filtered in glomerulumNot reabsorbed in tubulusNot secreted in tubulusNot protein boundNon‐toxicDoes not alter GFREasily measured in plasma and urine
INULIN (fructose polymere)
ClearanceCalculation from plasma concentration versus time
Clearance (Clplasma)Calculation from plama and urine data
Clearance (Clrenal)
If substance is excreted solely via kidneyClplasma = Clrenal
Without tubular secretion or reabsorptionClplasma = GFR (e.g. Inulin – Clearance)
Two types of ClearanceEndogenous Clearance
Renal ‐ Clearance
Exogenous ClearancePlasma ‐ Clearance
D = dose of marker; AUC= area under plasma concentration versus time curve

9
Glomerular filtration rate (GFR)Used substances
Renal Inulin clearance (Gold Standard)Endogenous creatinine clearanceExogenous creatinine clearancePlasma Inulin clearencePlasma Iohexol clearanceRadioactive isotopes (± Scintigraphy)
Single injection without collection of urine possible
Renal inulin clearenceGold standardInject inulin i.v. (bolus or constant rate infusion)Collect urine over 24 hours (metabolic cage)Measure inulin in plasma and urineCalculate GFR based on formula
Very cumbersome, rarely performed (only research)




![Geology · Geology Forthescientificjournal,seeGeology(journal). Geology(fromtheAncientGreekγῆ,gē,i.e.“earth”and-λoγία,-logia,i.e.“studyof,discourse”[1][2 ...](https://static.fdocument.org/doc/165x107/5f512a8dc36d4d05a271efd1/geology-geology-forthescientiicjournalseegeologyjournal-geologyfromtheancientgreekgieaoeearthaand-o-logiaieaoestudyofdiscoursea12.jpg)