![arXiv:1704.03747v2 [cond-mat.mes-hall] 30 Jun 2017 · dre−iq·r|ζ(r)|2 with ζ(r) being the one-electron atomicwavefunction, we takethe full angulardependence of the wave function](https://static.fdocument.org/doc/165x107/5be3b14d09d3f233038c1e36/arxiv170403747v2-cond-matmes-hall-30-jun-2017-dreiqrr2-with.jpg)
MALDI MS profiling of post-DRE urine samples highlights the potential of β-microseminoprotein as a...
9
Click here to load reader
Transcript of MALDI MS profiling of post-DRE urine samples highlights the potential of β-microseminoprotein as a...

MALDIMSProf|lingof Post-DREUrine SamplesHighlightsthe Potentialofb-Microseminoprotein as aMarker for
ProstaticDiseases
Brian Flatley,1,2 Karen G. Wilmott,2 Peter Malone,2 and Rainer Cramer1*1Departmentof Chemistry,Universityof Reading,Reading,UK
2Urology ResearchDepartment, Royal BerkshireHospital, Reading,UK
BACKGROUND. To use spectra acquired by matrix-assisted laser desorption/ionization(MALDI) mass spectrometry (MS) from pre- and post-digital rectal examination (DRE) urinesamples to search for discriminating peaks that can adequately distinguish between benignand malignant prostate conditions, and identify the peaks’ underlying biomolecules.METHODS. Twenty-five participants with prostate cancer (PCa) and 27 participants with avariety of benign prostatic conditions as confirmed by a 10-core tissue biopsy were included.Pre- and post-DRE urine samples were prepared for MALDI MS profiling using an automatedclean-up procedure. Following mass spectra collection and processing, peak mass andintensity were extracted and subjected to statistical analysis to identify peaks capable ofdistinguishing between benign and cancer. Logistic regression was used to combine markersto create a sensitive and specific test.RESULTS. A peak at m/z 10,760 was identified as b-microseminoprotein (b-MSMB) andfound to be statistically lower in urine from PCa participants using the peak’s average areas.By combining serum prostate-specific antigen (PSA) levels with MALDI MS-measuredb-MSMB levels, optimum threshold values obtained from Receiver Operator characteristicscurves gave an increased sensitivity of 96% at a specificity of 26%.CONCLUSIONS. These results demonstrate that with a simple sample clean-up followed byMALDI MS profiling, significant differences of MSMB abundance were found in post-DREurine samples. In combination with PSA serum levels, obtained from a classic clinicalassay led to high classification accuracy for PCa in the studied sample set. Our resultsneed to be validated in a larger multicenter prospective randomized clinical trial. Prostate74:103–111, 2014. # 2013 Wiley Periodicals, Inc.
KEY WORDS: biomarkers; urine; MALDI MS; prostatic diseases; b-microseminoprotein
INTRODUCTION
Prostate cancer (PCa) is the second most commoncancer in men and one of the leading causes of deathworldwide [1]. The blood level of prostate-specificantigen (PSA) is often elevated in men with PCa andthe use of the PSA test in conjunction with a digitalrectal examination (DRE) has become a clinicalstandard as part of various approaches for PCadetection [2]. The main drawback of PSA is its lack ofsensitivity to detect PCa patients with low levels ofPSA (early diagnosis) and lack of specificity to ade-quately distinguish between PCa and nonmalignantdisease forms such as benign prostate hyperplasia
(BPH) when the level of PSA is high. Numerousapproaches and methodologies have been applied in
Abbreviations: MALDI, matrix-assisted laser desorption/ionization;MS, mass spectrometry; ISD, in-source decay; PCa, prostate cancer;BPH, benign prostate hyperplasia; DRE, digital rectal examination;PSA, prostate-specific antigen; GCP, good clinical practice; MSMB,b-microseminoprotein.�Correspondence to: Prof. Rainer Cramer, Department of Chemistry,University of Reading, Whiteknights, Reading RG6 6AD, UK.E-mail: [email protected] 2 July 2013; Accepted 9 September 2013DOI 10.1002/pros.22736Published online 30 September 2013 in Wiley Online Library(wileyonlinelibrary.com).
The Prostate 74:103^111 (2014)
� 2013 Wiley Periodicals, Inc.

order to find a more suitable diagnostic test that wouldreduce the number of men with benign conditionsundergoing a prostate biopsy for confirmation ofmalignancy [3,4].
Matrix-assisted laser desorption/ionization (MALDI)[5] is a soft ionization method of mass spectrometry(MS) which is well suited for the analysis of largebiomolecules such as proteins. In this report, wepresent the results of an initial clinical study usingC18 ZipTip® pipette tips as part of a sample clean-upstrategy coupled with MALDI MS for the analysis ofurine, before and after DRE, from patients with avariety of benign prostate conditions as well asthose with confirmed PCa. The resulting differentialprotein expression is examined for possible use as anew diagnostic marker for PCa or other prostaticdiseases.
MATERIALSANDMETHODS
SampleCollection and Storage
Samples were obtained from men attending theUrology Procedures Clinic at the Royal BerkshireHospital for a prostate biopsy between May 2010 andJune 2011. These men present at the clinic with an agespecific raised PSA level and/or an abnormal DRE. Allspecimens were procured following approval from theBerkshire Research Ethics committee (10/H0505/18).Full written consent was granted by each participantprior to samples been taken by a good clinical practice(GCP)-trained research nurse. Details of the initialprocessing and storage can be found in the Supple-mentary Information.
MetadataAcquisition andHandling
Table I provides some of the study participants’details with more information given in the Supplemen-tary Table SI. Details of the PSA and creatinineanalysis methods can also be found in the Supplemen-tary Information. The disease status of each participantwas derived from a pathological examination of their10-core prostate tissue biopsy with a Gleason scoreassignment. Gleason scores were calculated by addingthe score of the most common grade (primary gradepattern) and the second most common grade (second-ary grade pattern) of the cancer cells, where more thantwo grades were observed the primary grade wasadded to the worst observable grade to arrive at theGleason score. Grades were assigned using the 2005(amended in 2009) International Society of UrologicalPathology (ISUP) Consensus Conference on GleasonGrading of Prostatic Carcinoma [6,7].
High-Throughput (HTP)MALDIMSProf|ling
Prior to MALDI MS analysis, all samples werepurified using C18 reverse phase micropipette tips(ZipTip®; Millipore, MA) on a fully automated roboticsystem (CyBi Robot; CyBio, Jena, Germany) similar toa previously described method [8] and as detailed inFigure 1. Details of the data acquisition and in-sourcedecay (ISD) analysis can be found along with sequencesearch parameters in the Supplementary Information.
Prof|ling of Creatinine-Normalized Samples
Following the measurement of the creatinine levelin each urine specimen, the urine samples were
TABLEI. Summaryof theMetadataAssociatedWith the Study Participants
Noncancer (n¼ 27) Cancer (n¼ 25)
Age (years) Minimum 53 Age (years) Minimum 55Median 66 Median 69Maximum 83 Maximum 90
Creatinine (mg/dl) Minimum 10.02 Creatinine (mg/dl) Minimum 16.57Median 39.60 Median 51.69Maximum 190.60 Maximum 183.30
PSA (ng/ml) Minimum 4.00 PSA (ng/ml) Minimum 0.65Median 6.60 Median 9.03Maximum 54.03 Maximum 127.90
Condition No. of patients Score No. of patients
Nonmalignant conditionsa BPH 11 Gleason score 6 3Prostatitis 20 7 16Atrophy 12 8 1
9 5
aMost patients had a combination of conditions in the nonmalignant group.
104 Flatley et al.
The Prostate

normalized with a 0.15-M NaCl solution to the lowestcreatinine level of the sample population, with a totalvolume of 50ml in each well. The maximum dilutionwas 1:48 for the sample with the highest level ofcreatinine. Sample positions across two 96-well plateswere randomized, mixing both pre- and post-DREsamples across the two plates, and the pathologyresults were unknown to the analyst at the time ofanalysis.
Prof|lingofNoncreatinine-Normalized Samples
Twelve samples of the above set were taken (6 PCa,6 benign) for another round of MALDI MS profiling,without normalization of the creatinine level. Thesamples were selected to match in both creatinine and
PSA levels as closely as possible. The samples markedwith an asterisk after the patient ID in the Supplemen-tary Table are the ones that were selected for profilingwith noncreatinine normalization. This experimentwas not blinded because the aim was to have similarcreatinine and PSA levels in both groups and so thedisease status was needed to select the relevantsamples. However, all plate positions were random-ized to remove potential plate or other sample orderbias.
Statistical Analysis
The raw spectra were processed, and peaks wereselected with a signal/noise cut-off set at 5, usingClinProTools (Version 2.1; Bruker Daltonics, Bremen,
Fig. 1. Schematic of the automatedworkflow for HTPMALDIMSprofiling of body fluids.Using a 5-ml aliquot per sample, the processingincluded the acidificationof the samplewith 2%TFA,bindingof thepeptides and smallproteins on themicropipetteresin, awashing stepwith0.1% TFA and finally the elution of the sample using a MALDI-compatible solvent (50:50; v/v; ACN/0.2%TFA).This eluent was mixed1:9with a 0.5-mg/ml solution of a-cyano-4-hydroxycinnamic acid (CHCA), and a 0.8-ml aliquot was spotted onto a MALDI MS anchorchipplate.
MALDIMSProfiling Reveals MSMB as PCaMarker 105
The Prostate

Germany). For each sample the average peak area atm/z 10,760 was obtained and used for statisticalanalysis. A Student’s t-test was used to examine thedifference in age between the PCa and benign group.Mann–Whitney U tests were used for pairwisecomparisons of PSA and b-microseminoprotein(MSMB) levels between PCa and benign groups.Receiver operator characteristics (ROC) analysis andboxplot visualization were done using RStudiopackages pROC [9]. The glmc package in R (http://www.stat.washington.edu/handcock/combining/software/glmc.html; accessed on December 10, 2012)was used to model the probability of correctly predict-ing the dichotomous outcome of either cancer ornoncancer, using the variables of PSA level (ng/ml)and MSMB peak intensity for each participant (seeSupplementary Table SI). For all experiments a P-value�0.05 was considered significant. All statistical analy-ses were performed using the R statistical package(version 2.6.0; R Foundation for Statistical Computing).
RESULTS
MS spectra were obtained from 27 patients diag-nosed with benign conditions such as BPH andprostatitis (chronic inflammation) and 25 patients withPCa ranging in Gleason score from 6 to 9 (see Table I).There was no significant difference between the ages
of the two groups with 68 years as the median age(range: 53–90 years).
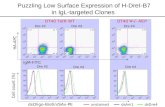
HTP MALDI MS profiling of creatinine-normalizedurine samples found 64 common peaks using the dataprocessing software ClinProTools 2.1. Figure 2 illus-trates the average spectra from pre- (Fig. 2a) and post-DRE (Fig. 2b) urine samples as obtained from ClinPro-Tools analysis. The peak at m/z 10,760 and itsassumed doubly charged version at m/z 5,380 aredetectable in substantial amounts only in the post-DRE urine samples. The stark increase in peak intensi-ty in the urine following the application of a DRE isthought to be a result of the physical massaging of theprostate gland causing stimulation and movement ofprostate fluids and detached epithelial cells into theurethra to be mixed with the urine and voided. Afterinitial processing (baseline subtraction and smooth-ing), spectra that failed to meet the quality criteria, forexample, null spectra and spectra with low shotnumbers, were removed. The samples were thendivided into their respective group, that is, cancer andbenign, depending on their disease status as deter-mined from the tissue biopsy pathology report.
Peak intensity values (based on peak area) wereexported from ClinProTools to Microsoft Excel®,where the average peak intensity from each samplewas calculated and used in all subsequent calculationsin RStudio. Using the Mann–Whitney U test it was
Fig. 2. MALDIMS average profiles frompre- (a) andpost-DRE (b) urine samples.The peak atm/z10,760 and its assumed doubly chargedversion atm/z 5,380 aremarkedwith dotted lines. Signal intensity levels of this peak were found to be significantly lower in cancer patients’MSprofiles.
106 Flatley et al.
The Prostate

found that the peak intensity at m/z 10,760 wassignificantly higher in the benign group than thecancer group.
To ensure none of the peaks identified were artifactsfrom the creatinine normalization step, that is, due tothe addition of 0.15M NaCl, HTP MALDI MS profilinganalysis was repeated on a smaller cohort with nonormalization step (patients marked with an asteriskin the Supplementary Table SI). No additional peakswere observed in the NaCl-normalized spectra overthe non-normalized spectra and the peak intensity atm/z 10,760 was found to be also significantly higherin the MS spectra of the non-normalized benignsamples when compared to the MS spectra from thenon-normalized urine of the cancer patients.
To identify the polypeptide at m/z 10,760, a smallvolume of a ZipTip-treated sample that previouslyshowed an intense signal at this m/z value wasanalyzed using MALDI-ISD MS (see SupplementaryInformation for details). Figure 3 shows the resultingISD spectrum with an amino acid sequence tag asproposed by the software BioTools. Part of thissequence tag (EWQTDN) was searched against theUniProtKB/Swiss-Prot database using BLASTP [10]and the best match for this sequence was found to bein MSMB (P08118). Next, MSMB without its signalpeptide was fragmented in silico, and its theoreticalfragment ion masses were compared with the experi-mentally obtained ones. This comparison clearlyshowed that there was a good match to the c31–c36ion series (see Fig. 3), which conforms with the typical
ISD fragmentation behavior, mainly leading to c- or z-type ions.
To compare the usefulness of MSMB and PSA asdiagnostic markers for PCa (in our cohort where allbut two participants had an age-specific raised PSAlevel), statistical tests were performed using serumPSA levels and the average peak intensity of the singlycharged MSMB peak from the MALDI MS profilingresults. Figure 4 shows boxplots of the decadiclogarithm of serum PSA levels and MSMB MALDI MSsignal intensity levels, plotting the analyte distributionin benign and cancer patients. Below both boxplots,constructed ROC curves are shown. A ROC curveplots the specificity (x-axis) and sensitivity (y-axis) ofeach analyte for all threshold levels. The area underthe curve (AUC) for both ROC curves is also providedunder each respective curve.
MSMB levels were found to be significantly differ-ent between the benign and cancer group using thenonparametric Mann–Whitney U test (P¼ 0.01), unlikethe PSA levels (P¼ 0.07). Examining the AUC resultsfrom the ROC curves, the serum PSA data give 65%AUC, whereas the MSMB data have an AUC of 70%.Furthermore, the ROC curve for PSA shows a relative-ly abrupt decline in sensitivity at high specificity forPSA, that is, below 10% sensitivity at 95–100% specific-ity, while for MSMB the sensitivity is still 28% at aspecificity of 100%.
In addition, a logistic regression model was usedto combine the serum PSA levels and the MALDI-measured MSMB levels to construct a model that is
Fig. 3. ISD-MALDImass spectrumrecorded from a post-DREurine samplewith1,5-DANasmatrix.The BioTools-derived amino acid se-quence tagandthe ISDfragmentionmasseswith theirerrors are shownabove thepeak.
MALDIMSProfiling Reveals MSMB as PCaMarker 107
The Prostate

more sensitive and specific than using PSA levelsalone in a population of men selected originally oneither or both a raised serum PSA and DRE examina-tion. A comparison of the tests using an MSMB peakintensity cut-off level obtained from the MALDI MSprofiling data and the logistic regression model (com-bining PSA and MSMB levels) found that the optimumfor accuracy, that is, sensitivity and specificity, wasfound when PSA and MSMB were combined. A testspecificity of 26% (CI 11–44%) was calculated for boththe MSMB test and the predictive values from thelogistic regression model. However, the sensitivityincreased by 4% to 96% (CI 88–100%) using the logisticregression model’s predictive values. A comparisonusing a single PSA cut-off value against the logisticregression model was not carried out as the patientsinvolved in this study were attending the prostatebiopsy clinic based on age-specific PSA cut-off values.
DISCUSSION
The ability of MALDI MS to analyze a large numberof samples in a short period of time has been usedpreviously to discover possible biomolecular signa-tures that can distinguish healthy from diseasedsamples [11–13]. In this study, HTP MALDI MSanalysis allowed the evaluation of pre- and post-DRE
urine samples in triplicate without high costs forconsumables or laboratory analyst/analysis time.Many HTP MS profiling techniques such as surface-enhanced laser desorption/ionization (SELDI) MSgenerate a pattern of peaks that can be used inalgorithms but a lot of these studies fall short ofidentifying the proteins that contribute to the differen-tial peak profile and explaining their biological originand function [14]. In the present study, MALDI-ISDMS allowed the identification of the main differentiat-ing protein as MSMB, which is one of the mostabundant proteins found in human ejaculate [15].
It was found that the level of MSMB drops in thecancer group, when using the average MS peak area.This decrease in MSMB levels in cancer patients isillustrated in the boxplot of MSMB levels of Figure 4and is the inverse of PSA levels in PCa patients,which is expected to rise with malignancy anddegradation of the basal cell membrane. In the case ofthe PSA levels of the patients in this study, theaverage PSA level rose as expected (Table I). Howev-er, the difference between the benign and cancergroup was not significant (P< 0.05) unlike the differ-ence in MSMB levels. The suitability of PSA as a PCadiagnostic marker has been the topic of a surfeit ofreviews, most recently by Prensner et al. [16] andRamirez et al. [17].
Fig. 4. Boxplots of the decadic logarithm of MSMB and PSA levels for benign and cancer patients with the constructed ROC curves forbothPSAandMSMBbeloweachboxplot.
108 Flatley et al.
The Prostate

It is surprising that changes in the expressionallevels of MSMB are measurable from a urine samplecontaining expressed proteins from the prostate that islargely made up of benign cells. Interestingly, it hasbeen reasoned that the decrease in MSMB levels isassociated with the expression of a small nucleotidepolymorphism (rs10993994) in the 50-UTR regioncoding for MSMB [18]. In a study by Whitakeret al. [19], it was shown that the staining for MSMB inprostate tissue that was homozygous for the risk allelewas weaker when compared to tissue from patientsthat were homozygous for the normal nucleotidesequence. There are a number of genome-wide associ-ation studies that implicated this risk allele in thelowered expression of MSMB [20,21]. Figure 5 outlinesthe protein interaction network of MSMB.
This is not the first time that a biomarker candidateof this approximate molecular weight has been identi-fied as down-regulated in post-DRE urine using MS.
In 2009, Okamoto et al. [14] published results fromSELDI experiments. They found through repeatedanalysis of post-DRE urine samples that a peak at m/z10,788 and also a doubly charged version of this peakwere significantly down-regulated in PCa patients. Inthe conclusion of their report, they believed that thepeak at m/z 10,788 had potential as an early diagnos-tic marker but unlike the study presented here noidentification of the peak was undertaken. MALDI is aless-expensive and easier method of protein profilingthan SELDI but the results from the SELDI studycorroborates the findings of this small pilot study andstrengthens the argument to progress with incorporat-ing MSMB into a larger panel of biomarkers for PCa.
In general, Teni et al. [22] were one of the first groupsto investigate the use of MSMB as a diagnostic markerfor PCa. A review published in 2009 summarizes theslightly sporadic research of MSMB over the past 20years [23]. MSMB has been shown to inhibit the activity
Fig. 5. Protein interaction networkof b-microseminoprotein (MSMB). Although the function of MSMB is not fully understood, one of itsmainroles is theinhibitionof follicle-stimulatinghormone [27].Aproposedbiologicalpathway forMSMBinbothbenignand tumor tissuewasoutlinedbyWhitakeret al. [23]. In normalorbenignconditionsMSMBbinds to cysteine-rich secretoryprotein 3 (CRISP-3),mainly in seminalplasma, and to cysteine-rich secretoryprotein 9 (CRISP-9, also known aspeptidase inhibitor16) or lamininreceptors (37kDa) at the cell sur-face or in serum.The peptide sequences responsible for MSMB and CRISP-9 binding in serumhave been under investigation as possible drugtargets [28]. In either interaction the resulting binding leads to apoptosis. In tumor tissue, the histone-lysine N-methyltransferase (EZH2)enzymesilences theproductionofMSMBthroughhistoneandpromoterhypermethylation [29].Loss ofMSMBleads to adecreaseinapoptosisandanincreaseinunregulatedcellgrowth.ThisproteininteractionnetworkwascreatedusingString9.0 [30].
MALDIMSProfiling Reveals MSMB as PCaMarker 109
The Prostate

of MMP-9 and CD44 [24], both of which facilitate cancercell adhesion to the extracellular matrix of the tumor andseveral stages in the metastatic pathway. Very recently areduction in MSMB expression was found in ovariancancer and it was concluded that the expression ofMSMB fits well with a tumor-suppressor function inovarian carcinogenesis [25]. All this indicates the strongcorrelation between a decrease in the levels of MSMBand the progression of PCa, and thus adding weight tothe argument for its use as a PCa biomarker.
It is clear that the specificity and sensitivity of eventhe combined PSA/MSMB model is insufficient forpopulation screening. However, taking into accountthat 96% of the participants were having a prostatebiopsy as a result of a raised PSA level (the other 4%has a PSA level below their age-specific threshold),we would have reduced the number of unnecessarybiopsies in the benign group by seven men with ourcombined logistic regression model. The work donehere demonstrates the potential of MSMB for inclusioninto perhaps a larger biomarker panel includingPCA3 [26] and PSA, whilst also justifies the proposalto expand this research to a multi center study, andinclude patients that have not previously had a PSAtest or DRE examination.
CONCLUSIONS
In conclusion, there is growing evidence thatMSMB is not only implicated in the pathogenesis ofPCa but can also be used as a potential biomarker inits diagnosis. In this study, utilizing a simple C18ZipTip® sample clean-up followed by MALDI MSprofiling, we were able to show significant differencesof MSMB abundance in post-DRE urine samplesbetween patients with PCa and benign prostate con-ditions, leading to improved patient classificationwhen compared to the classical PSA method. Themainly automated workflow could be extended byusing a barcode system linked to a laboratory informa-tion management system (LIMS) that could generatesample lists and reports without the need for manualintervention. We therefore propose that monitoringMSMB levels in post-DRE urine using HTP MALDIMS could be a viable approach for improved PCadiagnosis, in a similar way that PCA3 is measuredpost-DRE.
REFERENCES
1. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM.Estimates of worldwide burden of cancer in 2008: GLOBOCAN2008. Int J Cancer 2010;127(12):2893–2917.
2. Catalona WJ, Richie JP, Ahmann FR, Hudson MA, ScardinoPT, Flanigan RC, deKernion JB, Ratliff TL, Kavoussi LR,
Dalkin BL, Waters WB, MacFarlane MT, Southwick PC.Comparison of digital rectal examination and serum prostatespecific antigen in the early detection of prostate cancer:Results of a multicenter clinical trial of 6,630 men. J Urol1994;151(5):1283–1290.
3. Goessl C, Krause H, Muller M, Heicappell R, Schrader M,Sachsinger J, Miller K. Fluorescent methylation-specific polymer-ase chain reaction for DNA-based detection of prostate cancer inbodily fluids. Cancer Res 2000;60(21):5941–5945.
4. Hessels D, Klein Gunnewiek JM, van Oort I, Karthaus HF, vanLeenders GJ, van Balken B, Kiemeney LA, Witjes JA, SchalkenJA. DD3(PCA3)-based molecular urine analysis for the diagnosisof prostate cancer. Eur Urol 2003;44(1):8–15.
5. Karas M, Hillenkamp F. Laser desorption ionization of proteinswith molecular masses exceeding 10,000 daltons. Anal Chem1988;60(20):2299–2301.
6. Epstein JI, Allsbrook WC, Amin MB, Egevad LL, Committee IG.The 2005 International Society of Urological Pathology (ISUP)Consensus Conference on Gleason grading of prostatic carcino-ma. Am J Surg Pathol 2005;29(9):1228–1242.
7. Trock BJ, Guo CC, Gonzalgo ML, Magheli A, Loeb S, Epstein JI.Tertiary Gleason patterns and biochemical recurrence afterprostatectomy: Proposal for a modified Gleason scoring system.J Urol 2009;182(4):1364–1370.
8. Tiss A, Smith C, Camuzeaux S, Kabir M, Gayther S, Menon U,Waterfield M, Timms J, Jacobs I, Cramer R. Serum peptideprofiling using MALDI mass spectrometry: Avoiding the pitfallsof coated magnetic beads using well-established ZipTip technol-ogy. Proteomics 2007;7:77–89.
9. Robin X, Turck N, Hainard A, Tiberti N, Lisacek F, Sanchez JC,Muller M. pROC: An open-source package for R and Sþ toanalyze and compare ROC curves. BMC Bioinformatics 2011;12:77.
10. Altschul SF, Madden TL, Schaffer AA, Zhang J, Zhang Z, MillerW, Lipman DJ. Gapped BLAST and PSI-BLAST: A new genera-tion of protein database search programs. Nucleic Acids Res1997;25(17):3389–3402.
11. M’Koma AE, Blum DL, Norris JL, Koyama T, Billheimer D,Motley S, Ghiassi M, Ferdowsi N, Bhowmick I, Chang SS,Fowke JH, Caprioli RM, Bhowmick NA. Detection ofpre-neoplastic and neoplastic prostate disease by MALDIprofiling of urine. Biochem Biophys Res Commun 2007;353(3):829–834.
12. Ornstein DK, Rayford W, Fusaro VA, Conrads TP, Ross SJ, HittBA, Wiggins WW, Veenstra TD, Liotta LA, Petricoin EF III.Serum proteomic profiling can discriminate prostate cancer frombenign prostates in men with total prostate specific antigenlevels between 2.5 and 15.0 ng/ml. J Urol 2004;172(4 Pt 1):1302–1305.
13. Wright ME, Han DK, Aebersold R. Mass spectrometry-basedexpression profiling of clinical prostate cancer. Mol Cell Proteo-mics 2005;4(4):545–554.
14. Okamoto A, Yamamoto H, Imai A, Hatakeyama S, Iwabuchi I,Yoneyama T, Hashimoto Y, Koie T, Kamimura N, Mori K,Yamaya K, Ohyama C. Protein profiling of post-prostaticmassage urine specimens by surface-enhanced laser desorption/ionization time-of-flight mass spectrometry to discriminatebetween prostate cancer and benign lesions. Oncol Rep 2009;21(1):73–79.
15. Lilja H, Abrahamsson PA. Three predominant proteins secretedby the human prostate gland. Prostate 1988;12(1):29–38.
110 Flatley et al.
The Prostate

16. Prensner JR, Rubin MA, Wei JT, Chinnaiyan AM. Beyond PSA:The next generation of prostate cancer biomarkers. Sci TranslMed 2012;4(127):127rv3.
17. Ramirez ML, Nelson EC, Evans CP. Beyond prostate-specificantigen: Alternate serum markers. Prostate Cancer Prostatic Dis2008;11(3):216–229.
18. Lou H, Yeager M, Li H, Bosquet JG, Hayes RB, Orr N, Yu K,Hutchinson A, Jacobs KB, Kraft P, Wacholder S, Chatterjee N,Feigelson HS, Thun MJ, Diver WR, Albanes D, Virtamo J,Weinstein S, Ma J, Gaziano JM, Stampfer M, Schumacher FR,Giovannucci E, Cancel-Tassin G, Cussenot O, Valeri A, AndrioleGL, Crawford ED, Anderson SK, Tucker M, Hoover RN,Fraumeni JF, Thomas G, Hunter DJ, Dean M, Chanock SJ. Finemapping and functional analysis of a common variant in MSMBon chromosome 10q11.2 associated with prostate cancer suscep-tibility. Proc Natl Acad Sci USA 2009;106(19):7933–7938.
19. Whitaker HC, Kote-Jarai Z, Ross-Adams H, Warren AY, Burge J,George A, Bancroft E, Jhavar S, Leongamornlert D, Tymrakie-wicz M, Saunders E, Page E, Mitra A, Mitchell G, Lindeman GJ,Evans DG, Blanco I, Mercer C, Rubinstein WS, Clowes V,Douglas F, Hodgson S, Walker L, Donaldson A, Izatt L, DorkinsH, Male A, Tucker K, Stapleton A, Lam J, Kirk J, Lilja H, EastonD, Cooper C, Eeles R, Neal DE, Committee ISS, Collaborators IS,Collaborators UG. The rs10993994 risk allele for prostate cancerresults in clinically relevant changes in microseminoprotein-betaexpression in tissue and urine. PLoS ONE 2010;5(10):e13363.
20. Eeles RA, Kote-Jarai Z, Giles GG, Olama AA, Guy M, JugurnauthSK, Mulholland S, Leongamornlert DA, Edwards SM, MorrisonJ, Field HI, Southey MC, Severi G, Donovan JL, Hamdy FC,Dearnaley DP, Muir KR, Smith C, Bagnato M, Ardern-Jones AT,Hall AL, O’Brien LT, Gehr-Swain BN, Wilkinson RA, Cox A,Lewis S, Brown PM, Jhavar SG, Tymrakiewicz M, LophatananonA, Bryant SL, Horwich A, Huddart RA, Khoo VS, Parker CC,Woodhouse CJ, Thompson A, Christmas T, Ogden C, Fisher C,Jamieson C, Cooper CS, English DR, Hopper JL, Neal DE, EastonDF. Multiple newly identified loci associated with prostate cancersusceptibility. Nat Genet 2008;40(3):316–321.
21. Thomas G, Jacobs KB, Yeager M, Kraft P, Wacholder S, Orr N, YuK, Chatterjee N, Welch R, Hutchinson A, Crenshaw A, Cancel-Tassin G, Staats BJ, Wang Z, Gonzalez-Bosquet J, Fang J, Deng X,Berndt SI, Calle EE, Feigelson HS, Thun MJ, Rodriguez C,Albanes D, Virtamo J, Weinstein S, Schumacher FR, GiovannucciE, Willett WC, Cussenot O, Valeri A, Andriole GL, Crawford ED,Tucker M, Gerhard DS, Fraumeni JF Jr, Hoover R, Hayes RB,Hunter DJ, Chanock SJ. Multiple loci identified in a genome-wide association study of prostate cancer. Nat Genet 2008;40(3):310–315.
22. Teni TR, Sheth AR, Kamath MR, Sheth NA. Serum and urinaryprostatic inhibin-like peptide in benign prostatic hyperplasiaand carcinoma of prostate. Cancer Lett 1988;43(1–2):9–14.
23. Whitaker HC, Warren AY, Eeles R, Kote-Jarai Z, Neal DE. Thepotential value of microseminoprotein-beta as a prostate cancerbiomarker and therapeutic target. Prostate 2009;70(3):333–340.
24. Annabi B, Bouzeghrane M, Currie JC, Hawkins R, Dulude H,Daigneault L, Ruiz M, Wisniewski J, Garde S, Rabbani SA,Panchal C, Wu JZJ, Beliveau R. A PSP94-derived peptidePCK3145 inhibits MMP-9 secretion and triggers CD44 cellsurface shedding: Implication in tumor metastasis. Clin ExpMetastasis 2005;22(5):429–439.
25. Henriksen R, Lundwall A, Udby L, Fernlund P. The expressionof beta-microseminoprotein but not CRISP3 is reduced inovarian. Anticancer Res 2012;32(9):3993–3999.
26. Roobol MJ, Schröder FH, van Leeuwen P, Wolters T, van denBergh RC, van Leenders GJ, Hessels D. Performance of theprostate cancer antigen 3 (PCA3) gene and prostate-specificantigen in prescreened men: Exploring the value of PCA3 for afirst-line diagnostic test. Eur Urol 2010;58(4):475–481.
27. Yeager M, Deng Z, Boland J, Matthews C, Bacior J, Lonsberry V,Hutchinson A, Burdett LA, Qi L, Jacobs KB, Gonzalez-Bosquet J,Berndt SI, Hayes RB, Hoover RN, Thomas G, Hunter DJ, DeanM, Chanock SJ. Comprehensive resequence analysis of a 97 kbregion of chromosome 10q11.2 containing the MSMB geneassociated with prostate cancer. Hum Genet 2009;126(6):743–750.
28. Hawkins RE, Daigneault L, Cowan R, Griffiths R, Panchal C,Armstrong A, Fenemore J, Irvine A, Sereda K, Dulude H. Safetyand tolerability of PCK3145, a synthetic peptide derived fromprostate secretory protein 94 (PSP94) in metastatic hormone-refractory prostate cancer. Clin Prostate Cancer 2005;4(2):91–99.
29. Beke L, Nuytten M, Van Eynde A, Beullens M, Bollen M. Thegene encoding the prostatic tumor suppressor PSP94 is a targetfor repression by the polycomb group protein EZH2. Oncogene2007;26(31):4590–4595.
30. Snel B, Lehmann G, Bork P, Huynen MA. STRING: Aweb-serverto retrieve and display the repeatedly occurring. Nucleic AcidsRes 2000;28(18):3442–3444.
Supporting Information
Additional supporting information may be found inthe online version of this article at the publisher ’s web-site.
MALDIMSProfiling Reveals MSMB as PCaMarker 111
The Prostate