Long-term follow-up of bintrafusp alfa, a bifunctional ...
1
Abstract No. 1418. Presented at the ESMO Virtual Congress 2020, September 19-21, 2020 Long-term follow-up of bintrafusp alfa, a bifunctional fusion protein targeting TGF-β and PD-L1, in patients with pretreated biliary tract cancer C. Yoo 1 , D.-Y. Oh 2 , H. J. Choi 3 , M. Kudo 4 , M. Ueno 5 , S. Kondo 6 , L.-T. Chen 7 , M. Osada 8 , C. Helwig 9 , I. Dussault 10 , M. Ikeda 11 1 Asan Medical Center, University of Ulsan College of Medicine, Seoul, Republic of Korea; 2 Seoul National University Hospital, Cancer Research Institute, Seoul National University College of Medicine, Seoul, Republic of Korea; 3 Department of Medicine, Oncology, Yonsei University College of Medicine, Seoul, Republic of Korea; 4 Kindai University Faculty of Medicine, Osaka-Sayama, Japan; 5 Department of Gastroenterology, Hepatobiliary and Pancreatic Medical Oncology Division, Kanagawa Cancer Center, Yokohama, Japan; 6 National Cancer Center Hospital, Tokyo, Japan; 7 National Cheng Kung University Hospital, National Institute of Cancer Research, Tainan, Taiwan; 8 Merck Biopharma, Tokyo, Japan, an affiliate of Merck KGaA, Darmstadt, Germany; 9 Merck KGaA, Darmstadt, Germany; 10 EMD Serono Research & Development Institute, Inc., Billerica, MA, USA; a business of Merck KGaA, Darmstadt, Germany; 11 National Cancer Center Hospital East, Kashiwa, Japan Poster No. 73P BACKGROUND Biliary tract cancer (BTC) • BTC is a rare, heterogenous, and lethal group of cancers with limited treatment options • Gemcitabine plus cisplatin is the standard of care for first-line (1L) BTC treatment; however, no global standard of care has been established for second-line (2L) treatment of BTC because the efficacy of 2L chemotherapy in advanced BTC is low: – A recent meta-analysis of 2L chemotherapy in BTC found a median overall survival (OS) of 7.2 months and objective response rate (ORR) of 7.7% 1 – The ABC-06 study showed clinical benefit of treatment with mFOLFOX (oxaliplatin, leucovorin, and 5-fluorouracil) vs active symptom control for locally advanced/metastatic 2L BTC; however, the median progression- free survival (PFS) of 4.0 months, 12-month OS rate of 25.9%, and ORR of 5% indicate an unmet need 2 • Recent studies for the treatment of multiple cancers with immune checkpoint inhibitors (ICIs) have shown promising results, although the efficacy of ICIs has yet to be demonstrated in BTC: – In a phase 2 study of nivolumab in patients with pretreated advanced BTC, the ORR was 22% per the investigator (11% per independent review committee). 3 Furthermore, ORR with nivolumab monotherapy was 3.3% (1 partial response in 30 patients) in a phase 1 study in patients with unresectable/recurrent BTC refractory to or intolerant of gemcitabine 4 – In the phase 2 KEYNOTE-158 study of pembrolizumab monotherapy in patients with previously treated unresectable and/or metastatic BTC, the ORR was 5.8% (6 PRs in 104 patients) in the PD-L1–unselected population and 6.6% (4 PRs in 61 patients) in patients with PD-L1– positive tumors 5 Transforming growth factor β (TGF-β) • The TGF-β pathway can promote cancer progression and immune evasion in the tumor microenvironment via regulatory effects on immune cells, as well as by impacting processes such as angiogenesis, fibrosis, and epithelial-mesenchymal transition 6,7 • Preclinical studies have shown a link between aberrant TGF-β signaling and BTC pathogenesis – Genomic alterations in TGF-β signaling have been reported in 10% to 20% of the 3 major subtypes of BTC: intrahepatic cholangiocarcinoma (IHCC), extrahepatic cholangiocarcinoma (EHCC), and gallbladder cancer 8 – Data suggest a correlation between the expression of TGF-β1 in patients with BTC and lymph node metastasis, distant metastasis, and tumor recurrence 9 – TGF-β receptor inhibitors, such as galunisertib, can exert anticancer effects against human BTC cells 10 • Thus, inhibiting TGF-β activity in the tumor microenvironment while simultaneously blocking an additional immunosuppressive signaling mechanism, such as the PD-L1 pathway, may provide a novel treatment approach Bintrafusp alfa • Bintrafusp alfa is a first-in-class bifunctional fusion protein composed of the extracellular domain of the TGF-βRII receptor to function as a TGF-β “trap” fused to a human IgG1 mAb blocking PD-L1 (Figure 1) • The bifunctional nature of bintrafusp alfa might allow for colocalized, simultaneous inhibition of two nonredundant immunosuppressive pathways (TGF-β and PD-L1) within the tumor microenvironment, which may result in increased efficacy in locally advanced/metastatic BTC 11 • Overall safety/tolerability data from phase 1 studies of bintrafusp alfa and an exposure-safety analysis conducted on an integrated data set with >670 participants supported the selection of 1200 mg every 2 weeks (Q2W) as the monotherapy recommended phase 2 dose • Prior analysis of this phase 1 study (NCT02699515) expansion cohort found a manageable safety profile and an ORR of 20% per independent review committee (IRC) assessment and 23.3% as assessed by investigator in patients with pretreated BTC who received bintrafusp alfa 12 • The median duration of response (DOR) was 9.7 months as assessed by the investigator (not reached per IRC) and the median OS was 12.7 months 12 • Here, we present a 28-month update on the efficacy and safety follow-up in an expansion cohort of this phase 1 study of patients with BTC receiving bintrafusp alfa Figure 1. Proposed mechanism of action of bintrafusp alfa Fibroblast CAF Fibrosis and impaired drug access EMT (leading to metastasis and resistance to therapy [including checkpoint inhibition]) Tumor angiogenesis Tumor cells PD-L1 Bintrafusp alfa PD-1 T cell Suppression of immune response NK cell TAM Dendritic cell Cytotoxic T cell Tumor cells Mesenchymal-like tumor cell TGF-β “trap” moiety sequesters TGF-β to block downstream signaling Anti–PD-L1 mAb moiety blocks PD-L1 interactions with PD-1 TGF-β* CAF, cancer-associated fibroblast; NK, natural killer; TAM, tumor-associated macrophage. *Tumor cells are also a major source of TGF-β in the microenvironment. METHODS • NCT02699515 is an ongoing phase 1, open-label study of bintrafusp alfa with an expansion cohort of chemotherapy-experienced patients with BTC • Asian patients with BTC for whom 1L chemotherapy failed received bintrafusp alfa 1200 mg Q2W until confirmed disease progression, unacceptable toxicity, or withdrawal • The primary objective of this study was safety/tolerability – Key secondary objectives included investigator-assessed best overall response per RECIST 1.1, median OS, median DOR, and proportion of ongoing responses RESULTS Baseline patient and disease characteristics • Thirty patients were enrolled in this cohort; 13.3% (n=4) of patients had received ≥2 prior anticancer regimens – All patients had disease progression following 1L treatment and received no prior immunotherapy • This cohort consisted of patients with gallbladder carcinoma (40% [n=12]), intrahepatic cholangiocarcinoma (33.3% [n=10]), extrahepatic cholangiocarcinoma (23.3% [n=7]), and ampullary carcinoma (3.3% [n=1]) • This follow-up uses a database cutoff of October 24, 2019 (28 months from the last patient’s first dose), with a Kaplan-Meier estimate of follow-up time of 121.6 weeks Safety • Since the prior analysis, no additional deaths or safety signals were observed; 1 new grade ≥3 TRAE (grade 3 keratoacanthoma) was observed • At the August 24, 2018 data cutoff, 63.3% of patients experienced treatment-related adverse events (TRAEs) – Eleven patients (36.7%) experienced grade ≥3 TRAEs – Two patients experienced grade 4 events (increased amylase, aspartate aminotransferase, and lipase levels) • Three treatment-emergent deaths occurred – Septic shock (n=1) due to bacteremia of unknown etiology 249 days after the first dose and 14 days after the last dose – Interstitial lung disease (reported term, interstitial pneumonitis) in 2 patients Table 1. Investigator-assessed efficacy as of October 24, 2019 cutoff Outcome Efficacy ORR, % 23.3 DCR, % 36.7 Median DOR, months (95% CI) ≥6-month response, % (n) ≥12-month response, % (n) ≥18-month response, % (n) 18.0 (2.8-NE) 71.4 (5) 57.1 (4) 42.8 (3) Median PFS, months (95% CI) 12-month PFS, % (95% CI) 18-month PFS, % (95% CI) 24-month PFS, % (95% CI) 2.5 (1.3-4.0) 14.8 (4.7-30.3) 14.8 (4.7-30.3) 11.1 (2.8-25.7) Median OS, months (95% CI) 12-month OS, % (95% CI) 18-month OS, % (95% CI) 24-month OS, % (95% CI) 12.7 (6.7-15.8) 52.0 (32.8-68.2) 31.2 (15.7-48.1) 27.7 (13.1-44.5) NE, not estimable. • Since the initial analysis, the investigator-assessed ORR and DCR remained at 23.3% (20.0% per IRC) and 36.7% (40.0% per IRC), respectively ( Table 1 and Figure 2) • Responses were durable; 3 responses are ongoing of 7 responders (42.8%), with DORs of 18+, 23.5+, and 24+ months (Figure 5) • The median OS was 12.7 months, with a 24-month OS rate of 27.7% ( Figure 3 ) • The median PFS was 2.5 months, with a 24-month PFS rate of 11.1% (Figure 4) Figure 2. Change in sum of target lesion diameters per investigator 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 Months -80 -30 20 70 90 Change in sum of diameters, (%) First occurrence of new lesion Patients off treatment SD, PD or NE PR CR CR, complete response; SD, stable disease; PD, progressive disease; NE, not estimable. Patients with no postbaseline assessment (n=2) are not included in this graph. *Microsatellite instability-high patient. Figure 3. OS in the overall population No. at risk 30 26 26 26 21 21 17 17 15 11 12-month OS: 52.0% (95% CI, 32.8-68.2) 18-month OS: 31.2% (95% CI, 15.7-48.1) 24-month OS: 27.7% (95% CI, 13.1-44.5) 9 9 8 5 3 0 0 3 6 9 12 15 18 21 24 27 30 33 0 10 20 30 40 50 60 70 80 90 100 Months OS, % 6.7-15.8 95% CI 12.7 months Median 22 No. of events Figure 4. PFS for overall population No. at risk 30 9 7 5 4 4 4 4 3 2 2 0 0 3 6 9 12 15 18 21 24 27 30 33 0 10 20 30 40 50 60 70 80 90 100 PFS. % Months 1.3-4.0 95% CI 2.5 months Median 25 No. of events 12-month PFS: 14.8% (95% CI, 4.7-30.3) 18-month PFS: 14.8% (95% CI, 4.7-30.3) 24-month PFS: 11.1% (95% CI, 2.8-25.7) Figure 5. Time to and duration of response per investigator 0 10 20 30 Months Ongoing response Subsequent anticancer treatment End of treatment Death PD PR CR Median DOR: 18.0 months (95% CI 2.8-NE) Length of bar shows time to PD/death/last tumor assessment. Arrow indicates ongoing response (ie, no PD or death at cutoff date in patients with CR or PR). CONCLUSIONS • After 28 months of follow-up, bintrafusp alfa continues to demonstrate manageable safety with durable, long-lasting responses and long-term survival in this expansion cohort of Asian patients with pretreated BTC • As of the October 24, 2019 data cutoff, 8 patients out of 30 were still alive, with 3 remaining on treatment • No additional safety signals or deaths were observed since the initial analysis; 1 new grade ≥3 TRAE (grade 3 keratoacanthoma) was observed • Bintrafusp alfa showed a 20% response rate with a long duration of response ; 42.8% of the patients have an ongoing response after 18 months (18+, 23.5+, and 24+ months) • The median OS was 12.7 months; 24-month OS and PFS rates were 27.7% and 11.1%, respectively • The efficacy of bintrafusp alfa in patients with pretreated BTC compares favorably with that of mFOLFOX from the ABC-06 study (ORR, 5%; median OS, 6.2 months) 2 • Bintrafusp alfa is under further investigation as a 1L (NCT04066491) and 2L (NCT03833661) treatment option for patients with locally advanced/ metastatic BTC REFERENCES 1. Lamarca A, et al. Ann Oncol. 2014;25:2328-38 2. Lamarca A, et al. J Clin Oncol. 2019;37(Suppl 15):Abstract 4003. 3. Kim RD, et al. JAMA Oncol. 2020;6:1-8. 4. Ikeda M, et al. J Clin Oncol. 2019;37(Suppl 4):Abstract 306. 5. Ueno M, et al. Ann Oncol. 2018;29(Suppl 8):Abstract 625PD 6. Akhurst RJ, et al. Nat Rev Drug Discov. 2012;11:790-811. 7. Colak S, et al. Trends Cancer. 2017;3:56-71. 8. Nakamura H, et al. Nat Genet. 2015;47:1003-10. 9. Chen Y, et al. Biol Res. 2015;48:26. 10. Lustri AM, et al. PLoS One. 2017;12:e0183932. 11. Strauss J, et al. Clin Cancer Res. 2018;24:1287-95. 12. Yoo C, et al. J Immunother Cancer. 2020;8:e000564. ACKNOWLEDGMENTS Study sponsored by Merck KGaA, Darmstadt, Germany, as part of an alliance between Merck KGaA, Darmstadt, Germany, and GlaxoSmithKline. The authors thank the patients and their families, investigators, co-investigators, and study teams at each of the participating centers and at Merck KGaA, Darmstadt, Germany, and EMD Serono Research & Development Institute, Inc., Billerica, MA, USA; a business of Merck KGaA, Darmstadt, Germany. Medical writing support was provided by Spencer Hughes, PhD, of ClinicalThinking, Inc, Hamilton, NJ, USA, which was also funded by Merck KGaA, Darmstadt, Germany, and GlaxoSmithKline in accordance with Good Publication Practice guidelines (http://www.ismpp.org/gpp3). Correspondence: Changhoon Yoo, [email protected] DISCLOSURES CY reports: honoraria from Merck Serono, Servier, Bayer, Ipsen, MSD, Celgene, and AstraZeneca; advisory/consultancy fees from Servier, Bayer, Ipsen, MSD, and AstraZeneca; research funding from Servier, Bayer, AstraZeneca, and Ono Pharmaceuticals. D-YO reports: advisory/consultancy fees from AstraZeneca, Novartis, Genentech/Roche, Merck Serono, Bayer, Taiho, ASLAN, Halozyme, Zymeworks, and Celgene; research funding from AstraZeneca, Novartis, Array, and Eli Lilly. HJC reports: advisory/consultancy fees from Bayer, Ono Pharmaceuticals, and MSD. MK reports: honoraria from Eisai, Bayer, MSD, Bristol Myers Squibb, Eli Lilly, and EA Pharma; advisory/consultancy fees from Eisai, Ono, MSD, Bristol Myers Squibb, and Roche; research funding from Eisai, Gilead Sciences, Taiho, Sumitomo Dainippon Pharma, Takeda, Otsuka, EA Pharma, and AbbVie. MU reports: honoraria from Taiho Pharmaceutical, Yakult Honsha, AstraZeneca, Ono Pharmaceutical, Merck Biopharma, and MSD; research funding from Taiho Pharmaceutical, Daiichi Sankyo, Eisai, AstraZeneca, Ono Pharmaceutical, MSD, Merck Biopharma, Dainippon Sumitomo Pharma, Incyte, Yakult Honsha, and Astellas. SK reports research funding from MSD, AbbVie, Eli Lilly, AZD, Pfizer, Takeda, and Boehringer Ingelheim. L-TC reports: honoraria from Ono Pharmaceutical, Eli Lilly, MSD, PharmaEngine, TTY, SyncorePharm, Novartis, AstraZeneca, and Ipsen; a leadership role and employment at the National Institute of Cancer Research, Taiwan; research funding from Novartis, Merck Serono, TTY, Polaris, SyncorePharm, Pfizer, and BMS; licensing/ royalties from HuniLife; a position as an officer/Board of Directors at SinoPharm Taiwan, Ltd. MO is an employee of Merck Biopharma, Tokyo, Japan, an affiliate of Merck KGaA, Darmstadt, Germany. CH reports stock options and employment at Merck KGaA, Darmstadt, Germany. ID is an employee of EMD Serono, Billerica, Massachusetts, USA, a business of Merck KGaA, Darmstadt, Germany. MI reports: honoraria from Eli Lilly, Taiho, Chugai, Novartis, Yakult, Teijin, Servier, Eisai, and Bayer; advisory/consultancy fees from Eli Lilly, AstraZeneca, Eisai, Chugai, Servier, and Novartis; research funding from Yakult, Ono Pharmaceutical, Bristol Myers Squibb, MSD, J-Pharma, Chugai, ASLAN, Takeda, Bayer, Eli Lilly, Pfizer, Eisai, Merck Serono, Novartis, Astellas, and AstraZeneca Copies of this e-poster obtained through QR (Quick Response) and/or text key codes are for personal use only and may not be reproduced without written permission of the authors. GET POSTER PDF
Transcript of Long-term follow-up of bintrafusp alfa, a bifunctional ...

Abstract No. 1418. Presented at the ESMO Virtual Congress 2020, September 19-21, 2020
Long-term follow-up of bintrafusp alfa, a bifunctional fusion protein targeting TGF-β and PD-L1, in patients with pretreated biliary tract cancer
C. Yoo1, D.-Y. Oh2, H. J. Choi3, M. Kudo4, M. Ueno5, S. Kondo6, L.-T. Chen7, M. Osada8, C. Helwig9, I. Dussault10, M. Ikeda11
1Asan Medical Center, University of Ulsan College of Medicine, Seoul, Republic of Korea; 2Seoul National University Hospital, Cancer Research Institute, Seoul National University College of Medicine, Seoul, Republic of Korea; 3Department of Medicine, Oncology, Yonsei University College of Medicine, Seoul, Republic of Korea; 4Kindai University Faculty of Medicine, Osaka-Sayama, Japan; 5Department of Gastroenterology, Hepatobiliary and Pancreatic Medical Oncology Division, Kanagawa Cancer Center, Yokohama, Japan; 6National Cancer Center Hospital, Tokyo, Japan; 7National Cheng Kung University Hospital, National Institute of Cancer Research, Tainan, Taiwan; 8Merck Biopharma, Tokyo, Japan, an affiliate of Merck KGaA, Darmstadt, Germany; 9Merck KGaA, Darmstadt, Germany; 10EMD Serono Research & Development Institute, Inc., Billerica, MA, USA; a business of Merck KGaA, Darmstadt, Germany; 11National Cancer Center Hospital East, Kashiwa, Japan
Poster No. 73P
BACKGROUND
Biliary tract cancer (BTC)• BTC is a rare, heterogenous, and lethal group of cancers with limited
treatment options
• Gemcitabine plus cisplatin is the standard of care for first-line (1L) BTC treatment; however, no global standard of care has been established for second-line (2L) treatment of BTC because the efficacy of 2L chemotherapy in advanced BTC is low:
– A recent meta-analysis of 2L chemotherapy in BTC found a median overall survival (OS) of 7.2 months and objective response rate (ORR) of 7.7%1
– The ABC-06 study showed clinical benefit of treatment with mFOLFOX (oxaliplatin, leucovorin, and 5-fluorouracil) vs active symptom control for locally advanced/metastatic 2L BTC; however, the median progression-free survival (PFS) of 4.0 months, 12-month OS rate of 25.9%, and ORR of 5% indicate an unmet need2
• Recent studies for the treatment of multiple cancers with immune checkpoint inhibitors (ICIs) have shown promising results, although the efficacy of ICIs has yet to be demonstrated in BTC:
– In a phase 2 study of nivolumab in patients with pretreated advanced BTC, the ORR was 22% per the investigator (11% per independent review committee).3 Furthermore, ORR with nivolumab monotherapy was 3.3% (1 partial response in 30 patients) in a phase 1 study in patients with unresectable/recurrent BTC refractory to or intolerant of gemcitabine4
– In the phase 2 KEYNOTE-158 study of pembrolizumab monotherapy in patients with previously treated unresectable and/or metastatic BTC, the ORR was 5.8% (6 PRs in 104 patients) in the PD-L1–unselected population and 6.6% (4 PRs in 61 patients) in patients with PD-L1–positive tumors5
Transforming growth factor β (TGF-β) • The TGF-β pathway can promote cancer progression and immune evasion
in the tumor microenvironment via regulatory effects on immune cells, as well as by impacting processes such as angiogenesis, fibrosis, and epithelial-mesenchymal transition6,7
• Preclinical studies have shown a link between aberrant TGF-β signaling and BTC pathogenesis
– Genomic alterations in TGF-β signaling have been reported in 10% to 20% of the 3 major subtypes of BTC: intrahepatic cholangiocarcinoma (IHCC), extrahepatic cholangiocarcinoma (EHCC), and gallbladder cancer8
– Data suggest a correlation between the expression of TGF-β1 in patients with BTC and lymph node metastasis, distant metastasis, and tumor recurrence9
– TGF-β receptor inhibitors, such as galunisertib, can exert anticancer effects against human BTC cells10
• Thus, inhibiting TGF-β activity in the tumor microenvironment while simultaneously blocking an additional immunosuppressive signaling mechanism, such as the PD-L1 pathway, may provide a novel treatment approach
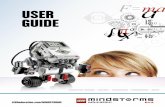
Bintrafusp alfa• Bintrafusp alfa is a first-in-class bifunctional fusion protein composed of the
extracellular domain of the TGF-βRII receptor to function as a TGF-β “trap” fused to a human IgG1 mAb blocking PD-L1 (Figure 1)
• The bifunctional nature of bintrafusp alfa might allow for colocalized, simultaneous inhibition of two nonredundant immunosuppressive pathways (TGF-β and PD-L1) within the tumor microenvironment, which may result in increased efficacy in locally advanced/metastatic BTC11
• Overall safety/tolerability data from phase 1 studies of bintrafusp alfa and an exposure-safety analysis conducted on an integrated data set with >670 participants supported the selection of 1200 mg every 2 weeks (Q2W) as the monotherapy recommended phase 2 dose
• Prior analysis of this phase 1 study (NCT02699515) expansion cohort found a manageable safety profile and an ORR of 20% per independent review committee (IRC) assessment and 23.3% as assessed by investigator in patients with pretreated BTC who received bintrafusp alfa12
• The median duration of response (DOR) was 9.7 months as assessed by the investigator (not reached per IRC) and the median OS was 12.7 months12
• Here, we present a 28-month update on the efficacy and safety follow-up in an expansion cohort of this phase 1 study of patients with BTC receiving bintrafusp alfa
Figure 1. Proposed mechanism of action of bintrafusp alfa
Fibroblast
CAF
Fibrosis and impaireddrug access
EMT (leading to metastasis and resistanceto therapy [including checkpoint inhibition])
Tumor angiogenesis
Tumor cells
PD-L1
Bintrafuspalfa
PD-1
T cell
Suppression of immune response
NK cell
TAMDendritic
cell
CytotoxicT cell
Tumor cellsMesenchymal-like
tumor cell
TGF-β “trap” moiety sequesters TGF-β to block downstream signaling
Anti–PD-L1 mAb moietyblocks PD-L1 interactions with PD-1
TGF-β*
CAF, cancer-associated fibroblast; NK, natural killer; TAM, tumor-associated macrophage.
*Tumor cells are also a major source of TGF-β in the microenvironment.
METHODS• NCT02699515 is an ongoing phase 1, open-label study of bintrafusp alfa
with an expansion cohort of chemotherapy-experienced patients with BTC
• Asian patients with BTC for whom 1L chemotherapy failed received bintrafusp alfa 1200 mg Q2W until confirmed disease progression, unacceptable toxicity, or withdrawal
• The primary objective of this study was safety/tolerability
– Key secondary objectives included investigator-assessed best overall response per RECIST 1.1, median OS, median DOR, and proportion of ongoing responses
RESULTS
Baseline patient and disease characteristics• Thirty patients were enrolled in this cohort; 13.3% (n=4) of patients had
received ≥2 prior anticancer regimens
– All patients had disease progression following 1L treatment and received no prior immunotherapy
• This cohort consisted of patients with gallbladder carcinoma (40% [n=12]), intrahepatic cholangiocarcinoma (33.3% [n=10]), extrahepatic cholangiocarcinoma (23.3% [n=7]), and ampullary carcinoma (3.3% [n=1])
• This follow-up uses a database cutoff of October 24, 2019 (28 months from the last patient’s first dose), with a Kaplan-Meier estimate of follow-up time of 121.6 weeks
Safety• Since the prior analysis, no additional deaths or safety signals were
observed; 1 new grade ≥3 TRAE (grade 3 keratoacanthoma) was observed
• At the August 24, 2018 data cutoff, 63.3% of patients experienced treatment-related adverse events (TRAEs)
– Eleven patients (36.7%) experienced grade ≥3 TRAEs
– Two patients experienced grade 4 events (increased amylase, aspartate aminotransferase, and lipase levels)
• Three treatment-emergent deaths occurred
– Septic shock (n=1) due to bacteremia of unknown etiology 249 days after the first dose and 14 days after the last dose
– Interstitial lung disease (reported term, interstitial pneumonitis) in 2 patients
Table 1. Investigator-assessed efficacy as of October 24, 2019 cutoff
Outcome Efficacy
ORR, % 23.3
DCR, % 36.7
Median DOR, months (95% CI)≥6-month response, % (n)≥12-month response, % (n)≥18-month response, % (n)
18.0 (2.8-NE)71.4 (5)57.1 (4)42.8 (3)
Median PFS, months (95% CI)12-month PFS, % (95% CI)18-month PFS, % (95% CI) 24-month PFS, % (95% CI)
2.5 (1.3-4.0)14.8 (4.7-30.3)14.8 (4.7-30.3)11.1 (2.8-25.7)
Median OS, months (95% CI)12-month OS, % (95% CI)18-month OS, % (95% CI) 24-month OS, % (95% CI)
12.7 (6.7-15.8)52.0 (32.8-68.2)31.2 (15.7-48.1)27.7 (13.1-44.5)
NE, not estimable.
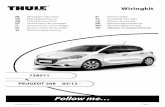
• Since the initial analysis, the investigator-assessed ORR and DCR remained at 23.3% (20.0% per IRC) and 36.7% (40.0% per IRC), respectively (Table 1 and Figure 2)
• Responses were durable; 3 responses are ongoing of 7 responders (42.8%), with DORs of 18+, 23.5+, and 24+ months (Figure 5)
• The median OS was 12.7 months, with a 24-month OS rate of 27.7% (Figure 3)
• The median PFS was 2.5 months, with a 24-month PFS rate of 11.1% (Figure 4)
Figure 2. Change in sum of target lesion diameters per investigator
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
Months
-80
-30
20
70
90
Cha
nge
in s
um o
f dia
met
ers,
(%
)
First occurrence of new lesionPatients off treatmentSD, PD or NEPRCR
CR, complete response; SD, stable disease; PD, progressive disease; NE, not estimable.Patients with no postbaseline assessment (n=2) are not included in this graph.*Microsatellite instability-high patient.
Figure 3. OS in the overall population
No. at risk30 262626 2121 1717 15 11
12-month OS: 52.0% (95% CI, 32.8-68.2)
18-month OS: 31.2%(95% CI, 15.7-48.1) 24-month OS: 27.7%
(95% CI, 13.1-44.5)
9 9 8 55 3 0
0 3 6 9 12 15 18 21 24 27 30 330
10
20
30
40
50
60
70
80
90
100
Months
OS,
%
6.7-15.895% CI12.7 monthsMedian
22No. of events
Figure 4. PFS for overall population
No. at risk30 99999 7 5 4 4 4 4 3 2 2 0
0 3 6 9 12 15 18 21 24 27 30 330
10
20
30
40
50
60
70
80
90
100
PFS.
%
Months
1.3-4.095% CI2.5 monthsMedian
25No. of events
12-month PFS: 14.8%(95% CI, 4.7-30.3)
18-month PFS: 14.8%(95% CI, 4.7-30.3) 24-month PFS: 11.1%
(95% CI, 2.8-25.7)
Figure 5. Time to and duration of response per investigator
0 10 20 30Months
Ongoing response Subsequent anticancer treatmentEnd of treatmentDeathPDPRCR
Median DOR: 18.0 months (95% CI 2.8-NE)
Length of bar shows time to PD/death/last tumor assessment. Arrow indicates ongoing response (ie, no PD or death at cutoff date in patients with CR or PR).
CONCLUSIONS• After 28 months of follow-up, bintrafusp alfa continues to demonstrate
manageable safety with durable, long-lasting responses and long-term survival in this expansion cohort of Asian patients with pretreated BTC
• As of the October 24, 2019 data cutoff, 8 patients out of 30 were still alive, with 3 remaining on treatment
• No additional safety signals or deaths were observed since the initial analysis; 1 new grade ≥3 TRAE (grade 3 keratoacanthoma) was observed
• Bintrafusp alfa showed a 20% response rate with a long duration of response ; 42.8% of the patients have an ongoing response after 18 months (18+, 23.5+, and 24+ months)
• The median OS was 12.7 months; 24-month OS and PFS rates were 27.7% and 11.1%, respectively
• The efficacy of bintrafusp alfa in patients with pretreated BTC compares favorably with that of mFOLFOX from the ABC-06 study (ORR, 5%; median OS, 6.2 months)2
• Bintrafusp alfa is under further investigation as a 1L (NCT04066491) and 2L (NCT03833661) treatment option for patients with locally advanced/metastatic BTC
REFERENCES1. Lamarca A, et al. Ann Oncol. 2014;25:2328-38
2. Lamarca A, et al. J Clin Oncol. 2019;37(Suppl 15):Abstract 4003.
3. Kim RD, et al. JAMA Oncol. 2020;6:1-8.
4. Ikeda M, et al. J Clin Oncol. 2019;37(Suppl 4):Abstract 306.
5. Ueno M, et al. Ann Oncol. 2018;29(Suppl 8):Abstract 625PD
6. Akhurst RJ, et al. Nat Rev Drug Discov. 2012;11:790-811.
7. Colak S, et al. Trends Cancer. 2017;3:56-71.
8. Nakamura H, et al. Nat Genet. 2015;47:1003-10.
9. Chen Y, et al. Biol Res. 2015;48:26.
10. Lustri AM, et al. PLoS One. 2017;12:e0183932.
11. Strauss J, et al. Clin Cancer Res. 2018;24:1287-95.
12. Yoo C, et al. J Immunother Cancer. 2020;8:e000564.
ACKNOWLEDGMENTSStudy sponsored by Merck KGaA, Darmstadt, Germany, as part of an alliance between Merck KGaA, Darmstadt, Germany, and GlaxoSmithKline. The authors thank the patients and their families, investigators, co-investigators, and study teams at each of the participating centers and at Merck KGaA, Darmstadt, Germany, and EMD Serono Research & Development Institute, Inc., Billerica, MA, USA; a business of Merck KGaA, Darmstadt, Germany.
Medical writing support was provided by Spencer Hughes, PhD, of ClinicalThinking, Inc, Hamilton, NJ, USA, which was also funded by Merck KGaA, Darmstadt, Germany, and GlaxoSmithKline in accordance with Good Publication Practice guidelines (http://www.ismpp.org/gpp3).
Correspondence: Changhoon Yoo, [email protected]
DISCLOSURESCY reports: honoraria from Merck Serono, Servier, Bayer, Ipsen, MSD, Celgene, and AstraZeneca; advisory/consultancy fees from Servier, Bayer, Ipsen, MSD, and AstraZeneca; research funding from Servier, Bayer, AstraZeneca, and Ono Pharmaceuticals. D-YO reports: advisory/consultancy fees from AstraZeneca, Novartis, Genentech/Roche, Merck Serono, Bayer, Taiho, ASLAN, Halozyme, Zymeworks, and Celgene; research funding from AstraZeneca, Novartis, Array, and Eli Lilly. HJC reports: advisory/consultancy fees from Bayer, Ono Pharmaceuticals, and MSD. MK reports: honoraria from Eisai, Bayer, MSD, Bristol Myers Squibb, Eli Lilly, and EA Pharma; advisory/consultancy fees from Eisai, Ono, MSD, Bristol Myers Squibb, and Roche; research funding from Eisai, Gilead Sciences, Taiho, Sumitomo Dainippon Pharma, Takeda, Otsuka, EA Pharma, and AbbVie. MU reports: honoraria from Taiho Pharmaceutical, Yakult Honsha, AstraZeneca, Ono Pharmaceutical, Merck Biopharma, and MSD; research funding from Taiho Pharmaceutical, Daiichi Sankyo, Eisai, AstraZeneca, Ono Pharmaceutical, MSD, Merck Biopharma, Dainippon Sumitomo Pharma, Incyte, Yakult Honsha, and Astellas. SK reports research funding from MSD, AbbVie, Eli Lilly, AZD, Pfizer, Takeda, and Boehringer Ingelheim. L-TC reports: honoraria from Ono Pharmaceutical, Eli Lilly, MSD, PharmaEngine, TTY, SyncorePharm, Novartis, AstraZeneca, and Ipsen; a leadership role and employment at the National Institute of Cancer Research, Taiwan; research funding from Novartis, Merck Serono, TTY, Polaris, SyncorePharm, Pfizer, and BMS; licensing/royalties from HuniLife; a position as an officer/Board of Directors at SinoPharm Taiwan, Ltd. MO is an employee of Merck Biopharma, Tokyo, Japan, an affiliate of Merck KGaA, Darmstadt, Germany. CH reports stock options and employment at Merck KGaA, Darmstadt, Germany. ID is an employee of EMD Serono, Billerica, Massachusetts, USA, a business of Merck KGaA, Darmstadt, Germany. MI reports: honoraria from Eli Lilly, Taiho, Chugai, Novartis, Yakult, Teijin, Servier, Eisai, and Bayer; advisory/consultancy fees from Eli Lilly, AstraZeneca, Eisai, Chugai, Servier, and Novartis; research funding from Yakult, Ono Pharmaceutical, Bristol Myers Squibb, MSD, J-Pharma, Chugai, ASLAN, Takeda, Bayer, Eli Lilly, Pfizer, Eisai, Merck Serono, Novartis, Astellas, and AstraZeneca
Copies of this e-poster obtained through QR (Quick Response) and/or text key codes are for personal use only and may not be reproduced without written permission of the authors.
GET POSTER PDF











![Complex Data For single channel data [1] – Real and imag. images are normally distributed with N(S, σ 2 ) – Then magnitude images follow Rice dist., which.](https://static.fdocument.org/doc/165x107/5519d135550346695e8b4cc1/complex-data-for-single-channel-data-1-real-and-imag-images-are-normally-distributed-with-ns-2-then-magnitude-images-follow-rice-dist-which.jpg)