Late blocking of peripheral TNF-α is ineffective after spinal cord injury in mice
4
Immunobiology 218 (2013) 281–284 Contents lists available at SciVerse ScienceDirect Immunobiology jou rnal h om epage: www.elsevier.com/locate/imbio Short communication Late blocking of peripheral TNF- is ineffective after spinal cord injury in mice Pía M. Vidal 1 , Evi Lemmens 1 , Lies Geboes, Tim Vangansewinkel, Sofie Nelissen, Sven Hendrix ∗ Department of Morphology & Biomedical Research Institute, Hasselt University, Belgium a r t i c l e i n f o Article history: Received 22 March 2012 Received in revised form 4 May 2012 Accepted 16 May 2012 Keywords: Basso mouse scale Enbrel Etanercept Tumor necrosis factor Rotarod a b s t r a c t Spinal cord injury (SCI) is characterized by different phases of inflammatory responses. Increasing evi- dence indicates that the early chronic phase (two to three weeks after SCI) is characterized by a dramatic invasion of immune cells and a peak of pro-inflammatory cytokine levels, such as tumor necrosis factor- (TNF-) derived from the injured spinal cord as well as from injured skin, muscles and bones. How- ever, there is substantial controversy whether these inflammatory processes in later phases lead to pro-regenerative or detrimental effects. In the present study, we investigated whether the inhibition of peripheral TNF- in the early chronic phase after injury promotes functional recovery in a dorsal hemisection model of SCI. Three different approaches were used to continuously block peripheral TNF- in vivo, starting 14 days after injury. We administered the TNF- blocker etanercept intraperitoneally (every second day or daily) as well as continuously via osmotic minipumps. None of these administration routes for the TNF- inhibitor influenced locomotor restoration as assessed by the Basso mouse scale (BMS), nor did they affect coordination and strength as evaluated by the Rotarod test. These data suggest that peripheral TNF- inhibition may not be an effective therapeutic strategy in the early chronic phase after SCI. © 2012 Elsevier GmbH. All rights reserved. Introduction The pluripotent pro-inflammatory cytokine tumor necrosis factor- (TNF-) is synthesized by many cell types including neu- rons, glia, activated macrophages, T cells, astrocytes, Schwann cells and mast cells (Hopkins and Rothwell 1995). It is immediately upregulated in response to central nervous system (CNS) trauma such as spinal cord injury (SCI) (Oshima et al. 2009; Pineau and Lacroix 2007; Tracey and Lowry 1990; Wajant et al. 2003) deriving from the injured CNS itself, as well as from injured skin, muscles and bones. Besides the first peak of TNF- mRNA levels in the acute and subacute phases after SCI (Pineau and Lacroix 2007; Bartholdi and Schwab 1997; Bethea et al. 1999; Koopmans et al. 2009; Streit et al. 1998), some authors have also reported a second TNF- mRNA peak around 14–28 days after injury (Pineau and Lacroix 2007). There is a lot of controversy about the in vitro and in vivo effects of TNF- after CNS trauma, reported to be either detrimental (Lee et al. 2000; Neumann et al. 2002; Clarke and Branton 2002; Chertoff et al. 2011) or neuroprotective (Oshima et al. 2009; Chertoff et al. 2011; D’Souza et al. 1995; Sullivan et al. 1999) and pro-regenerative ∗ Corresponding author at: Department of Morphology & Biomedical Research Institute, Hasselt University, Agoralaan, Building C, B-3590, Diepenbeek, Belgium. Tel.: +32 11 26 9246; fax: +32 11 26 9299. E-mail address: [email protected] (S. Hendrix). 1 Contributed equally. (Schmitt et al. 2010), depending on the animal model used. These contradicting results may be in part the result of TNF- interaction with two types of receptors, namely TNFR-1 and TNFR-2, which are expressed on different cell types and are associated with differ- ent cellular effects (Wajant et al. 2003). In different models of SCI, TNF- appears to have detrimental effects on spinal cord recov- ery, since treatment with TNF- blockers (Koopmans et al. 2009; Genovese et al. 2006, 2007) and antibodies to the TNFR-1 (Lee et al. 2000; Neumann et al. 2002; Clarke and Branton 2002) improved spinal cord recovery substantially. In contrast, the life-long absence of TNFR-1 and TNFR-2 in knockout mice reduces NF-B activation and functional recovery after SCI (Kim et al. 2001). Increased TNF- levels shortly after CNS trauma have been linked to a sequence of cellular dysregulations, accompanied by enhanced vascular permeability, impaired glutamate metabolism and clearance (Takahashi et al. 2003), and in some settings an excessive inflammatory reaction (Pineau and Lacroix 2007). Sev- eral studies indicate that it is important to regulate increased TNF- levels immediately after injury to control the excitotoxic effect of TNF- on AMPA and GABA receptors after injury (Stellwagen et al. 2005; Zhao et al. 2010), and to decrease TNF--induced apopto- sis (Genovese et al. 2006). Consistently, a single dose of etanercept immediately after injury appears to be sufficient to improve hind limb locomotor function and reduce apoptosis of neurons and oligodendrocytes in the rat spinal cord (Chen et al. 2011). However, in all functional studies TNF- antagonists were administered immediately or 6 h after injury (Genovese et al. 2006, 0171-2985/$ – see front matter © 2012 Elsevier GmbH. All rights reserved. http://dx.doi.org/10.1016/j.imbio.2012.05.007
Transcript of Late blocking of peripheral TNF-α is ineffective after spinal cord injury in mice

S
L
PD
a
ARRA
KBEETR
I
frausLfaaaep
oee2
IT
0h
Immunobiology 218 (2013) 281– 284
Contents lists available at SciVerse ScienceDirect
Immunobiology
jou rna l h om epage: www.elsev ier .com/ locate / imbio
hort communication
ate blocking of peripheral TNF-� is ineffective after spinal cord injury in mice
ía M. Vidal1, Evi Lemmens1, Lies Geboes, Tim Vangansewinkel, Sofie Nelissen, Sven Hendrix ∗
epartment of Morphology & Biomedical Research Institute, Hasselt University, Belgium
r t i c l e i n f o
rticle history:eceived 22 March 2012eceived in revised form 4 May 2012ccepted 16 May 2012
eywords:asso mouse scalenbreltanercept
a b s t r a c t
Spinal cord injury (SCI) is characterized by different phases of inflammatory responses. Increasing evi-dence indicates that the early chronic phase (two to three weeks after SCI) is characterized by a dramaticinvasion of immune cells and a peak of pro-inflammatory cytokine levels, such as tumor necrosis factor-�(TNF-�) derived from the injured spinal cord as well as from injured skin, muscles and bones. How-ever, there is substantial controversy whether these inflammatory processes in later phases lead topro-regenerative or detrimental effects. In the present study, we investigated whether the inhibitionof peripheral TNF-� in the early chronic phase after injury promotes functional recovery in a dorsalhemisection model of SCI. Three different approaches were used to continuously block peripheral TNF-�
umor necrosis factorotarod
in vivo, starting 14 days after injury. We administered the TNF-� blocker etanercept intraperitoneally(every second day or daily) as well as continuously via osmotic minipumps. None of these administrationroutes for the TNF-� inhibitor influenced locomotor restoration as assessed by the Basso mouse scale(BMS), nor did they affect coordination and strength as evaluated by the Rotarod test. These data suggestthat peripheral TNF-� inhibition may not be an effective therapeutic strategy in the early chronic phaseafter SCI.
ntroduction
The pluripotent pro-inflammatory cytokine tumor necrosisactor-� (TNF-�) is synthesized by many cell types including neu-ons, glia, activated macrophages, T cells, astrocytes, Schwann cellsnd mast cells (Hopkins and Rothwell 1995). It is immediatelypregulated in response to central nervous system (CNS) traumauch as spinal cord injury (SCI) (Oshima et al. 2009; Pineau andacroix 2007; Tracey and Lowry 1990; Wajant et al. 2003) derivingrom the injured CNS itself, as well as from injured skin, musclesnd bones. Besides the first peak of TNF-� mRNA levels in the acutend subacute phases after SCI (Pineau and Lacroix 2007; Bartholdind Schwab 1997; Bethea et al. 1999; Koopmans et al. 2009; Streitt al. 1998), some authors have also reported a second TNF-� mRNAeak around 14–28 days after injury (Pineau and Lacroix 2007).
There is a lot of controversy about the in vitro and in vivo effectsf TNF-� after CNS trauma, reported to be either detrimental (Lee
t al. 2000; Neumann et al. 2002; Clarke and Branton 2002; Chertofft al. 2011) or neuroprotective (Oshima et al. 2009; Chertoff et al.011; D’Souza et al. 1995; Sullivan et al. 1999) and pro-regenerative∗ Corresponding author at: Department of Morphology & Biomedical Researchnstitute, Hasselt University, Agoralaan, Building C, B-3590, Diepenbeek, Belgium.el.: +32 11 26 9246; fax: +32 11 26 9299.
E-mail address: [email protected] (S. Hendrix).1 Contributed equally.
171-2985/$ – see front matter © 2012 Elsevier GmbH. All rights reserved.ttp://dx.doi.org/10.1016/j.imbio.2012.05.007
© 2012 Elsevier GmbH. All rights reserved.
(Schmitt et al. 2010), depending on the animal model used. Thesecontradicting results may be in part the result of TNF-� interactionwith two types of receptors, namely TNFR-1 and TNFR-2, whichare expressed on different cell types and are associated with differ-ent cellular effects (Wajant et al. 2003). In different models of SCI,TNF-� appears to have detrimental effects on spinal cord recov-ery, since treatment with TNF-� blockers (Koopmans et al. 2009;Genovese et al. 2006, 2007) and antibodies to the TNFR-1 (Lee et al.2000; Neumann et al. 2002; Clarke and Branton 2002) improvedspinal cord recovery substantially. In contrast, the life-long absenceof TNFR-1 and TNFR-2 in knockout mice reduces NF-�B activationand functional recovery after SCI (Kim et al. 2001).
Increased TNF-� levels shortly after CNS trauma have beenlinked to a sequence of cellular dysregulations, accompanied byenhanced vascular permeability, impaired glutamate metabolismand clearance (Takahashi et al. 2003), and in some settings anexcessive inflammatory reaction (Pineau and Lacroix 2007). Sev-eral studies indicate that it is important to regulate increased TNF-�levels immediately after injury to control the excitotoxic effect ofTNF-� on AMPA and GABA receptors after injury (Stellwagen et al.2005; Zhao et al. 2010), and to decrease TNF-�-induced apopto-sis (Genovese et al. 2006). Consistently, a single dose of etanerceptimmediately after injury appears to be sufficient to improve hind
limb locomotor function and reduce apoptosis of neurons andoligodendrocytes in the rat spinal cord (Chen et al. 2011).However, in all functional studies TNF-� antagonists wereadministered immediately or 6 h after injury (Genovese et al. 2006,

282 P.M. Vidal et al. / Immunobiolo
Protein leve ls i n the spinal cord
0
100
200
300
400
500
7days 14 da ys 21 da ys
spina l cord injury
sha m ope ration
TN
F-α
(p
g/m
l)
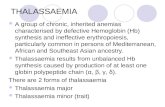
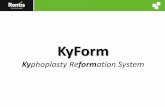
Fig. 1. TNF-� protein levels after SCI. Cytometric bead array analysis in spinal cordsso
2ltpas(eBCwraaa
M
S
(Nthsfstwbt
E
eatie
hows a slight but not statistically significant increase of local TNF-� levels in thepinal cord of mice at days 7, 14 and 21 after spinal cord injury compared to sham-perated mice (n = 5–12 mice per time point).
007; Chen et al. 2011) ignoring the second peak of TNF-� in theater phases after injury. There is still much controversy whetherhe inflammatory response in the chronic phase after CNS traumaromotes or inhibits regeneration (Hendrix and Nitsch 2007). Inddition, a modulation of peripheral inflammation may influenceubstantially the CNS immune status even if the blood brain barrierBBB) is intact (Teeling et al. 2010). Thus, a modulation of periph-ral TNF-� with inhibitors such as etanercept that do not cross theBB may be a promising approach during the chronic phases afterNS trauma when the BBB is already repaired. In the present study,e investigated the effects of different doses and administration
outes of the TNF-� inhibitor etanercept in the early chronic phasefter SCI. Our data, however, indicated that all three therapeuticpproaches were ineffective in modulating the functional outcomefter SCI.
aterials and methods
pinal cord hemisection injury
Dorsal hemisection SCI was performed as described previouslyBoato et al. 2010). Briefly, 10-week old C57BL/6 mice (Harlan, theetherlands) were anesthetized and underwent a partial laminec-
omy at thoracic level T8, and were subjected to a bilateral dorsalemisection consisting of a complete transection with iridectomycissors of all parts of the corticospinal tract: left and right dorsaluniculus, dorsal horns and the ventral funiculus. The muscles wereutured and the back skin closed with wound clips. After surgery,he mice were placed in a recovery chamber (32 ◦C) until they wereell awake and could be returned to their home cage. The animals’
ladders were manually voided daily until the animals were ableo urinate independently.
xperimental groups
The treatment protocols are summarized in Fig. 2A. For eachxperiment, mice were distributed equally among the groups
ccording to their Basso mouse scale (BMS) score after SCI, andreatment was started at day 14 after injury. For the first exper-ment, mice were injected i.p. every two days for 12 days withtanercept (Enbrel®, Amgen, Pfizer; 125 �g/mouse) (Genovesegy 218 (2013) 281– 284
et al. 2006), or with saline solution (0.9%, w/v NaCl) or IgG fromhuman serum (Sigma; 125 �g/mouse) as a control. For the secondexperiment, two groups of animals were injected daily i.p. withsaline solution or etanercept (125 �g) for seven days. Finally, for thethird experiment, the mice were deeply anesthetized with isoflu-rane, a small incision was made in the back skin to implant s.c anosmotic minipump (Alzet 2004; 0.25 �l/h) filled with etanercept orsaline, and after implantation the back skin was closed with woundclips.
Locomotion tests
Animals were scored daily for functional recovery after SCI usingthe BMS (Basso et al. 2006) starting at day 1 after injury or with theRotarod starting at day 7. The BMS is a 10-point scale (9, normallocomotion; 0, complete hind limb paralysis) which is based onhind limb movements made in an open field during a 4 min interval,provided the mouse is moving for at least three body lengths using aconsistent speed. After allowing mice to recover for 6 days, Rotarodperformance (Sheng et al. 2004) was determined daily up to the endof the observation periods. The mice were placed on an acceleratedrolling rod (Ugo Basile, Comeris VA, Italy) and the latency to jumpoff from the rod was automatically recorded by the action of themouse dropping onto a trigger plate. For BMS analysis we used themean of the left and right hindlimb scores for each animal.
Protein expression in spinal cord
Animals were transcardially perfused with ringer solution atselected time points 7, 14 and 21 days after injury. After perfusion,spinal cord tissue was dissected out in a standardized area (0.5 cmproximal and 0.5 cm distal from the lesion site) and homogenizedusing the Procarta lysis buffer (Panomics, Italy). Homogenizedtissue was centrifuged at 10,000 rpm for 10 min at 4 ◦C. The super-natant was collected and protein levels were determined by flowcytometry using the cytometric bead array mouse flex set system(BD Biosciences) according to manufacturer’s instructions. Analysiswas performed using FACS arrays Bioanalyzer and FCAP software(BD Biosciences). Data represent mean values ± SEM.
Statistical analysis
Rotarod and BMS data were analyzed using a two way ANOVAas previously described (Basso et al. 2006) and represent meanvalues for all the animals of each experimental group (±SEM).The analyses were performed using GraphPad Prism 5.0 software(GraphPad software Inc., CA, USA). Every experimental approachwas performed three times.
Results and discussion
Etanercept is an FDA-approved TNF-� inhibitor for treatingrheumatoid arthritis, psoriatic arthritis and ankylosing spondyli-tis, which has also been tested preclinically in rodents as a therapyfor SCI (Genovese et al. 2006; Chen et al. 2011). Interestingly, largemolecules, such as etanercept, cannot cross the BBB when deliveredsystemically (Zhou et al. 2011). However, blocking TNF-� signal-ing by etanercept confers improved functional recovery after SCI, ifit is administered immediately after injury (Genovese et al. 2006;Chen et al. 2011). These findings suggest that either the damage tothe BBB must be sufficient to reach an adequate concentration ofetanercept at the lesion site or that a modulation of the peripheral
TNF-� levels results in beneficial outcome, or both. The rationale ofour study is based on results published on TNF-� mRNA levels in theinjured mouse spinal cord using in situ hybridization (Pineau andLacroix 2007), showing a second peak of TNF-� in the early chronic
P.M. Vidal et al. / Immunobiology 218 (2013) 281– 284 283
0 10 20 30 40
0
2
4
6
8
SCI, N = 28
SCI, t rea ted with NaC l, N = 15
SCI, t rea ted etane rcept (125 µg), N = 13
Days aft er spinal cord i njury
Basso
Mo
use
Scale
D
Trea tment period
Trea tment period
C
0 10 20 30 40
0
2
4
6
8
SCI, t rea ted with NaC l, N = 4
SCI, t rea ted etane rcept (125 µg), N = 4
Days aft er spinal cord i njury
Basso
Mo
use
Scale
A
Trea tment period
B
0 5 10 15 20 25 300
2
4
6
SCI, t rea ted etane rcept (125 µg), N = 7
SCI, t rea ted with NaC l, N = 5
SCI, t rea ted with hu man IgG, N = 6
Days aft er spinal cord i njury
Basso
Mo
use
Scale
Day 0 Day14 Day26 Day 33
Every two days i.p injection of etanerceptSCI
Dail y i.p injection of etanerceptSCI
Day 0 Day14 Day21 Day 33
Continuou s rele ase of etanercept using osmotic minipu mps SCI
Day 0 Da y14 Day 36
Experimen t I
Experimen t II
Experimen t II I
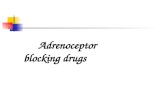
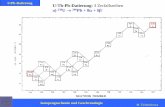
Fig. 2. TNF-� inhibition in the early chronic phase after SCI is ineffective. (A) Scheme of the three different treatment approaches used. For each experiment, treatment wasstarted at day 14 after SCI. (B) Mice received every second day i.p. injections with etanercept (125 �g) or human IgG (125 �g) or NaCl as controls. (C) Mice received dailyi ic mino In all
N
plWoiacseoSbut(oei
.p. injections with etanercept (125 �g), or NaCl as control, for 12 days. (D) Osmotf etanercept (125 �g, released at 0.25 �l/h) for three weeks or NaCl as a control.aCl-treated controls.
hase (14–28 days after injury) and our own data on TNF-� proteinevels in the spinal cord in mice after SCI or sham surgery (Fig. 1).
e found an average level of ∼200 pg/ml TNF-� in the spinal cordf sham-operated mice while in injured mice we found slightlyncreasing average levels of ∼200–300 pg/ml TNF-� at days 7, 14nd 21 after injury, however, these differences were not statisti-ally significant. Based on these data and the published findings wetarted treatment at day 14, and analyzed in the present study theffects of different doses as well as different administration routesf the TNF-� inhibitor etanercept in this early chronic phase afterCI (Fig. 2). Since etanercept is a fusion protein between the solu-le TNFR-2 and the Fc component of human IgG1, human IgG wassed as additional control. We analyzed the locomotor function inhese animals using the BMS score starting immediately after injury
Fig. 2B–D) and after 6 days of recovery, the mice were assessedn the Rotarod (data not shown). Surprisingly, administration oftanercept every 2 days for 12 days did not lead to any differencen motor performance of the treated animals, compared to miceipumps were implanted s.c. into mice in order to reach continuous daily releasethree treatment groups, no significant difference was found compared to IgG- or
treated with vehicle or control IgG (Fig. 2B, Rotarod: not shown). Ina second approach, we injected etanercept i.p. daily for one week(instead of every second day) in order to double the administereddose of etanercept over time. Again, no significant differences inthe BMS score were observed between the two control groups andthe etanercept-treated group (Fig. 2C; Rotarod: not shown). Sincedaily injections may not provide uninterrupted TNF-� inhibition,we used a third approach to obtain continuous levels of etanercept.We implanted osmotic minipumps to release a constant amount(125 �g/day) of etanercept during the early chronic phase startingat day 14 after SCI. Again, continuous release of etanercept duringthe early chronic phase did not influence the functional outcomeafter SCI (Fig. 2D; Rotarod: not shown).
In most SCI models, not only the spinal cord itself but also
the meninges, bones, muscles and skin are injured – especiallyafter a laminectomy. Thus, the precise source of TNF-� after SCI isnot well-defined. Furthermore, there is considerable controversywhether inflammatory processes in the different phases after CNS
2 obiolo
tretprtaimpIcetcaaeieh(soe
C
A
FsaWT
R
B
B
B
B
B
C
C
vation reduces TNFalpha-induced surface localization of AMPAR-type glutamate
84 P.M. Vidal et al. / Immun
rauma (acute, subacute, chronic) may either promote or impairegeneration (Hendrix and Nitsch 2007). In addition, there is goodvidence that peripheral inflammation exerts substantial effects onhe CNS without a damaged BBB (Moreno et al. 2011). For exam-le, systemic administration of LPS to mimic peripheral infectionevealed that systemic inflammation (=outside the BBB) modulateshe CNS cytokine profile and results in microglia and macrophagectivation as well as axon injury (Moreno et al. 2011). Therefore,t is important to keep in mind that blocking agents may indirectly
odulate the inflammatory milieu within the CNS by tuning theeripheral immune response to CNS injury (Teeling et al. 2010).
n summary, we have demonstrated that intraperitoneal etaner-ept injections every second day or daily as well as continuoustanercept release through osmotic minipumps, are ineffective asreatment in the early chronic phase after SCI. This is in strikingontrast to treatments that start in the highly acute phase immedi-tely after injury (Genovese et al. 2006; Chen et al. 2011). Although
lot of inflammatory processes have also been described in thearly chronic phase (Beck et al. 2010; Trivedi et al. 2006), our datandicate that an inhibition of TNF-� signaling is ineffective in influ-ncing the clinical outcome after SCI in the time period investigatedere. However, intrathecal administration of large TNF inhibitorswith all potential side effects) may be still an option as well aspecifically targeted molecules which pass the BBB. Nevertheless,ur data suggest that inhibition of peripheral TNF-� may not beffective in the early chronic phase after SCI.
onflict of interests
The authors declare that there are no conflicts of interests.
cknowledgements
This study was supported in part by grants from Deutscheorschungsgemeinschaft (SPP1394) to SH, from Fonds Weten-chappelijk Onderzoek – Vlaanderen to SH (G.0834.11N, G.0389.12)nd EL (1.2.703.10N), and from Agentschap voor Innovatie dooretenschap en Technologie (IWT) to TV. PV is a PhD student of the
ransnational University Limburg.
eferences
artholdi, D., Schwab, M.E., 1997. Expression of pro-inflammatory cytokine andchemokine mRNA upon experimental spinal cord injury in mouse: an in situhybridization study. Eur. J. Neurosci. 9, 1422.
ethea, J.R., Nagashima, H., Acosta, M.C., Briceno, C., Gomez, F., Marcillo, A.E., Loor, K.,Green, J., Dietrich, W.D., 1999. Systemically administered interleukin-10 reducestumor necrosis factor-alpha production and significantly improves functionalrecovery following traumatic spinal cord injury in rats. J. Neurotrauma 16, 851.
oato, F., Hendrix, S., Huelsenbeck, S.C., Hofmann, F., Grosse, G., Djalali, S., Kli-maschewski, L., Auer, M., Just, I., Ahnert-Hilger, G., Holtje, M., 2010. C3 peptideenhances recovery from spinal cord injury by improved regenerative growth ofdescending fiber tracts. J. Cell Sci. 123, 1652.
asso, D.M., Fisher, L.C., Anderson, A.J., Jakeman, L.B., McTigue, D.M., Popovich, P.G.,2006. Basso mouse scale for locomotion detects differences in recovery afterspinal cord injury in five common mouse strains. J. Neurotrauma 23, 635.
eck, K.D., Nguyen, H.X., Galvan, M.D., Salazar, D.L., Woodruff, T.M., Anderson, A.J.,2010. Quantitative analysis of cellular inflammation after traumatic spinal cordinjury: evidence for a multiphasic inflammatory response in the acute to chronicenvironment. Brain 133, 433.
larke, D.J., Branton, R.L., 2002. A role for tumor necrosis factor alpha in death of
dopaminergic neurons following neural transplantation. Exp. Neurol. 176, 154.hen, K.B., Uchida, K., Nakajima, H., Yayama, T., Hirai, T., Watanabe, S., Guerrero,A.R., Kobayashi, S., Ma, W.Y., Liu, S.Y., Baba, H., 2011. Tumor necrosis factor-alpha antagonist reduces apoptosis of neurons and oligodendroglia in rat spinalcord injury. Spine 36, 1350 (Phila Pa 1976).
gy 218 (2013) 281– 284
Chertoff, M., Di Paolo, N., Schoeneberg, A., Depino, A., Ferrari, C., Wurst, W., Pfizen-maier, K., Eisel, U., Pitossi, F., 2011. Neuroprotective and neurodegenerativeeffects of the chronic expression of tumor necrosis factor alpha in the nigrostri-atal dopaminergic circuit of adult mice. Exp. Neurol. 227, 237.
D’Souza, S., Alinauskas, K., McCrea, E., Goodyer, C., Antel, J.P., 1995. Differentialsusceptibility of human CNS-derived cell populations to TNF-dependent andindependent immune-mediated injury. J. Neurosci. 15, 7293.
Genovese, T., Mazzon, E., Crisafulli, C., Di Paola, R., Muia, C., Bramanti, P., Cuzzocrea,S., 2006. Immunomodulatory effects of etanercept in an experimental model ofspinal cord injury. J. Pharmacol. Exp. Ther. 316, 1006.
Genovese, T., Mazzon, E., Crisafulli, C., Esposito, E., Di Paola, R., Muia, C., Di Bella,P., Meli, R., Bramanti, P., Cuzzocrea, S., 2007. Combination of dexamethasoneand etanercept reduces secondary damage in experimental spinal cord trauma.Neuroscience 150, 168.
Hendrix, S., Nitsch, R., 2007. The role of T helper cells in neuroprotection and regen-eration. J. Neuroimmunol. 184, 100.
Hopkins, S.J., Rothwell, N.J., 1995. Cytokines and the nervous system I: expressionand recognition. Trends Neurosci. 18, 83.
Koopmans, G.C., Deumens, R., Buss, A., Geoghegan, L., Myint, A.M., Honig, W.H., Kern,N., Joosten, E.A., Noth, J., Brook, G.A., 2009. Acute rolipram/thalidomide treat-ment improves tissue sparing and locomotion after experimental spinal cordinjury. Exp. Neurol.
Kim, G.M., Xu, J., Song, S.K., Yan, P., Ku, G., Xu, X.M., Hsu, C.Y., 2001. Tumor necro-sis factor receptor deletion reduces nuclear factor-kappaB activation, cellularinhibitor of apoptosis protein 2 expression, and functional recovery after trau-matic spinal cord injury. J. Neurosci. 21, 6617.
Lee, Y.B., Yune, T.Y., Baik, S.Y., Shin, Y.H., Du, S., Rhim, H., Lee, E.B., Kim, Y.C., Shin, M.L.,Markelonis, G.J., Oh, T.H., 2000. Role of tumor necrosis factor-alpha in neuronaland glial apoptosis after spinal cord injury. Exp. Neurol. 166, 190.
Moreno, B., Jukes, J.P., Vergara-Irigaray, N., Errea, O., Villoslada, P., Perry, V.H.,Newman, T.A., 2011. Systemic inflammation induces axon injury during braininflammation. Ann. Neurol. 70, 932.
Neumann, H., Schweigreiter, R., Yamashita, T., Rosenkranz, K., Wekerle, H., Barde,Y.A., 2002. Tumor necrosis factor inhibits neurite outgrowth and branching ofhippocampal neurons by a rho-dependent mechanism. J. Neurosci. 22, 854.
Oshima, T., Lee, S., Sato, A., Oda, S., Hirasawa, H., Yamashita, T., 2009. TNF-alphacontributes to axonal sprouting and functional recovery following traumaticbrain injury. Brain Res. 1290, 102.
Pineau, I., Lacroix, S., 2007. Proinflammatory cytokine synthesis in the injured mousespinal cord: multiphasic expression pattern and identification of the cell typesinvolved. J. Comp. Neurol., 267.
Streit, W.J., Semple-Rowland, S.L., Hurley, S.D., Miller, R.C., Popovich, P.G., Stokes,B.T., 1998. Cytokine mRNA profiles in contused spinal cord and axotomized facialnucleus suggest a beneficial role for inflammation and gliosis. Exp. Neurol. 152,74.
Sullivan, P.G., Bruce-Keller, A.J., Rabchevsky, A.G., Christakos, S., Clair, D.K., Mattson,M.P., Scheff, S.W., 1999. Exacerbation of damage and altered NF-kappaB activa-tion in mice lacking tumor necrosis factor receptors after traumatic brain injury.J. Neurosci. 19, 6248.
Schmitt, K.R., Boato, F., Diestel, A., Hechler, D., Kruglov, A., Berger, F., Hendrix, S.,2010. Hypothermia-induced neurite outgrowth is mediated by tumor necrosisfactor-alpha. Brain Pathol. 20, 771.
Stellwagen, D., Beattie, E.C., Seo, J.Y., Malenka, R.C., 2005. Differential regulation ofAMPA receptor and GABA receptor trafficking by tumor necrosis factor-alpha. J.Neurosci. 25, 3219.
Sheng, H., Wang, H., Homi, H.M., Spasojevic, I., Batinic-Haberle, I., Pearlstein, R.D.,Warner, D.S., 2004. A no-laminectomy spinal cord compression injury model inmice. J. Neurotrauma 21, 595.
Takahashi, J.L., Giuliani, F., Power, C., Imai, Y., Yong, V.W., 2003. Interleukin-1betapromotes oligodendrocyte death through glutamate excitotoxicity. Ann. Neurol.53, 588.
Trivedi, A., Olivas, A.D., Noble-Haeusslein, L.J., 2006. Inflammation and spinal cordinjury: infiltrating leukocytes as determinants of injury and repair processes.Clin. Neurosci. Res. 6, 283.
Teeling, J.L., Cunningham, C., Newman, T.A., Perry, V.H., 2010. The effect ofnon-steroidal anti-inflammatory agents on behavioural changes and cytokineproduction following systemic inflammation: implications for a role of COX-1.Brain Behav. Immun. 24, 409.
Tracey, K.J., Lowry, S.F., 1990. The role of cytokine mediators in septic shock. Adv.Surg. 23, 21.
Wajant, H., Pfizenmaier, K., Scheurich, P., 2003. Tumor necrosis factor signaling. CellDeath Differ. 10, 45.
Zhao, P., Leonoudakis, D., Abood, M.E., Beattie, E.C., 2010. Cannabinoid receptor acti-
receptors and excitotoxicity. Neuropharmacology 58, 551.Zhou, Q.H., Sumbria, R., Hui, E.K., Lu, J.Z., Boado, R.J., Pardridge, W.M., 2011. Neuro-
protection with a brain-penetrating biologic tumor necrosis factor inhibitor. J.Pharmacol. Exp. Ther. 339, 618.