Lecture 6 II. Non-receptor Mechanisms. Direct Physical blocking of channel local anesthetic &...
14
Lecture 6 II. Non-receptor Mechanisms
Transcript of Lecture 6 II. Non-receptor Mechanisms. Direct Physical blocking of channel local anesthetic &...
Lecture 6II. Non-receptor Mechanisms
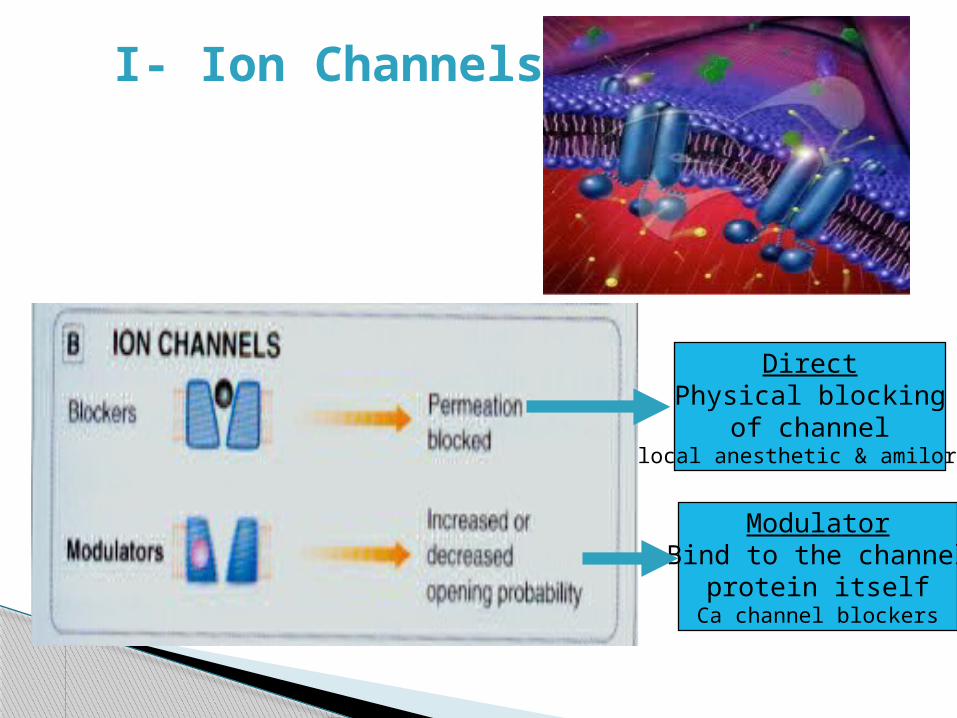
I- Ion Channels
DirectPhysical blocking
of channel local anesthetic & amiloride
ModulatorBind to the channel
protein itselfCa channel blockers
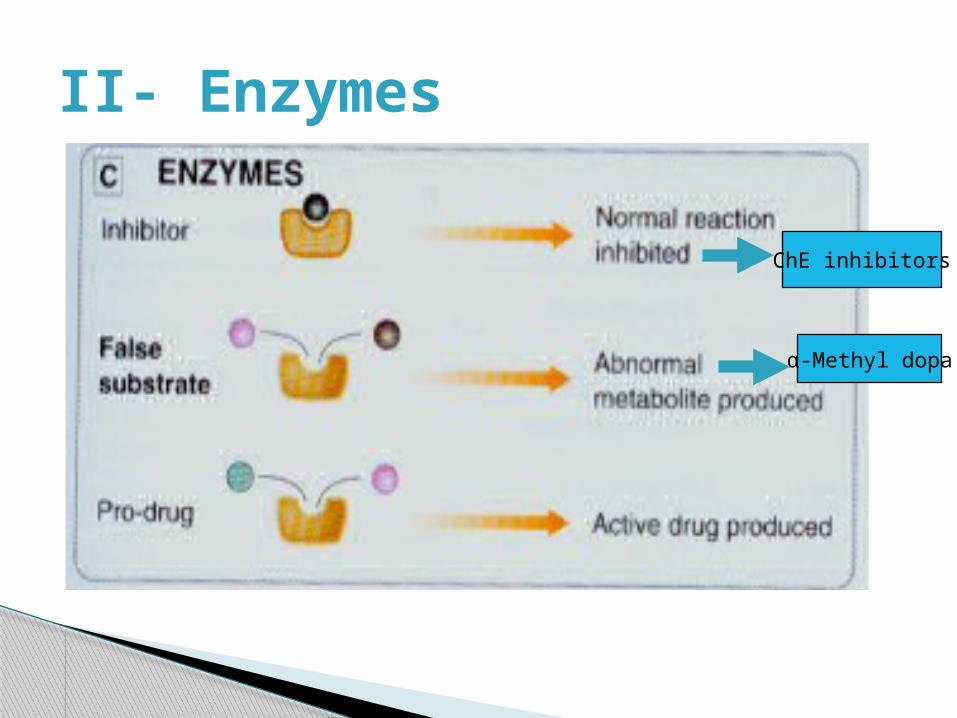
II- Enzymes
ChE inhibitors
α-Methyl dopa
II- Enzymes (cont.)
Drug acts as
Substrate leading to reversible OR irreversible inhibition of enzymereversible inhibition of cholinesterase by
neostigmine Irreversible inhibition of cyclo-oxygenase by aspirin
True/False substrateL-DOPA converted into dopamine α-methyldopa converted into α-
methylnorepinephrine (false transmitter)
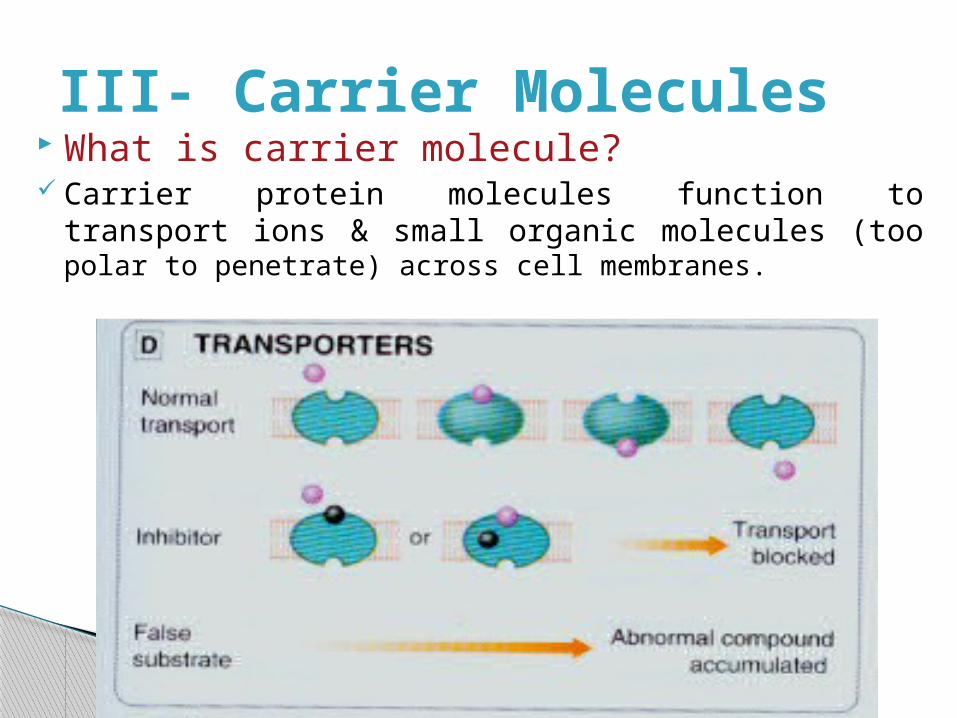
III- Carrier Molecules What is carrier molecule? Carrier protein molecules function to transport ions & small
organic molecules (too polar to penetrate) across cell membranes.
III- Carrier Molecules
They possess a recognition site that confers specificity for a particular carried agent.
Such recognition sites can be targets for drugs where they block the transport system.
An example is the inhibition of cardiac Na+K+-ATPase by cardiac glycosides.

IV- Extracellular Sites of Drug Action Stomach: neutralize acid with base
(antacids) Blood: bind metals (chelation) like lead
with EDTA GI Tract: bind drugs (adsorption) with
Cholestyramine. GI Tract: increase water by osmotic
effects (laxatives) Kidney: increase water elimination
(osmotic diuretics)
V- Anti-metabolitesAn anti-metabolite is a chemical with a similar structure to a
substance (a metabolite) required for normal biochemical reactions, yet different enough to interfere with the normal functions of cells, including cell division
Examples: Anti-neoplastics e.g., 5-FU (5-fluorouracil) inhibits DNA and RNA
synthesis Antimicrobials such as sulfonamide drugs, which inhibit
dihydrofolate synthesis in bacteria by competing with para-aminobenzoic acid (PABA)
Allergy: antigen-antibody………unpredictable
Idiosyncrasy: genetic abnormality…….. Unpredictable
Side effects: unavoidable, undesirable, normal actions by therapeutic doses.
Over-dose: high dose of drugs
Supersenstivity: exaggerated response to normal dose due to upregulation of receptors.
Dependance: habituation and addiction.
Adverse effects of drugs
Desensitization and Tachyphylaxis
tachyphylaxis ◦ When it is developing in the course of few
minutes.
Tolerance ◦ To describe a more gradual loss of drug-induced
clinical effects that develops in the course of days or weeks.
Refractoriness ◦ Used to indicate the loss of therapeutic response.
Drug resistance ◦ Describes the loss of the effect of antitumor and
antimicrobial drugs
Mechanisms of Desensitization
Receptor phosphorylation◦ Usually by phosphorylating serine or threonine residues
in the C-terminal domain of GPCRs leading to reduce efficiency and alter their binding affinity.
Down-regulation of receptors
◦ Phosphorylation also signals the cell to internalize the membrane receptor leading to decrease the number of receptors on the cell membrane.
◦ In contrast, continuous or repeated exposure to antagonists initially can increase the response of the receptor (supersensitivity or up-regulation)
Mechanisms of Desensitization
Depletion of mediators◦ Drugs acting indirectly via transmitter release can cause
depletion of that transmitter and hence loss of action e.g. amphetamine or ephedrine act by releasing catecholamines from nerve terminals.
Pharmacokinetic desensitization◦ Drugs which stimulate hepatic metabolism may enhance
their own metabolism and hence a lower plasma concentration with repeated administration of the same dose e.g. barbiturates
Pumping of drugs out from intracellular site (chemotherapy)
Via p-glycoprotein
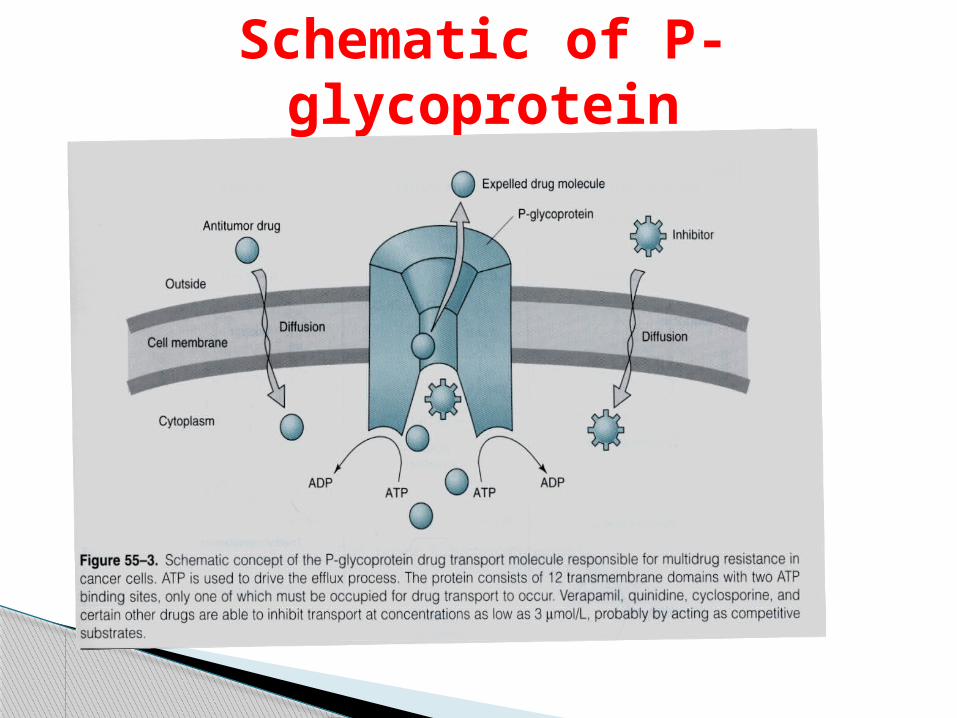
Schematic of P-glycoprotein

![[TI] SINGLE P-CHANNEL ENHANCEMENT-MODE MOSFETS.PDF](https://static.fdocument.org/doc/165x107/55cf8ec3550346703b95588a/ti-single-p-channel-enhancement-mode-mosfetspdf.jpg)