Lack of a Therapeutic Role for Interferon in Patients With Tuberculosis
3
0 MONTH Correspondence Lack of a Therapeutic Role for Interferon γ in Patients With Tuberculosis TO THE EDITOR—I read with interest the recent article by Wong and Jacobs on the effects of interferon γ (IFN-γ) on Myco- bacterium tuberculosis–infected macro- phages [1]. I believe their findings are an important contribution to our under- standing of the human biology of M. tu- berculosis infection. However, I must take issue with their speculation that their work is likely to enable future therapeutic trials of IFN-γ for tuberculosis. As the authors noted, the first trial of therapeutic IFN-γ in patients with tuber- culosis without overt defects in IFN-γ production or responsiveness was report- ed by Condos et al in 1997 [2]. In that un- controlled study, aerosolized IFN-γ 500 μg thrice weekly was added to the current therapy for 5 patients with multidrug-resis- tant tuberculosis. The study found that results of sputum smears became negative and that the number of colony-forming units tended to decrease. However, none of 2 small uncontrolled and 2 adequately powered controlled subsequent trials has been successful in replicating those results (Table 1). The most rigorous trial, con- ducted by InterMune, compared aerosol- ized IFN-γ 500 μg thrice weekly for 6 months to placebo in 80 patients with multidrug-resistant tuberculosis, all of whom also received standardized therapy with second-line drugs [6]. The study design included an aerosolized placebo. The study was halted prematurely by its external safety monitoring board because of a trend toward increased mortality in the experimental arm (10 deaths, com- pared with 5 in the control arm; P = .14), with no beneficial effect on sputum smear or culture results or chest radiography findings. The study findings have never been formally published but are described in an online supplement that accompanies the article by Dawson et al [5]. The only published randomized con- trolled trial of adjunctive IFN-γ in tuber- culosis compared the effects of standard therapy plus IFN-γ 200 μg given thrice weekly for 4 months by aerosol or by subcutaneous injection with the effects of standard therapy alone in 77 evaluable patients with drug-susceptible pulmo- nary tuberculosis [5]. All subjects also re- ceived standard 4-drug tuberculosis therapy. The study design did not include a subcutaneous or aerosolized placebo. The analysis of the study’s primary end points (ie, times to sputum smear and culture conversion) as it was reported dif- fered from that described in the study’s statistical analysis plan, because results of the subcutaneous IFN-γ and control arms were merged and because the planned intent-to-treat analysis was abandoned. Sputum smear findings were reported out to 120 days. A transient beneficial effect of aerosolized treatment on sputum smear results was noted at 4 weeks, but it was absent at all subsequent time points. A sputum culture conversion rate of 32% was reported at 4 weeks in the aerosol- ized IFN-γ arm, compared with 18% in the other arms combined (P = .15), but no subsequent data were provided. Spu- tum culture status at 2 months has recog- nized prognostic value in the evaluation of new tuberculosis regimens [7]. In con- trast, sputum smear has no recognized prognostic value, nor does any sputum parameter at 1 month [8, 9]. Subsequent research has found that most IFN-γ–induced genes are already upregulated in the lung during tubercu- losis and that therapeutic aerosolized IFN-γ has relatively little additional effect [10]. These findings indicate it is very un- likely that IFN-γ will have any future therapeutic role in patients with tubercu- losis without overt defects in its produc- tion. Note Potential conflict of interest. Author certi- fies no potential conflicts of interest. The author has submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Con- flicts that the editors consider relevant to the content of the manuscript have been disclosed. Robert S. Wallis Old Lyme, Connecticut References 1. Wong KW, Jacobs WR Jr. Mycobacterium tu- berculosis exploits human interferon γ to stimulate macrophage extracellular trap for- mation and necrosis. J Infect Dis 2013; 208: 109–19. 2. Condos R, Rom WN, Schluger NW. Treat- ment of multidrug-resistant pulmonary tu- berculosis with interferon-gamma via aerosol. Lancet 1997; 349:1513–5. 3. Suarez-Mendez R, Garcia-Garcia I, Fernan- dez-Olivera N, et al. Adjuvant interferon gamma in patients with drug-resistant pulmo- nary tuberculosis: a pilot study. BMC Infect Dis 2004; 4:44. 4. Koh WJ, Kwon OJ, Suh GY, et al. Six-month therapy with aerosolized interferon-gamma for refractory multidrug-resistant pulmonary tuberculosis. J Korean Med Sci 2004; 19:167–71. 5. Dawson R, Condos R, Tse D, et al. Immuno- modulation with recombinant interferon- gamma1b in pulmonary tuberculosis. PLoS One 2009; 4:e6984. 6. InterMune enrolls first patient in phase III trial in multidrug-resistant tuberculosis. Business Wire. 2000. http://www.thefreelibrary. com/InterMune+Enrolls+First+Patient+in +Phase+III+Trial+in...-a063778269. Accessed 22 October 2013. 7. Wallis RS, Wang C, Doherty TM, et al. Bio- markers for tuberculosis disease activity, CORRESPONDENCE • JID • 1 Journal of Infectious Diseases Advance Access published November 11, 2013 at Belgorod State University on December 5, 2013 http://jid.oxfordjournals.org/ Downloaded from
Transcript of Lack of a Therapeutic Role for Interferon in Patients With Tuberculosis

0 M O N T H
CorrespondenceLack of a Therapeutic Role forInterferon γ in Patients WithTuberculosis
TO THE EDITOR—I read with interest therecent article by Wong and Jacobs on theeffects of interferon γ (IFN-γ) on Myco-bacterium tuberculosis–infected macro-phages [1]. I believe their findings are animportant contribution to our under-standing of the human biology of M. tu-berculosis infection. However, I must takeissue with their speculation that theirwork is likely to enable future therapeutictrials of IFN-γ for tuberculosis.
As the authors noted, the first trial oftherapeutic IFN-γ in patients with tuber-culosis without overt defects in IFN-γproduction or responsiveness was report-ed by Condos et al in 1997 [2]. In that un-controlled study, aerosolized IFN-γ 500µg thrice weekly was added to the currenttherapy for 5 patients with multidrug-resis-tant tuberculosis. The study found thatresults of sputum smears became negativeand that the number of colony-formingunits tended to decrease. However, noneof 2 small uncontrolled and 2 adequatelypowered controlled subsequent trials hasbeen successful in replicating those results(Table 1). The most rigorous trial, con-ducted by InterMune, compared aerosol-ized IFN-γ 500 µg thrice weekly for 6months to placebo in 80 patients withmultidrug-resistant tuberculosis, all ofwhom also received standardized therapywith second-line drugs [6]. The studydesign included an aerosolized placebo.The study was halted prematurely by itsexternal safety monitoring board becauseof a trend toward increased mortality inthe experimental arm (10 deaths, com-pared with 5 in the control arm; P = .14),with no beneficial effect on sputum smearor culture results or chest radiography
findings. The study findings have neverbeen formally published but are describedin an online supplement that accompaniesthe article by Dawson et al [5].The only published randomized con-
trolled trial of adjunctive IFN-γ in tuber-culosis compared the effects of standardtherapy plus IFN-γ 200 µg given thriceweekly for 4 months by aerosol or bysubcutaneous injection with the effects ofstandard therapy alone in 77 evaluablepatients with drug-susceptible pulmo-nary tuberculosis [5]. All subjects also re-ceived standard 4-drug tuberculosistherapy. The study design did not includea subcutaneous or aerosolized placebo.The analysis of the study’s primary endpoints (ie, times to sputum smear andculture conversion) as it was reported dif-fered from that described in the study’sstatistical analysis plan, because results ofthe subcutaneous IFN-γ and control armswere merged and because the plannedintent-to-treat analysis was abandoned.Sputum smear findings were reportedout to 120 days. A transient beneficialeffect of aerosolized treatment on sputumsmear results was noted at 4 weeks, but itwas absent at all subsequent time points.A sputum culture conversion rate of 32%was reported at 4 weeks in the aerosol-ized IFN-γ arm, compared with 18% inthe other arms combined (P = .15), butno subsequent data were provided. Spu-tum culture status at 2 months has recog-nized prognostic value in the evaluationof new tuberculosis regimens [7]. In con-trast, sputum smear has no recognizedprognostic value, nor does any sputumparameter at 1 month [8, 9].Subsequent research has found that
most IFN-γ–induced genes are alreadyupregulated in the lung during tubercu-losis and that therapeutic aerosolized
IFN-γ has relatively little additional effect[10]. These findings indicate it is very un-likely that IFN-γ will have any futuretherapeutic role in patients with tubercu-losis without overt defects in its produc-tion.
Note
Potential conflict of interest. Author certi-fies no potential conflicts of interest.The author has submitted the ICMJE Form for
Disclosure of Potential Conflicts of Interest. Con-flicts that the editors consider relevant to thecontent of the manuscript have been disclosed.
Robert S. Wallis
Old Lyme, Connecticut
References
1. Wong KW, Jacobs WR Jr.Mycobacterium tu-berculosis exploits human interferon γ tostimulate macrophage extracellular trap for-mation and necrosis. J Infect Dis 2013; 208:109–19.
2. Condos R, Rom WN, Schluger NW. Treat-ment of multidrug-resistant pulmonary tu-berculosis with interferon-gamma via aerosol.Lancet 1997; 349:1513–5.
3. Suarez-Mendez R, Garcia-Garcia I, Fernan-dez-Olivera N, et al. Adjuvant interferongamma in patients with drug-resistant pulmo-nary tuberculosis: a pilot study. BMC InfectDis 2004; 4:44.
4. Koh WJ, Kwon OJ, Suh GY, et al. Six-monththerapy with aerosolized interferon-gammafor refractory multidrug-resistant pulmonarytuberculosis. J Korean Med Sci 2004;19:167–71.
5. Dawson R, Condos R, Tse D, et al. Immuno-modulation with recombinant interferon-gamma1b in pulmonary tuberculosis. PLoSOne 2009; 4:e6984.
6. InterMune enrolls first patient in phase IIItrial in multidrug-resistant tuberculosis.Business Wire. 2000. http://www.thefreelibrary.com/InterMune+Enrolls+First+Patient+in+Phase+III+Trial+in...-a063778269. Accessed22 October 2013.
7. Wallis RS, Wang C, Doherty TM, et al. Bio-markers for tuberculosis disease activity,
CORRESPONDENCE • JID • 1
Journal of Infectious Diseases Advance Access published November 11, 2013 at B
elgorod State University on D
ecember 5, 2013
http://jid.oxfordjournals.org/D
ownloaded from
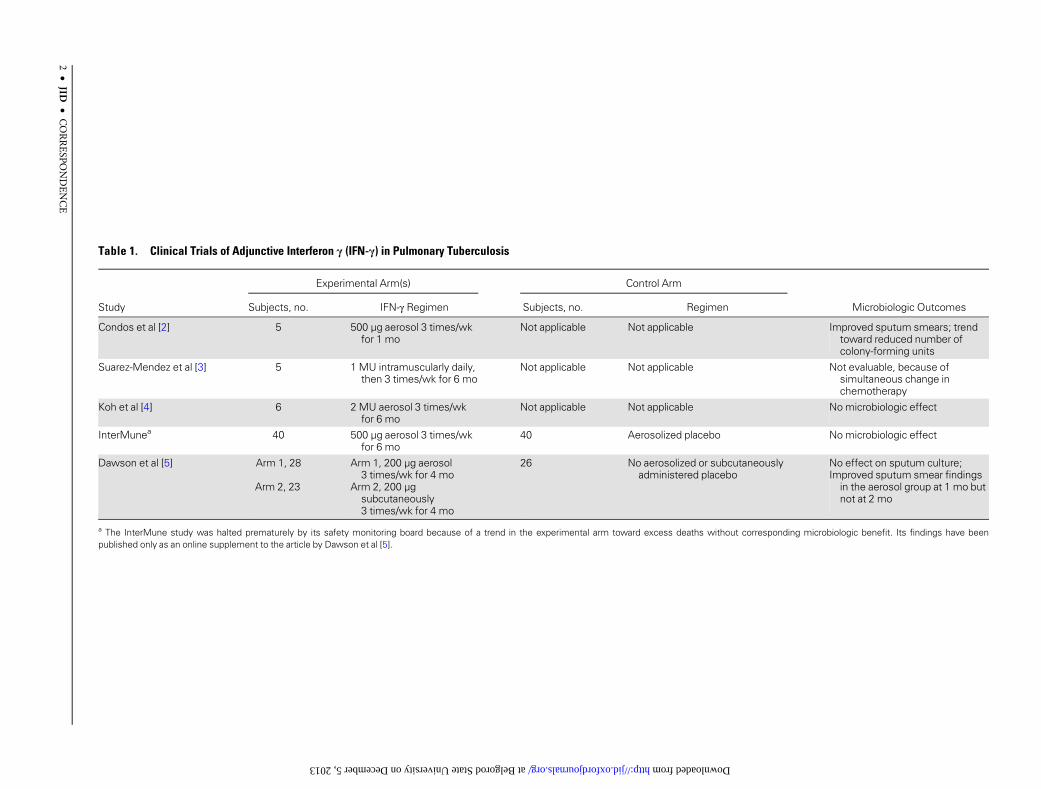
Table 1. Clinical Trials of Adjunctive Interferon γ (IFN-γ) in Pulmonary Tuberculosis
Study
Experimental Arm(s) Control Arm
Microbiologic OutcomesSubjects, no. IFN-γ Regimen Subjects, no. Regimen
Condos et al [2] 5 500 µg aerosol 3 times/wkfor 1 mo
Not applicable Not applicable Improved sputum smears; trendtoward reduced number ofcolony-forming units
Suarez-Mendez et al [3] 5 1 MU intramuscularly daily,then 3 times/wk for 6 mo
Not applicable Not applicable Not evaluable, because ofsimultaneous change inchemotherapy
Koh et al [4] 6 2 MU aerosol 3 times/wkfor 6 mo
Not applicable Not applicable No microbiologic effect
InterMunea 40 500 µg aerosol 3 times/wkfor 6 mo
40 Aerosolized placebo No microbiologic effect
Dawson et al [5] Arm 1, 28
Arm 2, 23
Arm 1, 200 µg aerosol3 times/wk for 4 mo
Arm 2, 200 µgsubcutaneously3 times/wk for 4 mo
26 No aerosolized or subcutaneouslyadministered placebo
No effect on sputum culture;Improved sputum smear findingsin the aerosol group at 1 mo butnot at 2 mo
a The InterMune study was halted prematurely by its safety monitoring board because of a trend in the experimental arm toward excess deaths without corresponding microbiologic benefit. Its findings have beenpublished only as an online supplement to the article by Dawson et al [5].
2•
JID•
CORRESPO
NDENCE
at Belgorod State University on December 5, 2013 http://jid.oxfordjournals.org/ Downloaded from

cure, and relapse. Lancet Infect Dis 2010; 10:68–9.
8. Horne DJ, Royce SE, Gooze L, et al. Sputummonitoring during tuberculosis treatmentfor predicting outcome: a systematic reviewand meta-analysis. Lancet Infect Dis 2010;10:387–94.
9. Phillips PP, Fielding K, Nunn AJ. An evalua-tion of culture results during treatment for
tuberculosis as surrogate endpoints for treat-ment failure and relapse. PLoS One 2013; 8:e63840.
10. Raju B, Hoshino Y, Kuwabara K, et al. Aerosol-ized gamma interferon (IFN-gamma) inducesexpression of the genes encoding the IFN-gamma-inducible 10-kilodalton protein but notinduciblenitricoxidesynthaseinthelungduringtuberculosis. Infect Immun 2004; 72:1275–83.
Received 23 June 2013; accepted 3 September 2013.Correspondence: Robert S. Wallis, MD, FIDSA (rswallis@
gmail.com).
The Journal of Infectious Diseases© The Author 2013. Published by Oxford University Presson behalf of the Infectious Diseases Society of America. Allrights reserved. For Permissions, please e-mail: [email protected]: 10.1093/infdis/jit555
CORRESPONDENCE • JID • 3
at Belgorod State U
niversity on Decem
ber 5, 2013http://jid.oxfordjournals.org/
Dow
nloaded from