INTERFERON-α PLUS RIBAVIRIN COMBINATION...
22
ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ ـــ* Correspondence Author (e mail: [email protected]) 132 The Egyptian Journal of Biochemistry & Molecular Biology VOL 32 (N.2) 132-153 December. 2014 PREDICATIVE FACTORS FOR PEGYLATED INTERFERON-α PLUS RIBAVIRIN COMBINATION THERAPY IN EGYPTIAN PATIENTS WITH CHRONIC HEPATITIS CINFECTED WITH GENOTYPE 4 SaraMohamed Massoud 1 , Mohamed Abbas Shemis 2 , Ehab Aly Drees 1* , Mamdoh Ahmed Taha 3 , Hanan Abdelmoniem Omar 2 , Mohamed Ali Saber 2 1 DIVISION OF BIOCHEMISTRY, DEPARTMENT OF CHEMISTRY, FACULTY OF SCIENCE, FAYOUM UNIVERSITY, FAYOUM, EGYPT; 2 DEPARTMENT OF MOLECULAR BIOLOG , THEODOR BILHARZ RESEARCH INSTITUTE, GIZA, EGYPT; 3 DEPARTMENT OF CHEMISTRY, FACULTY OF SCIENCE, FAYOUM UNIVERSITY, FAYOUM, EGYPT Received 25/6/2014– Accepted 13/10/2014 ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ ـــــــــــــــــABSTRACT Background:Hepatitis C virus genotype 4 is a common infection in Egypt and is the leading cause of liver disease. Most reports suggest that predicative factors for the efficacy of interferon α and ribavirincombination therapy for chronic hepatitis patients could be due to the mutations in the interferon sensitivity determining region. Aim:The present study aimed to investigate the predictive factors for combined pegylated interferon-αand ribavirin therapy for chronic hepatitis patients with HCV genotype 4. Methods:The study was carried out on forty patients with genotype 4 chronic hepatitis C receiving a weekly dose of 180 µg of PEG -IFN-α in combination with RBV for 48 weeks.HCV RNA serumviremialevels were determined by a real–time polymerase chain reaction. The RNA samples were genotyped using specific primers for HCV genotype 4, and the interferon sensitivity determining region was amplified using polymerase chain reaction and sequenced. The amino acid sequence of the ISDR was compared with the published sequence for HCV 4 (GenBank: ABD75831.1).
Transcript of INTERFERON-α PLUS RIBAVIRIN COMBINATION...

ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ * Correspondence Author (e mail: [email protected]) 132
The Egyptian Journal of Biochemistry & Molecular Biology VOL 32 (N.2) 132-153 December. 2014
PREDICATIVE FACTORS FOR PEGYLATED INTERFERON-α PLUS RIBAVIRIN COMBINATION
THERAPY IN EGYPTIAN PATIENTS WITH CHRONIC HEPATITIS CINFECTED WITH GENOTYPE 4
SaraMohamed Massoud1, Mohamed Abbas Shemis2, Ehab Aly Drees1*, Mamdoh Ahmed Taha3, Hanan Abdelmoniem
Omar2, Mohamed Ali Saber2
1DIVISION OF BIOCHEMISTRY, DEPARTMENT OF CHEMISTRY, FACULTY OF SCIENCE, FAYOUM UNIVERSITY, FAYOUM, EGYPT; 2DEPARTMENT OF MOLECULAR BIOLOG
, THEODOR BILHARZ RESEARCH INSTITUTE, GIZA, EGYPT; 3
DEPARTMENT OF CHEMISTRY, FACULTY OF SCIENCE, FAYOUM UNIVERSITY, FAYOUM, EGYPT
Received 25/6/2014– Accepted 13/10/2014 ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ABSTRACT
Background:Hepatitis C virus genotype 4 is a common infection in Egypt and is the leading cause of liver disease. Most reports suggest that predicative factors for the efficacy of interferon α and ribavirincombination therapy for chronic hepatitis patients could be due to the mutations in the interferon sensitivity determining region. Aim:The present study aimed to investigate the predictive factors for combined pegylated interferon-αand ribavirin therapy for chronic hepatitis patients with HCV genotype 4. Methods:The study was carried out on forty patients with genotype 4 chronic hepatitis C receiving a weekly dose of 180 µg of PEG -IFN-α in combination with RBV for 48 weeks.HCV RNA serumviremialevels were determined by a real–time polymerase chain reaction. The RNA samples were genotyped using specific primers for HCV genotype 4, and the interferon sensitivity determining region was amplified using polymerase chain reaction and sequenced. The amino acid sequence of the ISDR was compared with the published sequence for HCV 4 (GenBank: ABD75831.1).

PREDICATIVE FACTORS FOR PEGYLATED ……..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
133
Results: Our datarevealed that twenty one patients were responders (R; 52.2%), whereas 19 patients showed no-response (NR; 47.5%) to the combined pegylated interferon–α plus ribavirintherapy. The values of RNA titer in both responder and non-responder groups were statistically significantand could be used a predictive factor for combined pegylated interferon –α plus ribavirin efficacy. Other factors, such as gender, age, and interferon sensitivity determining region subtype were not related to its efficacy. Conclusion: These data collectively suggest that HCV RNA titer is an important factor for predicting the efficacy of pegylated interferon –α plus ribavirin combination therapy in Egyptian patients with chronic HCV genotype 4.
Keywords: Hepatitis C virus -4;Pegylated Interferon-α; Ribavirin;Interferon sensitivity determining region
INTRODUCTION
Chronic hepatitis C virus (HCV) infection affects approximately 300 million people worldwide and is the most common cause of chronic liver disease (DI Bisceglie, 1998).HCV is considered the leading cause of liver cirrhosis and hepatocellular carcinoma (HCC). It has been estimated to cause approximately 27% of cirrhosis and 25% HCC cases worldwide (Alter, 2007). Each year about 350, 000 people die due to HCV (Hatzakis et al., 2011).At least seven major HCV genotypes and subtypes have been identified, and each one differs from the others by 30-35% of its nucleotide site sequence(Hnatyszyan, 2005; Sharma, 2010). HCV genotype-4 (HCV-4) is common in the Middle East and Africa, and has recently spread to several European countries (Nguyen and Keefe, 2005). Egypt has one of the highest rates of HCV worldwide (~15%) and the highest prevalence of HCV-4, which is responsible for nearly 90% of all HCV cases(Asselah et al., 2012; Zekri et al., 2009). This particular genotype was considered difficult to treat with the combination of conventional IFN and ribavirin (RBV) (El-Zayadi et al.,1996; Elzaydi et al.,1999; Kamal et al., 2000; Koshy et al., 2000). Presently, the standard treatment for patients with chronic hepatitis C (CHC) consists of pegylated interferon (PEG-IFN) α-2a or α-2bplus RBV(Manns et al., 2001; Aman et al., 2012).Since then, significant accomplishments have been achieved in the treatment of

SaraMohamed Massoud et all..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
134
HCV-4 using PEG-IFN/RBV combination therapy. Several reports show that the combination of PEG-IFN with RBV markedly improved therapeutic outcomes, resulting in sustaining virologic response (SVR) rates ranging between 44% and 69% in Egyptian patients infected with HCV genotype 4 (Alfaleh et al., 2004; Hasan et al., 2004; El-Zayadi et al., 2005; Kamal et al., 2005). Previously, it has been suggested that different responses among patients with HCV genotypes and subtypes suggest that viral genetic heterogeneity may affect at least to some extent, the sensitivity to IFN- dependent therapy. In this context, sequence heterogeneity of the viral nonstructural protein 5A(NS5A) has been widely discussed with IFN responsiveness. In the era of IFN therapy alone, it was proposed that sequence variations within a region in NS5A of HCV-1b defined as the IFN sensitivity determining region (ISDR) are associated with IFN responsiveness (Enomoto et al., 1996). It is worth noting that the correlation between ISDR mutations and response to PEG-IFN-α plus RBV therapy in patients infected with HCV genotypes 1b and 2b were documented in previous studies (Yen et al., 2008; Kadokura et al., 2011). We therefore analyzed the predictive factors for combined Peg-IFN-α and RBV therapy in Egyptian patients with HCV genotype 4. To identify these factors, we investigated the relationship between combined Peg-IFN-α and RBV efficacy and a variety of factors such as ISDR sequence, age, gender, and HCV RNA titer in Egyptian patients infected with HCV genotype 4.
MATERIALS ANDMETHODS Subjects This study was carried on 40 patients seen at Theodor Bilharz Research Institute who were chronically infected with HCV infection were enrolled in the study. The study protocol was approved beforehand by the Ethics Committee in Theodor Bilharz Research Institute, and informed consent was obtained from each patient prior to the treatment. Patients were treated with IFN-α and RBV according to the standard regime of treatment. In general, for patients with HCV genotype 4 infection, combination treatment with PEG-IFN plus weight based RBV administered for 48 weeks appears to be the optimal regimen (Khuroo et al., 2004). Two PEG-IFNs are available; PEG-IFN α-2b (PEG-Intron®, Merck, Germany) and PEG-IFN α-2a (PEGASYS®, Roche, Germany) (Ascione et al., 2010; Rumi et al.,

PREDICATIVE FACTORS FOR PEGYLATED ……..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
135
2010). PEG-IFNα-2a is administered at a fixed dose of 180 µg/week given subcutaneously. RBV administered orally according to the bodyweight of the patient (about 1000 mg for those who weigh ≤75 kg and 1200 mg for those who weigh >75 kg, daily)(Fried et al., 2002). Serum samples were collected from the patients at intervals of 4 weeks before, during and after the treatment, and tested for HCV RNA titer according to Ghany et al., 2009. After the completion of the combination therapy, the patients were classified into two groups according to their responses to the combination therapy: Group A responders (14 males and 7 females). Their mean ages were (44.26± 8.67years) and HCV titerin the blood sample wasnegative at the end of the treatment period (week 48) and ALT levels were within the normal range; andGroup Bnon-responders (15 males and 4 females). Their mean ages were (47.62±8.01years) and HCV RNA titer was over 50 IU/ml even if ALT levels were normal. RNA extraction and quantitation HCV RNA was extracted from each serum using a commercially available RNA extraction kit(Abbott Molecular Inc., USA) following the manufacturer’s protocol.The HCV-RNA was quantitatively determined in serum before and after treatment using Abbott Real-Time HCV kit (Abbott Molecular Inc., USA) following the manufacturer’s protocol. HCV genotyping This study was carried out on patients infected with HCV genotype 4 as it is the predominant genotype in Egypt. For this purpose genotyping was done to determine the genotype of the virus and genotypes other than 4 were excluded. The genotyping protocol was reported by Shemis et al., 2012 which based on modification of nested PCR carried out by Idrees, 2008.Briefly, cDNA synthesis and First-Round PCR amplification were performed in a 50 µL reaction volume containing 20 µLRNA, 50 pmol of each of the following specific primers [All primers used in this study were manufactured and obtained from the Midland Certified Reagent Company Inc., Texas, USA](Forward :5’-TTG TGG TAC TGC CTG ATA GGG-3’ andReverse 5’-GGA TGT ACC CCA TGA GGA TCG-3’ for first PCR run), 200 µM of each deoxyribonucleotide triphosphate (dNTP)(Fermetas, Canada), 10 U of avian myeloblastosis virus reverse transcriptase (AMV RT) (Finnzymes, Finland), 2.5 U of Taq DNA polymerase (Promega, USA), 40 U of RNAsin (Promega, USA),

SaraMohamed Massoud et all..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
136
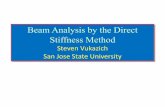
20 mM Tris-HCl (pH 8.4), and 50 mM KCl. Reaction was performed in a Bio-Rad thermal cycler (MJ Research, Inc. USA), programmed as follows:reverse transcription was performed at 42°C for 30 min and terminated at 95°C for 5 min, followed by the first-round PCR , 40 cycles of denaturation at 94°C for 1 min, annealing at 45°C for 1 min and extension at 72°C for 1 min, and final extension at 72°C for 5 minutes. The second round of nested PCR was performed according to Idrees, 2008, in which the following primers were used (Forward: 5’-GTG CCC CGG GAG GTC TCG TAG-3’ and Reverse: 5’-CCG TAA AGA GGC CAT GGA TA-3’). Tubes were placed into a thermal cycler that was programmed for 35 cycles as follows: 94°C for 45 sec, 50°C for 45 sec, 72°C for 1 min for 15 cycles, 94°C for 45 sec, 58°C for 45 sec, 72°C for 1 min for 20 cycles, and final extension at 72°C for 10 minutes.The final PCR products obtained after each round Nested PCR were subjected to electrophoresis and separated on 2% agarose gel. After staining with ethidium bromide, and the gel was visualized under UV-transilluminator. To determine genotype specific bands, the banding pattern was photographed using Canon G11 Powershot 11 Gel Documentation (Model PC1428 systems, Canon Inc., USA).One band observed at 288bp (Fig. 1). Amplification of ISDR cDNA synthesis and first PCR-Round were performed in a 50 µL reaction volume containing 25 µL RNA,10 pmol of each of the following specific primers(Forward: 5’-ATC TTG GCT ATG GGA GGT ATG GG-3’ andReverse: 5’-TGT CAC AGC AGA ACG GGT GGT C-3’for first PCR run) , 5 µL 10x PCR buffer , 25 mM MgCl2, 200 µM dNTPs, 1.25 unit Taq DNA polymerase (5u/µL), 15 units of reverse transcriptase (20u/µL), RNAsin (20u/µL)and sterile distilled water was added to a final volume of 50 µL. The reaction was done in a Bio-Rad thermal cycler programmed as follows: reverse transcription was performed at 42°C for 30 min and terminated at 95°C for 5 min, followed by the first-round PCR, 40 cycles of denaturation at 95°C for 1 min, annealing at 45°C for 1 min and extension at 72°C for 1 min, and final extension at 72°C for 5 minutes. Second-Round PCR was carried out in a total volume of 50 µL DNA template “1st PCR product”, 10 pmole of each of the following specific primers (Forward:5’-GTG GAG GTT CGC AGA GTG GG-3’ and Reverse 5’-GCG GTA GAA ACA ACG GAC TC-3’), 10x

PREDICATIVE FACTORS FOR PEGYLATED ……..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
137
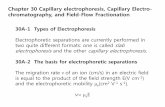
PCR buffer, 10 mM MgCl2, 10 mM dNTPs, and 1.25 units Taq DNA polymerase. The reaction was done in a Bio-Rad thermal cyclerprogrammed as follows: preheating at 95°C for 5 min, 35 cycles of 95°C for 45 sec, 53°C for 1 min, 72°C for 1 min, and final extension at 72°C for 10 minutes. DNA purification The nested RT-PCRproducts were loaded into 2 % agarose gel containing ethidium bromide and the DNA was extracted using GeneJET Gel extraction kit (Fermentas, Canada) following the manufacturer’s protocol which is modified of Vogelstein and Gillespie, 1979. The purified band was observed (~745bp) (Fig. 2) DNA sequencing of ISDR region The sequences of the amplified fragments were determined by direct sequencing without subcloning.Sequence reactions on PCR products were performed using BigDye Terminators Version 3.1 with Applied Biosystems 3730x1 DNA analyzer at MAcrogen, Inc. (Korea). To determine the order of nucleotides of the ISDR region, the sequencing of PCR product was done according to Sanger method (Sanger et al., 1977). The amino acid sequences were deduced and aligned using DNAMAN software version 4.1 and online NCBI Blast site. These sequences of the amplified fragments were aligned against Hepatitis C virus subtype 4a isolate L835 polyprotein gene, complete cds (GenBank: DQ418789.1) for DNA, and polyprotein [Hepatitis C virus subtype 4a] (GenBank: ABD75831.1) for protein (designated wild type in this study). The sequence data reported in this paper has been deposited in the GenBank nucleotide sequence databases with the accession number KF263686 (Fig. 3). Statistical Analysis Comparison between groups was made by the Students t-test. The P values were determined between the two groups with regard to age, gender, amino acid mutations in ISDR, and HCV RNA titer. P< 0.05 was considered statistically significant.
RESULTS
Characteristics ofpatients We collected serum from 40 patients, HCV genotype 4 infected patients. Among them, 21 patients (52.5%) completely responded (Group A) to the 48 weeks combination therapy, while 19 patients

SaraMohamed Massoud et all..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
138
(47.5%) showed no-response (Group B). The characteristics of each patient prior to combination therapy are shown in Tables1 and 2. HCV RNA quantitation As shown in Tables1 and 2, the HCV-RNA titer (expressed as a log of copies per milliliter) had a wide distribution. In the responder group, the HCV titer between 3.32-6.45, and 4.91-7.08, in the non-responder group. The average RNA titer of the responders and non-responders was 4.80 ± 0.98 and 6.06 ± 0.62, respectively. These values were statistically significant (P=0.001, Table 3). Response to combination therapy in different groups As shown in Table 3, there wasno statisticallysignificantdifference in age and gender between the two groups with the combination therapyeffectiveness (P=0. 211;P=0. 385, respectively). NS5A-ISDR amino acid sequences alignment and response to PEG-IFN plus RBV The ISDR amino acid sequence and HCV genotype 4a prototype sequence are shown in Fig. 4.The 40 patients NS5A-ISDR sequences were classified according to the criteria of Enomotoet al., 1996 into three groups based on the number of amino acid mutations. Our results showed that in the non- responders group i) 3 (15.8%) patients had HCV with wild-type ISDR (no amino acid mutations), ii) 3 (15.8%) had HCV with mutant-type ISDR (≥4 amino acid mutations) and iii) 13 (68.5%) patients had HCV with intermediate ISDR HCV-4 (1- 3 amino acid mutations). All responder patients had HCV-4 with intermediate–ISDR 21 (100%) (Table 4 and Fig.4). As seen in the sequence analysis of ISDR in all patients (Fig. 4), the responder group had 1-3 amino acid substitutions while the non-responder group had 1-6 amino acid substitutions in the ISDR.From these data, when the mean amino acid mutation in the ISDR region was determined, there was no a statistically significant difference between responders and non-responders (1.67±0.8 substitutions versus 1.95±1.58 substitutions, respectively; P=0. 491, Table 3) regarding to the effectiveness of PEG-IFN-α and RBV combination therapy in patients with HCV genotype 4.

PREDICATIVE FACTORS FOR PEGYLATED ……..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
139
Figure(1):Shows the agarose gel electrophoresis of PCR genotyping. Lane 1:positive control; lane 2:negative control; lanes 3, 5 and 7 indicate genotype 4 (288 bp); lanes 4 and 6: other genotypes; M: DNA ladder (50 bp).
Figure (2):Shows agarose gel electrophoresis of the purified RT-PCR products of samples after gel cleans up. M: DNA ladder (50 bp); lanes from 1 to 16: sixteen different samples of HCV-patients included in this study; the molecular size of the purified band (~ 745bp). ATAACGGCGGAAACGGCCAGCCGGAGACTGGCTCGAGGGTCACCACCCTCATTAGCTAGTTCCTCGGCTAGCCAGCTATCCGCCCCGTCTCTCAAGGCCACATGCACCACTCGCCATGACCACCCTGGTACCGATCTCCTCGTGGCTAACCTTTTGTGGGGGTCCTCTGCTACCAGGATTGAGACAGACAAGAAGGTCATAATAATGGACTCTTTTGAGCCATGTGTGGCTGAACCAGA
Figure (3) Showsthe sequence data of hepatitis C virus strain B-20-NR-NS5A gene, partial coding sequence. The sequence has been deposited in the GenBank nucleotide sequence databases with the accession number KF263686.

SaraMohamed Massoud et all..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
140
Table 1:Demographic and ISDR characteristics of HCV-4-infected patients with complete response to the PEG-IFN-α plus RBV combination therapy.
Group A: Responders
Serial Age (Year)
Sex HCV RNA titera
ISDR Typeb
No. of amino acid mutations of ISDR
A-1 46 F 5.78 2 2
A-2 57 M 3.93 2 3
A-3 42 M 3.99 2 1
A-4 48 M 5.56 2 2
A-5 52 M 4.47 2 3
A-6 39 M 4.07 2 1
A-7 55 M 4.61 2 1
A-8 25 M 3.32 2 1
A-9 59 M 3.46 2 1
A-10 57 M 4.68 2 2
A-11 45 F 5.77 2 3
A-12 53 M 5.55 2 1
A-13 46 M 6.22 2 2
A-14 52 F 4.47 2 2
A-15 55 F 4.36 2 3
A-16 48 F 5.42 2 1
A-17 50 M 6.45 2 1
A-18 40 F 3.47 2 1
A-19 40 M 5.70 2 1
A-20 41 M 3.73 2 2
A-21 50 F 5.75 2 1 a the unit of HCV RNA titer before treatment (log copies /mL); b ISDR type: 1(wild type no amino acid substitution), 2 (intermediate type 1-3 amino acid substitutions), 3 (mutant type, ≥ 4 amino acid substitutions).

PREDICATIVE FACTORS FOR PEGYLATED ……..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
141
Table 2:Demographic and ISDR characteristics of HCV-4-infected patients with no- response to the PEG-IFN-α plus RBV combination therapy.
Group B:Non-Responders
Serial Age (year)
Sex Log RNA titera
ISDR Typeb
No. of amino acid mutations of ISDR
B-1 55 M 5.68 3 4
B-2 53 F 5.74 1 0
B-3 30 M 5.59 2 3
B-4 39 F 5.56 2 1
B-5 40 M 4.91 2 1
B-6 44 M 6.95 2 1
B-7 53 M 4.98 3 4
B-8 47 M 6.11 2 3
B-9 45 M 6.21 2 3
B-10 34 M 6.25 2 1
B-11 44 M 6.22 1 0
B-12 49 M 6.37 3 6
B-13 36 M 6.75 2 2
B-14 53 F 6.78 1 0
B-15 51 M 5.58 2 2
B-16 23 M 5.88 2 2
B-17 46 M 6.67 2 1
B-18 49 M 7.08 2 2
B-19 50 F 5.86 2 1 a the unit of HCV RNA titer before treatment (log copies /mL); bISDR type: 1(wild type no amino acid substitution), 2 (intermediate type 1-3 amino acid substitutions), 3 (mutant type, ≥ 4 amino acid substitutions).

SaraMohamed Massoud et all..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
142
Table 3:Main features of patients and predictive factors according to their responses to treatment.
Character All Responders Non- Responders
P-value*
Number of patients
40 (100%) 21(52.5%) 19(47.5%)
Age (years) Range (min.- max)
Mean ± SD
23-59 46.03 ± 8.4
25-59 44.26 ± 8.67
23-55 47.62 ± 8.01
0.211 (NS)
Gender Males Females
29 11
14(66.67%) 7 (33.33%)
15 (78.95%) 4 (21.05%)
0.385 (NS)
HCV RNA titer(Log copies/ml)
4.28 ± 1.75 4.80 ± 0.98 6.06 ± 0.62 0.001
Amino acid mutations in the ISDR
1.73 ± 1.11 1.67 ± 0.8 1.95 ± 1.58 0.491 (NS)
NS: non- significant; Values of quantitative variables are expressed as mean ±SD" standard deviation".*P value < 0.05 is considered statistically significant. Table 4:Comparison of baseline features in subgroup patients as divided by the types of ISDR mutations defined by Enomoto et al., (1996).
Patients All Wild-ISDR
Intermediate-ISDR
Mutant-ISDR
Number of patients a
40 7.5b(3/40) 85 (34/40) 7.5 (3/40)
Responders 21 0(0/21) 100 (21/21) 0 (0/21)
Non-responders
19 15.8(3/19) 68.4 (13/19) 15.8 (3/19)
a includes all 40 patients with HCV-4 infection (21 patients are responders and 19 patients are non-responders).bData expressed as percentage of patients with indicated response (number of patients /total number).

PREDICATIVE FACTORS FOR PEGYLATED ……..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
143
Sample No.
ISDR Type 2209 2248
Response to IFN
Prototype (HCV4a)
PSLKATCTARHDSPGTDLLEANLLWGSTATRVETDEKVII
Wild type B-2 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - NR B-11 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - NR B-14 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - NR Intermediate type A-1 - - - - - - - - - - - - - - - - - - - - - - - - - - -A- - - - - - N - - - - - R A-2 - - - - - - - - - - - E- - - - - - - - - - - - - - -A- - - - - - - D - - - - R A-3 - - - - - - - - - - - - - - - - - - - - - - - - - - -A- - - - - - - - - - - - R A-4 - - - - - - - - - - - - - - - - - - -D - - - - - - -A- - - - - - - - - - - - R A-5 - - - - - - - - D- -N - - - - - - - - - - - - - - -A- - - - - - - - - - - - R A-6 - - - - - - - - - - - - - - - - - - - - - - - - - - -A- - - - - - - - - - - - R A-7 - - - - - - - - - - - - - - - - - - - - - - - - - - -A- - - - - - - - - - - - R A-8 - - - - - - - - - - - - - - - - - - - - - - - - - - -A- - - - - - - - - - - - R A-9 - - - - - - - - - - - - - - - - - - - - - - - - - - -A- - - - - - - - - - - - R A-10 - - - - - - - - - - - - - - - - - - - - - - - - - - -NT- - - - - - - - - - - R A-11 - - - - - - - - -H - - - - - - - - - - - - - - - - - - - - - - - - - K- - M - R A-12 - - - - - - - - - - - - - - - - - - - - - - - - - - -A- - - - - - - - - - - - R A-13 - - - - - - - - - - - - - - - - - - - - - - - - - - -A- - - - - - N - - - - - R A-14 - - - - - - - - - - - - - - - - - - - - - - - - - - -A- - - - - - N - - - - - R A-15 - - - - - - - - D- -N - - - - - - - - - - - - - - -A- - - - - - - - - - - - R A-16 - - - - - - - - - - - - - - - - - - - - - - - - - - -A- - - - - - - - - - - - R A-17 - - - - - - - - - - - - - - - - - - - - - - - - - - -A- - - - - - - - - - - - R A-18 - - - - - - - - - - - - - - - - - - - - - - - - - - -A- - - - - - - - - - - - R A-19 - - - - - - - - - - - - - - - - - - - - - - - - - - -A- - - - - - - - - - - - R A-20 - - - - - - - - - - - - - - - - - - - - - - - - - - -A- - - - - - N - - - - - R A-21 - - - - - - - - - - - - - - - - - - - - - - - - - - -A- - - - - - - - - - - - R B-3 - - - - - - - - D- - A - - - - - - - - - - - - - - - S - - - - - - - - - - - - NR B-4 - - - - - - - - - - - - - - - - - - - - - - - - - - - S - - - - - - - - - - - - NR B-5 - - - - - - - - - - - - - - - - - - - - - - - - - - - S - - - - - - - - - - - - NR B-6 - - - - - - - - D- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - NR B-8 - - - - - - - - D- -N - - - - - - - - - - - - - - - A - - - - - - - - - - - - NR B-9 - - - - - - - - - - -E - - - - - - - - - - - - - - A - - - - - - - N - - - - - NR B-10 - - - - - - - - - - - - - - - - - - - - - - - - - - - A - - - - - - - - - - - - NR B-13 - - - - - - - - - - - - - - - - E- -D - - - - - - - - - - - - - - - - - - - - NR B-15 - - - - - - - - - - - - - - - - - - - - - - - - - - -A - - - - - -N - - - - - NR B-16 - - - - - - - - - - - - - - - - - - - - - - - - - - -A - - - - - -N - - - - - NR B-17 - - - - - - - - - - - - - - - - - - - - - - - - - - -A - - - - - - - - - - - - NR B-18 - - - - - - - - - - - - - - - - - - - - - - - - - - -A - - - - - -N - - - - - NR B-19 - - - - - - - - - - - - - - - - - - - - - - - - - - -A - - - - - - - - - - - - NR Mutant type B-1 - - - - - - - - - - - - - LS A - - - - - - - - - - - S - - - - - - - - - - - - NR B-7 - - - - - - - - - H - - - - - - - - - - - - - - - - - S - - - - - - - R - -M- NR B-12 - - - - - - - - T- - -H - - - - - -V - - - - - - - S - - - I - - - K- - - - NR
Figure (4): ISDR sequences (2209-2248 a.a.) of HCV alignment of all samples according to ISDR type.Amino acid (a.a.) residues are indicated by the standard single-letter codes; Dashes indicate the a.a. residues identical to the sequences on the first line; ISDR type: wild (identical to wild type, no a.a. substitution), intermediate (1-3 a.a. substitutions) and mutant (from 4 or more a.a.substitutions); R represents responders; NR represents non-responders.

SaraMohamed Massoud et all..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
144
DISCUSSION
It is known that viral and host genetic factors are involved in predicting the clinical response to PEG-IFN/RBV therapy for HCV infection (Kau et al., 2008). The response of HCV-4 to the standard regimen of treatment PEG-IFN-α plus RBV has diminished behind other genotypes and HCV-4 has become the most resistant genotype to treat (El-Shamy et al., 2012). As PEG-IFN-α /RBV still remains to be used to treat HCV-4 infected patients. In the present study, the experimental design was aimed to determine the factors that could be useful to predict the effectiveness of PEG-IFN-α and RBV combination therapy in chronically infected patients with genotype 4. Thus, we analyzed the relationship between the response to combination therapy and a variety of factors. The worth of HCV genotyping prior to therapy could provide important information towards the development of an individualized HCV treatment regimen (Guo et al., 2012). Therefore, as shown in the present study only patients infected with HCV-4 that examined by genotyping assay were studied because this genotype is known to be the most resistant genotype to PEG-IFN-α plus RBV and is the highest prevalence genotype of HCV in Egypt (Abdel-Aziz et al., 2000; Ray et al., 2000). This study detected a significant difference of serum pretreatment HCV RNA titer between responders and nonresponders to the combination therapy for HCV genotype 4 infection. On the other hand, our data revealed that age, gender and amino acid mutations in ISDR were not significantly associated with the combination therapy effectiveness.This finding suggests that HCV RNA titer but not ISDR subtype, age and gender, would be a useful marker for predicting the efficacy of PEG-IFN-α/RBV combination therapy for HCV genotype 4 infection among Egyptian patients. These results are consistent with many previous studies, but contrary to others (Bae et al., 2000; Aslan et al., 2004; Yoon et al., 2007; Yen et al., 2008; Nakagawa et al., 2010, Hayshi et al., 2011; Kurosaki et al, 2011). This conflict in the results demonstrates that gender, age, HCV RNA titer and ISDR mutations are not always precise useful markers for prediction of combination treatment outcome in patients infected with HCV (Yoon et al., 2007).This effect may be due to the pleiotropism of IFN

PREDICATIVE FACTORS FOR PEGYLATED ……..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
145
activity, in addition to cellular and viral genetic factors that modulate the efficacy of PEG-IFN-α plus RBV therapy for chronic HCV infection (Yoon et al., 2007; El-Shamy et al., 2012). Noteworthy, the present study may also reflect the genetic characteristics of Egyptian patients. Conflicting data have been stated for the relationship between amino acid mutations in the ISDR and response to the IFN-based therapy. Some studies demonstrated that the ISDR is a reliable predictor of the response to the IFN- therapy, in particular in regard to Japanese patients with a specific subtype of HCV 1b called (HCV-J) (Enomoto et al., 1996; Murayama et al., 2007; Watanabe et al., 2005), while similar correlations were not detected in studies conducted in Europe, the United States, Turkey and one Korean study(Zeuzem et al., 1997; Gerotto et al., 2000; Murphy et al., 2002; Aslan et al., 2004; Bae et al., 2000) which were in agreement with our present study, when considering ISDR 2209-2248 revealed that no a significant difference in the mutation number of amino acid was observed between responders and non-responders to the combined PEG-IFN-α plus RBV treatment. Worth mentioning thatEnomoto et al., (1996) found a significant association between ISDR mutations and the response to the IFN- treatment, when classifying patients into three groups: wild-type (no mutations), intermediate type (1 to 3 mutations), and mutant type (≥4 mutations). In our cases, only 7.5% of the patients were mutant type whereas 85% were intermediate type and 7.5% wild type and these results are in harmony with previous studies (Munoz de Rueda et al., 2008). As our results revealed the non significant association between amino acid mutations in the ISDR of both groups to the combination treatment. Nevertheless,a sequence analysis of the ISDR in 40 patients also found a small number of amino acid mutations in responder group (all 21 isolates)compared to non-responder group (13 out of 19 isolates). These data are supported by previous western reports stated that most patients with HCV-1 infection and sustained virologic response to the IFN-based therapy demonstrated only a small number of amino acid mutations (one to three) detectable within ISDR (Pawlostky et al., 1998; Saize et al., 1998; Sarrazin et al., 1999; Sarrazin et al., 2000; Witherell and Beineke, 2001).These findings suggest the possibility that HCV-4 infection, the combination therapy and the presence of more mutations of the ISDR in the non-responder

SaraMohamed Massoud et all..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
146
patients may have associated with considerable unfavorable treatment responses (Fried et al., 2002). Moreover, the response to PEG-IFN-α plus RBV therapy in Egyptian patients with HCV-4 may not be convincingly explained by ISDR to be a useful marker for prediction of treatment outcome in HCV-4 infection. Also, the lack of the correlation between ISDR mutations and complete response to the combination therapy may be attributed to an inadequate sample size. Hence, further large-scale studies are needed to determine why more mutations only occur in the non-responders group of HCV-infected patients in Egypt and also a need for improved alternative treatment regimens.On the contrary, Yen et al., 2008 reported thatISDR mutations as predictive were correlated withthe response to PEG-IFN-α2b plus RBV in the examined population of Taiwan patients infected with HCV-1b. Likewise, Nakagawa et al., 2010, found that the number of mutations in the ISDR of HCV-1b is the most effective parameter predicting a favorable clinical outcome of 48 weeks PEG-IFN/RBV therapy in Japanese patients infected with genotype 1b. Thus, the association between ISDR mutations and PEG-IFN-α2b plus RBV responsiveness in chronically infected patients with different genotypes of HCV remains a controversial issue (Herion and Hoofnagle, 1997; Brechot, 1999). Conclusion Our results demonstrated that no significant association exists between the number of amino acid mutations in ISDR, gender and age and response to PEG-IFN-α plus RBV therapy. Also, we have shown that pretreatment HCV RNA titer estimation is significantly considered the most potent predictive factor for combination therapy effectiveness in Egyptian chronic hepatitis patients with HCV genotype 4. The data shown in the present study also provide the possible predictive factors for PEG-IFN-α and RBV combination therapy in patients with HCV genotype 4 that could be used to select its candidates. ACKNOWLEDGEMENTS The authors would like to acknowledge all physicians at the hospital of Theodor Bilharz who follow up the patients, researchers and assistance staff at Theodor Bilharz Research Institute for technical support.This work was adopted from a M. Sc. Thesis by Sara Mohamed Massoud submitted to Fayoum University, Fayoum, Egypyt (2014).

PREDICATIVE FACTORS FOR PEGYLATED ……..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
147
REFERENCES Abdel-Aziz, F., Habib, M, Mohamed, M.K., Abdel-Hamid, M., Gamil, F., Madkour, S, Mikhail, N. N., Thomas, D., Fix, A. D., Strickland, G. T., Anwar, W.and Sallam, I.(2000): Hepatitis C virus (HCV) infection in a community in the Nile Delta: population description and HCV prevalence. Hepatol., 32(1), 111-115. Alfaleh, F.Z., Hadad, Q., Khuroo, M.S., Aljumah, A., Algamedi, A., Alshgar, H., Al-Ahdal, M.N., Mayet, I., Khan, M. Q. and Kessie, G.(2004): Peginterferon alfa-2b plus ribavirin compared with interferon alpha-2b plus ribavirin for initial treatment of chronic C in Saudi patients commonly infected with genotype 4. Liver Int., 24(6), 568-574. Alter, M.J. (2007): “ Epidemiologyof hepatitis C virus infection”. World J. Gasteroenterol 13(17), 2436-2441. Aman, W., Mousa, S., Shiha, G. and Mousa, S.A. (2012): Current status and future directions in the management of chronic hepatitis C. Virol. J., 9, 57. Ascione, A., De Luca, M., Tartaglione, M.T., Lampasi, F., Di Costanzo, G.G., Lanza, A.G., Picciotto,F.P., Marino-Marsilia, G., Fontanella, L. and Leandro, G.(2010): Peginterferon alfa-2a plus ribavirin is more effective that peginterferon alfa-2b plus ribavirin for treating hepatitis C virus infection. Gasteroenterol.,138, 116-122. Aslan N., Bozday M., Cetinkayah H., Sarioglu M., Turkay C., Bozkaya H., Karayalcin, S., Yurdaydin, C. and Uzunalimoglu, O.(2004): The mutations in ISDR of NS5A gene are not associated with response to interferon treatment in Turkish patients with chronic hepatitis C virus genotype 1b infection. Turk. J. Gastroenerol.,15(1), 21-26. Asselah, T., De Muynck S., Broet, P., Masliah-Planchon, J., Blanluet, M., Bieche I., Lapalus M., Martinot-Peignoux M., Lada, O. and Estrabaud, E. (2012): IL28 polymorphism is associated with treatment response in patients with genotype 4 chronic hepatitis C. J. Hepatol., 56, 527-532. Bae,S. H., Park, Y. M., Yoo, D. G., Choi, J. Y., Byun, B. H., Yang, J. M., Lee, C. D., Cha, S. B., Park, D. H. and Kim, B. S. (2000): Mutations of hepatitis C virus 1b NS5A 2209-2248 amino acid sequence is not a predictive factor for response to interferon-alpha

SaraMohamed Massoud et all..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
148
therapy and development of hepatocellular carcinoma. J. Korean Med. Sci., 15, 53-58. Brechot, C. (1999): The direct interplay between HCV NS5A protein and interferon transduction signal:from clinical to basic science. J. Hepatol., 30, 1152-1145. Di Bisceglie, A.M. (1998): Hepatitis C. Lancet. 351:351-355. El-Shamy, A., Shoji, I., El-Akel, W., Bilasy, S. E., Deng, L., El-Raziky, M., Jiang, D., Esmat, G. and Hotta, H.(2012):NS5A sequence heterogeneity of hepatitis C virus genotype 4a predicts clinical outcome of pegylated-interferon-ribavirin therapy in Egyptian patients. J. Clin. Microbiol.,50(12), 3886-3892. El-Zayadi, A.R., Attia, M., Barakat, E.M., Badran, H.M., Hamdy, H., El-Twail A., El-Nakeeb, A., Selim, O. and Saied, A.(2005): Response of hepatitis C genotype-4 naïve patients to 24 weeks of Peginterferon-alpha2b/ribavirin or induction-dose interferon-alpha2b/ribavirin/amantadine: a non-randomized controlled study. Am. J. Gasteroenterol., 100(11), 2447-2452. El-Zayadi, A, Selim, O., Haddad, S., Simmonds, P., Hamdy, H., Badran, H.M. and Shawky, S.(1999):Combination treatment of interferon alpha-2b and ribavirin in comparison to interferon monotherapy in treatment of chronic hepatitis C genotype 4 patients. Ital. J. Gastroenterol. Hepatol.,31, 472-475. El-Zayadi, A., Simmonds, P., Dabbous, H., Prescott, L., Selim, O. and Ahdy., A. (1996): Response to interferon-alpha of Egyptian patients infected with hepatitis C virus genotype 4. J. Viral. Hepat.,3, 261-264. Enomoto, N., Sakuma, I., Asahina, Y., Kurosak,i M., Murakami, T., Yamamoto, C., Ogura, Y., Izumi, N., Marumo, F. and Sato, C.(1996): Mutations in the nonstructural protein 5A gene and response to interferon in patients with chronic hepatitis C virus 1b infection.N. Engl. J. Med., 334, 77-81. Fried, M.W., Shiffman, M.L., Reddy, K.R., Smith, C., Marinos, G. and Goncales, F.L., (2002): Peginterferon alfa-2a plus ribavirin for chronic hepatits C virus infection. N. Engl. J. Med.,374, 975-982. Gerotto, M., Dal Pero, F., Pontisso P. Noventa, ., Gatta, A. and Alberti, A. (2000): Two PKR inhibitor HCV proteins correlate with early but not sustained responseto interferon. Gastroenterol.,119, 1649-1655.

PREDICATIVE FACTORS FOR PEGYLATED ……..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
149
Ghany, M.G., Stader, D.B., Thomas, D.L. and Seeff, L.B. (2009): Diagnosis, management, and treatment of hepatitis C: an update. Hepatol., 49(4), 1335-1374. Guo, X., Zhao Z., Xie J., Cai Q, Zhang, X., Peng, L. and Gao, Z.(2012): Prediction of response to pegylated-interferon-α and ribavirin therapy in Chinese patients infected with different hepatitis C virus genotype. Virol. J.,9, 123-128. Hasan, F., Asker, H., Al-Khaldi, J., Siddique, I., Al-Aimi, M., Owaid, S., Varghese, R. and Al- Nakib, B. (2004): Peginterferon alfa-2b plus ribavirin for the treatment of chronic hepatitis C genotype 4. Am. J. Gasteroenterol., 99(9), 1733-1737. Hatzakis, A., Wait, S., Bruix, J. et al., (2011): “The state of hepatitis B and C in Europe: report from the hepatitis B and C summit confereance”. J. Viral. Hepat., 18(1), 1-16 Hayashi, K., Katano, Y., Ishigamia, M., Itoh, A., Hirooka, Y., Nakano,I., Urano, F., Yoshioka, K., Toyoda,H., Kumada, T. and Goto, H. (2011): Mutations in the core and NS5A region of hepatitis C virus genotype 1b and correlation with response to pegylated-interferon-alpha 2b and ribavirin combination therapy. J. Virl. Hepat., 18(4), 280-286. Herion, D. and Hoofnagle, J. H. (1997). The interferon sensitivity determining region : all hepatitis C virus isolates are not the same. Hepatol., 25, 769-771. Hnatyszyan, H. J.(2005):Chronic hepatitis C and genotyping: the clinical significance of determining HCV genotypes. Antivir. Ther.,10(1), 1-11. Idrees, M. (2008). Development of an improved genotyping assay for detection of hepatitis C virus genotypes and subtypes in Pakistan. J. Virol. Methods 150(1-2), 50-56. Kadokura, M., Maekawa, S., Sueki, R., Miura, M., Komase, K., Shindo, H., Amemiya, F.,Ueteke, T., Inoue, T., Sakamato, M., Nakagawa, M., Sakamato, N., Watanbe, M. and Enomoto, N. (2011): Analysis of the complete open reading frame of genotype 2b hepatitis C virus in association with the response to peginterferon and ribavirin therapy. Plos One 6(9), e24514. Kamal, S.M., El Tawil, A.A., Nakano,T., He, Q., Rasenack, J., Hakam, S.A. Saleh, W., A., Ismail, A., Aziz, A. A. and Madwar, M. A.(2005): Peginterferon (alpha)-2b and ribavirin therapy in chronic

SaraMohamed Massoud et all..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
150
hepatitis C genotype 4: impact of treatment duration and viral kinetics on sustained virological response. Gut 54(6), 858-866. Kamal, S.M., Madwar, M.A., Peters, T., Fawzy, R. and Rasenak, J. ( 2000): Interferon therapy in patients with chronic hepatitis C and schistosomiasis. J. Hepatol.,32, 172-174. Kau, A., Vermehren, J. and Sarrazin, C. (2008):Treatment predictors of sustained virologic response in hepatitis B and C. J. Hepatol.,49, 334-651. Khuroo, M.S., Khuroo, M.S. and Dahab, S.T. (2004): Meta-analysis: A randomized trial of peginterferon plus ribavirin for the initial treatment of chronic hepatitis C genotype 4. Aliment. Pharmacol.Ther.,20, 931-938. Koshy, A., Marcellin, P., Martinot, M.and Madda, J.P. (2000): Improved response to ribavirin interferon combination compared with interferon alone in patients with type 4 chronic hepatitis without cirrhosis. Liver20(4), 335-339. Kurosaki, M., Tanaka, Y., Nishida, N., Sakamoto, N., Enomoto, N., Honda, M., Sugiyama, M., Matsuura, K., Sugauchi, F., Asahina, Y., Nakagawa, M., Watanabe, M., Sakamoto, M., Maekawa, S., Sakai, A., Kaneko, S., Ito, K., Masaki, N., Tokunaga, K., Izumi, N. andMizokami, M.(2011): Pretreatment prediction of response to pegylated-interferon plus ribavirin for chronic hepatitis C using genetic polymorphism in IL28B and viral factors. J. Hepatol., 54(3), 439-448. Manns, M.P., McHutchison, J.G., Gordon, S.C., Rustgi, V.K., Shiffman, M., Reindollar, R., Goodman, Z. D., Koury, K., Ling, M.and Albrecht, J. K.(2001):Peginterferon alfa-2a plus ribavirin compared with interferon alfa-2b plus ribavirin for initial treatment for chronic hepatitis C: a randomized trial. Lancet358, 958-965. Munoz de Rueda, P., Casado, J., Patron, D., Quintero, A., Palacios, A., Gila, A., Quiles, R., Leon, J., Ruiz-Extremera, A. and Salmeron, J.(2008). Mutations in E2-PePHD, NS5A-PKRBD, NS5A-ISDR, and NS5A-V3 of hepatitis C virus genotype 1 and their relationships to pegylated interferon –ribavirin treatment responses. J. Virol.,82, 6644-6653. Murayama, M., Katano Y., Nakano, I., Ishigami, M., Hayashi, K. and Honda, T. (2007):A mutation in the interferon sensitivity-determining region is associated with responsiveness to interferon-ribavirin combination therapy in chronic hepatitis patients infected

PREDICATIVE FACTORS FOR PEGYLATED ……..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
151
with a Japanese-specific subtype of hepatitis C virus genotype 1b. J. Med. Virol., 79, 35-40. Murphy, M. D., Rosen, H. R., Marousek, G. I. and Chou, S. (2002): Analysis of sequence configurations of ISDR, PKR-binding domain, and V3 region as predictors of response to induction interferon-alpha and ribavirin therapy in chronic hepatitis C virus infection. Dig. Dis. Sci., 47, 1195-1205. Nakagawa, M., Sakamoto, N., Ueyama, M., Mogushi, K., Nagaie, S., Itsui, Y., Azuma, S., Kakinuma, S., Tanaka, H., Enomoto, N. and Watanabe, M. (2010): Mutations in the interferon determining region and virologic response to combination therapy with pegylated interferon alpha 2bplus ribavirin in patients with chronic hepatitis C-1b infection. J. Gastroenterol., 45 (6), 656-665. Nguyen, M.H. and Keeffe, E.B. (2005): Prevalence and treatment of hepatitis C virus genotypes 4, 5, and 6. Clin Gastroenterol Hepatol.,3(10 Suppl2), S97-S101. Pawlotsky, J. M., Germanidis, G., Neumann, A. U., Pellerin, M., Frainais, P. O. and Dhumeaux, D. (1998): Interferon resistance of hepatitis C virus genotype 1b: relation to non-structural 5A gene quasispecies mutations. J. Virol., 72, 2795-2805. Ray, S.C., Arthur, R.R., Carella, A., Bukh, J., and Thomas, D. (2000). Genetic epidemiology of hepatitis C virus throughout Egypt. J. Infect. Dis.,182, 698-707. Rumi, M.G., Aghemo, A., Prati, G.M., D'Ambrosio, R., Donato, M.F., Soffredini, R., Del, E., Russo, N. A. and Colombo, M.(2010): Randomized study of peginterferon-alpha2a plus ribavirin vs peginterferon-alpha2b plus ribavirin in chronic hepatitis C. Gastroenterol., 138, 108-115. Saiz, J. C., Lopez-Labrador, F. X., Ampurdanes, S. Dopazo, J, Forns, X., anchez-Tapias, J. M. and Rodes, J.(1998): The prognostic relevance of the nonstructural 5A gene interferon sensitivity determining region is different in infections with genotype 1band 3a isolates of hepatitis c virus. J. Infec. Dis 177, 839-847. Sarrazin, C., Berg, T., Lee, J. H., Gerlinde, T., Dietrich, C. F., Roth, W. K. and Zeuzem, S. (1999): Improved correlation between multiple mutations within the NS5A region and virologic response in European patients chronically infected with hepatitis C virus type 1b undergoing combination therapy. J. Hepatol.,30, 1004-1013.

SaraMohamed Massoud et all..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
152
Sarrazin, C., Berg, T., Lee, J. H., Ruster, B., Kronenberger,B., Roth, W. K. and Zeuzem, S. (2000): Mutations in the protein kinase –binding domain of the NS5A protein in patients infected with hepatitis c virus type 1a are associated with treatment response. J. Infec. Dis., 101, 432-441. Sanger, F., Nicklen, S. and Coulson A. R. (1977): DNA sequencing with chain-terminating inhibitors. Proc. Natl. Acad. Sci. USA, 74(12), 5463-5467. Sharma, S.D. (2010):Hepatitis C virus: molecular biology & current therapeutic options. Indian J. Med. Res.,131, 17-34. Shemis, M. A., El-Abd, D. M., Ramadan, D. I., El-Sayed, M. I., Guirgis, B. S., Saber, M. A. and Azzazy, H. M. (2012): Evaluation of multiplex nested polymerase chain reaction for routine hepatitis C virus genotyping in Egyptian patients. Hepat. Mon12(4), 265-270. Vogelstein, B. and Gillespie, D. (1979): Preparative and analytical purification of DNA from agarose. Proc. Natl. Acad. Sci. USA, 76, 615-619. Watanabe, K., Yoshioka, K., Yano, M., Ishigami, M., Ukai, K., Ito,H., Miyata, F., Mizutani, T. and Goto, H. (2005): Mutations in the nonstructural region 5B of hepatitis C virus genotype 1b: their relation to viral load, response to interferon, and the nonstructural 5A. J. Med. Virol., 75, 504-512. Witherell, G. W. and Beineke P. (2001):Statistical analysis of combined substitution in nonstructural 5A region of hepatitis C virus and interferon response. J. Med. Virol., 62, 8-16. Yen, Y.H., Hung, C.H., Hu, T.H., Chen, C.H., Wu, C.M., Wang, J.H., et al. (2008). Mutations in the interferon sensitivity-determining region (nonstructural 5A amino acid 2209-2248) in patients with hepatitis C-1b infection and correlated response to combined therapy of pegylated interferon and ribavirin. Aliment. Pharmcol. Ther.,27, 72-79. Yoon, J., Lee, J. I., Baik, S. K., Lee, K. H., Sohn, J. H., Lee, H-W., Namkung, J., Chang,S. J., Choi, J-W., Kim, H-W. and Yeh, B-I. (2007): Predictive factors for interferon and ribavirin combination therapy in patients with chronic hepatitis C. World J. Gastroenterol., 13(4):6236-6424. Zekri, A. R. N., Bahnassy, A. A., Abdel-Wahab, S. A., Khafagy, M. M., Loutfy, S. A., Radwan, H. and Shaarawy, S. M. (2009): Expression of pro- and anti-inflammatory cytokines in relation to

PREDICATIVE FACTORS FOR PEGYLATED ……..
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ
153
apoptotic genes in Egyptian liver disease patients associated with HCV-genotype-4. J. Gastroenterol.Hepatol.,24, 416-428. Zeuzem, S., Lee, J. H. and Roth, W., K. (1997): Mutations in the NS5A gene of European hepatitis C virus isolates and response to IFN alfa. Hepatol., 25,740-744.
الملخص العربي
انترفیرون و الریبافرین معا في المرضى - العوامل التنبؤیة للعالج بأستخدام البیج ٤النمط الجیني " ج"المصریین المصابین بااللتھاب الكبدي المزمن
٣، ممدوح أحمد طھ ١، ایھاب علي دریس٢محمد عباس شمیس ،١دسارة محمد مسعو
٢ر، محمد علي صاب٢حنان عبد المنعم عمر
قسم البیولوجیا ٢،جامعة الفیوم–كلیة العلوم –قسم الكیمیاء –شعبة الكیمیاء الحیویة ١
جامعة الفیوم–كلیة العلوم –قسم الكیمیاء ٣معھد تیودور بلھارس ، -الجزیئیة
ھو عدوي شائعة في مصر ، و ٤النمط الجینیي " ج"فیروس االلتھاب الكبدي الوبائي یعتبروتقترح التقاریر الي ان العوامل التنبؤیة لفاعلیة العالج .مراض الكبد السبب الرئیسي ال
في مرضي االلتھاب الكبدي الوبائي المزمن ترجع الي الفا و الریبافرین - باالنترفیرونو بناء علي ذلك تم فحص العوامل . المحددة لالنترفیرون -الطفرات في منطقة الحساسةانترفیرون و الریبافیرین معا في مرضي االلتھاب الكبدي –ج التنبؤیة للعالج بأستخدام البی
مریضا بااللتھاب عینوقد اجریت ھذه الدراسة علي ارب. ٤الوبائي المزمن النمط الجیني ١٨٠بأخذ جرعة اسبوعیا من م عالجھوتم ٤النمط الجینیي "ج"الكبدي الوبائي بفیروس
تم تقدیر معیار و. مدة ثمانیة و اربعین اسبوعاانترفیرون مع الریبافرین ل –میكروجرام بیج في امصال المرضي تفاعل البلمرة المتسلسل –بأستخدام الوقت الحقیقي "ج"للفیروس الرنا
منطقة الوایضا تكبیر " سي" و قد تم تحدید النمط الجیني بأستخدام اولیات معینة للفیروسلمرة المتسلسل وتعیین تتابع االحماض الحساسة لالنترفیرون بأستخدام تفاعل الب -المحددة
. الجینالموجودة في بنك " ج"ة لھا و مقارنتھا بتتابع االحماض االمینیة للفیروس ینیاالمولقد اوضحت النتائج ان احدي و عشرون مریضا استجابوا بینما لم یستجیب تسعة عشرة
ولوحظ ان ھناك فروقا معنویا في معیار . انترفیرون مع الریبافیرین -مریضا للعالج بالبیج - منطقةالمحددةالرنا للفیروس بینماالتوجد فروقا معنویا في احالالت االحماض االمینیة في ال
و دلت النتائج ایضا ان الجنس و العمر و . في كال من المجموعتیننترفیرونالحساسة لالال تعتبر عوامل تنبؤیة لفاعلیة االستجابة للعالج الحساسة لالنترفیرون - منطقة المحددةال
ومن ھذه النتائج یمكن استخالص ان معیار الرنا للفیروس . انترفیرون مع الریبافرین- بالبیجانترفیرون مع الریبافیرین في المرضي - نبؤ بفاعلیة العالج بالبیجعامل مؤثر للت" ج"
. ٤المزمن النمط الجیني " ج"المصریین بفیروس
.الكبدى الفیروسى سى المزمن قبل بدء العالج للوصول الفضل النتائج





![Release - Royal Society of Chemistry · The resulting ADA2+@HACD solution ([β-CD] =N/P[ADA2+] = 1.0 mM) was stored at 4 °C. Agarose gel electrophoresis experiments. Agarose gel](https://static.fdocument.org/doc/165x107/5f7fa88364f31173993e6861/release-royal-society-of-the-resulting-ada2hacd-solution-cd-npada2.jpg)