Inhibiting Janus kinases to treat alopecia areata
2
NEWS AND VIEWS NATURE MEDICINE VOLUME 20 | NUMBER 9 | SEPTEMBER 2014 989 complicating its role in AA 12 . Notably, block- ing antibodies against IL-2, IL-15R and IFN-γ, when given individually, did not reverse estab- lished AA in mice. Thus, the authors’ data indi- cate a role for IL-2, IL-15, IFN-γ and possibly IL-21 signaling in AA. The involvement of IFN-γ and the γ c cytokine family in AA suggests a role for downstream signaling via JAK molecules. This is supported by the authors’ gene expression data, which showed increased JAK1 and JAK3 expression in diseased human and mouse skin 2 . The authors further investigated the role of JAKs in AA in mice using small-molecule inhibitors of JAK both systemically (orally or subcutaneously) and topically, which arrested and reversed AA. Global transcriptional analysis validated these findings by showing reduced inflammation in skin of mice treated with small-molecule inhibitors of JAK. Finally, in preliminary data from a clinical trial, the oral JAK1/2 inhibitor ruxolitinib, a US Food and Drug Administration (FDA)- approved drug for the treatment of myelofibro- sis, reversed established AA in three patients 2 . This resulted in a reduction in inflammation within the patients’ skin biopsies. In serendipi- tous independent support of these observations, it was recently reported that a patient receiving treatment for psoriasis with tofacitinib, a JAK1/3 inhibitor, currently approved by the FDA for use in rheumatoid arthritis, experi- enced dramatic remission of his longstanding alopecia universalis 13 . Given these obser- vations, and their molecular findings, the authors proposed a positive feedback loop in AA in which skin-infiltrating CD8 + NKG2D + T cells produce IFN-γ, which induces IL-15 and IL-15Rα production by follicular epithe- lial cells, which in turn activates and sustains the CD8 + NKG2D + effector T cell response and autoimmunity. JAK inhibitors would serve to inhibit this loop (Fig. 1). Interestingly, despite the evidence supporting a role for cytotoxic T lymphocytes in AA, AA does not result in hair follicle destruction, as mentioned above—that is, it is a nonscarring alopecia 1 . Might nonlethal injury of hair follicle epithelial cells, mediated by CD8 + NKG2D + T cells, trigger the pathway of anagen arrest– mediated hair loss? Is the putative autoantigen Alopecia areata (AA) has a worldwide preva- lence of ~0.1–0.2%, and two-thirds of affected individuals are 30 years old or younger at the time of disease onset 1 . Although not life threat- ening, the disease is an affliction, particularly to people with more extensive disease including complete hair loss of the scalp (alopecia tota- lis) and body (alopecia universalis). Individuals with AA are subject to dramatic changes in their appearance caused by sporadic hair loss. Only recently has evidence for an immunological basis of AA become evident 1 . In this issue of Nature Medicine, Xing et al. 2 present evidence regarding the autoimmune mechanism underlying AA in a mouse model and in samples from subjects with the disease. They show that AA is mediated by CD8 + NKG2D + T cells via an interleukin-15 (IL-15) positive feedback loop with follicular epithelial cells, mediated in part through the JAK signaling pathway. Furthermore, they show that this provides a very promising avenue for therapy in human patients. It is known that AA is a T cell–mediated autoimmune disorder, and people with AA have higher rates of other autoimmune diseases 1 . Hair loss is induced through interference and arrest of the growth phase of the hair cycle (ana- gen), leading to premature follicle senescence rather than direct immune-mediated follicle destruction (reviewed in ref. 1). Unlike the case for other immune-mediated skin diseases, an animal model exists for AA that recapitulates human disease well 3,4 . Owing to a complex polygenic trait 5 , roughly 15% of susceptible C3H/HeJ mice spontaneously develop AA by 1 year of age 3 . Affected skin can be grafted onto disease-free syngeneic mice, resulting in nearly 100% transfer of the disease to graft recipients 4 . In the C3H/HeJ model, mice typically develop one or multiple foci of alopecia, and occasion- ally universal alopecia, similar to human disease, and a peribulbar T cell infiltrate is observed in mouse and human diseased skin 6 . A previous genome-wide association study (GWAS) of subjects with AA showed a strong association of predisposition to AA with cer- tain polymorphisms of ligands for the natu- ral killer cell–activating receptor NKG2D. The study further demonstrated increased expression of these ligands in the hair fol- licle and showed infiltrating CD8 + NKG2D + T cells in affected skin 7 . Xing et al. 2 therefore investigated the expression and function of NKG2D in T cells in the mouse model of AA. Biopsies of lesional skin in the AA mouse model revealed CD8αβ + NKG2D + T cells with an activated T effector memory cell phenotype (CD62 low CD44 hi ). Likewise, cutaneous lymph nodes had a robust CD8 + NKG2D + T cell popu- lation in affected mice. These CD8 + NKG2D + T cells also expressed CD103, a subunit of the α E β 7 integrin ligand for epithelial cadherin, which would allow T cells to migrate to epithe- lial sites such as skin. The AA phenotype could be adoptively transferred to normal recipient mice via transfer of whole lymph node prepa- rations or positively selected CD8 + NKG2D + T cells, but not by adoptive transfer of NKG2D- depleted T cells. These studies thus indicated that CD8 + NKG2D + T cells are both necessary and sufficient for disease. The previous GWAS also implicated members of the γ c cytokine-receptor path- way in AA 7 . Xing et al. 2 therefore performed comparative genomics of the transcrip- tional profiles of skin from both AA model mice and humans with AA, which provided evidence for the involvement of γ c cytokine and receptor family members, including IL-2, IL-7, IL-15 and IL-21, and interferon-γ (IFN-γ) response elements. Expression of the IL-2 receptor, and a role for IFN-γ, in AA had been previously demonstrated 8–10 . Xing et al. 2 also detected increased expression of IL-15 and its chaperone receptor IL-15Rα in hair follicles and of the receptor IL-15Rβ on infiltrating T cells of affected skin. Systemic administra- tion via intraperitoneal injection of antibodies to IL-2, IL-15R or IFN-γ, but not IL-21, blocked AA development. Whereas IFN-γ, IL-15 and IL-2 are well-known mediators of CD8 + T cell induction, maintenance and function (reviewed in ref. 11), IL-21 has broad actions on many immune cell types, potentially Sherrie J. Divito and Thomas S. Kupper are at the Department of Dermatology, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, USA. e-mail: [email protected] Inhibiting Janus kinases to treat alopecia areata Sherrie J Divito & Thomas S Kupper Alopecia areata is an immune-mediated, nonscarring form of hair loss. A new study using human clinical samples and a mouse model demonstrates that CD8 + NKG2D + T effector memory cells mediate alopecia areata in part through Janus kinase (JAK) signaling and that alopecia areata might be treated with JAK inhibitors. npg © 2014 Nature America, Inc. All rights reserved.
Transcript of Inhibiting Janus kinases to treat alopecia areata

n e w s a n d v i e w s
nature medicine volume 20 | number 9 | september 2014 989
complicating its role in AA12. Notably, block-ing antibodies against IL-2, IL-15R and IFN-γ, when given individually, did not reverse estab-lished AA in mice. Thus, the authors’ data indi-cate a role for IL-2, IL-15, IFN-γ and possibly IL-21 signaling in AA.
The involvement of IFN-γ and the γc cytokine family in AA suggests a role for downstream signaling via JAK molecules. This is supported by the authors’ gene expression data, which showed increased JAK1 and JAK3 expression in diseased human and mouse skin2. The authors further investigated the role of JAKs in AA in mice using small-molecule inhibitors of JAK both systemically (orally or subcutaneously) and topically, which arrested and reversed AA. Global transcriptional analysis validated these findings by showing reduced inflammation in skin of mice treated with small-molecule inhibitors of JAK.
Finally, in preliminary data from a clinical trial, the oral JAK1/2 inhibitor ruxolitinib, a US Food and Drug Administration (FDA)-approved drug for the treatment of myelofibro-sis, reversed established AA in three patients2. This resulted in a reduction in inflammation within the patients’ skin biopsies. In serendipi-tous independent support of these observations, it was recently reported that a patient receiving treatment for psoriasis with tofacitinib, a JAK1/3 inhibitor, currently approved by the FDA for use in rheumatoid arthritis, experi-enced dramatic remission of his longstanding alopecia universalis13. Given these obser-vations, and their molecular findings, the authors proposed a positive feedback loop in AA in which skin-infiltrating CD8+NKG2D+ T cells produce IFN-γ, which induces IL-15 and IL-15Rα production by follicular epithe-lial cells, which in turn activates and sustains the CD8+NKG2D+ effector T cell response and autoimmunity. JAK inhibitors would serve to inhibit this loop (Fig. 1).
Interestingly, despite the evidence supporting a role for cytotoxic T lymphocytes in AA, AA does not result in hair follicle destruction, as mentioned above—that is, it is a nonscarring alopecia1. Might nonlethal injury of hair follicle epithelial cells, mediated by CD8+NKG2D+ T cells, trigger the pathway of anagen arrest–mediated hair loss? Is the putative autoantigen
Alopecia areata (AA) has a worldwide preva-lence of ~0.1–0.2%, and two-thirds of affected individuals are 30 years old or younger at the time of disease onset1. Although not life threat-ening, the disease is an affliction, particularly to people with more extensive disease including complete hair loss of the scalp (alopecia tota-lis) and body (alopecia universalis). Individuals with AA are subject to dramatic changes in their appearance caused by sporadic hair loss. Only recently has evidence for an immunological basis of AA become evident1. In this issue of Nature Medicine, Xing et al.2 present evidence regarding the autoimmune mechanism underlying AA in a mouse model and in samples from subjects with the disease. They show that AA is mediated by CD8+NKG2D+ T cells via an interleukin-15 (IL-15) positive feedback loop with follicular epithelial cells, mediated in part through the JAK signaling pathway. Furthermore, they show that this provides a very promising avenue for therapy in human patients.
It is known that AA is a T cell–mediated autoimmune disorder, and people with AA have higher rates of other autoimmune diseases1. Hair loss is induced through interference and arrest of the growth phase of the hair cycle (ana-gen), leading to premature follicle senescence rather than direct immune-mediated follicle destruction (reviewed in ref. 1). Unlike the case for other immune-mediated skin diseases, an animal model exists for AA that recapitulates human disease well3,4. Owing to a complex polygenic trait5, roughly 15% of susceptible C3H/HeJ mice spontaneously develop AA by 1 year of age3. Affected skin can be grafted onto disease-free syngeneic mice, resulting in nearly 100% transfer of the disease to graft recipients4. In the C3H/HeJ model, mice typically develop one or multiple foci of alopecia, and occasion-ally universal alopecia, similar to human disease, and a peribulbar T cell infiltrate is observed in mouse and human diseased skin6.
A previous genome-wide association study (GWAS) of subjects with AA showed a strong association of predisposition to AA with cer-tain polymorphisms of ligands for the natu-ral killer cell–activating receptor NKG2D. The study further demonstrated increased expression of these ligands in the hair fol-licle and showed infiltrating CD8+NKG2D+ T cells in affected skin7. Xing et al.2 therefore investigated the expression and function of NKG2D in T cells in the mouse model of AA. Biopsies of lesional skin in the AA mouse model revealed CD8αβ+NKG2D+ T cells with an activated T effector memory cell phenotype (CD62lowCD44hi). Likewise, cutaneous lymph nodes had a robust CD8+NKG2D+ T cell popu-lation in affected mice. These CD8+NKG2D+ T cells also expressed CD103, a subunit of the αEβ7 integrin ligand for epithelial cadherin, which would allow T cells to migrate to epithe-lial sites such as skin. The AA phenotype could be adoptively transferred to normal recipient mice via transfer of whole lymph node prepa-rations or positively selected CD8+NKG2D+ T cells, but not by adoptive transfer of NKG2D-depleted T cells. These studies thus indicated that CD8+NKG2D+ T cells are both necessary and sufficient for disease.
The previous GWAS also implicated members of the γc cytokine-receptor path-way in AA7. Xing et al.2 therefore performed comparative genomics of the transcrip-tional profiles of skin from both AA model mice and humans with AA, which provided evidence for the involvement of γc cytokine and receptor family members, including IL-2, IL-7, IL-15 and IL-21, and interferon-γ (IFN-γ) response elements. Expression of the IL-2 receptor, and a role for IFN-γ, in AA had been previously demonstrated8–10. Xing et al.2 also detected increased expression of IL-15 and its chaperone receptor IL-15Rα in hair follicles and of the receptor IL-15Rβ on infiltrating T cells of affected skin. Systemic administra-tion via intraperitoneal injection of antibodies to IL-2, IL-15R or IFN-γ, but not IL-21, blocked AA development. Whereas IFN-γ, IL-15 and IL-2 are well-known mediators of CD8+ T cell induction, maintenance and function (reviewed in ref. 11), IL-21 has broad actions on many immune cell types, potentially
Sherrie J. Divito and Thomas S. Kupper are at the Department of Dermatology, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, USA. e-mail: [email protected]
Inhibiting Janus kinases to treat alopecia areataSherrie J Divito & Thomas S Kupper
Alopecia areata is an immune-mediated, nonscarring form of hair loss. A new study using human clinical samples and a mouse model demonstrates that CD8+NKG2D+ T effector memory cells mediate alopecia areata in part through Janus kinase (JAK) signaling and that alopecia areata might be treated with JAK inhibitors.
npg
© 2
014
Nat
ure
Am
eric
a, In
c. A
ll rig
hts
rese
rved
.

n e w s a n d v i e w s
990 volume 20 | number 9 | september 2014 nature medicine
Treatment of AA with topical JAK1/2 (IFN-γ pathway) and JAK3 (γc cytokines) inhibitors seems a very promising approach, particu-larly for localized disease, although a topical JAK inhibitor with sufficient skin penetration has not yet been developed. Because of their extensive nature, alopecia totalis and alopecia universalis will probably require oral therapy. The JAK1/2 inhibitor ruxolitinib has been used systemically successfully in myelofibrosis14, and the JAK 1/3 inhibitor tofacitinib has been used for rheumatoid arthritis15, another autoimmune disease with NKG2D ligand
in this disease preferentially expressed by anagen hair follicles? One effective treatment for AA is the induction of contact hypersensitivity (CHS) in skin by topically applied diphenylcyclopro-penone1. Moreover, the only pre-tofacitinib hair growth on the patient with psoriasis and alopecia universalis was within his psoriatic plaques13. How do the immunologic pathways in CHS or psoriasis short-circuit the pathogenic process in AA that leads to anagen arrest and interfere with this purported positive feedback loop? The stage is now set to answer these ques-tions experimentally.
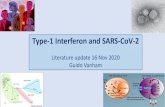
Figure 1 Positive feedback loop in AA. Xing et al.2 show that CD8+ NKG2D+T cells infiltrate the dermis and localize to the hair follicle bulb, where they form immune synapses with follicular epithelial cells through major histocompatibility complex (MHC) class I–peptide complexes and NKG2DL. Activated CD8+ T cells release IFN-, which binds the IFN-R on the surface of the follicular epithelial cell, which in turn signals via JAK1 and JAK2 to promote production of IL-15, a mediator of CD8+ T cell induction, and its chaperone IL-15R. This binds the IL-15R complex (IL-2R and c) on the CD8+ T cell surface, causing signaling via JAK1 and JAK3 to enhance the production of IFN- and amplify the feedback loop. Ruxolitinib and tofacitinib are small-molecule JAK inhibitors that interfere with this feedback loop; ruxolitinib inhibits JAK1 and JAK2, and tofacitinib inhibits JAK3 more strongly than JAK1. These inihbitors are able to alleviate the AA symptoms. STAT1, signal transducer and activator of transcription-1; TCR, T cell receptor; STAT5, signal transducer and activator of transcription-5.
Deb
bie
Mai
zels
/Nat
ure
Pub
lishi
ng G
roup
(NKG2DL)-mediated recruitment of CD8+ NKG2D+ T cells16. The efficacy of ruxolitinib for treatment of AA in this study by Xing et al.2 is striking, although only three patients were treated. The use of these drugs to treat AA must be validated in a larger clinical trial, and the risk-benefit ratio discussed, before their widespread clinical use. However, the authors’ elegant synergy of genetic data from GWAS, of human and mouse data, and new in vivo and in vitro studies dissecting the mechanism of disease have led to this very promising path for therapy.
COMPETING FINANCIAL INTERESTS The authors declare no competing financial interests.
1. Gilhar, A., Etzioni, A. & Paus, R. N. Engl. J. Med. 366, 1515–1525 (2012).
2. Xing, L. et al. Nat. Med. 20, 1043–1049 (2014).3. Sundberg, J.P., Cordy, W.R. & King, L.E. Jr. J. Invest.
Dermatol. 102, 847–856 (1994).4. McElwee, K.J., Boggess, D., King, L.E. Jr. & Sundberg, J.P.
J. Invest. Dermatol. 111, 797–803 (1998).5. Sundberg, J.P., Silva, K.A., Li, R., Cox, G.A. & King, L.E.
J. Invest. Dermatol. 123, 294–297 (2004).6. McElwee, K.J. et al. Pathobiology 66, 90–107
(1998).7. Petukhova, L. et al. Nature 466, 113–117
(2010).8. Gilhar, A., Kam, Y., Assy, B. & Kalish, R.S. J. Invest.
Dermatol. 124, 288–289 (2005).9. Freyschmidt-Paul, P. et al. Br. J. Dermatol. 155,
515–521 (2006).10. Brajac, I., Gruber, F., Petrovecki, M. & Malnar-Dragojevic, D.
Acta Dermatovenerol. Croat. 12, 154–156 (2004).
11. Weng, N.P., Liu, K., Catalfamo, M., Li, Y. & Henkart, P.A. Ann. NY Acad. Sci. 975, 46–56 (2002).
12. Spolski, R. & Leonard, W.J. Nat. Rev. Drug Discov. 13, 379–395 (2014).
13. Craiglow, B.G. & King, B.A. J. Invest. Dermatol. doi:10.1038/jid.2014.260 (17 July 2014).
14. Quintás-Cardama, A. et al. Blood 115, 3109–3117 (2010).
15. Ghoreschi, K. et al. J. Immunol. 186, 4234–4243 (2011).
16. Andersson, A.K. et al. Arthritis Rheum. 63, 2617–2629 (2011).
Follicularepithelial cell
Nucleus
Nucleus
MHC class I+ peptide
Hair follicle bulb(anagen phase)
CD8+
NKG2D+
T cells
CD8+NKG2D+
T cell
T cellproliferation
STAT1P
STAT5P
Tofacitinib
Tofacitinib
Ruxolitinib
Ruxolitinib
JAK1
JAK1
JAK2
JAK3
IFN-γR1
IFN-γγc
IFN-γR2
NKG2D
NKG2DL
CD8
TCR
IL-15 IL-15Rα
IL-2Rβ
npg
© 2
014
Nat
ure
Am
eric
a, In
c. A
ll rig
hts
rese
rved
.