Impact of genetic polymorphisms of the β -adrenergic receptor on albuterol bronchodilator...
7
Bronchodilator responsiveness to β 2 -adrenergic receptor agonists in patients with asthma varies consid- erably. 1 Gender, race, other diseases, age, and the administration of other drugs are thought to contribute to interpatient variability in responsiveness to β 2 - agonist administration, whereas diminished bronchodi- lation to long-term β 2 -agonist treatment, or tolerance (also called tachyphylaxis or desensitization) con- tributes to intrapatient variability. Tolerance to long- term β 2 -agonist treatment is thought to be the result of agonist-promoted uncoupling of the β 2 -adrenergic receptor from G s -binding protein and to receptor down- regulation. 2 Impact of genetic polymorphisms of the β 2 -adrenergic receptor on albuterol bronchodilator pharmacodynamics Objective: To determine whether genetic polymorphisms of the β 2 -adrenergic receptor gene affect the rela- tionship between albuterol (INN, salbutamol) plasma concentrations and the forced expiratory volume in 1 second (FEV 1 ) in subjects with moderate asthma. Methods: Sixteen clinically stable patients with moderate asthma who participated in a pharmacokinetic- pharmacodynamic study of albuterol volunteered to provide a blood sample for determination of β 2 - adrenergic receptor genotype. FEV 1 and plasma concentrations of albuterol were determined at various times after administration of an oral solution that contained 8 mg albuterol. Patients withheld inhaled β 2 - agonist and corticosteroid therapy 12 and 24 hours, respectively, before the study. β 2 -Adrenergic receptor genotype was determined by polymerase chain reaction with allele-specific oligonucleotide hybridization. Results: Albuterol-evoked FEV 1 was higher and the response was more rapid in Arg16 homozygotes com- pared with the cohort of carriers of the Gly16 variant: Maximal percentage increase in FEV 1 (%∆FEV 1 ), 18% versus 4.9% (P < .03); area under FEV 1 albuterol concentration curve, 194%·mL/ng versus 30%·mL/ng (P < .05); initial slope (dE/dC), 1.43%·mL/ng versus 0.55%·mL/ng (P < .003). Conclusions: The β 2 -adrenergic receptor gene polymorphism is a major determinant of bronchodilator response to albuterol. Future pharmacodynamic studies of β 2 -agonists should include determination of β 2 -adrenergic receptor genotype. (Clin Pharmacol Ther 1999;65:519-25.) John J. Lima, PharmD, a Donald B. Thomason, PhD, Mohamad H. N. Mohamed, PharmD, Louis V. Eberle, MD, Timothy H. Self, PharmD, and Julie A. Johnson, PharmD Memphis, Tenn From the Departments of Clinical Pharmacy, Pharmaceutical Sci- ences, Physiology and Biophysics, and Medicine, Colleges of Pharmacy and Medicine, University of Tennessee. Supported in part by a research grant from Glaxo-Wellcome, Inc (Research Triangle Park, NC); by grants RR00211 and GM-50979 from the National Institutes of Health (Bethesda, Md); and by grants from the Center for Pediatric Pharmacokinetics and Thera- peutics, University of Tennessee (Memphis, Tenn). Received for publication Oct 28, 1998; accepted Jan 13, 1999. Reprint requests: Julie A. Johnson, PharmD, Department of Phar- macy Practice, University of Florida, Box 100486; HSC, Gainesville, FL 32610. E-mail: [email protected] a Present address: Center for Clinical Pediatric Pharmacology, Nemours Children’s Clinic, 807 Nira St, Jacksonville, FL 32207. Copyright © 1999 by Mosby, Inc. 0009-9236/99/$8.00 + 0 13/1/97202 519 PHARMACODYNAMICS AND DRUG ACTION
Transcript of Impact of genetic polymorphisms of the β -adrenergic receptor on albuterol bronchodilator...

Bronchodilator responsiveness to β2-adrenergicreceptor agonists in patients with asthma varies consid-erably.1 Gender, race, other diseases, age, and theadministration of other drugs are thought to contributeto interpatient variability in responsiveness to β2-agonist administration, whereas diminished bronchodi-lation to long-term β2-agonist treatment, or tolerance(also called tachyphylaxis or desensitization) con-tributes to intrapatient variability. Tolerance to long-term β2-agonist treatment is thought to be the result ofagonist-promoted uncoupling of the β2-adrenergicreceptor from Gs-binding protein and to receptor down-regulation.2
Impact of genetic polymorphisms of theβ2-adrenergic receptor on albuterolbronchodilator pharmacodynamics
Objective: To determine whether genetic polymorphisms of the β2-adrenergic receptor gene affect the rela-tionship between albuterol (INN, salbutamol) plasma concentrations and the forced expiratory volume in1 second (FEV1) in subjects with moderate asthma.Methods: Sixteen clinically stable patients with moderate asthma who participated in a pharmacokinetic-pharmacodynamic study of albuterol volunteered to provide a blood sample for determination of β2-adrenergic receptor genotype. FEV1 and plasma concentrations of albuterol were determined at varioustimes after administration of an oral solution that contained 8 mg albuterol. Patients withheld inhaled β2-agonist and corticosteroid therapy 12 and 24 hours, respectively, before the study. β2-Adrenergic receptorgenotype was determined by polymerase chain reaction with allele-specific oligonucleotide hybridization.Results: Albuterol-evoked FEV1 was higher and the response was more rapid in Arg16 homozygotes com-pared with the cohort of carriers of the Gly16 variant: Maximal percentage increase in FEV1 (%∆FEV1),18% versus 4.9% (P < .03); area under FEV1 albuterol concentration curve, 194%·mL/ng versus30%·mL/ng (P < .05); initial slope (dE/dC), 1.43%·mL/ng versus 0.55%·mL/ng (P < .003).Conclusions: The β2-adrenergic receptor gene polymorphism is a major determinant of bronchodilatorresponse to albuterol. Future pharmacodynamic studies of β2-agonists should include determination ofβ2-adrenergic receptor genotype. (Clin Pharmacol Ther 1999;65:519-25.)
John J. Lima, PharmD,a Donald B. Thomason, PhD,Mohamad H. N. Mohamed, PharmD, Louis V. Eberle, MD,Timothy H. Self, PharmD, and Julie A. Johnson, PharmD Memphis, Tenn
From the Departments of Clinical Pharmacy, Pharmaceutical Sci-ences, Physiology and Biophysics, and Medicine, Colleges ofPharmacy and Medicine, University of Tennessee.
Supported in part by a research grant from Glaxo-Wellcome, Inc(Research Triangle Park, NC); by grants RR00211 and GM-50979from the National Institutes of Health (Bethesda, Md); and bygrants from the Center for Pediatric Pharmacokinetics and Thera-peutics, University of Tennessee (Memphis, Tenn).
Received for publication Oct 28, 1998; accepted Jan 13, 1999.Reprint requests: Julie A. Johnson, PharmD, Department of Phar-
macy Practice, University of Florida, Box 100486; HSC,Gainesville, FL 32610. E-mail: [email protected]
aPresent address: Center for Clinical Pediatric Pharmacology,Nemours Children’s Clinic, 807 Nira St, Jacksonville, FL 32207.
Copyright © 1999 by Mosby, Inc.0009-9236/99/$8.00 + 013/1/97202
519
PHARMACODYNAMICS ANDDRUG ACTION

Several mis-sense mutations in the coding region ofthe β2-adrenergic receptor gene have been identified.Five of these were degenerate in that they encoded thesame proteins. However, 2 of these mutations, at loci16 and 27, encoded different proteins and were presentin high-allelic frequencies.3 Among the general popula-tion (including patients with asthma),β2-adrenergicreceptor alleles are distributed in the following approxi-mate proportions: homozygous Arg16 (Arg16/Arg16),15%; heterozygous (Arg16/Gly16) 38%; homozygousGly16 (Gly16/Gly16), 45%; homozygous Gln27(Gln27/Gln27), 26%; heterozygous (Gln27/Glu27),49%; and homozygous Glu27 (Glu27/Glu27), 22%.4-13
The functional consequences of these polymorphismshave been studied by site-directed mutagenesis and therecombinant expression in Chinese hamster fibroblasts,as well as in human airway smooth muscle cells.14,15
The Gly16 allele has been associated with enhancedagonist-promoted β2-receptor down-regulation, whereasthe Glu27 allele showed minimal down-regulation com-pared with the Arg16 and Gln27 alleles, respectively.Although asthma is primarily an inflammatory diseaseof the airways, mutations in the β2-adrenergic receptormay be risk factors in certain asthma phenotypes.3-5,7,11
They may also be factors in determining responsivenessto β2agonists,6,9 although there are conflicting data.12,13
Therefore the relationship between genetic polymor-phism of the β2-adrenergic receptor and responsivenessto β2-agonist treatment is unclear.
We recently completed a study of the effects of raceand gender on the bronchodilator response to albuterolin white and black patients with asthma. To determinewhether or not genetic polymorphisms of β2-adrener-gic receptors influence bronchodilator responsiveness,we compared albuterol (INN, salbutamol)–evokedforced expiratory volume in 1 second (FEV1) in differ-ent genotypes. We report that albuterol-evokedincreases in FEV1 were higher and more rapid in Arg16homozygotes compared with the cohort of carriers ofthe Gly16 variant (heterozygotes [Arg16/Gly16] andGly16 homozygotes).
METHODSPatients. Fifteen black and 15 white patients with
moderate asthma (8 males and 7 females in each group)participated in this pharmacokinetic-pharmacodynamicstudy. The patients ranged from 18 to 50 years old, andall patients were clinically stable. Classification of apatient with moderate asthma was based on the guide-lines of the Expert Panel on the Management ofAsthma.16 Specifically, patients were required to bereceiving inhaled β2-agonists prn and inhaled cortico-
steroids. Patients taking other asthma medication orsystemic corticosteroids were excluded from the study.Daily inhaled corticosteroid use could not exceed thefollowing: 800 µg beclomethasone (INN, beclometa-sone), 800 µg triamcinolone, 1000 µg flunisolide, and660 µg for fluticasone. Patients withheld inhaled corti-costeroid therapy for 24 hours before the study andinhaled β-agonists for 12 hours before the study. Theyalso kept a diary of inhaled β2-adrenergic receptor ago-nist use for 3 days before the study. If they required use>3 times a day on any of those 3 days, they were stud-ied on a later date. Details of patient characteristics andstudy design have been published previously.17 Todetermine whether polymorphisms of the β2-adrener-gic receptor gene had any effect on the albuterol phar-macodynamics, we recalled the patients and asked themto volunteer a blood sample for determination of recep-tor genotype. Sixteen patients were genotyped; remain-ing patients either failed to respond to repeated calls,had moved from the area, or refused to participate. Thestudy protocol was approved by the University of Ten-nessee Institutional Review Board, and each subjectsigned informed written consent before participation inthe study. All studies were conducted in the Universityof Tennessee General Clinical Research Center.
Analytical and pharmacokinetic. Study patientsreported to the Clinical Research Center at 7 AM atwhich time they received a standard breakfast. Theywere instructed to abstain from caffeine and alcohol forat least 12 hours before the study and throughout thestudy day, as well as to avoid all over-the-counter med-ications for 24 hours before the study. Blood samplesfor determination of plasma albuterol concentrationswere collected in heparinized tubes at zero,1⁄2, 1, 11⁄2,2, 21⁄2, 3, 31⁄2, 4, 6, 8, 10, and 12 hours after administra-tion of an oral solution that contained 8 mg albuterol.Albuterol plasma concentrations were determined byHPLC with fluorescence detection as described previ-ously,17 with use of a modification of a publishedassay.18 The lower limit of detection was 0.5 µg/L.Intraday and interday coefficients of variation were<10%. Linearity was observed among albuterol con-centrations from 0.5 to 500 µg/L. The pharmacokinet-ics of albuterol in this patient population have been pub-lished previously.17
Spirometry. All subjects were trained before thestudy in the performance of standard spirometry on thebasis of the guidelines of the American Thoracic Soci-ety.19 Patients were coached vigorously and instructedto “blast” at the very start of the maneuver with con-tinuous coaching; the same coach was used throughoutthe study. FEV1 was determined by open circuit test-
520 Lima et alCLINICAL PHARMACOLOGY & THERAPEUTICS
MAY 1999

ing with a bedside spirometer (Spirometrics Flomate,model 2500) according to published standards.19 Thespirometer was calibrated on each study day with a 3-L syringe before the study was initiated. The time, date,temperature, and barometric pressure and each subject’srace, height, and study day’s weight were included inthe spirometer’s study profile. The method of Knudsonet al20 was selected for the calculation of predicted andreference values. Each subject used a nose clip and per-formed the spirometric maneuvers in the standing posi-tion. A minimum of 3 maneuvers was performed, witha minimum exhalation time of 6 seconds per maneu-ver, unless there was an obvious plateau (ie, no volumechange) for at least 1 second, or the subject could notexhale further. The paper printout of the volume-timeand flow-volume displays were subjected to otheracceptability criteria of the American Thoracic Society.Reproducibility was confirmed by ensuring that the dif-ference of the 2 largest FEV1 values from acceptablemaneuvers was less than 200 mL. Spirometry was per-formed just before and at 1, 2, 3, 4, 6, 8, 10, and 12hours after albuterol administration.
Determination of β2-adrenergic receptor genotype.β2-Adrenergic receptor genotype was determined bypolymerase chain reaction (PCR) with allele-specificoligonucleotide hybridization as described previously.7
In brief, 5 mL blood was collected in a blood collec-tion tube that contained ethylenediaminetetraacetic acidand stored at –20°C. Genomic DNA was extracted fromlymphocytes with a commercially available kit (Pure-gene, Gentra Systems, Inc, Minneapolis, Minn). PCRwas used to generate a 234-base pair fragment from the5´ end of the β2-adrenergic receptor, which spanned the2 polymorphisms of interest, as described by Dewar etal.7 The PCR primer sequences were as follows:upstream, 5´-CCC AGC CAG TGC GCT TAC CT-3´;downstream, 5´-CCG TCT GCA GAC GCT CGA AC-3´. Genomic DNA was denatured at 94°C for 5 min-utes followed by 60°C for 2 minutes; 2.5 units of Taqpolymerase was then added to the reaction mixture.PCR consisted of 35 cycles as follows: denature at 94°Cfor 90 seconds, anneal at 60°C for 90 seconds, extendat 72°C for 90 seconds, with final extension at 72°C for10 minutes. PCR product length was confirmed by useof a 2% agarose gel with ethidium bromide staining andthen blotted with a slot-blot apparatus. Membraneswere prehybridized with an unlabeled allele-specificoligonucleotide probe that was homologous for 1 formof the receptor, followed by hybridization with a biotin-labeled allele-specific oligonucleotide probe that washomologous for the other form of the receptor. A 10-fold excess of the Arg16 and Gly16 unlabeled probes
and 30-fold excess of Glu27 and Gln27 unlabeledprobes were used. Sequences for the allele-specificoligonucleotide probes were as follows: Arg16, GCAC-CCAATAGAAGCCATG; Gly16, GCACCCAATGG-AAGC CATG; Gln27, CACGCAGCAAAGGGAC-GAG; and Glu27, CACGCAGGAAAGGGACGAG.Both unlabeled and labeled probes were in 5× SSPEwith 1% sodium dodecyl sulfate (SDS); hybridizationwith the unlabeled probe was at 52°C for 30 minutes,followed by hybridization with the labeled probe at52°C for 60 minutes. Membranes were washed twicewith 2× SSPE and 0.1% SDS at 37°C for 30 minuteseach, followed by 2 washes of 15 minutes each with 5×SSPE and 0.1% SDS at 52°C. Detection of biotin wasaccomplished by chemiluminescence with use of acommercially available kit (Phototype-Star). β2-Adren-ergic receptor genotype in 4 subjects was confirmed bydirect dideoxysequencing.
Pharmacodynamics. Percentage changes in FEV1(%∆FEV1) from baseline (time 0) were calculated asfollows:
%∆FEV1 = 3 4 · 100
in which FEV1,TX and FEV1,R are values of FEV1 in thepresence of the drug and at 0 time (before drug admin-istration), respectively. The area under the response(%∆FEV1)–time curve (AURTC), and the area under theresponse–albuterol concentration curve (AURCC) weredetermined by the trapezoidal rule with use of the com-puter program WinNonLin (WinNonlin, ProfessionalEdition 1.5, Pharsight Corporation, Palo Alto, Calif). Theinitial slope of the %∆FEV1–albuterol concentrationrelationship (dE/dC) was determined by linear regres-sion of the response (%∆FEV1) versus the correspond-ing plasma albuterol concentration at 0 time and at 1 and2 hours after administration of the albuterol dose.
Statistical analysis. Response data were not distrib-uted normally; therefore differences in pharmacody-namics between cohorts were tested for statistical sig-nificance with the Mann-Whitney U test; differences inpretreatment FEV1 values and in areas under thealbuterol plasma concentration–time curve were testedwith the unpaired t test; differences in dE/dC weretested with a t test for comparing 2 slopes.21
RESULTSPatients. Nine women and 7 men participated in this
study; 8 were black and 8 were white. The mean ± SDage and weight were 32.5 ± 10.3 years and 84.3 ± 18.3kg, respectively. Five patients with asthma (31%) were
FEV1,TX – FEV1,R——FEV1,R
Lima et al 521CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 65, NUMBER 5

homozygous Arg16, 6 (38%) were Arg16/Gly16, and 5(31%) were homozygous Gly16; for codon 27, 1 (6%)was homozygous Glu27, 9 (56%) were heterozygous, and6 (38%) were homozygous Gln27. These proportions arewithin published values.4,6-12The mean ± SD predrugFEV1 in Arg16 homozygotes and Gly16 carriers weresimilar: 3.88 ± 1.31 L versus 3.09 ± 0.99 L (P = .22).
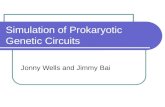
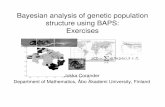
Pharmacodynamics. Figure 1 compares %∆FEV1and plasma concentrations as a function of time afteradministration of albuterol in Arg16 homozygotes andin carriers of the Gly16 variant. One hour after admin-
istration, albuterol maximally increased FEV1 to agreater extent in Arg16 homozygotes compared withthe cohort of Gly16 carriers: 18% versus 4.9% (P <.03). The median AURTC values were higher in Arg16homozygotes compared with Gly16 carriers: 161%/h(range, 36%/h to 190%/h) versus 32.5%/h (range,–428%/h to 142%/h), respectively (P < .05). Differ-ences in AURTC values between heterozygotes andGly16 homozygotes did not achieve statistical signifi-cance. Plasma albuterol concentrations in both cohortswere similar.
522 Lima et alCLINICAL PHARMACOLOGY & THERAPEUTICS
MAY 1999
Figure 1. Comparison of median FEV1 (top) and mean ± SE albuterol plasma concentrations ver-sus time after administration of a single 8-mg oral dose of albuterol in Arg16 homozygotes (solidcircles)and in heterozygotes and Gly16 homozygotes (open circles).

Peak %∆FEV1 values were observed earlier thanpeak plasma albuterol concentrations in some patients,whereas in other patients peak response and plasmaconcentrations were observed at the same time. β2-Adrenergic receptor genotype had no effect on the tim-ing of peak response relative to plasma concentrations.
The effect of the β2-adrenergic receptor genetic poly-morphism on the relationship between albuterol plasmaconcentrations and bronchodilator response is summa-rized in Table I. Values for dE/dC were higher (P <.003) and AURCC values were greater (P < .05) inArg16 homozygotes compared with carriers of theGly16 form of the receptor. Differences in AURCC val-ues between heterozygotes and carriers of the Gly16variant did not achieve statistical significance. No effecton albuterol-evoked FEV1 was observed at codon 27 ofthe β2-adrenergic receptor.
DISCUSSIONTo our knowledge, our study is the first to report that
a genetic polymorphism of the human β2-adrenergicreceptor can influence the bronchodilator response ver-sus β2-agonist plasma concentration relationship. Previ-ous studies compared responsiveness to inhaled doses ofβ2-agonist in different genotypes.6,9,12,13Patients withasthma who were homozygous for the Arg16 alleleshowed more rapid increases in response and a higherbronchodilator response (%∆FEV1) 1 hour after drugadministration than the cohort of patients with asthmathat carried the Gly16 form of the receptor. Moreover,areas under the FEV1–time curve and the FEV1–albuterolconcentration curve were higher in Arg16 homozygotesat equivalent plasma concentrations.Our data clearlyestablish that the genetic polymorphism of the β2-adren-ergic receptor at codon 16 is a major determinant of bron-chodilator response to albuterol.
Attempts to associate genetic polymorphisms of theβ2-adrenergic receptor with responsiveness to β2-agonist administration have met with mixed results. In astudy of both patients without asthma and patients with
asthma, FEV1 values were compared before and 15 min-utes after inhalation of 180 µg of albuterol.9 Comparedwith Gly16 homozygotes, Arg16 homozygotes were 5.3times more likely to respond to an inhaled dose ofalbuterol, with heterozygotes having an intermediatevalue. Tan et al6 compared bronchodilator responsivenessto inhaled doses of formoterol (6 to 108 µg) in patientswith moderately severe asthma after 4 weeks of for-moterol, 24 µg twice a day, and placebo. They reported agreater degree of bronchodilator desensitization in Gly16homozygotes compared with heterozygotes and Arg16homozygotes. These studies are consistent with the ideathat carriers of the homozygous Arg16 form of the recep-tor show less agonist-promoted receptor down-regulationthan heterozygotes or Gly16 homozygotes.
However, different results were reported in otherstudies.12,13In a previous study, Sears et al22 reportedthat most patients with asthma experienced deteriora-tion in asthma control during regular inhaled fenoteroltreatment compared with placebo treatment. In a fol-low-up study,12 they hypothesized that patients withasthma whose asthma control deteriorated would carrythe form of the receptor that showed enhanced agonist-promoted down-regulation (Gly16). However, no asso-ciation between receptor genotype and asthma controlwas observed. Furthermore, Gly16 homozygotes hadno increase in bronchial responsiveness to metha-choline during regular treatment, whereas heterozy-gotes and Arg16 homozygotes did have an increase. Inaddition, Glu27 homozygotes had no increase inevening peak expiratory flow rates during regular treat-ment, whereas heterozygotes and Gln27 homozygotesdid have an increase in flow rates. Aziz et al13 reportedthat β2-adrenergic receptor genotype had no influenceon FEV1 evoked by inhaled formoterol, although Arg16 homozygotes were underestimated in this study.These data are clearly not consistent with in vitro14,15
and in vivo studies.6,9
The reasons for this discrepancy among the in vivostudies are unknown; however, one possible explana-
Lima et al 523CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 65, NUMBER 5
Table I. Effect of β2-adrenergic receptor genotype on bronchodilator response to albuterol
Pharmacodynamic index
AURCC (% · mL/ng)
Receptor genotype dE/dC (% · mL/ng) Median Range
Homozygous Arg16 1.42* 194 45.1-237*Heterozygous and homozygous Gly16 0.55 30 –337-146
dE/dC, Initial slope of the FEV1–albuterol concentration curve; AURCC, area under the FEV1 response–albuterol concentration curve.*P < .05.

tion may be related to the assessment of bronchodila-tor response to inhaled doses of β2-agonists. Bron-chodilator response to β2-agonist is determined by thestate of the β2-adrenergic receptor–effector system (inpart determined by genotype) and by β2-agonist con-centrations at the receptor. β2-Agonist concentrationsat the receptor might have varied considerably becauseof different fractions of the inhaled dose reaching theeffect site and because of interpatient variability in thepharmacokinetics of the agonists. It is possible that dif-ferent agonist concentrations at the β2-receptor wereachieved, resulting in different levels of response. Inour study, FEV1 was related to plasma concentrationsachieved after the oral administration of a single doseof albuterol, which presumably reflect concentrationsof albuterol at the β2-adrenergic receptor. By relatingresponse to plasma concentrations, we removed phar-macokinetic variability as a response variable. The datain our study clearly establish that patients with asthmawho are homozygous for the Arg16 form of the β2-receptor respond better to albuterol than carriers of theGly16 variant.
The results of our study are consistent with expecta-tions one can infer from in vitro studies. Green et al14
studied the functional consequences of β2-adrenergicreceptor gene polymorphism by site-directed mutagen-esis and the recombinant expression of β2-adrenergicreceptor 16 and 27 forms in Chinese hamster fibro-blasts. Agonist-promoted down-regulation of the Gly16variant was enhanced compared with the Arg16 form,whereas the Glu27 form was resistant to down-regula-tion. Similar results were reported in primary culturesof human airway smooth muscle cells.15 These studiessupport the idea that Arg16 homozygotes should bemore responsive to agonist-induced bronchodilationthan Gly16 homozygotes and heterozygotes becausethe Arg16 variant undergoes less agonist-promoteddown-regulation. In the present study, Arg16 homozy-gotes responded more rapidly and to a greater extentthan Gly16 carriers at equivalent albuterol plasma con-centrations. Thus the most likely explanation for ourfindings is that Arg16 homozygotes had less receptordown-regulation than heterozygotes and Gly16homozygotes, although differences in receptor affini-ties cannot be disregarded.
The impact of the Glu27 polymorphism on agonist-evoked bronchodilation is less clear. Although cells thatexpress the Glu27 variant were resistant to agonist-promoted down-regulation, cells that coexpress theGly16 and Glu27 variants were down-regulated to thesame extent as the wild-type (Arg16/Gln27).14 Thesedata suggested that the enhanced down-regulation asso-
ciated with the Gly16 form of the receptor prevailedover the resistance to down-regulation associated withthe Glu27 variant. In support of this finding, Tan et al6
reported that although more desensitization wasobserved in Glu27 homozygotes, they were all Gly16.The small number of patients in our study limited ourability to detect whether polymorphisms at codon 27influences bronchodilator response to albuterol. Only 1patient was homozygous Glu27; however, he was alsohomozygous Gly16. He had the highest response–concentration profile of the patients with asthma whowere heterozygous at codon 16 or homozygous Gly16,with a maximal FEV1 of 26% above resting FEV1. Theeffect of the Glu27 variant on the bronchodilatorresponse versus plasma β2-agonist–concentration rela-tionship requires further study. However, the impact ofthe genetic polymorphism at codon 27 on agonist-evoked response may be difficult to evaluate because itis in linkage disequilibrium with the codon 16 polymor-phism.9,10,12
In some patients, FEV1 peaked earlier than plasmaconcentrations of albuterol, indicating the presence ofa clockwise hysteresis in the response versus concen-tration relationship. Clockwise hysteresis was a promi-nent feature of the response versus concentration rela-tionship in patients who have different genotypes atcodon 16; this will be the subject of a future report.
In summary, our data clearly establish that the Arg16polymorphism is a major determinant of bronchodila-tor response to albuterol. Moreover, our data implicatethe β2-adrenergic receptor gene polymorphism as amajor contributor to interpatient variability in bron-chodilator responsiveness to β2-adrenergic receptoragonist treatment. We conclude that future pharmaco-dynamic studies of β2-adrenergic receptor agonistsshould include determination of β2-adrenergic receptorgenotype.
References
1. Morgan DJ. Clinical pharmacokinetics of beta-agonists.Clin Pharmacokinet 1990;18:270-94.
2. Lohse MJ. Molecular mechanisms of membrane receptordesensitization. Biochim Biophys Acta 1993;1179:171-88.
3. Reihsaus E, Innis M, MacIntyre N, Liggett SB. Mutationsin the gene encoding for the beta 2-adrenergic receptorin normal and asthmatic subjects. Am J Respir Cell MolBiol 1993;8:334-9.
4. Turki J, Pak J, Green SA, Martin RJ, Liggett SB. Geneticpolymorphisms of the beta 2-adrenergic receptor in noc-turnal and nonnocturnal asthma: evidence that Gly16 cor-relates with the nocturnal phenotype. J Clin Invest1995;95:1635-41.
524 Lima et alCLINICAL PHARMACOLOGY & THERAPEUTICS
MAY 1999

5. Hall IP, Wheatley A, Wilding P, Liggett SB. Associationof Glu27 beta 2-adrenoceptor polymorphism with lowerairway reactivity in asthmatic subjects. Lancet 1995;345:1213-4.
6. Tan S, Hall IP, Dewar J, Dow E, Lipworth B. Associationbetween beta 2-adrenoceptor polymorphism and suscepti-bility to bronchodilator desensitisation in moderately severestable asthmatics [see comments]. Lancet 1997;350:995-9.
7. Dewar JC, Wilkinson J, Wheatley A, Thomas NS, DoullI, Morton N, et al. The glutamine 27 β2-adrenoceptor poly-morphism is associated with elevated IgE levels in asth-matic families. J Allergy Clin Immunol 1997;100:261-5.
8. Liggett SB. Polymorphisms of the β2-adrenergic recep-tor and asthma. Am J Respir Crit Care Med 1997;156:S156-62.
9. Martinez FD, Graves PE, Baldini M, Solomon S, Erick-son R. Association between genetic polymorphisms ofthe β2-adrenoceptor and response to albuterol in childrenwith and without a history of wheezing. J Clin Invest1997;100:3184-8.
10. Large V, Hellstrom L, Reynisdottir S, Lonnqvist F, Eriks-son P, Lannfelt L, et al. Human β2-adrenoceptor genepolymorphisms are highly frequent in obesity and asso-ciate with altered adipocyte β2-adrenoceptor function. JClin Invest 1997;100:3005-13.
11. Hopes E, McDougall C, Christie G, Dewar J, WheatleyA, Hall IP, et al. Association of glutamine 27 polymor-phism of β2-adrenoceptor with reported childhoodasthma: population based study. BMJ 1998;316:664.
12. Hancox RJ, Sears MR, Taylor DR. Polymorphism of theβ2-adrenoceptor and the response to long-term beta2-ago-nist therapy in asthma. Eur Respir J 1998;11:589-593.
13. Aziz I, Hall IP, McFarlane LC, Lipworth BJ. β2-Adreno-ceptor regulation and bronchodilator sensitivity after reg-
ular treatment with formoterol in subjects with stableasthma. J Allergy Clin Immunol 1998;101:337-41.
14. Green SA, Turki J, Innis M, Liggett SB. Amino-terminalpolymorphisms of the human β2-adrenergic receptorimpart distinct agonist-promoted regulatory properties[published erratum appears in Biochemistry 1994;33:14368]. Biochemistry 1994;33:9414-9.
15. Green SA, Turki J, Bejarano P, Hall IP, Liggett SB. Influ-ence of β2-adrenergic receptor genotypes on signal trans-duction in human airway smooth muscle cells. Am JRespir Cell Mol Biol 1995;13:25-33.
16. National Asthma Education and Prevention Program.Expert Panel Report: Guidelines for the diagnosis andmanagement of asthma. Bethesda (MD): National Insti-tutes of Health; 1991. Publication no 91-3042.
17. Mohamad M, Lima JJ, Eberle LV, Self TH, Johnson JA.Effects of gender and race on albuterol pharmacokinet-ics. Pharmacotherapy 1999;19:157-61.
18. Gupta RN, Fuller HD, Dolovich MB. Optimization of acolumn liquid chromatographic procedure for the deter-mination of plasma salbutamol concentration. J Chro-matogr B Biomed Appl 1994;654:205-11.
19. Standardization of spirometry, 1994 Update. AmericanThoracic Society. Am J Respir Crit Care Med 1995;152:1107-36.
20. Knudson RJ, Schroter RC, Knudson DE, Sugihara S.Influence of airway geometry on expiratory flow limita-tion and density dependence. Respir Physiol 1983;52:113-23.
21. Zar JH. Biostatistical analysis. 2nd ed. Englewood Cliffs(NJ): Prentice Hall; 1984.
22. Sears MR, Taylor DR, Print CG, Lake DC, Li QQ, FlanneryEM, et al. Regular inhaled β-agonist treatment in bronchialasthma [see comments]. Lancet 1990;336:1391-6.
Lima et al 525CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 65, NUMBER 5