Pirfenidone alleviates pulmonary fibrosis in vitro and in ...

JOURNAL OF INTERFERON & CYTOKINE RESEARCH 26:71–75 (2006)© Mary Ann Liebert, Inc.
IL-8 and IFN-� in Tear Fluid of Patients with Cystic Fibrosis
MALGORZATA MRUGACZ,1 MACIEJ KACZMARSKI,2 ALINA BAKUNOWICZ-LAZARCZYK,1
BEATA ZELAZOWSKA,3 JOLANTA WYSOCKA,3 and ALINA MINAROWSKA2
ABSTRACT
Cystic fibrosis (CF) is inherited as an autosomal recessive disorder. It is caused by mutations in the protein-coding gene of chromosome 7, resulting in chronic pulmonary disease and pancreatic insufficiency. The dis-ease affects all secretory epithelia, including the eye. The pathogenesis of ocular changes in CF is still un-known, but the involvement of immunologic processes in patients with CF has been studied in recent years.We measured interleukin-8 (IL-8) and interferon-� (IFN-�) levels in tears in a group of patients and a groupof normal controls to determine if the levels of these cytokines are elevated in CF. The levels of these cyto-kines in tears and the clinical severity of CF and eye disease were compared. Tear samples were collectedfrom 24 patients with CF at the department of pediatric diseases, Medical University of Bialystok, Poland.Cytokine levels were determined by ELISA. Ophthalmic examinations, including tests for keratoconjunctivi-tis sicca (dry eye), were used to study the ocular surface. The tear levels of IL-8 and IFN-� in the CF patientswere significantly higher than those in controls. The clinical severity of CF correlated significantly with theIL-8 and IFN-� levels. We found positive correlation between the tear levels of IFN-� and dry eye findingsin CF patients. Our results suggest that the inflammatory cytokines IL-8 and IFN-� may play key roles in theregulation of ocular surface inflammation and the immunologic reaction in patients with CF. The tear levelsof IL-8 and IFN-� may be candidate markers for evaluation of the clinical status of CF and eye disease. Thesefindings help to provide a new insight into the pathogenesis of dry eye in patients with CF and provide po-tential targets for therapy.
71
INTRODUCTION
CYSTIC FIBROSIS (CF) is a relatively common autosomal re-cessive disorder, affecting 1 of every 2005 live births in Cau-
casians.1,2 The defect is due to mutations in a 230-kb gene onchromosome 7 encoding a 1480-amino acid polypeptide, the CFtransmembrane regulator (CFTR), which functions as a chloridechannel in epithelial membranes.3,4 To date, over 1000 mutant al-leles have been identified.5 The most common mutation, �F508,results from deletion of a phenylalanine residue at codon 508 inthe CFTR. This mutation causes a severe reduction in CFTR func-tion and leads to the classic CF phenotype of raised sweat chlo-ride, recurrent respiratory infection with bronchiectasis, and early-onset pancreatic insufficiency.1,6,7 It is presumed that the diseaseaffects all secretory epithelia, including the eye. Apical localiza-tion of CFTR in the conjunctival epithelium is consistent with thefunction of this protein as a chloride channel or as a regulator ofchannel activity.8
The involvement of immunologic processes in patients withCF has been studied in recent years. CFTR dysfunction may
affect proinflammatory and anti-inflammatory balance.9–11 Ev-idence suggests that airway inflammation in CF is associatedwith increased production of proinflammatory cytokines in thelung. Airway epithelial cells, macrophages, and neutrophils areall capable of producing cytokines. Several studies have foundelevated concentrations of such proinflammatory cytokines asinterleukin-1 (IL-1), IL-6, and IL-8 in the sputum, bron-choalveolar lavage (BAL) fluid, blood, and nasal secretions ofpatients with CF and production of massively high levels of IL-8 by CF lung epithelial cells.11–16 Their synthesis is pro-moted by the transcription factor nuclear factor-�B (NF-�B),which plays an important role in intracellular signaling for theproduction of proinflammatory cytokines.17,18 IL-8 is a proto-typical chemokine (CXC subfamily) and a potent proinflam-matory cytokine that can be released by both epithelial cellsand fibroblasts at a number of body surfaces.19,20 It plays a cru-cial role in inflammation through its capacity to recruit T cellsand nonspecific inflammatory cells into sites of inflammationand its capacity to activate neutrophils, for example, in the up-per airways of CF patients.14,21,22
1Department of Pediatric Ophthalmology, 2Department of Childhood Diseases, and 3Department of Pediatric Laboratory Diagnostic, MedicalUniversity of Bialystok, 15-274 Bialystok, Poland.

Secretion of IL-8 in human bronchial epithelial cells is inducedby interferon-� (IFN-�).23,24 Excessive production of IFN-� ischaracteristic of immune responses mediated predominantly byTh1 lymphocytes.25 IFN-� plays an important role in the patho-genesis of inflammatory diseases and induces antiviral and an-
tiproliferative activities, stimulates macrophages, and controls theexpression of several adhesion molecules and surface cell re-ceptors, several cytokines, and major histocompatibility complex(MHC) class I and II molecules.26–28
Ocular tissues, such as conjunctival cells,29–31 corneal cells32
MRUGACZ ET AL.72
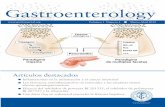
FIG. 1. Tear IL-8 levels in CF patients and normal controls. There was a significant difference between CF patients and con-trols, p � 0.001, Wilcoxon’s sum rank test.
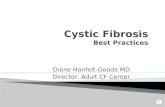
FIG. 2. Tear IFN-� levels in CF patients and normal controls. There was a significant difference between CF patients and con-trols, p � 0.001, Wilcoxon’s sum rank test.

and the tear fluid,31,33–35 are an important source of cytokinesthat regulate inflammation. The purpose of this study was toevaluate the level of the inflammatory cytokines IL- 8 and IFN-� in the tear fluid in patients with CF. We also investi-gated the correlation between levels of these cytokines in tearsand clinical severity of CF and eye disease.
MATERIALS AND METHODS
We studied 24 patients with CF at the III Department of Pedi-atric Diseases, Medical University of Bialystok, Poland, betweenMarch and December 2004. The studies were conducted accord-ing to the principles established in the declaration of Helsinki. In-formed consent was obtained from their patients or from the par-ents before sample collection. Tear samples were obtained from 15male and 9 female CF patients with a mean age of 14.21 years(range 6–20) and from 14 male and 10 female normal controls witha mean age of 14.85 years (range 7–21). At the time of examina-tion, all the CF patients were receiving vitamin A supplementation,15 were receiving oral pancreatic enzyme, 13 were receiving oralcarbocysteine, and 11 were using an n-acetyl cysteine inhaler.
The clinical status was scored according to Schwachmann andKulczycki36 (Schwachman score, scale 100–0: 100, excellent;100–55, without pulmonary insufficiency; �55, severe of CF).36
Tear samples were collected in graduated 30-�L disposablemicrocapillaries (ACCUFILL 90 MICROPET, Becton Dickin-son, Franklin Lakes, NJ) unilaterally or bilaterally from the con-junctival cul-de-sac without anesthesia. Care was taken to avoidtouching the lid margin or corneal surface. We collected 10–30�L (mean 20 �L) of basal tears from each eye. The cytokinelevels in tears were determined by ELISA. Highly sensitive im-munoassay kits for IL- 8 and IFN-� (Quantikine HS, R&D Sys-tems, Minneapolis, MN, and Pierce Endogen system, Rockford,IL, respectively) were used; the sensitivity was �3.5 pg/mL forIL- 8 and �2 pg/mL for IFN-�. The procedures recommendedby the manufacturer were followed without any modification.For IL-8 and IFN-� ELISA assays, 50–100 �L tears wasneeded. Pooled samples were collected two or three times at4–6-min intervals (in 2–3 days). The collected tears were im-mediately frozen to �80°C and thawed just before assaying.All samples were coded and read blind in the assay.
Subject complaints, such as redness, foreign body sensation, ir-ritation, intense burning, and blurred vision, were noted. The ex-ternal surface of the eye was examined using a slitlamp. Both pa-tients and controls were tested for keratoconjunctivitis sicca. Tearbreak-up time (TBUT) was measured to assess tear film stability.A value of �10 sec was abnormal. The Schirmer test was used toestimate tear film quantity; a value of �5 mm after 5 min was ab-
IL-8 AND IFN-� IN TEARS OF CF PATIENTS 73
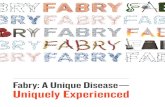
FIG. 3. Correlation between severity of CF and tear IL-8 lev-els in CF patients. Spearman’s correlation test: 2, coded as num-ber of patients with severe CF; 1, coded as number of patientswith mild CF. (Top) Positive correlation between severe CF(R � 0.869, p � 0.001) and IL-8 levels. (Bottom) Negativecorrelation between mild CF and tear IL-8 levels in CF patients(R � �0.817, p � 0.001).
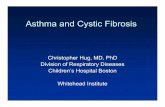
FIG. 4. Correlation between severity of CF and IFN-� levelsin CF patients. Spearman’s correlation test: 2, coded as num-ber of patients with severe CF; 1, coded as a number of patientswith mild CF. (Top) Positive correlation between severe CFand IFN-� levels in CF patients (R � 0.662, p � 0.001) (Bot-tom). Negative correlation between mild CF and IFN-� levelsin CF patients (R � �0.662, p � 0.001).

normal. Lissamine green was instilled into the inferior fornix toassess the amount of dead epithelial cells at the ocular surface. Iftwo of these variables were abnormal, dry eye was the diagnosis.37
Statistical analysis
Nonparametric analysis was conducted in this study.Wilcoxon’s sum rank test was used to identify differences be-tween tear cytokine levels in patients group and controls. Spear-man’s rank correlation test was used to establish the signifi-cance of correlation between tear cytokine levels and severityof CF and eye disease. A level of p � 0.05 was accepted as sta-tistically significant.
RESULTS
The IL-8 tear levels in patients with CF were 1023.99 � 365.04pg/mL (mean � SD), and in normal controls were 271.04 � 53.30pg/mL (Fig. 1). The tear levels of IL-8 in the CF patients weresignificantly higher when compared with healthy controls (p �0.001). The tear levels of IFN-� in patients with CF were 10.25 �1.49 pg/mL, whereas in normal controls, they were 4.00 � 1.10pg/mL (Fig. 2). The IFN-� levels in CF patients were significantlyhigher than in the controls (p � 0.001).
Symptoms of pulmonary insufficiency (�55 according to theSchwachmann-Kulczycki score) were found in 45% (11 of 24)of the CF patients. The Spearman correlation coefficient indi-cated a positive correlation between the tear levels of IL-8 andsevere clinical status of CF patients (R � 0.869, p � 0.001) (Fig.3), whereas a negative correlation was found between the tearlevels of IL-8 and mild CF (R � �0.817, p � 0.001) (Fig. 3).Dry eye symptoms, according to the Copenhagen criteria,37 wereobserved in 8 (33%) CF patients with elevated concentrations ofIL-8. A negative correlation was found between the tear levelsof IL-8 and the presence dry eye changes in CF patients (R �0.115, p � 0.529). As shown in Figure 4, severe CF correlatedsignificantly with IFN-� levels (R � 0.662, p � 0.001), but therewas a negative correlation between the tear levels of IFN-� andmild clinical status of CF patients (R � �0.662, p � 0.001).Thirteen of our CF patients (55%) with high levels of IFN-� hadclinical evidence of dry eye. The Spearman correlation coeffi-cient indicated a positive correlation between the tear levels ofIFN-� and dry eye findings in CF patients.
DISCUSSION
To the best of our knowledge, tears have not previously beeninvestigated for the presence of inflammatory cytokines in CFpatients. This study demonstrated that the chemokines IL-8 andIFN-� were present at high levels in CF patients’ tears.
High levels of IL-8 were found especially in patients with se-vere CF. Such high levels suggest that IL-8 may be produced lo-cally and may be used in evaluation of the clinical status of CF.Elaboration of IL-8 by resident tissues is an important mechanismfor directing leukocytes to migrate, especially through tissueswithout blood vessels. High levels of IL-8 have been regarded asa pathogenic cause of human and experimental inflammatory dis-eases and intraocular inflammation.22,38,39 In vitro and in vivostudies on epithelial cells of the airways of patients with respira-tory inflammation in CF indicate that inflammation plays an im-
portant role in its pathogenes.9 Inflammation appears to have arole in the pathogenesis of the ocular surface epithelial disease,keratoconjunctivitis sicca, that develops in dry eye patients.31 Itis known that ocular changes in CF patients occur mainly in thetear film, which is associated with general dysfunction of exocrineglands, and pertain to tear hyposecretion and abnormal composi-tion of tears. These are dry eye symptoms, which, according tosome authors, are the primary CF manifestations.40
IFN-� plays a significant role in the pathogenesis of in-flammatory disorders, including Sjögren’s syndrome,41,42 inwhich this cytokine is one of the principal molecules responsi-ble for stimulation of salivary, conjunctival, and lacrimal ex-pression of inflammation-related adhesion molecules, includingHLA-DR and intracellular adhesion molecule-1 (ICAM-1).29
The levels of each of these molecules should be evaluated infuture studies. As IFN-� activates macrophages, inflammatorycytokines, such as IL-6 and IL-8, are released in excess duringinitiation of the cytokine cascade in inflammation.26 Stimula-tion of the conjunctival epithelium with the proinflammatorymediators IFN-� and tumor necrosis factor-� (TNF-�) couldhave generated the release of chemotactic factors, such as IL-8, which could act to prolong inflammation.41
In the present study, there was a positive correlation be-tween tear levels of IL-8 and IFN-� and severe CF. There alsowas a negative correlation between the tear levels of the cyto-kines and mild CF. Our findings indicate that high levels ofIFN-� and IL-8, especially in tears of patients with severe CF,reflect the degree of local immunologic abnormality and areassociated with the severity of the clinical status of this dis-ease. We observed a positive correlation between the tear lev-els of IFN-� and the dry eye findings in CF patients. IFN-�might be useful as a reliable marker of clinical inflammationin CF patients.
In conclusion, the results of this study demonstrate that in-creased levels of inflammatory cytokines in the tear fluid mayplay an important role in the pathogenesis of dry eye in patientswith CF. The tear levels of IL-8 and IFN-� may be candidatemarkers to evaluate the clinical status of CF and eye disease.Our findings may contribute to further understanding of localand systemic immune responses and might lead to the devel-opment of new clinical approaches to inflammatory disorders.In addition, our observations may provide new specific targetsfor therapeutic intervention.
ACKNOWLEDGMENT
This work was supported by a grant from the Polish StateCommittee for Scientific Research (KBN, No. 3 P05E 04725).
REFERENCES
1. Welsh M, Ramsey B, Accurso F, Cutting G. Cystic fibrosis. In:Scriver CR, Beaudet AL, Sly WS, Valle D, eds. The Metabolic andMolecular Basis of Inherited Disease, 8th ed. New York: McGraw-Hill; 2001:5121–588.
2. Ratjen F, Doring G. Cystic fibrosis. Lancet 2003;361:681–689.3. Riodan JR, Rommens JM, Kerem B. Identification of the cystic fi-
brosis gene: cloning and characterization of complementary DNA.Science 1989;245:1066–1073.
MRUGACZ ET AL.74

4. Zielinski J, Rozmahel R, Bozon D. Genomic DNA sequence of thecystic fibrosis transmembrane conductance regulator. Genomics1991;10:241–248.
5. The Cystic Fibrosis Genetic Analysis Consortium. Cystic FibrosisMutation Data Base. www.genet.sickkids.on.ca/cftr/ Accessed No-vember 26, 2002.
6. Leigh MW. Diagnosis of CF despite normal or borderline sweatchloride. Paediatr. Respir. Rev. 2004;5:357–359.
7. McKone EF, Emerson SS, Edwards KL, Aitken ML. Effect ofgenotype on phenotype and mortality in cystic fibrosis: a retro-spective cohort study. Lancet 2003;361:1671–1676.
8. Turner HC, Bernstein A, Candia OA. Presence of CFTR in the con-junctival epithelium. Curr. Eye Res. 2002;24:182–187.
9. Muhlebach MS, Noah TL. Endotoxin activity and inflammatorymarkers in the airways of young patients with cystic fibrosis. Am.J. Respir. Care Med. 2002;165:911–915.
10. Sagel SD, Accurso FJ. Monitoring inflammation in CF. Cytokines.Clin. Rev. Allergy Immunol. 2002;23:41–57.
11. Richman-Eisenstadt J. Cytokine soup: making sense of inflamma-tion in cystic fibrosis. Pediatr. Pulmonol. 1996;21:3–5.
12. Colombo C, Constantini D, Rocchi A, Cariani L, Tirelli S, CaloriG, Copreni E, and Conese M. Cytokine levels in sputum of cysticfibrosis patients before and after antibiotic therapy. Pediatr. Pul-monol. 2005;40:15–21.
13. Terheggen-Lagro SW, Rijkers GT, Van Der Ent CK. The role of air-way epithelium and blood neutrophils in the inflammatory responsein cystic fibrosis. J. Cystic Fibrosis 2005;17 [Epub ahead of print].
14. Bergoin C, Gosset P, Lamblin C, Bolard F, Turck D, Tonnel AB,Wallaert B. Cell and cytokine profile in nasal secretions in cysticfibrosis. J. Cystic. Fibrosis 2002;1:110–115.
15. Brazova J, Sediva A, Pospisilova D, Vavrova V, Pohunek P, MacekM, Bartunkova J, Lauschmann H. Differential cytokine profile inchildren with cystic fibrosis. Clin. Immunol. 2005;115:210–215.
16. Courtney JM, Ennis M, Elborn JS. Cytokines and inflammatorymediators in cystic fibrosis. J. Cystic Fibrosis 2004;3:223–231.
17. Barnes TL, Konstan MW. Nuclear factor �B–a pivotal transcrip-tion factor in chronic inflammatory diseases. N. Engl. J Med.1997;336:1066–1071.
18. Joseph T, Look D, Ferkol T. NF-kappaB activation and sustainedIL-8 gene expression in primary cultures of cystic fibrosis airwayepithelial cells stimulated with Pseudomonas aeruginosa. Am. J.Physiol. Lung Cell. Mol. Physiol. 2005;288: L471–479.
19. Murphy PM. Neutrophil receptors for interleulin-8 and related CXCchemokines. Semin. Hematol. 1997;34:311–318.
20. Larsen CG, Anderson AO, Oppenheim JJ, Matsushima K. Pro-duction of interleukin-8 by human dermal fibroblasts and ker-atinocytes in response to interleukin-1 or tumor necrosis factor. Im-munology 1989;68:31–36.
21. Gern JE, Martin MS, Anclam KA. Relationships among specificviral pathogens, virus-induced interleukin-8, and respiratory symp-toms in infancy. Pediatr. Allergy Immunol. 2002;13:386–393.
22. Reato G, Cuffini AM, Tullio V. Immunomodulating effect of anti-microbial agents on cytokine production by human polymorphonu-clear neutrophils. Int. J. Antimicrob. Agents 2004;23:150–154.
23. Striz I, Mio T, Adachi Y, Carnevali S, Romberger DJ, Rennard SI.Effects of interferons alpha and gamma on cytokine production andphenotypic pattern of human bronchial epithelial cells. Int. J. Im-munopharmacol. 2000;22:573–585.
24. Nakamura H, Yoshimura K, Jaffe HA, Crystal RG. Interleukin-8gene expression in human bronchial epithelial cells. J. Biol. Chem.1991;266:19611–19617.
25. Del Prete G. The concept of type 1 and type 2 helper T cells andtheir cytokines in humans. Int. Rev. Immunol. 1998;16:427–455.
26. De Maeyer E, De Mayer-Guignard J. Interferon-�. Curr. Opin. Im-munol. 1992;4:321–332.
27. Gabrielian K, Osusky R, Sippy BD, Ryan SJ, Hinton DR. Effectof TGF-beta on interferon-gamma-induced HLA-DR expression in
human retinal pigment epithelial cells. Invest. Ophthalmol. Vis. Sci.1994;35:4253–4259.
28. Watanabe Y, Jacob CO. Regulation of MHC class II antigen ex-pression opposing effects of tumor necrosis factor-� on IFN-�-in-duced HLA-DR and Ia expression depends on the maturation anddifferentiation stage of the cell. J. Immunol. 1991;146:899–905.
29. Baudouin C, De Saint Jean M, Brignole F. Expression of apoptoticand inflammatory markers in the human conjunctival epithelium(ARVO Abstract). Invest. Ophthalmol. Vis. Sci. 1998;39:551.
30. Miyoshi T, Fukagawa K, Shimmura S. Interleukin-8 concentrationsin conjunctival epithelium brush cytology samples correlate withneutrophil, eosinophil infiltration, and corneal damage. Cornea2001;20:743–747.
31. Pflufelder SC, Jones D, Ji Z. Altered cytokine balance in the tearfluid and conjunctiva of patients with Sjögren’s syndrome kerato-conjunctivitis sicca. Curr. Eye Res. 1999;19:201–211.
32. Cubbit CL, Tang Q, Monteiro CA. IL-8 gene expression in cul-tures of human corneal epithelial cells and keratocytes. Invest. Oph-thalmol. Vis. Sci. 1993;34:3199–3206.
33. Uchio E, Ono SY, Ikezawa Z, Ohno S. Tear levels of interferon-�, interleukin (IL)-2, IL-4 and IL-5 in patients with vernal kerato-conjunctivitis, atopic keratoconjunctivitis and allergic conjunctivi-tis. Clin. Exp. Allergy 2000;30:103–109.
34. Thakur A, Willcox MDP. Cytokine and lipid inflammatory medi-ator profile of human tears contact lens associated inflammatorydiseases. Exp. Eye Res. 1998;67:9–19.
35. Thakur A, Willcox MDP, Stapleton F. The proinflammatory cyto-kines and arachidonic acid metabolites in human overnight tears:homeostatic mechanisms. J. Clin. Immunol. 1998;18:61–70.
36. Schwachmann H, Kulczycki LL. Long-term study of 105 patientswith cystic fibrosis. Studies made over a 5 to 14 year period. Am.J. Dis. Child. 1958;96:6–15.
37. Manthorpe R, Oxholm P, Prause JU. The Copenhagen criteria forSjögren’s syndrome. Scand. J. Rheumatol. (Suppl.) 1986;61:19–21.
38. Peichl P, Cheska M, Effenberger F. Presence of NAP-1/IL-8 insynovial fluids indicates a possible pathogenic role in rheumatoidarthritis. Scand. J. Immunol. 1991;34:333–339.
39. Brito BE, O’Rourke LM, Pan Y. Murine endotoxin-induced uveitis,but not immune complex-induced uveitis, is dependent on the IL-8 receptor homolog. Curr. Eye Res. 1999;19:76–85.
40. Ansari EA, Sahni K, Etherington CH. Ocular signs and vitamin Astatus in patients with cystic fibrosis treated with daily vitamin Asupplements. Br. J. Ophthalmol. 1999;83:688–691.
41. Hagendorens MM, Van Bever HP, Schuerwehg AJ. Determinationof T-cell subpopulations and intracellular cytokine production (in-terleukin-2, interleukin-4, and interferon-gamma) by cord blood T-lymphocytes of neonates from atopic and non-atopic parents. Pe-diatr. Allergy Immunol. 2000;11:12–19.
42. Brookes SM, Price EJ, Venables PJ, Maini RN. Interferon-gammaand epithelial cell activation in Sjögren’s syndrome. Br. J. Rheuma-tol. 1995;34:226–231.
Address reprint requests or correspondence to:Malgorzata Mrugacz
Department of Pediatric Ophthalmology Medical University of Bialystok
17 Washington Street15-274 Bialystok
Poland
Tel: �48857450862Fax: �48857450858
E-mail: [email protected]
Received 5 May 2005/Accepted 11 July 2005
IL-8 AND IFN-� IN TEARS OF CF PATIENTS 75