Human Vδ1 γδ T cells expanded from peripheral blood exhibit specific cytotoxicity against B-cell...
12
Correspondence: Gabrielle M. Siegers, PhD, Cell Therapy Program, Princess Margaret Hospital, 610 University Ave, Suite 5-3-03, Toronto, Ontario, M5G 2M9, Canada. E-mail: [email protected] (Received 8 September 2010; accepted 25 December 2010) Human V δ1 γδ T cells expanded from peripheral blood exhibit specific cytotoxicity against B-cell chronic lymphocytic leukemia-derived cells GABRIELLE M. SIEGERS 1 , HELENA DHAMKO 1 , XING-HUA WANG 1 , A. MARK MATHIESON 1 , YOKO KOSAKA 1 , TANIA C. FELIZARDO 2 , JEFFREY A. MEDIN 2 , SHUJI TOHDA 3 , JULIA SCHUELER 4,5 , PAUL FISCH 6 & ARMAND KEATING 1 1 Cell Therapy Program, Princess Margaret Hospital, University Health Network, Toronto, Ontario, Canada, 2 Division of Stem Cell and Developmental Biology, Ontario Cancer Institute, Toronto, Canada, 3 Department of Laboratory Medicine/Hematology, Tokyo Medical and Dental University, Tokyo, Japan, 4 Oncotest GmbH, Freiburg, Germany, 5 Hematology and Oncology Department, University of Freiburg Medical Center, Freiburg, Germany, and 6 Department of Pathology, University of Freiburg Medical Center, Freiburg, Germany Abstract Background aims. There is increasing interest in using γδ T cells (GDTC) for cancer immunotherapy. Most studies have been concerned with the V δ2 subset in blood, for which several expansion protocols exist. We have developed a protocol to expand V δ1 and V δ2 preferentially from human blood. We have characterized these subsets and their specificities for leukemic targets. Methods. GDTC were isolated from the peripheral blood mononuclear cells (PBMC) of healthy donors via positive magnetic cell sorting; their proliferation in vitro was induced by exposure to the mitogen concanavalin A (Con A). CD107 and cytotoxicity (Cr 51 -release and flow cytometric) assays were performed. GDTC clones and target cells were immunophenotyped via flow cytometry. Results. Longer initial exposure to Con A typically resulted in higher V δ1 prevalence. V δ1 were activated by and cytotoxic to B-cell chronic lymphocytic leukemia (B-CLL)-derived MEC1 cells, whereas V δ2 also responded to MEC1 but more so to the Philadelphia chromosome-positive [Ph ] leukemia cell line EM-enhanced green fluorescent protein (2eGFPluc). V δ2 clone cytotoxicity against EM-2eGFPluc correlated with V δ2 T-cell antigen receptor (TCR) and receptor found on Natural Killer cells and many T-cells (NKG2D), whereas V δ1 clone cytotoxicity versus MEC1 correlated with V δ1 TCR, CD56 and CD95 expression. V δ1 also killed Epstein-Barr Virus (EBV)-negative B-CLL-derived TMD2 cells. Immunophenotyping revealed reduced HLA-ABC expression on EM-2eGFPluc, whereas MEC1 and TMD2 exhibited higher Tumor Necrosis Factor-Related Apoptosis-Inducing Ligand (TRAILR1). Conclusions. Our ability to expand peripheral V δ1 cells and show their cytotoxicity to B-CLL-derived cell lines suggests that this novel approach to the cellular treatment of B-CLL may be feasible. Key Words: B-cell chronic lymphocytic leukemia, cell therapy, γδ T cell, immunotherapy ,V δ1 cells Introduction Human γδ T cells (GDTC) constitute 2–5% of cir- culating lymphocytes (1); within these, there are two main GDTC subsets. V δ1 cells predominate during fetal development and early childhood but by adult- hood constitute the minority of GDTC in blood; the majority is V γ9V δ2 (V δ2) in healthy Caucasians (2). Interestingly, this subset prevalence is reversed in healthy west Africans (3). GDTC recognize a broad range of peptide and non-peptide antigens derived from foreign micro-organisms and endogenous cellular products induced by infection and cellular transformation (4). Recognition is mediated through the T-cell anti- gen receptor (TCR) and/or the NKG2D receptor, present on both V δ1 and V δ2 subsets (5). V δ2 are activated by natural and synthetic phosphoantigens (6–9) as well as alkyl amines (10). V δ1 recognize lipid antigens presented by CD1 (11). NKG2D ligands include UL16-binding proteins (ULBP1–4) and major histocompatibility-like proteins MICA and MICB (5,12). Ensslin et al. (13) were the first to show that GDTC, activated via their TCR, lyse a variety of tumor cell lines in a major histocompatibility com- plex (MHC)-unrestricted manner (13). Indeed, Cytotherapy, 2011; 13: 753–764 ISSN 1465-3249 print/ISSN 1477-2566 online © 2011 Informa Healthcare DOI: 10.3109/14653249.2011.553595
Transcript of Human Vδ1 γδ T cells expanded from peripheral blood exhibit specific cytotoxicity against B-cell...

Correspondence: Gabrielle M. Siegers , PhD, Cell Therapy Program, Princess Margaret Hospital, 610 University Ave, Suite 5-3-03, Toronto, Ontario, M5G 2M9, Canada. E-mail: [email protected]
(Received 8 September 2010 ; accepted 25 December 2010 )
Human V δ 1 γ δ T cells expanded from peripheral blood exhibit specifi c cytotoxicity against B-cell chronic lymphocytic leukemia-derived cells
GABRIELLE M. SIEGERS 1 , HELENA DHAMKO 1 , XING-HUA WANG 1 , A. MARK MATHIESON 1 , YOKO KOSAKA 1 , TANIA C. FELIZARDO 2 , JEFFREY A. MEDIN 2 , SHUJI TOHDA 3 , JULIA SCHUELER 4,5 , PAUL FISCH 6 & ARMAND KEATING 1
1 Cell Therapy Program, Princess Margaret Hospital, University Health Network, Toronto, Ontario, Canada, 2 Division of Stem Cell and Developmental Biology, Ontario Cancer Institute, Toronto, Canada, 3 Department of Laboratory Medicine/Hematology, Tokyo Medical and Dental University, Tokyo, Japan, 4 Oncotest GmbH, Freiburg, Germany, 5 Hematology and Oncology Department, University of Freiburg Medical Center, Freiburg, Germany, and 6 Department of Pathology, University of Freiburg Medical Center, Freiburg, Germany
Abstract Background aims. There is increasing interest in using γ δ T cells (GDTC) for cancer immunotherapy. Most studies have been concerned with the V δ 2 subset in blood, for which several expansion protocols exist. We have developed a protocol to expand V δ 1 and V δ 2 preferentially from human blood. We have characterized these subsets and their specifi cities for leukemic targets. Methods. GDTC were isolated from the peripheral blood mononuclear cells (PBMC) of healthy donors via positive magnetic cell sorting; their proliferation in vitro was induced by exposure to the mitogen concanavalin A (Con A). CD107 and cytotoxicity (Cr 51 -release and fl ow cytometric) assays were performed. GDTC clones and target cells were immunophenotyped via fl ow cytometry. Results. Longer initial exposure to Con A typically resulted in higher V δ 1 prevalence. V δ 1 were activated by and cytotoxic to B-cell chronic lymphocytic leukemia (B-CLL)-derived MEC1 cells, whereas V δ 2 also responded to MEC1 but more so to the Philadelphia chromosome-positive [Ph � ] leukemia cell line EM-enhanced green fl uorescent protein (2eGFPluc). V δ 2 clone cytotoxicity against EM-2eGFPluc correlated with V δ 2 T-cell antigen receptor (TCR) and receptor found on Natural Killer cells and many T-cells (NKG2D), whereas V δ 1 clone cytotoxicity versus MEC1 correlated with V δ 1 TCR, CD56 and CD95 expression. V δ 1 also killed Epstein-Barr Virus (EBV)-negative B-CLL-derived TMD2 cells. Immunophenotyping revealed reduced HLA-ABC expression on EM-2eGFPluc, whereas MEC1 and TMD2 exhibited higher Tumor Necrosis Factor-Related Apoptosis-Inducing Ligand (TRAILR1). Conclusions. Our ability to expand peripheral V δ 1 cells and show their cytotoxicity to B-CLL-derived cell lines suggests that this novel approach to the cellular treatment of B-CLL may be feasible.
Key Words: B-cell chronic lymphocytic leukemia , cell therapy , γ δ T cell , immunotherapy , V δ 1 cells
Introduction
Human γ δ T cells (GDTC) constitute 2 – 5% of cir-culating lymphocytes (1); within these, there are two main GDTC subsets. V δ 1 cells predominate during fetal development and early childhood but by adult-hood constitute the minority of GDTC in blood; the majority is V γ 9V δ 2 (V δ 2) in healthy Caucasians (2). Interestingly, this subset prevalence is reversed in healthy west Africans (3).
GDTC recognize a broad range of peptide and non-peptide antigens derived from foreign micro-organisms and endogenous cellular products induced by infection and cellular transformation (4).
Recognition is mediated through the T-cell anti-gen receptor (TCR) and/or the NKG2D receptor, present on both V δ 1 and V δ 2 subsets (5). V δ 2 are activated by natural and synthetic phosphoantigens (6 – 9) as well as alkyl amines (10). V δ 1 recognize lipid antigens presented by CD1 (11). NKG2D ligands include UL16-binding proteins (ULBP1 – 4) and major histocompatibility-like proteins MICA and MICB (5,12).
Ensslin et al. (13) were the fi rst to show that GDTC, activated via their TCR, lyse a variety of tumor cell lines in a major histocompatibility com-plex (MHC)-unrestricted manner (13). Indeed,
Cytotherapy, 2011; 13: 753–764
ISSN 1465-3249 print/ISSN 1477-2566 online © 2011 Informa HealthcareDOI: 10.3109/14653249.2011.553595

754 G. M. Siegers et al.
tumor cells expressing low levels of HLA antigen are subject to lysis according to the ‘ missing self-hy-pothesis ’ (14 – 16).
GDTC subsets have varying specifi city for diverse targets. V δ 2 recognize and are activated by a number of hematologic malignancies (17 – 19). In contrast, the majority of V δ 1 are localized to tissue mucosae, where they provide defense against epithelial cancers (1). In renal cell carcinoma patients, V γ 3V δ 1 tumor-infi ltrat-ing lymphocytes (TIL) delivered a different cytolytic response than V δ 2 in peripheral blood (20,21). These TIL lysed autologous and allogeneic renal cell tumors but not hematopoietic tumors (20). V δ 1 isolated from TIL of metastatic colorectal cancers were profi cient effectors against autologous and allogeneic colorec-tal cancer as well as several epithelial tumor cells of renal and pancreatic origin (22,23). Further targets of V δ 1 include EBV-transformed B cells (24), B-cell acute lymphoblastic leukemia (ALL) (25) and primary Acute Myeloid Leukemia (AML) blasts (16,26). Cir-culating GDTC levels correlate with disease status in AML patients (27). Lamb et al. (28) showed that leu-kemia patients who had received T-cell depleted par-tially mismatched transplants and had increased V δ 1 thereafter had signifi cantly reduced relapse rates (28). Additionally, V δ 1 clones generated from donors pro-liferated in response to, bound and were cytotoxic to ALL cells from recipients and did not elicit a response in mixed lymphocyte cultures, suggesting that alloge-neic V δ 1 immunotherapy of leukemia may be feasible, as graft-ve rsus-host disease (GvHD) appears not to be an issue (29).
Increased V δ 1 in the blood of B-cell chronic lymphocytic leukemia (B-CLL) patients has been reported (30,31), hence our rationale for investi-gating GDTC cytotoxicity against B-CLL-derived cell lines. B-CLL is the most commonly diagnosed leukemia in western society (32). Although a recent retrospective study has shown an overall improve-ment in survival of B-CLL patients over the last 30 years, this disease remains incurable (33). Thus there is great interest in developing adoptive T-cell immunotherapy to combat this malignancy (34).
GDTC are promising candidates for cellular therapy, as evidenced by the small yet growing number of clinical trials reporting positive out-comes. In a recent phase I trial, autologous GDTC expanded ex vivo and infused into patients with recurrent non-small cell lung cancer were well tol-erated; however, the number of enrolled patients ( n � 10) was too small to determine effi cacy (35). Also, potentiated anti-lymphoma activity in a phase II study using GDTC agonist IPH1101 and ritux-imab for low-grade follicular lymphoma has been reported (36). Both of these trials relied on expan-sion of the V δ 2 subset.
Compared with our understanding of V δ 2 GDTC, the V δ 1 subset is poorly understood, because of its scarcity in accessible human tissues and also a lack of protocols to expand these cells in vitro . We have devised a protocol that expands V δ 1 cells from the blood of a majority of healthy donors and explored their potential to be activated by, and kill, B-CLL-derived cell lines.
Methods
Donors
Human blood samples were collected from healthy adult donors after obtaining written informed con-sent according to research ethics board-approved protocols.
Polyclonal GDTC
Peripheral blood mononuclear cells (PBMC) were recovered using density-gradient separation (Fycoll-Hypaque). GDTC were isolated using an anti-TCR γ δ MicroBead kit (MACS; Miltenyi, Auburn, CA,USA), eluted in complete medium containing 1 μ g/mL Concanavalin A (Con A; Sigma-Aldrich, Oakville, Canada) and plated at 2.5 � 10 5 /mL in 24-well plates. Complete medium was AIM-V (Gibco, Burlington, Ontario, Canada) supplemented with 5% human AB serum (Lonza, Walkersville, MD, USA) and 10 ng/mL each recombinant human interleukin (IL)-2 (Proleukin; Novartis Pharmaceuticals, Dorval, Quebec, Canada) and IL-4 (R&D Systems, Minneapolis, MN, USA). Cells were cultured in complete medium after an initial incubation with Con A for 6 – 8 days, as indicated. Cells were harvested, counted and replated at 2.5 � 10 5 /mL or 5.0 � 10 5 /mL in 24-well plates and maintained in a humidifi ed atmosphere at 37 ° C and 5% CO 2 . Pre-isolation GDTC levels and post-isolation purity were routinely monitored via staining with appropriate antibodies and subsequent acquisition and analysis via fl uorescence-activated cell sorting (FCM). Examples of this are shown in Supplementary Table SI.
V δ 2 depletion
1.0 � 10 7 7-day Con A GDTC, were harvested and labeled with 26 μ L anti-V δ 2 biotin antibody (purifi ed anti-V δ 2; Biolegend, San Diego, CA, USA; biotiny-lated according to standard protocols) in 84 μ L cold MACS buffer [phosphate-buffered saline (PBS), 0.5% human AB serum and 2 m M ethylene diamine tetra acetic acid (EDTA)] for 10 min at 4 ° C. After washing with 10 mL MACS buffer, cells were resuspended in 32 μ L MACS buffer plus 10 μ L streptavidin MACS beads (Miltenyi) and incubated at 4 ° C for 15 min. After washing, cells were separated on a MACS MS

V d 1 g d T cells cytotoxic to B-CLL 755
column; MACS-positive and -negative fractions were collected and plated out in AIM-V complete medium as above. It should be noted that this protocol was not optimized; Miltenyi LD or LS columns would be more suitable than the MS column used here.
GDTC clones
After PBMC isolation, cells were stained with anti-V δ 1 or anti-V δ 2 antibodies. Two-hundred V δ 1 and 600 V δ 2 cells were isolated via FCM and 1 cell/well plated in round-bottomed 96-well plates in RPMI containing 2 m M L -glutamine, 100 IU penicillin, 100 μ g/mL strep-tomycin, 25 m M Hepes buffer and 10% human AB serum. Cells were stimulated with 500 IU/mL recombi-nant (r)IL-2, 0.25 μ g/mL phytohemagglutinin (PHA) and irradiated feeder cells (2 � 10 4 PBMC and 1 � 10 4 EBV-transformed lymphoblastoid B-cell lines/well). Clones (37) were replated weekly at 2 � 10 4 cells/well with fresh medium and feeders and maintained at 37 ° C and 7% CO 2 .
Lentivirus production and cell transduction
A lentiviral vector encoding the cDNA for enhanced GFP and luciferase (eGFPluc) (pCCL.sin.cPPT.polyA.CTE.eGFP.minhCMV.hPGK.luc.Wpre) was constructed using a dual promoter system. eGFP expression was driven by the minimal human cytomegalovirus (CMV) promoter and luciferase expression by the human phosphoglycerate kinase promoter. The parent vector was obtained from Dr L. Naldini (38); the truncated version of low-affi nity nerve growth factor (NGF) receptor in this construct was replaced by fi refl y luciferase cDNA by standard molecular biology techniques. Recombinant lentiviral virions were generated following a previously pub-lished protocol (39). The EM-2 leukemia cell line was transduced with the eGFPluc lentiviral vector at an effective multiplicities of infection (MOI) of 1; positive cells were sorted for eGFP expression by FCM. EM-2eGFPluc was maintained in RPMI sup-plemented with 10% fetal bovine serum (FBS). This cell line was generated for in vivo studies underway in Keating lab and was easily distinguished from effec-tors in fl ow cytometry-based cytotoxicity studies.
MEC1 (DMSZ, Braunschweig, Germany), an EBV-positive B-cell line derived from B-CLL, was cultured in Iscove’s Modifi ed Dulbecco’s Media (IMDM) medium plus 10% FBS. TMD2 is an EBV-negative B-CLL-derived cell line maintained in mini-mum essential medium (MEM) alpha supplemented with 10% FBS and 1 ng/mL IL-3 (40). Target lines were maintained in a humidifi ed atmosphere at 37 ° C and 7% CO 2 . Cells were enumerated using trypan blue exclusion.
CFSE labeling
GDTC, 2 � 10 6 , were resuspended in 200 μ L warm RPMI supplemented with 2% FBS, and car-boxyfl uorescein succinimidyl ester (CFSE) added to a fi nal concentration of 1.25 μ M . Cells were incu-bated for 8 min at room temperature in the dark, then 1 mL cold RPMI � 2% FBS added to stop the reaction. Cells were centrifuged for 5 min at 400 g , washed twice in cold AIM-V and plated out in complete medium at 5 � 10 5 /mL.
CD107 assays
GDTC, 1 � 10 5 , were plated alone or mixed with 5 � 10 5 target cells in AIM-V complete media in a 96-well round-bottomed plate. Phorbol-12-myristate-13 acetate (PMA)/ionomycin (0.15 n M /0.3 μ g/mL fi nal concentrations) was added to positive control wells; 5 μ L anti-CD107Alexa647 (Biolegend) were added to all wells. Cells were incubated for 1 h at 37 ° C and then 8.5 μ L of a 1:50 dilution of Golgi stop BD Biosciences (BD) added. Incubation continued at 37 ° C for 2 h, then cells were covered and put on ice. Further staining was performed as described below (Flow cytometry).
Clone screening
Two wells of each clone were pooled and mixed with 5000 target cells in RPMI with 1% bovine serum albumin (BSA) and 150 IU/mL rIL-2. After a 4-h incubation at 37 ° C, cells were put on ice, washed with FCM buffer and stained with 5 μ L of a 1:5 propidium iodide (PI) dilution (Sigma) for 10 min prior to FCM acquisition. For screening assays, the clone ratio was calculated by dividing each clone frequency by that of the clone with the lowest value. Normalized percentage cytotoxicity was calculated by dividing the percentage cytotoxicity by the clone ratio.
Cytotoxicity assays
These were carried out as above, except effectors (E) and targets (T) were counted and mixed at an E:T of 10:1. Higher values may have been obtained if effectors and targets had been centrifuged briefl y prior to incu-bation. Live and dead cell gates were established based on live and dead cell controls. For EM-2eGFPluc targets, dead cells were GFP � PI � and live cells GFP � PI – ; for MEC1, dead cells were CD19 � PI � and live cells were CD19 � PI – . Percentage cytotoxic-ity � 100 � dead/(dead � live). Net cytotoxicity was percentage cytotoxicity at time ( t ) � 4 h minus per-centage cytotoxicity at t � 0. For t � 0, effectors and targets were incubated separately at 37 ° C and mixed together on ice just prior to PI staining.

756 G. M. Siegers et al.
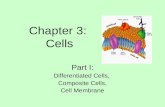
circulating GDTC are predominantly of the V δ 2 sub-set, we found that in 59% of GDTC cultures derived from peripheral blood of healthy donors ( n � 17 differ-ent donors) the V δ 1 subset was preferentially expanded (Figure 1). V δ 1 comprised 70.5 � 4.7% (mean � stan-dard error) of the total culture, as determined by fl ow cytometry (FCM). In 35% of cultures, V δ 2 GDTC were dominant, comprising 75.2 � 6.2%. Preferen-tial expansion of V δ 1 did not correlate with subset prevalence in donor blood on day 0; the V δ 2:V δ 1 ratio calculated from fl ow cytometric (FCM data) was 4.5 � 3.5 (average ratio � SD, n � 21 iso-lations, eight donors). For data pertaining to the purity of the initial selection procedure, please see Supplementary Table SI.
Exposure to Con A drives V δ 1/V δ 2 predominance
Our protocol stipulates an initial culture period of 6 – 8 days in Con A. Retrospectively, it appeared that shorter times in Con A correlated with V δ 2 predominance, whereas longer exposure tended to yield V δ 1-dominant cultures (donors 10 – 17; Figure 1). Interestingly, one donor expanded V δ 2 or V δ 1 on occa-sion and twice expanded both subsets equally (donor 11; Figure 1 and Supplementary Table SII).
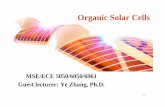
To test the hypothesis that Con A can drive poly-clonal GDTC cultures to V δ 1 or V δ 2 dominance, we isolated GDTC and cultured them for 6, 7 and 8 days in Con A in parallel. Using trypan blue exclusion and FCM, we monitored cell growth and V δ 1 and V δ 2 proportions over time. Donor 18 had similar circu-lating V δ 1 and V δ 2 proportions on day 0 (1.5% and 1.9%, respectively); however, after day 10 the 8-day Con A culture had consistently higher V δ 1 proportions compared with 7-day and 6-day cultures (Figure 2A, left panel). Conversely, 6-day cultures preferentially
Chromium release assay
Cr 51 release assays were performed according to standard protocols (41). Data are presented as mean percentage lysis of duplicate or triplicate samples, as indicated ( � SD).
Flow cytometry (FCM)
For FCM-based cytotoxicity assays, GDTC or clones were stained with anti-V δ 1 – fl uorescein isothiocyanate (FITC; 1:50; Thermo Scientifi c, Rockford, IL, USA) or anti-V δ 2 – phycoerythrin (PE) (1:100; Biolegend); MEC1 cells were stained with anti-CD19 – FITC (1:10; AbD Serotec, Medicorp Inc, Montreal, Que-bec, Canada). GDTC clone phenotyping was per-formed using anti-CD56 – FITC (1:10; BioLegend), anti-CD94 – PE (1:10; Ancell, Bayport, MN, USA), anti-CD95 – PE (1:10; BD Biosciences, Mississauga, Ontario, Canada) and anti-NKG2D – PE (1:50; R&D Systems). Tumor cells were phenotyped using anti-HLA-ABC – PE (1:10; BD Biosciences, eBioscience, Inc, San Diego, CA, USA), purifi ed anti-ULBP1, anti-ULBP2 and anti-ULBP3 (1:10; R&D Systems), followed by goat anti-mouse IgG – PE (1:50; BD Biosciences), anti-TRAILR1 – biotin (1:10; BioLegend), streptavidin –allophycocyanin fl uorescence (APC) (1:50; eBiosciences), anti-TRAILR2 – APC (1:10; BioLegend) and anti-MICA/MICB – PE (1:10; BioLegend). Samples were acquired using an FC-500 (Beckman-Coulter, Mississauga, Ontario, Canada). Analysis was performed using FlowJo © software.
Annexin V staining
Cells, 2.5 � 10 4 , were stained with anti-V δ 1 – FITC, anti-V δ 2 – PE and anti-CD3 – APC Cy7 (BioLegend), washed and then resuspended in 200 μ L 1 � Annexin V binding buffer (eBioscience), to which 2 μ L anti-Annexin V – APC (Southern Biotech, Birmingham, Alabama, USA) were added. Cells were incubated on ice in the dark for 10 min, 200 μ L binding buffer added and samples acquired.
Statistics
Means, standard deviations, standard error and P -values (Student ’ s t -tests) were calculated using Microsoft Excel.
Results
Expansion of V δ 1 and/or V δ 2 GDTC subsets derived from human blood, irrespective of day 0 V δ 1/V δ 2 prevalence
We have isolated and expanded GDTC as a fi rst step in developing a clinical protocol (42). Although
Figure 1. The V δ 1 subset is expanded preferentially in 59% of polyclonal γ δ T-cell cultures, despite V δ 2 predominance in blood. γ δ T cells were isolated from the peripheral blood of 17 different donors and expanded according to our protocol. Cells were stained with anti-V δ 1 – FITC and anti-V δ 2 – PE antibodies and subject to fl ow cytometry. Duration of Con A exposure is indicated below the donor number. V δ 1 culture composition is indicated by solid black bars, V δ 2 gray bars.

V d 1 g d T cells cytotoxic to B-CLL 757
cultures, with a greater difference in MFI (12.1 com-pared with 14.2). Annexin V staining showed that V δ 2 underwent apoptosis to a greater extent than V δ 1 under both conditions early in culture, which then limited the number of V δ 2 able to proliferate overall. This difference was signifi cant on day 10 in 8-day Con A cultures ( P � 0.007). On day 16, there were no signifi cant differences under either condition, but by day 20 V δ 2 Annexin V staining was signifi cantly higher in the 6-day Con A culture ( P � 0.020; Figure 3D, E). For fl ow cytometric data, please see Supplementary Figure S1.
V δ 2 is activated by the CML cell line EM-2eGFPluc, whereas V δ 1 is preferentially activated by B-CLL-derived MEC1
In one expanded culture (Figure 1, donor 11), V δ 1 and V δ 2 were equally present (40.3% and 41.3% respec-tively, on day 17). To determine V δ 1 and V δ 2 activation simultaneously when co-incubated with Philadelphia chromosome-positive [Ph( � )] EM-2eGFPluc leu-kemia cells, exposure of the degranulation-induced marker CD107 was determined by FCM. Assays performed on culture days 10 – 17 ( n � 8), with anal-ysis gating on live GDTC only, revealed that only 3.4 � 2.7% V δ 1 (V δ 2 – GFP – ) cells were activated, whereas V δ 2 cells exhibited 10-fold activation with 34.1 � 4.7% expressing CD107. A representative example is shown in Figure 4A.
expanded V δ 2 compared with V δ 1 (Figure 2A, right panel). Although the 8-day Con A cultures did not expand well, V δ 1 expansion was higher than V δ 2 (Figure 2B, both panels). V δ 2 expanded 25.4-fold in 6-day cultures compared with 15.9-fold in 7-day cul-tures (Figure 2B, right panel). Please see Supplemen-tary Table SIII for data from additional experiments (four donors, n � 6 including Figure 2).
A few donors expanded V δ 1 or V δ 2 irrespective Con A exposure. For example, in cultures from donor 15, the V δ 1 subset was signifi cantly predominant over-all (Figure 3A; 6-day Con A 80.3 � 2.1%, 8-day Con A 67.3 � 2.0%, mean � SE); V δ 1 expansion was greater than V δ 2 in 6-day Con A cultures (Figure 3B, left panel), yet 4-fold that in 8-day Con A cultures (Figure 3B, right panel; 35.1 � 1.0 versus 8.9 � 0.2). Please see Supplementary Table SIV for calculated P -values.
To investigate rates of V δ 1 and V δ 2 cell division, we labeled donor 15 GDTC with CFSE on day 10 and performed FCM on day 13. Because of rapid CFSE dilution, labeling prior to the exponential growth phase did not yield meaningful data (data not shown). Overall, 6-day Con A cultures prolif-erated more rapidly than 8-day Con A cultures, as evidenced by their lower mean fl uorescence intensity (MFI) values (Figure 3C; compare 12.1 and 14.2 with 17.6 and 16.8, respectively). Overlays (not shown here) of V δ 2 � and V δ 2 – showed no differ-ences in 8-day cultures (MFI were 17.6 and 16.8), but slightly higher proliferation of V δ 2 in 6-day
Figure 2. V δ 1 or V δ 2 prevalence can be driven by varying initial γ δ T-cell exposure to the mitogen Con A. (A) γ δ T cells were isolated from donor 18 and cultured in parallel in Con A for 6, 7 or 8 days, as indicated. Thereafter, cells were harvested and subject to staining with anti-V δ 1 – FITC, anti-V δ 2 – PE and anti-CD3 – APC antibodies. Shown is the percentage of CD3-positive cells that were V δ 1-positive (left panel) or V δ 2-positive (right panel). This is representative of seven experiments performed using samples from fi ve donors. (B) Cells from the cultures in (A) were enumerated and absolute numbers determined by multiplication by the percentages of V δ 1- and V δ 2-positive cells in (A).

758 G. M. Siegers et al.
Figure 3. Increased proliferation, yet also greater apoptosis, of V δ 2 in γ δ T-cell culture of a V δ 1 expander. (A) Triplicate wells of γ δ T cells isolated from donor 15 were handled as in Figure 2A. (B) Fold-expansion was determined as in Figure 2B. (C) γ δ T cells were CFSE-labeled on culture day 10 and fl ow cytometry performed on culture day 13. Cells were stained with anti-V δ 2 – PE prior to acquisition. MFI in the FL1 channel is indicated for the two populations. (D, E) Cells were harvested and stained with anti-V δ 1 – FITC, anti-V δ 2 – PE and anti-AnnexinV – APC antibodies and fl ow cytometry performed on the indicated days. Statistically signifi cant differences are indicated: ∗ P � 0.05; ∗ ∗ P � 0.005; ∗ ∗ ∗ P � 0.001. Error bars in all parts of this fi gure indicate SE.
An increase in circulating V δ 1 in B-CLL patients has been described (30,31), so we investigated V δ 1 activation versus the B-CLL-derived MEC1 cell line. We generated a culture with 33.6% V δ 1 and 51.7% V δ 2 (donor 18, 7-day Con A culture on day 14) and performed CD107 assays. MEC1, but not EM-2, activated V δ 1 cells (Figure 4B). V δ 2 were activated by both targets, although 1.5-fold higher percentage CD107 and MFI were obtained upon incubation with EM-2 compared with MEC1 (Figure 4C). Statistical analysis confi rmed these differences to be highly signifi cant ( P � 0.001). In contrast, CD107 MFI of V δ 1 versus V δ 2 against MEC1 was not signifi cant ( P � 0.708), although the
percentage CD107 values gave near signifi cance ( P � 0.0502). These results were confi rmed in assays with cells from three additional donors (data not shown).
Generation and screening of V δ 1 and V δ 2 GDTC clones demonstrates selective and superior cytotoxicity of individual clones compared with polyclonal GDTC from the same donor
We generated V δ 2 clones from donor 11 and both V δ 1 and V δ 2 clones from donor 17. In a fl ow cytometric screening assay, V δ 2 clones exhibited 4.5 – 10.6% cyto-toxicity against EM-2eGFPluc over a 4-h co-incubation at a 2.6:1 E:T (Figure 5A). Cytotoxicity ranking was

V d 1 g d T cells cytotoxic to B-CLL 759
confi rmed in a 4-h assay at a 10:1 E:T, ranging from 23.5% to 35.4% for clones A1, B3 and C6, respectively (data not shown). Donor 17 clone E5 exhibited 10-fold (49.2%) and E3 1.4-fold (7.6%) cytotoxicity of poly-clonal GDTC from the same donor (5.3%) (Figure 5B). Likewise, C6 was more cytotoxic than polyclonal GDTC from donor 11 (data not shown). At a 1.9:1 ratio over 4 h, the percentage cytotoxicity of V δ 1 clones was 7.0 – 13.8% (D3 most cytotoxic; data not shown). At a 10:1 E:T over 4 h, clone D3 again proved most cyto-toxic, with 40.8% compared with polyclonal cultures at 18.6% (Figure 5C; donor 15, 52% V δ 1) and 6.8% (Figure 5C; donor 17, 57% V δ 2). In Cr 51 release assays, the signifi cant V δ 1/V δ 2 specifi city for EM-2eGFPluc versus MEC1 in parallel was confi rmed (Table I). D3 killed MEC1 effi ciently (59.4 � 0.4) but showed 0%
Figure 4. V δ 2 is activated by the CML cell line EM-2eGFPluc, whereas V δ 1 is preferentially activated by B-CLL-derived MEC1. (A) γ δ T cells from donor 11 were subject to CD107 assays on culture days 10 – 17 ( n � 8) using EM-2eGFPluc as targets. A representative example of fl ow cytometric analysis is shown. (B) γ δ T cells from donor 18 were harvested on culture day 14, incubated with EM-2eGFPluc or MEC1 in triplicate for 3 h, stained with anti-V δ 1 – FITC, anti-V δ 2 – PE and anti-CD107aAlexaFluor647 antibodies and then subjected to fl ow cytometric analysis. V δ 1 – FITC cells were gated and both percentage CD107 (black symbols) and MFI (gray symbols) determined. (C) As in (B) but gated on the V δ 2 – PE-positive population. Statistically signifi cant differences are indicated: ∗ P � 0.001.
cytotoxicity to EM-2eGFPluc. Corroborating CD107 data showed V δ 2 activation by both targets; E5 killed both MEC1 and EM-2eGFPluc but was signifi cantly more cytotoxic to the latter (36.1 � 1.4 compared with 43.4 � 0.4; P � 0.0085). V δ 1 targeting of MEC1 was also signifi cantly greater than that of V δ 2 ( P � 0.0003). A FCM-based cytotoxicity assay gave similar results (data not shown).
Clone cytotoxicity differentially correlates with cell-surface expression of TCR, activation markers and NKG2D
We investigated cell-surface expression of the γ δ TCR, activating receptors CD56 and NKG2D, the inhibitory marker CD94 and death receptor CD95 (Fas) on V δ 1

760 G. M. Siegers et al.
Figure 5. V δ 2 clones kill EM-2eGFPluc, whereas V δ 1 clones kill MEC1; select clones are more cytotoxic than polyclonal γ δ T cells from the same donor. (A) V δ 2 clones from two donors were screened for their ability to lyse EM-2eGFPluc in vitro in a 4-h assay at an E:T of 2.6:1. Cells were stained with PI and subjected to fl ow cytometry. Percentage cytotoxicity was determined by subtracting the cytotoxicity of the t � 0 control from the t � 4 h samples. Percentage cytotoxicity � 100 � [dead/(dead � live)], where dead targets are GFP � PI � . (B) V δ 2 clones and polyclonal γ δ T cells from donor 17 were incubated with EM-2eGFPluc for 4 h at an E:T of 10:1. Fold cytotoxicity increase over polyclonal is indicated. (C) V δ 1 clones and polyclonal γ δ T cells from donor 17, as well as polyclonal γ δ T cells from donor 15, were incubated with MEC1 for 4 h at an E:T of 10:1. Cells were stained using anti-CD19 – FITC and cytotoxicity calculated as in (A), except that targets were FITC � .
and V δ 2 clones using FCM. The most cytotoxic clones, D3 and E5, had the highest γ δ TCR expression (Figure 6A, B, left panel); E5 in particular had levels far sur-passing the others (Figure 6B, left panel). The higher V δ 1 clone cytotoxicity of D3 also correlated with higher CD56 and CD95 expression (Figure 6A), whereas V δ 2 clone rankings correlated directly with NKG2D expression and inversely with CD56 and CD94 (Figure 6B, right panel).
V δ 1 activation by B-CLL is EBV-independent
The B-CLL cell line MEC1 is EBV positive and V δ 1 is activated by EBV (24). We thus used TMD2, an EBV-negative B-CLL cell line (40), to verify B-CLL activa-tion of V δ 1. When tested in parallel in both CD107 (data not shown) and Cr 51 release assays, V δ 1 was acti-vated by and cytotoxic against both MEC1 and TMD2 (Figure 7A). This suggested that V δ 1 activation by and cytotoxicity to B-CLL was not EBV-dependent.
EM-2eGFPluc, MEC1 and TMD2 immunophe-notyping using antibodies directed against several
Figure 6. V δ 1/V δ 2 clone phenotyping shows correlations between various surface markers and cytotoxicity ranking. (A) V δ 1 clones were stained using antibodies directed at the indicated surface markers and then subjected to fl ow cytometric analysis. (B) As in (A) with V δ 2 clones.

V d 1 g d T cells cytotoxic to B-CLL 761
known tumor antigens revealed that EM-2eGFP-luc expressed 3 – 5-fold less HLA-ABC compared with TMD2 and MEC1, respectively (Figure 7B). Similarly, the B-CLL lines expressed 1.8-fold more TRAILR1 than EM-2eGFPluc (Figure 7C). MEC1 had elevated ULBP2 and ULBP3 levels compared with the other two lines. As expected, MICA/B expression in all three lines was negligible (43) and they expressed low levels of ULBP1 and TRAILR2.
Discussion
We have developed a protocol to expand V δ 1 and V δ 2 GDTC from peripheral blood. Importantly, this protocol is straightforward and does not require the use of expensive antibodies or feeder cells. We chose the mitogen Con A after noting superior expansion of GDTC compared with that achieved with the anti-CD3 antibody OKT3 or PHA in the context of our protocol (data not shown). Prolonged initial exposure of most healthy donor GDTC to the mitogen Con A yielded higher percentages of V δ 1 compared with V δ 2 in mixed cultures, independent of day 0 subset levels in the blood. This contrasts with the GDTC expansion protocol recently published by Dokouhaki et al. (44), which uses OKT3 and expands GDTC subsets in proportion to their day 0 ratios (44). With our protocol, some donor variability was evident, as expected for primary cultures; however, the trends described applied in most cases.
Con A is a tetravalent lectin derived from Jack bean that binds to surface receptors on murine and human lymphocytes. At low doses, Con A is stimula-tory, inducing cell growth; however, at higher doses it becomes toxic. Interestingly, Con A is under investi-gation for its potential use in anti-cancer therapy, as its toxicity against hepatoma (45,46) and melanoma (47) has been documented recently. Con A toxicity was via autophagic programmed cell death (45) or caspase-dependent apoptosis (46,47). As longer Con A exposure led to increased Annexin V staining in V δ 2 compared with V δ 1 in mixed cultures, this argues for increased Con A-induced apoptosis of V δ 2. Perhaps higher TCR levels on V δ 2 render these cells more
susceptible to Con A toxicity; indeed, when the MFI of CD3 on the surface of V δ 1 and V δ 2 were com-pared, V δ 2 MFI was higher (data not shown). This could also account for the higher V δ 2 proliferation rates and might render these cells more suscepti-ble to activation-induced cell death. Further study is warranted to elucidate the mechanism by which longer Con A exposure leads to increased V δ 1.
Although V δ 1 was predominant in 8-day Con A cultures, purity was variable. We used biotinylated anti-V δ 1 or anti-V δ 2 antibodies and commercially available magnetic streptavidin MACS beads to purify the subsets further (data not shown). After separation, cell viability in the MACS-negative frac-tion was better than that of positively selected cells, thus it was used for further experiments (Figure 7A and data not shown). This also ruled out potential artifacts resulting from stimulation via the biotiny-lated antibody. Cultures undergoing MACS separa-tion late in the culture period (day 15) proliferated little or not at all. Perhaps earlier separation during the exponential growth phase would allow for fur-ther propagation. This strategy could be used for the initial GDTC isolation; however, V δ 1 cell numbers are extremely low. A further consideration is whether V δ 1 and V δ 2 infl uence one another in co-culture. The
Table I. Selective cytotoxicity of V δ 1 and V δ 2 clones. The most cytotoxic clones from donor 2, V δ 1 clone D3 and V δ 2 clone E5, were tested for their cytotoxicity against EM-2eGFPluc and MEC1 in parallel in a standard Cr 51 release assay at an E:T ratio of 10:1. Shown are average percentage cytotoxicity � SD; n is indicated.
EM-2eGFPluc MEC1
D3 (V δ 1), n � 2 0 59.4 � 0.6 1 E5 (V δ 2), n � 3 43.4 � 0.8 2 36.1 � 2.5 1,2
1 P � 0.0003. 2 P � 0.0085.
Figure 7. V δ 1 are cytotoxic to MEC1 and TMD2 B-CLL-derived cell lines. EM-2eGFPluc, MEC1 and TMD2 phenotyping revealed differences in tumor antigen expression on the cell surface. (A) γ δ T cells from donor 16 were subject to V δ 2-depletion on culture day 15. Day 18 fl ow cytometric analysis confi rmed V δ 1 predominance (75.3% V δ 1 � CD3 � , 8.2% V δ 2 � CD3 � ). On day 19, these cells were used in a Cr 51 release assay using EBV � MEC1 and EBV – TMD2 at the indicated ratios. Shown are the averages of triplicates; error bars indicate SD. (B, C) Equal numbers of EM-2eGFPluc, MEC1 and TMD2 were stained using antibodies directed at the indicated tumor antigens, as well as isotype controls. MFI was determined and the values shown calculated by dividing MFI by that of the appropriate isotype control.

762 G. M. Siegers et al.
shown for V δ 2 killing of HLA class I-defi cient Daudi lymphoma cells (15). In contrast, the comparatively high expression of the death domain-containing recep-tor TRAILR1, or DR4, on B-CLL cell lines MEC1 and TMD2 may play a role in V δ 1 cytotoxicity to these targets and warrants further investigation. Interestingly, the use of histone deacetylase (HDAC) inhibitors to up-regulate TRAIL receptors on apoptosis-resistant B-CLL lines is currently being explored as a potential therapy for B-CLL (50).
Our panel of clones exhibiting different levels of cytotoxicity provides a valuable tool for elucidating mechanisms of action, which we intend to validate by further studies. This approach is preferable to the use of blocking antibodies, which may have unwanted effects on target cells. For example, blocking antibod-ies in the presence of malignant B cells results in Fc receptor cross-linking that may lead to Fc receptor-mediated apoptosis even in the absence of effectors (51). Thus Fab fragments are necessary for conven-tional blocking studies using MEC1 and TMD2.
Bartkowiak et al. (30) reported increased GDTC in the peripheral blood of untreated B-CLL patients ( n � 30), attributed to signifi cant V δ 1 expansion resulting in its predominance; this was pronounced at the most severe stage of disease (30). In contrast, Poggi et al. (31) found increased circulating V δ 1 in less than half of B-CLL patients studied (15/38) compared with healthy controls (15), and these were in the low- to intermediate-risk categories. Increased V δ 1 levels, combined with detectable or inducible ULBP3 expression on leukemia cells, correlated with better outcome. This apparent contradiction may be attributed to relatively low sample numbers or differences in patient populations; however, the differing methods are probably the culprit. Whereas both groups studied untreated patients, Bartkowiak et al . (30) used reverse transcriptase polymerase chain reaction (RT-PCR) to quantify TCR δ gene segments, while Poggi et al . (31) performed absolute V δ 1 lym-phocyte counts, which are comparatively less sensi-tive. Encouragingly, Poggi et al. (31) showed that V δ 1 cells from B-CLL patients with increased V δ 1 counts can be expanded in vitro and that they secrete TNF- α and IFN- γ in response to co-culture with autologous PBMC containing leukemic cells. Unfor-tunately, these expanded V δ 1 did not kill targets unless they were transfected with MICA or their ULBP3 expression up-regulated via pokeweed mito-gen or all- trans -retinoic acid. Indeed, the targets used were not B-CLL-derived leukemia cells but rather manipulated variants of the lymphoma line C1R.
Using our protocol, we can expand functional V δ 1 cells that kill B-CLL lines MEC1 and TMD2 with-out manipulation. Of note, these lines did not express MICA/B; low ULBP3 expression was evident on
dominant subset may inhibit or stimulate the other. We have preliminary data suggesting that activation of V δ 2 results in V δ 1 inhibition (data not shown). This observation warrants further investigation and our protocol uniquely enables this kind of study.
It should also be noted that a third GDTC sub-set, V δ 3, is present in human blood, but we could not study V δ 3 because we had no access to an anti-V δ 3 antibody. It was possible to infer V δ 3 percentages by subtraction of V δ 1 and V δ 2 from total CD3 val-ues; these were negligible (data not shown). Also of note, when culturing GDTC using our protocol, it is important not to subject them to drastic tempera-ture changes; cell growth is better in 96-well round-bottomed or 24-well tissue culture-treated plates. The dramatic increase in Annexin V staining in cultures on day 20 suggests that GDTC should be harvested and used by day 16, when viability is still high.
We used CD107 assays to compare activation of V δ 1 and V δ 2 subsets in the presence of various targets. This assay is particularly well suited to this goal, as it requires comparatively few cells (1 � 10 5 /well) and multiple effectors (e.g. V δ 1 and V δ 2) can be investi-gated simultaneously. This contrasts with cytotoxic-ity assays, where target cells are the focus and, when using a mixture of effectors, one cannot know which effector was responsible for the observed cytotoxic-ity. Our results corroborate previous correlations of CD107 mobilization and GDTC cytotoxicity (48). We found that EM-2eGFPluc not only activated V δ 2 but was also effi ciently lysed by this subset (Figures 4 and 5); this was also true for MEC1 and V δ 1. Inter-estingly, we observed both activation by and killing of MEC1 by both V δ 1 and V δ 2 subsets, the latter to a lesser extent. This suggests that expansion of a mixed GDTC culture for cellular therapy of B-CLL patients would not require separation of subsets prior to infusion. Importantly, V δ 1 killed the EBV-negative B-CLL cell line TMD2, indicating that V δ 1 activa-tion and cytotoxicity with respect to these B-CLL cell lines is not EBV-dependent.
Several hints regarding V δ 1/V δ 2 mechanisms of action have been provided, including the obvious cor-relation between TCR levels and cytotoxicity of clones, which points to TCR involvement. CD56 expression correlated with V δ 1 cytotoxicity, suggesting not only greater activation but perhaps also apoptosis resistance (49). However, this contradicts with the direct correla-tion between CD95, or fas, expression on V δ 1 clones and their cytotoxicity, which may signal impending activation-induced cell death. NKG2D levels on V δ 2 clones correlated with cytotoxicity; however, the lack of known NKG2D ligands on EM-2eGFPluc argues against this mechanism. Rather, the striking lack of HLA class I on the surface of EM-2eGFPluc points to killing via the ‘ missing self ’ hypothesis, which has been

V d 1 g d T cells cytotoxic to B-CLL 763
Burk MR, Mori L, De Libero G. Human V gamma 9-V delta 8. 2 cells are stimulated in a cross-reactive fashion by a variety of phosphorylated metabolites. Eur J Immunol. 1995;25:2052 – 8. Sicard H, Ingoure S, Luciani B, Serraz C, Fournie JJ, 9. Bonneville M, et al. In vivo immunomanipulation of V gamma 9V delta 2 T cells with a synthetic phosphoantigen in a preclinical nonhuman primate model. J Immunol. 2005;175:5471 – 80. Bukowski JF, Morita CT, Brenner MB. Human gamma delta 10. T cells recognize alkylamines derived from microbes, edible plants, and tea: implications for innate immunity. Immunity. 1999;11:57 – 65. Spada FM, Grant EP, Peters PJ, Sugita M, Melian A, Leslie DS, 11. et al. Self-recognition of CD1 by gamma/delta T cells: implica-tions for innate immunity. J Exp Med. 2000;191:937 – 48. Cosman D, Mullberg J, Sutherland CL, Chin W, Armitage R, 12. Fanslow W, et al. ULBPs, novel MHC class I-related mole-cules, bind to CMV glycoprotein UL16 and stimulate NK cytotoxicity through the NKG2D receptor. Immunity. 2001;14:123 – 33. Ensslin AS, Formby B. Comparison of cytolytic and prolif-13. erative activities of human gamma delta and alpha beta T cells from peripheral blood against various human tumor cell lines. J Natl Cancer Inst. 1991;83:1564 – 9. Fisch P, Meuer E, Pende D, Rothenfusser S, Viale O, Kock S, 14. et al. Control of B cell lymphoma recognition via natural killer inhibitory receptors implies a role for human Vgamma9/Vdelta2 T cells in tumor immunity. Eur J Immunol. 1997;27:3368 – 79. Rothenfusser S, Buchwald A, Kock S, Ferrone S, Fisch P. 15. Missing HLA class I expression on Daudi cells unveils cyto-toxic and proliferative responses of human gammadelta T lymphocytes. Cell Immunol. 2002;215:32 – 44. Dolstra H, Fredrix H, van der Meer A, de Witte T, Figdor C, 16. van de Wiel-van Kemenade E. TCR gamma delta cytotoxic T lymphocytes expressing the killer cell-inhibitory receptor p58.2 (CD158b) selectively lyse acute myeloid leukemia cells. Bone Marrow Transplant. 2001;27:1087 – 93. Wright A, Lee JE, Link MP, Smith SD, Carroll W, Levy R, 17. et al. Cytotoxic T lymphocytes specifi c for self tumor immu-noglobulin express T cell receptor delta chain. J Exp Med. 1989;169:1557 – 64. Vollenweider I, Vrbka E, Fierz W, Groscurth P. Heterogeneous 18. binding and killing behaviour of human gamma/delta-TCR � lymphokine-activated killer cells against K562 and Daudi cells. Cancer Immunol Immunother. 1993;36:331 – 6. Kunzmann V, Bauer E, Feurle J, Weissinger F, Tony HP, 19. Wilhelm M. Stimulation of gammadelta T cells by aminobi-sphosphonates and induction of antiplasma cell activity in multiple myeloma. Blood. 2000;96:384 – 92. Choudhary A, Davodeau F, Moreau A, Peyrat MA, Bonneville 20. M, Jotereau F. Selective lysis of autologous tumor cells by recurrent gamma delta tumor-infi ltrating lymphocytes from renal carcinoma. J Immunol. 1995;154:3932 – 40. Kobayashi H, Tanaka Y, Yagi J, Toma H, Uchiyama T. Gamma/21. delta T cells provide innate immunity against renal cell carci-noma. Cancer Immunol Immunother. 2001;50:115 – 24. Maeurer MJ, Martin D, Walter W, Liu K, Zitvogel L, 22. Halusczcak K, et al. Human intestinal Vdelta1 � lymphocytes recognize tumor cells of epithelial origin. J Exp Med. 1996;183:1681 – 96. Chen J, Niu H, He W, Ba D. Antitumor activity of expanded 23. human tumor-infi ltrating gammadelta T lymphocytes. Int Arch Allergy Immunol. 2001;125:256 – 63. Hacker G, Kromer S, Falk M, Heeg K, Wagner H, Pfeffer K. 24. V delta 1 � subset of human gamma delta T cells responds to ligands expressed by EBV-infected Burkitt lymphoma cells
MEC1 cells, but not TMD2, suggesting that, in our system, ULBP3 is not required for V δ 1 recognition of B-CLL-derived cells. The increased expression of TRAILR1 on MEC1 and TMD2 compared with EM-2eGFPluc is a much more likely candidate. We will further explore the mechanisms of V δ 1 and V δ 2 cytotoxicity further against these leukemic targets.
In summary, we have shown differential cytotoxic-ity of V δ 1 and V δ 2 GDTC subsets against CML- and B-CLL-derived cell lines. Additionally, our protocol can be used to expand V δ 1 cells selectively from most healthy donors and these cells are cytotoxic to B-CLL-derived MEC1 and TMD2 cell lines. Further studies are underway to verify that V δ 1 cells from patients with B-CLL can be expanded using our method. Taken together, our data and those of others suggest that V δ 1 cells may constitute a promising immunotherapy for B-CLL. We now plan to test V δ 1 GDTC therapy in our established pre-clinical B-CLL mouse model.
Acknowledgments
We would like to thank our donors, without whom this work would not have been possible. We thank Vasiliki Economopoulos for assistance with statistical analysis. HD was supported by an American Society of Hematology Summer Studentship. AK holds the Gloria and Seymour Epstein Chair in Cell Therapy and Transplantation at University Health Network and the University of Toronto.
Confl ict of interest disclosure: JS is employed by Oncotest GmbH. Otherwise, the authors have no confl icts of interest to disclose.
References
Kabelitz D, Wesch D, He W. Perspectives of gammadelta 1. T cells in tumor immunology. Cancer Res. 2007;67:5 – 8. De Rosa SC, Andrus JP, Perfetto SP, Mantovani JJ, 2. Herzenberg LA, Roederer M. Ontogeny of gamma delta T cells in humans. J Immunol. 2004;172:1637 – 45. Hviid L, Akanmori BD, Loizon S, Kurtzhals JA, Ricke CH, 3. Lim A, et al. High frequency of circulating gamma delta T cells with dominance of the V(delta)1 subset in a healthy population. Int Immunol. 2000;12:797 – 805. Hayday AC. [gamma][delta] cells: a right time and a right 4. place for a conserved third way of protection. Annu Rev Immunol. 2000;18:975 – 1026. Bauer S, Groh V, Wu J, Steinle A, Phillips JH, Lanier LL, 5. et al. Activation of NK cells and T cells by NKG2D, a recep-tor for stress-inducible MICA. Science. 1999;285:727 – 9. Constant P, Davodeau F, Peyrat MA, Poquet Y, Puzo G, 6. Bonneville M, et al. Stimulation of human gamma delta T cells by nonpeptidic mycobacterial ligands. Science. 1994;264:267 – 70. Morita CT, Lee HK, Leslie DS, Tanaka Y, Bukowski JF, 7. Marker-Hermann E. Recognition of nonpeptide prenyl pyro-phosphate antigens by human gammadelta T cells. Microbes Infect. 1999;1:175 – 86.

764 G. M. Siegers et al.
Amendola M, Venneri MA, Biffi A, Vigna E, Naldini L. Coor-38. dinate dual-gene transgenesis by lentiviral vectors carrying synthetic bidirectional promoters. Nat Biotechnol. 2005;23:108 – 16. Yoshimitsu M, Sato T, Tao K, Walia JS, Rasaiah VI, Sleep GT, 39. et al. Bioluminescent imaging of a marking transgene and correction of Fabry mice by neonatal injection of recombinant lentiviral vectors. Proc Natl Acad Sci USA. 2004;101:16909 – 14. Tohda S, Nara N, Murohashi I, Aoki N. Establishment of an 40. interleukin-3-dependent leukemic cell line from a patient with chronic lymphocytic leukemia in the acute phase. Blood. 1991;78:1789 – 94. McCoy JL, Herberman RB, Rosenberg EB, Donnelly FC, 41. Levine PH, Alford C. 51 Chromium-release assay for cell-mediated cytotoxicity of human leukemia and lymphoid tis-sue-culture cells. Natl Cancer Inst Monogr. 1973;37:59 – 67. Siegers GM, Al-Beirouti BM, Mathieson AM, Felizardo TC, 42. Helke S, Medin JA, et al. Gamma delta T cells (GDTCs) to eliminate minimal residual disease (MRD) in chronic myeloid leukemia (CML): a pre-clinical model. Blood. 2008;112:215 – 6. Mistry AR, O ’ Callaghan CA. Regulation of ligands for the 43. activating receptor NKG2D. Immunology. 2007;121:439 – 47. Dokouhaki P, Han M, Joe B, Li M, Johnston MR, Tsao MS, 44. et al. Adoptive immunotherapy of cancer using ex vivo expanded human gammadelta T cells: a new approach. Cancer Lett. 2010;297:126 – 36. Chang CP, Yang MC, Liu HS, Lin YS, Lei HY. Concanavalin 45. A induces autophagy in hepatoma cells and has a therapeutic effect in a murine in situ hepatoma model. Hepatology. 2007;45:286 – 96. Liu Z, Li X, Ding X, Yang Y. In silico and experimental stud-46. ies of concanavalin A: insights into its antiproliferative activity and apoptotic mechanism. Appl Biochem Biotechnol. 2010;162:134 – 45. Liu B, Li CY, Bian HJ, Min MW, Chen LF, Bao JK. Antipro-47. liferative activity and apoptosis-inducing mechanism of Con-canavalin A on human melanoma A375 cells. Arch Biochem Biophys. 2009;482:1 – 6. Forsdyke DR. Role of receptor aggregation in complement-48. dependent inhibition of lymphocytes by high concentrations of concanavalin A. Nature. 1977;267:358 – 60. Alexander AA, Maniar A, Cummings JS, Hebbeler AM, 49. Schulze DH, Gastman BR, et al. Isopentenyl pyrophosphate-activated CD56 � gamma delta T lymphocytes display potent antitumor activity toward human squamous cell carcinoma. Clin Cancer Res. 2008;14:4232 – 40. Norian LA, Kucaba TA, Earel JK, Knutson T, Vanoosten RL, 50. Griffi th TS. Synergistic induction of apoptosis in primary B-CLL cells after treatment with recombinant tumor necrosis factor-related apoptosis-inducing ligand and histone deacety-lase inhibitors. J Oncol. 2009;2009:408038. Nimmerjahn F, Ravetch JV. Fcgamma receptors as regulators 51. of immune responses. Nat Rev Immunol. 2008;8:34 – 47.
and transformed B lymphocytes. J Immunol. 1992;149:3984 – 9. Duval M, Yotnda P, Bensussan A, Oudhiri N, Guidal C, 25. Rohrlich P, et al. Potential antileukemic effect of gamma delta T cells in acute lymphoblastic leukemia. Leukemia. 1995;9:863 – 8. Meeh PF, King M, O ’ Brien RL, Muga S, Buckhalts P, 26. Neuberg R, et al. Characterization of the gammadelta T cell response to acute leukemia. Cancer Immunol Immunother. 2006;55:1072 – 80. Aswald JM, Wang XH, Aswald S, Lutynski A, Minden MD, 27. Messner HA, et al. Flow cytometric assessment of autologous gammadelta T cells in patients with acute myeloid leukemia: potential effector cells for immunotherapy? Cytometry B Clin Cytom. 2006;70:379 – 90. Lamb LS Jr, Gee AP, Hazlett LJ, Musk P, Parrish RS, 28. O ’ Hanlon TP, et al. Infl uence of T cell depletion method on circulating gammadelta T cell reconstitution and potential role in the graft-versus-leukemia effect. Cytotherapy. 1999;1:7 – 19. Lamb LS Jr, Musk P, Ye Z, van Rhee F, Geier SS, Tong JJ, 29. et al. Human gammadelta( � ) T lymphocytes have in vitro graft vs leukemia activity in the absence of an allogeneic response. Bone Marrow Transplant. 2001;27:601 – 6. Bartkowiak J, Kulczyck-Wojdala D, Blonski JZ, Robak T. 30. Molecular diversity of gammadelta T cells in peripheral blood from patients with B-cell chronic lymphocytic leukaemia. Neoplasma. 2002;49:86 – 90. Poggi A, Venturino C, Catellani S, Clavio M, Miglino M, Gobbi 31. M, et al. Vdelta1 T lymphocytes from B-CLL patients recognize ULBP3 expressed on leukemic B cells and up-regulated by trans-retinoic acid. Cancer Res. 2004;64:9172 – 9. Rozman C, Montserrat E. Chronic lymphocytic leukemia. N 32. Engl J Med. 1995;333:1052 – 7. Abrisqueta P, Pereira A, Rozman C, Aymerich M, Gine E, 33. Moreno C, et al. Improving survival in patients with chronic lymphocytic leukemia (1980 – 2008): the Hospital Clinic of Barcelona experience. Blood. 2009;114:2044 – 50. Foster AE, Brenner MK, Dotti G. Adoptive T-cell immuno-34. therapy of chronic lymphocytic leukaemia. Best Pract Res Clin Haematol. 2008;21:375 – 89. Nakajima J, Murakawa T, Fukami T, Goto S, Kaneko T, 35. Yoshida Y, et al. A phase I study of adoptive immunotherapy for recurrent non-small-cell lung cancer patients with autologous gammadelta T cells. Eur J Cardiothorac Surg. 2010;37:1191 – 7. Lucas C, Ingoure S, Soule E, Faria B, Audibert F, Blery M, 36. et al. IPH1101, the fi rst specifi c gamma delta T cell agonist, shows potent immuno-biological effi cacy in low grade follicu-lar lymphoma patients when combined with rituximab: results from a phase II study. Blood. 2009;114:583. Fisch P, Malkovsky M, Braakman E, Sturm E, Bolhuis RL, 37. Prieve A, et al. Gamma/delta T cell clones and natural killer cell clones mediate distinct patterns of non-major histocom-patibility complex-restricted cytolysis. J Exp Med. 1990;171:1567 – 79.
Supplementary material available online
Supplementary Figure S1. Flow cytometric data showing Annexin V stainings pertaining to Figures 3D and 3E.Supplementary Table SI. Post-isolation purity data for isolations 10–1–7 in Figure 1.Supplementary Table SII. γδ T cell isolation and expansion data are summarized for Donor 11 from Figure 1.Supplementary Table SIII. Proportions of Vdelta1 and Vdelta2 cells in gamma delta T cell cultures from four donors are summarized.Supplementary Table SIV. Student’s t-test results for Figure 3A.