Functional PPAR-γ receptor is a novel therapeutic target for ACTH-secreting pituitary adenomas
7
NATURE MEDICINE • VOLUME 8 • NUMBER 11 • NOVEMBER 2002 1281 ARTICLES Peroxisome proliferator-activated receptor-γ (PPAR-γ), a member of the nuclear receptor superfamily 1,2 , functions as a transcription factor mediating ligand-dependent transcriptional regulation 3–5 . High-affinity PPAR-γ ligands include the insulin-sensitizing thia- zolidinedione compounds (TZDs) 6–8 . PPAR-γ activation leads to adipocyte differentiation 6 , glucose regulation 9 , inhibition of macrophage and monocyte activation 10,11 and inhibition of angio- genesis 12 . PPAR-γ is expressed in breast, prostate and colon epithe- lium, and administration of synthetic PPAR-γ ligands inhibits tumor cell growth in prostate and colon 13–16 . Rosiglitazone, a po- tent thiazolinedione oral antidiabetic agent, recently approved in the United States, differs structurally from pioglitazone and trogli- tazone, with greater PPAR-γ-binding affinity and antihyper- glycemic potency. Pituitary tumors account for approximately 15% of intracranial tumors, and they are associated with significant morbidity due to local compressive effects, hormonal hypersecretion or treatment- associated endocrine deficiency 17 . Adrenocorticotrophic hormone (ACTH)-secreting adenomas cause elevated, non-suppressible ACTH levels, hypercortisolemia and variable clinical manifesta- tions, including diabetes, hypertension and osteoporosis 18 . Unless treated, the disease is associated with high morbidity, and ulti- mately, mortality 19 . Dopamine agonists and somatostatin analogs effectively suppress prolactin (PRL) and growth hormone (GH) hy- persecretion, respectively, and they control tumor growth or in- duce shrinkage in most PRL- and GH-secreting pituitary tumors 20,21 . In contrast, there are no effective drug therapies for ACTH-secreting pituitary tumors 22–24 . Diagnosis and treatment of Cushing disease remains a chal- lenge 19,25,26 . Despite high-resolution MRI of the pituitary gland and petrosal sinus sampling to establish pituitary-derived ACTH hyper-secretion, pre-operative pituitary tumor localization and lateralization is difficult 19,25 . Although 70% of pituitary micro-ade- nomas are successfully resected by trans-sphenoidal approaches, surgical cure rates for macro-adenomas are achieved only in about one third of patients in specialized centers 23 . Post-surgical persis- tence of ACTH hypersecretion requires pituitary-directed radia- tion, the beneficial effects of which may not manifest for years, and are ultimately associated with pituitary damage and dysfunc- tion 27 . Hypercortisolism may be completely resolved by adrenalec- tomy, which does not suppress pituitary tumor growth, and is also associated with other morbidity 28 . Cyproheptadine, an anti-sero- tonin agent, has been used to suppress ACTH but ultimate efficacy was poor, and its use has been discontinued 29 . Although the anti- fungal compound ketoconazole suppresses adrenal cortisol biosynthesis, pituitary tumor growth and ACTH secretion are not inhibited, and hepatic impairment limits long-term use 30 . Here we report that PPAR-γ expression is restricted to ACTH-se- creting cells of the normal human anterior pituitary, and is abun- dantly expressed in human ACTH-secreting pituitary tumors. PPAR-γ ligands potently inhibit ACTH-secreting pituitary-tumor proliferation, and they inhibit pituitary tumor growth and secre- tion of ACTH and corticosterone. These results support the role for PPAR-γ as a novel target for treating patients with Cushing syn- drome. Selective PPAR-γ expression in pituitary corticotroph cells Using the avidin-biotin-peroxidase method in post mortem–de- rived normal human pituitary tissue, we carried out immunocyto- chemical analysis of ACTH and PPAR-γ expression. This demonstrated characteristic diffuse ACTH immunoreactive cells throughout the anterior pituitary in approximately 15% of cells; however, cells were concentrated in the intermediate region be- tween the anterior and posterior pituitary (Fig. 1a–c). PPAR-γ im- Functional PPAR-γ receptor is a novel therapeutic target for ACTH-secreting pituitary adenomas ANTHONY P. HEANEY 1 , MANORY FERNANDO 1 , WILLIAM H. YONG 2 & SHLOMO MELMED 1 Departments of 1 Medicine and 2 Pathology, Cedars-Sinai Research Institute, University of California Los Angeles School of Medicine, Los Angeles, California, USA Correspondence should be addressed to A.P.H.; email: [email protected] Published online 15 October 2002; doi:10.1038/nm784 Adrenocorticotrophic hormone (ACTH)-secreting pituitary tumors are associated with high morbidity due to excess glucocorticoid production. No suitable drug therapies are currently available, and surgical excision is not invariably curative. Here we demonstrate immunoreactive expression of the nuclear hormone receptor peroxisome proliferator-activated receptor-γ (PPAR-γ) exclusively in normal ACTH-secreting human anterior pituitary cells: PPAR-γ was abun- dantly expressed in all of six human ACTH-secreting pituitary tumors studied. PPAR-γ activators induced G 0 /G 1 cell-cycle arrest and apoptosis and suppressed ACTH secretion in human and murine corticotroph tumor cells. Development of murine corticotroph tumors, generated by subcutaneous injection of ACTH-secreting AtT20 cells, was prevented in four of five mice treated with the thiazolidinedione compound rosiglitazone, and ACTH and corticosterone secretion was suppressed in all treated mice. Based on these findings, thiazolidinediones may be an effective therapy for Cushing disease © 2002 Nature Publishing Group http://www.nature.com/naturemedicine
Transcript of Functional PPAR-γ receptor is a novel therapeutic target for ACTH-secreting pituitary adenomas

NATURE MEDICINE • VOLUME 8 • NUMBER 11 • NOVEMBER 2002 1281
ARTICLES
Peroxisome proliferator-activated receptor-γ (PPAR-γ), a memberof the nuclear receptor superfamily1,2, functions as a transcriptionfactor mediating ligand-dependent transcriptional regulation3–5.High-affinity PPAR-γ ligands include the insulin-sensitizing thia-zolidinedione compounds (TZDs)6–8. PPAR-γ activation leads toadipocyte differentiation6, glucose regulation9, inhibition ofmacrophage and monocyte activation10,11 and inhibition of angio-genesis12. PPAR-γ is expressed in breast, prostate and colon epithe-lium, and administration of synthetic PPAR-γ ligands inhibitstumor cell growth in prostate and colon13–16. Rosiglitazone, a po-tent thiazolinedione oral antidiabetic agent, recently approved inthe United States, differs structurally from pioglitazone and trogli-tazone, with greater PPAR-γ-binding affinity and antihyper-glycemic potency.
Pituitary tumors account for approximately 15% of intracranialtumors, and they are associated with significant morbidity due tolocal compressive effects, hormonal hypersecretion or treatment-associated endocrine deficiency17. Adrenocorticotrophic hormone(ACTH)-secreting adenomas cause elevated, non-suppressibleACTH levels, hypercortisolemia and variable clinical manifesta-tions, including diabetes, hypertension and osteoporosis18. Unlesstreated, the disease is associated with high morbidity, and ulti-mately, mortality19. Dopamine agonists and somatostatin analogseffectively suppress prolactin (PRL) and growth hormone (GH) hy-persecretion, respectively, and they control tumor growth or in-duce shrinkage in most PRL- and GH-secreting pituitarytumors20,21. In contrast, there are no effective drug therapies forACTH-secreting pituitary tumors22–24.
Diagnosis and treatment of Cushing disease remains a chal-lenge19,25,26. Despite high-resolution MRI of the pituitary gland andpetrosal sinus sampling to establish pituitary-derived ACTHhyper-secretion, pre-operative pituitary tumor localization and
lateralization is difficult19,25. Although 70% of pituitary micro-ade-nomas are successfully resected by trans-sphenoidal approaches,surgical cure rates for macro-adenomas are achieved only in aboutone third of patients in specialized centers23. Post-surgical persis-tence of ACTH hypersecretion requires pituitary-directed radia-tion, the beneficial effects of which may not manifest for years,and are ultimately associated with pituitary damage and dysfunc-tion27. Hypercortisolism may be completely resolved by adrenalec-tomy, which does not suppress pituitary tumor growth, and is alsoassociated with other morbidity28. Cyproheptadine, an anti-sero-tonin agent, has been used to suppress ACTH but ultimate efficacywas poor, and its use has been discontinued29. Although the anti-fungal compound ketoconazole suppresses adrenal cortisolbiosynthesis, pituitary tumor growth and ACTH secretion are notinhibited, and hepatic impairment limits long-term use30.
Here we report that PPAR-γ expression is restricted to ACTH-se-creting cells of the normal human anterior pituitary, and is abun-dantly expressed in human ACTH-secreting pituitary tumors.PPAR-γ ligands potently inhibit ACTH-secreting pituitary-tumorproliferation, and they inhibit pituitary tumor growth and secre-tion of ACTH and corticosterone. These results support the role forPPAR-γ as a novel target for treating patients with Cushing syn-drome.
Selective PPAR-γ expression in pituitary corticotroph cellsUsing the avidin-biotin-peroxidase method in post mortem–de-rived normal human pituitary tissue, we carried out immunocyto-chemical analysis of ACTH and PPAR-γ expression. Thisdemonstrated characteristic diffuse ACTH immunoreactive cellsthroughout the anterior pituitary in approximately 15% of cells;however, cells were concentrated in the intermediate region be-tween the anterior and posterior pituitary (Fig. 1a–c). PPAR-γ im-
Functional PPAR-γ receptor is a novel therapeutic target forACTH-secreting pituitary adenomas
ANTHONY P. HEANEY1, MANORY FERNANDO1, WILLIAM H. YONG2 & SHLOMO MELMED1
Departments of 1Medicine and 2Pathology, Cedars-Sinai Research Institute, University of California Los Angeles School of Medicine, Los Angeles, California, USA
Correspondence should be addressed to A.P.H.; email: [email protected]
Published online 15 October 2002; doi:10.1038/nm784
Adrenocorticotrophic hormone (ACTH)-secreting pituitary tumors are associated with highmorbidity due to excess glucocorticoid production. No suitable drug therapies are currentlyavailable, and surgical excision is not invariably curative. Here we demonstrate immunoreactiveexpression of the nuclear hormone receptor peroxisome proliferator-activated receptor-γ(PPAR-γ) exclusively in normal ACTH-secreting human anterior pituitary cells: PPAR-γ was abun-dantly expressed in all of six human ACTH-secreting pituitary tumors studied. PPAR-γ activatorsinduced G0/G1 cell-cycle arrest and apoptosis and suppressed ACTH secretion in human andmurine corticotroph tumor cells. Development of murine corticotroph tumors, generated bysubcutaneous injection of ACTH-secreting AtT20 cells, was prevented in four of five mice treatedwith the thiazolidinedione compound rosiglitazone, and ACTH and corticosterone secretion wassuppressed in all treated mice. Based on these findings, thiazolidinediones may be an effectivetherapy for Cushing disease
©20
02 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://w
ww
.nat
ure
.co
m/n
atu
rem
edic
ine

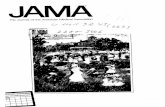
Fig. 1 Pituitary PPAR-γ expressionis restricted to normal human corti-cotroph cells. a–k, Immunocyto-chemical analysis of autopsy-derived normal human and rat pi-tuitary tissue, using immunoperox-idase (a–c and g) andTRITC-labeled ACTH (i) and im-munoperoxidase (d–f and h) andFITC-labeled (j) PPAR-γ antibodies.In human pituitary tissue, ACTH– and PPAR-γ–DAB immunoreactivity(brown) was visible in corticotroph cells throughout the anterior pituitaryand concentrated in the basophilic cells, which invade the posterior pitu-itary. In the rat pituitary, ACTH immunoreactivity was seen in the anteriorand intermediate pituitary (g and inset), whereas PPAR-γ immunoreactivitywas confined to the anterior pituitary corticotrophs (h and inset). Double
1282 NATURE MEDICINE • VOLUME 8 • NUMBER 11 • NOVEMBER 2002
ARTICLES
munoreactivity was evident throughout the anterior pituitary inlarge basophilic cells containing inclusion bodies characteristic ofcorticotrophs. Immunoreactivity was particularly apparent inACTH-immunoreactive basophilic cells, which typically invadedthe posterior pituitary region (Fig. 1d–f). In rat pituitary tissue,ACTH immunoreactivity was evident in the anterior and interme-diate pituitary (Fig. 1g and inset). In support of our findings inhuman pituitary tissues, PPAR-γ immunoreactivity occurredthroughout the rat anterior pituitary in large basophilic ACTH-im-munoreactive cells (Fig. 1h and inset). In the human pituitary,double immunofluorescence studies using tetra-methyl rho-damine isothiocyanate (TRITC)-labeled ACTH (Fig. 1i) and fluo-rescein isothiocyanate (FITC)-labeled PPAR-γ (Fig. 1j) antibodiesrevealed that PPAR-γ immunoreactivity colocalized with ACTH-immunoreactive cells (Fig. 1k). Co-immunostaining showed thatsome corticotrophs exhibited both PPAR-γ and α-melanocytestimulating hormone (α-MSH) expression. However, other corti-cotrophs selectively exhibited only PPAR-γ or α-MSH immunore-activity respectively (data not shown).
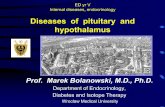
PPAR-γ expression in human ACTH-secreting pituitary tumorsGiven the observed colocalization of PPAR-γ and ACTH in normalhuman anterior pituitary corticotroph cells, PPAR-γ expressionwas assessed in six surgically resected ACTH-secreting pituitarytumor specimens. Western blotting of pituitary tumor–derivedprotein extracts revealed abundant PPAR-γ expression in all sixACTH-secreting pituitary tumors examined, in comparison with
modest PPAR-γ expression in two normal pituitary-derived ex-tracts (Fig. 2a). Longer film exposures confirmed low-level PPAR-γexpression in normal pituitary tissue extracts (data not shown).Immunocytochemical analysis demonstrated abundant PPAR-γimmunoreactivity localized to those pituitary adenoma cells thatalso expressed ACTH (Fig. 2b).
Functional role for pituitary PPAR-γ receptor in vitroTo determine the functional significance of pituitary corticotrophPPAR-γexpression, we tested the effects of PPAR-γ ligands on ACTH-secreting pituitary tumor cells in vitro. Troglitazone or rosiglitazonetreatment (1 × 10–6 to 10–4 M) for up to 48 hours in serum-free con-ditions, or up to 96 hours for cells maintained in serum-replete con-ditions, induced G0/G1 cell-cycle arrest, and led to decreasednumber of cells in S-phase (Fig. 3a). Western-blot analysis of proteinextracts derived from TZD-treated murine and human corticotrophcells showed an approximately 60% decrease in Ser795 phosphory-lated retinoblastoma (Rb) protein expression (Fig. 3b and c), indicat-ing an Rb-mediated mechanism for the G0/G1 cell-cycle arrest.
Rosiglitazone (1 × 10–5 to 10–4 M) treatment of mouse corti-cotroph pituitary tumor cells (AtT20) cells for 48 hours demonstrated a dose-dependent increase in Annexin-FITC im-munoreactive AtT20 cells, and enhanced apoptosis (Fig. 3d) (P <0.001). A similar increase in Annexin-FITC immunoreactive cellsoccurred after treatment of human pituitary corticotroph tumorcultures with rosiglitazone (1 × 10–5 M) (Fig. 3e). TUNEL analysisconfirmed that TZD induced cell death, and increased apoptosis
a b
f
c d
g h
i j k
immunofluorescence using TRITC-labeled ACTH (i) and FITC-labeled PPAR-γ (j) antibodies demonstrated colocalization of PPAR-γ and ACTH im-munoreactivity (k). AP, anterior pituitary; IP, intermediate pituitary; PP,posterior pituitary; BI, basophil invasion. Arrows indicate inclusion bodies, acharacteristic feature of corticotroph cells. Magnification: ×200 (a and d);×400 (b, e and i–k); ×100 (c, f and insets in g and h).
e
©20
02 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://w
ww
.nat
ure
.co
m/n
atu
rem
edic
ine

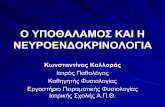
Fig. 3 Functional PPAR-γ in pituitarycorticotroph tumors. a–e, FACS analy-sis of troglitazone- or rosiglitazone(Ros)-treated serum-replete mouse(a,b,d and f) and human (c and e)ACTH-secreting pituitary tumor cells invitro demonstrated increased G1phase, decreased S phase (a) (*, P =0.009; **, P = 0.001), decreased ex-pression of Ser794 phosphorylatedretinoblastoma protein (b and c), and adose-dependent increase in Annexin-FITC immunoreactive cells in murine(d) and human (e) ACTH-secreting pi-tuitary tumor cells respectively, inkeeping with TZD-mediated inductionof G1 cell-cycle arrest and apoptosis.M, protein marker (b and c). d, �, vehi-cle; �, 1 × 10–5 M Ros; �, 2 × 10–5 MRos; �, 5 × 10–5 M Ros; , 10 × 10–5
M Ros. f, TUNEL analysis demonstrated a 2-fold increase in rosiglitazone-in-duced apoptosis. *, P = 0.0003. Pretreatment of AtT20 cells with rosiglita-zone blocked anti-apoptotic effects of CRH and induced corticotroph cellapoptosis (**, P = 0.0003). �, control; �, 1 × 10–6 M Ros; �, 1 × 10–5 M Ros;�, 50 nM CRH; , 50 nM CRH + 1 × 10–5 M Ros. Each bar representsmean ± s.e.m. of 3 fields in 2 separate experiments. JEG-3 choriocarcinomacells served as a positive control.
NATURE MEDICINE • VOLUME 8 • NUMBER 11 • NOVEMBER 2002 1283
ARTICLES
about three-fold (Fig. 3f). Corticotrophin-releasing hormone(CRH) is a potent corticotroph proliferative factor31. Pretreatmentof AtT20 cells with TZD before CRH treatment (50 nM) blockedthe growth-promoting effects of CRH (50 nM for 24 h) and in-duced corticotroph cell apoptosis (Fig. 3f).
Western-blot analysis of protein extracts derived from TZD-treated corticotroph cells showed decreased expression of the anti-apoptotic protein Bcl-2 and increased levels of pro-apoptotic Baxand p53 expression (Fig. 4a and b), indicating a mechanism forPPAR-γ mediated apoptosis. An approximately four-fold increasein cleaved caspase-3 and a concomitant decrease in total caspase-3resulted from TZD-treatment, and were consistent with enhancedapoptosis (Fig. 4c).
PPAR-γ ligands inhibit Pomc and Pttg expressionAlternate pro-opio melanocortin (POMC) precursor peptide pro-
cessing in corticotroph cells gives rise to ACTH (ref. 32), thetrophic hormone for adrenal steroidogenesis. Northern-blotanalysis of total RNA extracted from TZD-treated AtT20 cells re-vealed that the ligand inhibited Pomc mRNA abundance aboutfour-fold (Fig. 4d). In addition, we observed a three-fold decreasein mRNA expression of the proliferative marker, pituitary tumortransforming gene (Pttg), confirming decreased proliferative ratesof TZD-treated corticotroph tumor cells (Fig. 4d).
CRH-treatment of AtT20 cells, transiently transfected with thePomc-promoter, resulted in a 1.6-fold increase in Pomc-transcrip-tion. Rosiglitazone treatment alone, or prior to CRH-treatment,abrogated basal and CRH-induced Pomc transcription (Fig. 4e).
PPAR-γ ligands inhibit in vivo pituitary tumor growthAs the TZDs exhibited anti-proliferative and pro-apoptotic effectsin vitro, effects of TZD-treatment were assessed on growth of corti-cotroph pituitary tumors in vivo. Corticotroph AtT20 tumor cells(∼ 2 × 105 cells) were inoculated subcutaneously in four-week-oldfemale athymic nude mice, and animals randomized to receive ei-ther oral rosiglitazone (150 mg/kg/day) or vehicle. Baseline pre-treatment ACTH and corticosterone levels in serum werecomparable in the control and rosiglitazone-treated groups (datanot shown; P = not significant). After four weeks, four of five un-treated control mice had developed visible subcutaneous corti-cotroph tumors (1–2 cm diameter). In contrast, only one of fiverosiglitazone-treated animals developed a small subcutaneous cor-ticotroph cell tumor (0.1 cm diameter) (Fig. 5a and b). PlasmaACTH (98 ± 33 pg/ml versus 2085 ± 847 pg/ml, ACTH, mean ±
a
b
Fig. 2 PPAR-γ is abundantly expressed in human ACTH-secreting pituitarytumors. a–b, Western-blot (a) and immunocytochemical (b) analysis depict-ing abundant PPAR-γ expression in 6 surgically resected ACTH-secreting pitu-itary tumors (T1-6), in comparison with PPAR-γ expression in 2 normalpituitary tissue-derived extracts (NP). β-actin immunoblotting confirmedequivalent total protein loading. MCF-7 breast-cancer cells served as a posi-tive control. M, protein marker. High magnification confirmed cytoplasmicgranular PPAR-γ immunoreactivity; magnification: ×400 (b) and ×800 (inset).
Vehicle Ros (2 x 10–5 M)
G0-G1: 79 %S: 18 %
* G0-G1: 85 %** S: 11 %
50
200
400
600
800
1000
0
100 1500 50
200
400
600
800
1000
0
100 1500
apRb
β-actin
JEG
-3
M Vehi
cle
1 5 10 Ros (10–5 M)
97 kD
46 kD
bVe
hicl
e Ros (10–5 M)
pRb
β-actin
2 5MJEG
-3
c
0
25
50
75
100
Apo
ptot
ic c
ells
(%)d Vehicle 5 x 10–5 M
Ros
e
0
25
50
75
100
Ap
opot
ic c
ells
(%
)
*
*
**
f
©20
02 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://w
ww
.nat
ure
.co
m/n
atu
rem
edic
ine

1284 NATURE MEDICINE • VOLUME 8 • NUMBER 11 • NOVEMBER 2002
ARTICLES
s.e.m., P ≤ 0.05) and serum corticosterone (113 ± 17 ng/ml versus785 ± 374, corticosterone, mean ± s.e.m., P ≤ 0.05) levels weremarkedly lower in rosiglitazone-treated mice compared with vehi-cle-treated tumor-bearing animals (Fig. 5c and d).
Although TZD-treatment prevented experimental pituitary cor-ticotroph tumor development in vivo, patients invariably presentwith already established and actively growing pituitary tumors.We therefore tested the effects of TZD treatment on growth of al-ready established experimental pituitary corticotroph tumors andsteroid hormone levels in vivo. AtT20 were inoc-ulated subcutaneously in athymic nude mice,and tumors were allowed to develop. By threeweeks, all mice had developed large visible tu-mors, and they were then randomized to receiveeither oral rosiglitazone (150 mg/kg/day) or ve-hicle. Baseline levels of serum ACTH and corti-costerone and tumor volumes did not differamong the mice subsequently randomized ascontrol or rosiglitazone-treated groups (data notshown; P = not significant). In both groups,tumor growth continued, but it was diminished(P < 0.05) in three of five rosiglitazone-treatedmice (Fig. 6a and b). The phenotypic appearanceof the mice was markedly different, and vehicle-treated mice were wasted, developed skin atro-phy and appeared pigmented, with features ofhypercortisolism (Fig. 6b). In contrast, rosiglita-zone-treated mice continued to thrive and gainweight and did not display skin atrophy or pig-mentation. In addition, rosiglitazone treatmentled to an approximately 80% reduction in theproliferative marker, Pttg mRNA, and an approx-imately 60% reduction in Pomc mRNA (Fig. 6c),confirming the in vitro observations. Moreover,
there was a 75% reduction in plasma ACTH (Fig. 6d) (controls,3841 ± 308 versus Ros-treated, 978 ± 452 pg/ml, mean ± s.e.m.ACTH, P = 0.002) and a 96% reduction in serum corticosteronelevels (Fig. 6e) (controls, 4304 ± 2593 versus ros-treated, 181 ± 56ng/ml, mean ± s.e.m. corticosterone, P < 0.05).
Preserved normal pituitary-adrenal functionGiven the observed pituitary corticotroph PPAR-γ expression, theTZD-induced decrease in plasma ACTH and corticosterone levels
Bcl
Bax
β-actin
JEG
-3
M Vehi
cle
Ros 5 (10–5 M)
26 kD
30 kD
46 kD
a
p53
Ponceau S
53 kD
JEG
-3
M Vehi
cle Ros Trog
1 10 10 (10–5 M)
b
Caspase-3
Caspase-3 (cleaved)
JEG
-3
M Vehi
cle Ros Trog
1 10 10 (10–5 M)
30 kD
17 kD
c
Pomc
Pttg
18S
Rat
test
is
M Vehi
cle
5 10 10
Ros Trog
(x 10–5 M)
d
0
1
2
Vehicle CRH(50 nM)
Ros(10–5M)
CRH + Ros(50 nM + 10–5M)
POM
C-lu
cfo
ld in
crea
se
* **
e
Fig. 4 TZDs inhibit corticotroph cell proliferation, ACTH synthesis and se-cretion, and induce apoptosis. a and b, Western-blot analysis demon-strated reduced expression of the anti-apoptotic protein Bcl-2, increasedpro-apoptotic proteins Bax (a) and p53 (b). c, Dose-dependent increase inTZD-mediated cleaved caspase-3 and a concordant decrease in uncleavedcaspase-3 confirms the pro-apoptotic effect of PPAR-γ ligands. d, Northern-blot analysis of TZD-treated corticotroph cell-derived total RNA extractsdemonstrated inhibition of Pomc mRNA levels, and decreased Pttg mRNAexpression, confirming decreased proliferative rates in the TZD-treated cor-ticotroph pituitary tumor cells. 18S ribosomal RNA served to normalize RNAloading. Rat testis served as a positive control. e, Rosiglitazone effects onbaseline and CRH-induced (50 nM) Pomc transcription. AtT20 cells pre-treated for 48 h with 1 × 10–5 M rosiglitazone, and Pomc-luc transfectedusing lipofectamine. Results are expressed as fold induction of luciferase ac-tivity over control (vehicle), corrected for β-galactosidase activity (mean of3 wells in 3 independent experiments ± s.e.m.), by ANOVA and Bonferroni
multiple-comparison test. *, P < 0.05 compared with control; **, P < 0.05compared with CRH. JEG-3 choriocarcinoma cells served as a positive con-trol. M represents protein or RNA marker.
vehicle
ros
0
1
3
5
Tota
l tum
ornu
mb
er
*
a b
0
100
1000
3000
AC
TH(p
g/m
l)
*
c
0
500
1000
Cor
ticos
tero
ne(n
g/m
l)
*
d
Fig. 5 Rosiglitazone inhibits corticotroph pituitary tumor growth in vivo. Following subcu-taneous inoculation of corticotroph pituitary tumor cells (∼ 2000 cells) into 4-wk-old femaleathymic nude mice, animals were randomized to receive either oral rosiglitazone (150mg/kg/day; �) or vehicle (�). a, Representative photograph of mice treated with vehicle(upper panel) or rosiglitazone (lower panel). b–c, Tumor numbers (b), serum ACTH (c) andcorticosterone levels (d) after 4 wk treatment with vehicle or rosiglitazone. n = 5 per group.*, P < 0.05.
©20
02 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://w
ww
.nat
ure
.co
m/n
atu
rem
edic
ine

NATURE MEDICINE • VOLUME 8 • NUMBER 11 • NOVEMBER 2002 1285
ARTICLES
in vivo, and the potential useof these agents as medicaltherapy for Cushing disease,we assessed the effects ofprolonged rosiglitazone ad-ministration on endogenousnon-tumorous murine pitu-itary-adrenal responses instressed and unstressed con-ditions. Restraint stress is apotent inducer of ACTH andCorticosterone. Plasma ACTH(Fig. 6f) and serum corticos-terone (data not shown)were similar in rosiglita-zone-treated (150 mg/kg for6 wk) and untreated normalathymic nu/nu mice in bothunstressed (quiet environ-ment overnight) andstressed conditions (15 minrestraint).
DiscussionAbout 90% of ACTH-secret-ing pituitary tumors aremicro-adenomas (< 1 cm di-ameter), and cavernous sinusinvasion or optic chiasmcompression are uncommon-ly encountered18,19. However,steroid hypersecretion causedby Cushing syndrome causesparticularly disabling andlife-threatening symptomsincluding hypertension, dia-betes, osteo- porosis andmuscle weakness. No med-ical therapies are currentlyavailable for Cushing syn-drome. In specialized cen-ters, surgical resection ofACTH-secreting pituitarymicro-adenomas (< 1 cm di-ameter) offers an overall curerate of about 70–80%, but formacro-adenomas (> 1 cm diameter) control rates are only approxi-mately 30%. Moreover, the extensive surgical resection requiredportends significant risk to surrounding normal pituitary tissue,leading to partial or total hypopituitarism in about 80% ofcases22,23,33.
PPAR-γ expression in normal pituitary tissue is restricted andcolocalizes with ACTH-secreting cells in the pituitary intermediateregion. Immunoreactive PPAR-γ was not expressed in the rat pitu-itary intermediate lobe. In contrast, abundant PPAR-γ expressionwas seen in all of six corticotroph pituitary tumors examined, com-pared with minimal expression seen in normal pituitary tissues;the latter finding was confirmed by longer film exposures (data notshown). PPAR-γ protein immunostaining is localized within theACTH-secreting tumor cells themselves. TZD treatment of corti-cotroph pituitary tumor cells in vitro induced G0/G1 cell arrest andapoptosis, indicating the functional significance of PPAR-γ expres-
sion in corticotroph tumors. Furthermore, TZD-treatment pre-vented pituitary corticotroph tumor formation in vivo, and led tomarked abrogation of pituitary tumor growth of already estab-lished and actively growing pituitary corticotroph tumors.Notably, long-term rosiglitazone treatment (150 mg/kg for 6 wk)did not alter murine endogenous pituitary-adrenal responses.PPAR-γ expression appears restricted to a subset of corticotrophs,raising the possibility that PPAR-γ ligand-mediated actions in thecorticotroph cell may be selective, allowing their use in treatmentof Cushing disease without affecting functions of corticotroph cellsthat do not express PPAR-γ.
TZDs inhibit prostate, breast and colorectal tumor growth invitro13–15, and mechanisms proposed for TZD-induced cell-cycle ar-rest include preventing Rb phosphorylation by inhibiting cyclinD1-kinase activity34, and increased p21 (Cip)35 and p27 (Kip)36 ex-pression. Candidate molecules that mediate TZD-induced apopto-
1 2 3 4 5
25
50
75
Weeks
0Tum
or v
olum
e (c
m3 )
Ros
Baseline(3 wk)
Vehicle
Treatment(3 wk)
a
b
Vehicle Ros
Pttg
18s
Rat
test
is
M
Pomc
c
0500
10001500
30004000
AC
TH (
pg/
ml)
*d
0
100
200500
250045006500
Cor
ticos
tero
ne(n
g/m
l) **e
0
200
400
1000
3000
5000
AC
TH (
pg/
ml)
Controls Ros
f
Fig. 6 Rosiglitazone treatment retards growth of established pituitary corticotroph tumors and suppresses steroid hor-mone levels in vivo (n = 5). Mice were inoculated subcutaneously with corticotroph pituitary tumor cells, and tumorswere allowed to develop. By 3 wk, all mice developed large visible tumors and animals and were randomized to receiveeither rosiglitazone (150 mg/kg/day) (n = 5) or vehicle (n = 5). Baseline serum ACTH and corticosterone levels and tumorvolumes were comparable in vehicle- and rosiglitazone-treated groups. a, After 4 wk treatment, tumor volumes (repre-sentative growth curve) were diminished in rosiglitazone-treated animals (P < 0.05). �, vehicle-treated; �, rosiglitazone-treated mice. Arrow indicates time of treatment initiation. b, Amelioration of Cushing phenotypic appearance coincidedwith tumor reduction. c, Tumor abrogation was associated with reduced Pttg and Pomc mRNA expression. 18s ribosomalRNA served to normalize RNA loading. M, RNA marker. d and e, Tumor abrogation was associated with reduction inserum ACTH (d) and corticosterone (e). �, vehicle; �, rosiglitazone. *, P = 0.002; **, P < 0.05. Values represent samplesdrawn 4 wk after starting rosiglitazone or vehicle treatment. f, Pituitary corticotroph responsiveness is preserved follow-ing long-term rosiglitazone-treatment in normal mice. Plasma ACTH (at 14:00 hours, i.e. 2pm), unstressed (�) and fol-lowing 15 min restraint stress (�) in normal female athymic nu/nu mice following 6 wk oral treatment with vehicle orrosiglitazone (Ros; 150 mg/kg/day). P = not significant
©20
02 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://w
ww
.nat
ure
.co
m/n
atu
rem
edic
ine

1286 NATURE MEDICINE • VOLUME 8 • NUMBER 11 • NOVEMBER 2002
ARTICLES
sis include reduced Bcl-2, and increased Bax and tumor necrosisfactor–related apoptosis-inducing ligand (TRAIL) (refs. 13,37).Western-blot analysis of TZD-treated pituitary corticotroph tumorprotein extracts revealed reduced phosphorylated Rb and Bcl-2,and increased Bax expression, suggesting a mechanism for theTZD-mediated cell-cycle arrest and apoptosis. As a four-fold in-crease in p53 expression was observed following TZD-treatment ofAtT20 cells, additional mechanisms may underlie TZD-mediatedapoptosis in pituitary cells.
Much of the attendant morbidity of pituitary corticotroph tu-mors is due to exposure to steroid hormone excess prior to treat-ment, or consequential hormonal deficiency following surgical orradiotherapeutic pituitary ablation4,9,14. In this regard, a potentialrole for TZDs in the management of pituitary corticotroph tumorsis compelling, as in addition to exerting inhibitory effects on pitu-itary tumor growth, they also inhibit tumor ACTH synthesis andsecretion. However, the potential use of TZDs in treating patientswith Cushing disease requires validation in a controlled clinicaltrial.
Surveillance of more than 4,500 patients shows that rosiglita-zone is a safe, effective monotherapy or combination therapy forpatients with type 2 diabetes38, and unlike troglitazone, which hasbeen associated with idiosyncratic hepatotoxicity, rosiglitazone isassociated with low incidence of liver abnormalities. Given abun-dant and selective PPAR-γ expression in corticotroph pituitary tu-mors compared with normal pituitary tissue, we propose a role forthe use of PPAR-γ receptor ligands, such as rosiglitazone, in themanagement of Cushing syndrome due to ACTH-secreting pitu-itary tumors.
MethodsPatients and tissues. Surgically resected ACTH-secreting pituitary adenomasamples were obtained in accordance with Cedars-Sinai Institutional ReviewBoard guidelines. For primary human pituitary cultures, fresh pituitary tumortissue was minced mechanically and digested for 15 min at 37 °C with 0.35%collagenase and 0.1% hyaluronidase (Sigma) in 10 ml DMEM medium(Gibco BRL, Grand Island, New York). Cell suspensions were cultured for 24 hin low-glucose DMEM containing 10% FBS, 2 mM/l glutamine and anti- biotics, before treatment with vehicle or rosiglitazone.
Mice. In accordance with Cedars-Sinai Institutional Animal Care and UseCommittee guidelines, mouse pituitary ACTH-secreting AtT20 tumor cells (∼ 2× 105) were inoculated subcutaneously in 4-wk-old female nu/nu mice, andanimals randomized to receive rosiglitazone 150 mg/kg/day or vehicle. Micewere killed by CO2 inhalation, tumors weighed, and aliquots frozen andstored for subsequent analysis.
Cell culture. Subconfluent AtT20 mouse pituitary (ACTH-secreting) cells (1 ×106 per well) were cultured in DMEM medium in 6-well plates, supplementedwith 10% FBS and antibiotics at 37 °C in 5% CO2 for 24 h before treatmentwith troglitazone or rosiglitazone. Medium was replenished with ligandsevery 2 d, and cells maintained in medium with serum or in serum-freemedium for up to 96 h.
Cell-cycle distribution. AtT20 cells were trypsinized, centrifuged (1,500g for2 min), washed with PBS, and treated with 20 g/ml Rnase A (Calbiochem, LaJolla, California). DNA was stained with 100 µg/ml propidium iodide (PI) for30 min at 4 °C and protected from light, before analysis with a FACScan(Becton Dickinson, Franklin Lakes, New Jersey).
Apoptosis assays. AtT20 and human corticotroph tumor cells were treated,trypsinized, centrifuged and washed before incubation with a FITC-labeledmonoclonal Annexin antibody and PI for 30 min at room temperature ac-cording to manufacturer’s instructions (Pharmingen, San Diego, California).Approximately 1 × 106 cells were analyzed by flow cytometry, labeled nuclei(PI) were gated on light scatter to remove debris and the percentage of
Annexin-FITC-positive cells was determined. Apoptosis-induced nuclear DNAfragmentation (TUNEL) was detected using the in situ cell-death detection kit,TMR red (Roche Diagnostics, Indianapolis, Indiana). Briefly, TZD-treatedAtT20 cells were fixed in 4% paraformaldehyde, permeabilized with a solu-tion of 0.1% sodium citrate and 0.6% Tween 20 (pH 7.4) for 2 min at 4 °Cbefore incubation in a TUNEL reaction mix (TMR red in dNTP mix, TdT andlabeling buffer) for 60 min at 37 °C. Annexin-FITC- or TMR red-positive cellswere also visualized with an Olympus BH2 immunofluorescent microscope.
Transfection with Pomc promoter. Following incubation in serum-repletemedium with or without rosiglitazone (1 × 10–5 M) for 48 h, a Pomc promoterreporter construct (–706 to +64 rat Pomc-luc; provided by M. Low)39 wastransiently transfected into AtT20 cells using Lipofectamine 2000 (GibcoBRL). Cells were then incubated with rosiglitazone (1 × 10–5 M) or corti-cotrophic-releasing hormone (CRH, 50 nm) as described40.
Northern-blot analysis. Total RNA was extracted from cell cultures (∼ 3 × 107
cells per group) or from excised tissues with TRIzol (Gibco BRL). Rat testis RNAserved as a positive control for Pttg expression. Electrophoresed RNA wastransferred to Hybond-n nylon membranes (Amersham International,Buckinghamshire, UK) and hybridized as described41.
Immunocytochemical studies of pituitary glands. All tissues were fixed in4% paraformaldehyde and processed for paraffin embedment. 10-µm sec-tions were immunostained using antibodies to human or mouse ACTH(1:1000) (DAKO, Carpinteria, California) and PPAR-γ (1:500) (Calbiochem, LaJolla, California), using both the avidin-biotin-peroxidase method and avidin-biotin-FITC and -TRITC for double immunostaining, and then counter-stainedwith hematoxylin. Negative controls were performed for each slide, usingpre-absorbed or non-immune serum.
Western-blot analysis. Protein samples were prepared in RIPA buffer, re-solved on 12% SDS–PAGE, and proteins transferred to nitrocellulose mem-branes before blotting with antibodies to Bcl-2 (1:500), Bax (1:1000), TRAIL(1:500), p53 (1:1000) (all from Santa Cruz Biotechnology, Santa Cruz,California), p-Rb (Ser 795) (1:1000) and cleaved and uncleaved caspase-3(1:500) (Cell Signaling, Beverly, Massachusetts) overnight at 4 °C. After wash-ing, membranes were incubated with appropriate immunoglobulin G–horse-radish peroxidase conjugates, and immunoreactive protein bands werevisualized with ECL (Amersham International). Total protein was normalizedby reprobing with antibodies to actin (1:5000; Sigma) or Ponceau S staining,and protein bands were quantified by densitometry (Video Densitometermodel 620, Bio-Rad, Hercules, California).
AcknowledgmentsThis study was supported by the Doris Factor Molecular EndocrinologyLaboratory, the Annenberg Foundation and NIH grant CA75979.
Competing interests statementThe authors declare that they have no competing financial interests.
RECEIVED 3 JUNE; ACCEPTED 18 SEPTEMBER 2002
1. Issemann, I. & Green, S. Activation of a member of the steroid hormone receptor su-perfamily by peroxisome proliferators. Nature 347, 645–660 (1990).
2. Schoonjans, K., Martin, G., Staels, B. & Auwerx, J. Peroxisome proliferator-activatedreceptors, orphans with ligands and functions. Curr. Opin. Lipidol. 8, 159–166(1997).
3. Kliewer, S.A., Umesono, K., Noonan, D.J., Heyman, R.A. & Evans, R.M. Convergenceof 9-cis retinoic acid and peroxisome proliferator signaling pathways through het-erodimer formation of their receptors. Nature 358, 771–774 (1992).
4. Palmer, C.A.N., Hsu, M.H., Griffin, K.J. & Johnson, E.F. Interaction of the peroxisomeproliferator-activated receptor α with the retinoid X receptor α unmasks a crypticperoxisome proliferator response element that overlaps an ARP-1-binding site in theCYP4A6 promoter. J. Biol. Chem. 270, 16114–16121 (1995).
5. Tontonoz, P., Hu, E., Graves, R.A., Budavari, A.I. & Spiegelman, B.M. mPPARγ2:Tissue-specific regulator of an adipocyte enhancer. Genes Dev. 8, 1224–1234(1994).
6. Spiegelman, B.M. PPAR-γ: Adipogenic regulator and thiazolidinedione receptor.Diabetes 47, 507–514 (1998).
7. Kliewer, S.A. et al. A prostaglandin J2 metabolite binds peroxisome proliferator-acti-
©20
02 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://w
ww
.nat
ure
.co
m/n
atu
rem
edic
ine

NATURE MEDICINE • VOLUME 8 • NUMBER 11 • NOVEMBER 2002 1287
ARTICLES
vated receptor γ and promotes adipocyte differentiation. Cell 83, 813–819 (1995).8. Forman, B.M., Tontonoz, P., Chen, J., Brun, R.P., Spiegelman, B.M. & Evans, R.M.
15-Deoxy-∆12,14-prostaglandin J1 is a ligand for the adipocyte determination fac-tor PPAR γ. Cell 83, 803–812 (1995).
9. Saltiel, A.R. & Olefsky, J.M. Thiazolidinediones in the treatment of insulin resistanceand type II diabetes. Diabetes 45, 1661–1669 (1996).
10. Ricote, M., Li, A.C., Willson, T.M., Kelly, C.J. & Glass, C.K. The peroxisome prolifera-tor-activated receptor-γ is a negative regulator of macrophage activation. Nature391, 79–82 (1998).
11. Jiang, C., Ting, A.T. & Seed, B. PPAR-γ agonists inhibit production of monocyte in-flammatory cytokines. Nature 391, 82–86 (1998).
12. Xin, X., Yang, S., Kowalski, J. & Gerritsen, M.E. Peroxisome proliferator-activated re-ceptor γ ligands are potent inhibitors of angiogenesis in vitro and in vivo. J. Biol.Chem. 274, 9116–9121 (1999).
13. Staels, B. et al. Activation of human aortic smooth-muscle cells is inhibited by PPAR-α but not PPAR-γ activators. Nature 393, 790–793 (1998).
14. Elstner, E. et al. Ligands for peroxisome proliferator-activated receptor-γ and retinoicacid receptor inhibit growth and induce apoptosis of human breast cancer cells invitro and in BNX mice. Proc. Natl. Acad. Sci. USA 95, 8806–8811 (1998).
15. Kubota, T. et al. Ligand for peroxisome proliferator-activated receptor-γ (troglita-zone) has potent anti-tumor effects against prostate cancer both in vitro and in vivo.Cancer Res. 58, 3344–3352 (1998).
16. Sarraf, P. et al. Differentiation and reversal of malignant changes in colon cancerthrough PPAR γ. Nature Med. 4, 1046–1052 (1998).
17. Heaney, A.P. & Melmed, S. Molecular pathogenesis of pituitary tumors. in OxfordTextbook of Endocrinology (eds. Wass, J.A.H. & Shalet S.M.) 2, 109–120 (OxfordUniversity Press, Oxford, 2002).
18. Ross, E.J. & Linch, D.C. Cushing’s syndrome-killing disease: Discrimatory value ofsigns and symptoms aiding early diagnosis. Lancet 2, 646–649 (1982).
19. Oldfield, E.W. et al. Petrosal sinus sampling with and without corticotrophin-releas-ing hormone for the differential diagnosis of Cushing’s syndrome. N. Engl. J. Med.325, 897–905 (1991).
20. Shimon, I. & Melmed, S. Management of pituitary tumors. Ann. Intern. Med. 129,472–483 (1998).
21. Melmed, S. et al. Consensus: Guidelines for acromegaly management. J. Clin.Endocrinol. Metab. 87, 4054–4058 (2002).
22. Simmons, N.E., Alden, T.D., Thorner, M.O. & Laws, E.R. Jr. Serum cortisol responseto transphenoidal surgery for Cushing disease. J. Neurosurg. 95, 1–8 (2001).
23. Mampalam, T.J., Tyrrell, J.B. & Wilson, C.B. Transsphenoidal microsurgery forCushing’s disease: A report of 216 cases. Ann. Intern. Med. 109, 487–493 (1988).
24. Hoybye, C. et al. Adrenocorticotrophic hormone-producing pituitary tumors: 12 to22-year follow-up after treatment with sterotactic radiosurgery. Neurosurgery 49,
284–291 (2001).25. Findling, J.W. & Raff, H. Diagnosis and differential diagnosis of Cushing’s syndrome.
Endocrinol. Metab. Clin. North Am. 30, 729–477 (2001).26. Orth, D.N. Cushing’s syndrome. N. Engl. J. Med. 332, 791–803 (1995).27. Brada, M. et al. The long-term efficacy of conservative surgery and radiotherapy in
the control of pituitary adenomas. Clin. Endocrinol. 38, 571–578 (1993).28. Trainer, P.J. & Besser, M. Cushing’s syndrome: Therapy directed at the adrenal
glands. Endocrinol. Metab. Clin. North. Am. 23, 571–584 (1994).29. Krieger, D.T., Amorosa, L. & Linick, F. Cyproheptadine-induced remission of
Cushing’s disease. N. Engl. J. Med. 293, 893–896 (1975).30. Sonino, N. The use of ketoconazole as an inhibitor of steroid production. N. Engl. J.
Med. 317, 812–818 (1987).31. Vale, W., Spiess, J., Rivier, C. & Rivier, J. Characterization of a 41-residue ovine hypo-
thalamic peptide that stimulates secretion of corticotropin and β-endorphin. Science213, 1394–1397 (1981).
32. White, A. & Gibson, S. ACTH precursors: Biological significance and clinical rele-vance. Clin. Endocrinol. 48, 251–255 (1998).
33. Trainer, P.J. et al. Transsphenoidal resection in Cushing’s disease: Undetectableserum cortisol as the definition of successful treatment. Clin. Endocrinol. 38, 73–78(1993).
34. Wakino, S., et al. Peroxisome proliferator-activated receptor γ ligands inhibitretinoblastoma phosphorylation and G1 → S transition in vascular smooth cells. J.Biol. Chem. 275, 22435–22441 (2000).
35. Sugimura, A. et al. Troglitazone suppresses cell growth of myeloid leukemia cell linesby induction of p21WAF1/CIP1 cyclin-dependent kinase inhibitor. Biochem. Biophys.Res. Comm. 261, 833–837 (1999).
36. Motomura, W., Okumura, T., Takahashi, N., Obara, T. & Kohgo, Y. Activation ofperoxisome proliferator-activated receptor γ by troglitazone inhibits cell growththrough the increase of p27Kip1 in human pancreatic carcinoma cells. Cancer Res.60, 5558–5564 (2000).
37. Goke, R., Goke, A., Goke, B. & Chen, Y. Regulation of TRAIL-induced apoptosis bytranscription factors. Cell Immunol. 201, 77–81 (2000).
38. Goldstein, B.J. Rosiglitazone. Int. J. Clin. Pract. 54, 333–337 (2000).39. Hammer, G.D., Fairchild-Huntress, V. & Low, M.J. Pituitary-specific and hormonally
regulated gene expression directed by the rat proopiomelanocortin promoter intransgenic mice. Mol. Endocrinol. 4, 1689–1697 (1990).
40. Bousquet, C., Zatelli, M.C. & Melmed, S. Direct regulation of pituitary proopiome-lanocortin by STAT3 provides a novel mechanism for immuno-neuroendocrine in-terfacing. J. Clin. Invest. 106, 1417–1425 (2000).
41. Heaney, A.P., Horwitz, G.A., Wang, Z., Singson, R. & Melmed, S. Estrogen inducedpituitary Tumor Transforming Gene (PTTG) and bFGF in Pituitary TumorPathogenesis. Nature Med. 5, 1317–1321 (1999).
©20
02 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://w
ww
.nat
ure
.co
m/n
atu
rem
edic
ine