Epidemiologie de la résistance chez les bactéries à Gram...
89
Epidemiologie de la résistance chez les bactéries à Gram-négatif Youri Glupczynski, MD, PhD Clinical Microbiology Dept & Infection Control Unit National Reference Center for Monitoring of Antimicrobial Resistance CHU Dinant-Godinne, UCL-Namur Université Catholique de Louvain, Yvoir, Belgium
Transcript of Epidemiologie de la résistance chez les bactéries à Gram...

Epidemiologie de la résistance chez les bactéries à Gram-négatif
Youri Glupczynski, MD, PhD
Clinical Microbiology Dept & Infection Control Unit National Reference Center for Monitoring of Antimicrobial Resistance
CHU Dinant-Godinne, UCL-Namur
Université Catholique de Louvain, Yvoir, Belgium
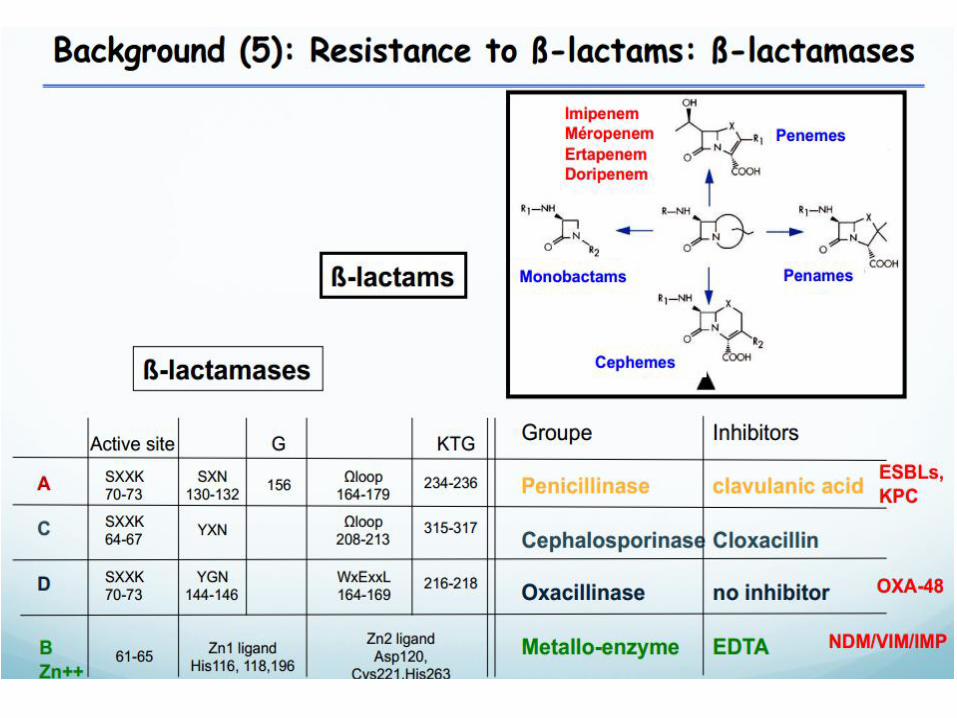
Recent evolution of β-lactamases
S.aureus
penicillinase
BLSE SHV/TEM
Carbapenemases
Penicillins
Amino-Penicillin oral cephalosporins
Inhibitors combinations
3 Generation cephalosporins
carbapenems Tigecycline
4 Generation cephalosporins
1943
1950
1960
1970
1980
1990
2010
TEM-1 SHV-1 OXA-1
Tn3 transposon Plasmid
CTX-M
AmpC
Inhibit Resist TEM
Epidemics Hysteria in hospitals
Plasmid: CMY, MOX, FOX, CAT, MIR
Epidemics, Endemics Hysteria in hospitals
Hysteria in community
Endemic panresistance No therapeutic options
Hysteria in globe
60% E.coli Ampi-R
Enterobacter Klebsiella BLSE
15% of E.coli BLSE AmpC+BLSE
Rivers bacteria, Animals (Farms/pets) Enterobacteriaceae carbapenemases AmpC+BLSE+porin loss
PANRESISTANCE
avibactam Vaccines Phages
Porins+AmpC
Selection
Mobilisation
ESAC
Local Therapeutic failure
Mutation Plasmid: carbapenemases KPC, MBL
Antibiotics into livestock Antibiotics into livestock, poultry, fish 70% of total ATB in USA is fed To healthy farm animals
BL 70 years ESBL: 30 years
Carbapenemases: 15 years
H. Rodriguez & Y Glupczynski submitted
06/06/13 Liège - certificat interuniversitaire 5
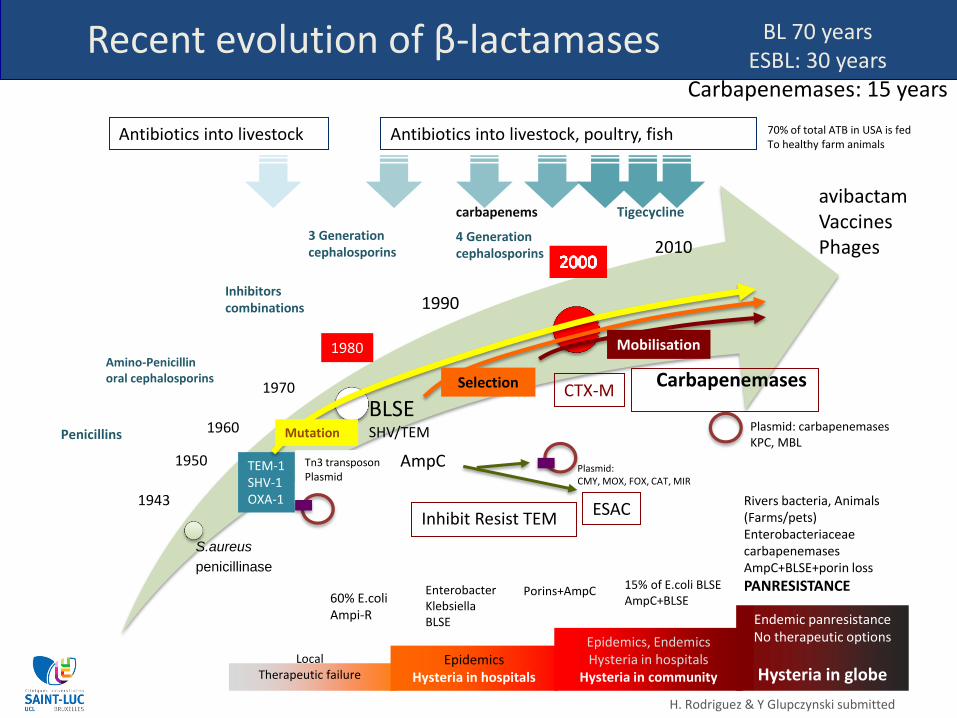
How does Industry address the problem ?
Cooper, Nature (2011) 472: 32; Boucher et al. CID (2013) 56:1685-94
Big Pharma:
• GlaxoSmithKline
• AstraZeneca
• Merck & Co
• (Pfizer)
X
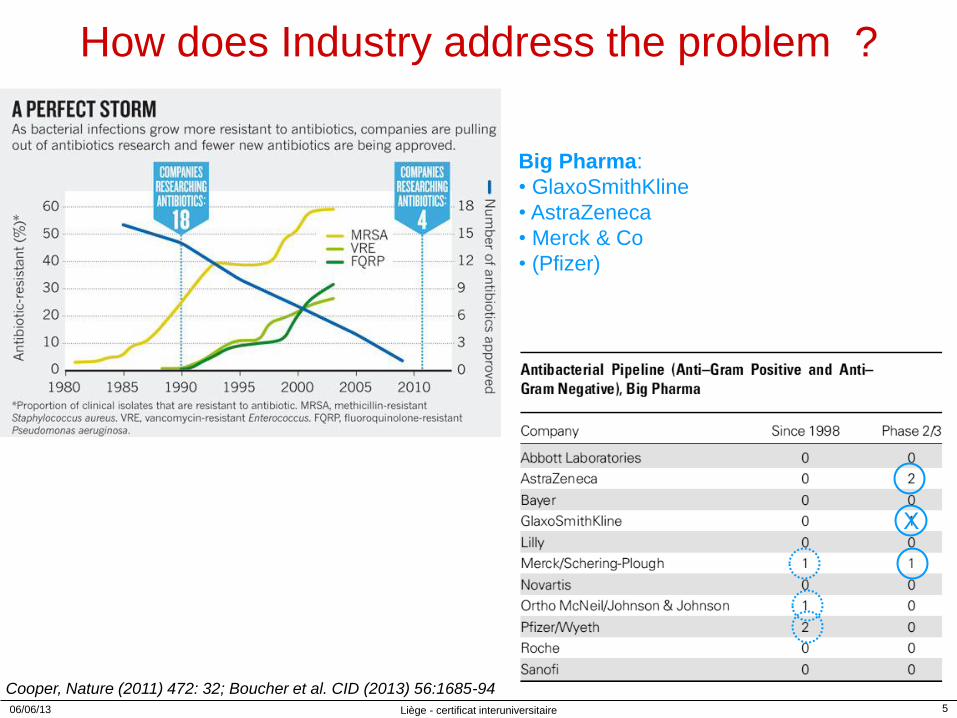
Antimicrobial resistance surveillance in Europe EARS-Net Report 2013 www.ecdc.europa.eu
Escherichia coli: Percentage of invasive isolates with resistance to 3rd gen. cephalosporins in Europe (2013)
weighted mean resistance : 12.6% 5% (Iceland) – 39.6% (Bulgaria) 14 countries: <10% 12 countries: 10-25% 4 countries: >25%
Mean weighed Resistance: 9.5% in 2010 -> 12.6% in 2013 Increasing resistance trend in 17 countries 85-100% of C3G-R E. coli: ESBL-positive
8%
39.6%
38.9%
26.2%
29.7%
13.3%
Antimicrobial resistance surveillance in Europe EARS-Net Report 2013 www.ecdc.europa.eu
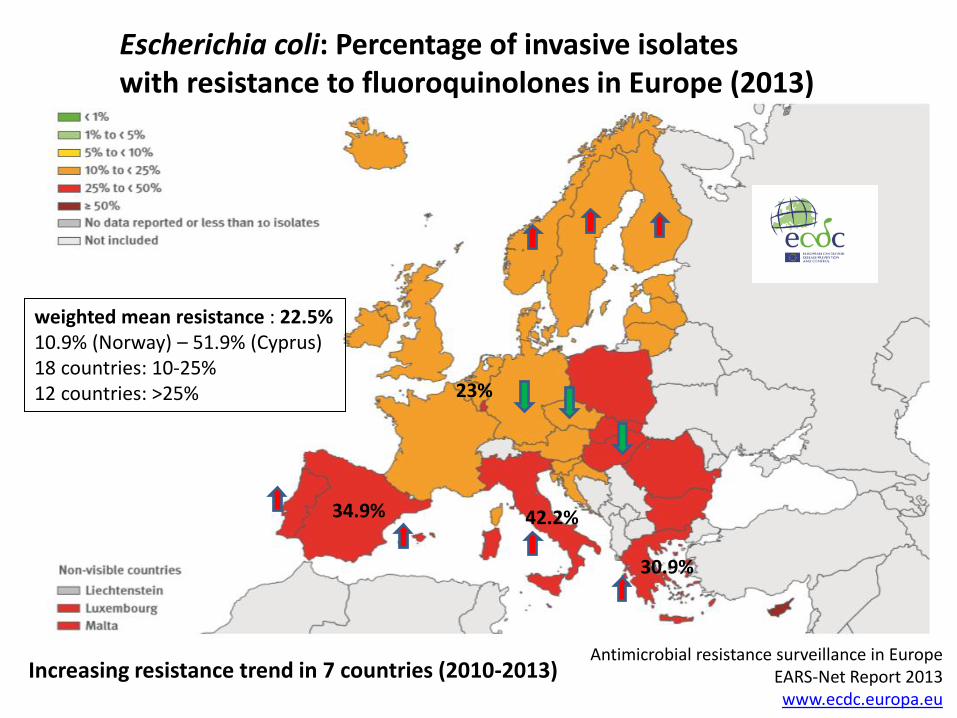
Escherichia coli: Percentage of invasive isolates with resistance to fluoroquinolones in Europe (2013)
weighted mean resistance : 22.5% 10.9% (Norway) – 51.9% (Cyprus) 18 countries: 10-25% 12 countries: >25%
Increasing resistance trend in 7 countries (2010-2013)
23%
42.2%
30.9%
34.9%
Antimicrobial resistance surveillance in Europe EARS-Net Report 2013 www.ecdc.europa.eu
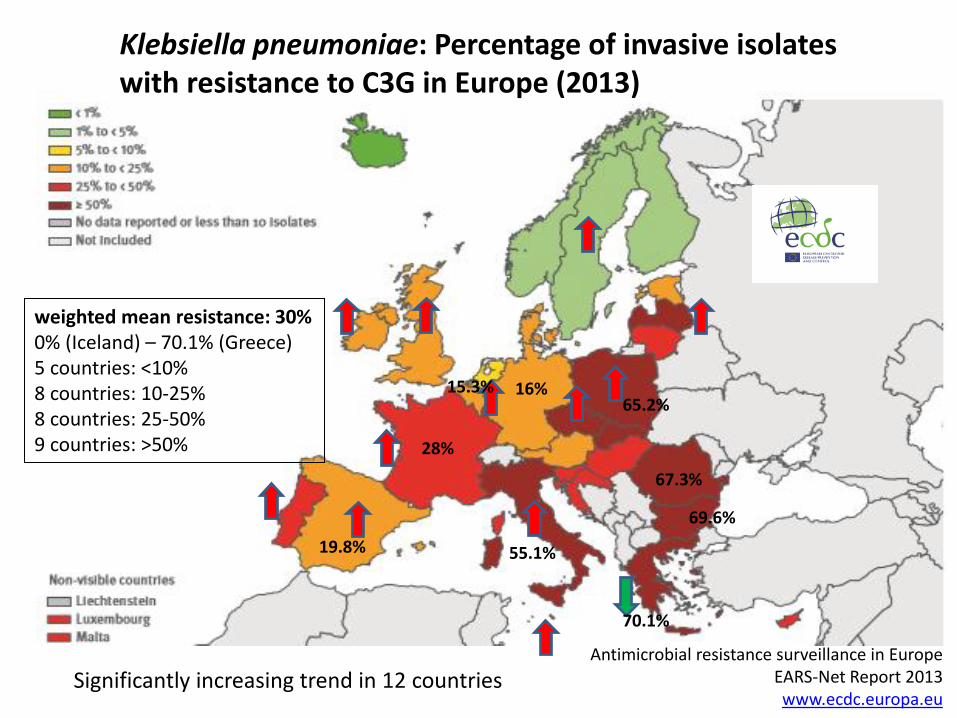
Klebsiella pneumoniae: Percentage of invasive isolates with resistance to C3G in Europe (2013)
weighted mean resistance: 30% 0% (Iceland) – 70.1% (Greece) 5 countries: <10% 8 countries: 10-25% 8 countries: 25-50% 9 countries: >50%
Significantly increasing trend in 12 countries
15.3%
70.1%
69.6%
67.3%
55.1%
28%
65.2% 16%
19.8%
Antimicrobial resistance surveillance in Europe EARS-Net Report 2013 www.ecdc.europa.eu
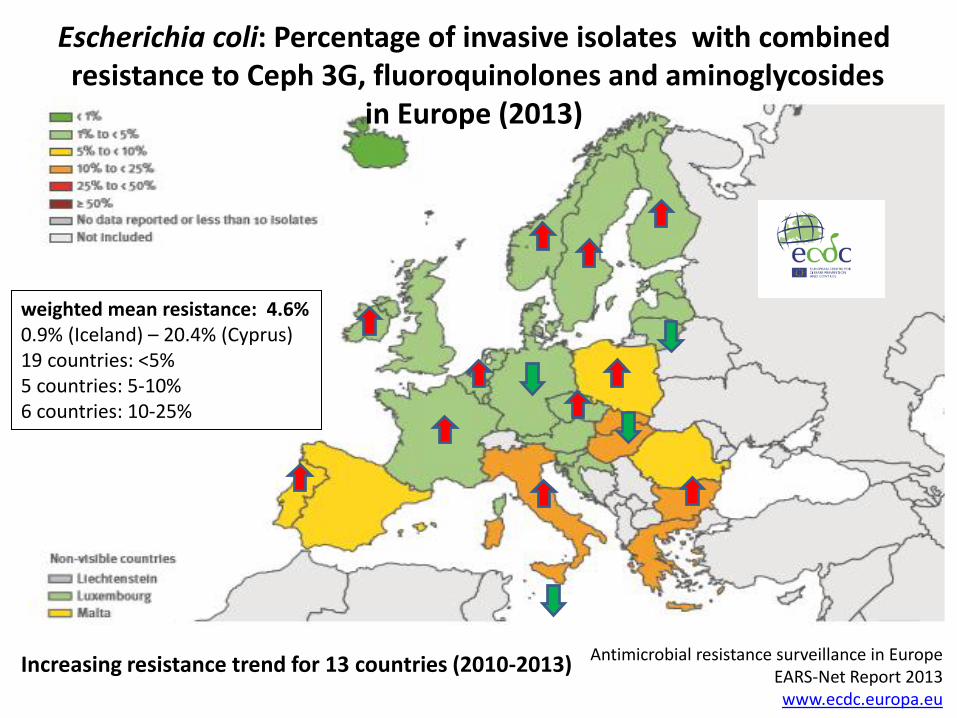
Escherichia coli: Percentage of invasive isolates with combined resistance to Ceph 3G, fluoroquinolones and aminoglycosides
in Europe (2013)
weighted mean resistance: 4.6% 0.9% (Iceland) – 20.4% (Cyprus) 19 countries: <5% 5 countries: 5-10% 6 countries: 10-25%
Increasing resistance trend for 13 countries (2010-2013)
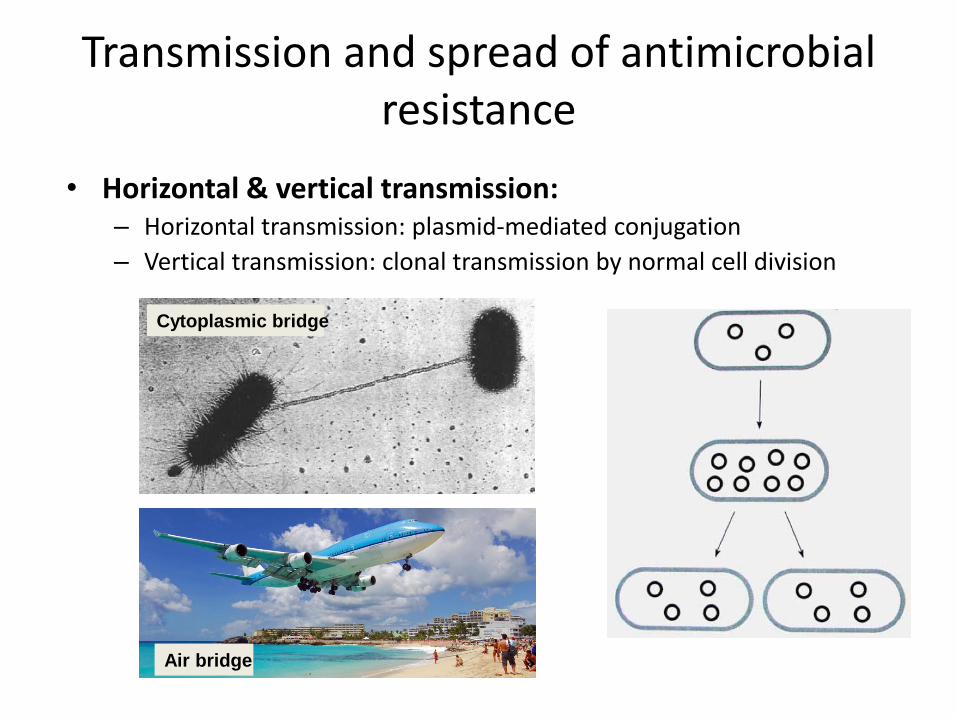
Transmission and spread of antimicrobial resistance
• Horizontal & vertical transmission: – Horizontal transmission: plasmid-mediated conjugation
– Vertical transmission: clonal transmission by normal cell division
Cytoplasmic bridge
Air bridge
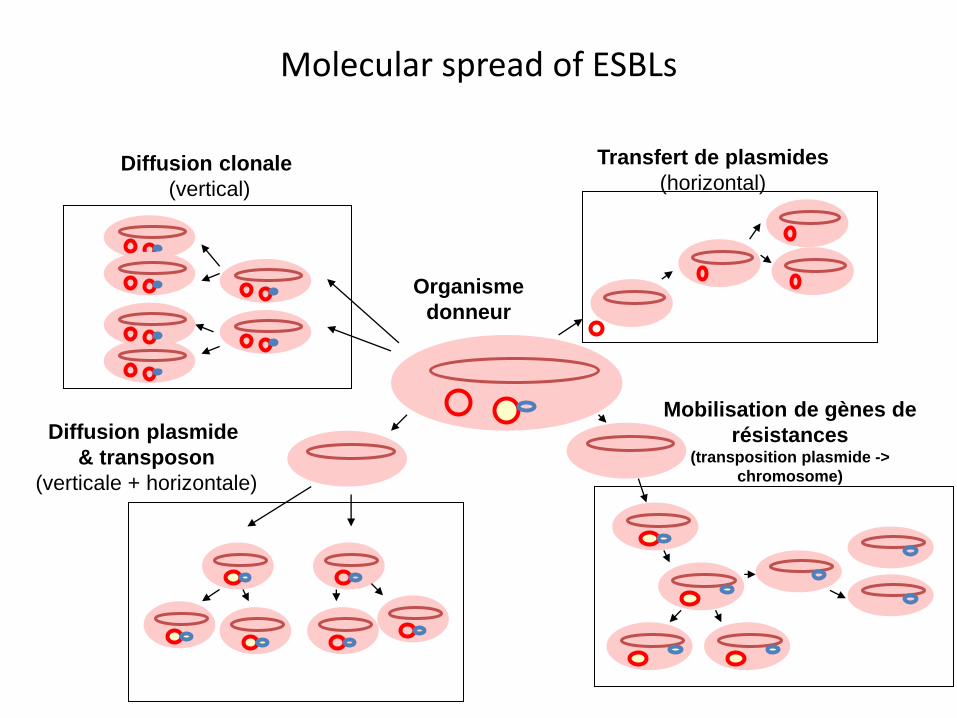
Molecular spread of ESBLs
Organisme
donneur
Diffusion clonale
(vertical)
Transfert de plasmides
(horizontal)
Diffusion plasmide
& transposon
(verticale + horizontale)
Mobilisation de gènes de
résistances (transposition plasmide ->
chromosome)
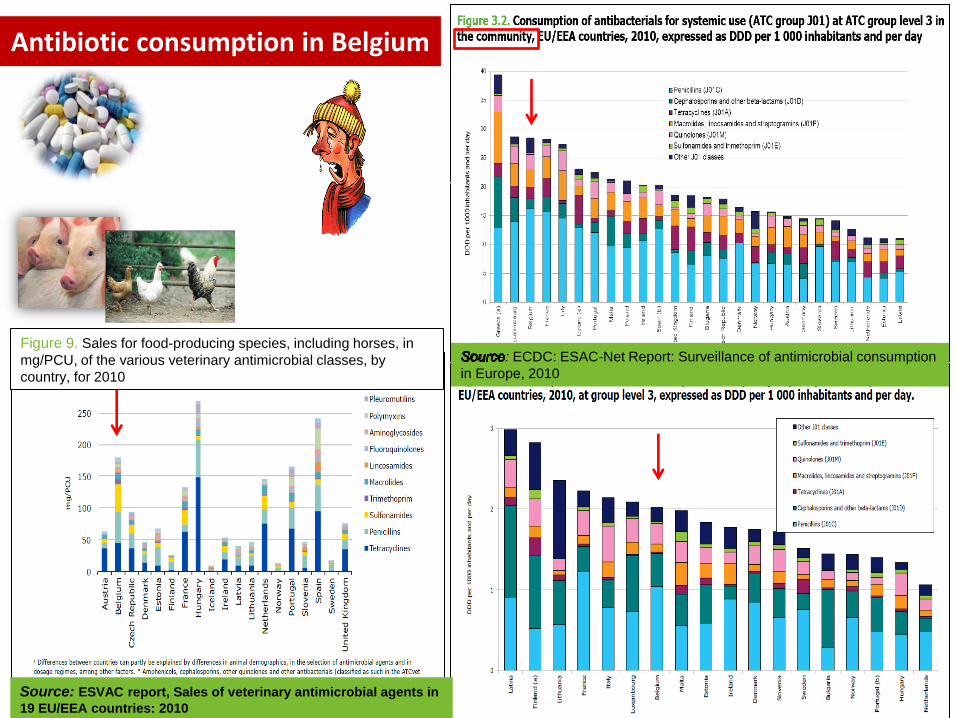
Antibiotic consumption in Belgium
: ECDC: ESAC-Net Report: Surveillance of antimicrobial consumption
in Europe, 2010
Figure 9. Sales for food-producing species, including horses, in
mg/PCU, of the various veterinary antimicrobial classes, by
country, for 2010
Source: ESVAC report, Sales of veterinary antimicrobial agents in
19 EU/EEA countries: 2010
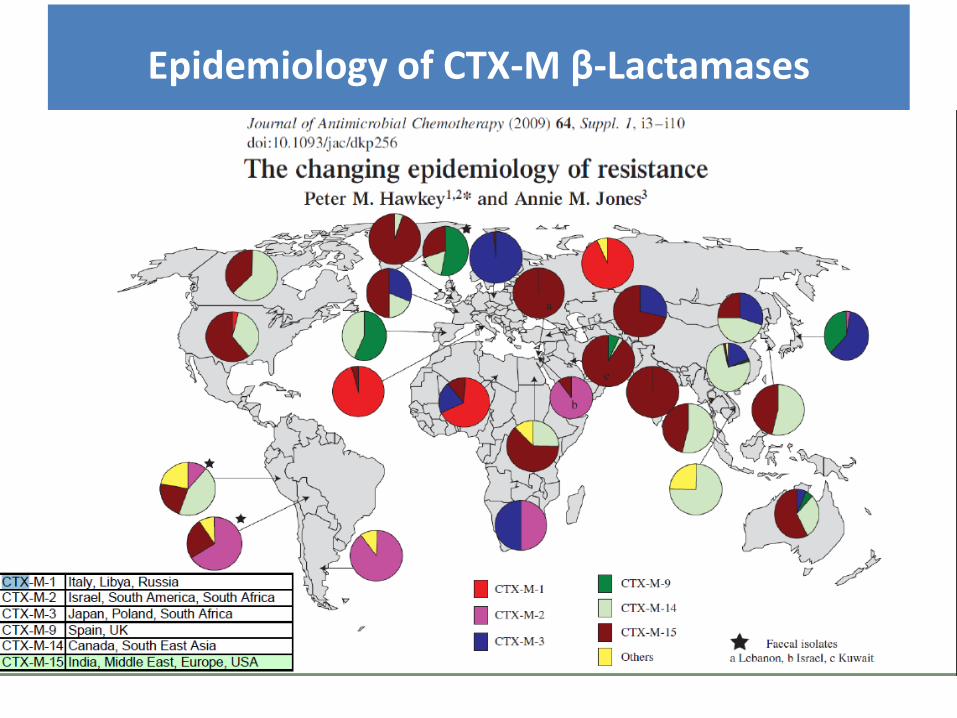
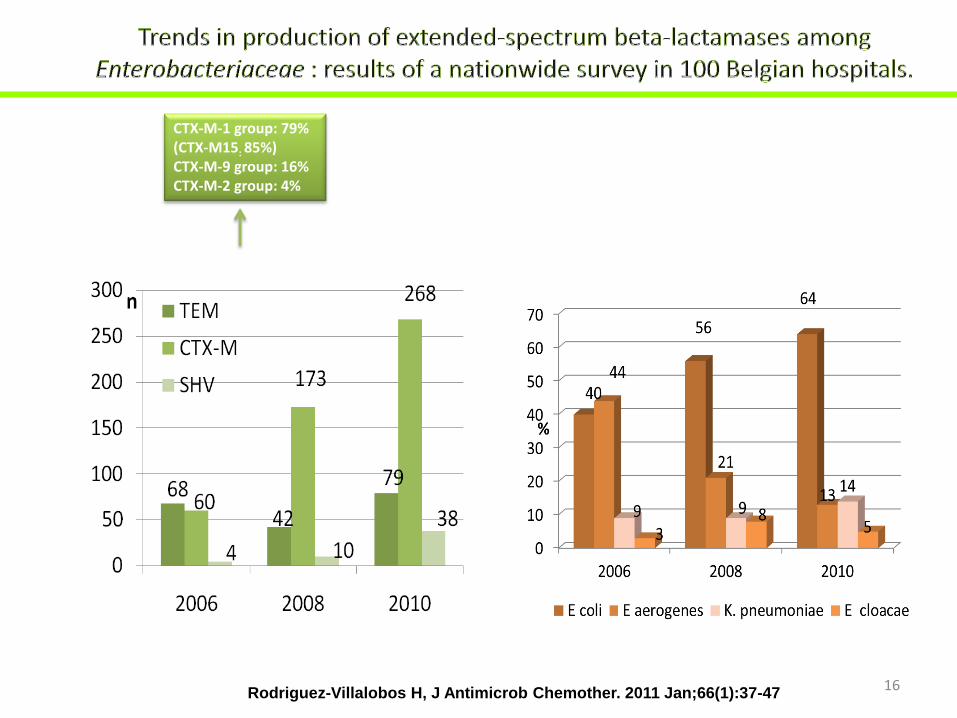
Epidemiology of CTX-M β-Lactamases
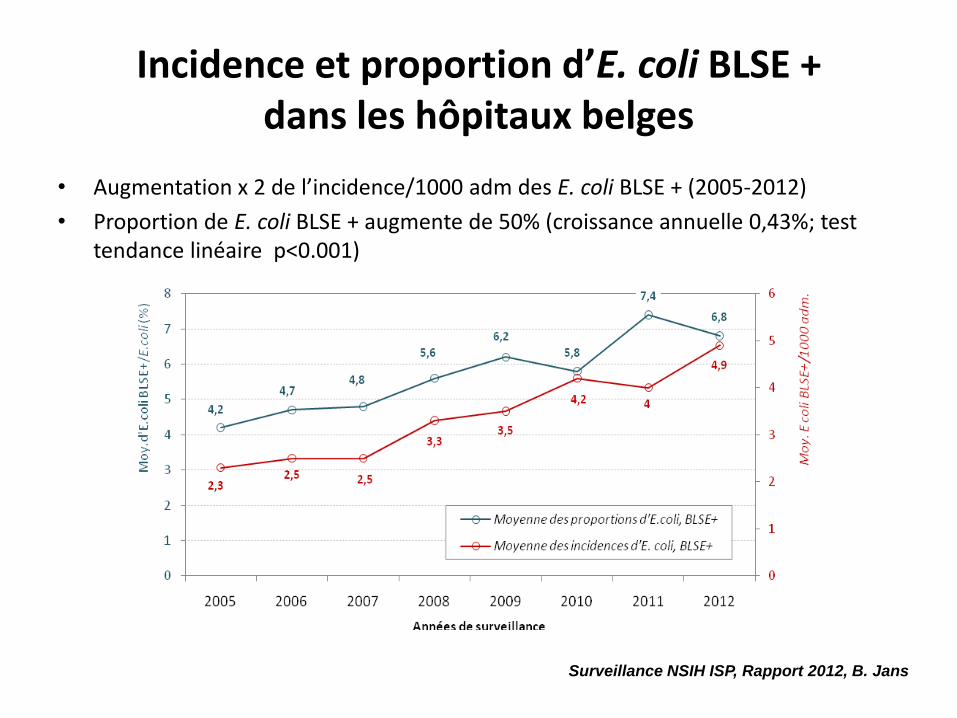
Incidence et proportion d’E. coli BLSE + dans les hôpitaux belges
• Augmentation x 2 de l’incidence/1000 adm des E. coli BLSE + (2005-2012)
• Proportion de E. coli BLSE + augmente de 50% (croissance annuelle 0,43%; test tendance linéaire p<0.001)
Surveillance NSIH ISP, Rapport 2012, B. Jans
16
CTX-M-1 group: 79% (CTX-M15: 85%) CTX-M-9 group: 16% CTX-M-2 group: 4%
Rodriguez-Villalobos H, J Antimicrob Chemother. 2011 Jan;66(1):37-47
17 17
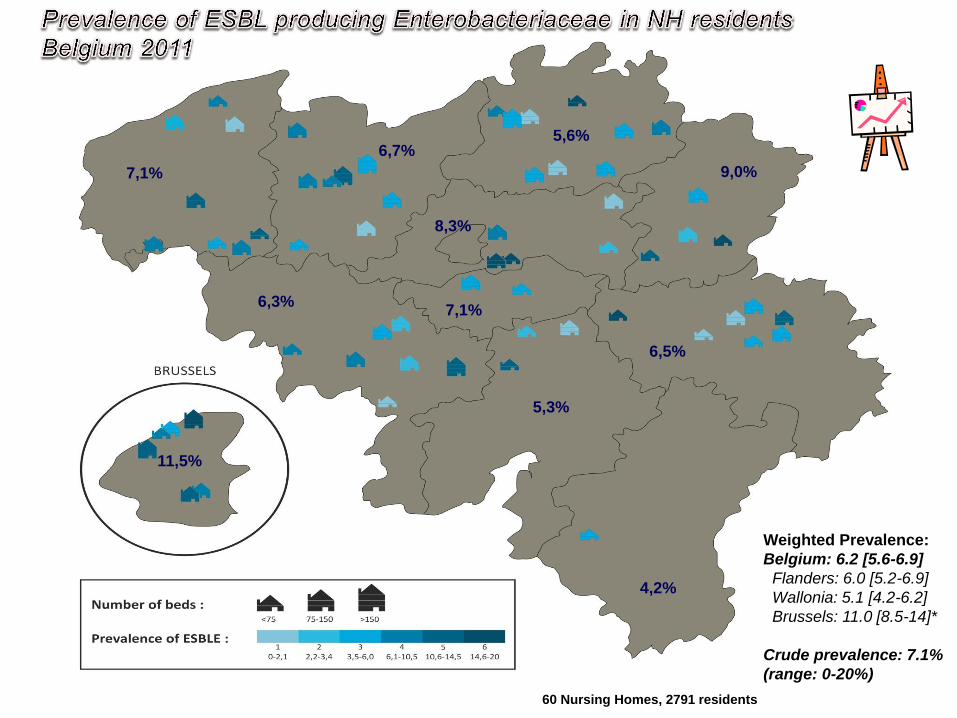
60 Nursing Homes, 2791 residents
7,1%
6,7% 5,6%
6,5%
8,3%
11,5%
6,3% 7,1%
9,0%
5,3%
4,2%
Weighted Prevalence:
Belgium: 6.2 [5.6-6.9]
Flanders: 6.0 [5.2-6.9]
Wallonia: 5.1 [4.2-6.2]
Brussels: 11.0 [8.5-14]*
Crude prevalence: 7.1%
(range: 0-20%)
18
18
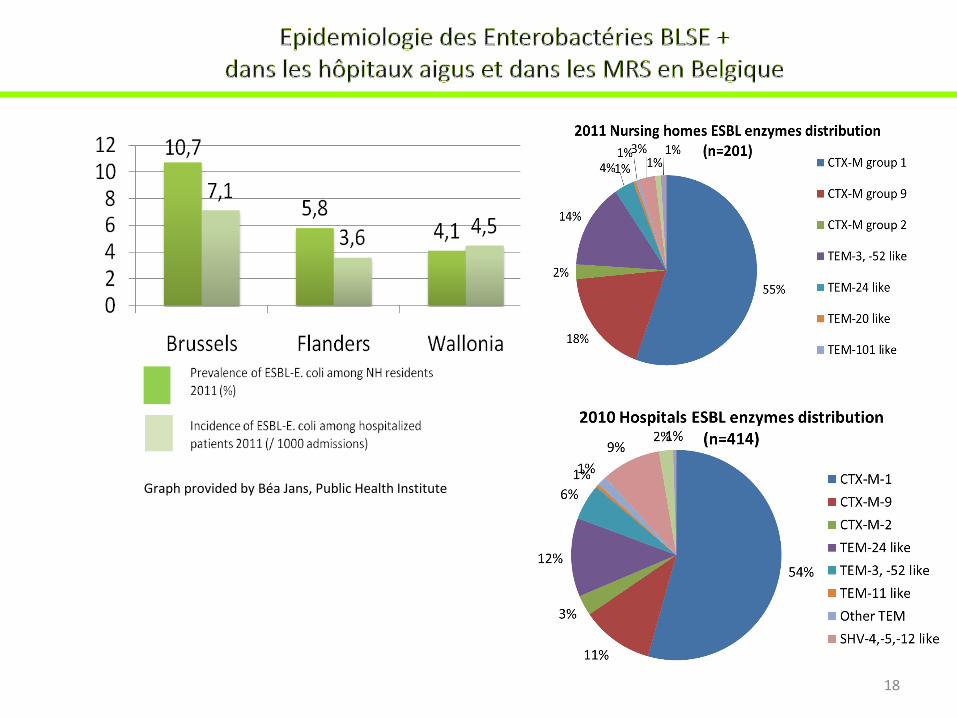
Graph provided by Béa Jans, Public Health Institute
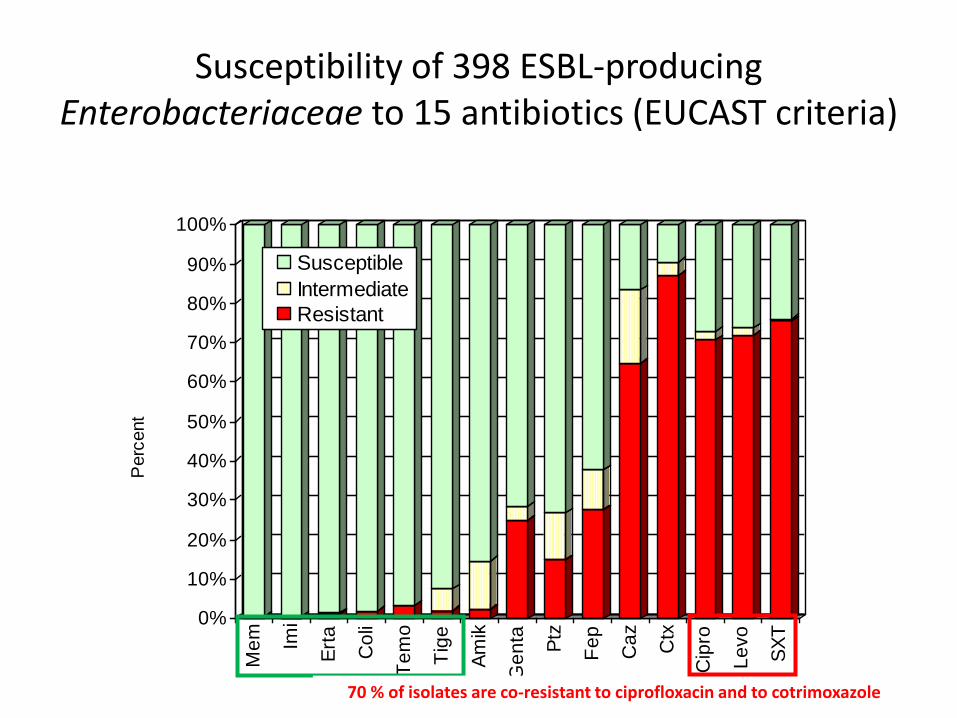
Susceptibility of 398 ESBL-producing Enterobacteriaceae to 15 antibiotics (EUCAST criteria)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Perc
ent
Me
m
Imi
Ert
a
Co
li
Te
mo
Tig
e
Am
ik
Ge
nta
Ptz
Fe
p
Ca
z
Ctx
Cip
ro
Le
vo
SX
T
Susceptible
Intermediate
Resistant
70 % of isolates are co-resistant to ciprofloxacin and to cotrimoxazole
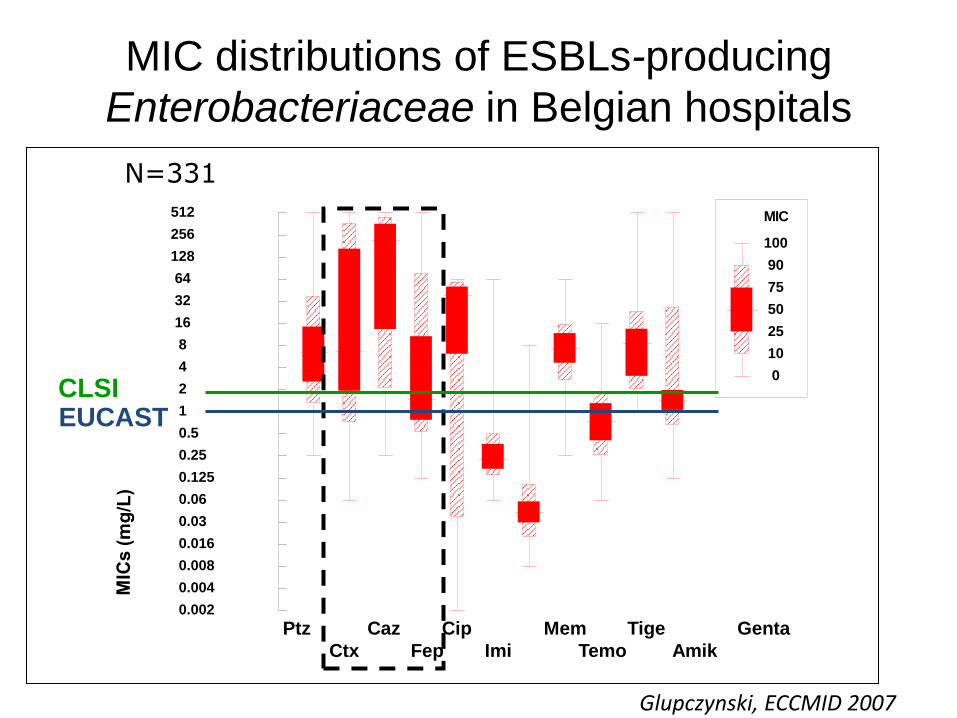
Ptz Caz Cip Mem Tige Genta
Ctx Fep Imi Temo Amik
MIC distributions of ESBLs-producing
Enterobacteriaceae in Belgian hospitals
MIC
100
90
75
50
25
10
0
0.002
0.004
0.008
0.016
0.03
0.06
0.125
0.25
0.5
1
2
4
8
16
32
64
128
256
512
MIC
s
CMI Ptz
CMI Ctx
CMI Caz
CMI Fep
CMI Cip
CMI Imi
CMI Mem
CMI Tem
CMI Tig
CMI Ami
CMI Gen
CLSI EUCAST
N=331
Glupczynski, ECCMID 2007

Clinical Outcome in Patients with ESBL-pos Klebsiella/E.coli Bacteremia
and Treated with Cephalosporin Therapy
8167
27
11
33
7389
19
0
20
40
60
80
100
<=1mg/L 2 mg/L 4 mg/L 8 mg/L
Failure
Success
D.Andes and W.Craig, Clin Microbiol Infect 2005; 11: 10-17
« In general, the exposure from usual regimens of C3 and C4 doesn’t achieve the PD target
For many of the ESBL organism currently classified as Susceptible »
Antimicrobial resistance surveillance in Europe EARS-Net Report 2013 www.ecdc.europa.eu
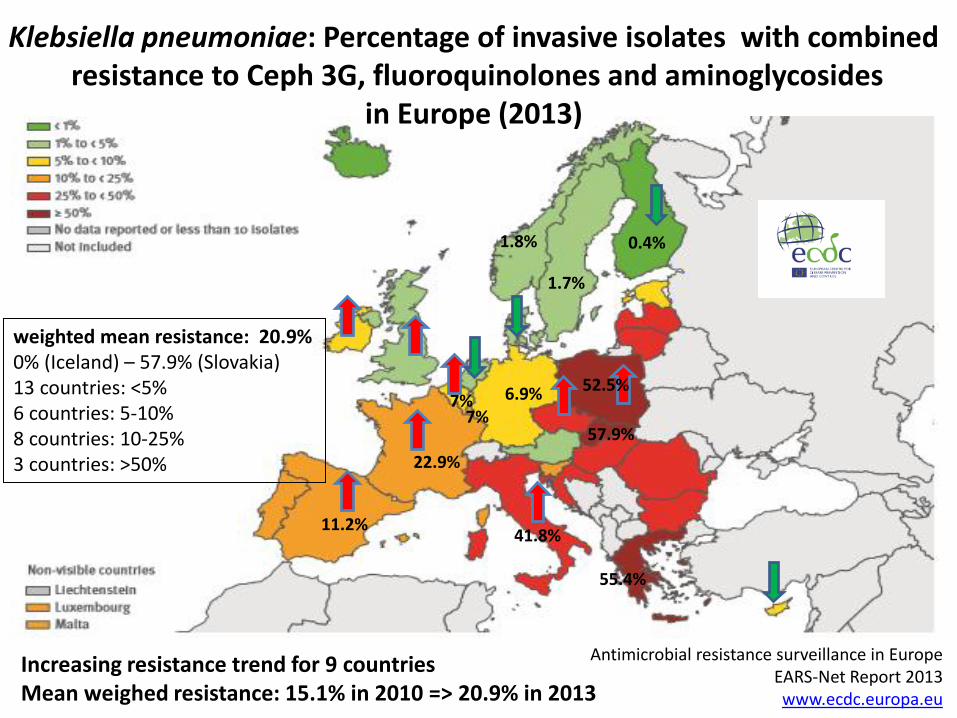
Klebsiella pneumoniae: Percentage of invasive isolates with combined resistance to Ceph 3G, fluoroquinolones and aminoglycosides
in Europe (2013)
weighted mean resistance: 20.9% 0% (Iceland) – 57.9% (Slovakia) 13 countries: <5% 6 countries: 5-10% 8 countries: 10-25% 3 countries: >50%
Increasing resistance trend for 9 countries Mean weighed resistance: 15.1% in 2010 => 20.9% in 2013
7%
57.9%
55.4%
52.5%
41.8%
22.9%
11.2%
6.9%
1.7%
7%
1.8% 0.4%
Antimicrobial resistance surveillance in Europe EARS-Net Report 2013 www.ecdc.europa.eu
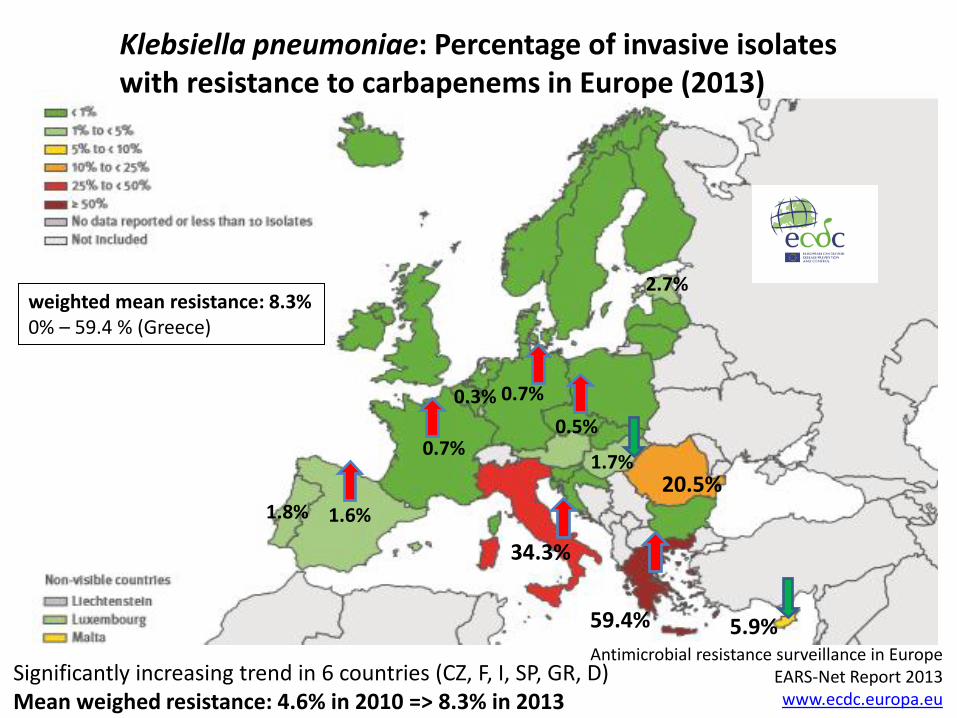
Klebsiella pneumoniae: Percentage of invasive isolates with resistance to carbapenems in Europe (2013)
weighted mean resistance: 8.3% 0% – 59.4 % (Greece)
Significantly increasing trend in 6 countries (CZ, F, I, SP, GR, D) Mean weighed resistance: 4.6% in 2010 => 8.3% in 2013
20.5%
59.4%
34.3%
5.9%
0.5%
0.3%
0.7%
0.7%
1.6%
1.7%
1.8%
2.7%
Antimicrobial resistance surveillance in Europe
EARS-Net Report 2013
www.ecdc.europa.eu
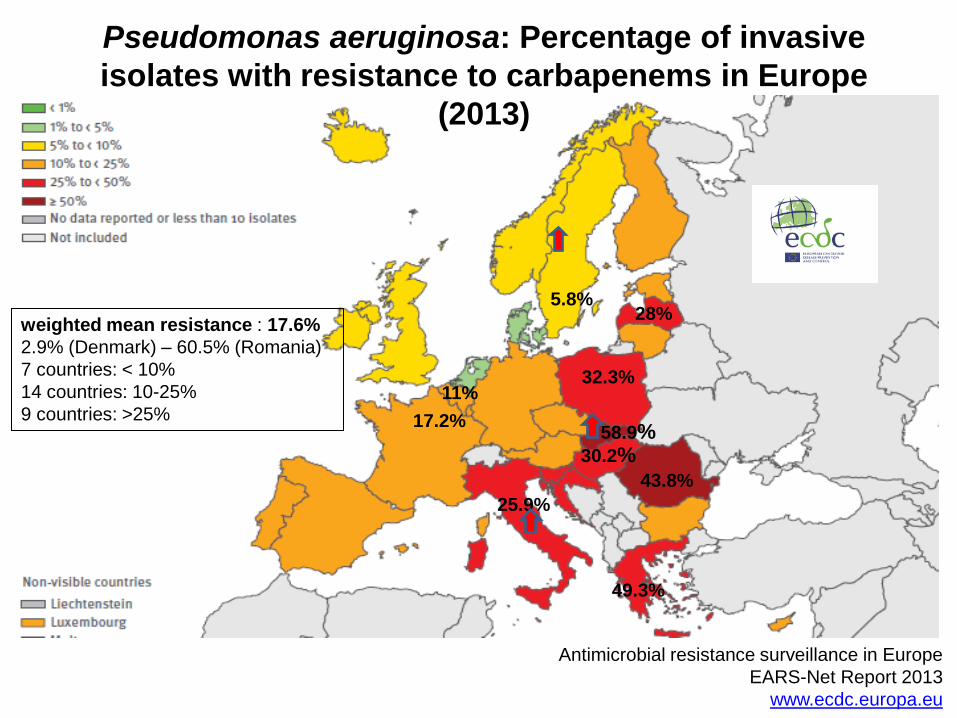
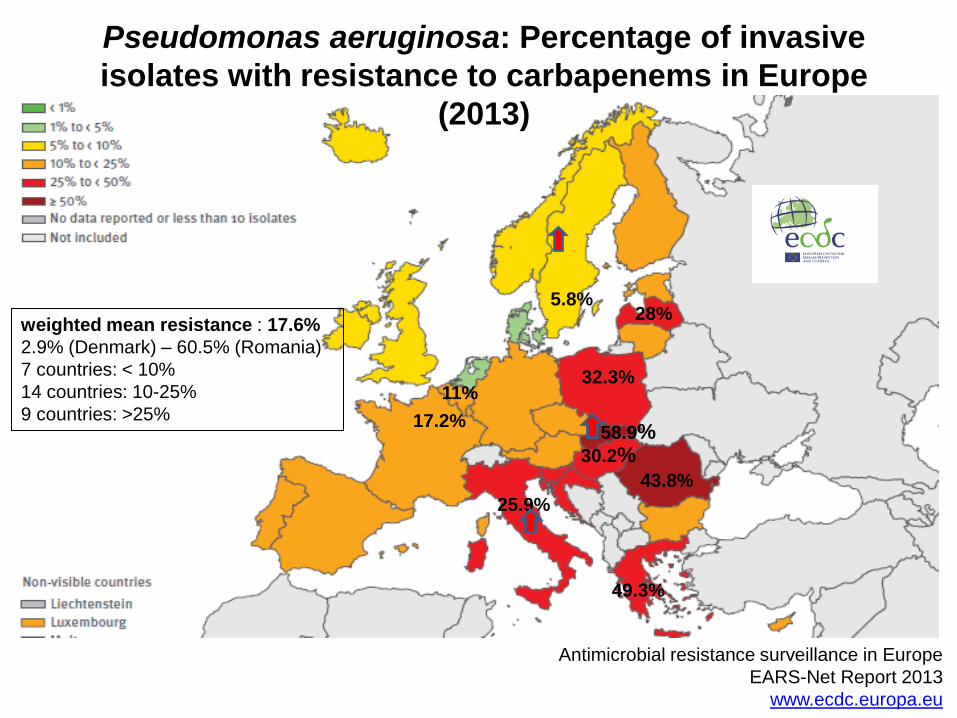
Pseudomonas aeruginosa: Percentage of invasive
isolates with resistance to carbapenems in Europe
(2013)
weighted mean resistance : 17.6%
2.9% (Denmark) – 60.5% (Romania)
7 countries: < 10%
14 countries: 10-25%
9 countries: >25% 11%
43.8%
58.9% 17.2%
25.9%
5.8%
49.3%
32.3%
28%
30.2%
Antimicrobial resistance surveillance in Europe
EARS-Net Report 2013
www.ecdc.europa.eu
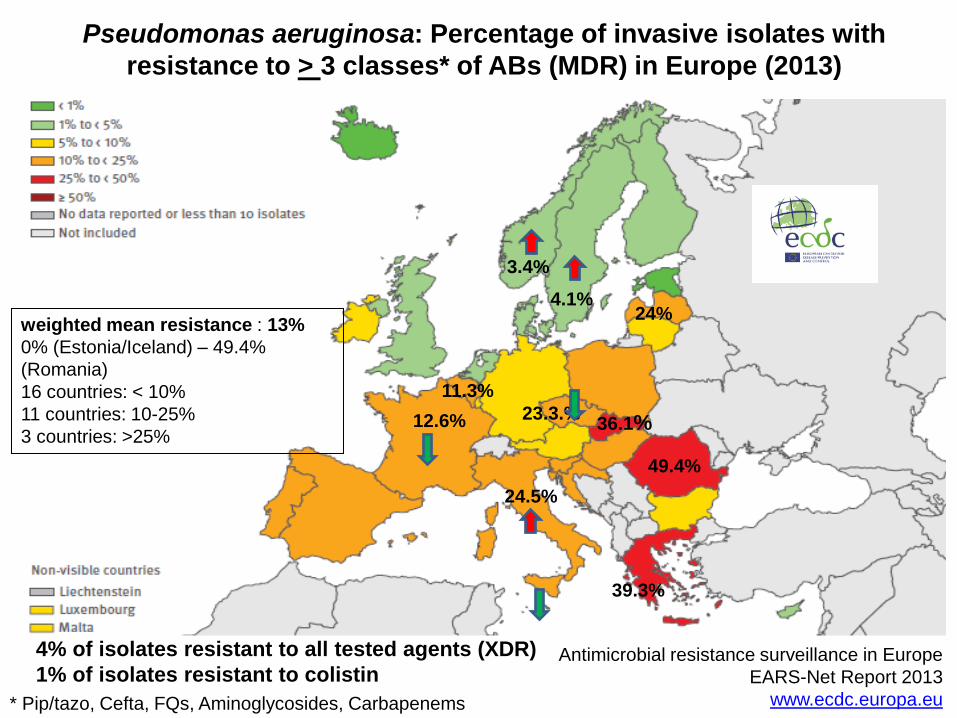
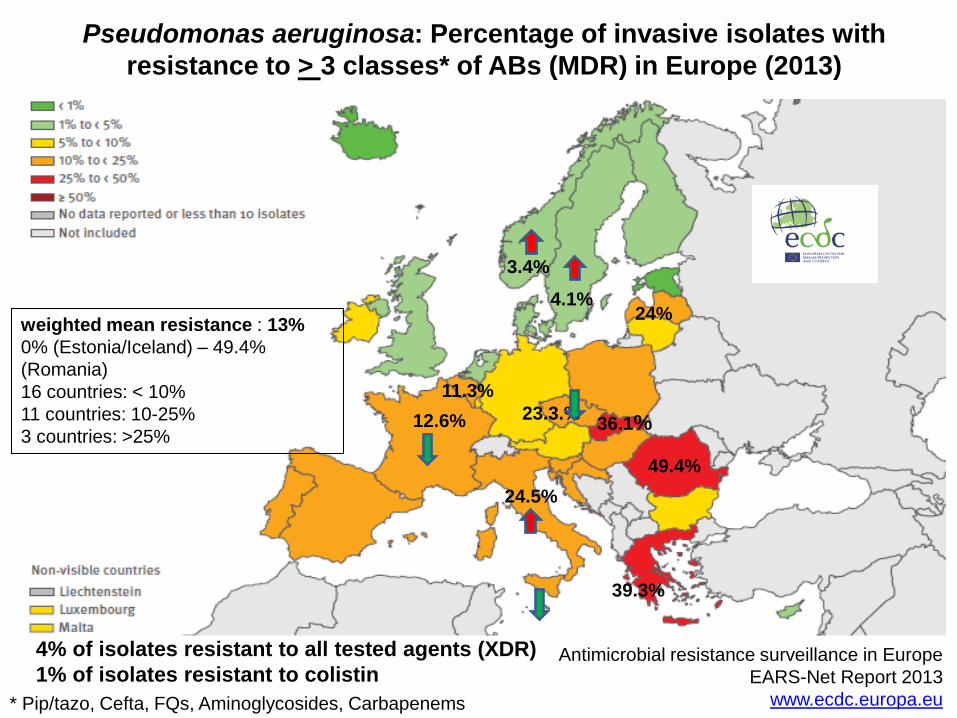
Pseudomonas aeruginosa: Percentage of invasive isolates with
resistance to > 3 classes* of ABs (MDR) in Europe (2013)
weighted mean resistance : 13%
0% (Estonia/Iceland) – 49.4%
(Romania)
16 countries: < 10%
11 countries: 10-25%
3 countries: >25%
11.3%
49.4%
36.1% 12.6%
24.5%
4.1%
39.3%
24%
23.3.%
* Pip/tazo, Cefta, FQs, Aminoglycosides, Carbapenems
3.4%
4% of isolates resistant to all tested agents (XDR)
1% of isolates resistant to colistin
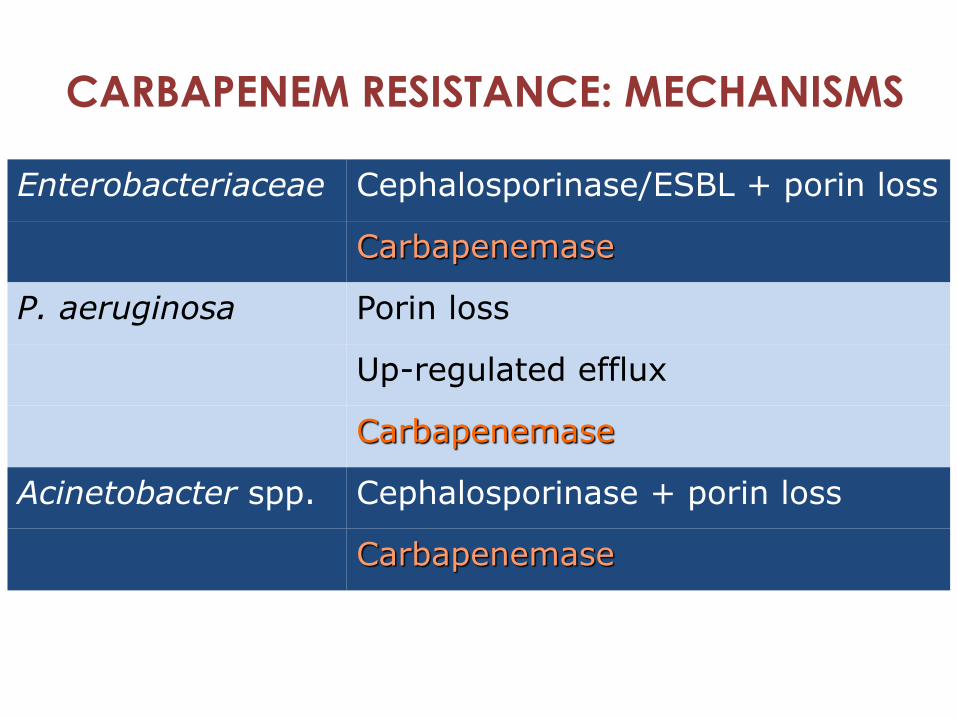
CARBAPENEM RESISTANCE: MECHANISMS
Enterobacteriaceae Cephalosporinase/ESBL + porin loss
Carbapenemase
P. aeruginosa Porin loss
Up-regulated efflux
Carbapenemase
Acinetobacter spp. Cephalosporinase + porin loss
Carbapenemase
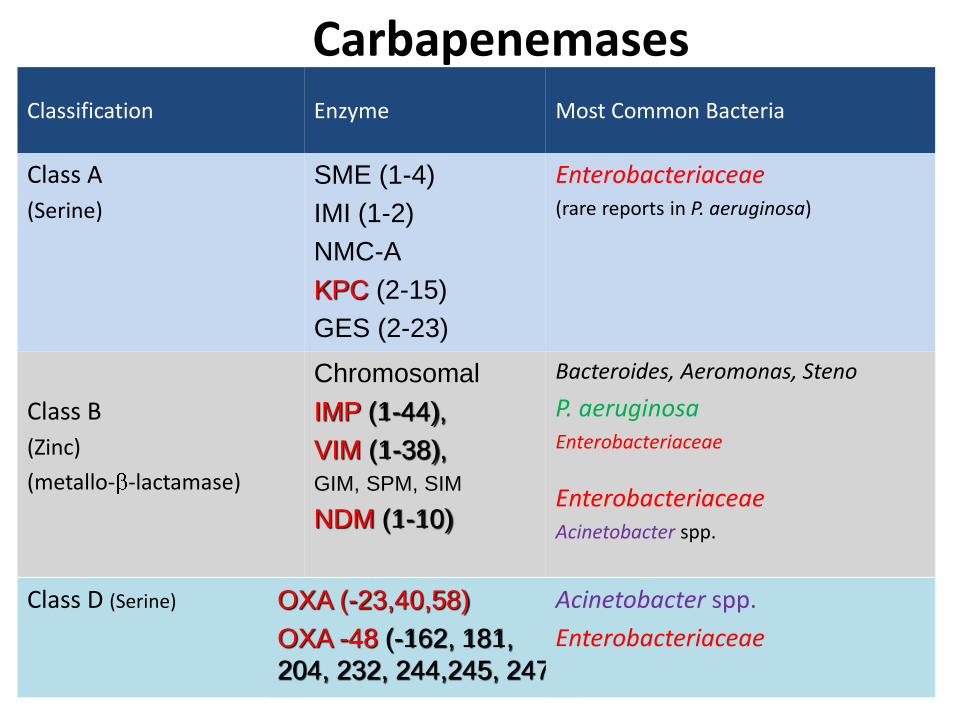
Carbapenemases Classification Enzyme Most Common Bacteria
Class A
(Serine)
SME (1-4)
IMI (1-2)
NMC-A
KPC (2-15)
GES (2-23)
Enterobacteriaceae (rare reports in P. aeruginosa)
Class B
(Zinc)
(metallo- -lactamase)
Chromosomal
IMP (1-44),
VIM (1-38),
GIM, SPM, SIM
NDM (1-10)
Bacteroides, Aeromonas, Steno
P. aeruginosa Enterobacteriaceae
Enterobacteriaceae Acinetobacter spp.
Class D (Serine) OXA (-23,40,58)
OXA -48 (-162, 181,
204, 232, 244,245, 247)
Acinetobacter spp.
Enterobacteriaceae
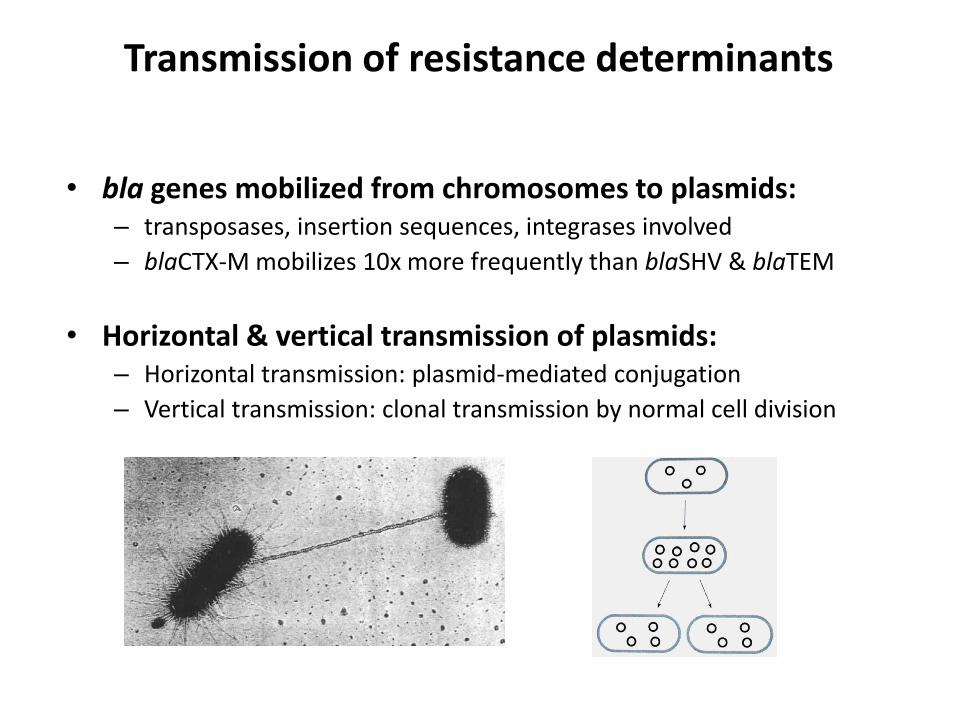
Transmission of resistance determinants
• bla genes mobilized from chromosomes to plasmids: – transposases, insertion sequences, integrases involved
– blaCTX-M mobilizes 10x more frequently than blaSHV & blaTEM
• Horizontal & vertical transmission of plasmids: – Horizontal transmission: plasmid-mediated conjugation
– Vertical transmission: clonal transmission by normal cell division
The molecular epidemiology of carbapenem resistance…in a nutshell
The genes move between plasmids (or chromosomes) ...and
The plasmids move between strains, species and genera ...and
The bacteria move between hosts and settings
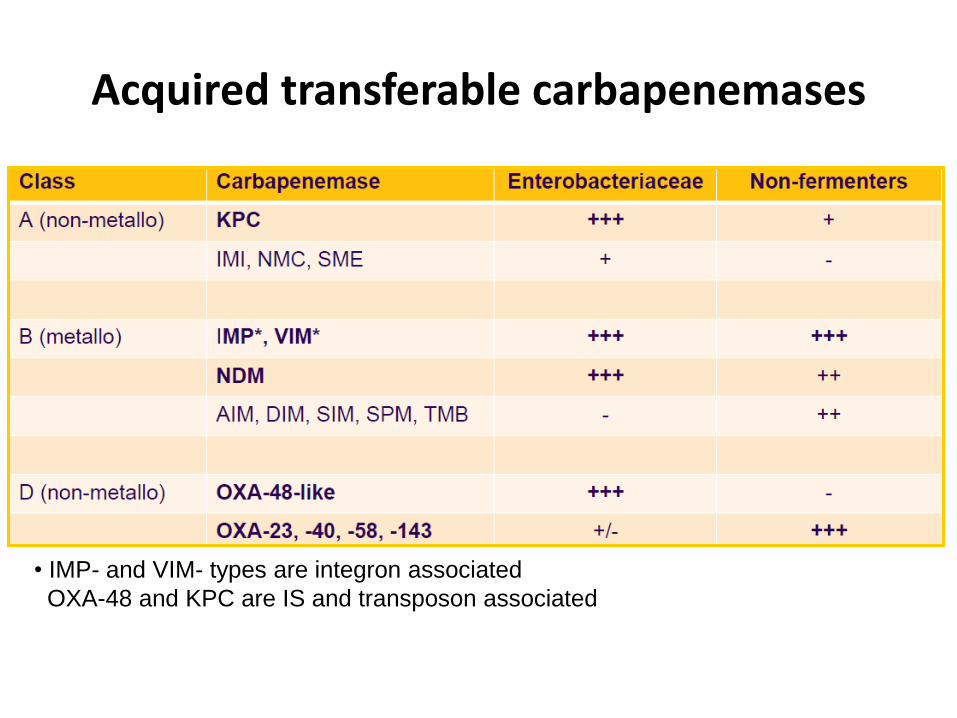
Acquired transferable carbapenemases
• IMP- and VIM- types are integron associated
OXA-48 and KPC are IS and transposon associated
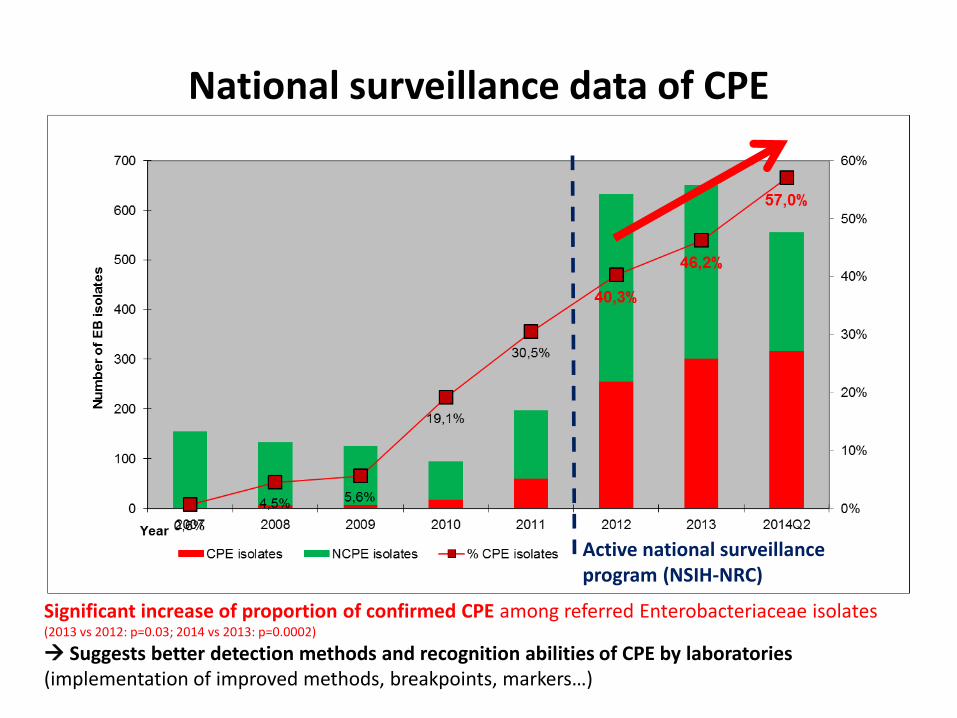
National surveillance data of CPE
Significant increase of proportion of confirmed CPE among referred Enterobacteriaceae isolates (2013 vs 2012: p=0.03; 2014 vs 2013: p=0.0002)
Suggests better detection methods and recognition abilities of CPE by laboratories (implementation of improved methods, breakpoints, markers…)
Active national surveillance program (NSIH-NRC)
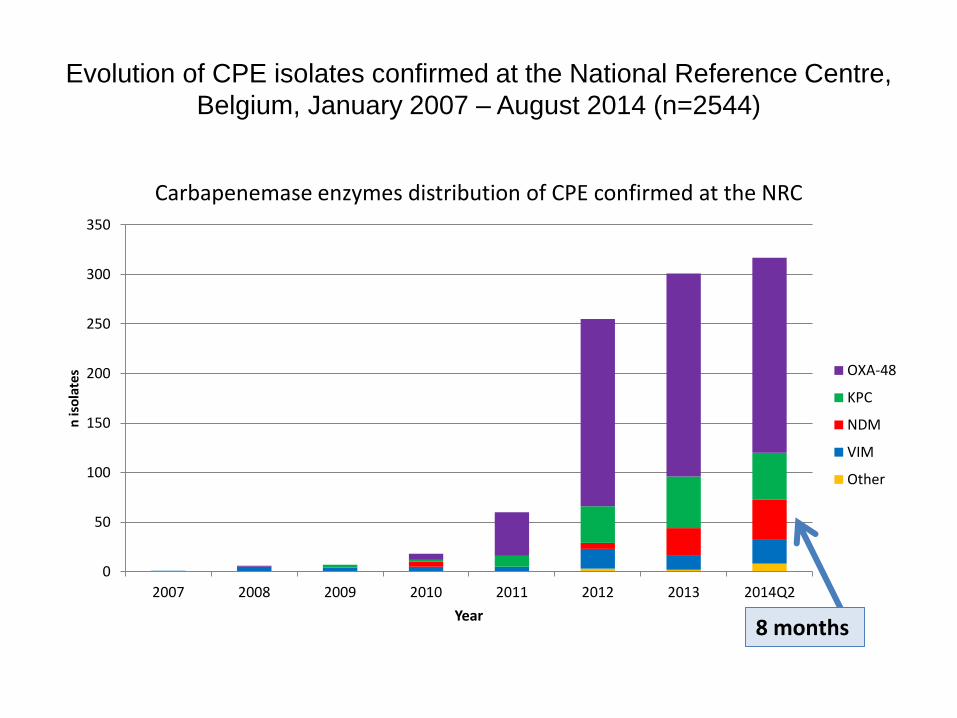
Evolution of CPE isolates confirmed at the National Reference Centre,
Belgium, January 2007 – August 2014 (n=2544)
0
50
100
150
200
250
300
350
2007 2008 2009 2010 2011 2012 2013 2014Q2
n is
ola
tes
Year
Carbapenemase enzymes distribution of CPE confirmed at the NRC
OXA-48
KPC
NDM
VIM
Other
8 months
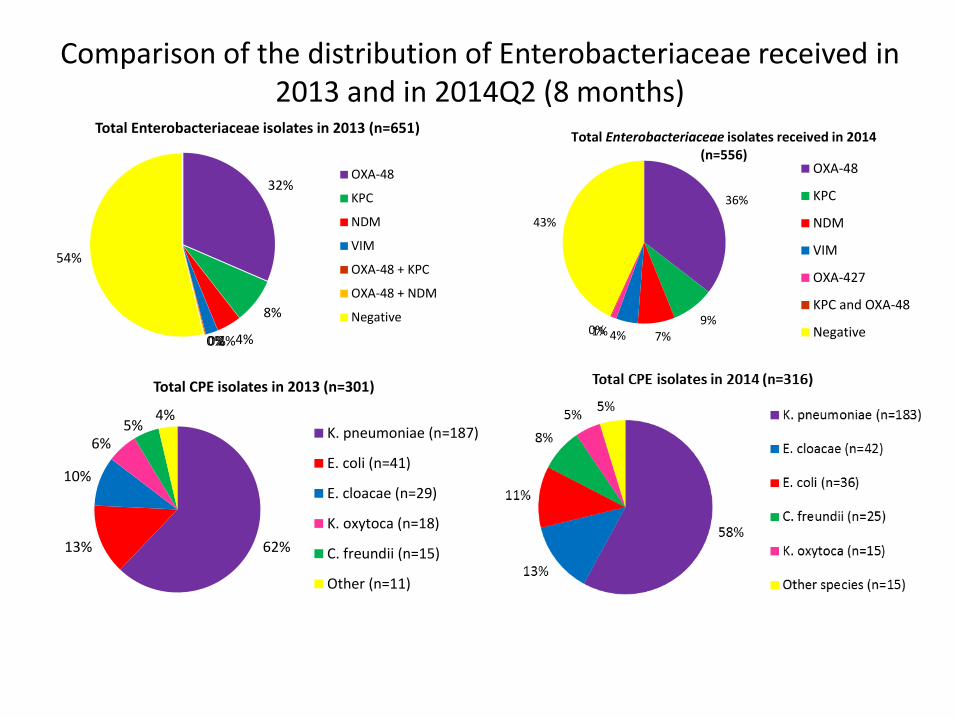
Comparison of the distribution of Enterobacteriaceae received in 2013 and in 2014Q2 (8 months)
32%
8%
4% 2% 0% 0%
54%
Total Enterobacteriaceae isolates in 2013 (n=651)
OXA-48
KPC
NDM
VIM
OXA-48 + KPC
OXA-48 + NDM
Negative
62% 13%
10%
6% 5%
4%
Total CPE isolates in 2013 (n=301)
K. pneumoniae (n=187)
E. coli (n=41)
E. cloacae (n=29)
K. oxytoca (n=18)
C. freundii (n=15)
Other (n=11)
36%
9% 7% 4% 1% 0%
43%
Total Enterobacteriaceae isolates received in 2014 (n=556)
OXA-48
KPC
NDM
VIM
OXA-427
KPC and OXA-48
Negative
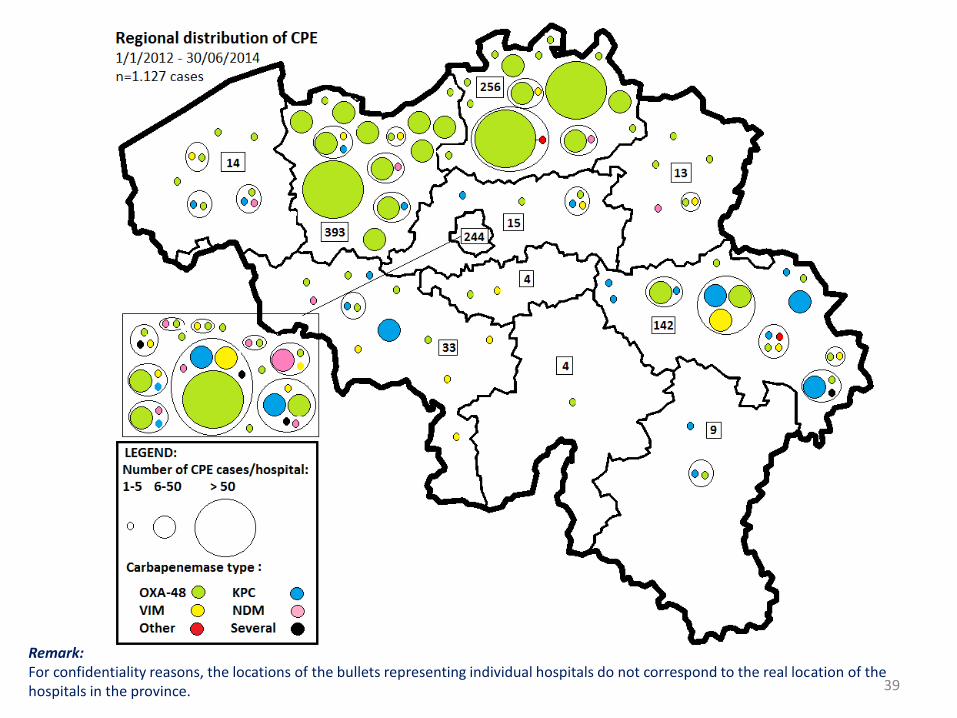
39
Remark: For confidentiality reasons, the locations of the bullets representing individual hospitals do not correspond to the real location of the hospitals in the province.
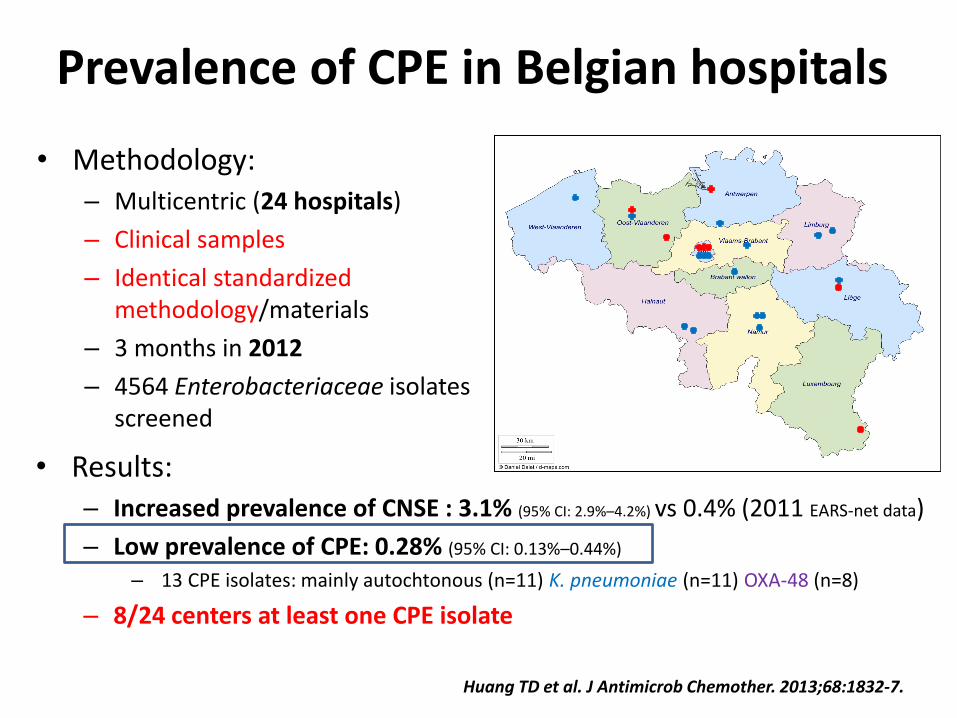
Prevalence of CPE in Belgian hospitals
• Methodology: – Multicentric (24 hospitals)
– Clinical samples
– Identical standardized methodology/materials
– 3 months in 2012
– 4564 Enterobacteriaceae isolates screened
Huang TD et al. J Antimicrob Chemother. 2013;68:1832-7.
• Results: – Increased prevalence of CNSE : 3.1% (95% CI: 2.9%–4.2%) vs 0.4% (2011 EARS-net data)
– Low prevalence of CPE: 0.28% (95% CI: 0.13%–0.44%)
– 13 CPE isolates: mainly autochtonous (n=11) K. pneumoniae (n=11) OXA-48 (n=8)
– 8/24 centers at least one CPE isolate
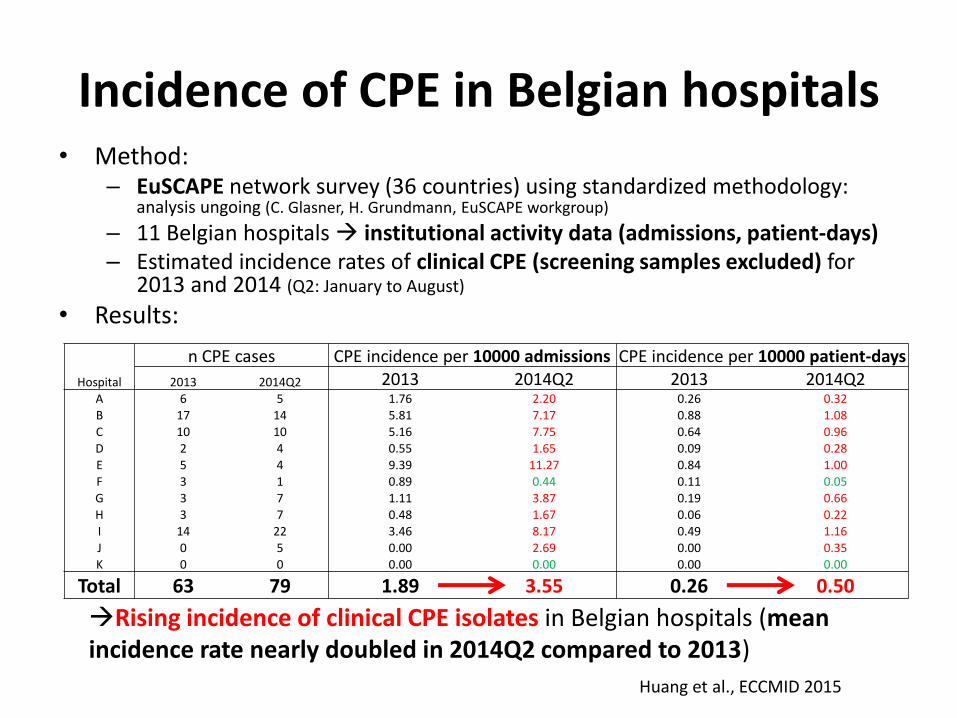
Incidence of CPE in Belgian hospitals • Method:
– EuSCAPE network survey (36 countries) using standardized methodology: analysis ungoing (C. Glasner, H. Grundmann, EuSCAPE workgroup)
– 11 Belgian hospitals institutional activity data (admissions, patient-days) – Estimated incidence rates of clinical CPE (screening samples excluded) for
2013 and 2014 (Q2: January to August)
• Results:
n CPE cases CPE incidence per 10000 admissions CPE incidence per 10000 patient-days
Hospital 2013 2014Q2 2013 2014Q2 2013 2014Q2 A 6 5 1.76 2.20 0.26 0.32
B 17 14 5.81 7.17 0.88 1.08
C 10 10 5.16 7.75 0.64 0.96
D 2 4 0.55 1.65 0.09 0.28
E 5 4 9.39 11.27 0.84 1.00
F 3 1 0.89 0.44 0.11 0.05
G 3 7 1.11 3.87 0.19 0.66
H 3 7 0.48 1.67 0.06 0.22
I 14 22 3.46 8.17 0.49 1.16
J 0 5 0.00 2.69 0.00 0.35
K 0 0 0.00 0.00 0.00 0.00
Total 63 79 1.89 3.55 0.26 0.50
Rising incidence of clinical CPE isolates in Belgian hospitals (mean incidence rate nearly doubled in 2014Q2 compared to 2013)
Huang et al., ECCMID 2015
Carbapenemases:
the triple difficulty (DDD)
• Difficulty of detection in the clinic and in the laboratory
• Difficulty of treatment (owing to their multi-drug resistant character, with few drugs remaining active)
• Difficulty to limit transmission and spread and to control
outbreak (local, regional, national, pandemic)
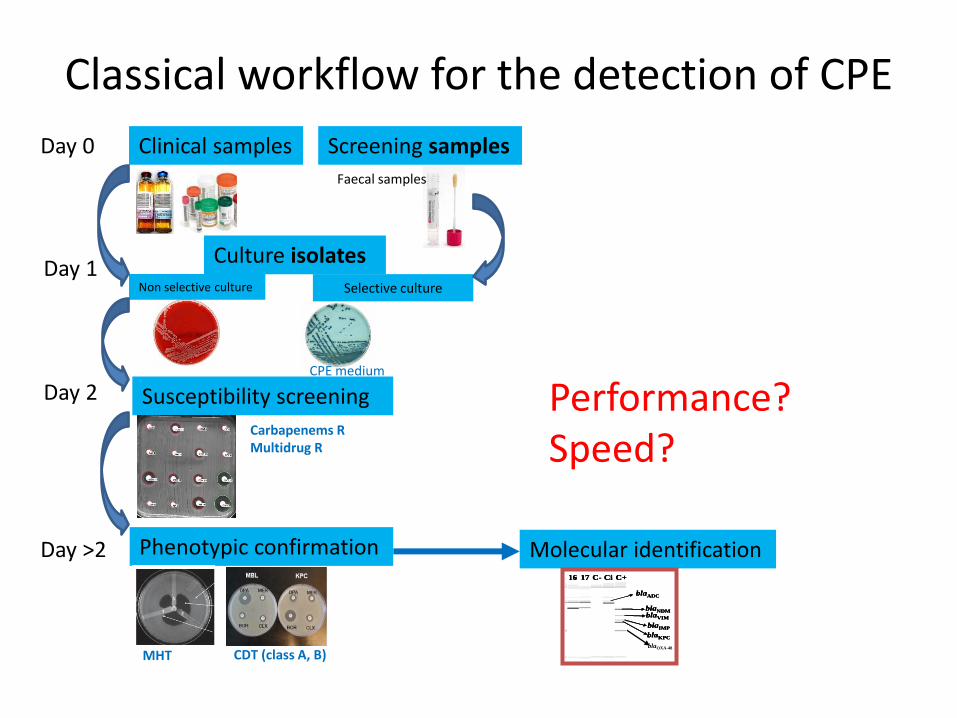
Classical workflow for the detection of CPE
Clinical samples Screening samples
Culture isolates
Susceptibility screening
Phenotypic confirmation Molecular identification
Day 0
Day 1
Day >2
Day 2
1 3 42 5 6 7 8 9 10 11 12 13 1514 C+C- CiM 1716
blaADC
blaVIM
blaIMP
blaKPC
blaNDM
1 3 42 5 6 7 8 9 10 11 12 13 1514 C+C- CiM 17161 3 42 5 6 7 8 9 10 11 12 13 1514 C+C- CiM 1716
blaADCblaADC
blaVIMblaVIM
blaIMPblaIMP
blaKPCblaKPC
blaNDMblaNDM
blaOXA-48
Non selective culture Selective culture
MHT CDT (class A, B)
Carbapenems R Multidrug R
CPE medium
Faecal samples
Performance? Speed?
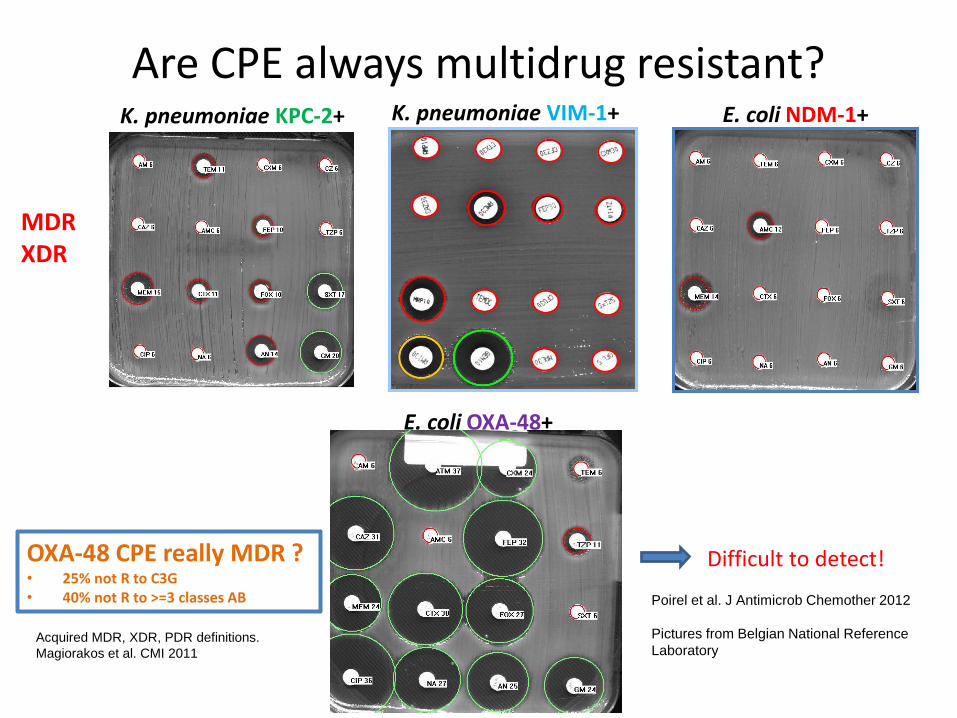
Are CPE always multidrug resistant? K. pneumoniae KPC-2+ K. pneumoniae VIM-1+ E. coli NDM-1+
Poirel et al. J Antimicrob Chemother 2012
Pictures from Belgian National Reference
Laboratory
E. coli OXA-48+
MDR XDR
OXA-48 CPE really MDR ? • 25% not R to C3G • 40% not R to >=3 classes AB
Difficult to detect!
Acquired MDR, XDR, PDR definitions.
Magiorakos et al. CMI 2011
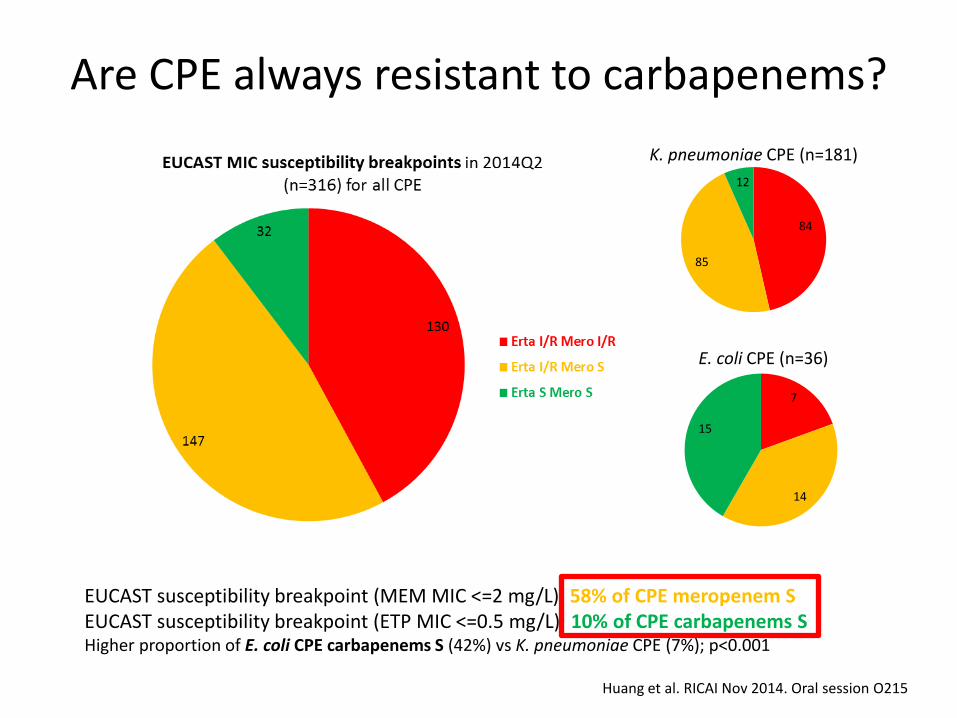
Are CPE always resistant to carbapenems?
EUCAST susceptibility breakpoint (MEM MIC <=2 mg/L): 58% of CPE meropenem S EUCAST susceptibility breakpoint (ETP MIC <=0.5 mg/L): 10% of CPE carbapenems S Higher proportion of E. coli CPE carbapenems S (42%) vs K. pneumoniae CPE (7%); p<0.001
Huang et al. RICAI Nov 2014. Oral session O215
84
85
12
K. pneumoniae CPE (n=181)
7
14
15
E. coli CPE (n=36)
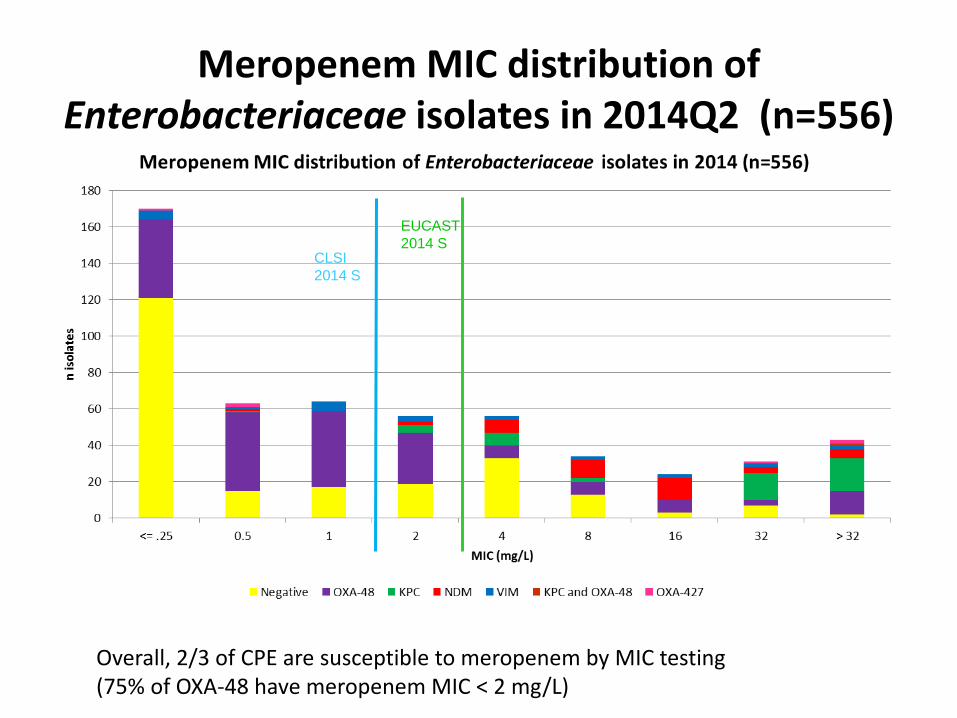
Meropenem MIC distribution of Enterobacteriaceae isolates in 2014Q2 (n=556)
CLSI
2014 S
EUCAST
2014 S
Overall, 2/3 of CPE are susceptible to meropenem by MIC testing (75% of OXA-48 have meropenem MIC < 2 mg/L)
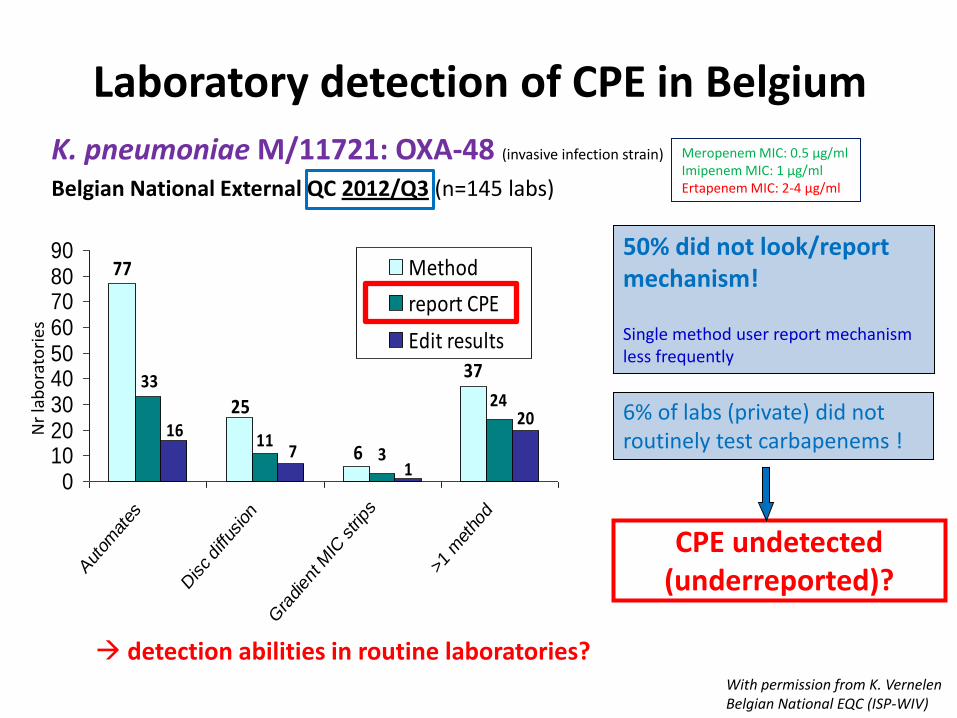
K. pneumoniae M/11721: OXA-48 (invasive infection strain)
Belgian National External QC 2012/Q3 (n=145 labs)
Laboratory detection of CPE in Belgium
24
37
6
25
77
311
33
20
17
16
0102030405060708090
Autom
ates
Disc diffu
sion
Gra
dien
t MIC
strips
>1 m
etho
d
Method
report CPE
Edit results
Nr
lab
ora
tori
es
With permission from K. Vernelen Belgian National EQC (ISP-WIV)
50% did not look/report mechanism! Single method user report mechanism less frequently
6% of labs (private) did not routinely test carbapenems !
CPE undetected (underreported)?
detection abilities in routine laboratories?
Meropenem MIC: 0.5 µg/ml Imipenem MIC: 1 µg/ml Ertapenem MIC: 2-4 µg/ml
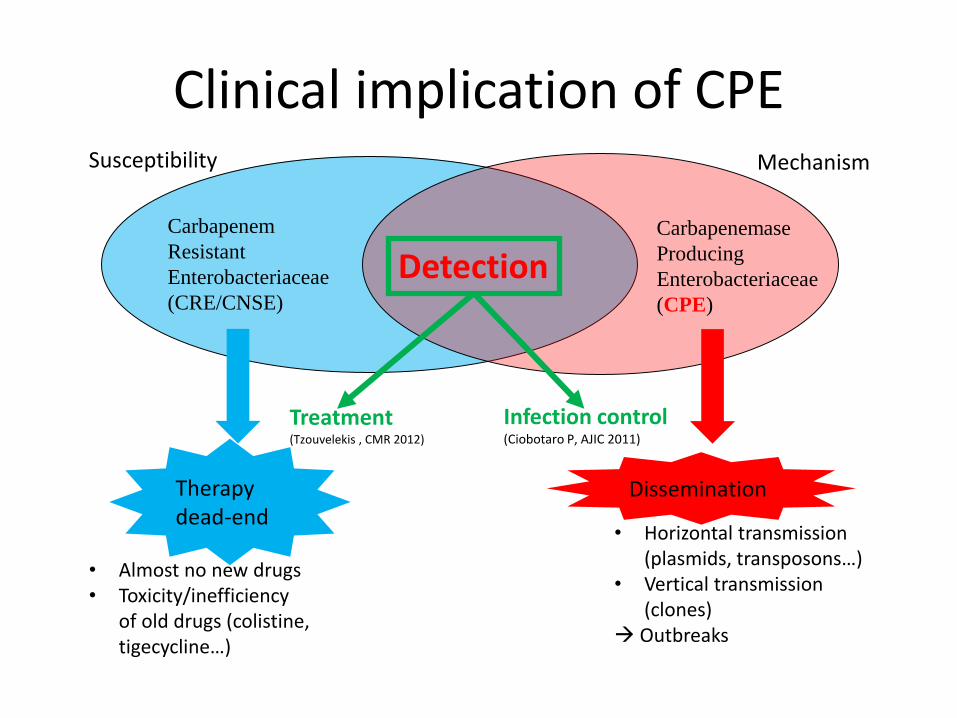
Clinical implication of CPE
Carbapenem
Resistant
Enterobacteriaceae
(CRE/CNSE)
Carbapenemase
Producing
Enterobacteriaceae
(CPE)
Therapy dead-end
Dissemination
Susceptibility Mechanism
Infection control (Ciobotaro P, AJIC 2011)
Treatment (Tzouvelekis , CMR 2012)
Detection
• Almost no new drugs • Toxicity/inefficiency
of old drugs (colistine, tigecycline…)
• Horizontal transmission (plasmids, transposons…)
• Vertical transmission (clones)
Outbreaks
Carbapenemase producing Enterobacteriacae
– High infection/colonization ratio:
• 9% in all hospital → 40% in ICU 1,2
– Infections are associated with 3-5
• Crude mortality: 30 to 44% (up to 70% for bacteremia)
• Risk x 3-4 mortality versus susceptible Enterobacteriacae
• Delay in adequate antibiotherapy5 (increase of the LOS)
3Borer et al ICHE 2009; 30: 972 4Schwaber et al Antimicrob Agents Chemother 2007;52:1028-33 5Patel et al ICHE 2008; 29: 1099 .
1Schechner et al CMI 2012 2Borer et al AJIC 2011
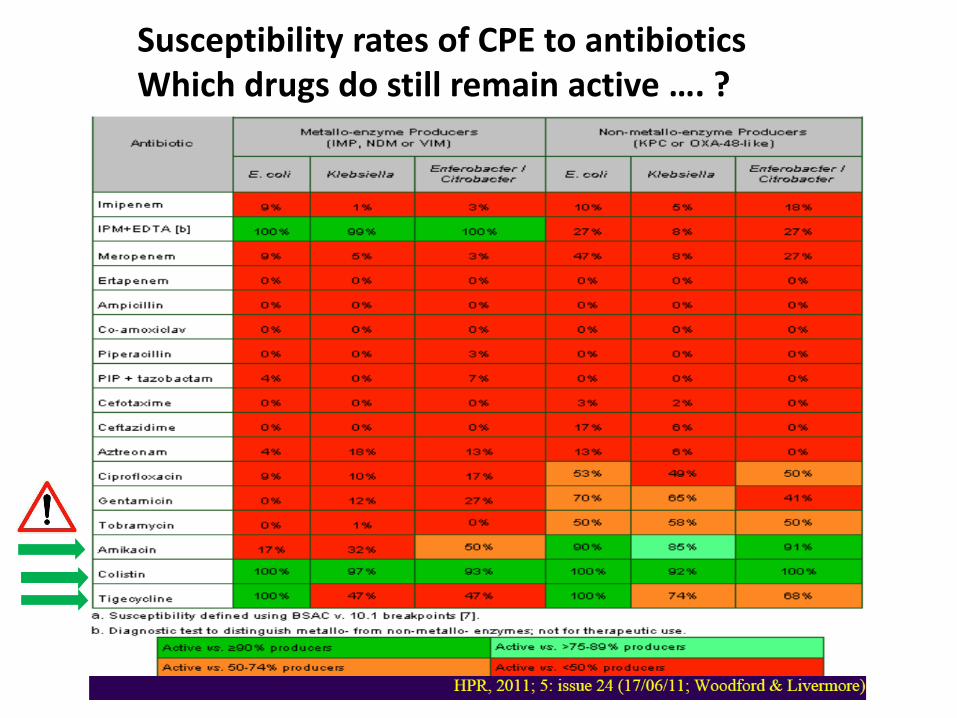
Susceptibility rates of CPE to antibiotics Which drugs do still remain active …. ?
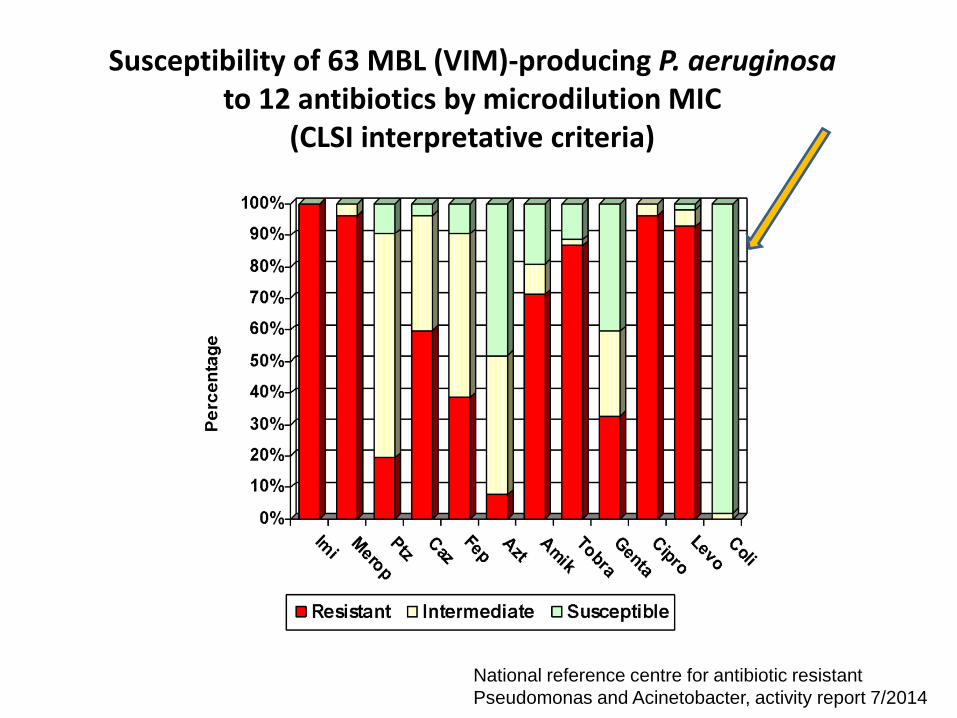
Susceptibility of 63 MBL (VIM)-producing P. aeruginosa to 12 antibiotics by microdilution MIC
(CLSI interpretative criteria)
National reference centre for antibiotic resistant
Pseudomonas and Acinetobacter, activity report 7/2014
06/06/13 Liège - certificat interuniversitaire 65
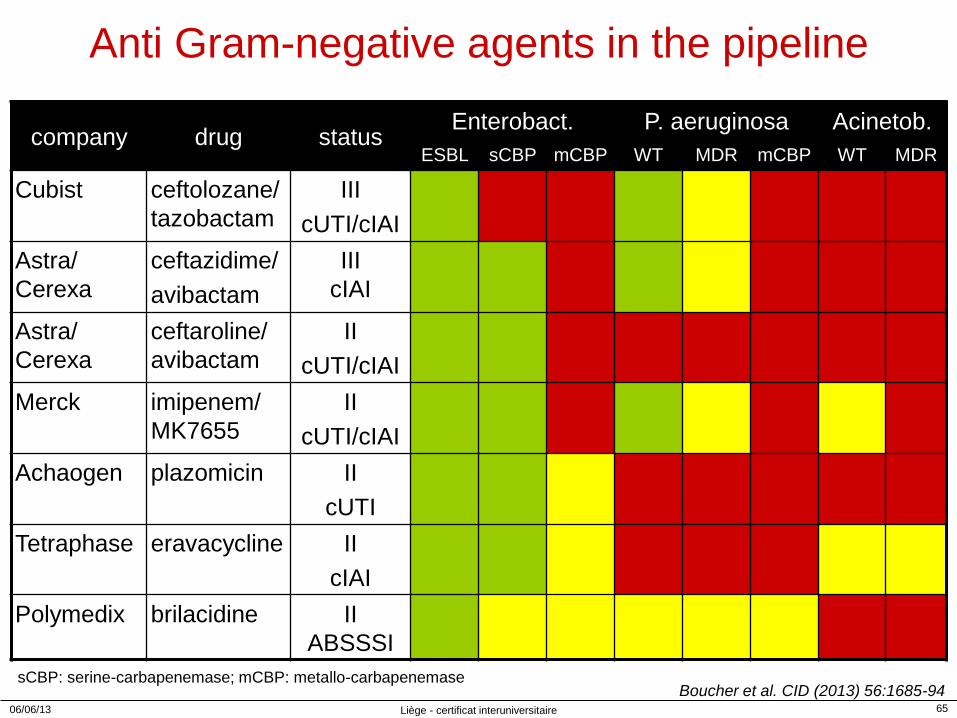
Anti Gram-negative agents in the pipeline
company drug status Enterobact. P. aeruginosa Acinetob.
ESBL sCBP mCBP WT MDR mCBP WT MDR
Cubist ceftolozane/
tazobactam
III
cUTI/cIAI
Astra/
Cerexa
ceftazidime/
avibactam
III
cIAI
Astra/
Cerexa
ceftaroline/
avibactam
II
cUTI/cIAI
Merck imipenem/
MK7655
II
cUTI/cIAI
Achaogen plazomicin II
cUTI
Tetraphase eravacycline II
cIAI
Polymedix brilacidine II
ABSSSI
Boucher et al. CID (2013) 56:1685-94 sCBP: serine-carbapenemase; mCBP: metallo-carbapenemase
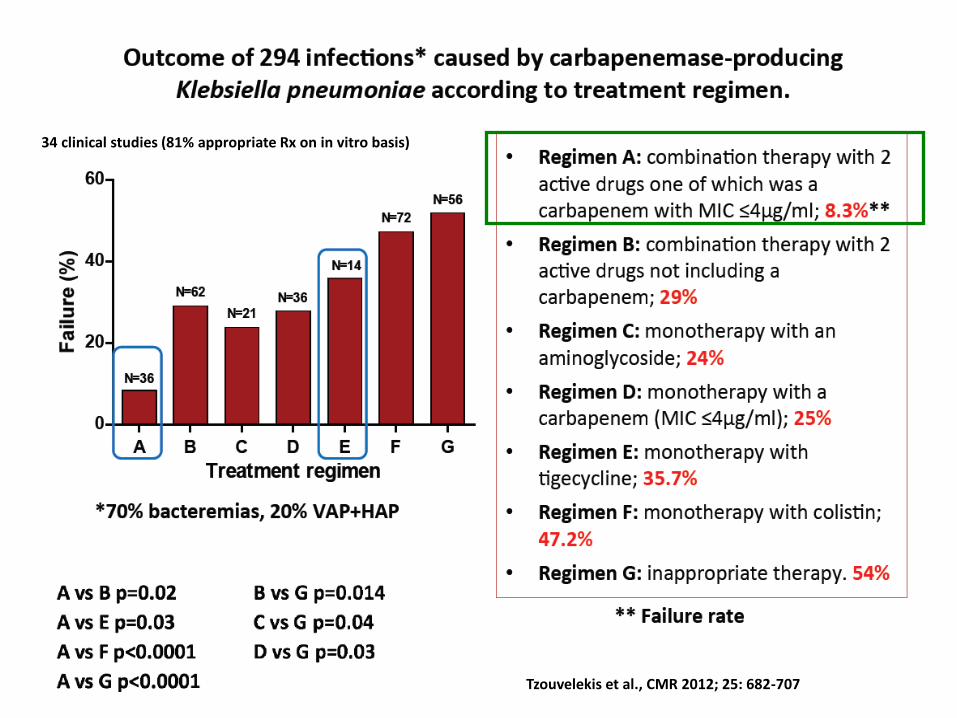
34 clinical studies (81% appropriate Rx on in vitro basis)
Tzouvelekis et al., CMR 2012; 25: 682-707
Importance of Infection control programs to reduce the spread of CRE
Israël (2006)
• Multidisciplinary infection control program (guidelines for
patient isolation, cohorting, environment cleaning, education of staff, computerization system for flagging of CR-KP carriers (provision of instructions)
• Increase in rate of active surveillance by rectal sample for
carriers from 20% to 89% (in 2006-8 and 2009-2010)
‒ of CRE incidence by 16x from 6.6/1000 patient to 0.5/1000 patient (p<0.001; sustained over 30 months)
‒ Decrease of rate of cross-infection from by 2-3x (6.6% in 2006-2008 to 2.7% in 2009-2010; (p <0.05)
Ciobotaro P, AJIC 2011: 39: 671-7
Carbapenem producing enterobacteriaceae (CPE) Risk factors and indications for screening
Absolute indications for screening: – Patients who received medical care abroad (last 6 months -CDC)
– Patients epidemiologically linked to previously unrecognized CRE carrier (roommate, shared HCW)
– Patients known as previously infected or colonized by CPE
Relative indication: – Functional dependency (low-level autonomy)
– Indwelling devices
– Prior hospitalization or transfer from LTFC
– Previous antibiotics
(several cures or long-lasting ABs in the last 3-6 months)
Geriatric wards !!!
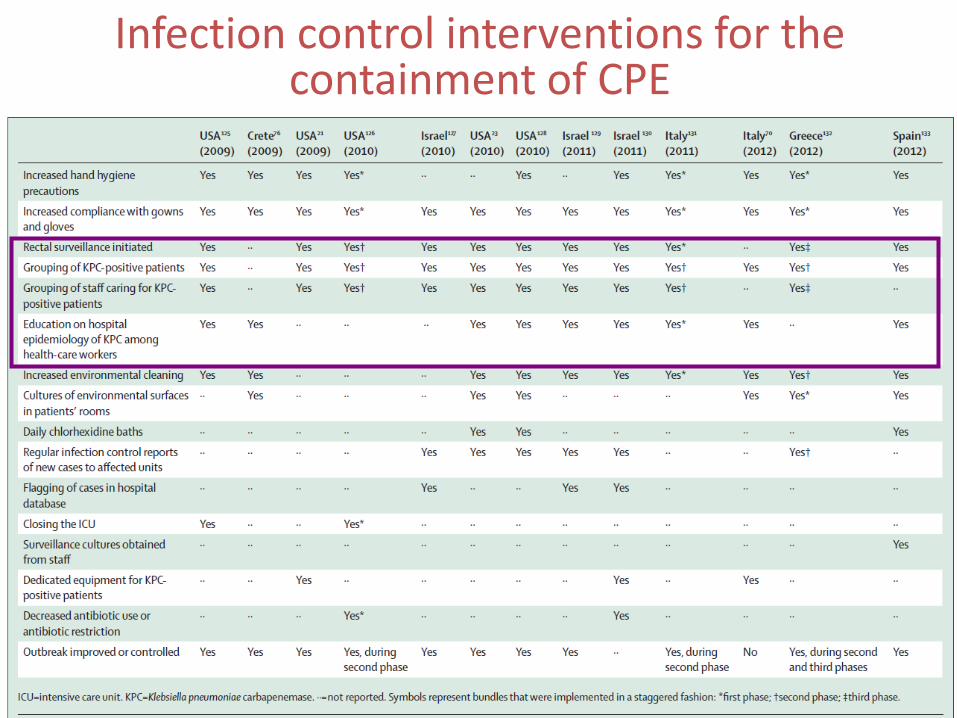
Infection control interventions for the containment of CPE
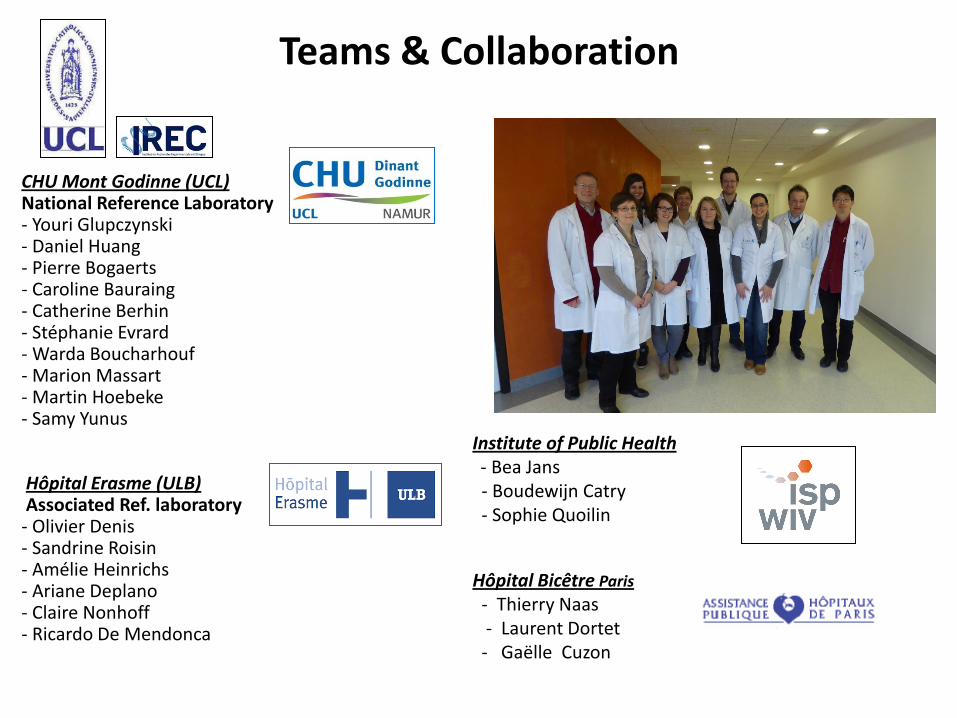
Institute of Public Health - Bea Jans - Boudewijn Catry - Sophie Quoilin
Hôpital Bicêtre Paris
- Thierry Naas - Laurent Dortet - Gaëlle Cuzon
Teams & Collaboration
CHU Mont Godinne (UCL) National Reference Laboratory - Youri Glupczynski - Daniel Huang - Pierre Bogaerts - Caroline Bauraing - Catherine Berhin - Stéphanie Evrard - Warda Boucharhouf - Marion Massart - Martin Hoebeke - Samy Yunus
Hôpital Erasme (ULB) Associated Ref. laboratory
- Olivier Denis - Sandrine Roisin - Amélie Heinrichs - Ariane Deplano - Claire Nonhoff - Ricardo De Mendonca

Epidemiologie de la résistance aux antibiotiques
chez P. aeruginosa
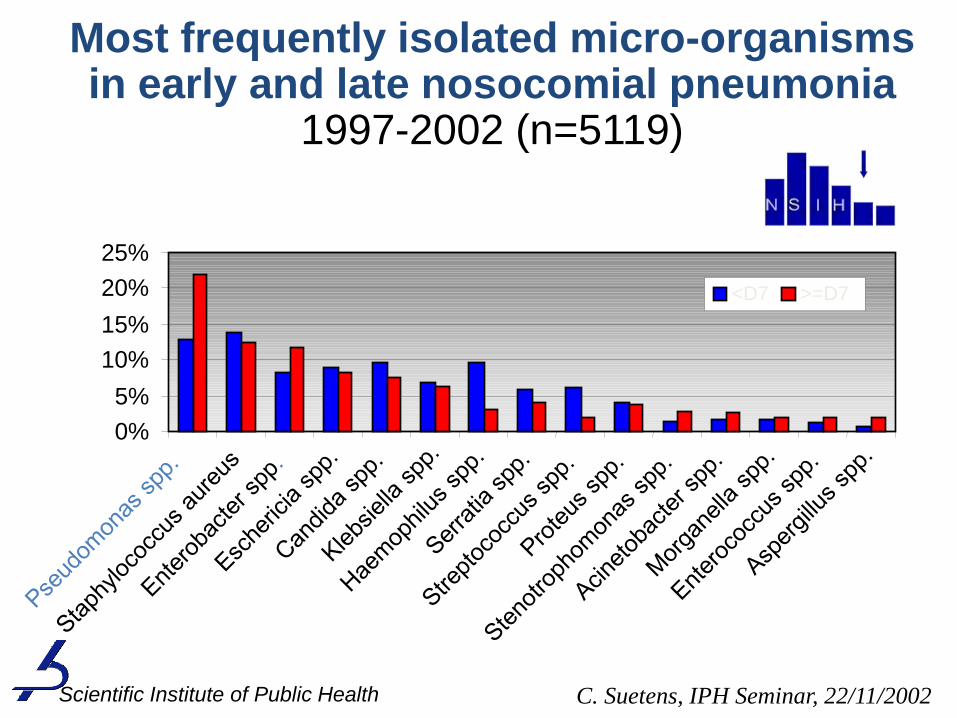
0%
5%
10%
15%
20%
25%
<D7 >=D7
Most frequently isolated micro-organisms in early and late nosocomial pneumonia
1997-2002 (n=5119)
C. Suetens, IPH Seminar, 22/11/2002 Scientific Institute of Public Health
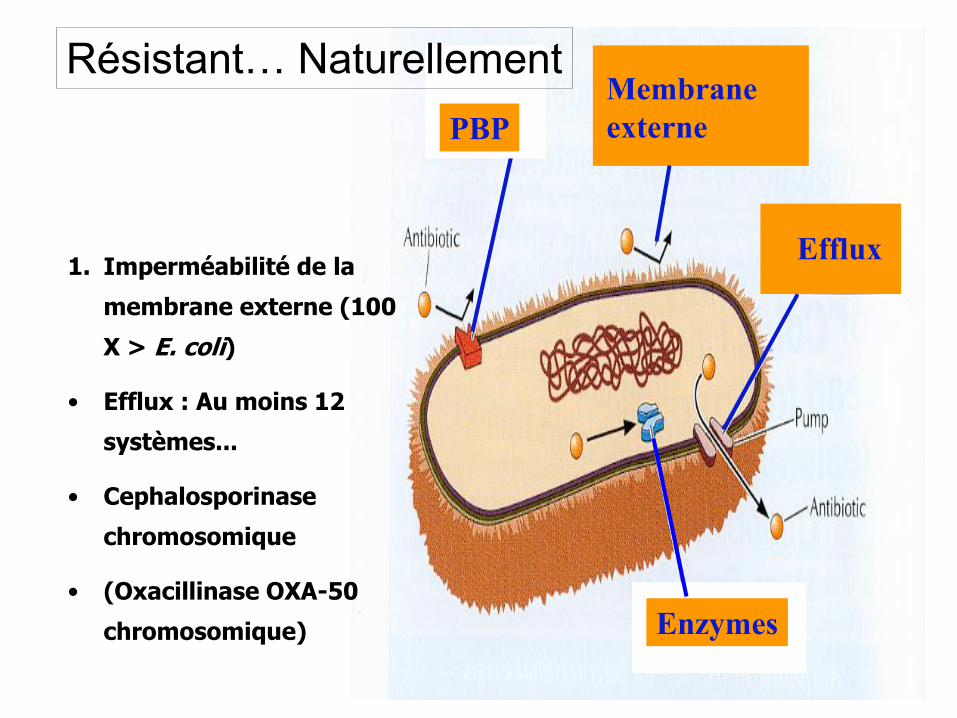
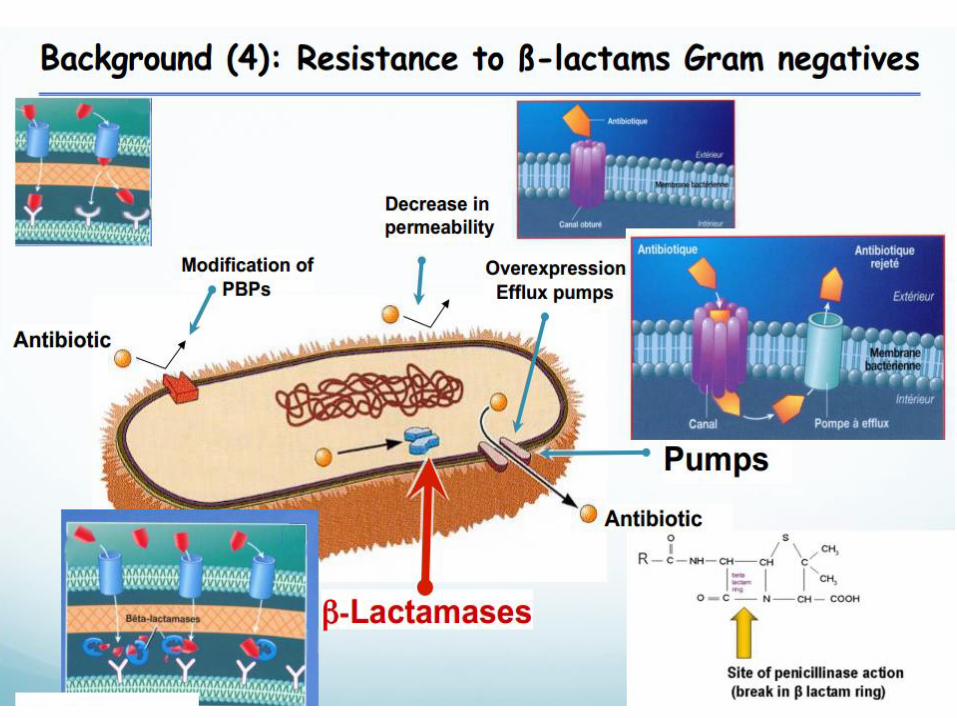
1. Imperméabilité de la
membrane externe (100
X > E. coli)
• Efflux : Au moins 12
systèmes...
• Cephalosporinase
chromosomique
• (Oxacillinase OXA-50
chromosomique)
Efflux
Membrane
externe PBP
Enzymes
Résistant… Naturellement
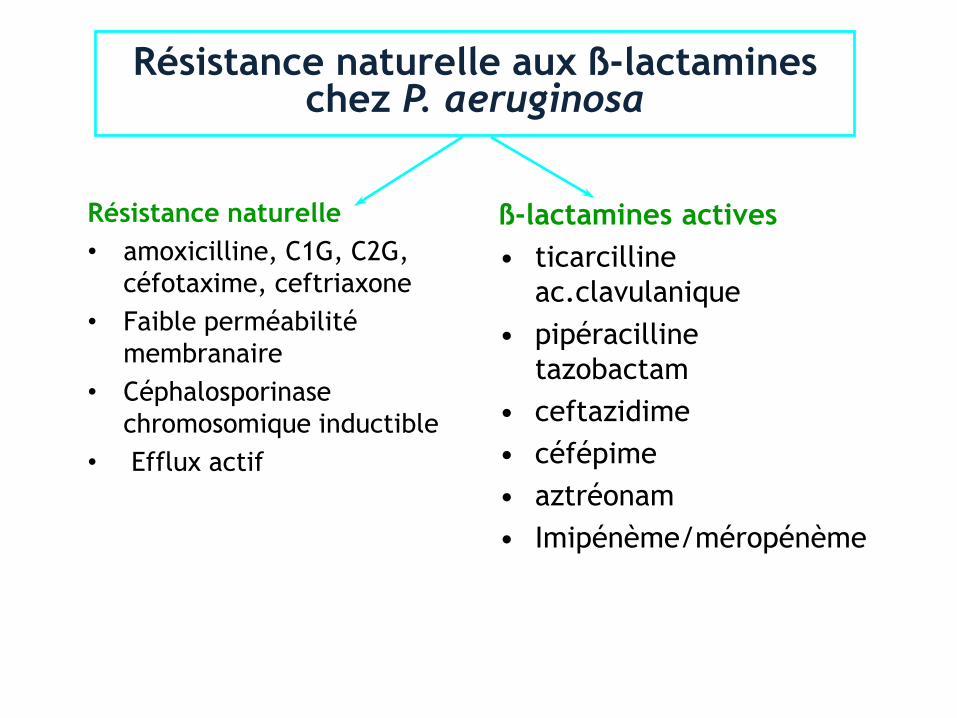
Résistance naturelle aux ß-lactamines chez P. aeruginosa
Résistance naturelle
• amoxicilline, C1G, C2G,
céfotaxime, ceftriaxone
• Faible perméabilité
membranaire
• Céphalosporinase
chromosomique inductible
• Efflux actif
ß-lactamines actives
• ticarcilline
ac.clavulanique
• pipéracilline
tazobactam
• ceftazidime
• céfépime
• aztréonam
• Imipénème/méropénème
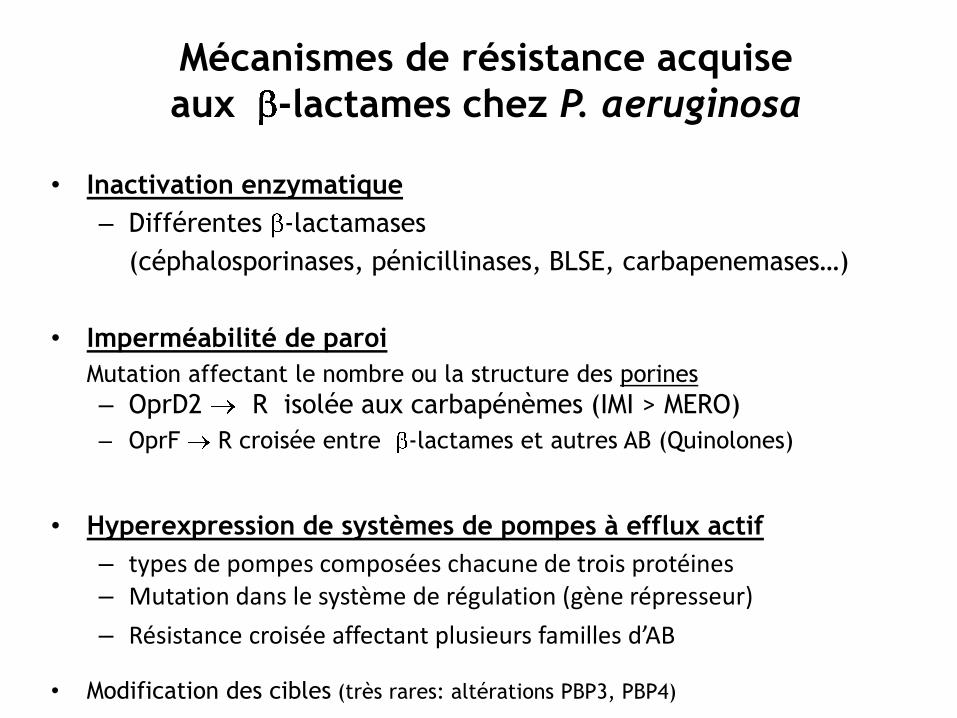
Mécanismes de résistance acquise
aux -lactames chez P. aeruginosa
• Inactivation enzymatique
– Différentes -lactamases
(céphalosporinases, pénicillinases, BLSE, carbapenemases…)
• Imperméabilité de paroi
Mutation affectant le nombre ou la structure des porines
– OprD2 R isolée aux carbapénèmes (IMI > MERO)
– OprF R croisée entre -lactames et autres AB (Quinolones)
• Hyperexpression de systèmes de pompes à efflux actif
– types de pompes composées chacune de trois protéines – Mutation dans le système de régulation (gène répresseur)
– Résistance croisée affectant plusieurs familles d’AB
• Modification des cibles (très rares: altérations PBP3, PBP4)
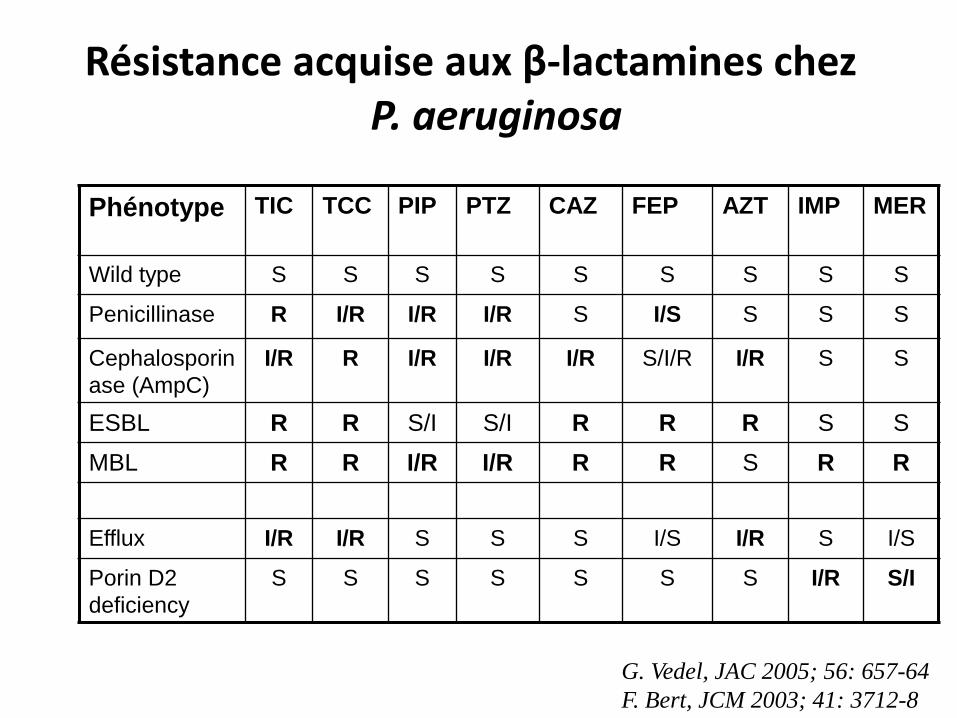
Résistance acquise aux β-lactamines chez P. aeruginosa
Phénotype TIC TCC PIP PTZ CAZ FEP AZT IMP MER
Wild type S S S S S S S S S
Penicillinase R I/R I/R I/R S I/S S S S
Cephalosporin
ase (AmpC)
I/R R I/R I/R I/R S/I/R I/R S S
ESBL R R S/I S/I R R R S S
MBL R R I/R I/R R R S R R
Efflux I/R I/R S S S I/S I/R S I/S
Porin D2
deficiency
S S S S S S S I/R S/I
G. Vedel, JAC 2005; 56: 657-64
F. Bert, JCM 2003; 41: 3712-8
Antimicrobial resistance surveillance in Europe
EARS-Net Report 2013
www.ecdc.europa.eu
Pseudomonas aeruginosa: Percentage of invasive
isolates with resistance to carbapenems in Europe
(2013)
weighted mean resistance : 17.6%
2.9% (Denmark) – 60.5% (Romania)
7 countries: < 10%
14 countries: 10-25%
9 countries: >25% 11%
43.8%
58.9% 17.2%
25.9%
5.8%
49.3%
32.3%
28%
30.2%
Antimicrobial resistance surveillance in Europe
EARS-Net Report 2013
www.ecdc.europa.eu
Pseudomonas aeruginosa: Percentage of invasive isolates with
resistance to > 3 classes* of ABs (MDR) in Europe (2013)
weighted mean resistance : 13%
0% (Estonia/Iceland) – 49.4%
(Romania)
16 countries: < 10%
11 countries: 10-25%
3 countries: >25%
11.3%
49.4%
36.1% 12.6%
24.5%
4.1%
39.3%
24%
23.3.%
* Pip/tazo, Cefta, FQs, Aminoglycosides, Carbapenems
3.4%
4% of isolates resistant to all tested agents (XDR)
1% of isolates resistant to colistin
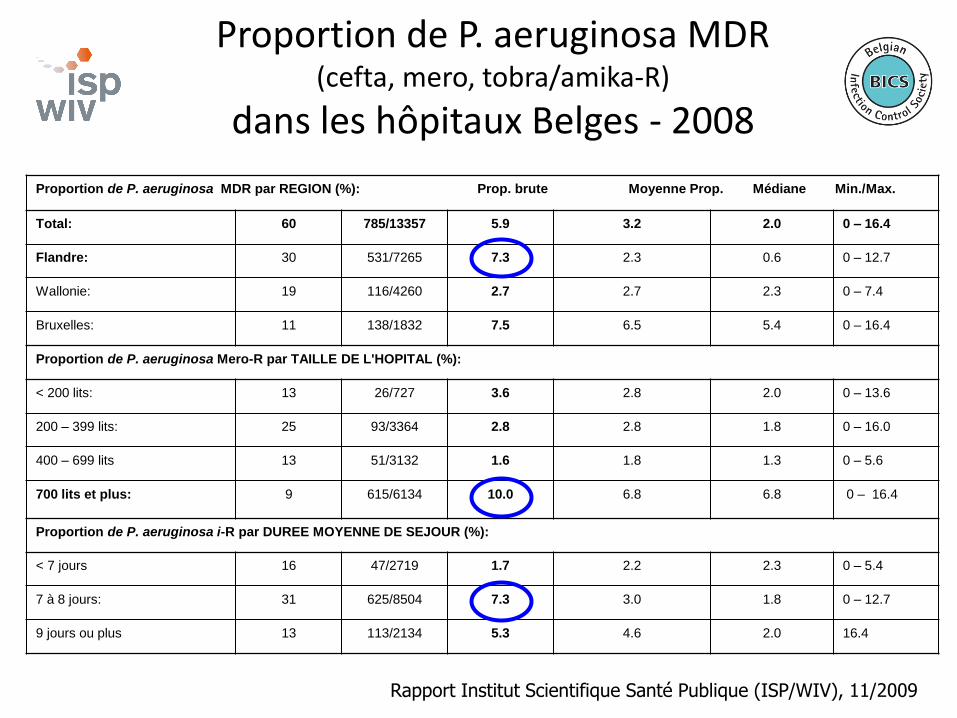
Proportion de P. aeruginosa MDR (cefta, mero, tobra/amika-R)
dans les hôpitaux Belges - 2008
Proportion de P. aeruginosa MDR par REGION (%): Prop. brute Moyenne Prop. Médiane Min./Max.
Total: 60 785/13357 5.9 3.2 2.0 0 – 16.4
Flandre: 30 531/7265 7.3 2.3 0.6 0 – 12.7
Wallonie: 19 116/4260 2.7 2.7 2.3 0 – 7.4
Bruxelles: 11 138/1832 7.5 6.5 5.4 0 – 16.4
Proportion de P. aeruginosa Mero-R par TAILLE DE L'HOPITAL (%):
< 200 lits: 13 26/727 3.6 2.8 2.0 0 – 13.6
200 – 399 lits: 25 93/3364 2.8 2.8 1.8 0 – 16.0
400 – 699 lits 13 51/3132 1.6 1.8 1.3 0 – 5.6
700 lits et plus: 9 615/6134 10.0 6.8 6.8 0 – 16.4
Proportion de P. aeruginosa i-R par DUREE MOYENNE DE SEJOUR (%):
< 7 jours 16 47/2719 1.7 2.2 2.3 0 – 5.4
7 à 8 jours: 31 625/8504 7.3 3.0 1.8 0 – 12.7
9 jours ou plus 13 113/2134 5.3 4.6 2.0 16.4
Rapport Institut Scientifique Santé Publique (ISP/WIV), 11/2009
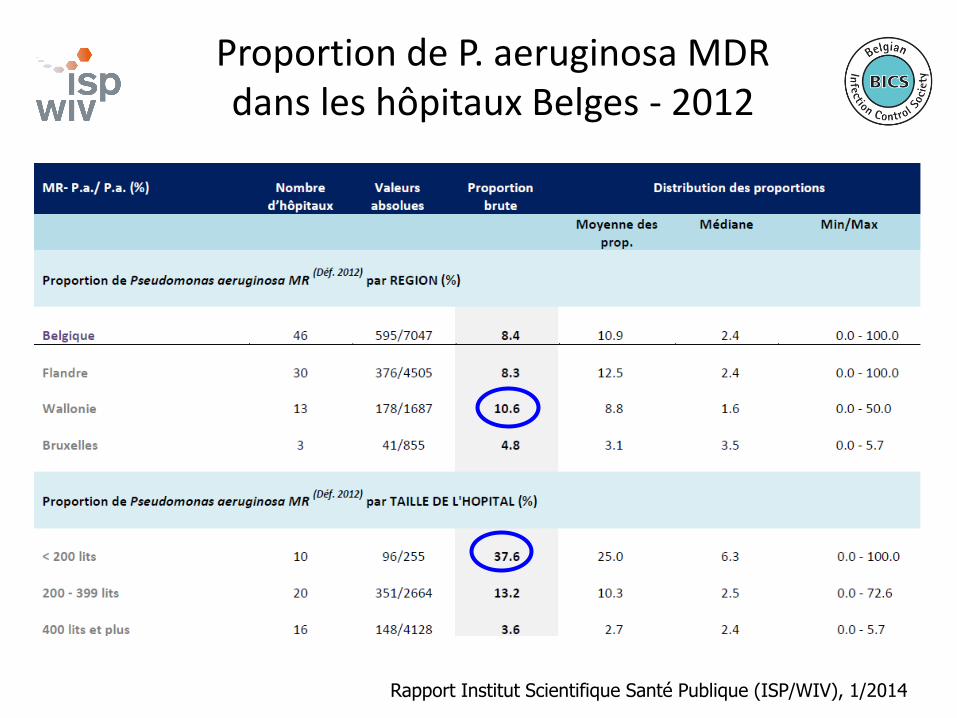
Proportion de P. aeruginosa MDR dans les hôpitaux Belges - 2012
Rapport Institut Scientifique Santé Publique (ISP/WIV), 1/2014
Susceptibility of P. aeruginosa to antimicrobials: Belgian multicentre hospital survey
• 25 representative university affiliated and general hospitals in Belgium (8 Wallonia, 11 Flanders, 5 Brussels)
• Clinically significant non-repetitive isolates from samples taken >48 hrs after admission – Collection period: 1st semester 2010
– Blood, deep respiratory isolates, sterile body fluids, urine
– Maximum of 40 isolates/hospital
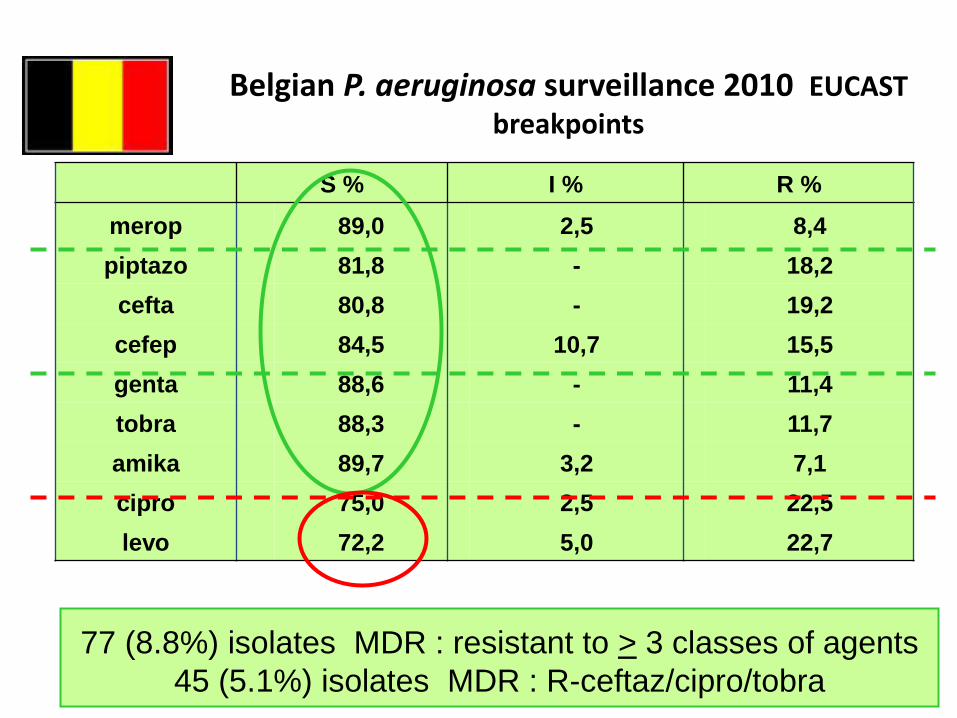
Belgian P. aeruginosa surveillance 2010 EUCAST breakpoints
S % I % R %
merop 89,0 2,5 8,4
piptazo 81,8 - 18,2
cefta 80,8 - 19,2
cefep 84,5 10,7 15,5
genta 88,6 - 11,4
tobra 88,3 - 11,7
amika 89,7 3,2 7,1
cipro 75,0 2,5 22,5
levo 72,2 5,0 22,7
77 (8.8%) isolates MDR : resistant to > 3 classes of agents
45 (5.1%) isolates MDR : R-ceftaz/cipro/tobra
Pseudomonas spp. and Acinetobacter spp. isolates referred to the National Reference
Centre in Belgium in 2013
National Reference Center for multidrug-resistant Pseudomonas spp. and Acinetobacter
spp. CHU Mont-Godinne, Yvoir, Belgium
2014-01-15
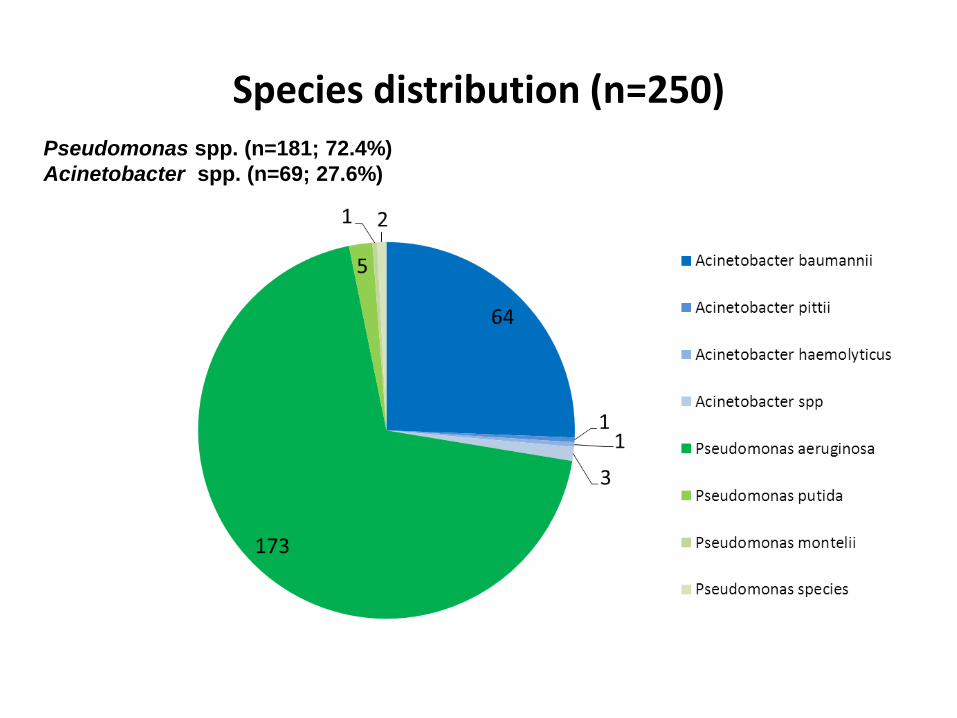
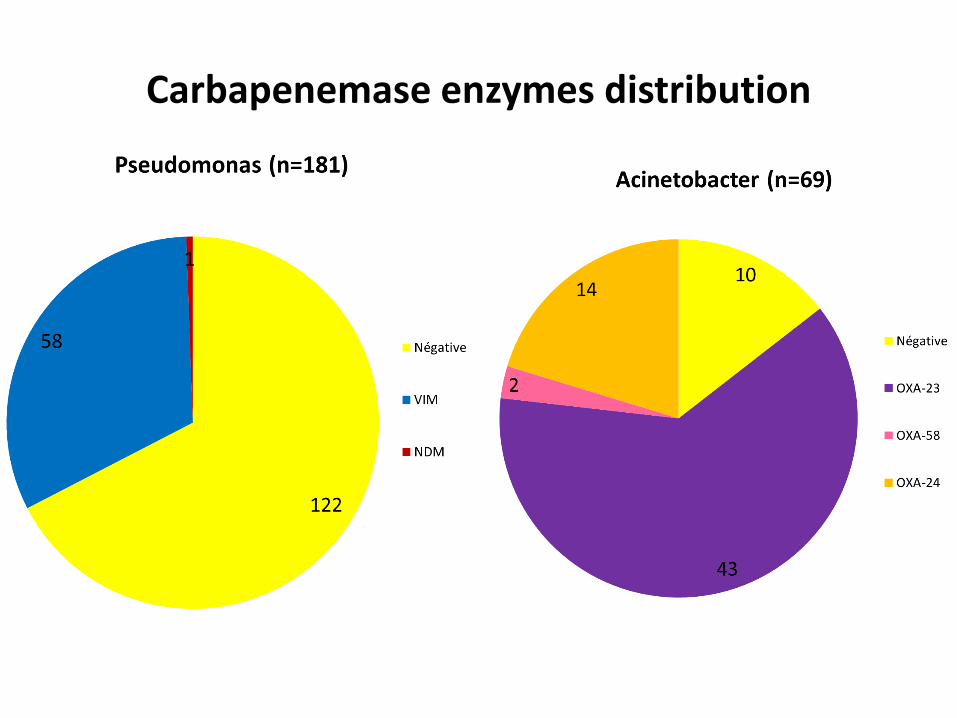
Species distribution (n=250) Pseudomonas spp. (n=181; 72.4%)
Acinetobacter spp. (n=69; 27.6%)
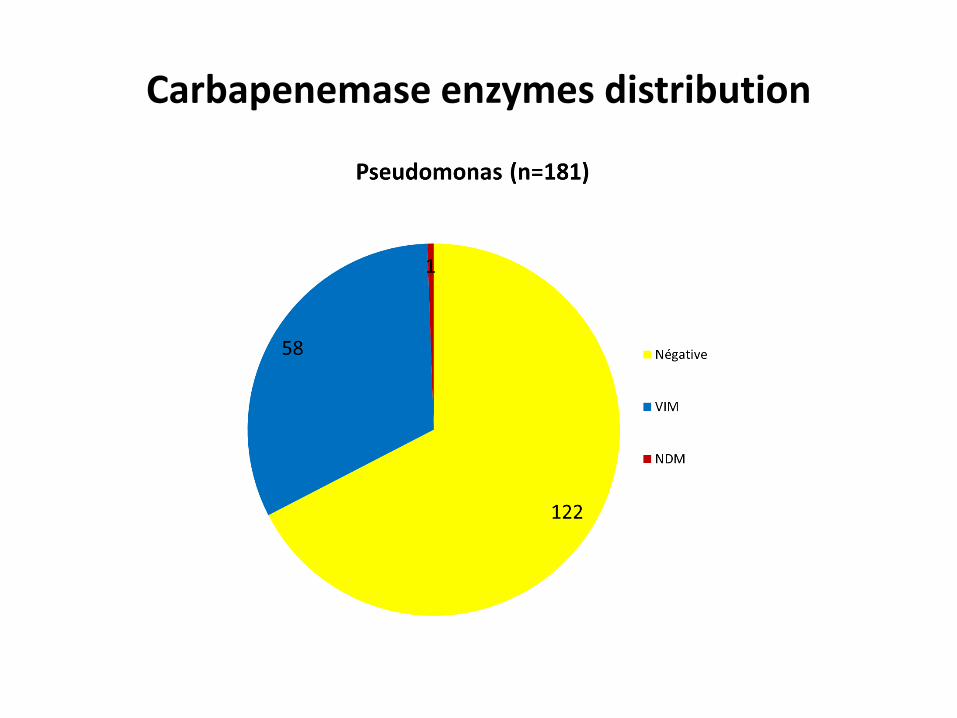
Carbapenemase enzymes distribution
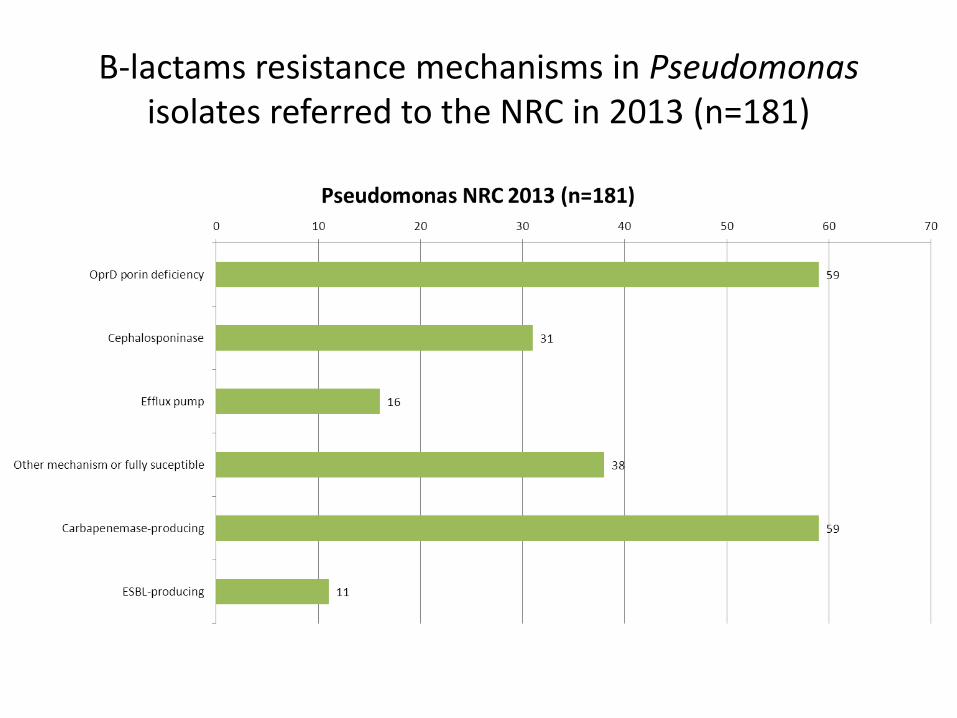
Β-lactams resistance mechanisms in Pseudomonas isolates referred to the NRC in 2013 (n=181)
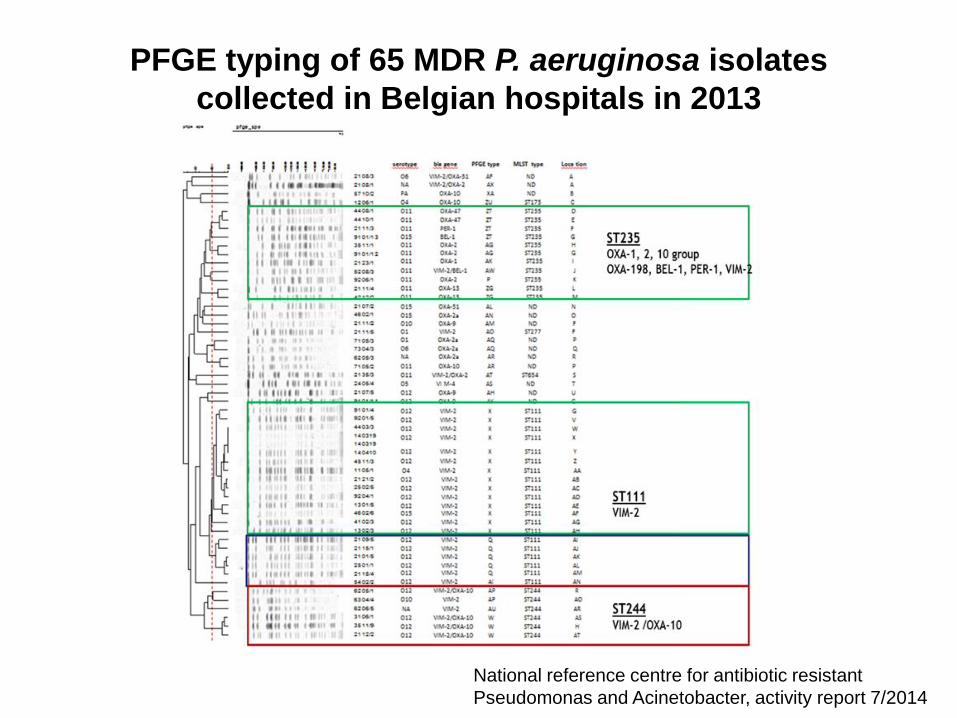
PFGE typing of 65 MDR P. aeruginosa isolates
collected in Belgian hospitals in 2013
National reference centre for antibiotic resistant
Pseudomonas and Acinetobacter, activity report 7/2014
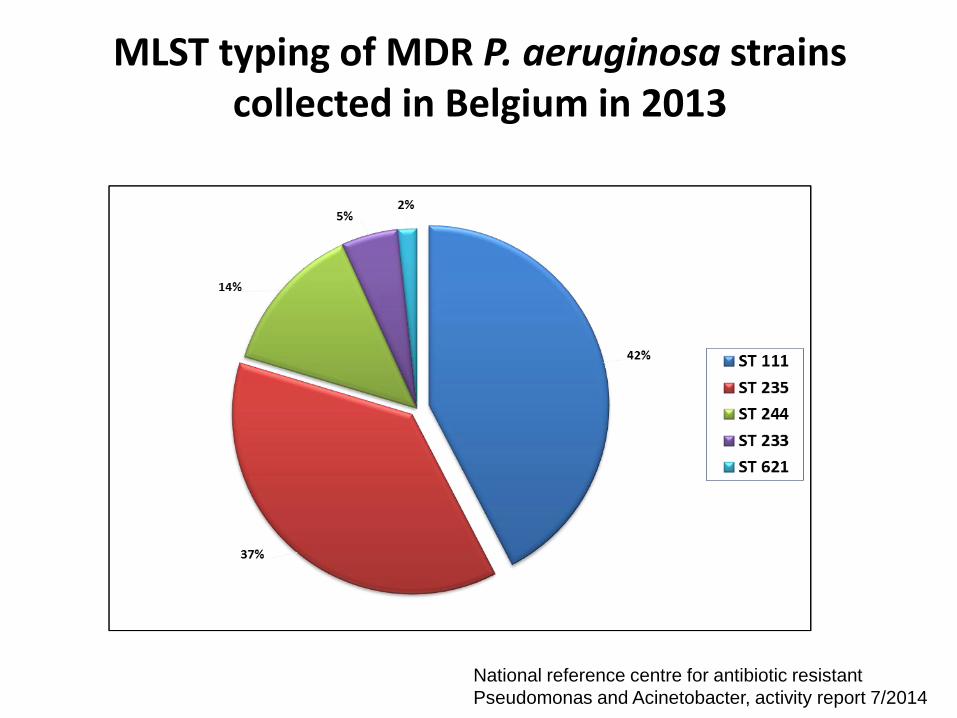
MLST typing of MDR P. aeruginosa strains collected in Belgium in 2013
National reference centre for antibiotic resistant
Pseudomonas and Acinetobacter, activity report 7/2014
Epidemiologie de la résistance aux antibiotiques
chez Acinetobacter spp.
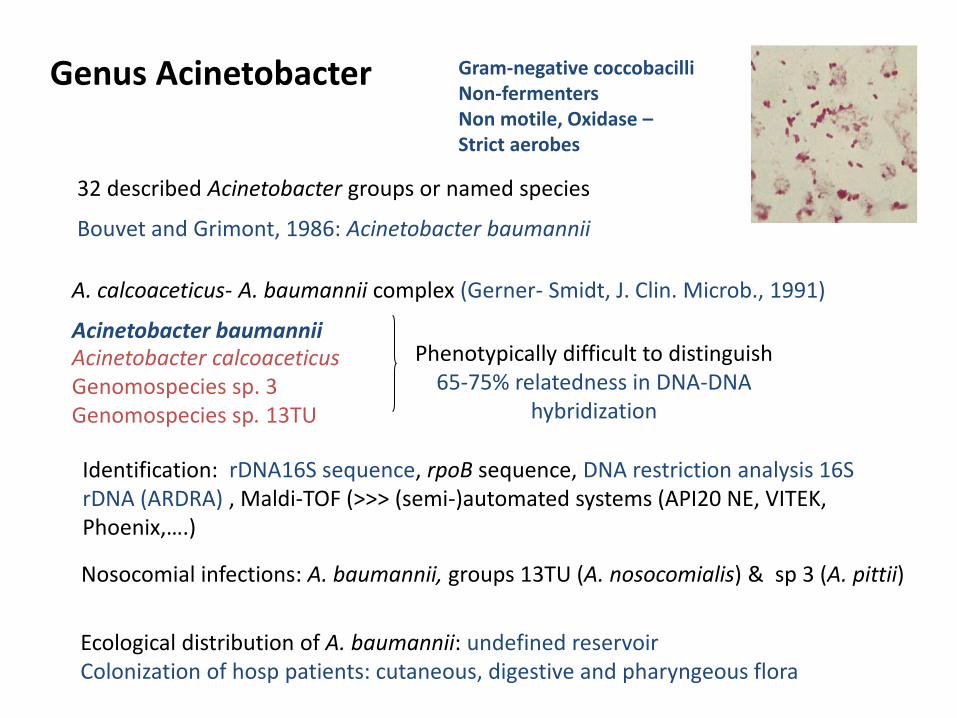
Genus Acinetobacter
32 described Acinetobacter groups or named species Bouvet and Grimont, 1986: Acinetobacter baumannii
A. calcoaceticus- A. baumannii complex (Gerner- Smidt, J. Clin. Microb., 1991) Acinetobacter baumannii Acinetobacter calcoaceticus Genomospecies sp. 3 Genomospecies sp. 13TU
Phenotypically difficult to distinguish 65-75% relatedness in DNA-DNA
hybridization
Gram-negative coccobacilli Non-fermenters Non motile, Oxidase – Strict aerobes
Identification: rDNA16S sequence, rpoB sequence, DNA restriction analysis 16S rDNA (ARDRA) , Maldi-TOF (>>> (semi-)automated systems (API20 NE, VITEK, Phoenix,….)
Nosocomial infections: A. baumannii, groups 13TU (A. nosocomialis) & sp 3 (A. pittii)
Ecological distribution of A. baumannii: undefined reservoir Colonization of hosp patients: cutaneous, digestive and pharyngeous flora
Significant nosocomial pathogen In immunocompromised patients or with underlying diseases
Mainly urinary infections, pneumomia, device-related infections(also bacteremia, meningitis, skin and wound infections)
Mainly ICU
1% of hospital pathogens. 10% of nosocomial pneumonia in ICU; 17-50% mortality for A. baumannii bacteremia
Outbreaks (+++); seasonal variations; 40% infected for 60% colonized
Recent reports of community acquired infections Pneumonia (rarely meningitis, cellulitis)
Alcohol abuse, diabetes, cancer, chronic lung diseases
Lowman W et al.,J. Med Microbiol. 2008 Garcia-Garmendia JL et al. Clin. Infect. Dis. 2001
Acinetobacter baumannii - Emergent Pathogen
Acinetobacter baumannii infections
• Propensity for clonal spread
• Persistence in the environment up to 12 months
• Involvement in hospital outbreaks, evolves in burst
• Endemicity in certain hospitals
• Resistance to multiple antimicrobial agents
• Many recent outbreaks have been caused by multidrug-
resistant (MDR) strains of A. baumannii
Stoeva et al., CMI. 2008 Quinteira et al. AAC. 2004 Manikal et al., CID 2000
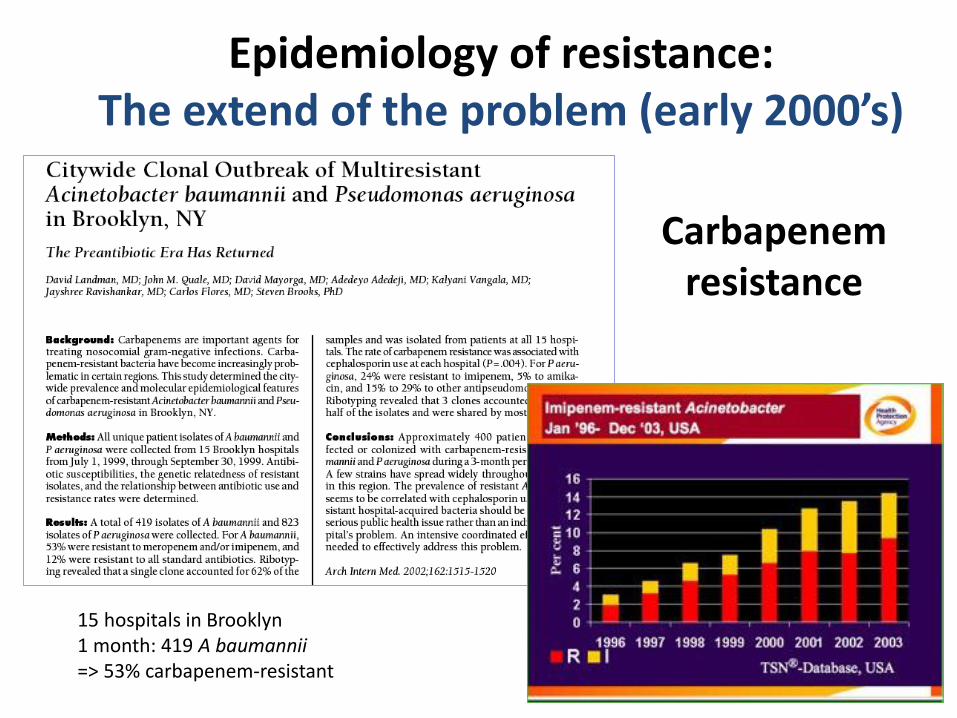
Epidemiology of resistance: The extend of the problem (early 2000’s)
Carbapenem resistance
15 hospitals in Brooklyn 1 month: 419 A baumannii => 53% carbapenem-resistant
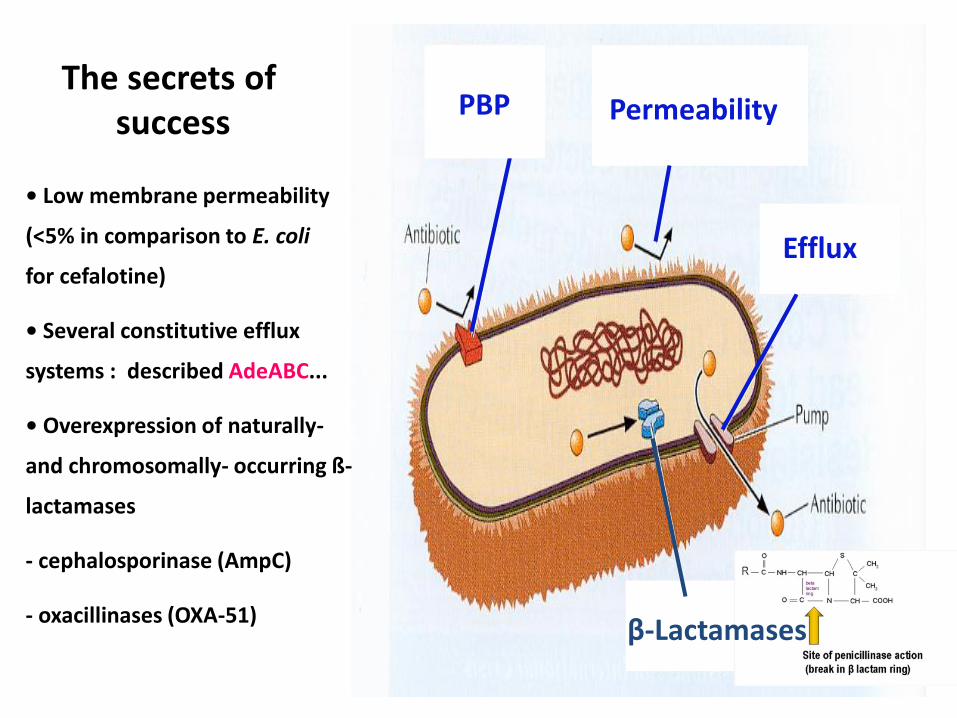
Efflux
Permeability PBP
• Low membrane permeability
(<5% in comparison to E. coli
for cefalotine)
• Several constitutive efflux
systems : described AdeABC...
• Overexpression of naturally-
and chromosomally- occurring ß-
lactamases
- cephalosporinase (AmpC)
- oxacillinases (OXA-51)
The secrets of success
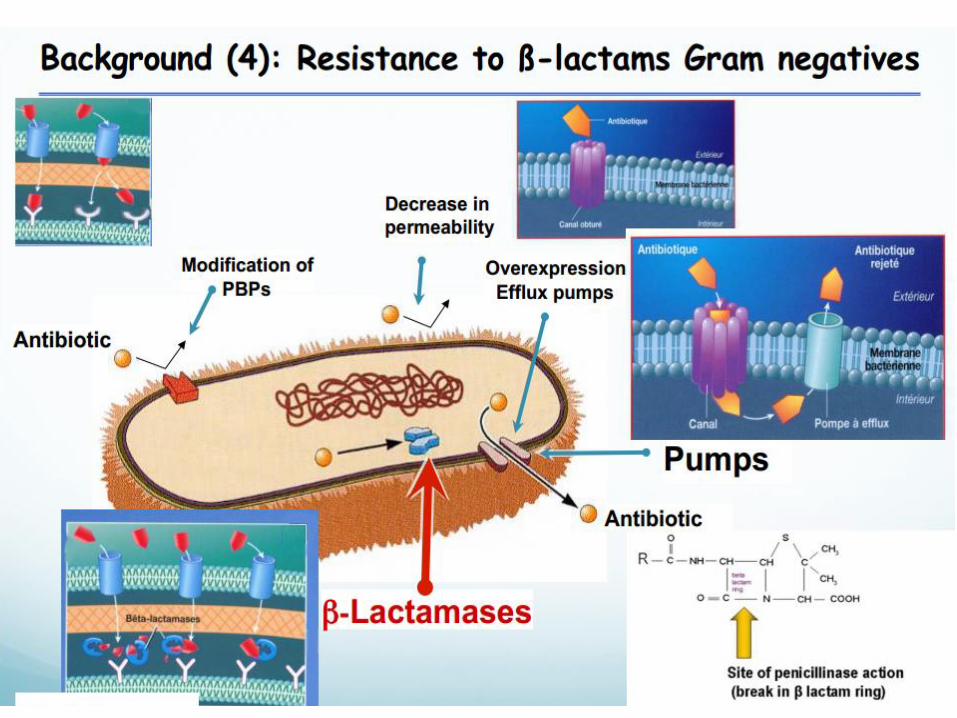
β-Lactamases
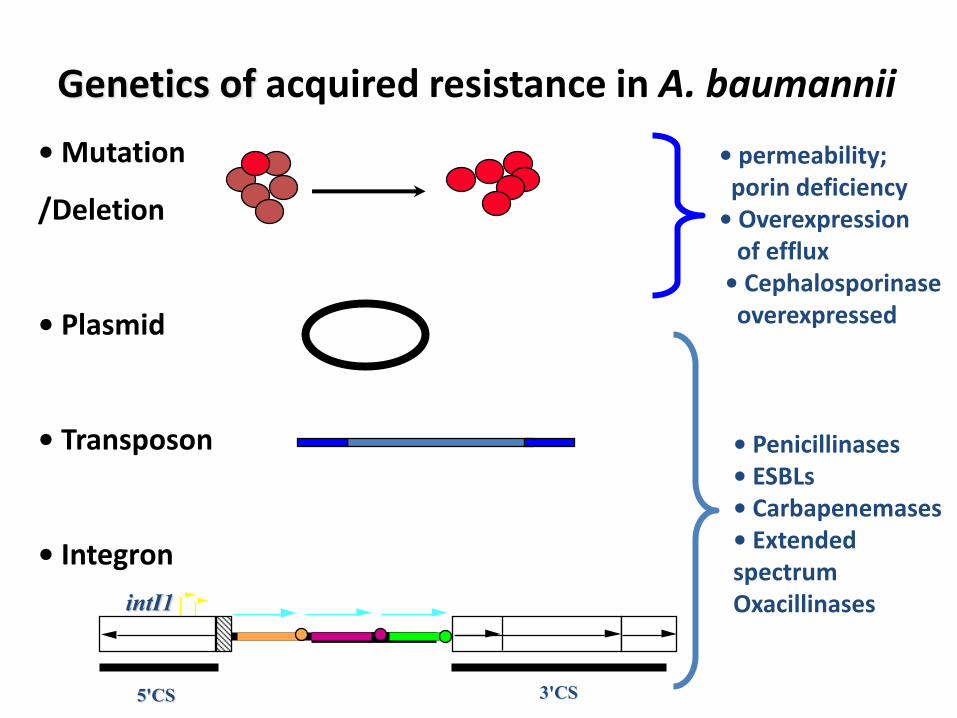
Genetics of acquired resistance in A. baumannii
• Mutation
/Deletion
• Plasmid
• Transposon
• Integron
• permeability; porin deficiency • Overexpression of efflux • Cephalosporinase overexpressed
• Penicillinases • ESBLs • Carbapenemases • Extended spectrum Oxacillinases
intI1
5'CS 3'CS
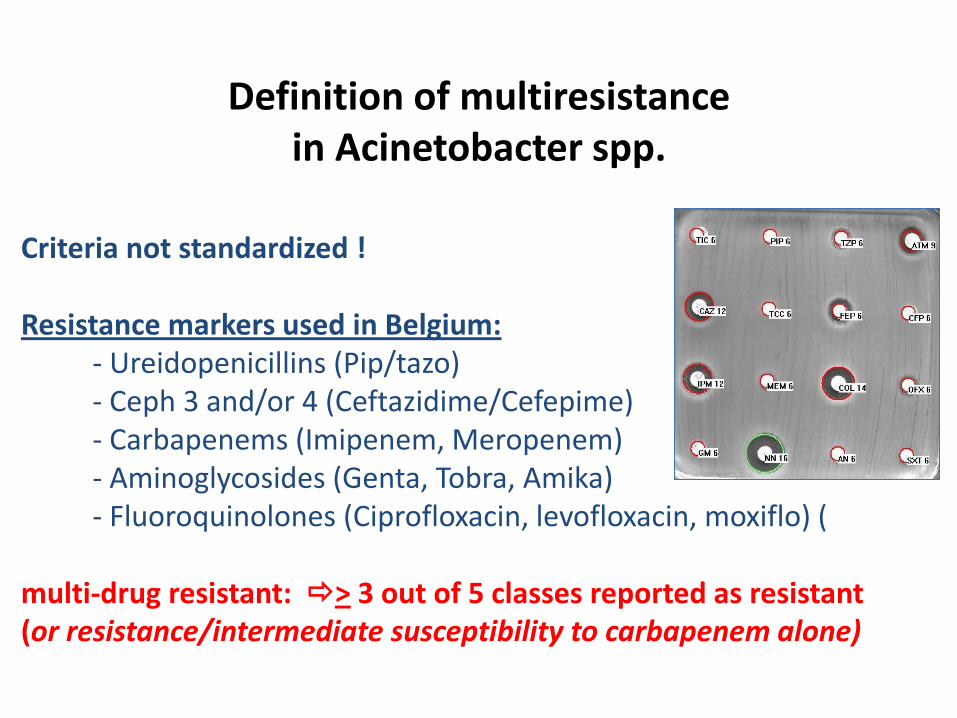
Definition of multiresistance in Acinetobacter spp.
Criteria not standardized ! Resistance markers used in Belgium: - Ureidopenicillins (Pip/tazo) - Ceph 3 and/or 4 (Ceftazidime/Cefepime) - Carbapenems (Imipenem, Meropenem) - Aminoglycosides (Genta, Tobra, Amika) - Fluoroquinolones (Ciprofloxacin, levofloxacin, moxiflo) ( multi-drug resistant: > 3 out of 5 classes reported as resistant (or resistance/intermediate susceptibility to carbapenem alone)
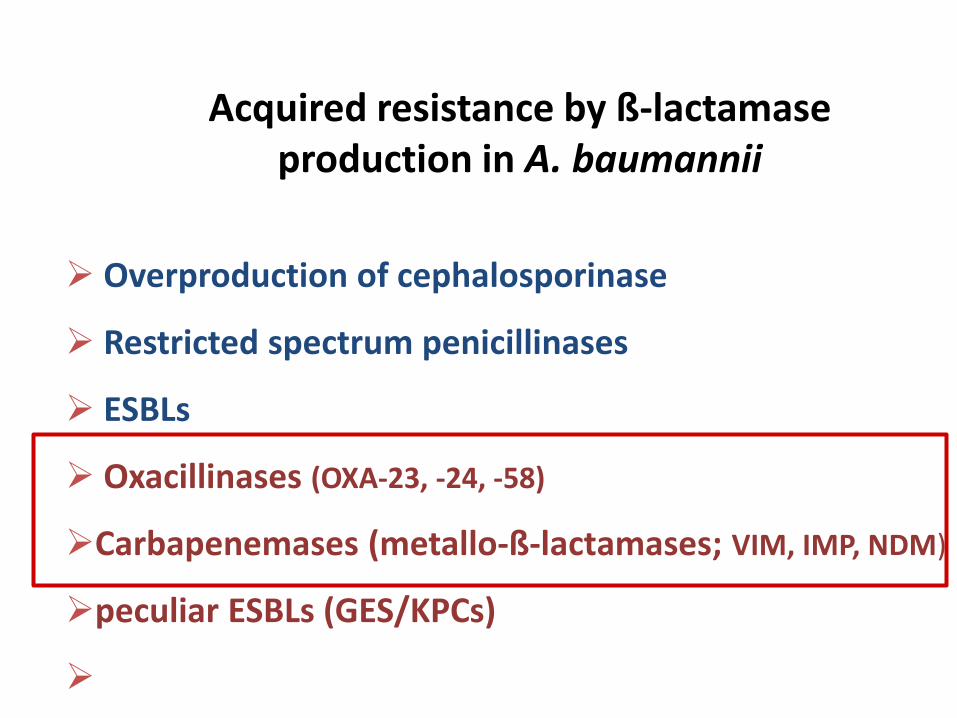
Acquired resistance by ß-lactamase production in A. baumannii
Overproduction of cephalosporinase
Restricted spectrum penicillinases
ESBLs
Oxacillinases (OXA-23, -24, -58)
Carbapenemases (metallo-ß-lactamases; VIM, IMP, NDM)
peculiar ESBLs (GES/KPCs)
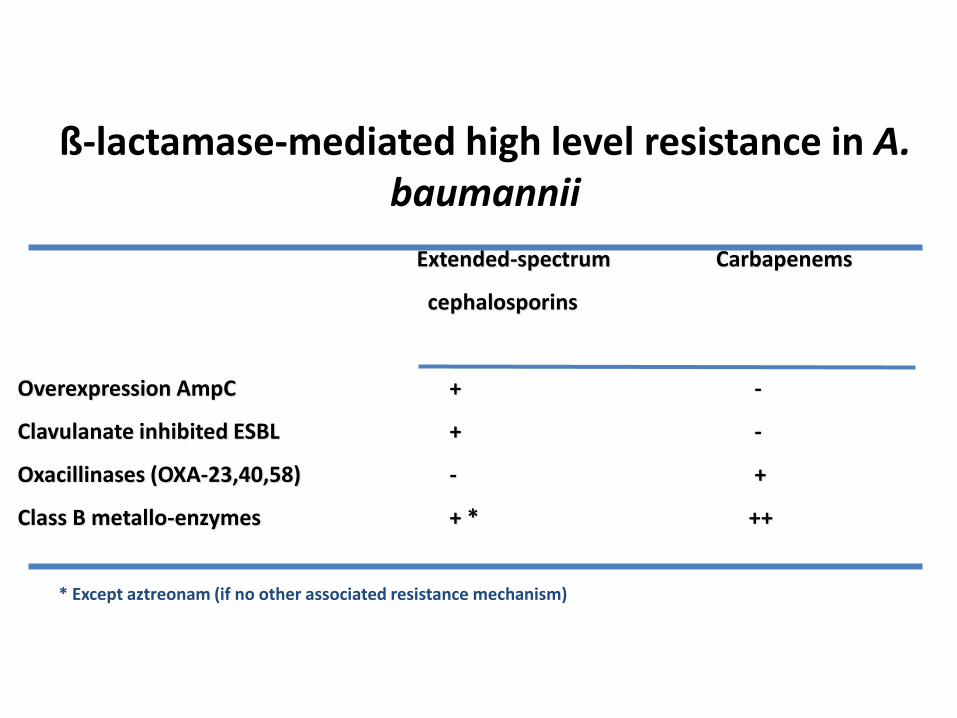
ß-lactamase-mediated high level resistance in A. baumannii
Extended-spectrum Carbapenems
cephalosporins
Overexpression AmpC + -
Clavulanate inhibited ESBL + -
Oxacillinases (OXA-23,40,58) - +
Class B metallo-enzymes + * ++
* Except aztreonam (if no other associated resistance mechanism)
Pseudomonas spp. and Acinetobacter spp. isolates referred to the National Reference
Centre in Belgium in 2013
National Reference Center for multidrug-resistant Pseudomonas spp. and Acinetobacter
spp. CHU Mont-Godinne, Yvoir, Belgium
2014-01-15
Carbapenemase enzymes distribution
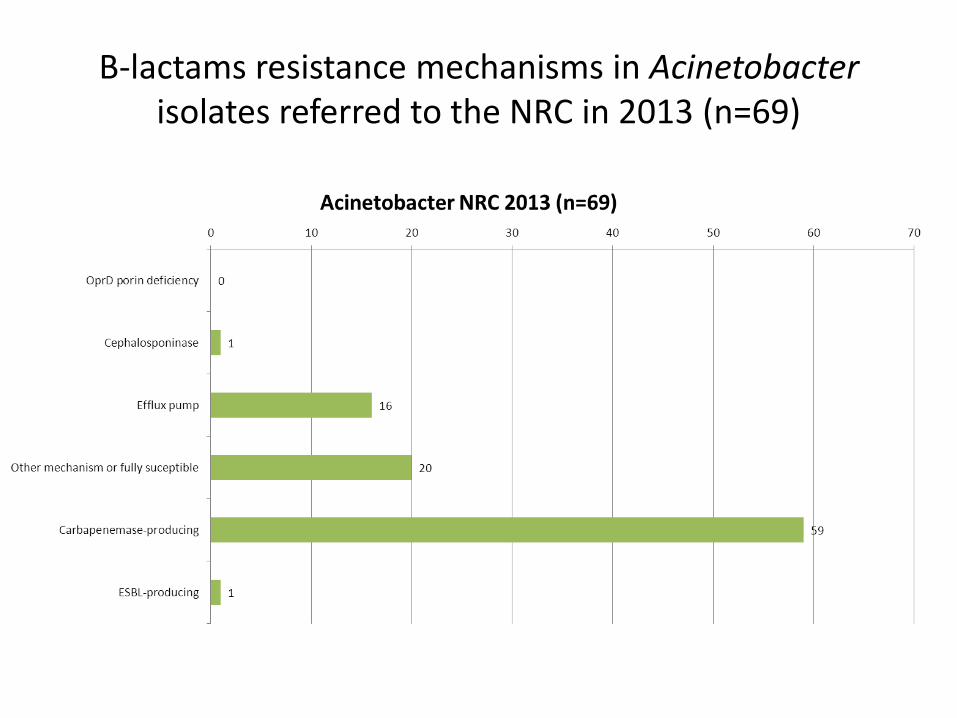
Β-lactams resistance mechanisms in Acinetobacter isolates referred to the NRC in 2013 (n=69)
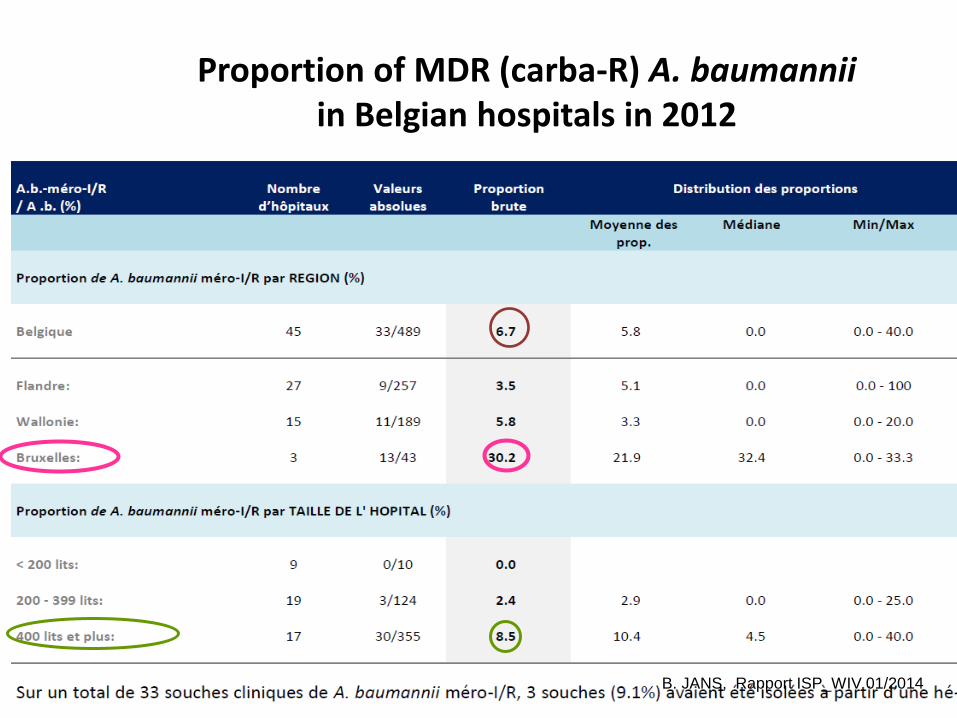
Proportion of MDR (carba-R) A. baumannii in Belgian hospitals in 2012
B. JANS, Rapport ISP_WIV 01/2014
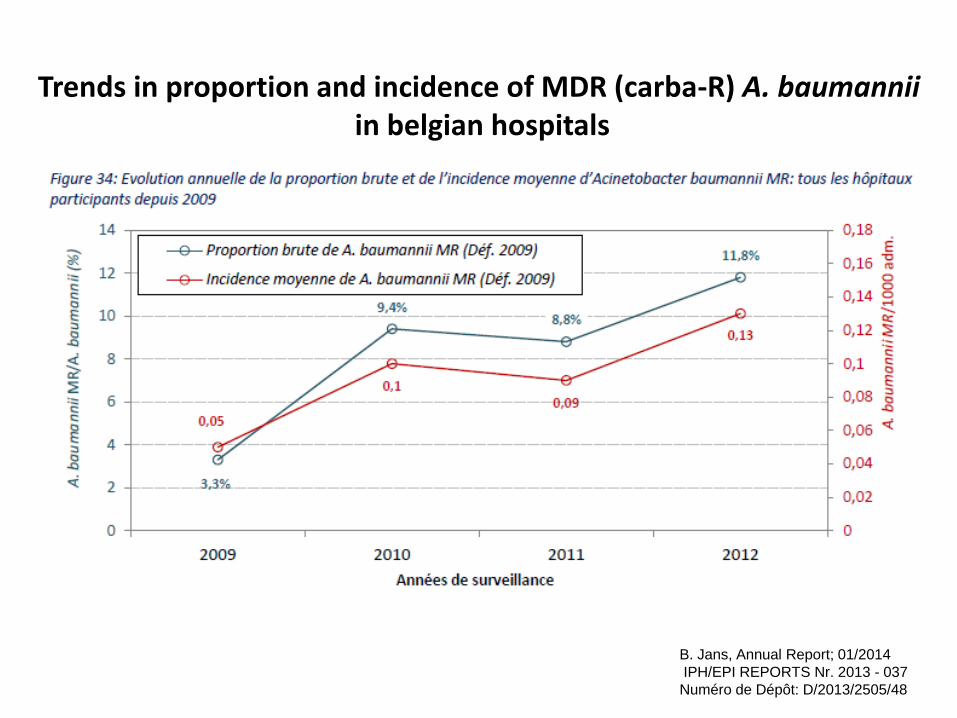
Trends in proportion and incidence of MDR (carba-R) A. baumannii in belgian hospitals
B. Jans, Annual Report; 01/2014
IPH/EPI REPORTS Nr. 2013 - 037
Numéro de Dépôt: D/2013/2505/48
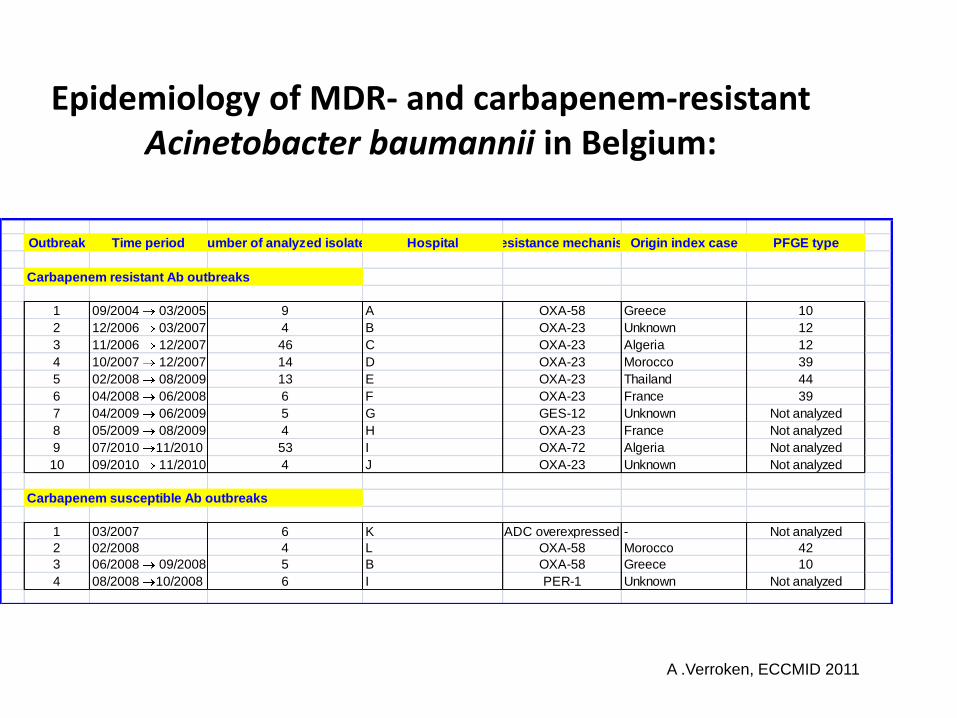
Epidemiology of MDR- and carbapenem-resistant Acinetobacter baumannii in Belgium:
Outbreak Time period Number of analyzed isolates Hospital Resistance mechanismOrigin index case PFGE type
Carbapenem resistant Ab outbreaks
1 09/2004 03/2005 9 A OXA-58 Greece 10
2 12/2006 03/2007 4 B OXA-23 Unknown 12
3 11/2006 12/2007 46 C OXA-23 Algeria 12
4 10/2007 12/2007 14 D OXA-23 Morocco 39
5 02/2008 08/2009 13 E OXA-23 Thailand 44
6 04/2008 06/2008 6 F OXA-23 France 39
7 04/2009 06/2009 5 G GES-12 Unknown Not analyzed
8 05/2009 08/2009 4 H OXA-23 France Not analyzed
9 07/2010 11/2010 53 I OXA-72 Algeria Not analyzed
10 09/2010 11/2010 4 J OXA-23 Unknown Not analyzed
Carbapenem susceptible Ab outbreaks
1 03/2007 6 K ADC overexpressed - Not analyzed
2 02/2008 4 L OXA-58 Morocco 42
3 06/2008 09/2008 5 B OXA-58 Greece 10
4 08/2008 10/2008 6 I PER-1 Unknown Not analyzed
A .Verroken, ECCMID 2011
Dice (Opt:0.50%) (Tol 0.8%-0.8%) (H>0.0% S>0.0%) [6.2%-89.0%]
PFGE Apa 23h (Marq OK)
10
0
90
80
70
60
PFGE Apa 23h (Marq OK)
5.0
0
10.0
0
20.0
0
40.0
0
60.0
070.0
075.0
0
80.0
0
90.0
0
100.0
0
110.0
0
140.0
0
160.0
0
180.0
0
200.0
0
220.0
0
250.0
0
400.0
0
1000
Kb
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
0529-2024
RUH 0875 clone Européen I (19.
GIL1
GIL2
GIL5
GIL6
GIL7
GIL4
GIL3
Ab2004
04-1638
04-2126
04-2263
05-1095
1008240888
40
70004
70006
080604495
070122/0020
050501924
HM1
1022 00430-2
06/0062
90020088747
RUH0134 clone Européen II (19.
282-310261
080602616
080608219
15212398
04/574
5547
19116115
20815672
804-20427996
80420156029
80420251897
80420269777
80420305745
80420306401
90020132454
LUH 05875 clone Européen III
80213182
80217060
80218626
80213336
6301086
HM2
51514
080609271
15345
2008B041
19172 (oxa-23) ( CM7265226)
19174 (oxa-23) ( DG7271622)
19169 (oxa-23) ( GJ7294232)
19175 (oxa-23) ( SML7296631)
19173 (oxa-23) (DA7302849)
19168 (oxa-23) (djo7292673)
19176 (oxa-23) ( DJa7281926)
15518 (414-9659)
2008B051(oxa-23)
2008B053 (oxa-23)
2008B052 (oxa-23)
2008B048 (oxa-23)
2008B049 (oxa-23)
17528
19055
19057
20175
18018
13220
17524
17117
15515
2008B016
2008B040
2008B098
20160
20252
2008B017
15953
15951
2008B096
2008B097
2008B099
2008B058 (oxa-23)
2008B056 (oxa-23)
2008B057 (oxa-23)
2008B055 (oxa-23)
2008B054 (oxa-23)
2008B018
2008B042
2008B023
2008B022
2008B021
2008B024
18021
17525
18020
20257
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
39g
spor ou 12/39 related?
39d
39d
39d
39d
39d
39a
39c
39b
39f
39f
39f
39f
39f
12a
12a
12i
12h
12c
12d
12e
41a
40a
spor
spor
spor
10d
10d
10c
10b
10a
10e
44
44
44
44
44
44
44
44
spor
42a
42a
42a
42a
42b
spor
11a
11b
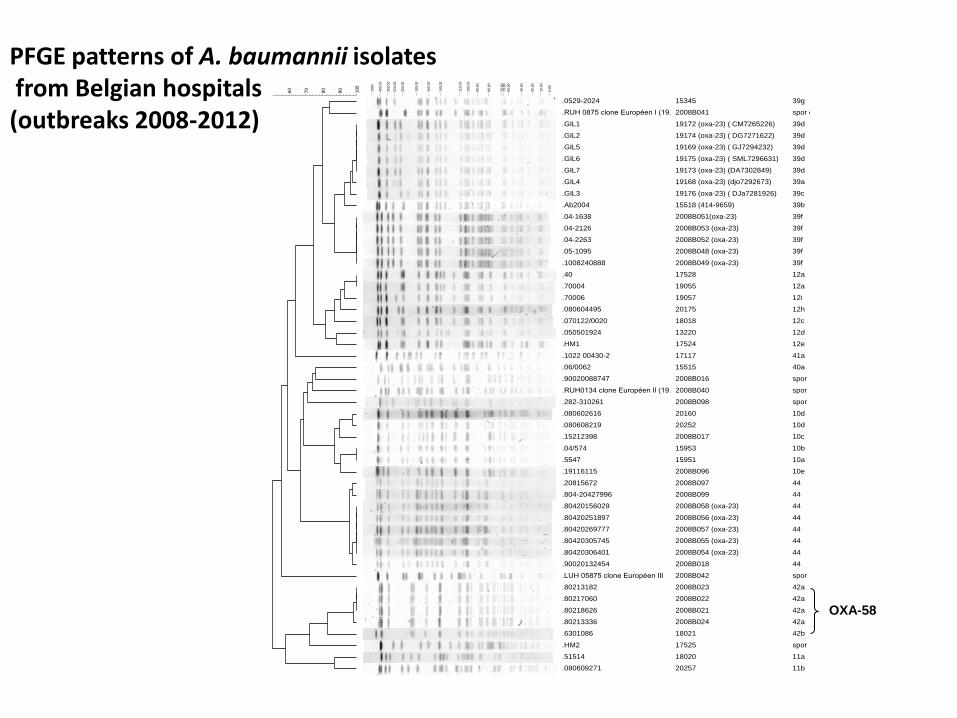
OXA-58
PFGE patterns of A. baumannii isolates from Belgian hospitals (outbreaks 2008-2012)
Summary
- Marked trends towards increased carbapenem resistance and multi-drug resistance in A. baumannii worldwide (Important regional and local geographic variations in prevalence/incidence)
-Outbreaks with different clones (sometimes several clones concomittantly) occurring mostly in critically ill patients in ICU patients
-Pandemic spread of a few number of successful clones (OXA-23 European clones I and II)
-Outbreaks difficult to control (long-term survival in environment, great diversity of reservoirs that are difficult to identify)
-- Reversion of resistance is rare ; most MDR strains remained susceptible to polymyxins, sulbactam and to tetracycline analogues only
- Interpretated reading of antibiotic susceptibility testing in A. baumannii is difficult and molecular testing is necessary for confirmation of mechanisms owing to the lack of phenotypic tests (OXA carbapenemases)













![1. L’opéron lactose - ac-aix-marseille.fr · CROISSANCE BACTÉRIENNE EN PRÉSENCE DE GLUCOSE ET DE LACTOSE log D.O. Croissance bactérienne [bactéries] [ONP] T (h) ... ARN de](https://static.fdocument.org/doc/165x107/5b99088209d3f2fd558d03bf/1-loperon-lactose-ac-aix-croissance-bacterienne-en-presence-de-glucose.jpg)