ELECTROSPUN POLY(ε-CAPROLACTONE) - BASED...
200
ELECTROSPUN POLY(ε-CAPROLACTONE) - BASED NANOCOMPOSITES FOR OSTEOPOROTIC BONE DEFECT REPAIR REMYA K.R. Ph.D. THESIS 2017 SREE CHITRA TIRUNAL INSTITUTE FOR MEDICAL SCIENCES AND TECHNOLOGY, THIRUVANANTHAPURAM INDIA
Transcript of ELECTROSPUN POLY(ε-CAPROLACTONE) - BASED...

ELECTROSPUN POLY(ε-CAPROLACTONE) - BASED
NANOCOMPOSITES FOR OSTEOPOROTIC
BONE DEFECT REPAIR
REMYA K.R.
Ph.D. THESIS
2017
SREE CHITRA TIRUNAL INSTITUTE FOR
MEDICAL SCIENCES AND TECHNOLOGY, THIRUVANANTHAPURAM
INDIA

ELECTROSPUN POLY(ε-CAPROLACTONE) - BASED
NANOCOMPOSITES FOR OSTEOPOROTIC
BONE DEFECT REPAIR
A THESIS PRESENTED BY
REMYA K.R.
TO
SREE CHITRA TIRUNAL INSTITUTE
FOR MEDICAL SCIENCES AND TECHNOLOGY,
THIRUVANANTHAPURAM
INDIA
IN PARTIAL FULFILMENT OF THE REQUIREMENTS
FOR THE AWARD OF
DOCTOR OF PHILOSOPHY
2017

i
CERTIFICATE
I, Remya K.R., hereby certify that I had personally carried out the work depicted
in the thesis entitled, “Electrospun Poly(ε-caprolactone) - based
nanocomposites for osteoporotic bone defect repair”, except where due
acknowledgement has been made in the text. No part of the thesis has been
submitted for the award of any other degree or diploma prior to this date.
Thiruvananthapuram REMYA K.R.
Reg.No: 2011/PhD/04

ii
SREE CHITRA TIRUNAL INSTITUTE FOR MEDICAL SCIENCES & TECHNOLOGY BIOMEDICAL TECHNOLOGY WING, POOJAPPURA
THIRUVANANTHAPURAM – 695011, INDIA (An Institute of National Importance under Govt. of India)
Phone-(91)0471-2520221 Fax-(91)0471-2341814 www.sctimst.ac.in
Dr. P. Ramesh
Scientist G & In-charge (joint)
Division of Polymeric Medical Devices
Department of Medical Devices Engineering
BMT Wing, SCTIMST
email: [email protected]
This is to certify that Ms. Remya K.R., Division of Polymeric Medical Devices,
Department of Medical Devices Engineering, of this Institute has fulfilled the
requirements prescribed for the Ph. D. degree of Sree Chitra Tirunal Institute for
Medical Sciences and Technology, Thiruvananthapuram. The thesis entitled,
“Electrospun Poly(ε-caprolactone) – based nanocomposites for osteoporotic
bone defect repair”, was carried out under my direct supervision. No part of the
thesis was submitted for the award of any degree or diploma prior to this date.
Thiruvananthapuram Dr. P. Ramesh
(Research Supervisor)

iii
The thesis entitled
ELECTROSPUN POLY(ε-CAPROLACTONE) - BASED
NANOCOMPOSITES FOR OSTEOPOROTIC
BONE DEFECT REPAIR
Submitted by
Remya K.R.
for the degree of
Doctor of Philosophy
of
SREE CHITRA TIRUNAL INSTITUTE
FOR
MEDICAL SCIENCES AND TECHNOLOGY, TRIVANDRUM
Is evaluated and approved by
……………………………. ……………………….. Dr. P. Ramesh
(Research Supervisor) Examiner

iv
Dedicated to
GOD ALMIGHTY & MY FAMILY

v
A C K N O W L E D G E M E N T S It is with a deep sense of gratitude, satisfaction and with the divine blessings of Supreme God Almighty that I submit this dissertation. I take this opportunity with much pleasure to acknowledge all those who have contributed in many ways for the success of this study.
First and foremost I express my sincere gratitude and respect to my Guide Dr. P. Ramesh, Scientist G, Division of Polymeric Medical Devices, SCTIMST for his continuous advice and encouragement throughout the course of my study. He was always accessible and took significant effort for the successful completion of this endeavour.
I am grateful to Dr. Asha Kishore, Director of SCTIMST, former Director, former Head and present Head of BMT Wing, Dr. H. K. Varma for all support provided during the course of my work. I am thankful to the Dean Dr. V. Kalliyana Krishnan, Associate Dean Dr. Roy Joseph, Deputy Registrar Dr. Santosh Kumar B and all former and present members of academic division for their assistance.
I thank members of Doctoral Advisory Committee, Dr. Annie John, Scientist G, Transmission electron microscope and Dr. Roy Joseph, Scientist G, Division of Polymeric Medical Devices, for their timely suggestions, ideas and comments which helped in the improvement of the quality of this work. I express my heartfelt thanks to Dr. Annie John for her sincere help and efforts taken for drafting and revising my publication.
I am extremely thankful to Dr. Annie John, Scientist G, Transmission electron microscope for granting me the permission to use some of their lab facilities. I extend my special appreciation to Dr. Sunitha Chandran for in vitro cell cuture experiments, for being with me, helping me in analyzing my data and training me on PMMA embedding, polishing, staining and imaging. I also extent my special thanks to Ms. Susan Mani for my initial cell culture experiments. .
I express my sincere gratitude to Dr. V.S. Harikrishnan for performing in vivo surgery on rat animal model and Mr. Manoj, Mr. Anoop, Mr. Sarath, Ms Sreeja, Mr.Sunil & all staff of DLAS for timely help, support and friendship.
I thank Dr. H. K. Varma, Dr Suresh Kumar for providing nHAP for my study and Mr. Nishad Mr. Sreekumar, Mr.Sanoj and all members of Bioceramics Laboratory who helped me in ESEM and SEM analysis. I thank Dr Anil Kumar P.R, Mr Vinod, Ms Deepa for their timely help and support during my in vitro experiments. I express my heartfelt gratitude all members of Histopathology Laboratory for valuable suggestions on sample preparation for histological analysis.

vi
I would like to acknowledge Dr. K. Sreenivasan, Dr. C. Radhakumary, Mr. Rowsen Moses and Mr. Hari of Laboratory for Polymer Analysis for ATR-FTIR, DSC, TGA and GPC analysis; Dr. V. Kalliyana Krishnan, Ms. Lakshmi, Mr. Satheesh and Dr. Priya of Dental Products Laboratory for Micro CT and ATR-FTIR analysis; Dr. Prabha D Nair, Ms. Geetha, Ms. Nimmy, Mr. Dhanesh and staff, Division of Tissue Engineering & Regenerative Technology for contact angle and conductivity measurements.
I also acknowledge Er.V Ramesh Babu, Mr. Subash and Staffs of Precision Fabrication Facility for developing punches for cutting the scaffolds.
I express my sincere gratitude to Dr. M. C. Sunny for his guidance, support and encouragement during the course of my tenure. I am extremely thankful to my dear friends in the campus for their help and whole-hearted cooperation during the study. I thank Dr. Mayuri, Dr. Priya, Dr. Arjun, Dr. Kiran, Dr. Sudhin, Mr. Susanth, Ms. Vibha, Dr. Shanti, Ms. Rakhi, Dr. Rethikala, Dr. Soumya Columbus , Mr. Harilal, Ms. Dhanya C. S., Ms. Jincy, Ms. Darsana, Ms. Sreelakshmi, Dr. Parvathy, Dr. Anupama, Ms. Nayana, Ms. Reshmi, Mr. Arungovil, Dr. Titash, Ms. Soorya, Mr. Sreeraj, Mr. Athiyappan, Mr. Sarath, Ms. Anitha, Ms. Anuja, Mr. Krishnachandran, Ms. Deepthi, Mr. Berwin Singh, Mr. Syam, Ms. Dhanya Thyagarajan, Mr. Arunkumar, Dr. Praveen, Mr. Riju, Mr.Kumaran, Mr. Sreevisakh, Ms. Lakshmi, Dr.Vidhu, Mr. Dhanesh, Dr. Finosh Ms. Christina and Ms. Sini for their friendship which relieved my stresses and made those days memorable.
I am extremely grateful to all my teachers within the campus who were involved in my PhD course work. Co-operation from staff of various administrative departments and library of the Institute is fondly remembered.
I wish to acknowledge Sree Chitra Tirunal Institute for Medical Sciences & Technology, India for providing me prestigious SCTIMST Institute fellowship during the course of study.
I have no words to express gratitude to my family members who provided the most precious support. I am indebted to my parents and my sister, for their unconditional love, support, encouragement and prayers.
God almighty, I bow before you for providing me strength, courage and health for completing this work and for being with me in all my good and hard times.
Remya K.R.

vii
TABLE OF CONTENTS
Page
No.
DECLARATION BY THE STUDENT……………………...…………….. I
CERTIFICATE OF GUIDE …………………………………………......... Ii
APPROVAL OF THESIS ………………………………………………….. Iii
ACKNOWLEDGEMENTS …………………………………………......... V
TABLE OF CONTENTS …………………………………………………... Vii
LIST OF FIGURES ………………………………………………………... Xv
LIST OF TABLES ……………………………………………………......... Xix
ABBREVIATIONS ………………………………………………………… Xx
SYNOPSIS ………………………………………………………………….. Xxi
CHAPTER 1 – INTRODUCTION ………………………………………... 1
1.1. Bone ……………………………………………..…………………….. 3
1.1.1. Bone macrostructure ………………………………..…………... 3
1.1.2. Bone matrix …………………………………………….………. 4
1.1.3. Bone cells ………………………………………………….….... 5
1.2. Bone remodelling ………..…………………………………………….. 5
1.3. Osteoporosis: A look into the problem ….…………………………….. 6
1.4. Osteoporosis epidemics in India ………………..……………………... 8
1.5. Pathogenesis of osteoporosis ……………………..……………………. 9
1.6. Treatment modalities for osteoporosis ……..………………………….. 10
1.7. Challenges in osteoporotic fracture treatment ……………..…………... 11
1.8. Tissue engineering approach in osteoporosis …………..…………….... 12
1.8.1 Scaffold requirements significant for bone tissue engineering ..... 13
1.8.2 Biodegradable polymers and polymer-ceramic composite as scaffolds …………………………………………………..…… 13

viii
1.8.3 Relevance of electrospinning for scaffolds fabrication ……….... 14
1.8.4 Cell requirements significant for bone tissue engineering ……... 15
1.8.5 Growth factors/bioactive drugs used in bone tissue engineering.. 16
1.9. Role of bisphosphonates in osteoporosis treatment …………………… 17
1.10. Need for animal models in osteoporosis research …………………….. 18
1.11. Rationale for choosing Poly (ε caprolactone),Nanohydroxyapatite &
Pamidronate for the study ……………………………………………... 19
1.11.1. Poly (ε-caprolactone)(PCL) …………………………………… 19
1.11.2. Significance of Nanohydroxyapatite (nHAP) …………...…….. 20
1.11.3. Role of Pamidronate (PDS) ………………………….………... 21
1.11.4. Rat as osteoporotic animal model ……………………………... 22
1.12 Hypothesis …………………………………………………………….. 22
1.13 Objectives of the study ………………………………………………... 23
CHAPTER 2 – LITERATURE REVIEW ………………………………... 25
2.1. Bone grafts: History and current status prevention …………………..... 25
2.1.1. Autografts ……...………………...…………….…………......... 27
2.1.2. Allografts …....………...………………………....…………….. 27
2.1.3. Synthetic grafts ……………………………….…………........... 28
2.1.3.1. Metals ………………………………………………… 28
2.1.3.2. Ceramics ……………………………………………... 30
2.1.3.3. Polymers ……………………………………………... 31
2.1.3.4. Polymer nanocomposites as bone grafts ……………... 32
2.2. Role of tissue engineering in treating osteoporotic bone fractures ……. 32
2.3. Scaffold fabrication techniques in tissue engineering ….……...…...….. 33
2.3.1. Electrospinning …………………………………........................ 34
2.4. Role of polycaprolactone as scaffolds in tissue regeneration …………. 35
2.5. Controlled release of bisphosphonates from polymeric scaffolds …….. 38
2.6. Studies based on pamidronate for bone tissue regeneration …………... 40
2.7. In vivo studies on rat animal model …………………………………… 42

ix
CHAPTER 3 - MATERIALS AND METHODS …………………………. 44
3.1 Synthesis of poly(ε-caprolactone) –polyethyleneglycol - poly(ε- caprolactone) copolymer (CEC) ………………………………………
45
3.1.1 Commercial reagents for copolymer synthesis ………………..... 45
3.1.2 Synthesis of CEC ………………………...................................... 45
3.2 Development of PCL based scaffolds with improved hydrophilicity, biodegradability and better cell viability ………………………………
45
3.2.1 Materials used for scaffold fabrication ………………………..... 45
3.2.1.1 Fabrication of scaffolds by electrospinning technique …. 46
3.2.2 Development of pamidronate incorporated PCL based scaffolds.. 47
3.2.2.1 Materials used and scaffold composition ……................ 47
3.2.2.2 Fabrication of PDS incorporated PCL based scaffolds… 48
3.3. Characterization of copolymer and scaffolds …………………………. 49
3.3.1. Characterization of copolymer CEC …………...……………….. 49
3.3.1.1. Fourier transform infra red spectrophotometer (FTIR) spectra ………………….…………………………….…
49
3.3.1.2. 1H- Nuclear Magnetic Resonance spectra (NMR) …...... 49
3.3.1.3. Gel permeation chromatography analysis …………….. 49
3.3.2. Characterization of nanohydroxyapatite (nHAP) …………….… 50
3.3.2.1. Particle size analysis …………………………………… 50
3.3.2.2. TEM Analysis ………………………………………….. 50
3.3.3. Characterization of pamidronate (PDS) ……………………….... 50
3.3.3.1. FTIR spectra …………………………………………..… 50
3.3.3.2. Particle size analysis …………………………….............. 50
3.3.4. Characterization of Electrospun scaffolds ………………………. 51
3.3.4.1. Scanning Electron Microscopy (SEM) ………………… 51
3.3.4.2. Microcomputed Tomography (µ-CT) Analysis ……..….. 51
3.3.4.3. Porosity analysis by liquid intrusion …………..………... 51

x
3.3.4.4. Surface wettability ……………………………………..... 52
3.3.4.4.1. Static Contact Angle Measurements ………... 52
3.3.4.4.2. Dynamic contact angle measurements ……… 52
3.3.4.5. Static mechanical properties …………………………...... 52
3.3.4.6. Dynamic mechanical properties using DMA ………….... 53
3.3.4.7. In-vitro release studies in PBS ………………………….. 53
3.3.4.8. In Vitro Hydrolytic Degradation Studies ……………….. 53
3.3.4.8.1. Mechanical property evaluation using UTM… 53
3.3.4.8.2. Morphology evaluation by ESEM analysis…. 54
3.4. In vitro studies ……..……………………...………………………….. 54
3.4.1. Ethical statement …………………………….………………… 54
3.4.2. Sterilization of scaffolds ………………………………………. 54
3.4.3. In vitro cytocompatibility evaluation using L929 cell line…….. 54
3.4.3.1. MTT assay …………………………………………… 54
3.4.4. In vitro cell culture studies using human osteosarcoma (hOS) cell lines ………………………………………………………..
55
3.4.4.1. Live/dead assay ……………………………………… 55
3.4.4.2. MTT assay …………………………………………….. 55
3.4.5. In-vitro cell culture studies using rabbit adipose derived
mesenchymal stem cells (RADMSCs) ………………………... 56
3.4.5.1. Cell Adhesion…………………………………...…..…. 56
3.4.5.2. Live/dead assay………………………………........…… 56
3.4.5.3. Alkaline Phosphatase assay (ALP activity) ……............ 57
3.4.5.4. LDH assay …………………………………………….. 57
3.4.5.5. Picogreen assay ……………………………………….. 57
3.4.6. In-vitro cell culture studies using rats adipose derived
mesenchymal stem cells(rADMSC) …………………………….. 58 3.4.6.1. MTT Assay - un induced rADMSCs ………………….. 58

xi
3.4.6.2. Cell adhesion - un induced rADMSCs ………………... 58
3.4.6.3. Live/dead assay-un induced rADMSCs ………………. 58
3.4.6.4. Cell adhesion - osteogenic induced rADMSCs ……….. 58
3.5. In vivo studies in rat animal model . …………………………………... 58
3.5.1. Development of osteoporotic rat animal model ……………..….. 59
3.5.1.1. Surgical procedure ………………………………………. 59
3.5.2. Evaluation of rat osteoporotic model …………………………..... 61
3.5.2.1. Histology of excised ovarian tissue - Haematoxylin & Eosin staining ……………………....…………....…….. 61
3.5.2.2. Micro Computed Tomography analysis-Assessment of
trabecular bone loss …………....…………..................... 62
3.5.2.3. Weight monitoring before and after model induction….. 62
3.5.2.4. Biochemical analysis of blood serum- Ca, P and ALP
assay ………………….…………....………….................. 63
3.5.3. Development of calvarial defect and scaffold implantation……... 64
3.5.3.1. Surgical procedure …………....…………...………….... 64
3.5.4. Osteogenic efficacy assessment of scaffolds in osteoporotic rat
animal model …………....…………....…………....…………..... 65
3.5.4.1. Gross evaluation of explants …………....…………......... 66
3.5.4.2. Radiographic evaluation …………....…………................ 66
3.5.4.3. Micro CT evaluation …………………………………… 66
3.5.4.4. Histological evaluation–PMMA embedding and
staining …….…………....…………....…………........... 66
3.5.4.5. Histomorphometry analysis - QWin software …………. 67
3.6. Statistical Analysis …………....…………....…………....…………...... 68
CHAPTER 4 – RESULTS …………....…………....…………..................... 69
4.1. Material Characterization …………....…………....…………............. 69
4.1.1. Synthesis & characterization of PCL-PEG-PCL triblock
copolymer (CEC) …………....………….................................... 69

xii
4.1.1.1. Synthesis of CEC …………...…………....………….. 69
4.1.1.2. Fourier transform infrared spectroscopy …………...... 70
4.1.1.3. 1H- Nuclear Magnetic Resonance spectroscopy …….. 71
4.1.1.4. GPC analysis …………....…………....…………........ 72
4.1.2. Characterization of nHAP …………....…………....……...….... 72
4.1.2.1. Particle size analysis …………....…………................. 72
4.1.2.2. TEM analysis …………....…………....…………........ 73
4.1.3. Characterization of PDS …………....…………....…………....... 74
4.1.3.1. Fourier transform infrared spectroscopy …………....... 74
4.1.3.2. Particle size analysis ……......…………....…………... 74
4.2. Development of biodegradable and bioactive scaffolds based on PCL
with improved hydrophilicity, biodegradability and better cell
viability ....…………....…… ....…………....…… ....………….....… 75
4.2.1. SEM analysis ....…………....…… ....…………....……...…… 75
4.2.2. Micro CT analysis ....…………....…… ....…………....……... 77
4.2.3. Contact Angle Measurements ....…………....…… ....………. 79
4.2.4. Static mechanical properties of scaffolds ....…………....……. 80
4.2.5. Dynamic mechanical properties of scaffolds ....…………...… 81
4.2.6. In Vitro Hydrolytic Degradation Studies ....…………....….… 83
4.2.7. Cytotoxicity Test: MTT Assay ....…………....……………… 84
4.2.8. Cell Attachment Studies ....…………....…… ....………….... 85
4.2.9. Live/Dead Assay ....…………....………..…………....……... 86
4.2.10. LDH Assay ....…………....…………….....…………....…… 87
4.2.11. Picogreen assay ....………….................…………....……… 88
4.2.12. Alkaline Phosphatase (ALP) activity of scaffolds …………... 89
4.3. Development and characterization of pamidronate (PDS)
incorporated PCL based scaffolds .......…………....….........………… 90

xiii
4.3.1. Environmental scanning electron microscopy (ESEM)
analysis .......…………....………....………………..……....… 90
4.3.2. Porosity evaluation using liquid intrusion method ………….. 93
4.3.3. Surface wetting property by contact angle measurements …... 94
4.3.4. Static mechanical properties using UTM ……....……………. 95
4.3.5. Dynamic mechanical properties using DMA ……....……....... 96
4.3.6. In-vitro release studies of PDS ……....………………………. 101
4.3.7. In vitro degradation studies in PBS ……....………………….. 104
4.3.8. In-vitro cell culture studies using human osteosarcoma (hOS)
cell lines ……....…………..……....………....……………….. 107
4.3.8.1. Live/dead assay …..……....………....……………….. 107
4.3.8.2. MTT assay …..……....………....…………………….. 108
4.3.9. In vitro cell culture studies rats adipose derived mesenchymal
stem cells (rADMSC) …..……....………....…………………. 111
4.3.9.1. MTT assay …..……....………....…………………….. 112
4.3.9.2. Live/dead assay ………....…………………………… 113
4.3.9.3. Cell adhesion …....…………………………………… 114
4.4. In vivo studies in rat animal model …....……………………………... 115
4.4.1. Establishment of rat osteoporotic model …....………………. 116
4.4.1.1. Histological evaluation of excised tissue using H & E
staining …....…………………………………………… 116
4.4.1.2. Evaluation of trabecular bone loss using micro CT
analysis …....…………………………………………… 116
4.4.1.3. Biochemical analysis of blood serum ………………... 118
4.4.1.4. Body weight …....……………………………………. 120
4.4.2. In vivo bone formation evaluation …....……………………… 121
4.4.2.1. Gross evaluation of explants ………………………… 121
4.4.2.2. Radiographic evaluation ……………………………... 122
4.4.2.3. Micro CT evaluation ………………………………… 123

xiv
4.4.2.4. Histology analysis …………………………………... 126
4.4.2.5. Histomorphometry …………………………………... 128
CHAPTER 5 – DISCUSSION …………………………………………….. 130
5.1. Development of biodegradable and bioactive scaffolds based on
PCL with improved hydrophilicity, biodegradability and better cell
viability ……………………………………………………………. 130
5.2. Development of pamidronate incorporated PCL based scaffolds …... 139
5.3. In vivo evaluation of PDS incorporated PCL based scaffold in a rat
animal model ……………………………………………………….. 145
5.4. Limitation of the study..........................................................................
5.5. Future perspective.................................................................................
150
150
CHAPTER 6 - SUMMARY AND CONCLUSION …………..................... 151
BIBLIOGRAPHY…………………………………………………………... 156
LIST OF PUBLICATIONS ……………………………….……………….. 169
CURRICULAM VITAE ...……………………………………..................... 171
APPENDIX ...……………………………………………………………….. 173

xv
LIST OF FIGURES
Figure
No Caption
Page
No
1. Morphological features of normal and osteoporotic bone………... 7
2. Structure of pyrophosphate and bisphosphonate ............................ 17
3. Structure of PCL……………………………………………….…. 19
4. Structure of pamidronate…………………………………….…… 21
5. Electrospinning setup for scaffold fabrication…………………… 47
6. Surgical procedure for rat ovariectomy……………………….….. 60
7. Surgical procedure for calvarial defect and implantation………... 65
8. Schematic representation of copolymer synthesis………............... 70
9. FTIR spectra of copolymer CEC……….....................................… 70
10. 1HNMR spectra of copolymer CEC………... ……….....………... 71
11. GPC analysis of copolymer CEC ...……………………………… 72
12. Particle size distribution of nHAP …….......................................... 73
13. TEM image of nHAP...................................................................... 73
14. FTIR spectra of PDS ……………………………..……..……...... 74
15. Particle size distribution of PDS ………………………..……..… 75
16. SEM micrograph showing fibrous morphology of (a) PCL (b)
PCL/CEC (c) PCL/nHAP and (d) PCL/CEC/nHAP……..………. 76
17. Average fiber diameter of scaffolds………... ………... ……….... 77
18. Micro CT analysis showing 3D morphometry of scaffolds (a)
PCL (b) PCL/CEC (c) PCL/nHAP and (d) PCL/CEC/nHAP …… 78

xvi
19. Pore size distribution of PCL, PCL/CEC, PCL/nHAP and
PCL/CEC/nHAP scaffolds……………………………………….. 79
20. Contact angle measurements of PCL and PCL/nHAP…………… 80
21. DMA analysis showing variation of storage modulus of scaffolds
with temperature …………………………………………………. 82
22. DMA analysis showing variation of tan delta of scaffolds with
temperature.……………................................................................. 82
23. Effect of PBS ageing on morphology of scaffolds after 90 days… 83
24. Effect of PBS ageing on tensile strength of scaffolds... …………. 84
25. MTT assay on scaffolds………………………………………….. 85
26. ESEM analysis showing adhesion of RADMSCs on scaffolds….. 86
27. Live/ dead assay on scaffolds…………………………………… . 87
28. LDH assay on scaffolds………………………………………….. 88
29. Picogreen assay on scaffolds …………………………………….. 88
30. ALP activity of scaffolds... ……………………………………… 89
31. ESEM analysis showing morphology of PDS incorporated
scaffolds (magnification: 4000x, scale bar = 10µm) ………..…… 91
32. Contact angle of PCL and PCL-PDS scaffolds ……………….…. 95
33. DMA analysis showing variation of storage modulus of PCL and
PCL-PDS scaffolds with temperature ……………………...……. 97
34. DMA analysis showing variation of tan delta of PCL and PCL-
PDS scaffolds with temperature ……………………………......... 97
35. DMA analysis showing variation of storage modulus of
PCL/CEC and PCL/CEC-PDS scaffolds with temperature……… 99
36. DMA analysis showing variation of tan delta of PCL/CEC and
PCL/CEC-PDS scaffolds with temperature……………………… 99

xvii
37. DMA analysis showing variation of storage modulus of PCL/CEC/nHAP and PCL/CEC/nHAP-PDS scaffolds with temperature………………………………………………..……… 100
38. DMA analysis showing variation of tan delta of PCL/CEC/nHAP
and PCL/CEC/nHAP-PDS scaffolds with temperature…………... 101
39. In-vitro release studies of PDS from PCL scaffolds……………... 102
40. In vitro release studies of PDS from PCL/CEC blend scaffolds…. 103
41. In vitro release studies of PDS from PCL/CEC/nHAP composite
scaffolds…………………………………………………….…….. 103
42. ESEM images showing fiber rupture after 3 months of PBS
aging................................................................................................ 104
43. Tensile strength of PCL-PDS scaffolds after 3 months of PBS
ageing…………………………………………………………..… 105
44. Tensile strength of PCL/CEC-PDS scaffolds after 3 months of
PBS ageing……………………………………………………….. 106
45. Tensile strength of PCL/CEC/nHAP-PDS scaffolds after 3
months of PBS ageing………………………………….………… 106
46. FDA/PI staining after 48h showing viability of hOS cells on
scaffolds (scale bar = 100µm) …………………………………… 107
47. MTT assay using hOS cells on PCL & PCL-PDS
scaffolds……...............................................................................… 109
48. MTT assay scaffolds using hOS cells on PCL/CEC & PCL/CEC-
PDS scaffolds…………………………………………………….. 110
49. MTT assay using hOS cells on PCL/CEC/nHAP &
PCL/CEC/nHAP-PDS scaffolds………………………………… 111
50. MTT assay using un-induced rADMSCs on PCL/CEC/nHAP-
PDS PCL/CEC/nHAP-PDS scaffolds………….………………… 112
51. Actin staining showing adhesion and morphology of rADMSCs
on scaffolds (scale bar = 10µm) ………………….……………… 113

xviii
52. ESEM analyis showing adhesion of un induced rADMSCs on
scaffolds scale bar = 20µm) ………………………..…………… 114
53. ESEM analyis showing formation of mineralized nodules by osteeogenic induced rADMSCs on on scaffolds surface scale bar = 40µm……………………………………………………………
115
54. H & E staining of rat ovary (scale bar 100µm) ………………….. 116
55. 2D slice from micro CT showing trabecular bone loss…………... 117
56. Biochemical analysis of serum for calcium……………………… 119
57. Biochemical analysis of serum for phosphorus…………………... 119
58. Biochemical analysis of serum for ALP activity…………….…… 120
59. Weight gain in osteoporotic rats………………………………..… 121
60. Gross morphology of explants…………………………………… 122
61. Radiographic analysis of explants………………………….…..… 123
62. Micro CT analysis of explants……………………………….…… 124
63. Density of new bone at the defect area of test group measured
using micro CT…………………………………………………… 125
64. Density of new bone at the defect area of control group measured
using micro CT…………………………………………………… 126
65. Histological analysis of control group…………………….……… 127
66. Histological analysis of test group………………………………. 128
67. Histomorphometrical analysis showing regeneration ratio of test and control group at different time period…..……………………. 129

xix
LIST OF TABLES
Figure
No Caption Page No
1. Bisphosphonate incorporated polymeric membranes................... 40
2. Scaffold composition used for the study………………………... 47
3. Scaffold composition of PDS incorporated PCL scaffolds........... 48
4. Scaffold composition of PDS incorporated PCL/CEC scaffolds.. 48
5. Scaffold composition of PDS incorporated PCL/CEC/nHAP
scaffolds........................................................................................ 49
6. Conductivity & average fiber diameter of scaffolds……………. 75
7. Static mechanical properties of scaffolds.………………………. 81
8. Conductivity of spinning dopes and average fiber diameter of
scaffolds.. ………………………………………………………. 92
9. Porosity of scaffolds determine using liquid intrusion method… 94
10. Static mechanical properties of scaffolds……………………….. 96
11. Trabecular bone parameters measured from micro CT………… 117

xx
ABBREVIATIONS
ADMSC Adipose derived mesenchymal stem cells
ALD Alendronate disodium pentahydrate ASC Adult stem cells BMD bone mineral density BMPs bone morphogenetic proteins BPs Bishosphonates CEC poly(ε-caprolactone) –polyethyleneglycol -
poly(ε-caprolactone) copolymer cLSM confocal laser scanning electron microscope ECM extracellular matrix ESC Embryonic stem cells
ESEM Environmental scanning electron microscopy
FTIR Fourier Transform Infrared Spectroscopy FDA Food and Drug Administration FGF fibroblast growth factors GPC Gel permeation chromatography HA hyaluronic acid
ICMR Indian Council for Medical Research IOF International Osteoporosis Foundation
IGF I/II insulin growth factor I and II MSC mesenchymal stem cells µ-CT Micro CT nHAP nanohydroxyapatite NBF neutral buffered formalin OVX ovariectomised PGA poly(glycolic acid) PLA poly(lactic acid)
PLGA poly(lactic-co-glycolic acid) PCL poly(ɛ-caprolactone) PEG Polyethylene glycol PDS pamidronate disodium pentahydrate

xxi
SYNOPSIS
Bone could be considered as a ‘smart tissue’ having an intrinsic capacity to
heal and regenerate even without leaving a scar. Even though bone being strong, it
often undergoes defects or damages resulting either from traumatic situations or from
pathological conditions. Osteoporosis is one of the most prevalent metabolic bone
disorders which is characterized by low bone mineral density, reduced bone mass,
and poor bone strength leading to skeletal fragility and increased susceptibility to
fractures. As per worldwide statistics of International Osteoporosis Foundation,
osteoporosis causes more than 8.9 million fractures annually, resulting in an
osteoporotic fracture in every 3 seconds.
The major clinical consequence of osteoporosis is fracture and the current
clinical treatment modalities include the use of either surgical interventions such as
autografts/allografts/ bone grafts based on biomaterials or the use of pharmacological
agents such as antiresorptive /anabolic agents. The limitations of surgical
interventions include limited availability of donor tissue, donor site morbidity, risk of
infection, immune rejection, long term hospitalization etc and that of pharmaceutical
agents is their poor bioavailability and undesired toxic side effects.
There are only a few reports available on antiresorptive agents incorporated
biomaterial scaffolds used for osteoporotic defect regeneration. However, developing
scaffolds with appropriate combination of mechanical support and morphological
guidance for cell proliferation and attachment while at the same time serving as
matrices for sustained delivery of pharmaceutical agent is a major challenge.

xxii
Poly(ε-caprolactone) (PCL) is one of the widely explored polymers in
biomedical field as scaffolding material for bone regeneration application owing to
its inherent properties such as biodegradability and biocompatibility. One major
drawback of PCL which limit its use as a functional scaffold is its hydrophobic
nature which is unfavourable for better cellular response. Hence strategies to
improve the hydrophilicity of PCL scaffolds are essential.
Hypotheses put forward on the basis of current knowledge are:
(1) Incorporation of a hydrophilic polymer to PCL can modify its surface wetting
property, improve its biodegradability and provide better cellular response
(2) Nanohydroxyapatite (nHAP) incorporation can improve the mechanical
properties and the osteogenic potential of PCL based scaffolds
(3) Incorporation of pamidronate disodium pentahydrate (PDS), an antiresorptive
agent used for osteoporotic treatment, in PCL based scaffolds can improve the
biofunctionality of the scaffolds and can be used for osteoporotic fracture repair
In order to prove the hypotheses, a 5-pronged approach was employed which
includes:
Synthesizing a hydrophilic copolymer based on ε-caprolactone and
polyethylene glycol (CEC)
Fabricating scaffolds based on PCL and its blend with CEC filled with and
without nHAP particles using electrospinning technique
Physical and biological characterization of scaffolds to prove its usefulness in
orthopaedic application
Fabricating PDS incorporated PCL based scaffolds and evaluating the effect
of PDS on physical and biological properties of PCL

xxiii
In-vivo osteogenic efficacy evaluation of PDS incorporated scaffolds in a rat
calvarial osteoporotic model
The work is presented in six chapters. The chapter 1 begins with an
introduction to bone, followed by detailing about osteoporosis, its pathophysiology,
current treatment modalities and challenges. It also briefly introduces the
requirements for an ideal scaffolding material and relevance of electrospinning for
scaffold fabrication. Properties of biodegradable polymer employed as scaffolding
material, antiresorptive agents used and animal models employed for osteoporosis
treatment are also described.
In Chapter 2, an exhaustive literature review highlights the current status of
bone grafts used for orthopaedic applications. The topics reviewed include history of
bone grafts, various scaffold fabrication strategies, osteoporotic drug incorporated
scaffolds and electrospun polymeric scaffolds as bone regeneration scaffolds.
Review also summarises about the animal models used for osteoporotic fracture
treatments.
In Chapter 3, the experimental design in order to achieve the proposed
objectives of the study is presented. This includes detailed description of the
materials employed, experimental protocols, instruments utilized and development of
rat animal model. The chapter is classified into different sections. The section 1
discusses in detail the procedure for synthesis of copolymer CEC, fabrication of
scaffolds by electrospinning and modification of PCL scaffolds with copolymer CEC
as well as nHAP incorporation. The fabrication of PDS incorporated PCL based
scaffolds is detailed in section 2. The physico-chemical characterization of
synthesized copolymer CEC and the fabricated scaffolds is explained in Section 3.

xxiv
The details of biological evaluation of fabricated scaffolds under in vitro conditions
using L929 mouse fibroblast cell lines, human osteosarcoma and adipiose derived
mesenchymal stem cells are discussed in Section 4. The section 5 elaborates the in
vivo evaluation of fabricated scaffolds in rat animal model. This section details the
development and validation of rat osteoporotic model and in vivo osteogenic efficacy
assessment in osteoporotic rat calvarial defect models.
Chapter 4 presents the results of the studies described using figures, tables
and graphs. The synthesized copolymer CEC was characterized in terms of
molecular weight using GPC, chemical structure by NMR and FTIR techniques. The
electrospinning parameters for scaffold fabrication, PCL/CEC blend ratio and nHAP
wt% were optimized. Both CEC and nHAP incorporation improved the surface
wettability, biodegradability as well as both static and dynamic mechanical
properties of PCL scaffolds. Comparative evaluation of both physical and biological
properties of PCL, PCL/CEC and their nHAP filled composites suggested that
PCL/CEC/nHAP composite scaffolds would be the best owing to the presence of
hydrophilic copolymer CEC and osteoconductive nHAP. The antiresorptive drug
PDS was successfully incorporated on PCL, PCL/CEC and PCL/CEC/nHAP
scaffolds which was reflected by the decreased fiber diameter, improved surface
wettability and enhanced mechanical properties of the bare scaffolds. In-vitro release
studies showed sustained release of PDS for the PCL/CEC/nHAP composite
scaffolds. In vitro cell culture studies proved cytocompatibility of PDS incorporated
scaffolds towards human osteosarcoma cell lines (hOS). Change in cell morphology
observed for higher amount of PDS 5wt%. The PCL/CEC/nHAP-PDS3 scaffolds
were chosen for in vivo evaluation based on in vitro release behavior, mechanical

xxv
property and cellular response. Prior to implantation in rat animal model, in vitro
cytocompatibility of scaffolds proved using rat adipose derived mesenchymal stem
cells (rADMSCs) using MTT assay, environmental scanning electron microscopy
(ESEM) and actin staining. Osteoporotic animal model was successfully developed
and micro computed tomography analysis, histology evaluation and serum analysis
confirms the osteoporotic model induction. Results of in vivo studies showed better
osseous tissue integration within PDS loaded scaffolds after 12 weeks as depicted by
X-ray radiographic, micro CT analysis, histology and histomorphometry analysis
suggesting the potential of fabricated PCL/CEC/nHAP-PDS3 scaffolds for the repair
of osteoporotic bone defects.
In Chapter 5, results are discussed and analyzed with the aid of current
literature. The concept of local delivery of antiresorptive drug PDS at the implant site
using electrospun PCL based scaffolds has showed improved osteogenesis in
osteoporotic condition in rat animal model. The importance of present study has also
been highlighted.
Chapter 6 summarises the results and conclusions which are drawn from the
study. Studies with PCL/CEC/nHAP-PDS scaffolds suggest that the above drug-
scaffold composite system has the ability to promote bone healing especially in
osteoporotic trauma.

1
CHAPTER 1
INTRODUCTION
Bone forms the major building block of human musculoskeletal system and plays
diverse role in our body. They serves both structural as well as reservoir functions which
includes protecting various vital internal organs, helping in locomotion, providing
mechanical support, act as store house of essential minerals and produce principal blood
components. Bone has the unique ability to heal and remodel without leaving a scar.
Though bone is considered as one of strongest tissue, it often undergoes defects or
damages resulting either from traumatic or pathological conditions such as accidents,
congenital abnormalities, infection, tumor resection, surgery, osteoporosis, etc. Though
nature has elegantly designed our body with an inbuilt mechanism for repair and
regeneration, the potential to heal may not be always sufficient.
Osteoporosis represents a metabolic bone disorder which is a worldwide
emerging health care issue and socioeconomic threat characterized by reduced bone
mass, and poor bone strength which results in fragile bones which are much susceptible
to fractures (Sartori et al., 2008). The clinical features of osteoporosis are pain, fracture
and deformity and the three major classic locations of fracture are hip, spine and wrist.
These fractures will lead to disability and reduce the quality of life and cause morbidity
and mortality especially in the elderly people. It is estimated that over 200 million
people are affected by osteoporosis worldwide. This figure will rise in future as the life
expectancy of ageing population is increasing and this will enhance the worldwide eco-

2
nomic cost. It has been reported that, the worldwide economic cost of osteoporosis in
1998 was US$34.8 billion, which is expected to rise to $131.5 billion by 2050 (Cauley et
al., 2014).
The treatment for osteoporotic fractures involves use of surgical interventions
such as autografts, allografts, bone grafts based on biomaterials (internal or external
fixatives such as screws, pins, intramedullary nails, braces) as well as pharmaceutical
agents (anabolic and catabolic agents). Since osteoporosis results in weakened bones
which are unable to heal on its own, it is often difficult to achieve a stable bone-implant
construct with the use of metallic implants. The pharmaceutical agents are usually
provided as a measure to prevent and treat osteoporotic fractures. However their poor
bioavailability and the undesirable side effects caused by routine administration is a
major concern. Hence localized delivery of these agents at the defect site is a possible
solution so as to enhance their bioavailability and efficacy.
Tissue engineering approaches utilizing scaffold, cells, growth factors or
bioactive drugs at the implant site can be a promising strategy for treating osteoporotic
bone fractures. The strategy adopted in the present study is to combine a biodegradable
scaffold with a pharmaceutical agent so as to develop an appropriate scaffolding
material for osteoporotic bone defect repair. In order to construct an ideal scaffold for
bone defect repair under osteoporotic condition, a thorough understanding about bone
anatomy, bone remodeling process, osteoporosis its types, causes, treatment modalities
and challenges is necessary, which is outlined below. This introductory chapter briefly
discusses the significance of tissue engineering in osteoporosis, requirements of an ideal

3
scaffolding material, the relevance of electrospinning technique for scaffold fabrication,
properties of biodegradable polymer, ceramic and the antiresorptive drug employed for
the study.
1.1. Bone
Bone is considered as a complex, dynamic and highly vascularized tissue having
huge variations of skeletal shapes in different regions of the body. Based on shape,
bones can be grouped into different categories such as long (e.g. femur, tibia, and
humerus), short (e.g. tarsus and carpus), flat (e.g. ribs and cranial bones), and irregular
(e.g. vertebrae of the spine) bones. Despite these variations in skeletal shapes,
macroscopically all bones are similar.
1.1.1. Bone macrostructure
In human body, there are two kinds of bone such as primary and secondary bone.
Primary bone also known as non woven bone is the initial bone which is formed during
the development and regeneration process. It comprises of large number of osteocytes
and irregularly arranged collagen fibers. Secondary bone also known as mature bone is
formed by replacement of the primary bone over time, and is present throughout a fully
developed human and is characterized by its dense mineralization and organized
structure.
The two types of secondary bones present in the body are cortical/compact bone
and cancellous/trabecular bone. The proportion of these bones varies at different
locations of the skeleton. The cortical bone accounts for 80 % of the human adult
skeleton which is almost solid and is of only 10 % porous. They are mostly found in the

4
outer part of long bones and in flat bones and are of about ~ 80-90 % mineralized. They
provide mechanical support and protect various delicate internal organs. The trabecular
bone accounts for rest 20% of the adult skeleton and is having a higher porosity of 50-
90% which makes their modulus and ultimate compressive strength around 20 times
inferior than that of the cortical bone. Their primary function is metabolic in nature as
they serve as the reservoir of calcium and phosphate ions. They are seen mostly in
metaphysic of long bones which are covered by cortical bone and also in the vertebral
bodies.
1.1.2. Bone matrix
Bone is a natural composite consisting of two phases, an organic (protein)
contributing about 25–30% of the total matrix and a inorganic (mineral) phase
contributing 65–70% of matrix. The mineral phase of the bone is calcium phosphate in
the form of crystalline hydroxyapatite, Ca10(PO4)6(OH)2. It also contains other mineral
ions such as magnesium, strontium, carbonate, citrate, and fluoride. The bone protein is
mainly composed of Type I collagen, which acts as a structural framework in which
plate-like tiny crystals of HAP are embedded to strengthen the bone. Non-collagenous
proteins constitute about 10 to 15% of total bone protein and make up approximately 3-
5% of the bone and it includes osteocalcin and glycoproteins including alkaline
phosphatase (ALP), osteonectin etc. This unique composition of bone ECM enables the
bone to provide mechanical support for the skeleton.

5
1.1.3. Bone cells
Bone tissue is populated mainly by four different cell types-osteoprogenitor cells,
osteoblasts, osteoclasts and osteocytes. Each cell type has defined task and they act
unanimously to maintain a healthy bone tissue. Osteoprogenitor cells originate from
mesenchymal stem cells and undergo osteogenic differentiation into osteoblasts. They
are most active during development of the skeletal system, but are frequently reactivated
during the normal bone turnover process and large numbers are activated during fracture
repair.Osteoblasts are metabolically active bone forming cells which originates from
bone marrow derived stem cells. They are cuboidal in shape when they are active and
become flattened out during inactive phase (resting). During the resting phase, they are
known as bone lining cells. They are involved in synthesizing collagenous as well as non
collagenous proteins and alkaline phosphatase which initiates the matrix
mineralization.Osteocytes are mature osteoblasts which are trapped within the bone
matrix and are responsible for its maintenance. Osteoclasts are multinucleated ruffle
bordered cells which are found on bone surfaces. They originate from monocytes and
macrophages and are responsible for the bone resorption process. The ruffled border
morphology of these cells enables them to attach to the bone surface and secrete acid
and enzymes into the mineralized bone, which results in the demineralization of the
bone.
1.2. Bone remodeling
Bone is a dynamic and metabolically active tissue which undergoes remodeling
throughout the entire life so as to maintain healthy skeleton and mineral homeostasis

6
(Kumar and Bhaskar, 2012). This process is controlled by the activity of osteoblasts
(bone formation) and osteoclasts (bone resorption). The remodeling process involves
continuous removal of discrete packets of old bone by osteoclasts followed by replacing
these packets with newly synthesized proteinaceous matrix, and subsequent
mineralization of the matrix to form new bone by the osteoblasts. During childhood and
adolescence period, remodeling is a balanced process where the rate of bone resorption
and bone formation is equal. After attaining the peak bone mass at adulthood, this
balance is maintained with small variations until the age of 50. After that, resorption
exceeds bone formation and loss of bone mass initiates. The bone loss increases with age
in both men and women and rate of bone loss is more in postmenopausal women.
1.3. Osteoporosis: A look into the problem
Osteoporosis is a global public health problem affecting millions of people
worldwide and its impact is pervasive in most of the nations which is associated with
significant morbidity, mortality, and socioeconomic burden (Aggarwal et al., 2011). It is
a silently progressing; multifactorial, age-related metabolic bone disease which is
characterized compromised bone strength predisposing to increased risk of fracture.
Bone strength reflects integration of two main features- bone quality and density. In
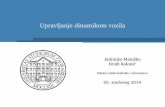
osteoporosis, both bone quality and density is affected. Morphological features of
normal and osteoporotic bone is represented in Figure 1.
As per World health organization (WHO), osteoporosis is diagnosed when the
value for the bone mineral density (BMD) is 2.5 standard deviations or more below the
mean of the young adult reference range. In India, it is estimated that about 50 million

7
are either osteoporotic (T-score lower than -2.5) or have low bone mass (T- score
between -1.0 and -2.5) (Mithal et al., 2014).
Normal bone Osteoporotic bone
Figure 1. Morphological features of normal and osteoporotic bone
(adapted from http://www.medguidance.com/thread/What-Causes-Osteoporosis.html)
Osteoporosis can be grouped into two categories based on their causes - Primary
and secondary. Primary osteoporosis related to estrogen deficiency and is termed as
Type I and generally affects women, particularly those who have undergone menopause
or ovariectomy. It is also known as post-menopausal / estrogen-induced osteoporosis as
it occurs due to the reduced level of estrogen hormone. Primary osteoporosis related to
ageing is known as Type II or senile or age-related osteoporosis. It affects both men and
women and is characterized by trabecular thinning, reduction in cortical thickness, and
increase in cortical porosity. Though these two types represents the most common
causes of osteoporosis in humans, their main difference is that in post-menopausal
osteoporosis, trabecular bone loss predominates over cortical bone loss whereas in age-
related osteoporosis there is a decline in both cortical and trabecular bone density.

8
Secondary osteoporosis results from external factors such as medications, endocrine
disorders, chronic renal disease, hematopoietic disorders, immobilization, nutrition and
gastrointestinal (GI) disorders and connective tissue disorders
The incidence of osteoporosis is more prominent in women due to their lower
peak bone mass and hormonal changes. Approximately one in two women and one in
four men over the age of 50 will have osteoporosis related fracture (Gudena et al.,
2011). This increased incident rate in women occurs due to the hormonal changes during
menopause, inadequate physical activity and low calcium intake. In aging population,
osteoporotic vertebral fractures are becoming more frequent and the increased incident
rate is associated with significant morbidity and mortality.
1.4. Osteoporosis epidemics in India
In India, fractures associated with osteoporosis is common in both men and
women, however owing to the lack of facilities for measuring of bone mineral density
(BMD), very little population-based research has been done in India (Anburajan et al.,
2011). As per Indian Council for Medical Research (ICMR) report on population based
studies, the prevalence of osteoporosis in male is of 3% and that of female is 8%
(Sreedevi & Ragi, 2016). Based on census data, out of 163 million aged people, 20%
percent of women and 10-15% of men were affected by osteoporosis (Malhothra &
Mithal, 2008). International Osteoporosis Foundation (IOF) Asian Audit, estimated that
about 50 million people in India are osteoporotic (T-score lower than - 2.5) or have low
bone mass (T score between -1.0 and -2.5). Studies by ICMR revealed that the lower
BMD values observed in Indians when compared to the western countries is due to the

9
genetic differences, nutritional deficiency and smaller skeletal size. The other factors
which contribute for poor bone health and osteoporosis in India are low intake of
calcium, high rate of vitamin D deficiency, lack of physical activity, sex inequality,
increasing longevity, lack of diagnostic facilities, poor knowledge on bone health, and
early menopause. The high rate of vitamin D deficiency in Indians is attributed to low
sun exposure, inadequate dietary vitamin D intake, and lack of food fortification with
vitamin D, pigmented skin, environmental pollution, and traditional dress code (Mithal
et al., 2013, Thulkar & Singh, 2015).
1.5. Pathogenesis of osteoporosis
Osteoporosis results mainly due to the imbalance in bone remodeling process,
which is determined by the activities of osteoblasts and osteoclasts. During normal bone
remodelling cycle, process of bone resorption and bone formation occurs in a
coordinated fashion. In case of osteoporosis, bone resorption exceeds bone
formation.The skeletal fragility associated with osteoporosis is due to various factors
such as (a) inadequate skeletal peak mass and strength during growth; (b) excessive bone
resorption resulting in decreased bone mass and micro architectural deterioration of the
skeleton and (c) an inadequate bone formation in response to increased resorption during
bone remodeling (Raisz, 2005).
In the case of post-menopausal osteoporosis, estrogen deficiency is a significant
cause of accelerated bone loss. Postmenopausal women are at the highest risk for
developing osteoporosis as their estrogen levels decline naturally which induce the
excessive proliferation of early osteoblast progenitors, which fuels excessive bone

10
turnover. Other factors affecting bone mass includes - Physical activity tends to increase
bone mass, whereas immobilization leads to increased bone loss. Obesity is associated
with higher bone mass. Typical patients who have osteoporosis tend to be thin and
possess less muscle mass. Low dietary intake of calcium, phosphorous, and vitamin D
are associated with age-related bone loss.
1.6. Treatment modalities for osteoporosis
Treatment of osteoporosis targets at reducing the fracture rate by means of
increasing bone strength which depends on bone mineral density (BMD) and bone
quality. Hip, wrist and spine are the three classic location of osteoporotic fracture.
Fractures occur mostly in skeletal regions with large proportion of cancellous bone such
as the vertebral body in the spine or the metaphyseal region of the long bones.
Non surgical, surgical and pharmacological approaches are used for osteoporotic
fracture treatment. Non-surgical approach involves immobilization which is mostly used
for elbow and knee fractures and is becoming less frequent (Larsson S, 2002). Surgical
interventions include use of intramedullary nails, bone impaction, buttress fixation,
fixed-angle devices, bone augmentation and joint replacement. Bone augmentation
involves use of bone autografts or allografts, bone cement or bone substitutes.
Pharmaceutical approach involves anabolic agents that stimulate bone formation [eg,
parathyroid hormone (PTH)] or antiresorptive agents that inhibit bone resorption [eg,
bisphosphonates, calcitonin, raloxifene, and estrogen] to slow down the progression of
disease (Malhothra & Mithal, 2008). And for most of these drugs, major concern is their
poor bioavailability and the long term use of these drugs has been often associated with

11
adverse side effects. Therefore, better strategy is to deliver these drugs locally at defect
site using drug loaded implants.
1.7. Challenges in osteoporotica fracture treatment
Fractures associated with osteoporosis are different from normal fracture and the
management of these fractures is challenging. The failure rates of fracture fixation in
osteoporotic bone range from 10% to 25% (Goldhahn et al., 2012). Even though
strategies for prevention and treatment for osteoporosis is available, the incidence of
fractures continues to rise with increasing aging population and is a major cause of
morbidity and mortality especially in elderly people. The implants developed for normal
bone fracture tend to fail in that of osteoporotic fractures. According to preclinical
evidence, fracture healing is delayed in osteoporotic patients due to the impaired
mechanosensitivity of osteoporotic bone (Jakob et al., 2013). The major challenge in
osteoporotic fracture treatment is to achieve a proper fixation and stability of implants.
The standard fracture fixating devices such as pins, intramedullary rods, plates and
screws often fails due to the inability of osteoporotic bone to hold them. The likelihood
of forming cavities in the area where devices are secured results in implant loosening
which also results in treatment failure (Lyet, 2006). The fixation strength of implants is
affected by the decreased thickness and increased porosity of the cortical bone, as well
as the rarefaction of the trabecular network (Schneider et al., 2005). The other factors
effecting fixation strength is changes in the remodelling cycle associated with
osteoporosis which results in the delayed fracture healing and high risk of non union.

12
Besides surgical interventions, pharmacological approaches involves using
bioactive agents which regulates bone remodeling process are used in preventing and
treating osteoporosis. However their poor bioavailability and undesirable side effects is a
major concern. Hence strategies for developing therapies which enables improved bone
repair, fracture healing, and implant fixation is essential in reducing osteoporosis
associated fractures.
1.8. Tissue engineering approach in osteoporosis
The development of tissue engineering constitutes a new platform for
translational medical research. Tissue engineering evolved as a result of lack of
availability of tissues and organs for transplantation and the inconvenience associated
with their transplantation such as donor site morbidity, immune rejection and pathogen
transfer (Subia et al., 2010). Tissue engineering approach utilizing biomaterial scaffold
represents a promising alternative for traditional osteoporosis therapies. The scaffold
based tissue engineering enables the delivery of cells, growth factors as well as bioactive
drugs at the defect site which aids in better bone formation and bone strength. Scaffolds
not only provide structural support to the growing tissue, but also play key role as a
construct in guiding tissue regeneration. Therefore the physical and chemical properties
of the scaffold, such as material composition, architecture, mechanical strength, pore
size and porosity, must be carefully designed which is the key challenge for the success
of tissue engineered bone grafts.

13
1.8.1. Scaffold requirements significant for bone tissue engineering
The key requirements for scaffolding material include non-immunogenicity, non-
toxicity, biocompatibility and biodegradability. Scaffold act as a temporary matrix to
deliver cells, growth factors as well as bioactive drug molecules and provide structural
support and serve as the template for cellular interactions and extracellular matrix
(ECM) formation. They should have a three dimensional architecture which favour the
growth and attachment of cells which has been cultured on it. Scaffolds must be highly
porous with interconnected pores and adequate pore size that allows cell in-growth and
proper cell distribution throughout the porous structure. Porosity and interconnectivity is
essential for diffusion of nutrients and gases and removal of metabolic waste resulting
from the cellular activity. The recommended pore size for bone tissue engineering
purposes lies within the range of 200–900 µm (Yang et al., 2001). Surface properties
such as surface chemistry and hydrophilicity govern in vitro and in vivo cellular
response. The mechanical properties of scaffolds should ideally match to that of the
living bone. The degradation rate of scaffolds must match with the neotissue growth
rate.
1.8.2. Biodegradable polymers and polymer-ceramic composites as scaffolds
The design and development of scaffold matrix from appropriate biocompatible
polymers with desired properties is the key challenge for the success of tissue
engineering. Natural as well as synthetic biodegradable polymers can be employed as
scaffolding material. Natural biodegradable polymers derived from natural sources
possess better biocompatibility and low immunogenic potential and the widely used

14
polymers includes collagen, fibrinogen, chitosan, starch, hyaluronic acid (HA) and
poly(hydroxybutyrate) (PHB). The inferior mechanical properties and the batch-to-batch
variation in properties associated with the natural polymers is a major drawback.
Synthetic polymers widely used for tissue engineering are aliphatic polyesters
such as poly(glycolic acid) or PGA, poly(lactic acid) (PLA), poly(lactic-co-glycolic
acid) (PLGA), poly(ɛ-caprolactone) (PCL) etc. These polymers have US Food and Drug
administration (FDA) approval and are already been used for clinically established
products such as implantable devices and sutures. These polymers also possess excellent
mechanical properties and their degradation behaviour could be tuned by blending with
other polymers or copolymers. However, they lack cell binding sites which results in
poor cell-material interaction. Currently, composite materials are being prepared using
biodegradable polymer and bioactive ceramic phase with the aim of increasing the
mechanical performance and bioactivity of the scaffolds. The most widely used
bioactive ceramics includes calcium phosphate ceramics such as hydroxyapatite (HAP),
tricalcium phosphate (TCP) , biphasic calcium phosphate (BCP) and bioactive glasses
(BAG).They have strong affinity to bind to the surrounding osseous tissue and enhance
bone tissue formation (Puppi et al., 2010).
1.8.3. Relevance of electrospinning technique for scaffold fabrication
Electrospinning is an enabling technique that allows fabrication of fibrous
scaffolds with well-defined architecture, controlled pore size, fiber diameter and
topography which favours cell growth and closely resembles the in vivo-like architecture
of ECM (Fischer et al., 2012, Kim et al., 2004). The unique feature of electrospinning

15
technique is its simplicity which enables fabrication of scaffolds in the required
architecture using appropriate polymer. Now researchers are increasingly interested in
developing drug delivery systems using electrospinning technique by incorporating
bioactive drugs in order to enhance the biofunctionality of the scaffolds. Drug molecules
can be embedded in the fiber either through dissolution or dispersion in the polymer
solution (Xie et al., 2010). The highly fibroporous architecture of electrospun fibers
along with their very high surface area enables the drug molecules to diffuse out from
the polymeric matrix. One major advantage of using drug loaded scaffolds is that, they
can be directly implanted on the defect site and thereby allows higher drug
bioavailability, improved therapeutic efficacy and reduced toxic side effects.
Advantages of using electrospinning technique for scaffold fabrication:
Process is a simple, straightforward, and cost-effective
Fibers with diameters ranging from microns down to few nanometers can be
obtained.
Scaffolds obtained is highly porous with interconnected pores and have
extremely large surface- area-to-volume ratio
Allows use of a variety of polymers, blends of different polymers, and inorganic
materials as well as incorporation of additives, biomolecules, and living cells for
tailoring different application requirements
1.8.4. Cell requirements significant for bone tissue engineering
The cell source should be non-immunogenic and could be easily isolated and
expandable (Heath, 2001).The osteoblast, owing to their non-immunogenicity is the first

16
choice and is usually isolated from biopsies of the patients (autologous cells). Their
usage is limited since their isolation is time consuming and only few cells with low
expansion rates could be obtained. Cells from non-human donors (xenogeneic cells) are
used as an alternative, to solve the problem of low cell number yields. However, the
associated immunogenicity and chance of transmission of infectious agents is a major
drawback.
Stem cells are more promising candidate in bone tissue engineering. They are un-
specialized cells that can self-renew indefinitely and can also differentiate into more
mature cells with specialized functions. They possess high proliferation capability and
multilineage differentiation. Embryonic stem cells (ESC) and adult stem cells (ASC) are
mostly used in bone tissue engineering (Salgado et al., 2004).There has been special
interest in use of mesenchymal stem cells (MSC) for bone tissue engineering
applications. Their source of isolation includes bone marrow, adipose tissue, muscle
tissue, amniotic fluid and periosteum. The advantage of using MSCs includes:
• Can be easily harvested and propagated
• Multipotent- Can differentiate to different lineages
• High proliferation rate
• Adherent to tissue culture plate
• Easily expanadable for long time without losing their osteogenic potential
1.8.5. Growth factors /bioactive drugs used in bone tissue engineering
Growth factors are cytokines that are secreted by many cell types and function as
signalling molecules Binding of a growth factor to its receptor initiates intracellular

17
signalling that will lead to promotion and/or prevention of cell adhesion, proliferation,
migration and differentiation by up-regulating or down-regulating the synthesis of
several proteins, growth factors and receptors. Bone morphogenetic proteins (BMP),
transforming growth factor beta (TGFb), fibroblast growth factors (FGFs), insulin
growth factor I and II (IGF I/II), and platelet derived growth factor (PDGF) are the most
commonly used growth factors.
The class of drugs used in bone tissue engineering includes antimicrobial agents
(Gentamicin, Tetracyclin, Vancomycin, Ciprofloxacin, silver ions), anti inflammatory
drugs (steroids such as dexamethasone and non steroids like ibuprofen) and
bisphosphonates (alendronate, zolendronate, pamidronate, Clodronate).
1.9. Role of bisphosphonates in treatment of osteoporosis
Bishosphonates (BPs) belong to the family of antiresorptive agents and are the
first-line medications for osteoporosis treatment being taken by millions of patients
worldwide, predominantly postmenopausal women (Gieger et al., 2013).
Figure 2. Structure of pyrophosphate and bisphosphonate
They are carbon-substituted analogues of pyrophosphate that act as powerful
inhibitors of osteoclastic activity. The structural difference between pyrophosphates and

18
bisphosphonates is the substitution of the oxygen connecting the two phosphates by a
carbon atom (Figure 2). The major site of action of bisphosphonate is bone. At any time,
approximately 10% of the adult skeleton undergoes active remodelling whereas the
remaining 90% is quiescent. Bisphosphonates have strong affinity for calcium in
hydroxyapatite. The calcium bound drug will be dissolved under the acidic conditions
created by osteoclasts during resorption. The solubilised bisphosphonate is then taken up
by the osteoclasts where they trigger various biochemical effects. At the molecular level,
nitrogen containing BPs inhibits the melvonate pathway which perturbs cell activity and
can induce apoptosis. At the cellular level, osteoclast recruitment and adhesion is
reduced and the loss of ruffled border on the osteoclasts makes it inactive for further
resorption resulting in shallow resorption sites. In addition to its effect on osteoclasts,
they promote osteoblasts proliferation and maturation. The net result is reduction in bone
resorption and net gain in bone density.
1.10. Need for animal models in osteoporosis research
Animal models provide uniform experimental material and allow extensive
testing of potential therapies. The osteoporosis research in particular is one of the most
common areas where animal models are necessary. Osteoporosis occurs naturally only
in humans and in nonhuman primates. Hence in other animal models, osteoporosis has to
be induced in the experimental setting by various approaches such as ovariectomy,
change of diet, use of drugs, immobolization etc. The performance of the tissue
engineering construct has to be evaluated in animal models prior to its evaluation in
humans. The Food and Drug Administration (FDA) guidelines recommends two

19
preclinical animal models, the ovariectomised (OVX) rat and a second non-rodent
model, to demonstrate the efficiency and safety of agents which is intended to use for
osteoporosis therapy (Thompson et al., 1995). Preclinical trials in smaller animals are
initially carried out as a proof of concept. If promising results are observed, further the
preclinical studies are extended to larger animals. The experimental animal model must
be carefully selected to evaluate the performance of the tissue engineering construct and
is critical for the success of the studies.
1.11. Rationale for choosing Poly (ε-caprolactone), Nanohydroxyapatite
and Pamidronate for the study
1.11.1. Poly (ε-caprolactone) (PCL)
PCL is the material of choice for the current study. The unique properties of PCL
are attributed to its chemical structure which consists of five non-polar methylene
groups and a single relatively polar ester group arranged in repeated fashion. The
presence of the olefinic group provides structural properties similar to polyolefin while
the hydrolytically liable ester group is responsible for the degradation property.
Figure 3. Structure of PCL
PCL has been intensively studied for tissue engineering applications owing to its
non toxicity, biodegradability and biocompatibility. It is a semi-crystalline polymer with

20
glass transition temperature of -60 °C and melting temperature of 58-63 °C which makes
it suitable for processing into various shapes with much ease. PCL degrades mainly by
hydrolysis of its ester linkages under enzymatic and hydrolytic conditions and hence
they received great deal of attention as an implantable material. The enzymatic
degradation occurs through the hydrolysis of their ester linkages by lipase, cholesterol
esterase, and carboxyl esterase (Gan et al., 1997, Labow et al., 2002). The nontoxic
nature of its degradation product i.e, caproic acid, a natural fatty acid of human skin
makes it an attractive candidate for biomedical applications. The complete resorption of
PCL requires more than 2 years (Yang et al., 2001).The versatility of PCL is due to the
fact that, it allows modification of its physical, chemical and mechanical properties by
co-polymerization or blending with many other polymers efficiently. It has been
observed that co-polymerization alters the chemical property that indirectly affects all
other properties such surface wettability and degradation behavior resulting in a
modified polymer with improved properties.
1.11.2 Significance of Nanohydroxyapatite (nHAP)
Nanohydroxyapatite (nHAP) has been widely used in biomedical implants for
bone regeneration due to its structural similarity to the mineral component of the bone.
The excellent biocompatibility, bioactivity, osteoconductivity and direct involvement in
bone cell differentiation and mineralization makes nHAP especially suitable for bone
tissue engineering. Moreover, HAP has the ability to induce mesenchymal stem cells
differentiation towards osteoblasts. Studies show that nanosized HAP particles (nHAP)
enhance protein adsorption and cell adhesion to the internal surfaces of the scaffold and

21
improve both mechanical and biological properties. However, the use of HAP alone is
limited due to its inherent brittle nature. Hence studies involving composites based on
HAP and biodegradable polymers are being carried out extensively with the aim to
confer high bioactivity and adequate mechanical properties to the scaffolds.
1.11.3. Role of Pamidronate (PDS)
Pamidronate disodium pentahydrate (PDS) belongs to the family of amino
bisphosphonates. Bisphosphonates (BPs) are important class of drugs which has been
widely used since 1970s for the management of various metabolic bone disorders such
as Paget’s disease, osteoporosis, hypercalcemia of malignancy as well as inflammation
related bone loss. They are stable analogues of pyrophosphates which are natural
modulators of bone metabolism. BPs binds strongly to hydroxyapatite mineral in bone
where they retain for many years, thereby providing potent pharmacological effects on
target tissue and act as potent inhibitor of osteoclast mediated bone resorption.
Figure 4. Structure of pamidronate
Studies have shown that administration of PDS seems to improve the bone
mineral density and helps in preventing bone loss associated with various bone related
disorders. However owing to its poor bioavailability, high dosage of PDS is necessary

22
which may result in various side effects. Hence localized delivery of PDS from polymer
matrix can increase the bioavailability and its therapeutic efficacy.
1.11.4. Rat as osteoporotic animal model
Rats are the most commonly used and excellent model for studying osteoporosis.
The choice of rat animal model is advantageous as they are quite inexpensive, easy to
house and maintain. They grow rapidly and have a well characterized skeleton. They
have cancellous bone remodeling with remodeling sites very similar to those seen in
human cancellous bone. Their short life span helps in studying the effect of ageing on
bone. Though rats do not experience natural menopause, an artificial menopause can be
induced by ovariectomy (Wronski et al., 1985). Ovariectomized animals are frequently
used as models for studying postmenopausal osteoporosis. Ovariectomy in rats results in
significant trabecular bone loss within 3-6 months (Bagi et al., 1997, Jee and Yao,
2001). The rapid loss of cancellous bone mass and strength observed in rats after
ovariectomy (OVX) mimic the bone changes following menopause in humans.
1.12. Hypothesis
The treatment of osteoporotic fractures are challenging due to the poor bone
quality which leads to higher rate of implant failure. Compared to the traditional
treatment modalities, biomaterial scaffold based tissue engineering approach is a
promising strategy for osteoporotic bone defect repair. On literature reviewing, only
very few studies has been focussed on the repair of critical-sized bone defects using
biomaterial scaffold based approach under osteoporotic condition. Similarly
pharmacological agents has been widely used for the treatment of osteoporosis and

23
fracture prevention, however less attention has been placed on the development of
pharmaceutical agent incorporated biomaterial scaffolds. Hence designing an
appropriate scaffold material that can effectively deliver pharmaceutical agents locally at
the defect site may be an effective strategy to promote osteoporotic bone repair.
Poly (ε-caprolactone) has been widely explored for bone tissue regeneration
application owing to it inherent biodegradability and biocompatibility. However, the
inherent hydrophobic nature of PCL limits its use as a functional scaffold owing to its
poor cellular response. This present study aims to investigate whether critical-sized
calvarial bone defects created in an osteoporotic rat animal model could be repaired
using an bisphosphonate based tissue engineering (TE) approach. In this context, the
hypothesis put forward is as follows:
(1) Incorporation of a hydrophilic polymer to PCL can modify its surface wetting
property, improve its biodegradability and provide better cellular response
(2) Nanohydroxyapatite (nHAP) incorporation can improve the mechanical properties
and the osteogenic potential of PCL based scaffolds
(3) Incorporation of pamidronate disodium pentahydrate (PDS), an antiresorptive agent
used for osteoporotic treatment, in PCL based scaffolds can improve the biofunctionality
of the scaffolds and can be used for osteoporotic bone defect repair
1.13. Objectives of the study
The main objective of the research study is to develop and characterize electrospun PCL
based nanocomposite scaffolds for osteoporotic bone defect repair. The study focussed

24
on validating the applicability of scaffolds under in vitro conditions and in vivo
conditions.To prove the hypothesis following objectives was defined:
1. To fabricate polymeric scaffolds based on biodegradable poly (ε-caprolactone)
(PCL) by electrospinning technique.
2. To improve the surface wettability and degradation behaviour of PCL by
blending with hydrophilic polymer and to evaluate its effect on the physical and
biological properties of PCL.
3. To fabricate bioactive scaffolds by incorporating nanohydroxyapatite (nHAP)
and to evaluate its effect on the physical and biological properties of PCL.
4. To fabricate and characterize pamidronate disodium pentahydrate (PDS)
incorporated PCL based scaffolds.
5. To evaluate the release profile of PDS and to determine the effect of PDS release
on cytocompatibility.
6. To develop an osteoporotic rat animal model by ovariectomy in female Wistar
rats.
7. To evaluate osteoporosis induced rat animal model.
8. To evaluate the osteogenic efficacy of PDS loaded PCL based scaffolds in
calvarial defects in rat osteoporotic model.

25
CHAPTER 2
LITERATURE REVIEW
The main goal of the study is to develop electrospun poly(ε-caprolactone) based
nanocomposite scaffolds with appropriate combination of mechanical support and
cellular response for osteoporotic bone defect repair. To develop an appropriate scaffold,
thorough knowledge of the current progress in this field is essential. This chapter
elaborates in detail the history of bone grafts and its current status, significance of tissue
engineering approach in osteoporosis, scaffold fabrication techniques in tissue
engineering. The chapter details the use of electrospun poly(ε-caprolactone) polymer as
bone regenerative scaffolds, studies on bisphosphonate incorporated polymeric scaffolds
and animal models used for osteoporotic fracture treatments. Thus with the aid of
published literature, experimental design strategies for the present study has been
deduced.
2.1. Bone grafts: History and current status
After blood, bone is the second most transplanted human tissue with
approximately 3.5 million bone graft procedures performed each year (Elsalanty and
Genecov, 2009). The concept of tissue transplantation is very ancient, dating back to the
early Christian era. The twin saints, St. Cosmas and St. Damian, who were surgeons in
the third century, were regarded as the pioneers of bone transplantation. They have
successfully removed the malignant and gangrenous limb of an aged sacristan of the
church and transplanted the leg of a deceased Ethiopian Moor to the sacristan.

26
In the modern era, bone grating began with the work by Dutch surgeon Job van
Meekeren, in 1668, who has repaired the traumatic defect in a soldier's cranium using
dog's skull (Blitch and Ricotta, 1996). It was in 1674, the Dutch scientist Anton van
Leeuwenhoek described the structure of bone. Ten years later, illustrations on callus
formation was also reported. The role of periosteum in bone formation was established
from the works of Duhamel in 1742. The first clinical autologous bone grafting was
performed by Dr. Philip von Walter in Germany in 1821, who replaced part of a skull
surgically removed after trephening the bone.Later in 1880, the first allograft
implantation was performed by Scottish surgeon Macewen on a four year old boy whose
infected humerus was reconstructed with a tibia graft taken from another child.
In 1915, Albee in his classical work concluded that the most suitable tissues for
transplantation are those originated from the connective tissue such as bone, fat and
fascia. The works on bone grafting and periosteum by Ollier, Barth and Axhausen has
laid the foundation for other researchers in this area. The works of Phemister and Albee
has elucidated the important factors in bone grafting which paved the way for the recent
work that has delineated the importance of osteoconductive scaffolding, osteoinductive
growth factors, and osteogenic progenitor stem cells in bone graft healing. Even with
such an extensive scientific history and various products available, till now, an ideal
bone graft substitute has not yet developed.
The demand for bone grafts is high in clinical practice for the substitution of
bone defects and recovery of atrophic bone regions. Based on the source, bone grafts can
be categorized as autografts, allografts and synthetic grafts.

27
2.1.1. Autografts
Autograft is one in which the source of the graft is from the same person i.e., the
donor bone is harvested from the patient itself. They are the primary material used in
bone grafting and is considered as the golden standard for replacing bone loss associated
with trauma, infection, tumor resection, revision arthroplasty, and arthrodesis (Williams
and Szabo, 2004). The main source of autograft bone is iliac crest of the patients and the
other site includes distal radius, proximal and distal tibia, and ribs. Since they are
harvested from the patient’s own body, they are highly accepted by the patient and
eliminate the risk of disease transmission. As the autograft bone is osteoconductive,
osteoinductive and provides osteogenic cells, faster bone formation at the implant site
can be easily achieved.
Though autografts provide best replacement alternate, its drawbacks may
sometimes outweighs its benefits. This includes pain and injury associated with
harvesting procedure, quality as well as quantity of the harvested bone, high cost
involved in the surgical procedure, the need for second surgery and the associated
morbidity.
2.1.2. Allografts
Allograft is one in which the source of the graft (donor bone) is from another
person but of the same species. The concept of using allograft is as old as autograft and
the allograft procedure become well established in 1960s by the works of Burwell which
led to the development of reliable bone banks. Bone allografts are being widely used in
the field of dentistry, orthopedics and craniofacial surgery. The main source of allogenic

28
bone is the femoral head which is obtained during hip arthoplasty. Based on the
processing, the allogenic bone grafts can be of two types-mineralized and demineralized
allografts. Mineralized allograft is available in fresh, frozen or freeze dried forms.
Demineralised allografts (mineral component of bone removed) comprises of collagen,
non collagenous proteins and some growth factors which provides it an osteoinductive
capacity.
The use of allografts is associated with various advantages such as it is available
in adequate quantities and eliminates the need for additional donor site surgery thus
relieving the patient from pain and injury. However, host incompatibility, and potential
risk of disease transmission from donor to recipient and the high cost requirement for
maintaining bone banks is a major concern (Laurencin et al., 2006)
2.1.3. Synthetic grafts
Synthetic bone grafts evolved as a result of the limitations associated with
autografts and allografts such as donor shortage, chance for rejection or transmission of
infectious disease. However, synthetic bone grafts are selected based on the nature and
complication of the bone defects as well as choice of available bone grafts.
2.1.3.1. Metals
Metals have been used in clinical orthopedics since early 1900s. Due to their
good mechanical durability, high strength and ductility metals are normally used for load
bearing applications such as pins, plates and femoral stems. The most commonly used
implants are based on austenitic stainless steel, cobalt-chromium alloy, titanium and its
alloys. Implants based on stainless steel have been the tradition metal which is used as

29
screws, plates and nails for bone fixation. Cobalt-chromium alloys based implants have
better corrosion resistance, wear resistance and have higher elastic modulus. The elastic
modulus of stainless steel and Co–Cr alloys is higher than that of natural bone, i.e.,
about 10 times greater which results in mechanical incompatibility. Titanium and its
alloys (e.g., Ti–6Al–4V) are now widely used in load-bearing applications due to its
excellent biocompatibility, light weight and good mechano-chemical properties. The
elastic modulus of these materials is much lesser than other metals and is found to be
about 5 times greater than natural bone. They are used mainly for prostheses to replace
large joints such as hip and knee. Their poor shear strength makes it less desirable for
bone screws, plates and similar applications which can be overcome by alloying with
other metals such as aluminium and vanadium.
Although metals have superior mechanical properties, problems such as elastic
modulus mismatch with host tissue, no active bonding to the tissue, low
biocompatibility, inflammatory and allergic reactions is of major concern.. The corrosive
nature of metals also weakens the implant and the corroded products may escape into the
tissue resulting in undesirable effects. Biodegradable magnesium alloys with low density
and mechanical properties closer to bone has been developed by researchers. However
the degrade rapidly and resulted in loose integrity prior to bone formation (Staiger et
al.,2006).

30
2.1.3.2. Ceramics
Ceramics are refractory, polycrystalline compounds usually inorganic, including
silicates, metallic oxides, carbides and various refractory sulphides and selenides.
Specially designed ceramics for the repair, reconstruction and replacement of diseased
or damaged parts of the body are termed “bioceramics” (Laverna and Schoenung,1991).
They were introduced to orthopedics during 1960s. They have high compressive
strength and hardness and highly biocompatible and tissue responsive. Based on tissue
response, they are classified into three types; nearly bioinert (e.g., alumina and zirconia),
bioactive (e.g., hydroxyapatite (HA) and bioglass), and bioresorbable (tri-calcium
phosphate (TCP)
The first clinically used bioceramic material was alumina in 1970 owing to its
excellent biocompatibility, hardness, strength to resist fatigue, and corrosion resistance.
Zirconia has been in use in orthopedics since 1985 and they exhibits fracture toughness
greater than alumina. Alumina and zirconia are predominantly used as femoral heads of
total hip joints. Due to exceptional bioactivity, HAP and bioglasses are frequently used
as bone graft substitute and as coating-agent on biometallic or biocomposite implants.
They elicit a strong interfacial interaction with host tissue due to their bioactivity;
thereby they are considered to provide osteointegrative stimuli. However, they are very
less bioresorbable. TCP is widely used as a bioresorbable bone graft. However, the rate
of bioresorption of TCP is unpredictable and they have certain drawbacks, which include
poor mechanical properties (e.g., brittleness and low toughness). Therefore, they are
used only in low-weight bearing orthopedic applications. Overall, the ceramics have

31
many advantages that include biocompatibility, easy availability, shapeability, non-
toxic, and non-immunogenic.
2.1.3.3. Polymers
Polymers are relatively new class of materials which is widely used as bone
graft substitutes owing to their biocompatibility, design flexibility, functional groups
availability, surface modifiability, light weight, and ductile nature (Hollinger and
Battistone, 1985). The category of polymers used as bone graft substitutes includes
biodegradable and non-biodegradable polymers. Collagen, gelatin, poly (ε-
caprolactone), poly (lactic acid) (PLA), poly (glycolic acid) (PGA) and their copolymers
poly(lactic-co-glycolic acid) (PLGA) belongs to the class of biodegradable polymers and
poly(ethylene) (PE), poly(ethylene terephthalate) (PET), and Poly(methyl methacrylate)
(PMMA) belongs to that of non-biodegradable polymers. The first synthetic polymer
used in clinical practice was of PMMA in 1937. Since then, numerous polymers has
been developed and used in orthopedic and other medical applications. Ultra high
molecular weight polyethylene is used to fabricate acetabular cups and used in total hip
arthoplasty. The acrylic cements are used alone or in combination with HAP for
cementing the metallic implants to natural bone.
The extensive interest in polymers is mainly due to their design flexibility and
the biodegradability of certain polymers at body pH which has resulted in the use of
polymers as scaffolding material for bone tissue engineering (BTE) applications. Both
natural as well as synthetic polymers are used as scaffolds for the delivery of cells,
growth factors or bioactive drugs to the site of injury. The most widely studied of natural

32
polymers includes collagen, gelatin, chitosan, silk, alginate, hyaluronic acid, and
peptides and that of synthetic polymers are polyesters such as poly glycolic acid, poly
lactic acid, and their copolymer of poly lactic-co-glycolic acid.
2.1.3.4. Polymer nanocomposites as bone grafts
Nanocomposites could play a pivotal role in bone grafting as a new class of bone
graft material, which uses a combination of several nanoscale bone graft materials
and/or in conjunction with osteoinductive growth factors and osteogenic cellular
components (Murugan and Ramakrishna, 2005).The term nanocomposite can be defined
as a heterogeneous combination of two or more materials in which at least one of those
materials should be on a nanometer-scale. Since bone is a typical example of a
nanocomposite, designing bone graft in the form of nanocomposite is perceived to be
beneficial. Polymer ceramic composites are the most investigated class for bone tissue
repair as they mimic the organic-inorganic hybrid nature of native bone tissue.
Nanocrystalline HA promotes osteoblast cells adhesion, differentiation, and
proliferation, osteointegration and deposition of calcium containing minerals on its
surface thus enhancing the formation of new bone tissue within a short period. Studies
have shown that incorporation of nano HA on polymer enhances the mechanical
property as well as tissue interactions.
2.2. Role of tissue engineering in treating osteoporotic bone fractures
Tissue engineering strategies may be adopted for osteoporotic fracture
treatments, wherein the cellular part of the scaffold helps in bone regeneration and the
scaffold/implant helps to maintain the contour and aesthetics of the fractured bone.

33
Effective therapies for bone tissue engineering typically employ the coordinated
manipulation of cells, biologically active signaling molecules, and biomimetic,
biodegradable scaffolds. Studies have been reported that reported that in aged and
osteoporotic patients the number as well as proliferation and differentiation potential of
MSCs will be lower. Hence this approach may be particularly beneficial for osteoporotic
patients for whom the number and renewal capability of osteoprogenitors cells is poor.
Manipulation of the local fracture environment in terms of application of growth factors,
scaffolds, MSCs or agents promoting bone formation and bone strength have been
considered as a treatment option from which promising results may arise.
2.3 Scaffold fabrication techniques in tissue engineering
Based on the specific requirements, various techniques can be adopted for
fabricating scaffolds based on appropriate material for tissue engineering applications.
While choosing the processing technique, it must be ensured that it will not adversely
affect the materials properties, especially the biocompatibility. The conventional
techniques employed for scaffold fabrication involves solvent casting and particulate
leaching, phase separation, gas foaming, melt moulding, fiber bonding and textile
methods such as electrospinning. Advanced techniques based on computer-aided
designing (CAD) or computer aided modelling (CAM) includes three-dimensional
printing, stereolithography, fused deposition modelling, selective laser sintering. Among
these various techniques, electrospinning technique can be employed to fabricate fibrous
structures consisting of macro/nano fibers. Due to the high resemblance to the extra
cellular matrix (ECM), scaffolds fabricated using electrospinning is considered as

34
potential candidates for temporary templates in tissue engineering. The simplicity of this
technique also allows encapsulation of bioactive drug molecules and hence can be used
as drug delivery device.
2.3.1. Electrospinning
Electrospinning is a unique and facile technique for producing ultrafine micron /
nano fibers from polymer solution or melts. A wide range of polymeric materials had
been electrospun for various applications. In order to develop materials with specific
functional applications, predominantly for bone tissue engineering composite nanofibers
based on polymeric materials incorporated with inorganic nanoparticles has been mostly
used. In a typical electrospinning process, when a high potential is applied to a
polymeric solutions or melts from few to tens of kilovolts (depending on the
electrospinnability of the material), an electrical field is simultaneously induced between
the spinneret and collecting device. The ball-shaped drop pendent on the nozzle exit is
then deformed, as a consequence of the force interactions between the coulombic force
(exerted by the external electric field) and the surface tension of the polymer solution,
into a conical shape termed as the Taylor cone. When the electric field strength is
increased to a threshold value, the electrostatic forces overcome the surface tension,
resulting in an ejection of a polymer liquid jet. This jet is then subjected to an extremely
high ratio of stretching and rapid evaporation of solvents, leading to the formation of
nano-/micro- meter sized fibers on the collecting device The mechanism of forming
nanoscale polymeric fibers with electrospinning has recently been identified as a result
of the bending instability or whipping of the charged jet, which was previously

35
described phenomenally as splitting or splaying. To date, with the electrospinning
process, more than 100 different types of materials have been electrospun into ultrafine
fibers with diameters ranging from a few nanometers to tens of micrometers.
2.4. Role of polycaprolactone as scaffolds in tissue regeneration
Poly (ε-caprolactone) (PCL) was synthesized in early 1930s by the Carothers
group (Van Natta et al., 1934). It can be synthesized either by ring-opening
polymerisation of ε-caprolactone using a variety of anionic, cationic and coordination
catalysts or via free radical ring-opening polymerisation of 2- methylene-1-3-dioxepane
(Pitt., 1990). PCL is semi-crystalline and hydrophobic in nature with a polar ester group
and five non-polar methylene groups in its repeating unit. The high olefin content
imparts polyolefin-like properties to PCL (Kim et al., 2004). PCL exhibits molecular
weight (Mw) ranging from 1000 to over 100,000 (Chen et al., 1998; Fields et al., 1974;
Tang et al., 2004) and its melting point (Tm) depends on Mw and can range from 45 ºC
to 60 ºC. PCL exhibits glass transition temperature (Tg) around -60ºC. The low melting
point along with its solubility in wide range of solvents, and exceptional blend-
compatibility has stimulated extensive research in its potential application in the
biomedical field.
During the resorbable-polymer-boom of the 1970s and 1980s, PCL and its
copolymers were used in a number of drug-delivery devices. Attention was drawn to
these biopolymers owing to their numerous advantages over other biopolymers in use at
that time. These included tailorable degradation kinetics and mechanical properties, their

36
ease of shaping and ease of manufacture enabling appropriate pore sizes conducive to
tissue in-growth, and the controlled delivery of drugs contained within their matrix.
Polycaprolactone has been modified by researchers in order to enhance its
surface wettability, mechanical properties, degradation behavior and biocompatible
properties. Blending techniques have been widely used to modify physical and chemical
properties of PCL. Numerous studies have been carried out on blends and composites
based on PCL for biomedical applications especially in the area of tissue engineering
and drug delivery. PCL has been blended with both natural as well as synthetic
biodegradable polymers. Prabhakaran et al has reported that PCL blended with chitosan
showed improved wettability, tensile property and cellular response (Molamma et al.,
2008). The studies by Kim et al suggested that PCL blended with water-soluble poly(N-
vinyl-2-pyrrolidone) (PVP) exhibited with tunable fiber surface morphology and
controllable degradation rates. The washing out of hydrophilic PVP resulted in
formation of nanopores on fiber surface leading to enhanced porosity which would
facilitate their use in tissue engineering (Kim et al., 2013). Aghdam et al modified PCL
with different concentration of PGA and observed improved wettability and mechanical
properties (Aghdam et al., 2011). The PCL/PMMA blend scaffold (7/3 wt ratio)
developed by Son et al exhibited improved growth of MG-63 osteoblast cells under in
vitro conditions and promoted bone formation of calvarial defect in Sprague Dawley
under in vivo conditions (Son et al., 2013).
Studies have shown that mechanical properties and biocompatibility of PCL can
be improved with of incorporation of ceramic (Wutticharoenmongkol et al., 2006).

37
Calcium phosphate based ceramics are widely used as fillers to overcome the
mechanical inferiority of the polymeric scaffolds (Xu, and Simon, 2005). The various
class of calcium phosphate based ceramics used in bone tissue engineering includes
Hydroxyapatite (HAP), beta-tricalcium phosphate (β-TCP), octa calcium phosphates
(OCP) and biphasic calcium phosphates (BCP) (Bose and Tarafder., 2012).
Among these, nano-sized hydroxyapatite (nHAP) particles are the most
promising filler which has been mostly incorporated in polymers owing their structural
similarity to the inorganic phase of the bone. Polymer composites are made either by the
direct incorporation of nanohydroxyapatite (nHAP) within polymeric matrices or by the
mineralization of nHAP on the surface of polymeric substrates (Liao et al., 2008). The
biologically beneficial characteristics of nHAP, includes the similarilty to the major
inorganic component of bone matrix, specific affinity to many adhesive proteins, and
direct involvement in the bone cell differentiation and mineralization processes which
make nHAP especially suited for utilization in the bone regeneration field.
Wutticharoenmongkol et al has observed improved tensile properties, enhanced
viability of human osteoblasts and highest ALP activity on PCL scaffolds incorporated
with 1wt% nHAP particles (Wutticharoenmongkol et al., 2006). Comparative evaluation
of attachment, proliferation, and alkaline phosphatise (ALP) activity of human
osteoblasts cells (SaOS2) on electrospun scaffolds and solvent casted films based on
PCL and PCL/nHAP revealed that fibrous scaffolds promoted much better adhesion and
proliferation than the corresponding film scaffolds (Wutticharoenmongkol et al., 2006).
Studies by Shalumon et al have shown that PCL nanofibers appear to show a significant

38
disposition towards initiating cell attachment and spreading than the micro-fiber
geometries. They observed that incorporation of nHAP (1.5wt %) into the nanofibrous
PCL scaffold enhanced the adhesion of human osteoblastic cell line (MG63) and protein
adsorption which was due to the high surface activity of nHAP.
2.5. Controlled release of bisphosphonates from polymeric scaffolds
Bisphosphonates (BPs) were discovered by the Theodor Salzer in 1894 and have
been used in textile and oil industries as corrosion inhibitors and complexing agents
(Petroianu., 2011).However the pharmacological activity of BPs was discovered in the
late 1960s by Herbert Fleisch (Giger et al, 2013). The works by Fleisch in collaboration
with Francis at Procter & Gamble revealed the high affinity of BPs for hydroxyapatite
which later resulted in their use for treating various bone diseases such as osteoporosis,
Paget's disease, bone metastases, malignancy-associated hypercalcemia, etc (Giger et al,
2013).
Now BPs is the first-line medications for osteoporosis treatment and is being
taken by millions of patient’s worldwide, predominantly postmenopausal women. They
are powerful inhibitors of osteoclastic bone resorption and reports are available
regarding their ability to proliferate bone-building osteoblast cells (Fleisch.,1998, von
Knoch et al., 2005, Im et al., 2004, Reinholz et al., 2000). The oral bioavailability of the
bisphosphonates is low (1–6%) and drug absorption decreases dramatically in the
presence of food as they form insoluble complexes with calcium or iron which is a major
concern. In fact, oral absorption ranges from about 0.7% (for alendronate and
risedronate) to only 6% (for etidronate and tiludronate).Studies have shown the

39
localized, controlled delivery of bisphosphonates has the potential to improve drug
efficacy and reduce the side effects by targeting the site of action. It avoids the
inconvenience of fasting and the patient morbidity associated with gastrointestinal
disturbance or musculoskeletal pain associated with the systemic delivery of these drugs.
Clinically, bisphosphonates effectively increase bone density, prevent bone loss
and reduce the risk of vertebral and non-vertebral fractures (Verron et al, 2010). Studies
have shown that local delivery of bisphosphonates can improve bone growth around
dental and orthopedic implants. In most of these studies, bisphosphonate has been
applied either topically into the implant cavity or as a drug coating on the implant itself,
but neither of these approaches affords controlled drug release. Only limited number of
reports is available on the development and characterization of polymer-based,
controlled-release delivery systems for bisphosphonates. Though polymeric
microspheric preparations of bisphosphonates clodronate, alendronate and pamidronate
have been reported, only very few reports are available on biodegradable films for
controlled and localized delivery of bisphosphonates (Table 1).
Literature review shows that very few works has been reported on the fabrication
and characterization of electrospun polymeric scaffolds for the delivery of
bisphosponates. Puppi et al has reported on the development of bioactive composite
scaffolds using three-arm branched-star poly(ε-caprolactone) (PCL), hydroxyapatite
nanoparticles(HNPs) and clodronate (CD) and evaluated their physico-chemical
characteristics (Puppi et al.,2011) . Lu et al has fabricated sandwich like nanofiber
meshes using polylactic acid and polyethyleneoxide for the controlled delivery of

40
zolendronic acid. Their results demonstrated that the drug release speed and initial burst
release were controllable by adjusting the thicknesses of electrospun barrier mesh and
drug-loaded mesh. Similarly, Yun et al has evaluated the effect of alendronate (Aln)
loading on in-vitro osteogenic differentiation of adipose-derived stem cells (ADSC) on
electrospun PCL scaffolds. They also investigated the in-vivo bone regenerative
capability of scaffolds in rat calvarial defect model and their results suggested that
Aln/PCL nanofibrous scaffolds enhanced the osteogenic differentiation of ADSCs in
vitro and bone formation in vivo (Yun et al.,2014).
Polymer used
Fabrication Bisphosphonate Author
PCL Electrospun
Alendronate
Yun et al.,2014
Chitosan and hydroxypropylmethyl
cellulose (HPMC)
Solvent cast Risendronate DhrubojyotiMukherjee et al., 2013
Three-arm branched-star PCL / hydroxyapatite
Electrospun
Clodronate
Doustagni et al.,2011
Three-arm branched-star PCL / hydroxyapatite
Electrospun
Clodronate
Puppi et al.,2011
PLA
Electrospun
Zolendronate
Jian et al., 2011
PDLLA
Solvent casted
Pamidronate
Yu et al.,2010
PLGA/PLLA-methoxy PEG
Solvent casted
Alendronate
Long et al.,2009
Table 1. Bisphosphonate incorporated polymeric membranes
2.6. Studies based on pamidronate for bone tissue regeneration
Studies based on pamidronate on evaluating their efficacy on clinical studies
especially in post menopausal women are reported by various researchers. Reid et al

41
demonstrated improvements in bone mineral density throughout the skeleton of
postmenapausal women as a result of continuous daily therapy with pamidronate dosage
of 150 mg/day (Reid et al., 1994). Morabito et al showed the effect combined use of
cyclic use of intravenous pamidronate and fluoride produced continuous increases in
BMD, at the lumbar level in post menopausal women (Morabito et al., 2004). The
treatment of postmenopausal osteoporotic women with intermittent intravenous
pamidronate increased bone mass at spine, hip and radius, and also potentially reduced
the incidence of new fractures (Thiebaud et al., 1994).The effectiveness of intravenous
doses of pamidronate in the prevention of femoral neck and lumbar spine bone loss in
men during the first 12 months after renal transplantation has also been reported (Stanley
et al., 2000).
Surface modifications of dental and orthopedic implants have been carried out to
improve the biological properties of implant materials. The surface properties of
implants play vital role in tissue acceptance and cell survival and modification of the
metallic implant surface can improve initial mechanical fixation and can increase bone-
to-implant bonding. The studies by Kajiwara et al demonstrated more new bone
formation around the pamidronate-immobilized titanium implant than around the
calcium-immobilized and pure titanium implants (Kajiwara et al., 2004). Studies by
Ponader et al has demonstrated the effectiveness of pamidronate-containing sodium
silicate coatings in enhancing the in vitro bioactivity, osteoblast attachment,
proliferation and vitality of cellulose-based scaffolds in terms of in vitro bioactivity and
osteoblast attachment, proliferation and vitality (Ponader et al., 2008). Shin et al has

42
fabricated pamidronate immobilized TiO2/HA nanofiber mats and studied the adhesion
and proliferation of osteoblasts on nanofibers. The results indicated better cellular
response of TiO2/HA-P composite nanofiber mats than bare TiO2/HA composites (Shin
et al., 2013).Very few studies have been reported on in vitro and in vivo analysis of
pamidronate incorporated polymeric scaffolds for osteoporotic treatment. Local co-
delivery of bone morphogenic protein (BMP) with via biodegradable poly-D, L-lactic-
acid (PDLLA) polymer implanted in the hind limbs of female C57BL6/J mice shows
that with appropriate dosing, local pamidronate may have the potential to improve BMP-
induced bone formation.
2.7. In vivo studies on rat animal model
Preclinical studies in animal models are essential in order to evaluate the
potential of developed materials which are intended to use in humans so as to confirm its
safety and efficacy. Ovariectomized animal model is widely recognized to closely
represent the pathophysiological situations of postmenopausal osteoporosis. Laboratory
ovariectomized rats are FDA-recommended models for osteoporosis research. The
endocrine gland ovary is responsible for the estrogen production. In cases of early
menopause, late menarche and ovariectomy, the level of estrogen secretion is decreased
which results in uncontrolled bone remodelling characterized by reduced deposition of
calcium and phosphorus in bone. These alterations will damage bone microarchitecture,
predisposing to the occurrence of osteoporosis (Cunha et al, 2010).
On literature reviewing, very few studies are reported on the use of polymeric
scaffolds in ovariectomised rats. Shen et al. has reported reduction in estrogen

43
concentration of ovariectomized rats which resulted in decreased bone mineral density
and biomechanical changes in the femur (Shen et al., 2000). Zhang et al has developed
strontium-incorporated mesoporous bioactive glass (Sr-MBG) scaffolds and implanted
in critical size femur defects created in ovariectomized rats so as to evaluate the in vivo
osteogenic efficacy. The results revealed improved ability of Sr-MBG scaffolds to
regenerate osteoporotic bone defects (Zhang et al., 2013) The studies by Cheng et al on
the evaluation of the efficacy of pure silk and hybrid CaP/silk scaffolds in treating
critical sized defects created in distal femoral epiphysis suggested enhanced
osseointegration with the use of hybrid CaP/silk scaffolds. Chandran et al has reported
the osteogenic efficacy of Strontium incorporated hydroxyapatite (SrHA) microgranules
in treating 3mm cortical bone defect in ovariectomised rats. Their findings suggest that
the improved osteogenesis observed with SrHA can be attributed to the released Sr2+ in
the defect site (Chandran et al., 2016).
To summarize, though significant progress has been made in the area of
developing bone graft substitutes. The development of an ideal bone graft with adequate
properties for osteoporosis bone defect repair still remains as a challenge. The present
work is an initiative in this area of research utilizing the advantage of the biodegradable
polymer PCL and the bisphosphonate drug pamidronate. The study focus on showing
how electrospun nanofibrous scaffolds based on PCL and PDS with adequate properties
can serve the purpose and efforts are being taken to achieve this goal.

44
CHAPTER 3
MATERIALS AND METHODS
In this study, efforts were made to develop an appropriate scaffolding material
based on PCL based nanocomposite for osteoporotic bone defect repair. The study
involves (1) development of biodegradable and bioactive scaffolds based on PCL with
improved hydrophilicity, biodegradability and better cell viability (2) development and
characterization of PDS incorporated PCL based scaffolds (3) In vivo evaluation of
PDS incorporated PCL based scaffold in a rat animal model to corroborate its
applicability.
Electrospinning technique was employed for scaffold fabrication. PCL scaffolds
were modified by blending with synthesized copolymer polycaprolactone–
polyethyleneglycol–polycaprolactone (CEC) and by incorporating nanohydroxyapatite
(nHAP) particles and were evaluated for their applicability in bone tissue engineering.
The amino bisphosphonate PDS incorporated PCL based scaffolds were fabricated and
characterized to evaluate the effect of PDS on physical and biological properties of
scaffolds. The experimental procedure related to copolymer CEC synthesis and scaffold
fabrication based on PCL is detailed in section 3.1. Fabrication of PDS incorporated
scaffolds is described in section 3.2. The section 3.3 details about characterization of
CEC copolymer and physico-mechanical property evaluation of scaffolds. The in vitro
cytocompatibility evaluation and cell culture studies on scaffolds using mesenchymal
stem cells (MSCs), L929 and human osteosarcoma cell lines (hOS) is described in

45
section 3.4. The in vivo evaluation of developed scaffolds in rat animal model is detailed
in section 3.5.
3.1. Synthesis of poly(ε-caprolactone) – polyethyleneglycol - poly(ε-
caprolactone) copolymer (CEC)
3.1.1. Commercial reagents for copolymer synthesis
-Caprolactone (ε-CL) and tin (II) 2-ethylhexanoate (stannous octoate) were
purchased from Sigma-Aldrich Chemical Company Inc., USA and polyethylene glycol
(PEG, Mn 2000) was procured from Merck, Germany.
3.1.2. Synthesis of CEC
The copolymer CEC was synthesized by polymerizing the monomer -
caprolactone monomer using polyethyleneglycol as the macro initiator and tin (II)
ethylhexanoate as the catalyst at a temperature of 130oC for 3 h. The triblock copolymer
formed was dissolved in dichloromethane and then precipitated in petroleum ether and
dried under vacuum at 40 oC.
3.2. Development of PCL based scaffolds with improved hydrophilicity,
biodegradability and better cell viability
3.2.1. Materials used for scaffold fabrication
Poly(ε-caprolactone) (PCL) with number average molecular weight Mn 80,000 was
procured from Sigma Aldrich, USA, Synthesized triblock copolymer PCL–PEG– PCL
(CEC) with number average molecular weight (Mn 7500) determined by GPC, Spray
dried nanohydroxyapatite (nHAP) particles with average particle size of 89 nm

46
provided by Bioceramics laboratory, SCTIMST, Trivandrum, India. The solvents
dichloromethane (DCM) and N,N-dimethyl formamide (DMF) (puris AR grade) were
purchased from Spectrochem, India.
3.2.1.1. Fabrication of scaffolds by electrospinning technique
Scaffolds were fabricated by electrospinning technique using PCL, PCL/CEC
blend (80/20 wt%) and their nHAP (2 wt%) filled composites in a solvent mixture of
80:20 (v/v) of dichloromethane (DCM) and dimethyl-formamide (DMF). Prior to
electrospinning, conductivity of spinning solution was measured using PC Scan 300
conductivity meter (Eutech instruments). Electrospinning was performed at a
predetermined condition of 10% solution concentration, applied potential of 12-15 kV
with a feed rate of 1 mL/h. The desired solutions were loaded into a 10 ml syringe, the
opening end of which was connected to a 21 gauge stainless steel needle that was used
as the nozzle. A mandrel rotating at 500 rpm was used as the collector and was placed at
a distance of 13-15 cm from the needle tip. A high-voltage power supply ((Gamma High
Voltage Research, Inc.,U.S.A.) was used to generate a high DC potential. A syringe
pump (Holmarc opto-mechatronics,Kochi, India) was used to control the feed rate of the
polymer solution.. After the process, the electrospun fibers were dried in a vacuum oven
at 40ºC for about 48 h to remove the residual solvent.

47
Figure 5. Electrospinning setup for scaffold fabrication
Table 2. Scaffold composition used for the study
3.2.2. Development of pamidronate incorporated PCL based scaffolds
3.2.2.1. Materials used and scaffold composition
Poly (ε-caprolactone) (PCL) , PCL–PEG– PCL (CEC), spray dried nanohydroxyapatite
(nHAP) , pamidronate disodium pentahydrate (PDS). The drug PDS was supplied as a
gift sample by JPN Pharma limited (Bangalore).
Sample Code Wt %
PCL CEC nHAP
PCL 100 - -
PCL/CEC 80 20 -
PCL/nHAP 100 - 2
PCL/CEC/nHAP 80 20 2

48
3.2.2.2. Fabrication of PDS incorporated PCL based scaffolds
Scaffolds were fabricated as described in section 3.2.1.1. The drug PDS (1, 3 and
5 wt %) was incorporated in the spinning solution and the drug loaded scaffolds based
on PCL, PCL/CEC and PCL/CEC /nHAP scaffold were fabricated. The scaffold details
are described in Table 3-
Table 3. Scaffold composition of PDS incorporated PCL scaffolds
Table 4. Scaffold composition of PDS incorporated PCL/CEC scaffolds
Sample Code
Wt % PCL PDS
PCL-PDS 1 100 1
PCL-PDS 3 100 3
PCL-PDS 5 100 5
Sample Code
Wt %
PCL CEC PDS
PCL/CEC-PDS 1 80 20 5
PCL/CEC-PDS 3 80 20 5
PCL/CEC-PDS 5 80 20 5

49
Table 5. Scaffold composition of PDS incorporated PCL/CEC/nHAP
scaffolds
3.3. Characterization of copolymer and scaffolds
3.3.1. Characterization of copolymer CEC
3.3.1.1. Fourier transform infrared spectra (FTIR)
The structural characterization of copolymer CEC was recorded using Thermo
Nicolet 5700 spectrometer with a diffused reflectance sample mode (Thermo Scientific,
Germany). The sample was mixed with optical grade KBR and scanned in the range of
400 and 4000 cm-1.
3.3.1.2. 1H- Nuclear Magnetic Resonance spectra (NMR)
1H-NMR spectra of the synthesized copolymer CEC was recorded using 500-MHz
spectrophotometer (Bruker Avance DPX 300) in deuterated chloroform (CDCl3),
containing small amount of tetramethylsilane (TMS) as internal standard.
3.3.1.3 Gel permeation chromatography (GPC) analysis
The molecular weight distribution and weight average molecular weight of the
synthesized copolymer CEC was determined by gel permeation chromatography (GPC,
Waters HPLC system, 600 series pump Milford, USA) with THF as the mobile phase
Sample Code
Wt %
PCL CEC nHAP PDS
PCL/CEC/nHAP - PDS1 80 20 2 1
PCL/CEC/nHAP - PDS3 80 20 2 3
PCL/CEC/nHAP - PDS5 80 20 2 5

50
with a flow rate 1mL/min. Polystyrene standards used for relative calibration was of
Mp-100000, 34300, 1470. The mobile phase was THF with a flow-rate of 1 mL /min.
The injection volume was usually 100 ml of stock solutions (0.1–0.5 w/v %).
3.3.2. Characterization of nanohydroxyapatite (nHAP).
3.3.2.1. Particle size analysis
Particle size of nHAP was measured using particle size analyzer, Zetasizer (Nano
ZS-90, Malvern Instruments, UK). For DLS measurements, nHAP was re-dispersed in
de-ionized water. The temperature was kept at 25oC during the measuring process and
measurements were recorded as the average of three test runs. The particle size was
measured with regard to the volume of particles in the sample. On volume basis the
average particle size is taken to be the size of particles occupying the maximum volume.
3.3.2.2 TEM Analysis
TEM analysis of nHAP was performed on a Hitachi H-7650 (Tokyo, Japan) at an
acceleration voltage of 80 kV. The suspension of nHAP was administered onto a 200
mesh copper grid coated with a formvar film and air dried prior to imaging.
3.3.3. Characterization of pamidronate (PDS)
3.3.3.1 FTIR spectra
FTIR analysis of PDS was carried out as described in section 3.3.11.
3.3.3.2. Particle size analysis
Particle size analysis of PDS was carried out as described in section 3.3.2.1.

51
3.3.4. Characterization of Electrospun scaffolds
3.3.4.1. Scanning Electron Microscopy (SEM)
The 3D morphology of the electrospun fibrous scaffolds was observed by
scanning electron microscopes (Hitachi-model-S-2400, JEOL, JSM-6390, model 7582,
Japan). The samples were sputter coated with gold palladium and imaged in order to
study the fiber morphology and average fiber diameter. The fiber diameter was
measured using Image J software.
3.3.4.2. Microcomputed Tomography (µ-CT) Analysis
Percentage porosity, pore size distribution, 3D structure and architecture of the
fibrous scaffolds were evaluated by microcomputed tomography ( µ-CT) analysis using
Scanco 40 equipment (µ-CT 40, Scanco Medicals, Switzerland). A series of about 302
2D slices with a scanning resolution of 6 µm were obtained by irradiating the specimen
with penetrative X-rays of 45 keV. CT tomography V5.5 was used as image processing
software and CT Evaluation Programme V6.0 was used as evaluation software. The
porosity along the scaffolds was also evaluated by 2D histomorphometric analysis using
a threshold 27 (Th 27).
3.3.4.3. Porosity analysis by liquid intrusion
The porosity of the scaffolds was measured using liquid intrusion method.
Scaffolds (n = 6) were weighed prior to immersion in ethanol (liquid intrusion) and the
scaffolds were left overnight on a shaker table to allow diffusion of ethanol into the void
volume. The scaffolds were taken out, blotted with a wipe and reweighed. The porosity
was calculated by dividing the volume of intruded ethanol (as determined by the change

52
in mass due to intrusion and the density of ethanol, 0.789 g/mL) by the total volume
after intrusion (i.e., volume of the intruded ethanol combined with the volume of the
PCL fibers determined from the initial mass of the PCL scaffold and the density of PCL,
1.145 g/mL)
3.3.4.4. Surface wettability
3.3.4.4.1. Static Contact Angle Measurements
Surface wettability of the scaffolds (n=3) was estimated with Goniometer (Data
Physics OCA 15 plus Germany). A drop of distilled water (5 l) was automatically
dropped onto a specially prepared plate of substratum and the image was immediately
sent via the camera to the computer and imaged using Imaging SCA20 software.
3.3.4.4.2. Dynamic contact angle measurements
The scaffolds (n=6) were cut to the dimensions 4 cm x 1.5 cm. The samples were
cleaned in a sonicate bath prior to the measurements. The contact angle was determined
in water using Wilhelmy method using KSV sigma 701 tensiometer. The immersion
depth was set to 10 mm with the speed of immersion of 5 mm/min. The initial 2 mm
length from each samples were ignored during the measurements. Six measurements
from each sample were recorded and the average of consecutive three values from each
samples were taken.
3.3.4.5. Static mechanical properties
The static mechanical properties were determined with universal testing machine
(Instron 3345, single column, UK) with the use of a 10 N load cell under a cross-head
speed of 10 mm/min (gauge length 20 mm) at ambient conditions. Dump bell specimens

53
as per ISO 527-2 was employed for the test. At least six set of specimens were tested for
each type of electrospun fibrous scaffolds.
3.3.4.6. Dynamic mechanical properties using DMA
The dynamic mechanical properties of scaffolds were assessed using Tritec 2000 B
(Triton Technology Limited, UK). Samples were tested under tensile mode at a
frequency of 1 Hz, and temperature range from −100 ºC to 40 ºC.
3.3.4.7. In-vitro release studies in PBS
Scaffolds (n=5) having 8 mm diameter and 0.2 mm thickness were in placed a
vial filled with 2 ml phosphate buffer solution (PBS). The release study of PDS was
carried out by keeping the samples at a temperature of 37 °C in a thermostatic shaking
incubator (Julabo SW22). At different time intervals, the drug eluted medium (2ml) is
taken and then the same volume of fresh PBS was added as replacement. The amount of
PDS released was quantified by Ninhydrin assay and evaluated using UV visible
spectrophotometer (SHIMADZU1500) at the wavelength of 568 nm.
3.3.4.8. In vitro Hydrolytic Degradation Studies
3.3.4.8.1. Mechanical property evaluation using UTM
Dumb-bell specimens as per ISO 527-2 were placed in closed bottles containing
30 mL phosphate buffer solution (pH: 7.4) and incubated in vitro at 37 ºC for different
time periods. At the end of each degradation period, the aged specimens were
characterized for mechanical properties using universal testing machine (Instron 3345,
single column, UK).

54
3.3.4.8.2 Morphology evaluation by ESEM analysis
The morphological changes of scaffolds in PBS after a period of 14 days were
observed using scanning electron microscope (Hitachi-model-S-2400).
3.4 In vitro studies
3.4.1. Ethical statement
In vitro cell culture studies using rabbit and rat derived mesenchymal stem cell
research work was carried out with the approval of Institutional Committee for Stem
Research and Therapy (ICSCRT) - Approval No:– SCT/IC-SCRT/28/Jan 2016.
3.4.2. Sterilization of scaffolds
Prior to cell culture studies, scaffolds (8 mm disc) were sterilized by immersing
in 70% alcohol under the laminar air flow over 2 h. Alcohol is then drained off and
samples were exposed to UV overnight.
3.4.3. In vitro cytocompatibility evaluation using L929 cell line
3.4.3.1. MTT assay
The MTT assay was performed to measure the metabolic activity of cells to
reduce yellow coloured tetrazolium salt 3-(4,5-Dimethylthiazol-2-yl)-2,5-diphenyl
tetrazolium bromide to purple coloured formazan. Material extract was prepared by
incubating test material with culture medium containing serum at 37 ± 2 ºC for 24 to 26
h at an extraction ratio of 6 cm2/ ml. The extract (100%) was diluted to 50% and 25%
with culture medium. A 100% extract prepared using HDPE was considered as negative
control. Extract and control medium were added to subconfluent monolayer of mouse
fibroblasts L929 cells in triplicate in a 96 well culture plate and incubated at 37 ± 2 °C

55
for 24 ± 2 h. Extract and control medium were replaced with 200 µl fresh culture
medium to which 50 µl MTT (1mg/ml in serum free medium) was added. Cells were
incubated at 37 °C for 2 h. After discarding the MTT medium, 200 µl of isopropanol
was added to all wells and mixed. The color developed was quantified by measuring
absorbance at 570 nm using a microplate reader (Biotek).
3.4.4. In vitro cell culture studies using human osteosarcoma (hOS) cell lines
The hOS cells obtained from National Centre for Cell Science, Pune were
cultured in Dulbecco’s modified Eagle’s medium (DMEM, Sigma) supplemented with 10 %
(v/v) fetal bovine serum (Sigma) and 1% (v/v) antibiotic/antimycotic solution at 37 °C in
a humidified, 5 % CO2 atmosphere. After harvest, cells were seeded at a concentration
of 1x 104 cells/cm on each sterilized scaffolds.
3.4.4.1. Live/dead assay
The morphology and viability of hOS cells was observed using DM 6000
fluorescence microscope (Leica, Germany, 20x objective, equipped with DFC 300 FX
digital camera). Fluorescein diacetate (FDA) / propidium iodide (PI) staining was
carried out to visualize viable and dead cells on scaffolds.
3.4.4.2. MTT assay
MTT assay was carried out to measure the proliferation of hOS on scaffolds.
Scaffolds were incubated at 37 °C in 5 % CO2 for 4 h in serum-free a-minimum essential
medium supplemented with 0.5 g of 3-(4,5-dimethylthiazol-2-yl)2,5-diphenyltetrazolium
bromide and the purple formazan was extracted using 0.04 M HCl in 2-propanol. The
extracted solution was measured at 570 nm using a UV-VIS spectrophotometer.

56
3.4.5. In vitro cell culture studies using rabbit adipose derived mesenchymal stem
cells (RADMSCs)
3.4.5.1. Cell Adhesion
The sterilized scaffolds were conditioned in α-MEM (alpha Mini-mum Essential
Medium, Invitrogen) for one hour prior to cell seeding. The cell seeded scaffolds were
maintained in osteogenic medium (α-MEM supplemented with 15% FBS, 10 mM
glycerophosphate, 10−8 M dexamethasone and 0.05 mg/ml L-ascorbic acid-Sigma) for a
period of 5 days. Each of the scaffolds were then retrieved at 2nd hour, 4th hour, 1st day
and 5th day respectively, then fixed in 3% gluteraldehyde and processed for SEM
(Hitachi-model-S- 2400) to evaluate the cell morphology and cell spreading over the
scaffold.
3.4.5.2. Live/dead assay The viability of RADMSCs on the scaffolds was determined using LIVE/DEAD
viability/cytotoxicity kit (Molecular Probes, Eugene). After 5 days in osteogenic
medium, the cell loaded scaffolds were incubated with DMEM containing 4 mM
acridine orange and 2 mM ethidium homodimer for 30 min. The non fluorescent
acridine permeates the intact membrane of living cells and appears bright green
fluorescent. The ethidium homodimer enters damaged cells and is fluorescent when
bound to nucleic acids. The cell-seeded scaffolds were washed with phosphate buffered
saline (PBS) thrice and imaged using Confocal Laser Scanning Microscope (cLSM).
Calcein flu- orescence was excited with the Ar+ laser at 495 nm, and ethidium
homodimer excitation was carried out using 528 nm HeNe laser.

57
3.4.5.3. Alkaline Phosphatase assay (ALP activity) The cell-seeded scaffolds on day 5 were washed with PBS and fixed with 3.7%
paraformaldehyde. After permeabilizing with 0.2% Triton-X-100 in PBS, the samples
were blocked with 3% bovine serum albumin in PBS and stained with ELF-97
endogenous phosphatise detection kit (Molecular probes) and viewed under cLSM (Carl
Zeiss LSM 510 Meta) for ALP activity.
3.4.5.4. LDH assay
The viability of osteogenic induced cells after 14 and 28 days of cultivation were
determined by measurement of cytosolic LDH activity using Cytotox96 kit (Promega,
Madison, USA). An aliquot of each cell lysate (50 µl) and LDH substrate (50 µl) were
allowed to react at 37 °C and the enzymatic reaction was stopped after 30 min with 0.1
M acetic acid. The absorbance was read at 492 nm (Hidex, Chamaleon). A calibration
line was plotted with an increase in the concentration of cells.
3.4.5.5. Picogreen assay
The DNA content of the cells after 14 and 28 days of cultivation were
determined using Picogreen® dsDNA Quantitation reagent (Molecular probes)
according to manufacturers instructions. The intensity of fluorescence was measured
(Hidex, Chamaleon) at an excitation and emission wavelength of 485/535 nm. Relative
fluorescence units were correlated with cell number using a calibration line constructed
from cell suspensions with increasing concentrations of cell numbers.

58
3.4.6. In vitro cell culture studies using rat adipose derived mesenchymal stem cells
(rADMSCs)
3.4.6.1. MTT Assay - un induced rADMSCs
MTT assay of un induced rADMSCs after 24h was performed as discussed in
section 3.4.3.1.
3.4.6.2. Cell adhesion - un induced rADMSCs
Cell adhesion of un induced rADMSCs after 24h were performed as discussed in
section 3.4.5.1.
3.4.6.3. Live/dead assay –un induced rADMSCs
Live/ dead of un induced rADMSCs were performed as discussed in section
3.4.4.1.
3.4.6.4 Cell adhesion – osteogenic induced rADMSCs
Cell adhesion of osteogenic induced rADMSCs after 14 days were performed as
discussed in section 3.4.5.1.
3.5. In vivo studies in rat animal model
Ethical statement
Animal surgical procedures were carried out at Division of Laboratory Animal
Science (DLAS), BMT Wing, SCTIMST. All experimental procedures and protocols
were conducted as per the guidelines and recommendations of Committee for the
Purpose of Control and Supervision of Experiments on Animals (CPCSEA), India and
with the approval of the Institutional Animal Ethics Committee (IAEC), B Form No:
98/PO/bc/99/CPCSEA

59
Animals were housed in individually ventilated cages (IVC, Citizen Industries,
India) at 22±2°C and 55±10% Relative Humidity (RH). Light levels measured at 1 meter
height less than 300 Lux and a 12:12 hour dark: light was maintained. Animals were fed
with standard pelleted rat feed and drinking ad libitum. The health of animal colony was
monitored as per Federation of European Laboratory Animal Science Associations
(FELASA) guidelines for parasitology and was stamped negative of any infectious
agents. All operations were carried out under sterile conditions with minimal invasive
surgical technique.
3.5.1. Development of osteoporotic rat animal model
3.5.1.1. Surgical procedure
Three month old female wistar rats weighing approximately about 250g were
selected for the study. In order to develop osteoporosis, rats were subjected to
interventional bilateral ovariectomy. The surgery was carried out under general
anaesthesia using xylazine (Xylaxin, Neon Lab, India) at a rate of 5mg/kg body weight
and Ketamine (Anket, Neon Lab, and India) at a rate of 70 mg/kg body weight as
intraperitoneal injections.The abdominal skin was shaved and the area for surgical
intervention was clipped and prepared with 5% povidone iodine solution (Win Media
care, India) prior to surgery. The incisions were made on flank on both sides laterally
towards the dorsal plane. The peritoneal fat pad was exposed and was exteriorized to
view the ovary and uterine horn on each side using a pair of fine tweezers. The ovary
was clamped using mosquito forceps an excised. The distal region of the uterine horn
was also clamped and a portion of the uterine horn was excised. Clamps were removed

60
and ascertained that haemostasis was achieved. The fat pad was retracted to the
peritoneal cavity using the blunt end of a vascular forceps and skin and muscle wounds
were closed using braided silk sutures 3-0 (Mersilk, Johnson Johnson, USA). Povidone
iodine solution was applied daily for 7 post operative days until the sutures were
removed. Post operatively; animals received subcutaneous injection of Analgesic-
Meloxicam (Melonex, Indian Immunologicals Ltd, India) @ 1mg/kg twice daily and
Buprenorphine (Buprigesic, Neon Lab, India) @ 0.05 mg/Kg i/m (intra muscular) twice
daily for 7 days. The animals were maintained for 4 months post induction to develop
osteoporosis.
Figure 6. Surgical procedure for rat ovariectomy
[a-incision made on lateral side of abdomen, b-external oblique muscle exposed, c-peritonial space and
adipose tissue surrounding ovary exposed, d-removal of ovaries, e-suturing the incision]

61
3.5.2. Evaluation of rat osteoporotic model
3.5.2.1. Histology of excised ovarian tissue - Haematoxylin & Eosin staining
The ovarian tissue collected during ovariectomy procedure were fixed in 10%
neutral buffered formalin (NBF) and stored at room temperature until histological
evaluation. The formalin fixed ovaries were further processed in series of alcohol
followed by embedding in paraffin to prepare 4 μm thick paraffin sections for
haematoxylin and eosin staining.
The processing steps involves dehydrating the formalin fixed ovaries in series of
alcohol - 80% isopropyl alcohol (2 hours), 95%isopropyl alcohol (2 hours), 95%
isopropyl alcohol (1 hour), 100% isopropyl alcohol for 1 hour –(three changes) followed
by clearing in xylene for 45 min (three changes) and infiltrated in paraffin wax for 1 h
(two changes) followed by 2 h (one change). The tissues capsules were then placed in
cassettes which were then put in a tissue processor. The paraffinized tissues were
removed from the tissue processor and were then formed into blocks. Thin paraffin
sections of approximately 4 micron thickness were collected using rotary microtome
(RM 2255, Leica, Germany). Sections were placed in hot air oven at 37°C for one day.
The hematoxylin and eosin (H & E) staining protocol involves deparaffinising
the sections by immersing it in xylene for 15 min (2 times) followed by processing the
sections in descending series of isopropanol (100%, 80% and 70% for 3 min each.
After washing with running tap water for 5 min, stain with Haris Hematoxylin (Sigma
chemicals, India) for 12 min and brought to running tap water (5 min). Sections were
then dipped in 1% acid alcohol (twice) followed by incubation in 0.2% ammonia water

62
solution for 2 min. Sections were counterstained with Eosin (sigma chemicals, India) (5
min) and underwent dehydration in ascending series of alcohol – 95% and 100% (2 min
each); three changes of xylene wash (15 min) and mounted using DPX. H & E stained
sections were then viewed and micrographed using DM 6000 microscope.
3.5.2.2. Micro Computed Tomography analysis-Assessment of trabecular bone loss
Micro CT analysis was carried out to confirm the osteoporotic model induction
by evaluating both qualitatively and quantitatively the trabecular bone loss by examining
the metaphyseal cancellous bone area. The ovariectomised rats after 4 months of post
induction (n=3) and normal rats (n=3) of same age group were sacrificed and their
proximal tibia was retrieved. The metaphyseal cancellous bone at the tibial head region
was scanned using micro-CT desktop scanner CT 40, Scanco Medical AG which was
operated at 70 kVp and 114 μA. Three dimensional model reconstructions were
performed using in built software V6.5 by selectively contouring approximately 200
slices of 20μm thickness from the volume of interest. The various parameters like
trabecular number (Tb.N.), trabecular spacing (Tb.Sp.), bone volume per total volume
(Bv/Tv) and trabeculat thickness (Tb.Th) were automatically determined which enables
the confirmation of osteoporotic model induction.
3.5.2.3. Weight monitoring before and after model induction
In order to assess the effect of ovariectomy on weight of normal and
ovariectomised rats (n=5) were weighed at definite time periods.

63
3.5.2.4. Biochemical analysis of blood serum - Calcium, Phosphorus and ALP assay
Blood samples were collected from rats (n = 6) before and after ovariectomy at
definite time period 0, 2 and 4 months was isolated from the animals by centrifugation at
1500 rpm at 37 °C for 10 min and stored in freezer until analysis.
Isolated serum were then analyzed for calcium concentration based on the
Arsenazo III method end point as per protocol (Cat No: BLT0001 Erba, Germany) (1 ml
reagent mixed with 20 μl sample and absorbance read at 630 nm against blank). Calcium
concentration was calculated as:
Calcium (mg/dl) = (absorbance of test/absorbance of standard) x concentration standard
(mg/dl)
Phosphorus concentration was analysed based on molybdate assay as per
protocol (Cat No: BLT00047 Erba, Germany) (1 ml reagent mixed with 10 μl sample,
incubate for 5 min. at 37 °C and absorbance read at 340 nm against blank) Phosphorus
concentration was calculated as:
Phosphorus (mmol/l) = (absorbance of test/absorbance of standard) x concentration
standard (mg/dl)
ALP concentration was analysed based on molybdate assay as per protocol (Cat
No: BLT00003 Erba, Germany) (1 ml reagent mixed with 20 μl sample, incubate for 1
min. at 37°C and absorbance read at 405nm against blank). ALP concentration was
calculated as:
ALP (U/I) = (absorbance of test/absorbance of standard) x concentration standard
(mg/dl).

64
3.5.3. Development of calvarial defect and scaffold implantation
3.5.3.1. Surgical procedure
The 8 mm critical size defect was created in calvaria of post osteoporotic rats
(n=21). The animals were weighed and housed singly in cages from one day before the
surgery. All the equipment used for surgery were sterilized by autoclaving. The surgery
was performed under general anaesthesia using xylazine at a rate of 5 mg/kg body
weight and Ketamine at a rate of 70 mg/kg body weight as intraperitoneal injections.
The surgical site was shaved and scrubbed with povidone iodine solution. Under aseptic
precautions, incision was made in the sagittal plane across the cranium. A full-thickness
flap including the periosteum was reflected, exposing the calvarial bone. Then a critical-
size (8 mm diameter) circular defect will be created on the cranium by using a saline-
cooled trephine drill without damaging the meninges and neural tissues. The polymeric
scaffold will be implanted on the defect in test group and the defect area will be kept as
such in sham group. The incisions will be finally closed by using 3-0 catgut sutures. The
wound will be cleaned and will be dressed using betadine ointment daily. The skin
sutures will be removed after 7 days of surgery. Animals will receive antibiotic
ampicillin-cloxacillin at a rate of 10mg/kg bid intramuscular injection and analgesic
Meloxicam at a rate of 1.0 mg/kg body weight subcutaneously once daily and
Buprenorphine at a rate of 0.1 mg/kg BID intramuscular as injections for a period of 5
post operative days.

65
Figure 7. Surgical procedure for calvarial defect and implantation
[a-incision on skin, b- exposing calvarial bone, c-drilling to create 8 mm CSD, d-
removal of calvarial bone, e-CSD created, f-placing 8 mm scaffold, g-suturing incision
area, h-sutured defect area, i- scaffold used and removed calvarial bone]
3.5.4. Osteogenic efficacy assessment of scaffolds in osteoporotic rat animal model
The osteogenic efficacy of PDS loaded scaffolds was evaluated through
histology (Stevenal's blue and vanGieson's picrofuchsin staining), histomorphometry,
radiographic and micro-CT.analysis

66
3.5.4.1. Gross evaluation of explants:
Animals were euthanized at definite time periods of 3, 6 and 12 weeks post
implantation. The implant site along with the adjacent host bone of each animal was
desected and fixed in 10% NBF. Prior to any other evaluations, gross examination of
retrieved explants was carried out.
3.5.4.2. Radiographic evaluation
Radiographic analysis of explants containing test and control at different post
implantation periods (3,6 and 12 weeks) was carried out at standard conditions using
X- ray film unit and imaging CR -30X (AGFA, USA) .
3.5.4.3. Micro CT evaluation:
The effect of bone healing ability was assessed from the formalin fixed samples
of 3, 6 and 12 weeks implantation studies. The explants were scanned using desktop
μCT (μCT 40, Scanco Medical AG, Brüttisellen, Switzerland). The 2D and
morphometry images generated from micro CT were assessed for evaluating the overall
healing efficacy. In vivo healing in the test was compared with of control animal post 12
weeks of implantation. The de novo bone formation and de novo bone mineralization
was assessed from the density histograms (included host bone and de novo bone)
generated from 2 D 61 of control and test group. Mineralization was estimated from the
density drawn on corresponding 2D slices.
3.5.4.4. Histological evaluation – PMMA embedding and staining
Prior to histological evaluation, the formalin fixed explants (3, 6 and 12
weeks) were dehydrated in graded ascending series of isopropyl alcohol

67
(Finar, India) (70% isopropyl alcohol for 4 days, 80% isopropyl for 4 days, 96%
isopropyl alcohol for 4 days, 100% isopropyl alcohol for 2 days, 100% isopropyl alcohol
for 1 day). Samples were then infiltrated in methyl methacrylate (MMA) (Merck,India)
for 6 days (2 changes) and finally embedded in MMA containing 1% peroxide under
vacuum in desiccator. The plastic sections of about 130-150 microns thickness were
sliced from PMMA embedded blocks using high-speed precision saw (Isomet TM 2000
Precision Saw, Buehler, USA) and polished down manually to 70–90 microns using
variable speed grinder polisher (Ecomet 3000, Buehler, USA). The PMMA sections
stained with Stevenal’s blue and van Gieson’s picrofuchsin. The staining protocol
involves incubating PMMA sections in hot water for 3 min followed by immersing in
pre-heated Stevenal’s blue stain (stain filtered and heated to a temperature of 60-65°C
for 5-15 min. The section is then water wash and counter stained with van Gieson’s
Picrofuchsin for 3- 5 min at room temperature. The sections were then viewed under
light microscope (Leica DM6000). Stevenal's blue stains cells and extracellular
structures in a subtle gradation of blue tones and van Giesen's picrofuchsin colours
collagen fibres (green or green blue), bone (orange or purple) and osteoid matrix (yellow
green).
3.5.4.5. Histomorphometry analysis - QWin software
Histomorphometry analysis was carried out to assess the osteointegrative and
osteogenic efficacy of scaffolds. The analysis was performed on three consecutive
sections of each implant and analyzed using image analyzing software (Leica Qwin,
Germany). The Stevenal's blue and van Gieson's picrofuchsin stained sections were

68
scanned for determining and the area of newly formed bone using the Quips programme
of QWin software of the microscope (Leica DM 6000). Bone formation indices were
evaluated within the defect boundaries alone. Regeneration efficiency (RE) of implant
was calculated and expressed as ratio of new bone formed to total defect area.
Measurements were taken from equidistant sites across sections under same
magnification.
3.6. Statistical Analysis
Data of all non-biological studies presented in this work were the mean of 6
samples. All the biological studies were done in triplicate. Data is reported as mean ±
SD. Statistical analysis was performed with one way ANOVA using Microsoft excel
2007 version or using Graph pad prism (Version 6.01). The values for which p<0.05
were considered as statistically significant.

69
CHAPTER 4
RESULTS
The results obtained from the current study are detailed in Chapter 4 which is
further divided into four subsections. The first section discusses the synthesis and
characterization of materials used for scaffold fabrication. The second section details the
fabrication and characterization of nHAP and CEC incorporated PCL scaffolds. The
fabrication and characterization of PDS incorporated PCL based scaffolds are discussed
in third section. The in vivo evaluation of scaffolds in an osteoporotic rat animal model
is detailed in section four.
4.1. Material Characterization
This section details the synthesis and characterization of copolymer CEC, nHAP
and drug PDS used for scaffold fabrication.
4.1.1. Synthesis & characterization of PCL-PEG-PCL triblock copolymer (CEC)
4.1.1.1. Synthesis of CEC
The PCL-PEG-PCL (CEC) triblock copolymer was synthesized by the ring-
opening polymerization of ε-caprolactone monomer using PEG as macro initiator,
whose hydroxyl end group initiated the ring opening. The schematic representation of
the copolymer synthesis is shown in Figure 8. The yield obtained was about 90%.

70
Figure 8. Schematic representation of copolymer synthesis
4.1.1.2. Fourier transform infrared spectroscopy
The chemical structure of synthesized copolymer was confirmed by the
characteristics bands observed using FTIR spectroscopy (Figure 9).
Figure 9. FTIR spectra of copolymer CEC
The FTIR analysis of CEC copolymer exhibited characteristic peaks of both PEG
and PCL. The absorption band at 1720 cm-1 is attributed to the C=O stretching vibrations
of the ester carbonyl group. The absorption bands at 1100 cm-1 and 1240 cm-1 are
attributed to the characteristic C–O–C stretching vibrations of the repeated –OCH2CH2
units of PEG and the –COO- bonds stretching vibrations, respectively. The absorption

71
band at ~3450 cm-1 is assigned to terminal hydroxyl groups in the copolymer. All the C–
H stretching bonds are centered at 2942 cm-1 and 2864 cm-1.
4.1.1.3. 1H- Nuclear Magnetic Resonance spectroscopy
The chemical structure of CEC was further fortified with 1H NMR spectra
(Figure 10).
Figure 10: 1H NMR spectra of copolymer CEC
The peaks at 1.62 ppm corresponds to methylene protons of - (CH2)3 - in PCL
units, 2.34 pmm to that of methylene protons of –OCCH2– in PCL units, and 4.09 ppm
to that of methylene protons of –CH2OOC– in PCL units respectively. The sharp single
peak at 3.66 ppm is attributed to the methylene protons of homosequences of the PEG
oxyethylene units. Peak at 7.26 is the peak for small amount of CHCl3 present in CDCl3.

72
4.1.1.4. GPC analysis
The copolymer CEC showed narrow molecular weight distribution with PDI 1.33
(Figure 11). The number average (Mn) and weight average (Mw) molecular weights
obtained are 5508 and 7305 respectively.
Figure 11. GPC analysis of copolymer CEC
4.1.2. Characterization of nHAP
4.1.2.1. Particle size analysis
The average particle size of nHAP particles was found to be 90 nm and the
polydispersity index was 0.292 as measured by particle size analyzer (Figure 12).

73
Figure 12. Particle size distribution of nHAP
4.1.2.2. TEM analysis
TEM analysis of nHAP showed rod shaped particles and the size was found to be in the
range of 12-35 nm width and 90-120 nm length (Figure 13).
Figure 13. TEM image of nHAP

74
4.1.3. Characterization of PDS
4.1.3.1. Fourier transform infrared spectroscopy
The FTIR analysis (Figure 14) revealed that the drug amino bisphosphonate PDS
showed strong absorption bands for their characteristic N-H stretching vibrations at 3386
cm-1, N-H bending vibrations at 1651 cm-1 and that of the O-H stretching at 3122 cm-1
respectively. The broad band at 1062 cm-1 is attributed to the vibrational band for the
PO3 group of PDS and the sharp bands at 1178 cm-1 and 921 cm-1 are assigned to P=O
and P–OH stretching vibrations respectively .
4000 3500 3000 2500 2000 1500 1000 50030
40
50
60
70
80
90
100
% T
rans
mitt
ance
Wave number(cm-1)
N-H stretchingO-H stretching
N-H bending
P= O stretching
P-OH Strectching
Figure 14. FTIR spectra of PDS
4.1.3.2. Particle size analysis
The size of PDS drug particles analysed using particle size analyzer (Figure 15)
was found to be in the range of 162nm with PDI value of 0.433.

75
Figure 15. Particle size distribution of PDS
4.2. Development of biodegradable and bioactive scaffolds based on PCL
with improved hydrophilicity, biodegradability and better cell viability
4.2.1. SEM analysis
Electrospun PCL, PCL/CEC blend and their nHAP filled composite scaffolds
exhibited fibrous morphology as revealed by the SEM micrographs (Figure 16).
Samples Average fiber diameter (µm)
Conductivity(µS/cm-1)
PCL 1.53 ± 0.53 0.98 ± 0.05
PCL/CEC 0.40 ± 0.10 2.87 ± 0.15
PCL/nHAP 0.66 ± 0.16 4.80 ± 0.14
PCL/CEC/nHAP 0.37 ± 0.09 9.20 ± 0.05
Table 6. Conductivity & average fiber diameter of scaffolds

76
Figure 16. SEM micrograph showing fibrous morphology of (a) PCL (b) PCL/CEC
(c) PCL/nHAP and (d) PCL/CEC/nHAP
The analysis of fiber diameter using Image J revealed that the fiber diameter
varied among all the scaffolds (Figure 17.). Electrospun PCL exhibited non uniform
fibers with an average diameter of 1.53 µm. Significant decrease in fiber diameter exist
among all the scaffolds (p value <0.0002). PCL/CEC blend scaffold had diameter of
about 0.40 ± 0.1µm. PCL/nHAP composite scaffolds exhibited rough surface with
average fiber diameter around 0.66 ± 0.16 µm. The PCL/CEC/nHAP composite scaffold

77
showed an average fiber diameter of 0.37 ± 0.09 µm. The conductivity and average fiber
diameter is summarized in Table 6. AV
ERAG
E FI
BER
DIA
MET
ER (M
ICRO
NS)
****
****
****
Figure 17. Average fiber diameter of scaffolds
4.2.2. Micro CT analysis
The 3D morphometry of scaffolds analyzed using µ-CT (Figure 18) revealed the
porous nature of the scaffolds. All the scaffolds were found to be porous in nature with
PCL scaffolds having percentage porosity of about 92%. The incorporation of both CEC
and nHAP reduced the porosity to about 80%. The fibrous scaffold PCL/CEC/nHAP
showed a percentage porosity of 48%.
The pore size distribution of scaffolds is shown in Figure 19. The average pore
size for PCL, PCL/CEC, PCL/nHAP and PCL/CEC/nHAP composite scaffolds were 48,
40, 34 and 20 µm respectively. This reduced pore size can be due to the decreased fiber
diameter of both CEC and nHAP incorporated scaffolds.

78
Figure 18. Micro CT analysis showing 3D morphometry of scaffolds (a) PCL (b)
PCL/CEC (c) PCL/nHAP and (d) PCL/CEC/nHAP

79
Figure 19. Pore size distribution of PCL, PCL/CEC, PCL/nHAP and
PCL/CEC/nHAP scaffolds
4.2.3. Contact Angle Measurements The results of contact angle measurements showed a higher water contact angle
of 119 ± 2° and 112±1° for PCL and PCL/nHAP scaffolds indicating their inherent
hydrophobic nature (Figure 20). The contact angle of copolymer blended scaffolds
dropped to zero suggesting that the incorporation of hydrophilic CEC resulted in
changes in the surface wettabilty.

80
Figure 20. Contact angle measurements of (a) PCL and (b) PCL/nHAP
4.2.4. Static mechanical properties of scaffolds
The static mechanical properties (Table 7) of the scaffolds revealed that
electrospun PCL exhibited inferior tensile strength owing to its very high porosity of
about 92% and increased fiber diameter of 1.53 µm when compared to both PCL/CEC
(80% porosity, 0.40µm fiber diameter) and PCL/nHAP (80% porosity, 0.66 µm fiber
diameter) scaffolds. The tensile strength of PCL increased from 5.3 MPa to 7.0MPa with
the addition of CEC and to 8.5 MPa with that of nHAP. The PCL/CEC/nHAP composite
scaffold showed an ultimate tensile strength of 13.1 MPa. The tensile modulus decreased
with CEC from 34 MPa to 19 MPa for PCL/CEC and to 21 MPa for PCL/nHAP
scaffolds. PCL/CEC/nHAP composite scaffold showed a tensile modulus of 17.2 MPa.
The reinforcing effect of nHAP particles in PCL matrix was reflected by an increase in
tensile strength by 60%. The copolymer blended scaffold exhibited an enhancement in
tensile strength by 32% whereas for PCL/CEC/nHAP scaffold the tensile strength
increased by 149%. The superior tensile strength of this composite scaffold can be

81
attributed to the decreased porosity (48%) as well as fine fiber diameter (0.37µm) which
may provide more contacts and stronger cohesion among these fibers.
Sample Tensile strength (MPa)
Elongation at break (%)
Youngs modulus (MPa)
PCL 5.3 ± 0.20 144 ± 17 34 ± 1.9
PCL/CEC 7.0 ± 0.30 111 ± 62 19.± 2.0
PCL/nHAP 8.5 ± 1.40 182 ± 15 21 ± 2.7
PCL/CEC/nHAP 13.1 ± 0.80 189 ± 42 17 ±1.8
Table 7. Static mechanical properties of scaffolds
4.2.5. Dynamic mechanical properties of scaffolds
Figure 21 shows the result of DMA analysis showing variation of storage
modulus with temperature for the scaffolds with temperature. Electrospun PCL exhibited
storage modulus of 8.1 MPa which was found to increase with the incorporation of CEC
and nHAP. The storage modulus of PCL/CEC blend and PCL/nHAP composite was of
9.5 MPa and 9.2 MPa respectively. The PCL/CEC/nHAP composite scaffold exhibited
storage modulus of about 10.4 MPa.
The variation of tan delta with temperature for the scaffolds is shown in Figure
22. The temperature corresponding to the tan delta peak is taken as the glass transition
temperature (Tg). It was observed that the T
g values of PCL and the PCL/CEC/nHAP
composite scaffold were almost similar around – 47.7 °C and – 47.4 °C respectively
where as for PCL/CEC and PCL/nHAP scaffolds, there was slight decrease in Tg
to

82
−49.4 °C and -51.6 °C which may be due to the enhancement in the chain flexibility of
PCL with the incorporation of both nHAP and CEC.
-120 -100 -80 -60 -40 -20 0 20 40 60
0.00E+0002.00E+0074.00E+0076.00E+0078.00E+0071.00E+0081.20E+0081.40E+0081.60E+0081.80E+0082.00E+0082.20E+0082.40E+008
Mod
ulus
(Pa)
Temperature (0C)
PCL PCL/CEC PCL/nHAP PCL/CEC/nHAP
Figure 21. DMA analysis showing variation of storage modulus of scaffolds with
temperature
-100 -80 -60 -40 -20 0 20 40 60
0.020.030.040.050.060.070.080.090.100.110.120.130.140.15
Tan
del
ta
Temperature(0C)
PCL PCL/CEC PCL/nHAP PCL/CEC/nHAP
Figure 22. DMA analysis showing variation of tan delta of scaffolds with
temperature

83
4.2.6. In vitro Hydrolytic Degradation Studies
SEM images (Figure 23) illustrates the effect of ageing in hydrolytic medium on
the fibrous morphology of the scaffolds.
Figure 23. ESEM analysis showing effect of PBS ageing on morphology of scaffolds
(a) PCL (b) PCL/CEC (c) PCL/nHAP and (d) PCL/CEC/nHAP
After 3 months of PBS ageing, thinning as well as rupture of fibers occurred
indicating the biodegradation phenomenon. This was further confirmed by the
significant drop in mechanical properties for all the scaffolds. On 3 months of PBS
aging, the tensile strength of neat PCL decreased by 26%. The incorporation of CEC
resulted in a decrease of strength by 40%. In the case of composite scaffolds, the

84
decrease in tensile strength was about 17% for PCL/nHAP and 35% for
PCL/CEC/nHAP systems (Figure 24).
PCL PCL/CEC PCL/nHAP PCL/CEC/nHAP0
2
4
6
8
10
12
14
Tens
ile s
tren
gth
(MPa
)
Samples
Befor immersion in PBS After 1 month After 3 month
Figure 24. Effect of PBS ageing on tensile strength of scaffolds
4.2.7. Cytotoxicity Test: MTT Assay
Figure 25 shows the percentage metabolic activity of the L929 mouse fibroblast
cells which were cultured with the extraction media in comparison with the control. All
the scaffolds were found to be non-cytotoxic with more than 80% metabolic activity.

85
PCL
PCL/CEC
PCL/nHAP
PCL/CEC/nHAPHDPE
Dilute
Phenol
Figure 25. MTT assay on scaffolds
4.2.8. Cell Attachment Studies
The attachment of RADMSC on the scaffolds is shown in Figure 26. The cell
morphology as well as the interaction between cells and scaffolds is well evident in the
ESEM image. The cells that were cultured on the fibrous scaffolds expanded and
stretched out to attach themselves on the fiber surface. After 2 h of cell seeding, SEM
images depicted round morphology for the cells with few spread cells on all the
scaffolds. The adhesion and spreading became more after 4 h seeding and the cells
appeared well spread on all the scaffolds. Spreading of cells was more pronounced after
5 days of culture. The results suggested that the fibrous as well as porous nature of the
scaffolds promote the attachment of RADMSCs. However in comparison with PCL,
cells seeded on PCL/CEC/nHAP composite scaffold covered most of the pores and

86
formed a sheet like morphology. This indicates the better biocompatibility of the
composite scaffold for attachment of RADMSCs.
Figure 26. ESEM analysis showing adhesion of RADMSCs on scaffolds
4.2.9. Live/Dead Assay
The RADMSCs were viable on all the scaffolds as shown by the live dead
staining (Figure 27). Acridine orange enters living cells that will appear bright green
fluorescent, whereas ethidium bromide stains nuclei of dead cells orange. The elongated
spindle morphology of the RADMSCs was also very well evident in the confocal
images.

87
Figure 27. Live/ dead assay on scaffolds
(a) PCL (b) PCL/CEC (c) PCL/nHAP (d) PCL/CEC/nHAP
4.2.10. LDH Assay
Cell viability determined by LDH assay reveals the influence of both copolymer
CEC and osteoconductive nHAP particles on PCL. Quantitative LDH activity
measurement showed that all the scaffolds exhibited an increase in cell viability with
culturing period (Figure 28). However, a significant increase was observed for
PCL/CEC/nHAP scaffold at a later period of 28 days in comparison with other scaffolds.

88
PCL PCL/CEC PCL/nHAP PCL/CEC/nHAP0
100
200
300
400
500A
bsor
banc
e (4
92nm
)
SAMPLES
Day 14 Day 28
Figure 28. LDH assay on scaffolds
4.2.11. Picogreen assay
Cell proliferation determined by Picogreen assay further fortifies the results of
LDH assay (Figure 29).
PCL PCL/CEC PCL/nHAP PCL/CEC/nHAP0
2
4
6
8
10
12
14
16
18
20
Cel
l num
ber/1
0,00
0
SAMPLES
Day 14 Day 28
Figure 29. Picogreen assay on scaffolds

89
The results revealed that the cell number increased with increasing culturing period for
all the scaffolds with PCL/CEC/nHAP scaffolds having a significant higher proliferation
rate at a later period of 28 days when compared with other scaffolds. The enhanced
proliferation of cells can be attributed to the scaffold’s greater hydrophilicity (water
contact angle dropped to zero), higher extent of degradation and the presence of
osteoconductive nHAP.
4.2.10. Alkaline Phosphatase (ALP) activity of scaffolds
Confocal laser scanning micrographs depicted ALP activity of osteogenic
induced cultured RADMSCs (Figure 30). Qualitative determination of ALP activity
confirms the presence of osteogenic induced RADMSCs on all the scaffolds.
Figure 30. ALP activity of scaffolds
(a) PCL (b) PCL/CEC (c) PCL/nHAP (d) PCL/CEC/nHAP

90
4.3. Development and characterization of pamidronate (PDS) incorporated PCL
based scaffolds
This section discusses the fabrication and characterization of pamidronate (PDS)
incorporated PCL, PCL/CEC blend and PCL/CEC/nHAP composite scaffolds. The
effect of PDS on the phyisco-mechanical and biological properties of PCL based
scaffolds was analyzed in order to choose an appropriate scaffold for the in-vivo study.
4.3.1 Environmental scanning electron microscopy (ESEM) analysis
The morphology of PDS incorporated PCL based scaffolds observed using
ESEM is depicted in Figure 31. All the scaffolds exhibited fibrous morphology
characteristic of electrospinning process. The fiber diameter measured using image J
analysis depicted that bare PCL scaffold exhibited non uniform fibers with an average
fiber diameter of about 1.54 ± 0.5 µm. The PCL/CEC blend scaffold had an average
fiber diameter of 0.40 ± 0.10 µm and the PCL/CEC/nHAP composite scaffolds exhibited
an average fiber diameter of 0.37 ± 0.10 µm.
The conductivity of spinning dopes prior to spinning was also measured and the
results are summarized in Table 8. The results indicated that the incorporation of CEC,
nHAP and PDS has enhanced the solution conductivity of PCL which resulted in
reduced fiber diameter. It was also observed that significant difference exist between
fiber diameter of PCL and PDS incorporated PCL scaffolds (p value <0.001).

91
Figure 31. ESEM analysis showing morphology of PDS incorporated
scaffolds (magnification: 4000x, scale bar = 10µm)
a. PCL b. PCL-PDS1 c. PCL-PDS3 d. PCL-PDS5e. PCL/CEC f. PCL/CEC-
PDS1 g. PCL/CEC-PDS3 h. PCL/CEC-PDS5 i. PCL/CEC/nHAP j.
PCL/CEC/nHAP-PDS1 k. PCL/CEC/nHAP-PDS3 l. PCL/CEC/nHAP-PDS5

92
Sample Conductivity (µS/cm-1)
Average fiber diameter (µm)
PCL 0.98 ± 0.05 1.53 ± 0.53
PCL-PDS1 5.40 ± 0.14 0.46 ± 0.20
PCL-PDS3 9.75 ± 0.21 0.42 ± 0.10
PCL-PDS5 9.85 ± 0.07 0.39 ± 0.10
PCL/CEC 2.87 ± 0.15 0.40 ± 0.10
PCL/CEC-PDS1 4.14 ±0.22 0.40 ± 0.20
PCL/CEC-PDS3 5.10 ± 0.48 0.30 ±.0.10
PCL/CEC-PDS5 9.91 ± 0.03 0.28 ± 0.20
PCL/CEC/nHAP 9.20 ± 0.05 0.37 ± 0.10
PCL/CEC/nHAP-PDS1 12.36 ± 0.20 0.33± 0.10
PCL/CEC/nHAP-PDS3 13.29 ± 0.07 0.30 ± 0.10
PCL/CEC/nHAP-PDS5 13.76 ± 0.14 0.32 ± 0.11
Table 8. Conductivity of spinning dopes and average fiber diameter of scaffolds
For PCL scaffolds, incorporation of PDS resulted in formation of smooth
uniform beadless fibers with narrow fiber diameter distribution. The fiber diameter of
PCL/PDS scaffolds varied in the range of 0.4-0.45 µm and no significant difference in
fiber diameter exist between PDS incorporated scaffolds (p value = 0.4046). The
average fiber diameter of PCL-PDS1, PCL-PDS3 and PCL-PDS5 was of 0.46 ± 0.2 µm,
0.42 ± 0.1 µm and 0.39 ± 0.10 µm respectively.
In case of PCL/CEC blend scaffolds, PDS incorporation resulted in formation of
smooth bead free fibers with fiber diameter varying from 0.3-0.4 µm. The fiber diameter

93
of PCL/CEC blends reduced significantly with the incorporation of PDS (p value =
0.0001). The PCL/CEC-PDS1 scaffolds had an average fiber diameter of 0.4 ± 0.2 µm
and that of PCL/CEC-PDS3 exhibited fiber diameter of 0.3 ±.0.1 µm. Significant
difference in fiber diameter exist between PCL/CEC-PDS1 and PCL/CEC-PDS3
scaffolds (p value = 0.0153) and that of PCL/CEC-PDS1 and PCL/CEC-PDS5 scaffolds
(p value = 0.013). The PCL/CEC-PDS5 scaffold had an average fiber diameter of 0.28 ±
0.2 µm. No significant difference exist in fiber diameter between PCL/CEC-PDS3 and
PCL/CEC-PDS5 scaffolds (p value = 0.4430).
The fiber diameter of PCL/CEC/nHAP scaffolds was of 0.37 ± 0.10 µm. The
fiber diameter of PCL/CEC/nHAP-PDS composite scaffolds varied from 0.3-0.37µm
with PCL/CEC/nHAP-PDS1, PCL/CEC/nHAP-PDS3 and PCL/CEC/nHAP-PDS5
scaffolds having fiber diameter of about 0.33 ± 0.10 µm, 0.30 ± 0.1 and 0.32 ± 0.11 µm
respectively. No significant difference observed in fiber diameter among PDS
incorporated scaffolds (p value 0.0001)
4.3.2. Porosity evaluation using liquid intrusion method
The porosity evaluation using liquid intrusion method revealed that all the
scaffolds were porous in nature with more than 80% porosity (Table 9). The bare
scaffold exhibited increased porosity; however PDS incorporation has slightly lowered
the porosity which may be due to the lower fiber diameter of PDS loaded scaffolds
which resulted in effective fiber packing.

94
Sample Porosity (%)
PCL 89 ± 0.8
PCL-PDS1 80 ± 3.1
PCL-PDS3 83 ± 0.3
PCL-PDS5 84 ± 0.2
PCL/CEC 82 ± 1.4
PCL/CEC-PDS1 80 ± 0.3
PCL/CEC-PDS3 82 ± 0.8
PCL/CEC-PDS5 85 ± 0.3
PCL/CEC/nHAP 79 ± 6.2
PCL/CEC/nHAP-PDS1 79± 1.9
PCL/CEC/nHAP-PDS3 76 ± 2.4
PCL/CEC/nHAP-PDS5 71 ± 1.6
Table 9. Porosity of scaffolds determined using liquid intrusion method
4.3.3. Surface wetting property by contact angle measurements
The inherent hydrophobic nature of PCL is depicted by its higher water contact
angle of 97 ± 10º (Figure 32). Both PCL/CEC and PCL/CEC/nHAP scaffolds were
found to be hydrophilic in nature with complete wetting of scaffolds. In case of
PCL/PDS scaffolds, the incorporation of hydrophilic PDS has altered the surface wetting
property of PCL which is reflected by the drop in the contact angle value with increasing
PDS content. The PCL-PDS5 scaffolds exhibited contact angle value of 36 ± 4º
indicating hydrophilic nature of PDS incorporated scaffolds. Both PCL/CEC-PDS and

95
PCL/CEC/nHAP-PDS scaffolds were found to be hydrophilic with water contact angle
almost zero.
PCL PCL-PDS 1 PCL-PDS3 PCL-PDS 50
20
40
60
80
100
120
DYN
AM
IC C
ON
TAC
T A
NG
LE(0 )
SAMPLES
Figure 32. Contact angle of PCL & PCL-PDS scaffolds
4.3.4. Static mechanical properties using UTM
The PDS incorporated scaffolds demonstrated improved tensile properties on
comparison with the bare scaffolds. The data obtained from UTM is summarized in
Table 10. The tensile strength of PCL scaffolds was about 5.3 ± 0.2 MPa which was
found to increase with the incorporation of PDS. The PCL-PDS scaffolds exhibited
tensile strength in the range of 13 MPa. For PCL/CEC scaffolds, the tensile strength was
about 7.0 ± 0.3MPa which was found to increase to 11 MPa with PDS incorporation.
The PCL/CEC/nHAP composite scaffold exhibited tensile strength of 13.08 ± 0.8MPa
which was found to increase to 15.02 ± 0.5 MPa for PCL/CEC/nHAP-PDS3 scaffolds.
The PCL/CEC/nHAP-PDS5 composite scaffolds exhibited tensile strength of 11.00 ±
0.7 MPa.

96
Sample Tensile strength (MPa)
Elongation at break (%)
Youngs modulus (MPa)
PCL 5.3 ± 0.20 144. ± 17 34 ± 1.9
PCL-PDS1 13.5 ± 1.60 174 ± 10 23 ± 5.8
PCL-PDS3 13.7 ± 0.04 172 ± 0.4 29 ± 5.9
PCL-PDS5 13.4 ± 0.16 186 ± 5.3 34 ± 5.3
PCL/CEC 7.0 ± 0.30 111 ± 62 19 ± 2
PCL/CEC-PDS1 11.2 ± 0.22 113 ± 20 23 ± 1.3
PCL/CEC-PDS3 11.4 ± 0.05 143 ± 28 17 ± 2.7
PCL/CEC-PDS5 11.5 ± 1.50 132 ± 56 20 ± 2.8
PCL/CEC/nHAP 13.12 ± 0.80 189 ± 42 17 ± 1.8
PCL/CEC/nHAP -PDS1 13.30 ± 0.45 111 ± 42 23 ± 4.4
PCL/CEC/nHAP -PDS3 15.02 ± 0.54 161 ± 68 32 ± 5.6
PCL/CEC/nHAP -PDS5 11.00 ± 0.71 129 ± 23 18 ± 4.4
Table 10. Static mechanical properties of scaffolds
4.3.5. Dynamic mechanical properties using DMA
The temperature dependence of storage modulus of PDS incorporated PCL
scaffolds are depicted in Figure 33. The storage modulus of PDS incorporated scaffolds
at 37 °C was higher than that of PCL scaffolds. For PCL scaffolds, the storage modulus
at 37 °C was found to be 8.1 MPa , whereas for the PDS incorporated scaffolds storage
modulus was of 14.3 MPa, 14.6MPa and 15.3 MPa for PCL-PDS1, PCL-PDS3 and
PCL-PDS5 scaffolds respectively.

97
-120 -100 -80 -60 -40 -20 0 20 40 60
0.00E+0002.00E+0074.00E+0076.00E+0078.00E+0071.00E+0081.20E+0081.40E+0081.60E+0081.80E+0082.00E+0082.20E+0082.40E+008
Mod
ulus
(Pa)
Temperature(C)
PCL PCL-PDS1 PCL-PDS3 PCL-PDS5
Figure 33. DMA analysis showing variation of storage modulus of PCL and PCL-
PDS scaffolds with temperature
.
-80 -60 -40 -20 0 20 40 600.020.03
0.040.05
0.06
0.070.08
0.090.10
0.110.12
0.13
Tan
del
ta
Temperature (0C)
PCL PCL-PDS1 PCL-PDS3 PCL-PDS5
Figure 34. DMA analysis showing variation of tan delta of PCL and PCL-PDS
scaffolds with temperature

98
Figure 34 represents the variation of tan delta of PDS incorporated PCL
scaffolds. The PCL scaffold exhibited glass transition temperature (Tg) at - 47.7°C. The
observed Tg values for PCL-PDS1, PCL-PDS3 and PCL-PDS5 scaffolds are - 48.2°C, -
48.7.°C and -49.2°C respectively.
The temperature dependence of storage modulus of PDS incorporated PCL/CEC
blend scaffold is shown in Figure 35. The storage modulus of PCL/CEC blend scaffolds
at 37 °C was higher than that of the PDS incorporated scaffolds. The storage modulus at
37 °C for PCL/CEC blend was found to be 9.5 MPa whereas for the PDS incorporated
scaffolds the storage modulus was of 7.8 MPa, 6.3 MPa and 4.3 MPa for PCL/CEC-
PDS1, PCL/CEC -PDS3 and PCL/CEC -PDS5 scaffolds respectively.
The temperature dependence of tan delta of PDS incorporated PCL/CEC blend
scaffold is shown in Figure 36. The broadening of tan delta peak was observed with the
incorporation of CEC on to PCL scaffolds. The PCL/CEC blend scaffold exhibited Tg
around - 49.4°C whereas for PDS incorporated scaffolds increment in Tg was observed.
The Tg values observed for PCL/CEC-PDS1 scaffolds was about - 44.5°C, and - 46.8 °C
for PCL/CEC-PDS3 scaffolds and that of - 46.2.°C for PCL/CEC-PDS5 scaffolds.

99
-120 -100 -80 -60 -40 -20 0 20 40 60
0.00E+000
5.00E+007
1.00E+008
1.50E+008
2.00E+008
2.50E+008M
odul
us (P
a)
Temperature (0C)
PCL/CEC PCL/CEC-PDS1 PCL/CEC-PDS3 PCL/CEC-PDS5
Figure 35. DMA analysis showing variation of storage modulus of PCL and
PCL/CEC-PDS scaffolds with temperature
-120 -100 -80 -60 -40 -20 0 20 40 60
0.02
0.04
0.06
0.08
0.10
0.12
0.14
0.16
Tan
delta
Temperature (0C)
PCL/CEC PCL/CEC-PDS1 PCL/CEC-PDS3 PCL/CEC-PDS5
Figure 36. DMA analysis showing variation of tan delta of PCL and PCL/CEC-
PDS scaffolds with temperature

100
The variation of storage modulus of PCL/CEC/nHAP composite scaffolds is
represented in Figure 37. The storage modulus of PCL/CEC/nHAP scaffold at 37 °C was
higher than that of PDS incorporated scaffolds. The storage modulus of
PCL/CEC/nHAP composite scaffold was of 10.4 MPa whereas for the PDS incorporated
scaffolds storage modulus was of 6.4 MPa, 7.4 MPa and 8.1 MPa for PCL/CEC/nHAP-
PDS1, PCL/CEC/nHAP-PDS3 and PCL/CEC/nHAP-PDS5 scaffolds respectively.
-120 -100 -80 -60 -40 -20 0 20 40 60
0.00E+000
2.00E+007
4.00E+007
6.00E+007
8.00E+007
1.00E+008
1.20E+008
1.40E+008
1.60E+008
1.80E+008
2.00E+008
Mod
ulus
(Pa)
Temperature (0C)
PCL/CEC/nHAP PCL/CEC/nHAP-PDS1 PCL/CEC/nHAP-PDS3 PCL/CEC/nHAP-PDS5
Figure 37. DMA analysis showing variation of storage modulus of PCL/CEC/nHAP
and PCL/CEC/nHAP -PDS scaffolds with temperature
The temperature dependence of tan delta with temperature for PDS incorporated
PCL/CEC/nHAP composite scaffolds is represented in Figure 38. The broadening of tan
delta peak was also observed for the PCL/CEC/nHAP scaffolds. The PCL/CEC/nHAP
composite scaffold exhibited Tg at - 47.4 °C whereas for PDS incorporated scaffolds
increment in Tg was observed. The Tg values observed for PCL/CEC/nHAP-PDS1

101
scaffolds was about - 43.8°C, - 44.4°C for PCL/CEC/nHAP-PDS3 scaffolds and that of
- 43.2.°C for PCL/CEC/nHAP-PDS5 scaffolds.
-120 -100 -80 -60 -40 -20 0 20 40 60
0.02
0.04
0.06
0.08
0.10
0.12
0.14
0.16
Tan
delta
Temperture (0C)
PCL/CEC/nHAP PCL/CEC/nHAP-PDS1 PCL/CEC/nHAP-PDS3 PCL/CEC/nHAP-PDS5
Figure 38. DMA analysis showing variation of tan delta of PCL/CEC/nHAP and
PCL/CEC/nHAP-PDS scaffolds with temperature
4.3.6. In vitro release studies of PDS
The release profile of PDS from PCL, PCL/CEC and PCL/CEC/nHAP scaffolds is
shown in figures 39 to 40. An initial burse release of PDS was observed from all the
scaffolds for the first few hours. The amount of PDS released depends on the polymer
composition as well as on the initial concentration of PDS and its distribution within the
scaffold. The amount of PDS released form PCL scaffolds after 21 days were 197 µg/ml,
259 µg/ml and 290 µg/ml respectively for 1, 3 and 5 wt% PDS scaffolds. The PCL-
PDS5 exhibited higher release rate compared to that of PCL-PDS1 and PCL-PDS3
scaffolds.

102
0 100 200 300 400 5000
50
100
150
200
250
300C
umul
ativ
e re
leas
e of
PD
S (µ
g/m
L)
Time (h)
PCL-PDS1 PCL-PDS3 PCL-PDS5
Figure 39. In-vitro release studies of PDS from PCL scaffolds
In case of PCL/CEC scaffolds, the amount of PDS released after 21 days were
245 µg/ml, 316 µg/ml and 324 µg/ml respectively for 1, 3 and 5 wt% PDS scaffolds.
The PCL/CEC-PDS5 exhibited higher release rate compared to that of PCL/CEC-PDS1
and PCL/CEC-PDS3 scaffolds.

103
0 100 200 300 400 5000
50
100
150
200
250
300
350
Cum
ulat
ive
rele
ase
of P
DS
(µg/
mL)
Time (h)
PCL/CEC-PDS1 PCL/CEC-PDS3 PCL/CEC-PDS5
Figure 40. In vitro release studies of PDS from PCL/CEC blend scaffolds
For PCL/CEC/nHAP composite scaffolds, the amount of PDS released after 21
days were 214 µg/ml, 246 µg/ml and 265 µg/ml respectively for 1, 3 and 5 wt% PDS
scaffolds. The PCL/CEC/nHAP -PDS5 exhibited higher release rate compared to that of
PCL/ CEC/nHAP –PDS1 and PCL/ CEC/nHAP –PDS3 scaffolds.
0 100 200 300 4000
50
100
150
200
250
Cum
ulat
ive
rele
ase
of P
DS
(µg/
mL)
Time (h)
PCL/CEC/nHAP-PDS1 PCL/CEC/nHAP-PDS3 PCL/CEC/nHAP-PDS5
Figure 41. In vitro release studies of PDS from PCL/CEC/nHAP scaffolds

104
4.3.7 In vitro degradation studies in PBS
The effect of PBS ageing on bare and PDS incorporated scaffolds is
depicted in Figure 42.
Figure 42. ESEM images showing fiber rupture after 3 months of PBS
aging
a. PCL b. PCL-PDS1 c. PCL-PDS3 d. PCL-PDS5
e. PCL/CEC f. PCL/CEC-PDS1 g. PCL/CEC-PDS3 h. PCL/CEC-PDS5
i. PCL/CEC/nHAP j. PCL/CEC/nHAP-PDS1 k. PCL/CEC/nHAP-PDS3
l. PCL/CEC/nHAP-PDS5

105
The degradation behavior is well evident from the morphological changes
occurred in scaffolds which is depicted by the ESEM images showing the fiber thinning
and rupture. This was further supported by the drop in tensile strength observed after 90
days of PBS ageing. After 3 months of PBS ageing, in case of PCL scaffolds, the drop in
tensile strength was of 26% (Figure 43-45). Compared to bare PCL scaffolds, drop in
tensile strength was more prominent on PDS incorporated scaffolds. It was observed that
drop in tensile strength was of 30% for PCL-PDS1, 56% for PCL-PDS3 and 68% for
PCL-PDS5 scaffolds. For PCL/CEC blend scaffolds, drop in tensile strength observed
after 3 months of PBS ageing was of 35%. The drop in tensile strength was of 52%, 67%
and 77% for PCL/CEC-PDS1, PCL/CEC-PDS3 and PCL/CEC-PDS5 scaffolds. The
drop in tensile strength observed for PCL/CEC/nHAP composite scaffolds was of 40%.
It was observed that drop in tensile strength was of 47% for PCL/CEC/nHAP-PDS1,
51% for PCL/CEC/nHAP-PDS3 and 55% for PCL/CEC/nHAP-PDS5 scaffolds.
PCL PCL - PDS1 PCL - PDS3 PCL- PDS50
2
4
6
8
10
12
14
16
Tens
ile s
tren
gth
(MPa
)
SAMPLES
Before immersion in PBS After 1 month After 3 month
Figure 43. Tensile strength of PCL-PDS scaffolds after 3 months of PBS ageing

106
PCL/CEC
PCL/ CEC -P
DS1
PCL/CEC-P
DS3
PCL/CEC-P
DS5
0
2
4
6
8
10
12
14
Tens
ile s
tren
gth
(MPa
)
SAMPLES
Before immersion in PBS After 1 month After 3 month
Figure 44 Tensile strength of PCL/CEC-PDS scaffolds after 3 months of PBS
ageing
.
PCL/CEC/nH
AP
PCL/CEC/nH
AP- PDS1
PCL/CEC/nH
AP-PDS3
PCL/CEC/nH
AP- PDS5
0
2
4
6
8
10
12
14
Tens
ile s
tren
gth
(MPa
)
SAMPLES
Before immersion in PBS After 1 month After 3 month
Figure 45 Tensile strength of PCL/CEC/nHAP-PDS scaffolds after 3 months PBS
ageing

107
4.3.8. In vitro cell culture studies using human osteosarcoma (hOS) cell lines
4.3.8.1. Live/dead assay
The viability of hOS cells on PDS incorporated PCL scaffolds were analyzed
using FDA /PI staining (Figure 46) in which the cytoplasm of the live cells stained with
FDA appears green and that of nucleus of the dead cells stained with PI appears red.
Figure 46. FDA/PI staining after 48 h showing viability of hOS cells on
scaffolds (scale bar = 100 µm)
a. PCL b. PCL-PDS1 c. PCL-PDS3 d. PCL-PDS5
e. PCL/CEC f. PCL/CEC-PDS1 g. PCL/CEC-PDS3 h. PCL/CEC-PDS5
i. PCL/CEC/nHAP j. PCL/CEC/nHAP-PDS1 k. PCL/CEC/nHAP-PDS3
l. PCL/CEC/nHAP-PDS5

108
It was observed that hOS cells adhered well on both bare as well as PDS incorporated
scaffolds (especially on scaffolds with PDS1 and PDS3). The assay revealed that
majority of the adhered cells were viable (green) thus proving the cytocompatibility of
scaffolds towards hOS cells. However, at higher PDS content, i.e, on scaffolds with
PDS5, cells lost their characteristic spindle morphology which is well evident in the
fluorescent microscopic images.
4.3.8.2. MTT assay
MTT assay (Figure 47), further fortify the results of live/dead assay showing
that all the scaffolds supported cell proliferation with ~100 % metabolic activity
especially in PDS incorporated scaffolds which further prove their non toxicity of
scaffolds towards hOS cells. The metabolic activity of hOS cells were not affected
even after 48 h of incubation. It was observed that in case of PCL-PDS scaffolds,
significant difference exists in cell viability between PCL and PCL-PDS scaffolds (p
value = 0.0004). On comparison among PCL-PDS scaffolds, no significant difference
exist in cell viability between PCL-PDS1 and PCL-PDS5 scaffolds (p value = 0.07406)
whereas significant difference exist between PCL-PDS1 and PCL-PDS3 (p value=
0.0057), PCL-PDS3 and PCl-PDS5 (p value= 0.0082) scaffolds. The PCL-PDS3
scaffolds exhibited higher percentage of metabolic activity.

109
PCL
PCL-PDS1
PCL-PDS3
PCL-PDS5
Cell al
one
***** **
Figure 47. MTT assay using hOS cells on PCL & PCL-PDS scaffolds
In case of PCL/CEC-PDS scaffolds (Figure 48), all the scaffolds exhibited
metabolic activty of ~ 100% and no significant difference in cell viability was obseved
among bare PCL/CEC and PCL/CEC-PDS scaffolds (p value = 0.7935) as well as
among PCL/CEC-PDS scaffolds (p value = 0.8549).

110
PCL/CEC
PCL/CEC-P
DS1PCL/C
EC-PDS3
PCL/CEC-P
DS5Cell
alone
ns
ns ns
ns
Figure 48. MTT assay scaffolds using hOS cells on PCL & PCL/CEC-PDS scaffolds
In case of PCL/CEC/nHAP scaffolds also (Figure 49), % metabolic activity was
higher for PDS incorporated scaffolds and significant difference exist in cell viability
among bare PCL/CEC/nHAP and PCL/CEC/nHAP-PDS scaffolds (p value = 0.0237) as
well as among PCL/CEC/nHAP-PDS scaffolds (p value = 0.0453). On comparison
among PCL/CEC/nHAP-PDS scaffolds, no significant difference exist in cell viability
between PCL/CEC/nHAP-PDS1 and PCL/CEC/nHAP-PDS5 scaffolds (p value =
0.9381) as well between PCL/CEC/nHAP-PDS3 and PCL/CEC/nHAP-PDS5 scaffolds
(p value = 0.0585) whereas significant difference exist between PCL/CEC/nHAP-PDS1
and PCL/CEC/nHAP-PDS3 (p value= 0.0071), PCL/CEC/nHAP and PCL/CEC/nHAP-

111
PDS3 scaffolds (p value= 0.0021). The percentage metabolic activity was higher for the
PCL/CEC/nHAP-PDS3 composite scaffolds. PCL/CEC/nHAP
PCL/CEC/nHAP-PDS1
PCL/CEC/nHAP-PDS3
PCL/CEC/nHAP-PDS5
Cell al
one
** nsns
**
Figure 49. MTT assay using hOS cells on PCL/CEC/nHAP & PCL/CEC/nHAP-
PDS scaffolds
4.3.9. In vitro cell culture studies rats adipose derived mesenchymal stem cells
(rADMSC)
Based on the physico-mechanical properties, the PCL/CEC/nHAP composite
scaffolds were selected for further in-vitro cytocompatibility evaluation using rat’s
adipose derived mesenchymal stem cells (rADMSC). Rat ADMSCs were chosen for the

112
study since the potential of the scaffolds has to be evaluated under in vivo conditions in a
rat animal model.
4.3.9.1. MTT assay
The results of MTT assay (using un-induced rADMScs (Figure 50) after 24h
revealed that all the scaffolds were found to be cytocompatible with more than 90%
metabolic activity.
PCL/CEC/nHAP
PCL/CEC/nH
AP-PDS1
PCL/CEC/nH
AP-PDS3
PCL/CEC/nHAP-P
DS5Cell
s
Phenol
**
ns
*
Figure 50. MTT assay using un-induced rADMSCs on PCL/CEC/nHAP-PDS
PCL/CEC/nHAP-PDS scaffolds

113
The percentage metabolic activity was more pronounced on PCL/CEC/nHAP-
PDS scaffolds than that of PCL/CEC/nHAP scaffold (p value = 0.0203). On comparison
among PCL/CEC/nHAP-PDS scaffolds, significant difference exist in metabolic activity
among PCL/CEC/nHAP-PDS1 and PCL/CEC/nHAP-PDS3 (p value = 0.0193)
scaffolds as well as between PCL/CEC/nHAP-PDS3 and PCL/CEC/nHAP-PDS5 (p
value = 0.0280). However no significant difference in viability was observed between
PCL/CEC/nHAP-PDS1 and PCL/CEC/nHAP-PDS5 scaffolds (p value = 0.1519).
4.3.9.2. Live/dead assay
The rADMSCs adhered on the scaffolds and were found to be viable as depicted
actin staining (Figure 51). The cells exhibited their characteristic spindle morphology on
all the scaffolds except on PCL/CEC/nHAP-PDS5.
Figure 51. Actin staining showing adhesion and morphology of rADMSCs on
scaffolds (scale bar = 10 µm) a. PCL/CEC/nHAP b. PCL/CEC/nHAP-PDS1 c.
PCL/CEC/nHAP-PDS3 d. PCL/CEC/nHAP-PDS5

114
4.3.9.3. Cell adhesion
The adhesion of un-induced rADMSCs after 24 h (Figure 52) and osteogenic
induced rADMSCs (Figure 53) after 14 days on the scaffolds was qualitatively analyzed
by ESEM analysis. The rADMSc had favourable interraction on all the scaffold and they
adhered and spread well on the fibroporous scaffold surface further proving their
cytocompatibility. The in vitro osteogenic efficacy of scaffolds was depicted by the
formation of mineralized nodules by osteogenic induced rADMSCs on scaffold surface.
Figure 52. ESEM analyis showing adhesion of un induced rADMSCs on scaffolds
scale bar = 20 µm) a. PCL/CEC/nHAP b. PCL/CEC/nHAP-PDS1 c. PCL/CEC/nHAP-
PDS3 d. PCL/CEC/nHAP-PDS5

115
Figure 53. ESEM analyis showing formation of mineralized nodules by
osteeogenic induced rADMSCs on scaffolds surface scale bar = 40 µm)
a. PCL/CEC/nHAP b. PCL/CEC/nHAP-PDS1 c. PCL/CEC/nHAP-PDS3
d. PCL/CEC/nHAP-PDS5
4.4. In vivo studies in rat animal model
The main objective of this section was to evaluate the osteogenic potential of the
fabricated scaffold under in vivo conditions. The work is divided into two sections. The
first section deals with the development and validation of osteoporotic rat animal model.
The second section involves creating critical size calvarial defect (8 mm) in osteoporotic
rats and implanting scaffolds (bare as well as PDS incorporated scaffolds) so as to
evaluate their efficacy for bone regeneration. The test material was selected based on the
results of preliminary in vitro cell culture studies. The created calvarial defect area was

116
treated with PCL/CEC/nHAP-PDS3 scaffold (test) and PCL/CEC/nHAP scaffold
(control) to evaluate the effect of PDS on the calvarial bone defect regeneration.
4.4.1 Establishment of rat osteoporotic model
This section confirms the establishment of rat osteoporotic model by
ovariectomy. The rat animal model was evaluated for the induction of osteoporosis after
four months post ovariectomy.
4.4.1.1. Histological evaluation of excised tissue using H & E staining
Histological evaluation (Figure 54), of excised tissue using H & E staining
confirmed that the excise tissue is of rat ovary showing typical follicular structures
(primary and secondary) which are characteristic of ovarian structure and organization.
Figure 54. H & E staining of rat ovary (scale bar 100 µm)
4.4.1.2. Evaluation of trabecular bone loss using micro CT analysis
Micro CT analysis of metaphyseal cancellous bone of normal and
ovariectomised rats (post 4 months) was carried out to evaluate the trabecular bone loss

117
both qualitatively and quantitatively. The analysis of 2D slices generated from micro CT
revealed disruption of the trabecular structure and thereby confirming trabecular bone
loss in ovariectomised rats which is evident from the Figure 55.
Figure 55. 2D slice from micro CT showing trabecular bone loss
The quantitative evaluation of various trabecular bone parameters such as
trabecular number (Tb.N), trabecular thickness (Tb.Th), trabecular spacing (Tb.Sp),
trabecular density and ratio of bone volume to total volume (BV/TV) of normal and
ovariectomised rats is summarized in Table 11.
Table 11.Trabecular bone parameters measured from micro CT
Sample Tb.N 1/mm
Tb.Th mm
Tb.Sp Mm
Tb.density mg HA/ccm
BV/TV
Normal rat 3.6846 0.1622 0.2832 374.17 0.3897
Ovariectomised Rat
1.5938 0.1247 0.6507 276.83 0.2596

118
On comparison with normal rats, decrease in Tb.N, Tb.Th, Tb.density and
BV/TV and increase in Tb.Sp was observed for ovariectomised rats which validates the
induction of osteoporosis in rat animal model
4.4.1.3. Biochemical analysis of blood serum
The level of calcium, phosphorus and alkaline phosphatase (Figure 56 - 58) in
blood serum was evaluated before and after ovariectomy (2 & 4 week post
ovariectomy). The initial calcium level in blood serum before ovariectomy was of 8.17 ±
0.1 mg/dl and which was found to increase significantly to 9.0 ± 0.4 mg/dl and 11.4 ±
0.8 mg/dl respectively after 2 and 4 week post ovariectomy. The phosphorus level in
blood serum before ovariectomy was 4.04 ± 0.5 mg/dl which was found to increase
significantly to 4.63 ± 0.2 mg/dl and 6.2 ± 0.6 mg/dl respectively after 2 and 4 week post
ovariectomy. The initial value of ALP activity was of 145 ± 4.7 IU/L and after 2 and 4
weeks post ovariectomy, the ALP activity decreased to 132 ± 5.6 IU/L and 128 ± 4.7
IU/L respectively. Hence the increase in level of calcium and phosphorus after
ovariectomy and decrease in ALP activity confirms the osteoporotic model induction.

119
***** * *
Figure 56. Biochemical analysis of serum for calcium
*****
**
Figure 57. Biochemical analysis of serum for phosphorus

120
****
Figure 58. Biochemical analysis of serum for ALP activity
4.4.1.4. Body weight
The weight of rats was monitored before and after 1, 2 and 4 months post
ovariectomy. The loss of ovarian function in rats resulted in hyperphagia which resulted
in increased weight gain and adiposity which is evident in Figure 59. The percentage
weight gain observed in rats after 1, 2 and 4 months post ovariectomy was of 6.5 ±
3.5% , 16.4 ± 3.1% and 24.9 ± 4.3% respectively.

121
Figure 59. Weight gain in osteoporotic rats
4.4.2. In vivo bone formation evaluation
4.4.2.1. Gross evaluation of explants:
There were no complications observed in animals in association with the surgical
procedure to create the calvarial defect followed by the scaffold implantation. All the
animals survived and were available during the experiment period for further evaluation.
At definite time period (3, 6 and 12 weeks post implantation), the animals were
euthanized and the gross evaluation of the retrieved explants confirmed the absence of
any fibrous / inflammataory tissue formation (Figure 60). The gross evaluation also
confirmed the stern adherence of scaffolds to the defect area within the host tissue even
without any fixation and no signs of scaffold disintegration were observed.

122
Figure 60.: Gross morphology of explants
4.4.2.2. Radiographic evaluation
The qualitative analysis of bone mineralization using radiographic analysis
(Figure 61) depicted bone formation at the rounded edge of the rat calvarium with
increasing time period. The images revealed that the use of PCL/CEC/nHAP-PDS3
scaffolds (test group) enabled the regeneration of calvarial defect after 12 weeks post
implantation. The presence of PDS on PCL/CEC/nHAP scaffolds has promoted better
bone formation and had better healing effect on the defect area and on comparison with
PCL/CEC/nHAP scaffolds (control group), almost complete bridging of the defect site
was observed in PCL/CEC/nHAP-PDS3 scaffolds (test group).

123
Figure 61. Radiographic analysis of explants
4.4.2.3. Micro CT evaluation
The 3D morphometric images (Figure 62) obtained from micro CT analysis
clearly depicts the extend of new bone formation within the defect area. The level of
bone formation varied among the test and control group at different time periods. The
formation and integration of new bone tissue was more profound with the use of
PCL/CEC/nHAP-PDS3 scaffolds (test group) than that of PCL/CEC/nHAP scaffolds

124
(control group). It is clearly evident from the figure that almost complete bridging of
defect area with new bone was observed for test group after12 weeks post implantation.
Figure 62. Micro CT analysis of explants
The analysis of 2D slice of the defect area followed by the evaluation of bone
mineral density from micro CT further confirms the improved bone formation using the
test group at 12 weeks post implantation (Figure 63). The defect size got reduced and

125
more bony islands were observed thereby indicating the better osteogenic efficacy of
PCL/CEC/nHAP-PDS3 scaffolds. The quantitative measurement of density from the 2 D
slice reveals that the newly formed bone exhibited density which was almost comparable
to the host bone in the test group. Whereas in the case of control group (Figure 64), i.e.,
for defect area treated with PCL/CEC/nHAP scaffolds, bone formation was more
prominent on one of the interface of defect area.
Figure 63. Density of new bone at the defect area of test group measured using
micro CT

126
Figure 64.Density of new bone at the defect area of control group measured using
micro CT
4.4.2.4. Histology analysis
The explants after processing were stained with Stevenal’s blue & van Gieson’s
picrofuchsin and were analyzed. The stitched image showing the entire defect area and
one of the bone-implant interface is depicted in the figures 65 and 66. It was observed
that the level of healing was much slower in the control group compared to that of test
group. After 3 and 6 week post implantation, not much improvement in bone formation
was observed and at 12 weeks post implantation, the new bone formation at the bone
implant interface with cellular infiltration was observed.

127
Figure 65. Histological analysis of control group
However in the test group (defect area treated with PCL/CEC/nHAP-PDS3
scaffolds), the healing effect was more effective and even at 3weeks, new bone
formation was evident at the bone-implant interface. The better osteoingeration of test
group was revealed by the observation of bone formation within the defect area as well
as at the bone material at 6 and 12 week post implantation.

128
NB – new bone, HB – Host Bone , M – Material, CI – Cellular infiltration
Figure 66. Histological analysis of test group
4.4.2.5. Histomorphometry
The results of histomorphometric analysis (Figure 67.) further confirm that the
new bone formation was more pronounced with the use of PCL/CEC/nHAP-PDS3
scaffolds rather than that of PCL/CEC/nHAP scaffolds. The regeneration ratio observed
after 12 weeks was of 0.159 ± 0.006 for PCL/CEC/nHAP-PDS3 scaffolds and 0.058 ±
0.005 for PCL/CEC/nHAP scaffolds respectively.

129
3W 6W 12W
Figure 67. Histomorphometrical analysis showing regeneration ratio of test and
control group at different time period

130
CHAPTER 5
DISCUSSION
Chapter 5 details the discussion and interpretation of the results presented in
Chapter 4. The major findings of this study are correlated with published literature in the
relevant field and interpretations made wherever possible.
5.1. Development of biodegradable and bioactive scaffolds based on PCL
with improved hydrophilicity, biodegradability and better cell viability
PCL is one of the widely explored polymers for biomedical application
especially in the area of bone tissue engineering as well as drug delivery. The major
feature which attracts the biomaterial researchers is its FDA approval which allows its
safer use in humans. Moreover, its compatibility with wide variety of polymers along
with good processability, excellent biocompatibility, biodegradability and relatively low
cost makes PCL an excellent candidate as scaffolding material for tissue engineering and
drug delivery applications (Shalumon et al., 2010; Wutticharoenmongkol et al., 2006).
The inherent hydrophobic nature of PCL results in long degradation period of about 2-3
years which recommends its suitability for long term implants (Bölgen et al., 2005; Nam
et al., 2007).
However the hydrophobicity of PCL limits its use as a functional scaffold as it is
unfavourable for cell adhesion, migration, proliferation, and differentiation (Fabbri et
al., 2010; Kim et al., 2006)). Different strategies have been adopted by researchers to

131
improve hydrophilicity of PCL scaffolds which includes blending or copolymerizing
with hydrophilic polymers (Wang et al., 2011; Bajgai et al., 2008; Shafiee et al., 2011;
Chong et al., 2007; Oh et al., 2003)).
Besides improving the hydrophilicity, the cellular response as well as the
mechanical properties of PCL can be improved by incorporating bioactive nHAP
particles. The excellent biocompatibility, bioactivity, osteoconductivity and direct
involvement in bone cell differentiation and mineralization makes nHAP suitable for
bone tissue engineering applications. The advantage of using nHAP is its structural
similarity to the mineral component of the bone. Moreover nHAP has the ability to
induce mesenchymal stem cells differentiation towards osteoblasts. Studies have shown
that nHAP particles enhance protein adsorption and cell adhesion to the internal surfaces
of the scaffold and improve both mechanical and biological properties. However the use
of nHAP alone is limited due to its inherent brittle nature. Hence studies involving
composites based on nHAP and biodegradable polymers are promising and are being
carried out extensively with the aim to confer high bioactivity and adequate mechanical
properties to the scaffolds.
In this section, the study focus on improving the hydrophilicity, degradation
behaviour and cellular response of PCL scaffolds by blending with the synthesized
copolymer CEC as well as by incorporating nHAP particles. The copolymer CEC was
successfully synthesized by the ring-opening copolymerization of ε-CL initiated by PEG
using stannous octoate as catalyst. The reaction was carried out in bulk with a monomer
to initiator ratio of 2:1 (w/w) at 130oC for a period of 3 hours. Yield obtained (90%)

132
indicates that the feed ratio was almost retained in the prepared polymer. PEG is a non
toxic biocompatible polymer which is soluble in water and organic solvents. The
absence of antigenicity and immunogenicity allows PEG to be used for many clinical
applications (Bramfeldt al.,2007). Though PEG is not susceptible to hydrolysis; its
incorporation into the polymer backbone has been shown to enhance the rate of
degradation by improving the hydrophilicity (Shafieyan et al., 2011).
With the aim to modify PCL, the copolymer CEC was synthesized and
chemically characterized and confirmed using FTIR and NMR analysis.. The GPC
analysis revealed that the copolymer CEC exhibited narrow molecular weight
distribution with number and weight average molecular weight of 5508 and 7305
respectively. The nHAP particles gifted by Bioceramic Laboratory was characterized for
its size using TEM and particle size analyzer. TEM analysis depicted rod shaped
particles of 12-35 nm width and 90-120 nm length. The average particle size of nHAP
particles measured by particle size analyzer was of 89 nm with polydispersity index of
0.292.
Electrospinning technique provides a simple and direct way for developing novel
functional biomaterials. The proper choice of material components and their
combination in appropriate ratio enables one to tailor the physical and biological
properties of the resultant electrospun fibers such as hydrophilicity, mechanical modulus
and strength, biodegradability, biocompatibility, and specific cell interactions (Liang et
al., 2007). In this study, electrospinning technique has been explored to fabricate
scaffolds based on PCL, PCL/CEC blend and their nHAP filled composites.

133
Comparative evaluation of the physical and biological properties of the scaffolds (PCL,
PCL/CEC, PCL/nHAP and PCL/CEC/nHAP) was carried out to evaluate their
applicability for bone tissue engineering applications. The PCL/CEC blend ratio and
nHAP weight percentage used for the study was of 80:20 ratio and 2 wt% (optimized
based on preliminary mechanical property evaluation).
The selection of suitable solvent for electrospinning is crucial since it affects the
fiber morphology and diameter. DCM is a good solvent for PCL, however using it alone
results in formation of fibers with large fiber diameter. Hence the solvent DMF with
high dielectric constant was also added so as to improve the fiber formation as well as to
get fine fibers. The spinning was done using DCM/DMF solvents mixtures in 80:20 v/v
ratio at predetermined optimized condition of 10 % concentration, feed rate of 1mL/h,
applied voltage of 10-13 kV, mandrel speed of 500 rpm and needle to collector distance
of 13 cm so as to get bead free fine fibers.
The morphology and diameter of fibers depends on the conditions of
electrospinning process (Han et al, 2010, Huang et al., 2003). The morphological
features of the scaffolds analyzed by SEM (Figure 16) revealed random nonwoven
fibrous architecture with PCL having a fiber diameter around 1.53 µm. It was observed
that blending PCL with the copolymer CEC resulted in smooth fibers with reduced fiber
diameter. This reduced fiber diameter observed for the blend scaffold can be attributed
to the difference in solution viscosity between PCL and PCL/CEC (80/20) blend. The
nHAP incorporation has altered the surface texture of PCL fibers. Similar phenomenon
was observed by Wutticharoenmongkol et al. in electrospun PCL with incorporation of

134
nHAP particles (Wutticharoenmongkol et al., 2006). Lao et al. has reported that PLGA
nanofibers with varying HAP content have introduced surface roughness (Lao et al.,
2011). The decreased fiber diameter exhibited by PCL/nHAP composite scaffold can be
attributed to the presence of calcium and phosphate ions in nHAP which has imparted
higher conductivity (Jose et al., 2010). Chuenjitkuntaworn et al. has reported regarding
decrease in fiber diameter of PLLA/HAP composite fibers in comparison with neat
PLLA which was reported to be observed due to the increase in the restriction to flow
due to the presence of HAP particles Chuenjitkuntaworn et al., 2010).
The porosity of scaffolds plays vital role in their biological performance as it
determines both cell–cell as well as cell scaffold interaction. High porosity, adequate
pore size and interconnected pore network are essential criteria for a tissue engineering
scaffold as it enables better cell infiltration and vascularisation. Micro CT analysis
revealed the porous nature of the scaffolds and it was observed that electrospun PCL
was highly porous with percentage porosity of about 92 % and an average pore size of
48 µm. Compared to PCL, both copolymer blended and nHAP incorporated composite
scaffolds exhibited reduced percentage porosity and average pore size. The reduction in
pore size occurs as more layers of fibers might overlap with each other, especially when
the fiber diameter is smaller, resulting in smaller pore diameter (Li et al., 2002). It was
observed that the pore size distribution lies in a range below 100 µm for all the scaffolds
(Figure 19). The preferable pore size for osteoblast cells ranges from 200 to 400 µm for
encouraging migration, attachment and proliferation. However for electrospun matrices
pores formed are much smaller than the normal cell size of a few to tens of micrometer.

135
Pores in an electrospun structure are formed by the randomly oriented fibers lying
loosely upon each other. Cells can migrate through pores by their amoeboid movement
and can push surrounding fibers aside to expand the pore. This dynamic architecture of
fibers allows cells to adjust according to pore size and grow into nanofiber matrices (Li
et al., 2002).
Surface properties of scaffolds such as wettability, chemistry and roughness have
significant influence on appropriate cell response. The hydrophilic/hydrophobic
characteristic of scaffold can influence the initial cell adhesion and cell migration to a
greater extend (Masaeli et al., 2012; Cao et al., 2011).
Surfaces with moderate
hydrophilicity will promote better cell adhesion, proliferation and cellular activities. The
surface of PCL and PCL/nHAP scaffolds were hydrophobic indicated by their higher
contact angle value of 119 ± 2° and 112 ± 1° respectively. Blending PCL with
copolymer CEC resulted in imparting hydrophilicity which was reflected by the
complete wetting of scaffolds by the water drop within few seconds. It has been reported
by Li et al. that incorporating PEG moiety in the polymer backbone improves the
hydrophilicity of multiblock copolymers with respect to PCL homopolymer (Li et al.,
1998).
The mechanical properties of scaffolds are significant as the scaffold must be
strong enough to resist the forces from body movement or outer environment and must
also keep its structural integrity during the initial stages of the new bone formation. For
electrospun fibers, the mechanical properties are closely related to the fiber orientation,
bonding between fibers and fiber slippage rather than the mechanical properties of

136
individual fibers. The evaluation of both static and dynamic mechanical properties of the
scaffolds confirmed the enhancement of mechanical properties of electrospun PCL with
incorporation of both CEC and nHAP. Liao et al. in their studies with Poly (L-
lactide)/Poly(ε-caprolactone) blend fibers observed that the tensile strength of the blend
was reduced owing to the porous nature of the electrospun membranes which were
compared with that of cast film (Liao et al., 2011). Studies on PCL/multiwalled carbon
nanotubes (MWCNTs) composites by Meng et al. reported that nanocomposite fibers of
PCL with 0.5 wt.% MWCNTs with less agglomeration and finest fiber size had better
mechanical properties (Meng et al., 2010). The dynamic mechanical properties of the
scaffolds evaluated using DMA also revealed the significant enhancement in the storage
modulus of PCL with incorporation of both CEC and nHAP. As discussed earlier,
scaffolds with smaller fiber diameters will provide higher overall relative bonded areas
between fibers due to the increased surface area, bonding density, and better distribution
of bonds. PCL and PCL/CEC/nHAP composite scaffold exhibited comparable glass
transition temperature. However, slight decrease in Tg
for both nHAP and CEC
incorporated scaffolds was observed which may be due to the enhancement in the chain
flexibility of PCL. Bianco et al. has reported that decrease in Tg
of electrospun poly(L-
lactic acid)/Ca-deficient-hydroxyapatite composites with increasing filler content may
be due to the enhancement in the chain mobility of poly(L-lactic acid) (Bianco et al.
2009). In comparison, results of both static and dynamic mechanical properties reveals
that blending with copolymer CEC and incorporation of nHAP has significantly

137
increased the strength of PCL scaffold. On comparison, the PCL/CEC/nHAP composite
exhibited superior mechanical properties.
Apart from favourable physico-chemical and mechanical properties, the most
important requirement for a biomaterial is its biocompatibility in a specific environment,
together with the non cytotoxicity of its degradation products (Gomes et al., 2001). One
of the main reasons for choosing PCL for the present study is its slow degradation.
Degradation of PCL occurs mainly by hydroxylation and fragmentation of high
molecular weight chains, followed by changing to carbondioxide and water in the
environment of water or body fluid with or without enzyme. ESEM analysis of the
scaffolds after 3 months of of PBS incubation depicted fibre rupture as well as fiber
thinning. The incorporation of CEC has enhanced the degradation of PCL which was
reflected by the significant drop in the tensile strength of the PCL/CEC/nHAP composite
scaffold. This was mainly due to the hydrophilicity imparted by the introduction of
copolymer CEC which allows the more water molecules to diffuse into the polymer and
thereby enhancing degradation.
As a preliminary step towards the evaluation of cytocompatibility of the scaffold,
MTT assay was performed using L929 cell lines and the result revealed the non-
cytotoxic nature of all the scaffolds with more than 80 % viability. The attachment,
viability and proliferation of cells on the scaffold determine the suitability of the
material for the intended application. The electrospun fibrous scaffolds were assessed
for its ability for cell attachment, viability and proliferation in vitro using RADMSCs
which showed favourable interaction with all the fibrous scaffolds. The initial cell

138
attachment and spreading are significant factors in developing scaffolds for tissue
engineering. The morphology of the cells after seeding provides a wealth of information
regarding the interaction between the scaffold and cells. The morphology of RADMSCs
that adhered to the scaffold at different time period was examined using ESEM (Figure
31). The RADMSC cells expanded on the scaffolds with anchoring ligands stretching
out to attach themselves on the fiber surface. ESEM micrographs revealed that the
electrospun fibroporous architecture of PCL, PCL/CEC and their nHAP incorporated
scaffolds could provide a suitable ECM-like environment for the cells to attach and
proliferate. During 2 h, the RADMSCs exhibited a small spherical shape, a typical non-
adherent and non-spreading morphology. With increasing time period cells actively
proliferated on the scaffolds and after 5days the spreading of cells was more pronounced
on the PCL/CEC/nHAP composite scaffold indicating their superior cellular response.
The fibroporous architecture of scaffold allowed the cells to adhere, proliferate and to
migrate into the scaffold and confirmed that the porosity and pore size of the scaffolds
were sufficient for tissue engineering applications.
The qualitative determination of viability of ADMSCs using cLSM depicts high
ratio of viable green cells homogenously distributed over all the scaffolds (Figure 27).
All the fibrous scaffolds showed increase in cell viability and cell number with culturing
period. The higher LDH value of PCL/CEC/nHAP composite scaffold suggests that
more viable cells were present on this composite scaffold compared to neat PCL. The
cell number on the fibrous scaffolds determined by picogreen analysis was also found to
increase during the culture period of 28 days. The number of osteogenic-induced

139
RADMSCs was also significantly higher on PCL/CEC/nHAP composite scaffold at a
later time period of 28 days than other scaffolds. The enhanced viability and
proliferation of cells on PCL/CEC/nHAP composite scaffold can be attributed to the
scaffold’s greater hydrophilicity, and the presence of osteoconductive nHAP particles
which may be responsible for stimulating cell proliferation and differentiation. ALP
activity of osteogenic induced ADMSC on fibrous scaffolds was further demonstrated
by ELF-97 staining followed by cLSM investigation (Figure 30). Alkaline Phosphatase
(ALP) is an enzyme secreted by osteoblasts that is normally present in high
concentration in growing bone, essential for the deposition of minerals and is considered
as an early bone marker (Nair et al., 2009). These observations confirm the bioactivity
and osteoconductivity of the PCL/CEC/nHAP composite scaffold and its usefulness in
bone tissue engineering as a template for cell adhesion, proliferation and differentiation
into the specific bone lineage.
5.2 Development of pamidronate incorporated PCL based scaffolds
The simplicity of electrospinning technique has been utilized for fabricating PDS
loaded PCL based scaffolds so as to enhance the biofunctionality of the scaffold. Three
different loadings of drug PDS has been incorporated on PCL, PCL/CEC blend and
PCL/CEC/nHAP composite scaffold and a comparative evaluation was carried out to
choose an appropriate scaffold for in vivo studies.
PDS belongs to the family of aminobisphosphonate drug which is widely used
for the clinical treatment of bone related loss associated with osteoporosis, paget diseae,
hypercalcemia etc (Wilkinson and Little, 2011; Groff et al., 2001; Wang et al., 2014;

140
Fan et al., 2005) Since the oral administration of bisphosphonate drugs is associated
with drawbacks such as poor bioavailability and gastrointestinal ulcerations, it is
expected that the local delivery of these drugs at the defect site can enhance its efficacy.
On reviewing literature, only a few works has been reported on the developments of
electrospun polymeric scaffolds for the delivery of bisphosponates ( Puppi et al., 2010;
Lu et al 2011; Yun et al 2014) To the best of our knowledge, no studies have been
reported in literature on the delivery of PDS from electrospun PCL scaffolds.
The successful incorporation of drug PDS on to PCL, PCL/CEC blend and
PCL/CEC/nHAP composite scaffolds were revealed by the morphological anaysis using
ESEM. All the scaffolds exhibited beadless smooth fibers with reduced fiber diameter.
The significant reduction in the fiber diamter observed for PDS incorporated scaffolds
could be related to the conductivity measurement values (Table 8). The PDS
incorporation has improved the solution conductivity of PCL based scaffolds. Generally
during electrospinning process, increased solution conductivity will impart more electric
charges to the electrospinning jet which results in higher elongation forces under
electric field. Moreover increased solution conductivity will also cause more bending
instability which increases the jet path and more stretching of spinning solution. Hence
this reduction in fiber dimater observed for PDS incorporated scaffolds also suggest the
homogenous distribution of the drug PDS in the scaffolds. There was no aggregates of
drug on the fiber surface.
An ideal tissue engineering scaffold must be porous so as to facilitate cell
seeding and to enable gaseous and nutrient exchange. Porosity measurement by ethanol

141
intrusion method revealed the porous nature of PCL and PDS incorporated scaffolds.
The surface wetting behaviour of PCL scaffolds was influenced by the incorporation of
hydrophilic PDS. PCL is inherently hydrophobic in nature owing to presence of five
CH2 groups. Imaparting hydrophilicity can have positive impact on the biological
performance of the scaffolds. The incorporation of hydrophilic PDS altered the surface
wetting behaviour of PCL scaffolds which is indicated by the decreased contact angle
value of 36° for PCL-PDS5 scaffolds. However for PCL/CEC and PCL/CEC/nHAP
scaffolds, contact angle couldnot be measured as complete wettiing of scaffolds with
water was observed.
Besides improving surface wettability, mechanical perfomance of scaffolds were
also enhanced with PDS incorporation. When PDS content was of 5 %, the tensile
strength of PCL scaffolds increased from 5.2 MPa to 13.4 MPa and for that of
PCL/CEC scaffolds, tensile strength increased from 7 MPa to 11.5 MPa. However for
the PCL/CEC/nHAP composite scaffolds, there was no significant difference in tensile
strength after PDS incorporation. The superior mechanical properties of PDS scaffolds
observed in PCL and PCL/CEC blend scaffolds can be attributed to the improved
solution conductivity which favoured the formation of fibers with reduced fiber
diameter.
Dynamical mechanical analysis showed that storage modulus of scaffolds
enhanced with PDS incorporation for PCL scaffolds and there was not much difference
in the Tg values observed for scaffolds. PCL exhibited Tg around - 47.7 °C whereas for
PDS incorporated scaffolds Tg ranged from - 48 °C to - 49 °C. For PCL/CEC blend and

142
PCL/CEC/nHAP composites scaffolds, storage modulus dropped with PDS
incorporation and increase in Tg was observed.
It is difficult to dissolve hydrophilic PDS into hydrophobic PCL scaffolds. Hence
the successful incorporation and sustained release of hydrophilic PDS is a challenge.
Studies have shown that amphiphilic block copolymers like PEG-b-PCL have been
reported to incorporate hydrophilic drugs into hydrophobic polymers by electrospinning
to produce controlled-release nanofibrous scaffolds (Kim et al., 2004). In vitro relase
studies in PBS at 37 °C showed that all the scaffolds exhibited quick release of PDS
during the initial time period of about 12 h. The initial amount of drug release vary as a
function of PDS content and its distribution in the scaffold. The initial quick release of
PDS can be attributed to the release of drug which is localized on the fiber surface.
When the drug concentration is increased, the drug molecules may aggregate more on
the fiber surface, which would lead to an even larger initial burst of drug as seen in the
scaffold with 5 wt% of drug loading. In our study it was observed that the drug release
from PCL/CEC blend scaffolds was higher than that of PCL and PCL/CEC/nHAP
composite scaffolds suggesting the enhancement in drug release with incorporation of
CEC. However, the presence of nHAP in the composite scaffold enabled sustained
release of drug from the scaffold.
The incorporation of PDS has influence on the degradation behaviour of
scaffolds. PCL is a slow degrading polymer having a degradation time of about 2 to 3
years owing to its inherent hydrophobic nature. It was observed that PDS incorporation

143
accelerated the degradation behaviour which was revealed by the thinning and rupture of
fibers observed after 3 months of PBS ageing (Figure 43). This was further substantiated
by the results of tensile strength of scaffolds observed after 3 months of PBS ageing.
The tensile strength of scaffolds decreased with PBS ageing and the drop in tensile
strength was more prominent on PDS incorporated scaffolds. For PCL, after 3 months of
PBS ageing, tensile strength dropped by 26 % whereas in case of PCL-PDS scaffolds,
the drop in tensile strength was more prominent on PCL-PDS5 scaffolds which was
about 68%. This drastic drop in tensile strength of PCL-PDS5 scaffolds was mainly due
to the improved hydrophilicity imparted by PDS incorporation which is reflected by its
lower contact angle value of 36°. The study also demonstrated that higher the PDS
content, the more is the chance of PDS to be located on the scaffold surface which can
be easily dissolved and washed out using PBS resuting in faster degradation. For
PCL/CEC blend scaffolds, incorporation of hydrophilic CEC and PDS further enhanced
the degradation profile of PCL scaffold showing about 77% drop in tensile strength for
PCL/CEC-PDS5 scaffolds. In case of PCL/CEC/nHAP composite scaffolds, owing to
the presence of nHAP particles the drop in PCL/CEC/nHAP-PDS5 scaffolds was of
only 55 %. However all the scaffolds maintained their structural integrity in the original
dimension till the end of the experiment.
The in vitro biocompatibility of PDS loaded scaffolds were assessed using hOS
cell lines to evaluate the effect of PDS on the cell viability and proliferation. The hOS
cells were used for the study as they maintain the cellular features of osteoblasts. The
results suggested that PDS was not toxic to hOS cells, highlighting that PDS loaded

144
scaffolds provides a favourable microenvironment for osteogeneic ability. The scaffolds
favoured the adhesion of hOS and maintained their typical spindle morphology as
revealed by the live/dead assay (Figure 46). However at higher PDS content, cells lost
their spindle morphology. The quantification of cell viability using MTT assay after 48h
indicated that all the scaffolds had favorable interaction with cells and the cells were
viable on all the scaffolds proving their cytocompatibility.
The PCL/CEC/nHAP composite scaffolds were selected for the in vivo study
based on the physico-mechanical properties and was further evaluted for in vitro
cytocompatibility using rat’s adipose derived mesenchymal stem cells (rADMSC). Rat
ADMSCs were chosen since the potential of the scaffolds has to be evaluated in a rat
animal model. The MTT assay using un-induced rADMSC proved the cytocompatibility
of the scaffolds with more than 90% cell viability and on comparison it was observed
that cell viability was more prominent on PCL/CEC/nHAP-PDS3 scaffolds. Studies by
Ponader et al have showed that pamidronate has the ability to affect positively the
vitality of human osteoblasts in a concentration dependent manner. It was observed that
the lowest pamidronate accumulation led to the highest enhancement of osteoblast
vitality. Higher concentrations of pamidronate seem to block the anabolic effect
(Ponader et al., 2008). This finding correlates with the conclusion of Correia et al., who
found a cytotoxic effect of alendronate, one of the most potent osteoclast inhibitors
among bisphosphonates, in higher concentrations (Correia et al., 2006). This effect
could be explained by the dual effect of bisphosphonates, influencing the calcification,

145
which seems to be elevated in low bisphosphonate doses and the bone resorption, which
is dominant in higher doses.
Live/dead assay using actin staining depicted the viable rADMSCs adhered on
the fibrous scaffolds (Figure 51). It was observed that cells maintained their
characteristic spindle morphology only at lower PDS content. The disruption in
morphology at higher PDS i.e. on PCL/CEC/nHAP-PDS5 scaffolds was observed.
The ability of scaffolds to support the attachment of un-induced rADMScs after
24 h (Figure 52) and osteogenic induced rADMSCs after 14 days was analyzed using
ESEM analysis (Figure 53). The cells adhered well on all the scaffolds and interestingly
it was observed that the un-induced rADMSCs after 14 days of osteogenic induction
synthesized mineralized nodules on scaffold surface proving their osteogenic efficacy.
Similar findings were observed by Venugopal et al in which mineralization was
observed in PCL/HAP-modified nanofibrous scaffolds (Venugopal et al., 2008). Hence
the PCL/CEC/nHAP-PDS3 scaffolds were chosen for the in vivo based on its enhanced
physico-mechanicl and biological properties..
5.3. In vivo evaluation of PDS incorporated PCL based scaffold in a rat animal
model
After the in vitro biofunctional assessment, the in vivo osteogenic potential of the
fabricated PCL/CEC/nHAP-PDS3 scaffolds was evaluated under in vivo conditions as a
critical indicator for future clinical translational application. The present study is an
attempt to explore the potential of local delivery of PDS in healing rat calvarial bone

146
defect under osteoporotic conditions. Rat animal model was chosen for the study as it is
the FDA recommended preclinical small animal model for evaluating the potential of
pharmaceutical agents intended for osteoporosis treatment (Reinwald & Burr, 2008,
Colman, 2003). No single animal model precisely mimics all the characteristics of
human osteoporosis. However there are different strategies for inducing osteoporotic
conditions in animals which includes ovareiectomy, low calcium diet, steroid usage etc.
Among these, ovariectomized animals are widely accepted for bone loss related research
since they closely mimics the physiological condition of postmenopausal osteoporosis.
The high reproducibility of ovariectomized animal model and the bone loss associated
with estrogen deficiency makes rat an ideal candidate for inducing osteoporosis.
The first phase of the in vivo study was to develop osteoporosis in rat animal
model and to validate the model induction. To induce osteoporosis, 4 months aged
female wistar rats were subjected to bilateral ovariectomy and kept for a period of four
months for model induction. A time period of 3 to 4 months is usually provided after
ovariectomy for inducing osteoporotic condition. The surgical procedure adopted was
bilateral ovariectomy in order to remove the ovaries so as to induce estrogen deficiency
which could result in osteoporosis. There were no signs of complications observed
during as well as after the surgery.
The removed ovarian tissue after surgery was further analyzed by histology using
H & E staining (Figure 54) which depicted typical follicular structures thereby
confirming that the excised tissue is of rat ovary. In order to further validate the
trabecular bone loss associated with ovariectomy, the metaphyseal cancellous bone area

147
at the tibial head of normal rats and ovariectomised rats after 4 months of induction was
quantitatively and qualitatively analyzed and compared by micro CT analysis.
Since bone loss associated with osteoporosis is more evident in trabecular area,
measurement of trabecular bone parameters enables the confirmation of osteoporotic
model induction. As expected, the effect of ovariectomy was marked by the disruption
of trabecular network in case of ovariectomised rats (Figure 55) as well as decrease in
various trabecular parameters such as Tb.N, Tb.Th Tb.density and BV/TV. Similar
observations were reported by Majumdar et al on the effect on trabecular micro-
architecture after osteoporosis induction (Majumdar et al., 1997).
The analysis of serum showed increase in serum calcium and phosphorus level as
well decreased serum ALP level which further supports the bone loss in the induced rat
animal model. As a secondary effect of ovariectomy, weight gain was observed in
animals which further confirm the model induction. Hence the results of histological
analysis, µ-CT and blood serum analysis confirm the development and validation of
osteoporosis in rat animal model.
The second phase of the in vivo study was to create calvarial defect in the
developed osteoporotic rat animal model and to evaluate the efficacy of the fabricated
scaffolds in healing the defect. The PCL/CEC/nHAP-PDS3 scaffold was chosen as the
test material and that of PCL/CEC/nHAP composite scaffold as the control material for
the study based on the physico-mechanical properties and in vitro assessment. The
defect site chosen was of calvaria and 8 mm critical size defect (Szpalski et al, 2010)
was created using dental burr. The calvarial defect site offers advantage of not requiring

148
any internal fixation devices and eliminates the dislocation of implant associated with
the motion of animal.
The gross evaluation of explants confirms the proper fixation of scaffold to the
defect site and absence of any inflammatory responses. The implanted scaffolds were
well integrated into the calvarial bone defect. The scaffolds adhered strictly to the host
bone tissue even without any fixation. There were no mortality or complications
observed in animals during the period of our study. No signs of bleeding, wound fester,
infection, scalp edema, or effusion were seen at the site of surgery.
The bone regenerative capacity of scaffolds analyzed by radiography revealed
bony infiltrations in the cavity after 12 week post implantation with the use of
PCL/CEC/nHAP-PDS3 scaffolds (test group). These results were further confirmed by
the µ-CT data which presented more detailed bone regeneration. Almost complete
bridging of the defect site was evident after 12 weeks post implantation with the use of
PCL/CEC/nHAP-PDS3 scaffolds (test group) in comparison with that of
PCL/CEC/nHAP(control group).
The extend of mineralization (in-terms of bone density) was assessed from the
density histograms generated from 2 D slice of the defect area treated with control and
test group (included host bone and de novo bone). The defect area treated with
PCL/CEC/nHAP-PDS3 scaffolds (test group) exhibited better osteointegration as the
bone density (in terms of mg HA/ccm) of the new bone equalised to that of the host
bone, indicating improved mineralization efficiency. However, new bone formed with
the use of control group scaffolds in the defect area exhibited poor mineralization

149
efficiency as compared to the mineral content of host bone. Results indicate that PDS
loaded PCL/CEC/nHAP scaffolds exhibited better matrix formation, with promising
results which is probably as a result of release of PDS at the defect area from the test
group. The PDS released from PCL/CEC/nHAP-PDS3 scaffolds may have positively
regulated the excessive mineralization along with the inherent bioactivity of nHAP.
Similar findings were observed by Yu et al in which the local co-delivery of BMP /
pamidronate using poly-D, L-lactic-acid implants have improved calvarial bone defect
healing in healthy rat models (Yu et al., 2010).
Histological analysis using Stevenal’s blue and van Gieson's picrofuchsin
staining was carried out to determine the area of cells infiltered around and within the
defect area as well as the newly formed bone area (Figure 65-66). Stevenal's blue stains
cells and extracellular structures in a subtle gradation of blue tones and van Giesen's
picrofuchsin bone as orange or purple and osteoid matrix as yellow green. It was
observed that defect area treated with test group scaffolds exhibited new bone formation
at the bone implant interface after 3 week post implantation. With increasing time
period, i.e., after 12 week post implantation new bone formation was observed within
the defect area (bridging of defect site) as well as at the bone implant interface further
confirming the better osseointegration. In case of defect area treated with control
scaffolds, cellular infiltration with new bone formation was observed only at the bone
implant interface after 12 week post implantation and no bridging of defect site was
observed. The osteogenic efficacy of scaffolds in terms of regeneration efficiency (RE)
ratio (New bone formed per total defect area of the implant materials) obtained from the

150
histomorphometric analysis further substantiate the results of histology data revealing
that the new bone formation was more pronounced with the use of test scaffolds and
significant difference exist in new bone formation between test and control scaffolds
after 3, 6 and 12 week post implantation (Figure 67). The result of in vivo bone
regeneration studies reveals that the PDS incorporated scaffolds promoted the
reconstruction of calvarial defect in osteoporotic rat. This study shows proof-of concept
that the local delivery of pamidronate using PCL based scaffold have the potential to
improve bone formation and thus may have translational applications for maximising
bone formation in mechanically unfavourable environments.
5.4. Limitations of Study
The present study explored the feasibility of electrospinning technique for the
fabrication scaffolds based on PCL for bone tissue engineering application. The study
undertook the modification of PCL scaffolds in order to improve its surface wettability,
mechanical properties, degradation behaviour and cellular response and evaluated its
applicability for osteoporotic bone defect repair. It was also made sure that the relevant
properties required for a scaffolding material to be used for bone tissue engineering
applications have been evaluated. However, the study lacks the effect of PDS on
osteoclast activity, which is an important criteria which could not be evaluated due to
limitations.
5.5. Future perspectives
Extension of the work into large animal models will be the final criteria in
deciding the potential application of these scaffolds in clinical practice.

151
CHAPTER 6
SUMMARY AND CONCLUSIONS
Bone fractures associated with osteoporosis is becoming a major concern all over
the world especially in the elderly population and in postmenopausal women.
Conventional treatment modality involves use of autografts, allografts, synthetic grafts
as well as pharmaceutical agents for treating osteoporotic fractures. However, the
scarcity of availability of tissues and organs for transplantation, donor site morbidity,
immune rejection, pathogen transfer associated with the use of grafts and that of poor
bioavailability and undesirable toxic side effects of pharmaceutical agents is a major
concern.
Tissue engineering emerged as a promising alternative to traditional osteoporosis
therapy. The scaffold based tissue engineering approach enables the delivery of cells,
growth factors as well as bioactive drugs at the defect site which helps in stimulating
bone formation. The main focus of the study was to design a scaffold based on PCL with
appropriate combination of mechanical properties, cellular response and at the same
time serving as matrix for sustained delivery of a pharmaceutical agent which can be
used for osteoporotic bone defect repair.
The present study utilized the electrospinning technique for fabricating
nanofibrous scaffolds based on synthetic biodegradable polymer PCL. The relatively
low cost, inherent biocompatibility and biodegradability, along with its FDA approval
makes PCL an ideal candidate as scaffolding material. The main concern in using PCL

152
as scaffolding material is its inherent hydrophobicity which results in slow degradation
rate as well as poor cellular response.
The primary objective of the present study is to address the above problem by
blending PCL with a hydrophilic polymer. With this aim, the copolymer PCL-PEG-PCL
(CEC) was successfully synthesized by the ring opening polymerization of ε-
caprolactone monomer using PEG as the macro initiator. The chemical characterization
of CEC using FTIR and NMR confirms its formation and GPC analysis revealed its Mw
as 7305. The copolymer CEC was incorporated on PCL scaffolds to modify its physical
and biological properties. In addition to the blending approach, developing composites
based on bioactive ceramics is an effective strategy to improve the cellular response and
mechanical performance of the scaffolds. Hence the present study also focussed on
incorporating nHAP particles into PCL and PCL/CEC blend scaffolds. The nHAP
particles used in the study was of rod shaped and the size was found to be in the range of
12-35 nm width and 90-120 nm length as revealed by the TEM analysis.
Nanofibrous scaffolds using PCL, PCL/CEC blend and their nHAP filled
composites were fabricated by electrospinning technique and evaluated for their physical
and biological properties to identify scaffold with superior properties suitable for bone
tissue engineering applications. The morphological features of the scaffolds analyzed by
SEM showed bead free fibers confirming that the spinning parameters were optimal. The
blending of PCL with the synthesized copolymer CEC resulted in smooth fibers with
reduced fiber diameter, improved hydrophilicity, superior mechanical properties and
enhanced degradation behavior. The nHAP incorporation resulted in fibers with rough

153
surface which may encourage better cellular response and reduced fiber diameter
thereby improved mechanical properties. The effect of CEC and nHAP incorporation on
the morphological properties, fiber diameter, pore size, percentage porosity, wettability,
mechanical properties and degradation behaviour of PCL scaffolds were also well
established in the study. The in vitro studies using RADMSCs revealed that fibroporous
architecture of scaffold allowed the cells to adhere, proliferate and migrate into the
scaffold and confirmed that the porosity and pore size of the scaffolds were sufficient for
bone tissue engineering applications. An overall enhanced performance was shown by
PCL/CEC/nHAP composite scaffold in cell viability (LDH assay) and proliferation
(Picogreen assay) studies. Among the different scaffolds, the PCL/CEC/nHAP
composite scaffolds exhibited superior performance in terms of physico-mechanical and
biological properties which can be attributed to the combined effect of hydrophilic CEC
and osteoconductive nHAP particles. Hence the results suggest that the PCL/CEC/nHAP
composite scaffold can be a promising candidate for bone tissue engineering
applications.
Pamidronate (PDS) is found to be an effective antiresorptive drug which has
been used clinically in treating fractures associated with osteoporosis. Studies have
shown that local delivery of PDS can improve the bone growth around dental and
orthopedic implants. As an initial step towards developing scaffolds for osteoporotic
bone defect repair, the study demonstrated the incorporation of different loadings of
PDS onto PCL, PCL/CEC blend and PCL/CEC/nHAP composite scaffolds and
evaluated the effect of PDS on the physico-mechanical and biological properties of

154
scaffolds. The study was designed to choose an appropriate scaffold with effective PDS
loading that can be for used in vivo studies. The drug PDS was successfully incorporated
on PCL, PCL/CEC blend and PCL/CEC/nHAP composite scaffolds which were
reflected by the reduced fiber diameter and enhanced surface wettability of scaffolds. In
vitro release study in PBS showed that sustained release of PDS was observed with the
PCL/CEC/nHAP composite scaffolds. It was observed that PDS incorporation didn’t
elicit any cytotoxic response towards hOS cells during in vitro studies. However it was
observed that at higher loadings of PDS, hOS cells lost their spindle morphology.
Similar findings were observed with in vitro studies using osteogenic induced rADMSCs
on PCL/CEC/nHAP composite scaffolds. The PCL/CEC/nHAP-PDS3 composite
scaffold was selected for the in vivo studies based on the physico mechanical properties
and in vitro release behavior.
The performance of the scaffolds under in vivo conditions was further evaluated
by developing and validating an osteoporotic rat animal model. The potential of
PCL/CEC/nHAP-PDS3 scaffold (test group) in healing 8 mm critical size calvarial
defects created in osteoporotic was evaluated for different time period and was
compared with that of the PCL/CEC/nHAP scaffolds (control group). Micro CT
evaluation of the explants confirmed the improved osteointegrative ability of PDS
incorporated scaffolds after 12 week post implantation. Histological analysis further
supports the results of µ-CT data and shows the better osteointegration of test group
indicated by the presence of bony islands within the defect area as well as at the bone-
material interface after 6 and 12 week post implantation.The PDS incorporation in

155
PCL/CEC/nHAP scaffolds aided osteogenesis which was further depicted quantitatively
in terms of regeneration efficiency ratio (new bone formed /total defect area).
The concept of local delivery of PDS at the implant site via PCL/CEC/nHAP
composite scaffolds demonstrated better osteogenesis and osteointegration under
osteoporotic condition. Our results suggest that incorporating PDS onto
PCL/CEC/nHAP scaffolds is a promising and effective method to construct tissue
engineering scaffolds utilising the combined effect of bioactivity of nHAP and the anti-
osteoporotic effect of PDS.
The study suggests that PCL/CEC/nHAP-PDS composite scaffolds can be used
as bone substitutes for local implantation into critical sized osteoporotic defects, owing
to the enhanced in vitro cell attachment, proliferation and osteogenic differentiation, and
accelerated in vivo healing progress on compared with PCL/CEC/nHAP scaffolds
(control group). The better cytocompatibility of scaffolds under in vitro conditions
supported by its performance under in vivo conditions in rat osteoporotic model predicts
the clinical application of tissue engineered PDS incorporated PCL/CEC/nHAP
scaffolds for osteoporotic bone defect repair.

156
BIBILOGRAPHY
Aggarwal N, Raveendran A, Khandelwal N, Sen RK, Thakur JS, Dhaliwal LK, Singla
V, Manoharan SR (2011) Prevalence and related risk factors of osteoporosis in
peri-and postmenopausal Indian women. Journal of mid-Life health. 2(2):81.
Aghdam RM, Najarian S, Shakhesi S, Khanlari S, Shaabani K, Sharifi S (2012)
Investigating the effect of PGA on physical and mechanical properties of
electrospun PCL/PGA blend nanofibers. Journal of Applied Polymer Science.
124(1):123-31.
Babel B. Investigations on bone metabolism in intact and ovariohysterectomised
miniature pigs (Doctoral dissertation, lmu).
Bagi CM, Ammann P, Rizzoli R, Miller SC (1997) Effect of estrogen deficiency on
cancellous and cortical bone structure and strength of the femoral neck in rats.
Calcified tissue international. 61(4):336-44.
Bajgai MP, Aryal S, Bhattarai SR, Bahadur KC, Kim KW, Kim HY (2008) Poly
(ϵ-caprolactone) grafted dextran biodegradable electrospun matrix: A novel
scaffold for tissue engineering. Journal of Applied Polymer Science.108(3):1447-
54.
Bianco A, Di Federico E, Moscatelli I, Camaioni A, Armentano I, Campagnolo L,
Dottori M, Kenny JM, Siracusa G, Gusmano G (2009) Electrospun poly (ε-
caprolactone)/Ca-deficient hydroxyapatite nanohybrids: microstructure,
mechanical properties and cell response by murine embryonic stem cells.
Materials Science and Engineering: C. A29(6):2063-71.
Blitch EL, Ricotta PJ. (1996) Introduction to bone grafting. The Journal of foot and
ankle surgery. 35(5):458-62.

157
Bölgen N, Menceloğlu YZ, Acatay K, Vargel I, Pişkin E (2005) In vitro and in vivo
degradation of non-woven materials made of poly (ε-caprolactone) nanofibers
prepared by electrospinning under different conditions. Journal of Biomaterials
Science, Polymer Edition. 16(12):1537-55.
Bramfeldt H, Sarazin P, Vermette P (2007) Characterization, degradation, and
mechanical strength of poly (D, L-lactide-co-ϵ-caprolactone)-poly (ethylene
glycol)-poly (D, L-lactide-co-ϵ-caprolactone). Journal of Biomedical Materials
Research Part A. 83(2):503-11.
Cao D, Wu YP, Fu ZF, Tian Y, Li CJ, Gao CY, Chen ZL, Feng XZ. (2011) Cell
adhesive and growth behavior on electrospun nanofibrous scaffolds by designed
multifunctional composites. Colloids and Surfaces B: Biointerfaces. 84(1):26-34.
Cauley JA, Chalhoub D, Kassem AM, Fuleihan GE (2014) Geographic and ethnic
disparities in osteoporotic fractures. Nature Reviews Endocrinology. 10(6):338-
51.
Chandran S, Babu S S, Varma HK, John A (2016) Osteogenic efficacy of strontium
hydroxyapatite micro-granules in osteoporotic rat model. Journal of biomaterials
applications. 31(4):499-509.
Cheng N, Dai J, Cheng X, Li SE, Miron RJ, Wu T, Chen W, Zhang Y, Shi B (2013)
Porous CaP/silk composite scaffolds to repair femur defects in an osteoporotic
model. Journal of Materials Science: Materials in Medicine. 24(8):1963.
Chong EJ, Phan TT, Lim IJ, Zhang YZ, Bay BH, Ramakrishna S, Lim CT (2007)
Evaluation of electrospun PCL/gelatin nanofibrous scaffold for wound healing
and layered dermal reconstitution. Acta biomaterialia.3(3):321-30.
Chuenjitkuntaworn B, Supaphol P, Pavasant P, Damrongsri D (2010) Electrospun poly
(L-lactic acid)/hydroxyapatite composite fibrous scaffolds for bone tissue
engineering. Polymer International. 59(2):227-35.

158
Colman EG (2003) The Food and Drug Administration's osteoporosis guidance
document: past, present, and future. Journal of Bone and Mineral Research.
18(6):1125-8.
Correia VD, Caldeira CL, Marques MM. (2006) Cytotoxicity evaluation of sodium
alendronate on cultured human periodontal ligament fibroblasts. Dental
Traumatology. 22(6):312-7.
Cunha MR, Santos Jr AR, Petinari L, Goissis G, Nonaka KO, Wang CC, Genari SC
(2010) Characterization of the physical and mechanical properties of femoral
bone defects filled with polyanionic collagen scaffolds in ovariectomized rats.
Materials Research. 13(2):239-44.
Elsalanty ME, Genecov DG (2009) Bone grafts in craniofacial surgery.
Craniomaxillofacial Trauma and Reconstruction. 2(03):125-34.
Fabbri P, Bondioli F, Messori M, Bartoli C, Dinucci D, Chiellini F(2010) Porous
scaffolds of polycaprolactone reinforced with in situ generated hydroxyapatite
for bone tissue engineering. Journal of Materials Science: Materials in
Medicine. 21(1):343-51.
Fan TM, Lorimier LP, Charney SC, Hintermeister JG. (2005) Evaluation of intravenous
pamidronate administration in 33 cancer-bearing dogs with primary or secondary
bone involvement. Journal of veterinary internal medicine. 19(1):74-80.
Fischer RL, McCoy MG, Grant SA. (2012) Electrospinning collagen and hyaluronic
acid nanofiber meshes. Journal of Materials Science: Materials in Medicine.
23(7):1645-54.
Gan Z, Liang Q, Zhang J, Jing X (1997) Enzymatic degradation of poly (ε-caprolactone)
film in phosphate buffer solution containing lipases. Polymer degradation and
stability. 56(2):209-13.

159
Galia CR, Moreira LF (2012) The Biology of Bone Grafts. InRecent Advances in
Arthroplasty InTech.
Ghasemi-Mobarakeh L, Prabhakaran MP, Morshed M, Nasr-Esfahani MH, Ramakrishna
S (2008)Electrospun poly (ɛ-caprolactone)/gelatin nanofibrous scaffolds for
nerve tissue engineering. Biomaterials. 29(34):4532-9.
Giannoudis PV, Schneider E. (2006) Principles of fixation of osteoporotic fractures.
Bone & Joint Journal. 88(10):1272-8.
Giger EV, Castagner B, Leroux JC (2013) Biomedical applications of bisphosphonates.
Journal of controlled release. 167(2):175-88.
Goldhahn J, Féron JM, Kanis J, Papapoulos S, Reginster JY, Rizzoli R, Dere W, Mitlak
B, Tsouderos Y, Boonen S (2012) Implications for fracture healing of current
and new osteoporosis treatments: an ESCEO consensus paper. Calcified tissue i
nternational. 90(5):343-53.
Gomes ME, Reis RL, Cunha AM, Blitterswijk CA, De Bruijn JD (2001)
Cytocompatibility and response of osteoblastic-like cells to starch-based
polymers: effect of several additives and processing conditions. Biomaterials.
22(13):1911-7.
Groff L, Zecca E, De Conno F, Brunelli C, Boffi R, Panzeri C, Cazzaniga M, Ripamonti
C. (2001) The role of disodium pamidronate in the management of bone pain due
to malignancy. Palliative medicine. 15(4):297-307.
Gross TP, Cox QG, Jinnah RH (1993) History and current application of bone
transplantation. Orthopedics. 16(8):895-900.
Han J, Branford-White CJ, Zhu LM (2010) Preparation of poly (ε-caprolactone)/poly
(trimethylene carbonate) blend nanofibers by electrospinning. Carbohydrate
Polymers. 79(1):214-8.

160
Heath CA. (2000) Cells for tissue engineering. Trends in biotechnology. 18(1):17-9.
Hollinger JO, Battistone GC. (1985) Biodegradable bone repair materials: synthetic
polymers and ceramics. ARMY INST OF DENTAL RESEARCH
WASHINGTON DC;
Huang ZM, Zhang YZ, Kotaki M, Ramakrishna S (2003) A review on polymer
nanofibers by electrospinning and their applications in nanocomposites.
Composites science and technology. 63(15):2223-53.
Jakob F, Ebert R, Ignatius A, Matsushita T, Watanabe Y, Groll J, Walles H (2013) Bone
tissue engineering in osteoporosis. Maturitas. 75(2):118-24.
Jee WS, Yao W (2001) Overview: animal models of osteopenia and osteoporosis. J
Musculoskelet Neuronal Interact.1(3):193-207.
Jose MV, Thomas V, Xu Y, Bellis S, Nyairo E, Dean D (2010) Aligned bioactive
multi-component nanofibrous nanocomposite scaffolds for bone tissue
engineering. Macromolecular bioscience. 10(4):433-44.
Kajiwara H, Yamaza T, Yoshinari M, Goto T, Iyama S, Atsuta I, Kido MA, Tanaka T
(2005) The bisphosphonate pamidronate on the surface of titanium stimulates
bone formation around tibial implants in rats. Biomaterials. 26(6):581-7.
Kim CH, Khil MS, Kim HY, Lee HU, Jahng KY (2006) An improved hydrophilicity via
electrospinning for enhanced cell attachment and proliferation. Journal of
Biomedical Materials Research Part B: Applied Biomaterials. 78(2):283-90.
Kim GM, Huyen K, Le T, Giannitelli SM, Lee YJ, Rainer A, Trombetta M. (2013)
Electrospinning of PCL/PVP blends for tissue engineering scaffolds. Journal of
Materials Science: Materials in Medicine. 24(6):1425.

161
Kim KH, Cui GH, Lim HJ, Huh J, Ahn CH, Jo WH. (2004) Synthesis and Micellization
of Star-Shaped Poly (ethylene glycol)-block-Poly (ε-caprolactone).
Macromolecular Chemistry and Physics. 205(12):1684-92.
Kumar KS, Bhaskar P. (2012) Osteoporosis-An Emerging Disease of the 21st Century,
Part 1: An Overview. Journal of family medicine and primary care. 1(1):66.
Labow RS, Meek E, Matheson LA, Santerre JP (2002) Human macrophage-mediated
biodegradation of polyurethanes: assessment of candidate enzyme activities.
Biomaterials. 23(19):3969-75.
Lao L, Wang Y, Zhu Y, Zhang Y, Gao C (2011) Poly (lactide-co-
glycolide)/hydroxyapatite nanofibrous scaffolds fabricated by electrospinning for
bone tissue engineering. Journal of Materials Science: Materials in Medicine.
22(8):1873-84.
Larsson S. Treatment of osteoporotic fractures. (2002) Scandinavian journal of surgery.
1(2):140-6.
Laurencin C, Khan Y, El-Amin SF (2006) Bone graft substitutes. Expert review of
medical devices. 3(1):49-57.
Laverna C, Schoenung JM. (1991) Calcium phosphate ceramics as bone substitutes.
American Ceramic Society Bulletin. 70(1):95-100.
Li S, Garreau H, Vert M, Petrova T, Manolova N, Rashkov I (1998) Hydrolytic
degradation of poly (oxyethylene)–poly-(ε-caprolactone) multiblock copolymers.
Journal of applied polymer science. 68(6):989-98.
Li WJ, Laurencin CT, Caterson EJ, Tuan RS, Ko FK (2002) Electrospun nanofibrous
structure: a novel scaffold for tissue engineering. Journal of Biomedical
Materials Research Part A. 60(4):613-21.

162
Liang D, Hsiao BS, Chu B (2007) Functional electrospun nanofibrous scaffolds for
biomedical applications. Advanced drug delivery reviews.59(14):1392-412.
Liao GY, Chen L, Zeng XY, Zhou XP, Xie XL, Peng EJ, Ye ZQ, Mai YW (2011)
Electrospun poly (L-lactide)/poly (ε-caprolactone) blend fibers and their cellular
response to adipose-derived stem cells. Journal of applied polymer science.
120(4):2154-65.
Lu J, Liu JG, Song XF, Chen XS, Wu XD (2011) Sandwich structure-like meshes
fabricated via electrospinning for controllable release of zoledronic acid. Chem
Res Chin Univ. 27:524.
Luhmann T, Germershaus O, Groll J, Meinel L. (2016) Bone targeting for the treatment
of osteoporosis. Journal of controlled release. 1(2):198-213.
LYET JP. (2006) Fragility Fractures in the Osteoporotic Patient: Special Challenges.
The Journal. 1(3):91.
Majumdar, S., Genant, H.K., Grampp, S., Newitt, D.C., Truong, V.-H., Lin, J.C.,
Mathur, A., 1997. Correlation of Trabecular Bone Structure with Age, Bone
Mineral Density, and Osteoporotic Status: In Vivo Studies in the Distal
Radius Using High Resolution Magnetic Resonance Imaging. J. Bone Miner.
Res. 12, 111–118.
Masaeli E, Morshed M, Rasekhian P, Karbasi S, Karbalaie K, Karamali F, Abedi D,
Razavi S, Jafarian-Dehkordi A, Nasr-Esfahani MH, Baharvand H (2012) Does
the tissue engineering architecture of poly (3-hydroxybutyrate)scaffold
affects cell–material interactions?. Journal of Biomedical Materials
Research Part A. 100(7):1907-18.
Meng ZX, Zheng W, Li L, Zheng YF (2010) Fabrication and characterization of three-
dimensional nanofiber membrance of PCL–mwcnts by electrospinning.
Materials Science and Engineering: C. 30(7):1014-21.

163
Mithal A, Bansal B, Kyer CS, Ebeling P (2014) The Asia-pacific regional audit-
epidemiology, costs, and burden of osteoporosis in India 2013: a report of
international 18(4):449
Morabito N, Gaudio A , Lasco, A, Vergara C, Tallarida F, Crisafulli G, Trifiletti A,
Cincotta M., Pizzoleo MA, Frisina N. (2003) Three-year effectiveness of
intravenous pamidronate versus pamidronate plus slow-release sodium fluoride
for postmenopausal osteoporosis. Osteoporosis international. 14(6):500-506.
Mukherjee D, Bharath S (2013) Design and characterization of double layered
mucoadhesive system containing bisphosphonate derivative. ISRN
pharmaceutics. 19;2013.
Murugan R, Ramakrishna S (2005) Development of nanocomposites for bone grafting.
Composites Science and Technology. 65(15):2385-406.
Nair MB, Bernhardt A, Lode A, Heinemann C, Thieme S, Hanke T, Varma H, Gelinsky
M, John A (2009) A bioactive triphasic ceramic-coated hydroxyapatite promotes
proliferation and osteogenic differentiation of human bone marrow stromal cells.
Journal of Biomedical Materials Research Part A. 90(2):533-42.
Nam J, Huang Y, Agarwal S, Lannutti J (2007) Improved cellular infiltration in
electrospun fiber via engineered porosity. Tissue engineering. 13(9):2249-57.
Natta FJ, Hill JW, Carothers WH (1934) Studies of polymerization and ring formation.
XXIII. 1 ε-Caprolactone and its polymers. Journal of the American Chemical
Society. (2):455-7.
Oh SH, Kang SG, Kim ES, Cho SH, Lee JH (2003) Fabrication and characterization of
hydrophilic poly (lactic-co-glycolic acid)/poly (vinyl alcohol) blend cell
scaffolds by melt-molding particulate-leaching method. Biomaterials.
24(22):4011-21.

164
Pitt CG. (1990) Poly-ε-caprolactone and its copolymers. Drugs and the pharmaceutical
sciences. 45:71-120.
Ponader S, Brandt H, Vairaktaris E, von Wilmowsky C, Nkenke E, Schlegel KA,
Neukam FW, Holst S, Müller FA, Greil P. (2008) In vitro response of hFOB
cells to pamidronate modified sodium silicate coated cellulose scaffolds.
Colloids and Surfaces B: Biointerfaces. 64(2):275-83.
Ponader S, Brandt H, Vairaktaris E, von Wilmowsky C, Nkenke E, Schlegel KA,
Neukam FW, Holst S, Müller FA, Greil P (2008) In vitro response of hFOB
cells to pamidronate modified sodium silicate coated cellulose scaffolds.
Colloids and Surfaces B: Biointerfaces. 64(2):275-83.
Prabhakaran MP, Venugopal JR, Chyan TT, Hai LB, Chan CK, Lim AY, Ramakrishna S
(2008) Electrospun biocomposite nanofibrous scaffolds for neural tissue
engineering. Tissue Engineering Part A. 14(11):1787-97.
Puppi D, Chiellini F, Piras AM, Chiellini E (2010) Polymeric materials for bone and
cartilage repair. Progress in Polymer Science. 35(4):403-40.
Raisz LG. (2005) Pathogenesis of osteoporosis: concepts, conflicts, and prospects.
Journal of Clinical Investigation. 115(12):3318.
Reid IR, Wattie DJ, Evans MC, Gamble GD, Stapleton JP, Cornish JI. (1994)
Continuous therapy with pamidronate, a potent bisphosphonate, in
postmenopausal osteoporosis. The Journal of Clinical Endocrinology &
Metabolism. 79(6):1595-9
Reinwald S, Burr D (2008) Review of nonprimate, large animal models for osteoporosis
research. Journal of Bone and Mineral Research. 23(9):1353-68.
Salgado AJ, Coutinho OP, Reis RL (2004) Bone tissue engineering: state of the art and
future trends. Macromolecular bioscience. 4(8):743-65.

165
Sartori AR, Moreira JA, Santos AM, Cintra DE, Sartori LR, Baraúna MA, Canto RS
(2008) Bone repair process in normal and osteopenic female rats' tibiae: a
comparative study. Acta Ortopédica Brasileira, 16(1), 37-40.
Schneider E, Goldhahn J, Burckhardt P (2005) The challenge: fracture treatment in
osteoporotic bone. Osteoporosis International. 16:S1-2.
Shafiee A, Soleimani M, Chamheidari GA, Seyedjafari E, Dodel M, Atashi A, Gheisari
Y (2011) Electrospun nanofiber-based regeneration of cartilage enhanced by
mesenchymal stem cells. Journal of biomedical materials research Part A.
99(3):467-78.
Shafieyan Y, Sharifi S, Imani M, Shokrgozar MA, Aboudzadeh N, Atai M. A (2011)
biocompatible composite based on poly (ε-caprolactone fumarate) and
hydroxyapatite. Polymers for Advanced Technologies. 22(12):2182-90.
Shalumon KT, Binulal NS, Deepthy M, Jayakumar R, Manzoor K, Nair SV. (2010)
Preparation, characterization and cell attachment studies of electrospun multi-
scale poly (caprolactone) fibrous scaffolds for tissue engineering. Journal of
Macromolecular Science, Part A. 48(1):21-30.
Shen V, Birchman R, Wu DD, Lindsay R(2000) Skeletal effects of parathyroid hormone
infusion in ovariectomized rats with or without estrogen repletion. Journal of
Bone and Mineral Research. 15(4):740-6.
Shin YS, Borah JS, Haider A, Kim S, Huh MW, Kang IK (2013) Fabrication of
pamidronic acid-immobilized TiO 2/hydroxyapatite composite nanofiber mats
for biomedical applications. Journal of Nanomaterials. 2013:152.
Son SR, Linh NT, Yang HM, Lee BT (2013) In vitro and in vivo evaluation of
electrospun PCL/PMMA fibrous scaffolds for bone regeneration. Science and
technology of advanced materials. 14(1):015009.

166
Son SR, Linh NT, Yang HM, Lee BT. (2013) In vitro and in vivo evaluation of
electrospun PCL/PMMA fibrous scaffolds for bone regeneration. Science and
technology of advanced materials. 14(1):015009.
Sridevi A, Ragi V. Management of osteoporosis in women-A prevalence and
interventional study.
Staiger MP, Pietak AM, Huadmai J, Dias G (2006) Magnesium and its alloys as
orthopedic biomaterials: a review. Biomaterials. 27(9):1728-34.
STANLEY L, BALL KE. Pamidronate therapy as prevention of bone loss following
renal transplantation1. Hypertension. (2000);50:2.
Subia B, Kundu J, Kundu SC. Biomaterial scaffold fabrication techniques for potential
tissue engineering applications. InTissue engineering (2010). InTech.
Szpalski C, Barr J, Wetterau M, Saadeh PB, Warren SM (2010) Cranial bone defects:
current and future strategies. Neurosurgical focus. 29(6):E8.
Thiebaud D, Burckhardt P, Melchior J, Eckert P, Jacquet AF, Schnyder P, Gobelet C
(1994) Two years' effectiveness of intravenous pamidronate (APD) versus oral
fluoride for osteoporosis occurring in the postmenopause. Osteoporosis
international. 4(2):76-83.
Thulkar J, Singh S. (2015) Overview of research studies on osteoporosis in menopausal
women since the last decade. Journal of mid-life health. 6(3):104.
Venugopal J, Low S, Choon AT, Kumar AB, Ramakrishna S (2008)
Electrospun-modified nanofibrous scaffolds for the mineralization of osteoblast
cells. Journal of biomedical materials research Part A. 85(2):408-17.
Verron E, Gauthier O, Janvier P, Pilet P, Lesoeur J, Bujoli B, Guicheux J, Bouler JM.
(2010) In vivo bone augmentation in an osteoporotic environment using
bisphosphonate-loaded calcium deficient apatite. Biomaterials. 31(30):7776-84.

167
Wang JH, Cheng XB, Huang G, Dong FC, Jia YT (2011) Preparation and
Characterization of PCL/PVP Blend Membrane. InAdvanced Materials Research
(Vol. 311, pp. 1638-1641). Trans Tech Publications.
Wang Z, Han Z, Tao J, Lu P, Liu X, Wang J, Wu B, Huang Z, Yin C, Tan R, Gu M
(2014) Clinical efficacy and safety of pamidronate therapy on bone mass density
in early post-renal transplant period: a meta-analysis of randomized controlled
trials. PloS one. Se9(9):e108106.
Wilkinson JM, Little DG (2011) Bisphosphonates in orthopedic applications. Bone.
49(1):95-102.
Williams A, Szaso RM (2004) Bone transplantation. Orthopedics. 27(5):488-95.
Wronski TJ (1991) The ovariectomized rat as an animal model for postmenopausal bone
loss. Cells Materials. 1:69-74.
Wronski TJ, Lowry PL, Walsh CC, Ignaszewski LA (1985) Skeletal alterations in
ovariectomized rats. Calcified tissue international. 37(3):324-8.
Wutticharoenmongkol P, Sanchavanakit N, Pavasant P, Supaphol P (2006)Preparation
and characterization of novel bone scaffolds based on electrospun
polycaprolactone fibers filled with nanoparticles. Macromolecular
bioscience.6(1):70-7.
Xie Z, Buschle-Diller G. (2010) Electrospun poly (D, L-lactide) fibers for drug delivery:
The influence of cosolvent and the mechanism of drug release. Journal of
applied polymer science. 115(1):1-8.
Yang S, Leong KF, Du Z, Chua CK. (2001) The design of scaffolds for use in tissue
engineering. Part I. Traditional factors. Tissue engineering. 7(6):679-89.

168
Yu NY, Schindeler A, Peacock L, Mikulec K, Baldock PA, Ruys AJ, Little DG (2010)
In vivo local co-delivery of recombinant human bone morphogenetic protein-7
and pamidronate via poly-D, L-lactic acid. Eur Cell Mater. 20:431-1.
Yun YP, Kim SJ, Lim YM, Park K, Kim HJ, Jeong SI, Kim SE, Song HR (2014) The
effect of alendronate-loaded polycarprolactone nanofibrous scaffolds on
osteogenic differentiation of adipose-derived stem cells in bone tissue
regeneration. Journal of biomedical nanotechnology. 10(6):1080-90.
Zhang Y, Wei L, Chang J, Miron RJ, Shi B, Yi S, Wu C (2013) Strontium-incorporated
mesoporous bioactive glass scaffolds stimulating in vitro proliferation and
differentiation of bone marrow stromal cells and in vivo regeneration of
osteoporotic bone defects. Journal of Materials Chemistry B. 1(41):5711-22.

169
LIST OF PUBLICATIONS
Remya K. R., Joseph, J., Mani, S., John, A., Varma, H. K., & Ramesh, P.
Nanohydroxyapatite incorporated electrospun Polycaprolactone/Polycaprolactone –
Polyethyleneglycol - Polycaprolactone Blend Scaffold for Bone Tissue Engineering
Applications (2013). Journal of biomedical nanotechnology, 9(9), 1483-1494.
Remya K.R., Sunitha Chandran, Annie John and P.Ramesh, Pamidronate encapsulated
electrospun nanofibrous polycaprolactone scaffolds as a potential drug eluting scaffold
for the treatment of osteoporotic bone defects. (manuscript submitted)
Remya K.R., Sunitha Chandran, Annie John and P.Ramesh, Hybrid
Polycaprolactone/Polyethylene oxide scaffolds with tunable fiber surface morphology,
improved hydrophilicity and biodegradability for bone tissue engineering application.
(under revision)
Remya K.R., Sunitha Chandran, Harikrishnan V.S, Annie John and P.Ramesh. In-vitro
and in-vivo evaluation of pamidronate incorporated PCL based scaffolds in an
osteoporotic rat animal model. (manuscript to be submitted)

170
Conference presentations
Remya K.R. and P. Ramesh, Controlled release of Pamidronate from electrospun
Polycaprolactone nanofibrous mats for orthopaedic application, National seminar on
Biopolymers & Green Composites (BPGC 2015), October 9-10, 2015 organized by
Centre for Biopolymer Science & Technology, Kochi.
Remya K.R, Sunitha Chandran, Annie John, Harikrishna Varma P.R. and Ramesh P ,
Pamidronate loaded electrospun Polycaprolactone/ Polycaprolactone –
Polyethyleneglycol-Polycaprolactone / nanohydroxyapatite composite scaffold for
orthopaedic application , National Conference on Material Science & Technology
(NCMST 2015),July 6-8,2015 organized by IIST Thiruvananthapuram.
Remya K.R. and P. Ramesh, In-vitro degradation behaviour of electrospun
Polycaprolactone/Polyethyleneoxide blends for tissue engineering applications , an
international conference FAPS – MACRO, May 15-18, 2013 organized by Indian
Institute of Science, Bangalore.

171
CURRICULUM VITAE
Personal
Name : Remya K R
Date of birth : 30th April 1985
Marital status : Unmarried
Phone number : 9847226094
Address : Raj Bhavan
Chithrapuzha
Irumpanam P. O.
Ernakulam-682309
Kerala, India
E-mail : [email protected]
Education
Ph.D Scholar (January 2011- present) at Sree Chitra Tirunal Institute for Medical
Sciences and Technology, BioMedical Technology Wing, Thiruvananthapuram, Kerala,
India. Supervisor : Dr. P. Ramesh
Master of Technology in Polymer Technology (2007-2009) Cochin University of
Science and Technology, Cochin, Kerala, India
Master of Science in Chemistry (Polymer science) (2005-2007), School of Chemical
Sciences, Mahatma Gandhi University, Kottayam, Kerala, India

172
Bachelor of Science in Chemistry (2002-2005), St Teresa’s College, (Mahatma Gandhi
University), Kochi, Kerala, India
Professional Experience
August 2009- December 2010: Junior Research Fellow at Sree Chitra Tirunal Institute
for Medical Sciences and Technology, Trivandrum, Kerala, India. Project Supervisor:
Dr. P. Ramesh.
July 2008 – April 2009: MTech Project at HLL Lifecare, Trivandrum. Project
Supervisor: Dr. Abi Santosh Aprem
February 2007 – May 2007: MSc Project at National Chemical Laboratory (NCL) ,
Pune, Maharashtra Project Supervisor: Dr. Jyoti P.Jog
Achievements
Prestegious SCTIMST Institute Fellowship 2011
Best oral presentation award, National conference on Biopolymers and Green
composites (BPGC) 2015, organized by Centre for Biopolymer Science &
Technology , Kochi
First prize in Quiz competition during National Conference on Biopolymers and Green
composites 2015, organized by Centre for Biopolymer Science & Technology ,
Kochi

173
APPENDIX
PBS (1000ml) pH 7.4 NaCl - 8g KCl - 0.2g Na2HPO4 - 1.44g KH2PO4 - 0.24g (Added distilled water to a final volume of 1000 ml, solution is filtered and stored at room temperature) Ninhydrin reagent (0.2 %) Ninhydrin - 0.2 % w/v in methanol Stevenal’s blue stain Methylene Blue – 1 gm in 75 ml distilled water Potassium permanganate – 1.5 gm in 75 ml distilled water Van Gieson’s Picrofuchsin stain Acid Fuchsin – 0.1 gm in 10 ml distilled water Saturated picric acid – 100ml