Effect of the C825T polymorphism of the G protein β3 subunit on the systolic blood...
8
Effect of the C825T polymorphism of the G protein 3 subunit on the systolic blood pressure–lowering effect of clonidine in young, healthy male subjects The T allele of the C825T polymorphism in the gene encoding the G-protein 3 subunit (GNB3) is associated with hypertension. An enhanced signal transduction in response to 2 -adrenergic receptor stimulation has been shown in carriers of the T allele in vitro. We hypothesized that T allele carriers would show an enhanced antihypertensive response to stimulation of central 2 -adrenergic receptors by clonidine. We compared the response to intravenous clonidine in 30 young, healthy male subjects with and without the T allele (15 CC, 10 CT, and 5 TT). Clonidine lowered blood pressure and total peripheral resistance, lengthened the duration of electromechanical systole (QS 2 c), and slowed down pulse wave velocity. Carriers of the T allele showed significantly greater reductions in systolic blood pressure (P .009; mean change SEM: CC, 8.9 0.5; CT and TT, 10.6 0.4) and total peripheral resistance (P < .0001; mean change SEM: CC, 40 17; CT and TT, 48 14) and more marked lengthening of QS 2 c(P .002; mean change SEM: CC, 2.2 0.5; CT and TT, 4.7 0.6) and slowing of pulse wave velocity (P .012; mean change SEM: CC, 0.25 0.02; CT and TT, 0.33 0.03). The results of this study suggest that the 825T allele may be a relevant pharmacogenetic marker in the use of centrally acting sympatholytic drugs. (Clin Pharmacol Ther 2003;74: 53-60.) Jens Nu ¨rnberger, MD, Sandra Dammer, BSc, Anna Mitchell, MD, Winfried Siffert, MD, Rene ´ R. Wenzel, MD, Mario Go ¨ssl, MD, Thomas Philipp, MD, Martin C. Michel, MD, and Rafael F. Scha ¨fers, MD Essen, Germany Effective pharmacotherapy of high blood pressure (BP) significantly reduces cardiovascular morbidity and mortality. 1 The response to antihypertensive drug therapy varies greatly among individual subjects, as reflected by responder rates to initial single-drug ther- apy, which rarely exceed 50%. 2,3 This variability in response to drug therapy is determined by many factors including age, gender, and the presence of various diseases. However, the importance of genetic factors in determining drug response variability is increasingly being recognized. 4 One genetic factor that may contribute to the drug response variability is the C825T polymorphism. This polymorphism was identified in the gene encoding the G-protein 3 subunit (GNB3), 5 and an association of the T allele with hypertension has been found in several studies. 5-9 Even though the mechanisms linking the T allele to the development of hypertension are unclear, it has been show in in vitro studies that carriers of the 825T allele show an enhanced intracellular signal trans- duction of pertussis toxin (PTX)– dependent path- ways. 10,11 2 -Adrenergic receptors are the prototype of receptors that are coupled to PTX-sensitive G pro- teins 12 in which the C825T polymorphism was identi- fied. 2 -Adrenergic receptors are located in the brain stem, and stimulation of these adrenergic receptors decreases the activity of the central sympathetic ner- vous system, thereby lowering BP. 13 Thus, when com- pared with control subjects without the T allele, carriers From the Departments of Medicine and Pharmacology, Essen Uni- versity. Drs Nu ¨rnberger and Dammer contributed equally to this study. Supported in part by the Deutsche Forschungsgemeinschaft (DFG, WE 1773/3-1) and the Oertel Foundation. Received for publication Dec 23, 2002; accepted Feb 27, 2003. Reprint requests: Rafael F. Scha ¨fers, MD, Department of Medicine, Hufelandstrasse 55, 45122, Essen, Germany. E-mail: [email protected] Copyright © 2003 by the American Society for Clinical Pharmacol- ogy & Therapeutics. 0009-9236/2003/$30.00 0 doi:10.1016/S0009-9236(03)00087-0 53
Transcript of Effect of the C825T polymorphism of the G protein β3 subunit on the systolic blood...
Effect of the C825T polymorphism of theG protein �3 subunit on the systolic bloodpressure–lowering effect of clonidine inyoung, healthy male subjects
The T allele of the C825T polymorphism in the gene encoding the G-protein �3 subunit (GNB3) is associatedwith hypertension. An enhanced signal transduction in response to �2-adrenergic receptor stimulation hasbeen shown in carriers of the T allele in vitro. We hypothesized that T allele carriers would show an enhancedantihypertensive response to stimulation of central �2-adrenergic receptors by clonidine. We compared theresponse to intravenous clonidine in 30 young, healthy male subjects with and without the T allele (15 CC,10 CT, and 5 TT). Clonidine lowered blood pressure and total peripheral resistance, lengthened the durationof electromechanical systole (QS2c), and slowed down pulse wave velocity. Carriers of the T allele showedsignificantly greater reductions in systolic blood pressure (P � .009; mean change � SEM: CC, �8.9 � 0.5;CT and TT, �10.6 � 0.4) and total peripheral resistance (P < .0001; mean change � SEM: CC, 40 � 17; CTand TT, �48 � 14) and more marked lengthening of QS2c (P � .002; mean change � SEM: CC, 2.2 � 0.5;CT and TT, 4.7 � 0.6) and slowing of pulse wave velocity (P � .012; mean change � SEM: CC, �0.25 �
0.02; CT and TT, �0.33 � 0.03). The results of this study suggest that the 825T allele may be a relevantpharmacogenetic marker in the use of centrally acting sympatholytic drugs. (Clin Pharmacol Ther 2003;74:53-60.)
Jens Nurnberger, MD, Sandra Dammer, BSc, Anna Mitchell, MD, Winfried Siffert,MD, Rene R. Wenzel, MD, Mario Gossl, MD, Thomas Philipp, MD, Martin C.Michel, MD, and Rafael F. Schafers, MD Essen, Germany
Effective pharmacotherapy of high blood pressure(BP) significantly reduces cardiovascular morbidityand mortality.1 The response to antihypertensive drugtherapy varies greatly among individual subjects, asreflected by responder rates to initial single-drug ther-apy, which rarely exceed 50%.2,3 This variability inresponse to drug therapy is determined by many factorsincluding age, gender, and the presence of variousdiseases. However, the importance of genetic factors in
determining drug response variability is increasinglybeing recognized.4
One genetic factor that may contribute to the drugresponse variability is the C825T polymorphism. Thispolymorphism was identified in the gene encoding theG-protein �3 subunit (GNB3),5 and an association ofthe T allele with hypertension has been found in severalstudies.5-9 Even though the mechanisms linking the Tallele to the development of hypertension are unclear, ithas been show in in vitro studies that carriers of the825T allele show an enhanced intracellular signal trans-duction of pertussis toxin (PTX)–dependent path-ways.10,11 �2-Adrenergic receptors are the prototype ofreceptors that are coupled to PTX-sensitive G pro-teins12 in which the C825T polymorphism was identi-fied. �2-Adrenergic receptors are located in the brainstem, and stimulation of these adrenergic receptorsdecreases the activity of the central sympathetic ner-vous system, thereby lowering BP.13 Thus, when com-pared with control subjects without the T allele, carriers
From the Departments of Medicine and Pharmacology, Essen Uni-versity. Drs Nurnberger and Dammer contributed equally to thisstudy.
Supported in part by the Deutsche Forschungsgemeinschaft (DFG,WE 1773/3-1) and the Oertel Foundation.
Received for publication Dec 23, 2002; accepted Feb 27, 2003.Reprint requests: Rafael F. Schafers, MD, Department of Medicine,
Hufelandstrasse 55, 45122, Essen, Germany.E-mail: [email protected] © 2003 by the American Society for Clinical Pharmacol-
ogy & Therapeutics.0009-9236/2003/$30.00 � 0doi:10.1016/S0009-9236(03)00087-0
53

of the T allele may show a greater BP-lowering effectof stimulating central �2-adrenergic receptors.
In this study we tested the hypothesis that carriers ofthe 825T allele would show an increased responsive-ness after the stimulation of central �2-adrenergic re-ceptors. We evaluated the hemodynamic response toclonidine, a classic �2-adrenergic receptor agonist,14 in2 groups of young, healthy male subjects who differedonly with regard to the status of the C825T polymor-phism.
METHODSStudy population. The study population included
young, nonsmoking male subjects who gave writteninformed consent (mean age � SEM, 26.5 � 0.7years). Thirty subjects classified according to the GNB3genotype (15 CC, 10 CT, and 5 TT) participated. Sub-jects and investigators were blinded with regard to thegenotype at the GNB3 locus. Subjects were drug-freeand judged to be healthy on the basis of medical his-tory, physical examination, electrocardiogram, and rou-tine laboratory screening. The study was approved bythe Ethics Committee of the University of Essen, Essen,Germany, and was performed in accordance with theprinciples of the Declaration of Helsinki.
Study protocol. On the study day, subjects reportedto the laboratory at 7 to 8 AM after an overnight fast andremained in the supine position during the entire inves-tigation. Measurements were performed in a quiet roomat a constant ambient temperature. A BP cuff, circulartape electrodes for measurement of transthoracic im-pedance, and a microphone for phonocardiographic re-cordings were used in each subject. After a period of 30minutes of complete rest, baseline hemodynamic andneurohumoral measurements were performed. Thereaf-ter each subject received the �2-adrenergic receptoragonist clonidine, given as a single intravenous dose of1 �g · kg�1 over a 5-minute period (Catapresan; Boehr-inger Ingelheim, Ingelheim, Germany). After injection,hemodynamic measurements were repeated and bloodsamples for the measurement of plasma norepinephrineand serum growth hormone were drawn at regularintervals as shown in the figures.
Hemodynamic and neurohumoral measurements. He-modynamics were assessed noninvasively by heart rateand BP measurement, determination of systolic timeintervals, performance of impedance cardiography, anddetermination of aortofemoral pulse wave velocity(PWV).
We measured systolic time intervals to characterizeleft ventricular performance. These provide an accurateand sensitive measure of left ventricular function.15,16
This method is particularly advantageous becauseclonidine lowers central sympathetic activity, resultingin reduced myocardial contractility. Stroke volume wasobtained by impedance cardiography. This methodyields measurements that agree closely with those ob-tained by Doppler echocardiography or thermodilu-tion17 and is acceptable for clinical use particularly instudies investigating young subjects free of any cardio-vascular disease.18 In our laboratory we have deter-mined that the variability of stroke volume measured byimpedance cardiography is less than 5.5% (expressedas a percentage of the coefficient of variation).19 Aor-tofemoral PWV was determined to investigate vascularfunction. Measuring PWV is the classic method used toinvestigate the elastic properties of the arterial tree.20,21
Stroke volume (measured by impedance cardiogra-phy with a Kardio-Dynagraph; Heinz Diefenbach Ele-ktromedizin, Frankfurt, Germany), cardiac output, andtotal peripheral resistance (TPR) were calculated fromthe directly measured parameters by standard formulas.BP (in millimeters of mercury) was measured with avalidated oscillometric device (Dinamap Monitor;Johnson & Johnson, Norderstedt, Germany). Systolictime intervals were measured by standard techniques.The duration of electromechanical systole (QS2) wascorrected for HR to yield QS2c. Pulse transmission timewas determined from pressure tracings over the carotidand femoral artery, and PWV was calculated as theratio of the distance traveled by the pulse wave to thepulse transmission time. Details of all methods andtheir within- and between-day variability have beenreported previously by our group.19,22 Plasma norepi-nephrine was analyzed by HPLC with electrochemicaldetection (Cromosystems Instruments & ChemicalsGmbH, Munchen, Germany), and serum growth hor-mone was measured with a commercially available kit(Chemiluminescence Immunoassay; Nichols InstituteDiagnostics, San Juan Capistrano, Calif). Plasmaclonidine levels were measured by radioimmunoassayat 60 minutes after injection (ie, at the time of maximalBP reduction).
Salivary flow was measured from the change inweight of preweighted dental rolls inserted in themouth, and the degree of sedation evoked by clonidinewas quantified by visual analog scales as describedpreviously23 with slight modifications.
Data analysis. Data from in vitro experiments5,11
and indirect evidence from population studies5-8 dem-onstrate that the presence of the T allele, whetherhomozygous or heterozygous, changes cardiovascularand neurohumoral regulation relative to the CC geno-type. Therefore our primary statistical comparisons de-
CLINICAL PHARMACOLOGY & THERAPEUTICS54 Nurnberger et al JULY 2003
termined the significance of differences between T al-lele carriers and subjects with the CC genotype (ie, CTand TT subjects were pooled for analyses). The effectsof clonidine were quantified as changes from baselinevalues determined before clonidine administration, andpossible differences between the 2 groups were com-pared by repeated-measures ANOVA. P � .05 wasconsidered statistically significant. All values areshown as mean � SEM.
RESULTSAnthropometric and hemodynamic parameters,
plasma norepinephrine levels, and serum growth hor-mone levels at baseline after 30 minutes of completesupine rest were not significantly different between Tallele carriers and subjects with the CC genotype (TableI). Similarly, plasma clonidine levels at 60 minuteswere not different between groups (CC, 0.34 � 0.04 ng· mL�1, and CT/TT, 0.37 � 0.02 ng · mL�1; P � .54).
The intravenous injection of clonidine induced a fallin plasma norepinephrine levels, BP, and TPR, length-ened the duration of QS2c, and slowed down PWV. Thechanges from baseline in norepinephrine levels, sys-
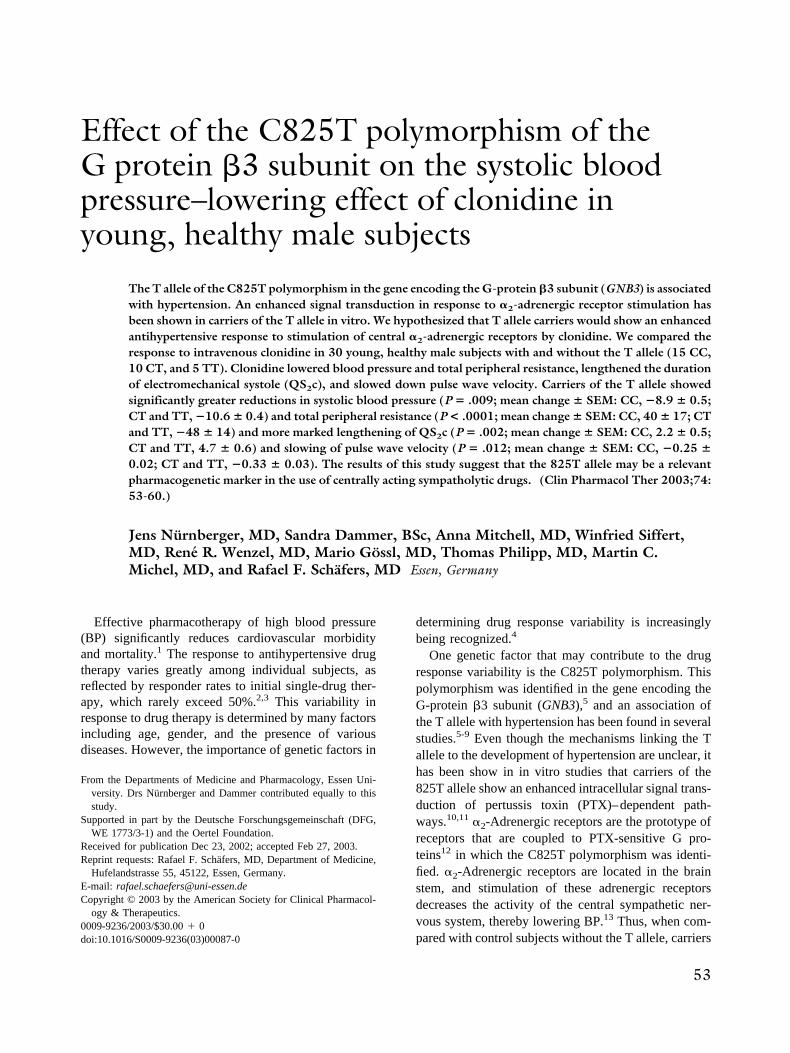
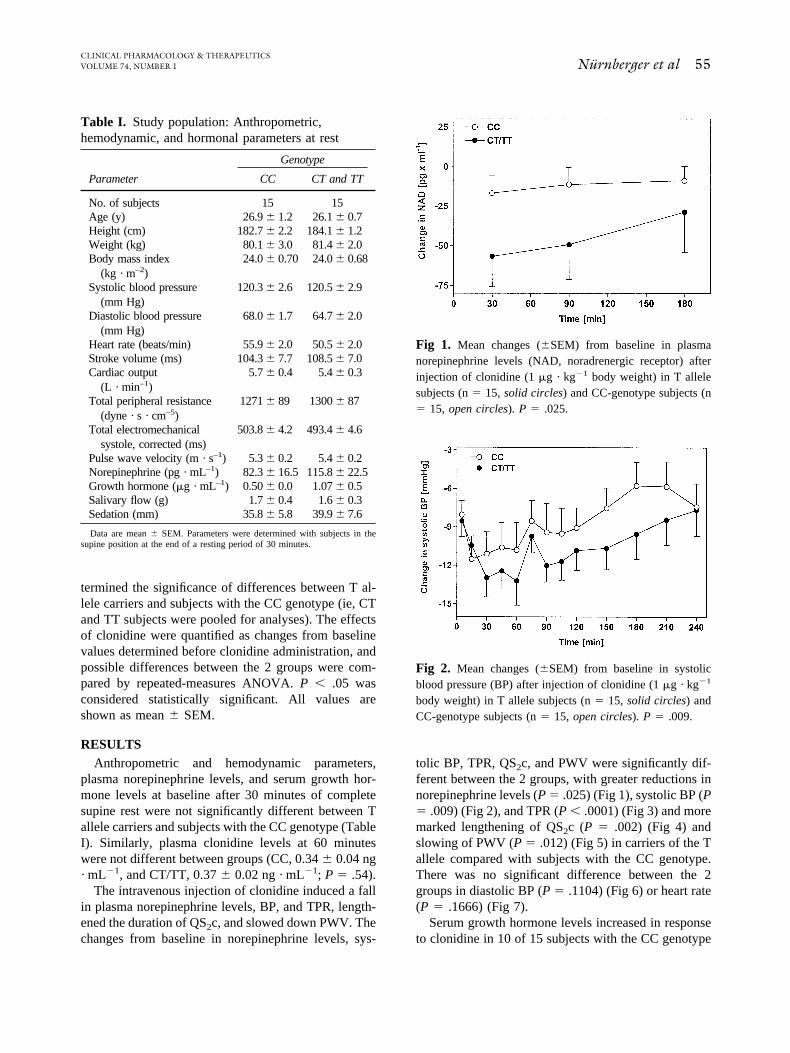
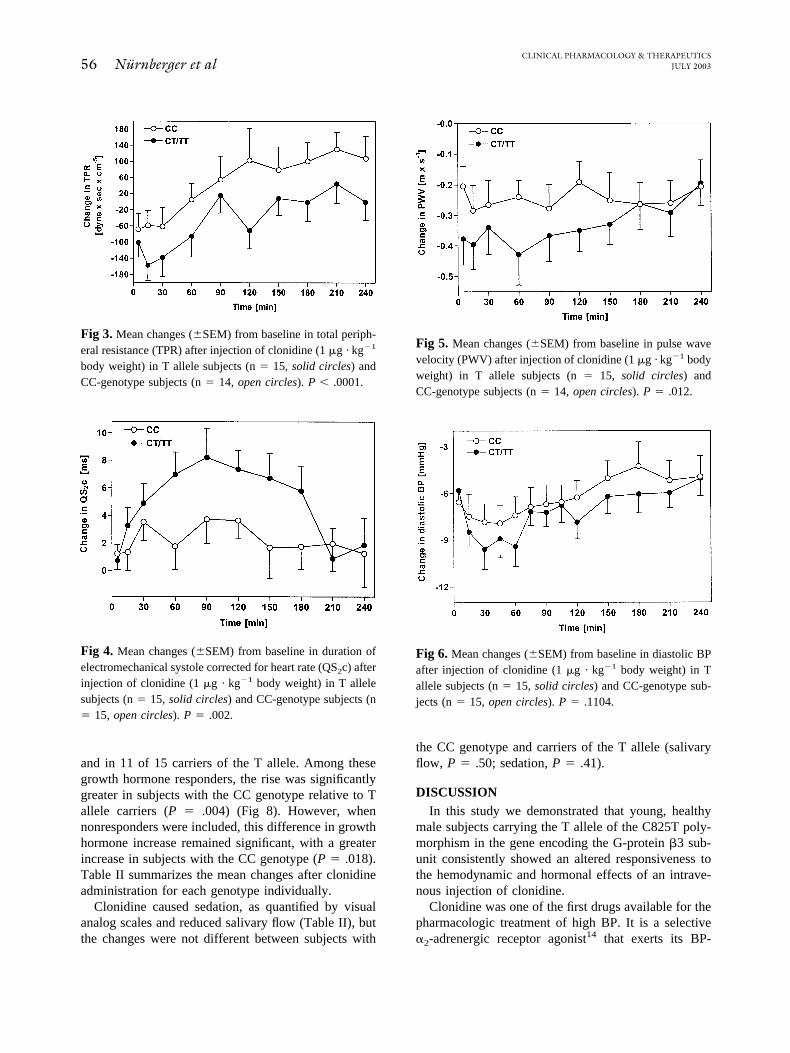
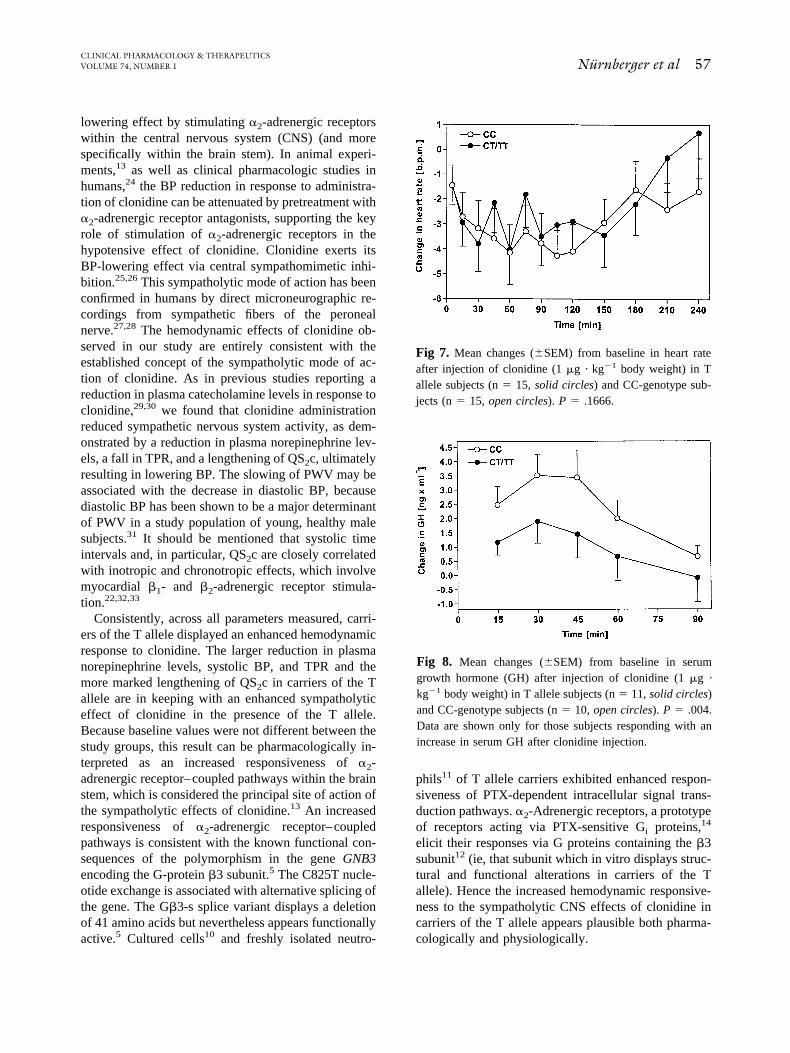
tolic BP, TPR, QS2c, and PWV were significantly dif-ferent between the 2 groups, with greater reductions innorepinephrine levels (P � .025) (Fig 1), systolic BP (P� .009) (Fig 2), and TPR (P � .0001) (Fig 3) and moremarked lengthening of QS2c (P � .002) (Fig 4) andslowing of PWV (P � .012) (Fig 5) in carriers of the Tallele compared with subjects with the CC genotype.There was no significant difference between the 2groups in diastolic BP (P � .1104) (Fig 6) or heart rate(P � .1666) (Fig 7).
Serum growth hormone levels increased in responseto clonidine in 10 of 15 subjects with the CC genotype
Table I. Study population: Anthropometric,hemodynamic, and hormonal parameters at rest
Parameter
Genotype
CC CT and TT
No. of subjects 15 15Age (y) 26.9 � 1.2 26.1 � 0.7Height (cm) 182.7 � 2.2 184.1 � 1.2Weight (kg) 80.1 � 3.0 81.4 � 2.0Body mass index
(kg · m–2)24.0 � 0.70 24.0 � 0.68
Systolic blood pressure(mm Hg)
120.3 � 2.6 120.5 � 2.9
Diastolic blood pressure(mm Hg)
68.0 � 1.7 64.7 � 2.0
Heart rate (beats/min) 55.9 � 2.0 50.5 � 2.0Stroke volume (ms) 104.3 � 7.7 108.5 � 7.0Cardiac output
(L · min–1)5.7 � 0.4 5.4 � 0.3
Total peripheral resistance(dyne · s · cm–5)
1271 � 89 1300 � 87
Total electromechanicalsystole, corrected (ms)
503.8 � 4.2 493.4 � 4.6
Pulse wave velocity (m · s–1) 5.3 � 0.2 5.4 � 0.2Norepinephrine (pg · mL–1) 82.3 � 16.5 115.8 � 22.5Growth hormone (�g · mL–1) 0.50 � 0.0 1.07 � 0.5Salivary flow (g) 1.7 � 0.4 1.6 � 0.3Sedation (mm) 35.8 � 5.8 39.9 � 7.6
Data are mean � SEM. Parameters were determined with subjects in thesupine position at the end of a resting period of 30 minutes.
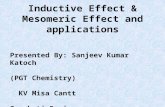
Fig 1. Mean changes (�SEM) from baseline in plasmanorepinephrine levels (NAD, noradrenergic receptor) afterinjection of clonidine (1 �g · kg�1 body weight) in T allelesubjects (n � 15, solid circles) and CC-genotype subjects (n� 15, open circles). P � .025.
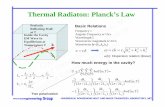
Fig 2. Mean changes (�SEM) from baseline in systolicblood pressure (BP) after injection of clonidine (1 �g · kg�1
body weight) in T allele subjects (n � 15, solid circles) andCC-genotype subjects (n � 15, open circles). P � .009.
CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 74, NUMBER 1 Nurnberger et al 55
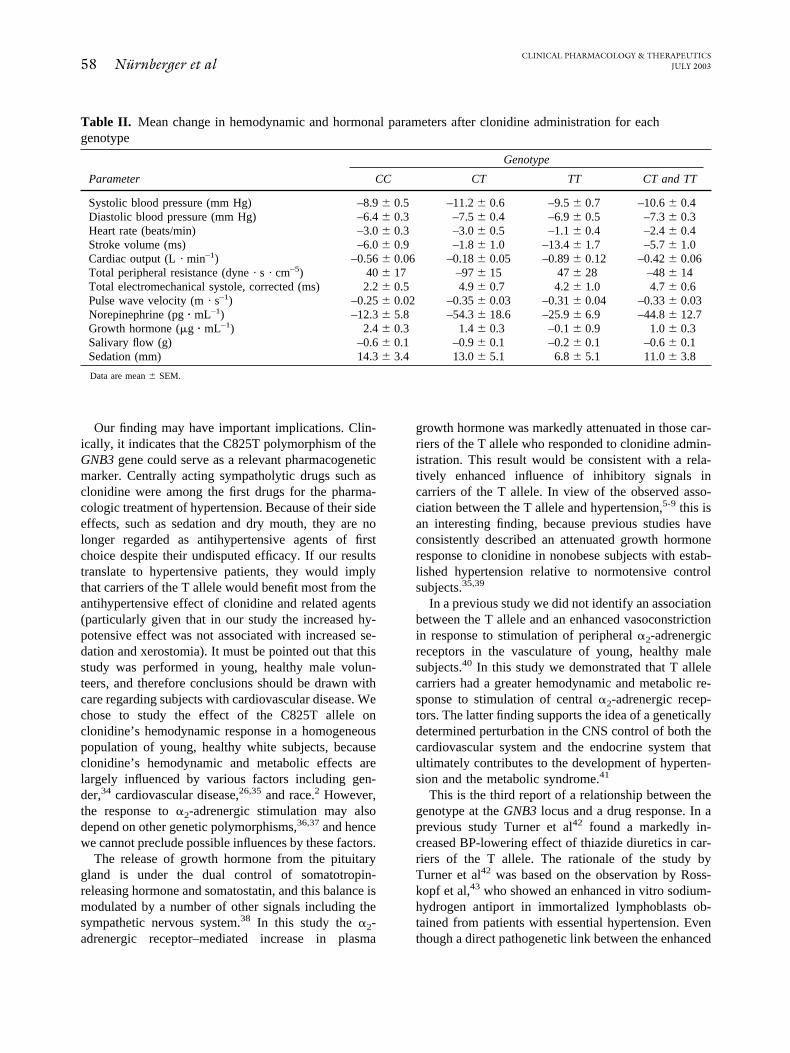
and in 11 of 15 carriers of the T allele. Among thesegrowth hormone responders, the rise was significantlygreater in subjects with the CC genotype relative to Tallele carriers (P � .004) (Fig 8). However, whennonresponders were included, this difference in growthhormone increase remained significant, with a greaterincrease in subjects with the CC genotype (P � .018).Table II summarizes the mean changes after clonidineadministration for each genotype individually.
Clonidine caused sedation, as quantified by visualanalog scales and reduced salivary flow (Table II), butthe changes were not different between subjects with
the CC genotype and carriers of the T allele (salivaryflow, P � .50; sedation, P � .41).
DISCUSSIONIn this study we demonstrated that young, healthy
male subjects carrying the T allele of the C825T poly-morphism in the gene encoding the G-protein �3 sub-unit consistently showed an altered responsiveness tothe hemodynamic and hormonal effects of an intrave-nous injection of clonidine.
Clonidine was one of the first drugs available for thepharmacologic treatment of high BP. It is a selective�2-adrenergic receptor agonist14 that exerts its BP-
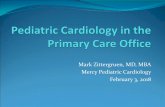
Fig 3. Mean changes (�SEM) from baseline in total periph-eral resistance (TPR) after injection of clonidine (1 �g · kg�1
body weight) in T allele subjects (n � 15, solid circles) andCC-genotype subjects (n � 14, open circles). P � .0001.
Fig 4. Mean changes (�SEM) from baseline in duration ofelectromechanical systole corrected for heart rate (QS2c) afterinjection of clonidine (1 �g · kg�1 body weight) in T allelesubjects (n � 15, solid circles) and CC-genotype subjects (n� 15, open circles). P � .002.
Fig 5. Mean changes (�SEM) from baseline in pulse wavevelocity (PWV) after injection of clonidine (1 �g · kg�1 bodyweight) in T allele subjects (n � 15, solid circles) andCC-genotype subjects (n � 14, open circles). P � .012.
Fig 6. Mean changes (�SEM) from baseline in diastolic BPafter injection of clonidine (1 �g · kg�1 body weight) in Tallele subjects (n � 15, solid circles) and CC-genotype sub-jects (n � 15, open circles). P � .1104.
CLINICAL PHARMACOLOGY & THERAPEUTICS56 Nurnberger et al JULY 2003
lowering effect by stimulating �2-adrenergic receptorswithin the central nervous system (CNS) (and morespecifically within the brain stem). In animal experi-ments,13 as well as clinical pharmacologic studies inhumans,24 the BP reduction in response to administra-tion of clonidine can be attenuated by pretreatment with�2-adrenergic receptor antagonists, supporting the keyrole of stimulation of �2-adrenergic receptors in thehypotensive effect of clonidine. Clonidine exerts itsBP-lowering effect via central sympathomimetic inhi-bition.25,26 This sympatholytic mode of action has beenconfirmed in humans by direct microneurographic re-cordings from sympathetic fibers of the peronealnerve.27,28 The hemodynamic effects of clonidine ob-served in our study are entirely consistent with theestablished concept of the sympatholytic mode of ac-tion of clonidine. As in previous studies reporting areduction in plasma catecholamine levels in response toclonidine,29,30 we found that clonidine administrationreduced sympathetic nervous system activity, as dem-onstrated by a reduction in plasma norepinephrine lev-els, a fall in TPR, and a lengthening of QS2c, ultimatelyresulting in lowering BP. The slowing of PWV may beassociated with the decrease in diastolic BP, becausediastolic BP has been shown to be a major determinantof PWV in a study population of young, healthy malesubjects.31 It should be mentioned that systolic timeintervals and, in particular, QS2c are closely correlatedwith inotropic and chronotropic effects, which involvemyocardial �1- and �2-adrenergic receptor stimula-tion.22,32,33
Consistently, across all parameters measured, carri-ers of the T allele displayed an enhanced hemodynamicresponse to clonidine. The larger reduction in plasmanorepinephrine levels, systolic BP, and TPR and themore marked lengthening of QS2c in carriers of the Tallele are in keeping with an enhanced sympatholyticeffect of clonidine in the presence of the T allele.Because baseline values were not different between thestudy groups, this result can be pharmacologically in-terpreted as an increased responsiveness of �2-adrenergic receptor–coupled pathways within the brainstem, which is considered the principal site of action ofthe sympatholytic effects of clonidine.13 An increasedresponsiveness of �2-adrenergic receptor–coupledpathways is consistent with the known functional con-sequences of the polymorphism in the gene GNB3encoding the G-protein �3 subunit.5 The C825T nucle-otide exchange is associated with alternative splicing ofthe gene. The G�3-s splice variant displays a deletionof 41 amino acids but nevertheless appears functionallyactive.5 Cultured cells10 and freshly isolated neutro-
phils11 of T allele carriers exhibited enhanced respon-siveness of PTX-dependent intracellular signal trans-duction pathways. �2-Adrenergic receptors, a prototypeof receptors acting via PTX-sensitive Gi proteins,14
elicit their responses via G proteins containing the �3subunit12 (ie, that subunit which in vitro displays struc-tural and functional alterations in carriers of the Tallele). Hence the increased hemodynamic responsive-ness to the sympatholytic CNS effects of clonidine incarriers of the T allele appears plausible both pharma-cologically and physiologically.
Fig 7. Mean changes (�SEM) from baseline in heart rateafter injection of clonidine (1 �g · kg�1 body weight) in Tallele subjects (n � 15, solid circles) and CC-genotype sub-jects (n � 15, open circles). P � .1666.
Fig 8. Mean changes (�SEM) from baseline in serumgrowth hormone (GH) after injection of clonidine (1 �g ·kg�1 body weight) in T allele subjects (n � 11, solid circles)and CC-genotype subjects (n � 10, open circles). P � .004.Data are shown only for those subjects responding with anincrease in serum GH after clonidine injection.
CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 74, NUMBER 1 Nurnberger et al 57
Our finding may have important implications. Clin-ically, it indicates that the C825T polymorphism of theGNB3 gene could serve as a relevant pharmacogeneticmarker. Centrally acting sympatholytic drugs such asclonidine were among the first drugs for the pharma-cologic treatment of hypertension. Because of their sideeffects, such as sedation and dry mouth, they are nolonger regarded as antihypertensive agents of firstchoice despite their undisputed efficacy. If our resultstranslate to hypertensive patients, they would implythat carriers of the T allele would benefit most from theantihypertensive effect of clonidine and related agents(particularly given that in our study the increased hy-potensive effect was not associated with increased se-dation and xerostomia). It must be pointed out that thisstudy was performed in young, healthy male volun-teers, and therefore conclusions should be drawn withcare regarding subjects with cardiovascular disease. Wechose to study the effect of the C825T allele onclonidine’s hemodynamic response in a homogeneouspopulation of young, healthy white subjects, becauseclonidine’s hemodynamic and metabolic effects arelargely influenced by various factors including gen-der,34 cardiovascular disease,26,35 and race.2 However,the response to �2-adrenergic stimulation may alsodepend on other genetic polymorphisms,36,37 and hencewe cannot preclude possible influences by these factors.
The release of growth hormone from the pituitarygland is under the dual control of somatotropin-releasing hormone and somatostatin, and this balance ismodulated by a number of other signals including thesympathetic nervous system.38 In this study the �2-adrenergic receptor–mediated increase in plasma
growth hormone was markedly attenuated in those car-riers of the T allele who responded to clonidine admin-istration. This result would be consistent with a rela-tively enhanced influence of inhibitory signals incarriers of the T allele. In view of the observed asso-ciation between the T allele and hypertension,5-9 this isan interesting finding, because previous studies haveconsistently described an attenuated growth hormoneresponse to clonidine in nonobese subjects with estab-lished hypertension relative to normotensive controlsubjects.35,39
In a previous study we did not identify an associationbetween the T allele and an enhanced vasoconstrictionin response to stimulation of peripheral �2-adrenergicreceptors in the vasculature of young, healthy malesubjects.40 In this study we demonstrated that T allelecarriers had a greater hemodynamic and metabolic re-sponse to stimulation of central �2-adrenergic recep-tors. The latter finding supports the idea of a geneticallydetermined perturbation in the CNS control of both thecardiovascular system and the endocrine system thatultimately contributes to the development of hyperten-sion and the metabolic syndrome.41
This is the third report of a relationship between thegenotype at the GNB3 locus and a drug response. In aprevious study Turner et al42 found a markedly in-creased BP-lowering effect of thiazide diuretics in car-riers of the T allele. The rationale of the study byTurner et al42 was based on the observation by Ross-kopf et al,43 who showed an enhanced in vitro sodium-hydrogen antiport in immortalized lymphoblasts ob-tained from patients with essential hypertension. Eventhough a direct pathogenetic link between the enhanced
Table II. Mean change in hemodynamic and hormonal parameters after clonidine administration for eachgenotype
Parameter
Genotype
CC CT TT CT and TT
Systolic blood pressure (mm Hg) –8.9 � 0.5 –11.2 � 0.6 –9.5 � 0.7 –10.6 � 0.4Diastolic blood pressure (mm Hg) –6.4 � 0.3 –7.5 � 0.4 –6.9 � 0.5 –7.3 � 0.3Heart rate (beats/min) –3.0 � 0.3 –3.0 � 0.5 –1.1 � 0.4 –2.4 � 0.4Stroke volume (ms) –6.0 � 0.9 –1.8 � 1.0 –13.4 � 1.7 –5.7 � 1.0Cardiac output (L · min–1) –0.56 � 0.06 –0.18 � 0.05 –0.89 � 0.12 –0.42 � 0.06Total peripheral resistance (dyne · s · cm–5) 40 � 17 –97 � 15 47 � 28 –48 � 14Total electromechanical systole, corrected (ms) 2.2 � 0.5 4.9 � 0.7 4.2 � 1.0 4.7 � 0.6Pulse wave velocity (m · s–1) –0.25 � 0.02 –0.35 � 0.03 –0.31 � 0.04 –0.33 � 0.03Norepinephrine (pg � mL–1) –12.3 � 5.8 –54.3 � 18.6 –25.9 � 6.9 –44.8 � 12.7Growth hormone (�g � mL–1) 2.4 � 0.3 1.4 � 0.3 –0.1 � 0.9 1.0 � 0.3Salivary flow (g) –0.6 � 0.1 –0.9 � 0.1 –0.2 � 0.1 –0.6 � 0.1Sedation (mm) 14.3 � 3.4 13.0 � 5.1 6.8 � 5.1 11.0 � 3.8
Data are mean � SEM.
CLINICAL PHARMACOLOGY & THERAPEUTICS58 Nurnberger et al JULY 2003

antihypertensive response to the thiazide diuretic andthe GNB3 locus was not established, the authors sug-gested that an unidentified mechanism regulating thebalance of intravasal fluid volume may be responsiblefor this observed association.42 In another study Zill etal44 reported an improved therapeutic efficacy of anti-depressant treatment in patients carrying the T allele.Antidepressant treatment increases the bioavailabilityof neurotransmitters such as norepinephrine and hy-droxytryptamine in the synaptic cleft. These neuro-transmitters mediate their effect via various receptorsincluding those coupled to G proteins. Given that it hasbeen shown in vitro that carriers of the 825T alleleshow an enhanced intracellular signal transduction viaG proteins,10,11 it is possible that such enhanced intra-cellular signaling may contribute to the improved drugresponse in patients with depression who are carryingthe T allele. These studies support the idea that theG-protein �3 gene may be a clinically relevant phar-macogenetic marker. However, further studies areneeded to investigate potential mechanisms that mayexplain the observed relationships between the C825Tpolymorphism and the response to different drugs.
In summary, this study first suggests that the C825Tpolymorphism in the GNB3 gene could serve as aclinically relevant pharmacogenetic marker in the useof centrally acting sympatholytic agents. Second, itpoints to a possible CNS mechanism linking the pres-ence of the T allele to the later development of elevatedBP.
References1. Neal B, MacMahon S, Chapman N. Effects of ACE
inhibitors, calcium antagonists, and other blood-pressure-lowering drugs: results of prospectively designed over-views of randomised trials. Blood Pressure LoweringTreatment Trialists’ Collaboration. Lancet 2000;356:1955-64.
2. Materson BJ, Reda DJ, Cushman WC, Massie BM, FreisED, Kochar MS, et al. Single-drug therapy for hyperten-sion in men. A comparison of six antihypertensive agentswith placebo. The Department of Veterans Affairs Co-operative Study Group on Antihypertensive Agents.N Engl J Med 1993;328:914-21.
3. Philipp T, Anlauf M, Distler A, Holzgreve H, MichaelisJ, Wellek S. Randomised, double blind, multicentre com-parison of hydrochlorothiazide, atenolol, nitrendipine,and enalapril in antihypertensive treatment: results of theHANE study. HANE Trial Research Group. BMJ 1997;315:154-9.
4. Roden DM, George AL Jr. The genetic basis of variabil-ity in drug responses. Nat Rev Drug Discov 2002;1:37-44.
5. Siffert W, Rosskopf D, Siffert G, Busch S, Moritz A,Erbel R, et al. Association of a human G-protein beta3subunit variant with hypertension. Nat Genet 1998;18:45-8.
6. Benjafield AV, Jeyasingam CL, Nyholt DR, Griffiths LR,Morris BJ. G-protein beta3 subunit gene (GNB3) variantin causation of essential hypertension. Hypertension1998;32:1094-7.
7. Schunkert H, Hense HW, Doring A, Riegger GA, SiffertW. Association between a polymorphism in the G proteinbeta3 subunit gene with lower renin and elevated dia-stolic blood pressure. Hypertension 1998;32:510-3.
8. Beige J, Hohenbleicher H, Distler A, Sharma AM.G-protein beta3 subunit C825T variant and ambulatoryblood pressure in essential hypertension. Hypertension1999;33:1049-51.
9. Dong Y, Zhu H, Sagnella GA, Carter ND, Cook DG,Cappuccio FP. Association between the C825T polymor-phism of the G protein beta3-subunit gene and hyperten-sion in blacks. Hypertension 1999;34:1193-6.
10. Siffert W, Rosskopf D, Moritz A, Wieland T,Kaldenberg-Stasch S, Kettler N, et al. Enhanced G pro-tein activation in immortalized lymphoblasts from pa-tients with essential hypertension. J Clin Invest 1995;96:759-66.
11. Virchow S, Ansorge N, Rubben H, Siffert G, Siffert W.Enhanced fMLP-stimulated chemotaxis in human neutro-phils from individuals carrying the G protein beta3 sub-unit 825 T-allele. FEBS Lett 1998;436:155-8.
12. Richardson M, Robishaw JD. The alpha2A-adrenergicreceptor discriminates between Gi heterotrimers of dif-ferent betagamma subunit composition in Sf9 insect cellmembranes. J Biol Chem 1999;274:13525-33.
13. Aicher SA, Drake CT. Clonidine evokes vasodepressorresponses via alpha2-adrenergic receptors in gigantocel-lular reticular formation. J Pharmacol Exp Ther 1999;289:688-94.
14. Bylund DB, Bond RA, Clarke DE, Eikenburg DC, HiebleJP, Langer SZ, et al. Adrenoceptors. In: The IUPHARcompendium of receptor characterization and classifica-tion. London: IUPHAR Media; 1998. p. 58-74.
15. Li Q, Belz GG. Systolic time intervals in clinical phar-macology. Eur J Clin Pharmacol 1993;44:415-21.
16. Boudoulas H. Systolic time intervals. Eur Heart J 1990;11:93-104.
17. Northridge DB, Findlay IN, Wilson J, Henderson E,Dargie HJ. Non-invasive determination of cardiac outputby Doppler echocardiography and electrical bioimped-ance. Br Heart J 1990;63:93-7.
18. White SW, Quail AW, de Leeuw PW, Traugott FM,Brown WJ, Porges WL, et al. Impedance cardiographyfor cardiac output measurement: an evaluation of accu-racy and limitations. Eur Heart J 1990;11(Suppl I):79-92.
19. Schafers RF, Nurnberger J, Herrmann B, Wenzel RR,Philipp T, Michel MC. Adrenoceptors mediating the car-diovascular and metabolic effects of alpha-
CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 74, NUMBER 1 Nurnberger et al 59
methylnoradrenaline in humans. J Pharm Exp Ther 1999;289:918-25.
20. Bramwell JC, Hill AV. Velocity of transmission of thepulse wave and elasticity of arteries. Lancet 1922;1:891-2.
21. Haynes FW, Ellis L, Weiss S. Pulse wave velocity andarterial elasticity in arterial hypertension, arteriosclerosisand related conditions. Am Heart J 1936;11:385-401.
22. Schafers RF, Adler S, Daul A, Zeitler G, Vogelsang M,Zerkowski HR, et al. Positive inotropic effects of the beta2-adrenoceptor agonist terbutaline in the human heart:effects of long-term beta 1-adrenoceptor antagonist treat-ment. J Am Coll Cardiol 1994;23:1224-33.
23. Macphee GJ, Howie CA, Elliot HL, Reid JL. A compar-ison of the haemodynamic and behavioural effects ofmoxonidine and clonidine in normotensive subjects. Br JClin Pharmacol 1992;33:261-7.
24. Johnson A, Blackwell CP, Smith J. Antagonism of theeffects of clonidine by the alpha2-adrenoceptor antago-nist, fluparoxan. J Clin Pharmacol 1995;39:477-83.
25. Benedict CR. Centrally acting antihypertensive drugs:re-emergence of sympathetic inhibition in the treatmentof hypertension. Curr Hypertens Rep 1999;1:305-12.
26. Lang CC, Stein CM, Nelson RA, He HB, Belas FJ, BlairIA, et al. Sympathoinhibitory response to clonidine isblunted in patients with heart failure. Hypertension 1997;30:392-7.
27. Grassi G, Turri C, Seravalle G, Bertinieri G, Pierini A,Mancia G. Effects of chronic clonidine administration onsympathetic nerve traffic and baroreflex function in heartfailure. Hypertension 2001;38:286-91.
28. Kienbaum P, Heuter T, Michel MC, Scherbaum N, Gast-par M, Peters J. Sympathetic neural activation evoked bymu-receptor blockade in patients addicted to opioids isabolished by intravenous clonidine. Anesthesiology2002;96:346-51.
29. Wing LM, Reid JL, Hamilton CA, Sever P, Davies DS,Dollery CT. Effects of clonidine on biochemical indicesof sympathetic function and plasma renin activity innormotensive man. Clin Sci Mol Med 1977;53:45-53.
30. Hokfelt B, Hedeland H, Hansson BG. The effect ofclonidine and penbutolol, respectively on catecholaminesin blood and urine, plasma renin activity and urinaryaldosterone in hypertensive patients. Arch Int Pharmaco-dyn Ther 1975;213:307-21.
31. Nurnberger J, Dammer S, Opazo Saez A, Philipp T,Schafers RF. Diastolic blood pressure is an importantdeterminant of augmentation index and pulse wave ve-locity in young, healthy males. J Hum Hypertens 2003;17:153-8.
32. Schafers RF, Piest U, von Birgelen C, Jakubetz J, DaulAE, Philipp T, et al. Disodium cromoglycate does notprevent terbutaline-induced desensitization of beta
2-adrenoceptor-mediated cardiovascular in vivo func-tions in human volunteers. J Cardiovasc Pharmacol 1999;33:822-7.
33. Boudoulas H, Lewis RP, Kates RE, Dalamangas G. Hy-persensitivity to adrenergic stimulation after propranololwithdrawal in normal subjects. Ann Intern Med 1977;87:433-6.
34. Karlsson S, Scheurink AJ, Ahren B. Gender difference inthe glucagon response to glucopenic stress in mice. Am JPhysiol Regul Integr Comp Physiol 2002;282:R281-8.
35. Barbieri C, Ferrari C, Caldara R, Curtarelli G. Growthhormone secretion in hypertensive patients: evidence fora derangement in central adrenergic function. Clin Sci(Lond) 1980;58:135-8.
36. Small KM, Liggett SB. Identification and functionalcharacterization of alpha(2)-adrenoceptor polymor-phisms. Trends Pharmacol Sci 2001;22:471-7.
37. Freeman K, Farrow S, Schmaier A, Freedman R, SchorkT, Lockette W. Genetic polymorphism of the alpha2-adrenergic receptor is associated with increased plateletaggregation, baroreceptor sensitivity, and salt excretionin normotensive humans. Am J Hypertens 1995;8:863-9.
38. Muller EE, Locatelli V, Cocchi D. Neuroendocrine con-trol of growth hormone secretion. Physiol Rev 1999;79:511-607.
39. Giustina A, Doga M, Bossoni S, Bodini C, Legati F,Pizzocolo G, et al. Central alpha-2 adrenergic function inpatients with essential hypertension. Comparative studyof growth hormone (GH) secretion stimulated byclonidine and GH-releasing hormone. Horm Metab Res1990;22:451-2.
40. Schafers RF, Nurnberger J, Rutz A, Siffert W, WenzelRR, Mitchell A, et al. Haemodynamic characterization ofyoung normotensive men carrying the 825T-allele of theG-protein beta3 subunit. Pharmacogenetics 2001;11:461-70.
41. Bjorntorp P, Holm G, Rosmond R, Folkow B. Hyperten-sion and the metabolic syndrome: closely related centralorigin? Blood Press 2000;9:71-82.
42. Turner ST, Schwartz GL, Chapman AB, Boerwinkle E.C825T polymorphism of the G protein beta(3)-subunitand antihypertensive response to a thiazide diuretic. Hy-pertension 2001;37:739-43.
43. Rosskopf D, Fromter E, Siffert W. Hypertensive sodium-proton exchanger phenotype persists in immortalizedlymphoblasts from essential hypertensive patients. A cellculture model for human hypertension. J Clin Invest1993;92:2553-9.
44. Zill P, Baghai TC, Zwanzger P, Schule C, Minov C,Riedel M, et al. Evidence for an association between aG-protein beta3-gene variant with depression and re-sponse to antidepressant treatment. Neuroreport 2000;11:1893-7.
CLINICAL PHARMACOLOGY & THERAPEUTICS60 Nurnberger et al JULY 2003