HF Primary Care Roadmap · 3 HFpEF vs HFrEF 1) HF w/ Reduced EF (HFrEF), Systolic: EF ≤ 40% 2) HF...
45
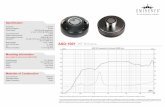
1 Jennifer Jones, MD North Florida Regional Medical Ctr. Family Medicine GME Program [email protected] HF Primary Care Roadmap HFrEF Diuretics Digoxin ACE/ARB β-Blocker Aldosterone Antagonist Ivabradine Sacubitril-Valsartan Lifestyle Modification: H20/Na+ Restriction; Flu & Pneumovax; Weight Management; Exercise/Cardiac Rehab Disease Modifying Rx Symptom Modifying Rx ECHO / BNP HFpEF Comorbidities: HTN, Anemia, COPD, ETOH, CAD, Arrhythmia Cardiology Consult AICD/CRT ISDN/Hydralazine (African Am) HF: The Hemodynamic Malignancy “The prognosis of affected individuals is dismal, as fewer than 50% of these people survive 5 years from the time of initial Dx.” - Mulrow C. JAMA 1987;259(23):3422-3425 “Mortality from CHF is high, averaging 30% within the 1 st year, 50% by 3-4 years, and 80% by 6-10 years” – Anderson J. Modern Medicine 1987;55(May)
Transcript of HF Primary Care Roadmap · 3 HFpEF vs HFrEF 1) HF w/ Reduced EF (HFrEF), Systolic: EF ≤ 40% 2) HF...

1
Jennifer Jones, MD
North Florida Regional Medical Ctr.
Family Medicine GME Program
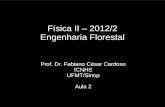
HF Primary Care Roadmap
HFrEF
Diuretics
Digoxin
ACE/ARB
β-Blocker Aldosterone Antagonist
Ivabradine
Sacubitril-Valsartan
Lifestyle Modification: H20/Na+ Restriction; Flu & Pneumovax;
Weight Management; Exercise/Cardiac Rehab
Disease
Modifying Rx
Symptom
Modifying Rx
ECHO / BNP HFpEF
Comorbidities: HTN, Anemia, COPD, ETOH, CAD, Arrhythmia
Cardiology
Consult AICD/CRT
ISDN/Hydralazine (African Am)
HF: The Hemodynamic Malignancy
“The prognosis of affected individuals is dismal,
as fewer than 50% of these people survive 5
years from the time of initial Dx.” - Mulrow C. JAMA 1987;259(23):3422-3425
“Mortality from CHF is high, averaging 30%
within the 1st year, 50% by 3-4 years, and 80%
by 6-10 years” – Anderson J. Modern Medicine 1987;55(May)

2
HF: The Hemodynamic Malignancy
Prospective Cohort Study (n= 558)
Total Mortality at 5 years
Systolic Dysfunction= 42%
Diastolic Dysfunction = 25%
MacCarthy PA, Kearney MT, Nolan J, et al. “Prognosis in heart failure with preserved left
ventricular systolic function: prospective cohort study” BMJ 2003; 327:78-9.
“Although survival has improved, the
absolute mortality rates for HF remain
~50% within 5 yrs of dx.”
-2013 ACCF/AHA Guidelines
HF: The Hemodynamic Malignancy
Clyde W. Yancy et al. Circulation. 2013;128:1810-1852
Definition of HF
Clinical syndrome resulting from structural or functional
impairment of ventricular filling or ejection of blood.
• Exercise Intolerance (dyspnea & fatigue)
• Fluid Retention (NOT everyone; ≠CHF)
Cardiac output(CO) ≠ tissue metabolic requirement
Sustained Sympathetic Nervous Sys (SNS) Activation
Sustained RAAS activation
Clyde W. Yancy et al. Circulation. 2013;128:1810-1852

3
HFpEF vs HFrEF
1) HF w/ Reduced EF (HFrEF), Systolic: EF ≤ 40%
2) HF w/ Preserved EF (HFpEF), Diastolic : EF > 50%
& clinical syndrome HF, abnormal LV diastolic filling
• ~50%; more challenging dx
• Elderly female w/ HTN; Obese, CAD, DM, Afib, HLD
HFpEF, borderline: EF = 41-49%
HFpEF previously with HFrEF
Clyde W. Yancy et al. Circulation. 2013;128:1810-1852
Functional Classifications
ACCF/AHA: development & progression of dz
NYHA: exercise capacity & symptomatic status
Stages are progressive
• Progression ↓ 5-yr survival; ↑ BNP
Clyde W. Yancy et al. Circulation. 2013;128:1810-1852
ACCF/AHA Stages of HF NYHA
A At high risk but Asymptomatic +
NO structural heart disease
B Structural heart dz but
Asymptomatic I
C Structural heart dz with current
or prior symptoms I-IV
D Refractory HF IV
Clyde W. Yancy et al. Circulation. 2013;128:1810-1852c

4
Functional Classifications: NYHA
Criteria Committee of the New York Heart Association, 1964.
Class I Ordinary physical activity does NOT cause
undue fatigue, palpitations, SOB +/or angina.
Class II Ordinary physical activity causes undue Sx
Class III < ordinary physical activity causes undue Sx
Class IV Sx with any physical activity or at rest
Functional Classifications: NYHA
Strenuous→Sx (Class I)
Ordinary → Sx (Class II)
Minimal → Sx (Class III)
Anything → Sx (Class IV)
Neurohormones
• ↑ SNS/Catecholamines
• ↑ RAAS (A-II, ADH)
• ↑ANP/BNP
• LV Remodeling
• ↓CO
• Systolic dysfxn
• Diastolic dysfxn
• Combined dysfxn
G. Hasenfuss and D. Mann. Braunwald’s Heart Disease: A Textbook of CV Medicine, 22, 454-472.e3
Ischemia
HTN
Myopathy
Compensation Consequence

5
…once upon a time, a young man
was walking his elephant….
The Story of RAAS
Lots & lots
Of
Blood
OUCH!
RAAS To The RESCUE!!
• A-I: Selective Vasoconstriction
• NE: Vascular Tone, Heart Rate, Contractility
• Aldosterone: Salt, Water retention, Thirst
Argggh!
Ssshhh…
I’m Hiding.

6
• Selective vasoconstriction bleeding stopped • Flow maintained to muscles, heart, brain • 4 quarts low: heart beat faster, harder • Insensitive fluid losses (saliva, sweat, urine) • Thirsty
…and they all LIVED
happily ever after
• ↑ SNS/Catecholamines
• ↑ RAAS (A-II, ADH)
• ↑ANP/BNP
• LV Remodeling
• ↓CO
• Systolic dysfxn
• Diastolic dysfxn
• Combined dysfxn
G. Hasenfuss and D. Mann. Braunwald’s Heart Disease: A Textbook of CV Medicine, 22, 454-472.e3
Index Event
Ischemia
HTN
Myopathy
Compensation Consequence

7
RAAS ⇆ HF
Aldosterone
Angiotensinogen
Na+ retention/ ↑ IVV
Angiotensin I
Angiotensin II
Vasoconstrict/↑SVR
RENIN
ACE
Angiotensin II NE Aldosterone
Blastic Cardiac Fibroblast
Collagen
Proliferation
Clastic Cardiac Fibroblast
Collagen
Degradation
RAA Hyperactivation Excess collagen

8
Brain Natriuretic Peptide (BNP)
• First isolated in porcine brain
• Synthesized but not stored in ventricular myocytes
• Ventricular Stress (↑ LVEDP) ↑ BNP
Cheung BM, Kumana CR. “Natriuretic Peptides-Relevance in Cardiovascular Disease.” JAMA.
1998;280(23):1983-1984.
BNP : Potential Clinical Roles
1) Diagnosis or Exclusion of HF
2) Monitor CHF progress/Guide Rx
3) Prognostic Indicator/Preventing Readmission
–Congestion End-diastolic wall stress ↑BNP
–Studies show congestion may precede Ac.HF Sx by 7-10 days
Maisel AS, Daniels LB. Breathing Not Properly 10 Years Later: What We Have Learned and What We
Still Need to Learn. J Am Coll Cardiol.2012;60(4):277-282.

9
Causes for ↑ Natriuretic Peptide Levels
Cardiac Noncardiac
Heart failure, including RV
Acute coronary syndrome
Heart muscle dz (LVH)
Valvular heart disease
Pericardial disease
Atrial fibrillation
Myocarditis
Cardiac surgery
Cardioversion
Advancing age
Anemia
Renal failure
Pulm: OSA; PNA, Pulm HTN
Critical illness
Bacterial sepsis
Severe burns
Toxic-metabolic insults (eg
chemotherapy, envenomation)
Clyde W. Yancy et al. Circulation. 2013;128:1810-1852
*Decreased levels in Obesity
BNP: Diagnostic Role
• Study: n=250 Pts w/ Ac. SOB in VA Urgent
Care/ED
• 2 Cardiologists retrospectively reviewed clinical
data (blinded to BNP) and made an opinion as to
etiology
Dao Q, Krishnaswamy P, Kazanegra R, et al. “Utility of B-Type Natriuretic Peptide in the
Dx of CHF in an Urgent Care Setting.” J Am Coll Cardiol. 2001 Feb;37(2):379-85.
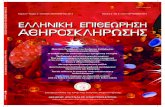
BNP Levels in Dyspneic Pts
0
200
400
600
800
1000
1200
COPD (n=56) CHF (n=94)
COPD (n=56)
CHF (n=94)
86 ± 39
1076 ± 138
BN
P C
on
ce
ntr
ati
on
(p
g/m
l)
Dao Q, Krishnaswamy P, Kazanegra R, et al. “Utility of B-Type Natriuretic Peptide in the
Dx of CHF in an Urgent Care Setting.” J Am Coll Cardiol. 2001 Feb;37(2):379-85.

10
BNP: CHF Severity
0
500
1000
1500
2000
2500
Mild (n=27) Moderate (n=34) Severe (n=36)
186 ± 22
791 ± 165
2013 ± 266
BN
P C
on
cen
tra
tio
n (
pg
/ml)
Dao Q, Krishnaswamy P, Kazanegra R, et al. “Utility of B-Type Natriuretic Peptide in the
Dx of CHF in an Urgent Care Setting.” J Am Coll Cardiol. 2001 Feb;37(2):379-85.
• BNP ≥80 pg/ml accurately predicted dx of CHF (95%)
• BNP <80 pg/ml had high negative predictive value (98%).
• BNP measurements could have potentially corrected 29
of the 30 diagnoses missed by urgent-care physicians.
BNP: Diagnostic Role
Dao Q, Krishnaswamy P, Kazanegra R, et al. “Utility of B-Type Natriuretic Peptide in the
Dx of CHF in an Urgent Care Setting.” J Am Coll Cardiol. 2001 Feb;37(2):379-85.
STARS-BNP: BNP-guided Tx
• n=220 NYHA II-III pts on ACE, BB, diuretics randomized:
– Clinical Group (tx guided by HF specialists/guidelines)
– BNP Group (tx guided to target BNP <100 pg/ml)
• F/u every month x 3 mos q3 mos x ~15 mos
• 1° Outcome: HF related Death or Hospitalization
Jourdain P, et al. Plasma BNP-guided therapy to improve outcome in heart failure: the STARS-BNP
Multicenter Study. J Am Coll Cardiol. 2007 Apr 24;49(16):1733-9.

11
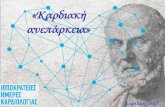
STARS-BNP: Results
BNP grp: fewer
HF Deaths and
Hospitalizations
(24% vs 52%)
Jourdain P, et al. Plasma BNP-guided therapy to improve outcome in heart failure: the STARS-BNP
Multicenter Study. J Am Coll Cardiol. 2007 Apr 24;49(16):1733-9.
EV
EN
T F
RE
E S
UR
VIV
AL
(%
)
DAYS (15 mos)
BNP
Clinical
p<0.001
STARS-BNP: Results
At 3 months,
more med Δ’s
in the BNP grp
w/ higher mean
dosages of
ACEIs and BBs
Jourdain P, et al. Plasma BNP-guided therapy to improve outcome in heart failure: the STARS-BNP
Multicenter Study. J Am Coll Cardiol. 2007 Apr 24;49(16):1733-9.
Breathing Not Properly (BNP) Study: Dx and Prognosis
• Prospective Obs. study; n=1,586 w/ Ac. SOB
• 2 Dx Methods compared to Cardiologist Dx
1. NHANES and Framingham criteria for Dx CHF
2. BNP
• OUTCOME:
– Single BNP more accurate than criteria scores for Dx of CHF
– pts whose 30d BNP level was > discharge BNP level were at
highest risk for decompensation/readmission
Maisel AS, Daniels LB. Breathing Not Properly 10 Years Later: What We Have Learned and What We
Still Need to Learn. J Am Coll Cardiol.2012;60(4):277-282.

12
BNP Study: Obesity and BNP Levels
52 35 25
643
462
247
BMI < 25 25≤ BMI <35 BMI ≥ 35
No Acute CHF Acute CHF
BN
P (
pg
/mL
)
Daniels LB, Clopton P, et al. How Obesity Affects the Cut-Points for B-Type Natriuretic Peptide in the
Diagnosis of Acute Heart Failure. Am Heart J. 2006;151(5):999-1005.
P<0.05)
170
110
54
0
20
40
60
80
100
120
140
160
180
BMI < 25 25≤ BMI < 35 BMI ≥ 35 Daniels LB, Clopton P, et al. How Obesity Affects the Cut-Points for B-Type Natriuretic Peptide in the
Diagnosis of Acute Heart Failure. Am Heart J. 2006;151(5):999-1005.
BNP Study: Obesity and BNP Levels 90% Sensitivity BNP cut-offs for different BMIs
BN
P (
pg
/ml)
BNP: Good for Dx, Guided Tx & Px
• “Although trials examining BNP-guided HF management
were small, 2 comprehensive meta-analysis showed
BNP-guided Tx reduces all-cause mortality in pts w/
chronic HF vs usual clinical care….this may be
attributed to increased achievement of GDMT.”
• Falsely low levels in obesity and HFpEF.
Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.

13
Noninvasive Cardiac Imaging
Patients with suspected or new-onset HF, or
acute decompensated HF, should undergo a
chest x-ray to assess heart size and pulmonary
congestion, and detect alternative cardiac,
pulmonary, and other diseases that may cause
or contribute to the patients’ symptoms.
I IIa IIb III
Noninvasive Cardiac Imaging
A 2-D Echo w/ Doppler should be performed
for initial eval of pts presenting with HF to
assess ventricular fxn, size, wall thickness, wall
motion, and valve fxn.
Repeat Echo in pts w/ HF who have had
significant change in clinical status, received
GDMT, or candidate for device therapy.
I IIa IIb III
I IIa IIb III
Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.

14
Goal Directed Medical Tx (GDMT) and HRQOL
HF decreases Health-Related Quality of Life (HRQOL)
Lack of improvement in HRQOL after hosp discharge is
a predictor of re-hospitalization and mortality
• ACE/ARBs modestly improve or delay progressive
worsening of HRQOL
• Cardiac Resynchronization therapy (CRT) and dz
management/education are shown to improve HRQOL
Clyde W. Yancy et al. Circulation. 2013;128:1810-1852
Stages in the development of HF and recommended therapy by stage.
Clyde W. Yancy et al. Circulation. 2013;128:e240-e327
STAGE A = At High risk for HF but w/o structural heart dz/Sx
e.g. Patients with:
• HTN
• ATH
• DM
• Obesity
• Or patients
• using
cardiotoxins
• w/ FH CM
Goals:
• Heart healthy lifestyle
• Prevent vasc/CAD
• Prevent LV structural
abnormalities
Drugs:
• ACEI/ARB (vasc dz or DM)
• Statins
Structural
Heart
Disease
Clyde W. Yancy et al. Circulation. 2013;128:e240-e327

15
STAGE B: Structural Heart Dz w/o S/Sx HF
GOALS: DRUGS:
•Prevent HF Sx - ACE/ARB
•Prevent further Cardiac Remodeling -Beta Blockers
In Selected Patients: ICD or Revascularization or Valve Sx
Patients with:
• Prior MI
• LV Remodeling (LVH, Low EF)
• Valvular Disease
HF Sx
Develop
Clyde W. Yancy et al. Circulation. 2013;128:e240-e327
Modifiable Risk Factors
• HTN
• Salt Intake
• Dyslipidemia/ATH
• Obesity/Overweight
• Diabetes Mellitus
• Substance Abuse (ETOH/Tobb/Cocaine)
• AFib (rate control)
• OSA (CPAP improve EF/functional status)
Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.
BP Control
• Long-term tx of both systolic and diastolic HTN
reduces risk of HF by ~ 50%
– 2013 ACCF/AHA HF Guidelines
• SPRINT Trial (n=9,361)
–Non DM pts with HTN were ~40% less likely to
develop HF if treated to a goal SBP <120
compared to a SBP goal <140
The SPRINT Research Group. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med 2015;373:2103-2016

16
BP Control: To Prevent HF Intensive BP Control Intensive BP Control in
pts w/ prior MI
Decreases
risk of new
HF by ~50%;
56% in DM2
Decreases
risk of HF by
~ 80%
Lancet 1991;338:1281:1281-5 (STOP-Hypertension).
UKPDS Group. UKPDS 38.BMJ 1998;317:703-713. JAMA 1997;278:121-6 (SHEP).
Sodium Restriction?
• Obs. study: 902 pts NYHA II-III; Systolic or Diastolic HF
• METHOD: Na+ intake assessed over 36 months using a
food freq. questionnaire; pts classified as either Na+
Restricted (<2500mg/d) or Unrestricted (≥2500 mg/d).
• OUTCOME: composite of death or HF hospitalization
Doukky R, Avery E, Mangla A, et al. Impact of Dietary Sodium Restriction on Heart Failure
Outcomes. JCHF. 2016;4(1):24-35.
Sodium Restriction?
• Na+ Restriction Higher Risk of HF hospitalization or
death (42% v 26%; HR 1.85; p=0.004)
• Highest risk increase in those not taking ACE/ARB
(HR 5.78; P=0.002) and NYHA II (HR 2.36; P=0.003)
• ACCF/AHA SOR for Na+ restriction downgraded
– Class I (recommended) Class IIa (reasonable)
Doukky R, Avery E, Mangla A, et al. Impact of Dietary Sodium Restriction on Heart Failure
Outcomes. JCHF. 2016;4(1):24-35.

17
ACCF/AHA Guideline Rec on Na+
• “No study to date has evaluated the effects of Na+
restriction on neurohormonal activation and outcomes in
optimally treated HF pts.”
– 1 observational study that evaluated pts with HFpEF.
• Should Na+ recommendations vary w/ HF type, severity,
related comorbidities, or race?
Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.
Cardiac Rehabilitation
• “Cardiac rehab reduces mortality; improves
functional capacity, exercise duration, and
HRQOL and reduces hospitalizations.”
–ExTraMATCH Trial: Exercise Training Meta-
Analysis of Trials in pts with Chronic HF
–RCT (HF-ACTION Trial) did NOT show benefit w/
ex training except in subgrp of pts w/ CAD RFs
Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.
ExTraMATCH: Ex Training in HF 9 studies; n= 801; Training programs 8 wks to >1yr
ExTraMATCH Collaborative. BMJ 2004;328:189.
26%
43%
22%
32%
0%
10%
20%
30%
40%
50%
Mortality(HR 0.65; p=0.02)
Mortality or Admission(HR 0.72; p=0.01)
Control Exercise Training

18
Statistically Sig No Significant Diff ? Insuff Evidence
Transitional Care Interventions vs Usual Care for HF
AHRQ ↓ All-Cause
Readmit
↓HF
Readmit
↓Mortality ↓ # Hosp
Days
Home Visit Program
Phone Support
Multidisciplinary HF
Clinics ? ?
Nurse-Led HF Clinics ? ?
Guirguis-Blake J. Transitional Care Interventions to Prevent Readmissions for Patients with Heart Failure.
Am Fam Physician. 2016; 93(5):401-403.
AHRQ: HF Transitional Care Intervention
High-Intensity Home Visiting Programs (5+ visits)
–Meta-analysis (15 RCTs)
• 25% ↓ All-cause Readmits (n=1,563; NNT=9)
• 49% ↓ HF Readmits (n=282; NNT=7)
• 23% ↓ Mortality (n=1,693; NNT=33)
Structured Telephone Support
– Meta-analysis (13 RCTs)
• 26% ↓ HF Readmissions (n=1,790); NNT=14)
• 26% ↓ Mortality (n=2,011; NNT=27) Guirguis-Blake J. Transitional Care Interventions to Prevent Readmissions for Patients with Heart Failure.
Am Fam Physician. 2016; 93(5):401-403.
AHRQ: HF Transitional Care Interventions
Multidisciplinary HF Clinics: frequent regular
scheduled visits with multiple clinicians
–Meta-analysis (7 RCTs)
•30% ↓ All-Cause Readmits (n=336; NNT=8)
•44% ↓ Mortality (n=536; NNT=18)
Guirguis-Blake J. Transitional Care Interventions to Prevent Readmissions for Patients with Heart Failure.
Am Fam Physician. 2016; 93(5):401-403.

19
HFrEF Stage C (NYHA I-III) Treatment:
ACEI/ARB
and
BBlker
Hydral-
Nitrates
Loop
Diuretic
Volume Overloaded
(NYHA II-IV)
AA w/ persistant Sx
(NYHA III-IV)
CrCl>30mL/min
K+ <5.0mEq/dL
(NYHA II-IV)
ADD ADD ADD
Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.
Aldosterone
Antagonist
Class I Recommendations
NYHA I ???
Guideline Recommended HFrEF Txs Guideline Rec’d Tx RRR in RCTs NNT for Mortality (12 m)
ACE/ARB 17% 77
Beta-Blocker 34% 28
Aldosterone Antagonist 30% 18
Hydralazine + Nitrate * 43% 21
Cardiac Resynchronization (CRT) 36% 24
Implantable Cardioverter Defib (ICD) 23% 70
Colucci, WS. Overview of therapy in heart failure with reduced ejection fraction. In: UpToDate,
Post TW (Ed), UpToDate, Waltham, MA. (Accessed on March 31, 2016). Figure Modified. *African-Americans
• Evidence diuretics improve symptoms and
exercise tolerance in HF
• Loop diuretics (Bumetanide, furosemide, torsemide)
• Thiazides (Chlorthalidone, HCTZ, Metolazone)
• K-sparing (Spironolactone, Triamterene, Amiloride)
• Goal: eliminate clinical fluid retention
–Titrate to ↑UOP and ↓weight by 0.5-1.0 kg/d
Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.

20
ACE-Inhibitors in HFrEF
• Shown to reduce HF progression, mortality &
hospitalization; improve HRQOL
• Initiate at low doses and titrate to target dose
(shown to reduce CV risk in clinical trials)
– Lisinopril 20 mg/d
• Reassess renal function 1-2 weeks after initiation
Delahaye F, Gevigney G. Is the Optimal Dose of ACEI in Patients with CHF Definitely
Established? JACC. 2000;36(7): 2096-2097.
RAAS ⇆ HF
Aldosterone
Angiotensinogen
Na+ retention/ ↑ IVV
Angiotensin I
Angiotensin II
Vasoconstrict/↑SVR
RENIN
ACE

21
ACE Inhibitor RAA Modulation
Angiotensinogen
Bradykinin
Angiotensin I
Angiotensin II
RENIN
ACE
Inactive
Bradykinin
components
Aldosterone AT I
ACEI ACE
↑ ↑ NO
Bronchoconstriction
ARB
Fosinopril in Chr. HFrEF
• STUDY: RCT; N=241 NYHA II-III and LVEF 25±7%
• 24wk Fosinopril 10-20mg/d or Placebo
• OUTCOMES:
– ∆ max treadmill exercise time
– worsening heart failure (death, hosp, ED, NYHA progression)
Brown E, et al. Effects of fosinopril on exercise tolerance and clinical deterioration in patients with
chronic congestive heart failure not taking digitalis. Am Journal Card. 1995;75(8):596-600.
ETT improved w/ Fosinopril Group
+ 28.4
-13.5 -20
-15
-10
-5
0
5
10
15
20
25
30
35
Placebo Fosinopril
Tre
adm
ill E
xerc
ise
Tim
e (s
ecs)
p = 0.047
Brown E, et al. Effects of fosinopril on exercise tolerance and clinical deterioration in patients with
chronic congestive heart failure not taking digitalis. Am Journal Card. 1995;75(8):596-600.

22
Fosinopril: NYHA Class Progression
13%
32%
24%
18%
Improved Worsened
Placebo
Fosinopril
Brown E, et al. Effects of fosinopril on exercise tolerance and clinical deterioration in patients with
chronic congestive heart failure not taking digitalis. Am Journal Card. 1995;75(8):596-600.
p=0.003
-35%
-30%
-25%
-20%
-15%
-10%
-5%
0%
Sx Improvement/Worsening: Fosinopril
0%
10%
20%
30%
40%
50%
60%
70%
80%
Placebo
Fosinopril
30% 28%
70%
8%
15% 17%
33%
23%
29%
Brown E, et al. Am Journal Card. 1995;75(8):596-600.
% W
ors
ened
%
Imp
rove
d
Dyspnea Fatigue
PND
*p ≤ 0.002
16% 25%
14%
SOLVD: Enalapril in HFrEF
• STUDY: DB RCT; n=2,569 pts w/ Chr. HF (EF≤35%)
• Mean F/u 41 mos; Enalapril 2.5mg-20mg/day or Placebo
• OUTCOMES:
–1⁰ Death
–2⁰ Hospitalization + Death
The SOLVD Investigators. Effect of Enalapril on Survival in Patients with Reduced Left Ventricular
Ejection Fractions and Congestive Heart Failure. N Engl J Med 1991; 325:293-302.

23
SOLVD: Enalapril in HFrEF
40%
57%
35%
48%
0%
10%
20%
30%
40%
50%
60%
Death Hosp or Death
Placebo EnalaprilThe SOLVD Investigators. Effect of Enalapril on Survival in Patients with Reduced Left Ventricular
Ejection Fractions and Congestive Heart Failure. N Engl J Med 1991; 325:293-302.
p<0.05
SAVE: Captopril for HFrEF Post-MI
• N=2,231; 3-16d post-MI w/ EF ≤40% but w/o overt HF
• Mean f/u 42 months; Captopril or Placebo
• Outcomes: 1° Mortality
– CV Morbidity (severe CHF or recurrence of MI)
– CV Morbidity + Mortality
Pfeffer MA. Effect of Captopril on Mortality and Morbidity in Patients with Left Ventricular Dysfunction after Myocardial
Infarction — Results of the Survival and Ventricular Enlargement Trial. N Engl J Med. 1992;327(10):669-77.
Pfeffer MA et al. N Engl J Med 1992;327:669-677. Figure 3 Modified.
SAVE: CV Morbidity and Mortality.
Pla
ceb
o
Cap
top
ril
*p < 0.05
† p < 0.005

24
Any ACEI will do.
• Meta-Analysis 32 RCTs (n=7105); Rx min 8 wks
• Total Mortality (P<0.001)
Placebo 21.9% vs ACEI 15.8%
• Combined Mortality and Hospitalization for HF (P<0.001)
Placebo 32.6% vs ACEI 22.4%
• Benefits observed with several different ACE Inhibitors:
(Enalapril, Captopril, Ramipril, Quinapril, Lisinopril)
Garg R, Yusuf S. Overview of randomized trials of ACEIs on mortality and morbidity in patients with
heart failure. Collaborative Group on ACE Inhibitor Trials. JAMA. 1995 May 10;273(18):1450-6
2013 ACCF/AHF HF Guidelines: ARBs
“ARBs are recommended in pts w/
HFrEF w/ current or prior Sx who are
ACEI intolerant, to reduce morbidity and
mortality.” (Class I Rec; LOE: A)
Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.
ARBS in Patients Not Taking ACE Inhibitors:
Val-HeFT & CHARM-Alternative
Val-HeFT
Valsartan
Placebo
p = 0.017
Months
Su
rviv
al
%
CV
De
ath
or
HF
Ho
sp
%
Placebo
Candesartan
CHARM-Alternative
HR 0.77, p = 0.0004
Months
Maggioni AP et al. JACC 2002;40:1422-4.
Granger CB et al. Lancet 2003;362:772-6.
50
60
70
80
90
100
0 3 6 9 12 15 18 21 24 27
0
10
20
30
40
50
0 9 18 27 36 42

25
2013 ACCF/AHA HF Guidelines: Beta-Blkers (BB)
“1 of the 3 BBs proven to reduce mortality
(bisoprolol, carvedilol, metoprolol succinate)
is recommended for ALL pts w/ current or prior
symptoms of HFrEF to reduce morbidity and
mortality.”
(Level of Evidence: A)
Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.
Beta-Blockers in HFrEF
• Lessen Sx of HF
• Improve clinical status
• Enhance overall sense of well-being
• Reduce mortality
• Reduce hospitalization
*Benefits observed in pts already on ACE inhibitors Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.

26
COPERNICUS: Carvedilol in HFrEF
• RCT; n=2,289 NYHA III-IV and EF <25%
• Placebo (n=1,133) vs. carvedilol (n=1156) x ave 10 mos
• OUTCOMES
–↓ Risk of CV Death or Hosp by 27% (p*)
–↓ Risk HF Death or Hosp by 31% (p*)
–↓ Days in Hosp by 27%; 40% fewer days for HF (p*)
–↓ Serious AE (worsened HF, cardiac death/shock, VT)
Milton Packer et al. Circulation. 2002;106:2194-2199 *p < 0.05
COPERNICUS: Time to CV Death or Hosp
Milton Packer et al. Circulation. 2002;106:2194-2199
↓ Risk of CV
Death or Hosp by
27%
(p=0.00002)
COPERNICUS: Time to HF Death or Hosp
Milton Packer et al. Circulation. 2002;106:2194-2199
↓ Risk of HF
Death or Hosp by
31%
(p=0.000004)

27
MERIT-HF: Metoprolol Succinate
• RCT; n=3,991 stable NYHA II-IV, EF ≤40%
(already on ACE, Digoxin, Hydralazine/Nitrate, Diuretic)
• Initially Randomized to:
– Metoprolol CR/XL 12.5mg or 25mg qd or Placebo
• Target: Metoprolol CR/XL 200mg qd (titrated x 8 wks)
– mean dose = 159mg/d
• 1° OUTCOME: All-Cause Mortality
MERIT-HF Study Group. The Lancet , Volume 353 , Issue 9169 , 2001 – 2007.
MERIT-HF: All-Cause Mortality
Reduction in
Total Mortality
7.2% vs 11 %
34% RRR (p=0.006)
MERIT-HF Study Group. The Lancet , Volume 353 , Issue 9169 , 2001 – 2007.
Metoprolol CR/XL
Placebo
Cum
ulat
ive
Mor
talit
y, %
Follow-up, months
MERIT-HF: ↓ CV Hospitalizations
10% 10%
15% 10%
0%
5%
10%
15%
20%
25%
30%
Placebo Metoprolol CR/XL
CV Causes, Not HF Heart Failure
Metoprolol XL Placebo
MERIT-HF Study Group. The Lancet , Volume 353 , Issue 9169 , 2001 – 2007.

28
Beta Blockers: Risk of Tx
• Adverse Rxns requiring attn:
– Fluid retention
–Worsened HF
– Fatigue
–Bradycardia/Heart block
–Hypotension
Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.
• Caution w/:
–Diabetics w/ recurrent hypoglycemia
–Asthma
–Resting limb ischemia
“Because of its favorable effects on survival and disease progression, a clinical trial-proven
BB should be initiated as soon as HFrEF is diagnosed…it should not be delayed until
disease progression.”
(Do not wait for adv dz; Add when stable)
2013 Guidelines: Don’t Delay
Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.
Which is the Better Beta-Blocker?
• No good head to head trials comparing BBs
– Metoprolol succinate, bisoprolol, carvedilol
– COMET Trial: doses not comparable; metoprolol tartrate
• Consider BP lowering effect (Carvedilol>Metoprolol)
–SR/XL Metoprolol Succinate
–Bisoprolol
–Carvedilol α-1, β-1, and β-2 receptors
Colucci WS. Rationale for and clinical trials of beta blockers in heart failure due to systolic dysfunction.
In: UpToDate, Gottlieb SS, UpToDate, Waltham, MA. (Accessed on April 1, 2016.)
β-1 Selective

29
RALES: Spironolactone in Severe HF
• 1,663 pts NYHA III-IV; LVEF ≤35% on ACEI/Loop (Dig and Vasodilators OK)
• Randomized to Spironolactone 25mg or Placebo
– Titrated to 50mg over 8 wks
• Mean f/u 24 mos
• OUTCOMES:
–1°: All-Cause Mortality
–2°: CV Mortality; CV Hospitalization; Δ NYHA class
Pitt B, Zannad F, Remme W. et al “The Effect of Spironolactone on Morbidity and Mortality in Pts with Severe Heart
Failure” N Engl J Med. 1999;341(10):709-17
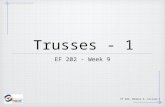
RALES: Spironolactone in Severe HF
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
% Deaths
Placebo
Spironolactone35%
n=386
46%
n=284
Pitt B, Zannad F, Remme W. et al “The Effect of Spironolactone on Morbidity and Mortality in Pts with Severe Heart
Failure” N Engl J Med. 1999;341(10):709-17
p < 0.001

30
RALES: Spironolactone in Severe HF
Pitt B, Zannad F, Remme W. et al “The Effect of Spironolactone on Morbidity and Mortality in Pts with Severe Heart
Failure” N Engl J Med. 1999;341(10):709-17
Risk of Death 30% lower with
Spironolactone vs Placebo (p*)
RALES Trial Spironolactone
(N=822)
Placebo
(N=841) p Value
CV Hospitalizations 32% 40% *
Improved NYHA Class 41% 33% *
No Δ NYHA Class 21% 18% *
Worsened NYHA Class 38% 48% *
Hyperkalemia 2% 1% NS
Gynecomastia 10% 1% *
Pitt B, Zannad F, Remme W. et al “The Effect of Spironolactone on Morbidity and Mortality in Pts with Severe Heart
Failure” N Engl J Med. 1999;341(10):709-17
RALES: Conclusion
“Blockade of aldosterone receptors by
spironolactone, in addition to standard tx,
↓ the risk of both morbidity and death
among patients with severe HF.”
N Engl J Med. 1999;341(10):709-17

31
EPHESUS: Eplerenone Post-Acute MI HF Efficacy and Survival Study
• 6,632 pts Post-MI HF pts
• Randomized to Eplerenone 25-50mg qd or Placebo x 16m
• OUTCOMES:
– All-Cause Mortality
– CV Death or Hospitalization
– Acute MI/CVA/Ventricular Arrhythmia
Pitt B, Remme W, Zannad F, et al. Eplerenone, a Selective Aldosterone Blocker, in Patients with Left
Ventricular Dysfunction after Myocardial Infarction. NEJM. 2003;348:1309-1321
EPHESUS: Eplerenone in Post MI HF
Pitt B et al NEJM 2003;348:1309-1321
Placebo
(16.7%)
Eplerenone
(14.4%)
All-
Cau
se M
ort
alit
y (%
)
Months since Randomization
Pitt B et al NEJM 2003;348:1309-1321
EPHESUS: Eplerenone in Post MI HF
Months since Randomization
CV
Dea
th o
r H
osp
ital
izat
ion
(%
)
Placebo
(30%)
Eplerenone
(27%)

32
EMPHASIS: Eplerenone in Mild Pts Hospitalization And Survival Study
• STUDY: 2,737 pts NYHA II; EF >30% on BB/ACEI
• Exclusion: NYHA III-IV, CKD, Acute MI
• Randomized to Eplerenone 25-50mg or Placebo x 21 mos
• OUTCOMES:
– Composite CV Death or 1st HF Hospitalization
– All-Cause Mortality
– HF Hospitalization
– Hyperkalemia
Zannad F et al. N Engl J Med 2011;364:11-21
EMPHASIS: Eplerenone in Mild HF
Zannad F et al. N Engl J Med 2011;364:11-21
Eplerenone
(18.3%)
Placebo
(25.9%)
EMPHASIS: Eplerenone in Mild HF
Zannad F et al. N Engl J Med 2011;364:11-21
Placebo
(15.5%)
Eplerenone
(12.5%)

33
Aldosterone Antagonist in HFrEF
“Clinicians should strongly consider the
addition of the aldosterone receptor
antagonists spironolactone or eplerenone
for all patients with HFrEF already on
ACEI (or ARBs) and BBs.” -2013 ACC/AHA Guidelines
Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.
A-HeFT: African Am Heart Failure Trial
• V-HeFT I: ISDN/H did NOT significantly reduce HF
mortality but positive trend (no ACEI)
• V-HEFT II: ISDN/H vs. ACEI showed ACEI more
beneficial, but ISDN/H more efficacious in AA cohort
• A-HeFT: ISDN/H in AA on ACE/ARB+BB+Aldosterone
Antagonist
Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.

34
A-HeFT: ISDN/Hydralazine in AA HF
• 1050 AA pts w/ NYHA III-IV on standard HF Tx
• Randomized to ISDN/H 20/37.5mg TID 40/75mg TID
or placebo
• Study ended early (18mos)
• 1° OUTCOME: Composite score of weight values for…
– All-Cause Death
– 1st HF Hosp
– HRQOL. Taylor AL, Ziesche S, Yancy C, et al “Combination of Isosorbide Dinitrate and Hydralazine in Blacks
with Heart Failure” N Engl J Med 2004;351:2049-57.
Taylor, A. et al. N Engl J Med 2004;351:2049-2057
A-HeFT Trial: Scoring System (Higher is Better)
Minnesota Living w/
HF Questionnaire
-0.6
-0.5
-0.4
-0.3
-0.2
-0.1
0
A-HeFT: 1° Outcome (*Higher is Better)
Taylor, A. et al. N Engl J Med 2004;351:2049-2057
Mea
n 1
° C
om
po
site
Sco
re
ISDN/H
-0.1±1.9
Placebo
-0.5±2.0 p = 0.01

35
A-HeFT: Overall Survival *Mortality 10.2% (placebo) vs 6.2% (ISDN/H); p = 0.02
Taylor, A. et al. N Engl J Med 2004;351:2049-2057
43% ↓ rate in
All-Cause Mortality
Ove
rall
Sur
viva
l (%
)
Days since Baseline Visit
Placebo
ISDN/H
A-HeFT: ∆ QOL Score (Lower is Better)
-6
-5
-4
-3
-2
-1
0
Placebo ISDN/H
∆ Q
OL
Sco
re
-5.6
-2.7
Taylor, A. et al. N Engl J Med 2004;351:2049-2057
P = 0.02
A-HeFT: 1st HF Hospitalization
24.4%
16.4%
Placebo ISDN/H
Taylor, A. et al. N Engl J Med 2004;351:2049-2057
p=0.001

36
A-HeFT: Adverse Events
Taylor, A. et al. N Engl J Med 2004;351:2049-2057
2013 ACCF/AHA Recommendation
“The combination of ISDN/H is recommended
for pts self-described as AA w/ NYHA III-IV
HFrEF receiving optimal tx w/ ACEI/B-blkers.”
(Level of Evidence: A)
Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.
ACCF/ACC 2013 HF Guidelines:
Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.

37
Digoxin: DIG Trial
• RCT 6800 HF pts w/ LVEF ≤45%
–988 pts EF >45% in ancillary trial ║main study
• Randomized to Digoxin or Placebo
• F/U @ 4 wks, 16wks, then q4mos
• 1° Outcome: All-Cause Mortality
• 2° Outcome: HF Hosp, CV Death, Dig Tox
The Digitalis Investigation Group. The Effect of Digoxin on Mortality and Morbidity in Patients with Heart
Failure. N Engl J Med . Feb 20,1997; 336:525-533
DIG Trial: All-Cause Mortality
The Digitalis Investigation Group. The Effect of Digoxin on Mortality and Morbidity in Patients with Heart
Failure. N Engl J Med . Feb 20,1997; 336:525-533
Digoxin (34.8%) vs. Placebo (35.1%); p=0.8
No Effect on Mortality

38
DIG Trial: Mortality Due to Worsening HF
The Digitalis Investigation Group. The Effect of Digoxin on Mortality and Morbidity in Patients with Heart
Failure. N Engl J Med . Feb 20,1997; 336:525-533
*HF Hosp: Digoxin (13.4%) vs Placebo (17.4%); RR 0.72; p<0.001
No Difference
BUT…
Digoxin in HF
• DIG Trial Conclusion: “Digoxin tx is likely to affect the freq of hosp, but not survival.”
(no significant benefit seen in HFpEF)
• 2013 ACC/ACCF Guidelines
–Digoxin can be beneficial in pts w/ HFrEF to decrease hospitalizations for HF (LOE: B)
The Digitalis Investigation Group. The Effect of Digoxin on Mortality and Morbidity in Patients with Heart
Failure. N Engl J Med . Feb 20,1997; 336:525-533

39
Ivabradine (Corlanor)
• Selective Inhibitor of the “funny channel (If)” which
modulates SA pacemaker ↓ Sinus Rate
• Does not effect atrial conduction, AV node, or ventricles
no effect on contractility
– Difference from BB and CCB
• Reduces HR by ~ 10 bpm ↓ cardiac workload
Colucci, WS. Use of beta blockers and ivabradine in heart failure with reduced ejection fraction. In:
UpToDate, Gottlieb SS (Ed), UpToDate, Waltham, MA. (Accessed on March 31, 2016).
SHIFT Trial: Systolic Heart Failure tx
with lf Inhibitor Ivabradine Trial
• RCT; 6558 pts w/ HF Sx and LVEF ≤ 35%
–HR ≥ 70bpm
–HF Admission in previous year
–On background GDMT (ACE/ARB, BB, Aldo Antagonist)
• 1° Outcome: CV Death or Hosp for worsening HF
Swedberg, Karl et al. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-
controlled study. The Lancet , Volume 376 , Issue 9744 , 875 – 885.
SHIFT: CV Death or Hosp for Worsening HF
0%
5%
10%
15%
20%
25%
Placebo Ivabradine
HF Hospitalization(p<0.0001)HF Death(p=0.014)CV Death
21%
3% 5%
Swedberg, Karl et al. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-
controlled study. The Lancet , Volume 376 , Issue 9744 , 875 – 885.
16%
29% 24%
p<0.0001

40
• Serious AES
–Increased Sx’tic Bradycardia (5% vs 1%)
–Increased Visual side effects (3% vs 1%)
• Conclusion: HR reduction w/ Ivabradine ↓HF
Mortality and Hospitalizations for pts with
persistent HF Sx, HF > 70bpm on background tx
SHIFT Trial: Ivabradine in Chronic HF
Swedberg, Karl et al. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-
controlled study. The Lancet , Volume 376 , Issue 9744 , 875 – 885.
Sacubitril-valsartan
• Sacubitril = neprilysin inhibitor
• Neprilysin inhibition ↑ vasoactive peptides
vasodilatation, natriuresis/diuresis, ↓ LV remodeling
• Indicated for NYHA II-IV HFrEF in place of ACE/ARB
• Increased risk of angioedema w/ concurrent ACEI
Colucci, WS and Pfeffer MA. Use of angiotensin II receptor blocker and neprilysin inhibitor in HF with
reduced EF. UptoDate, Gottlieb SS (Ed), UpToDate, Waltham, MA. (Accessed on April 12, 2016).

41
PARADIGM-HF: Sacubitril-valsartan in HFrEF
• 8442 HF NYHA II-IV and EF ≤ 40%
• Randomized to:
–LCZ696 (Sacubitril + Valsartan) 200mg BID
–Enalapril 10mg BID
• 27 months
• OUTCOMES:
–1° Outcome: Composite CV death or HF Hosp
–2° Outcomes: CV Death; All-Cause Death
McMurray JJV et al. N Engl J Med 2014;371:993-1004
PARADIGM-HF: 1° Outcome (CV Death or HF Hospitalization; HR 0.80, p*)
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
Enalapril LCZ696
CV Death(HR 0.80; p*)
HF Hospitalization(HR 0.79; p*)
26.5% 21.8%
*p<0.001
McMurray JJV et al. N Engl J Med 2014;371:993-1004
PARADIGM-HF: All-Cause Mortality
McMurray JJV et al. N Engl J Med 2014;371:993-1004

42
PARADIGM-HF: Adverse Events
More Hypotension
Less Hyperkalemia
Less Renal Impairment
McMurray JJV et al. N Engl J Med 2014;371:993-1004
PARADIGM-HF: Conclusion
Sacubitril-losartan was superior to
enalapril in reducing risk of death and
risk of HF hospitalization.
*No guideline recommendations
McMurray JJV et al. N Engl J Med 2014;371:993-1004

43
HF Guideline Recommendations: ICD (Implantable Cardioverter-Defibrillator)
• 1° SCD prevention in pts > 40 days Post-MI, on GDMT and expected survival > 1 yr:
–nonischemic DCM or ischemic heart disease w/ EF ≤ 35%, NYHA II-III Sx (LOE: A)
–w/ EF ≤ 30%, NYHA I Sx (LOE: B)
• Refer to cardiology when EF ≤ 35% Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.
MADIT-II: Multictr Automatic Defib Implantation Trial II
Prophylactic ICD compared w/ standard of
care led to 31% RRR in all-cause mortality
in post-MI pts w/ EF ≤ 30%
-Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with
myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877–83.
HF Guidelines: Cardiac Resynchronization Therapy (CRT)
• CRT is indicated for pts w/ EF ≤ 35%, NSR,
LBBB, QRS ≥150ms, and NYHA class II-IV
Sx on GDMT
–May consider in non-LBBB pattern, QRS
duration 120-149ms, Afib
• Refer to cardiology when EF ≤ 35% Clyde W. Yancy et al. 2013 ACCF/AHA HF Guideline. Circulation. 2013;128:1810-1852.

44
MADIT-CRT Trial
CRT-ICD decreased risk of HF event in
ASx’tic pts (NYHA I-II) w/ LVEF ≤30% and
wide QRS (≥130ms)
–1 Outcome: All-cause death or Nonfatal HF
event (ICD-CRT 17.2% vs ICD alone
25.3%; HR 0.66; p=0.001)
Moss AJ, Hall WJ, et al. Cardiac-Resynchronization Therapy for the prevention of Heart Failure
Events. N Engl J Med 2009; 361:1329-1338.
HFpEF: ACCF/ACC 2013 Guidelines
• Control BP according to guidelines to ↓ morbidity (LOE C)
• Diuretics should be used for relief of Sx due to
volume overload in patients with HFpEF. (LOE: C)
*Piller LB, Baraniuk S, Simpson LM, et al. Long-term follow-up of participants with heart failure in the Antihypertensive and Lipid-Lowering
Treatment to Prevent Heart Attack Trial (ALLHAT). Circulation. 2011;124:1811–8.
Beckett NS, Peters R, Fletcher AE, et al. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008;358:1887–98.

45
• The use of ARBs might be considered to
decrease hospitalizations (LOE B)
–CHARM-Preserved Trial
• Candesartan did NOT ↓CV death compared to
Placebo in HFpEF
• HF Hosp was lower with Candesartan
(15% vs 18% in placebo grp; HR 0.84; p=0.047)
Yusuf S, et al. Effects of candesartan in patients with chronic heart failure and preserved left-ventricular
ejection fraction: the CHARM-Preserved Trial. The Lancet , Volume 362 , Issue 9386 , 777 - 781
HFpEF: ACCF/ACC 2013 Guidelines
HFpEF Management • No evidence has demonstrated mortality benefit of
neurohormonal antagonists (BB, ACE/ARBs) or CRT
• Tx contributing factors and comorbidities:
–HTN, Pulm Dz, CAD, AF, Obesity, Anemia, DM, CKD, OSA
• Exercise training has shown to improve exercise
capacity and quality of life in HFpEF.
Borlaug BA, Colucci, WS. Treatment and prognosis of heart failure with preserved ejection
fraction. In: UpToDate, Gottlieb SS(Ed), UpToDate, Waltham, MA. (Accessed on April 2, 2016).
HF Primary Care Roadmap
HFrEF
Diuretics
Digoxin
ACE/ARB
β-Blocker Aldosterone Antagonist
Ivabradine
Sacubitril-Valsartan
Lifestyle Modification: H20/Na+ Restriction; Flu & Pneumovax;
Weight Management; Exercise/Cardiac Rehab
Disease
Modifying Rx
Symptom
Modifying Rx
ECHO / BNP HFpEF
Comorbidities: HTN, Anemia, COPD, ETOH, CAD, Arrhythmia
Cardiology
Consult AICD/CRT
ISDN/Hydralazine (African Am)