Effect of d , α-Tocopheryl Succinate and Polyethylene Glycol on...
11
JOURNAL OF NEUROTRAUMA Volume 6, November 2, 1989 Mary Ann Liebert, Inc., Publishers Effect of d, a-Tocopheryl Succinate and Polyethylene Glycol on Performance Tests After Fluid Percussion Brain Injury GUY L. CLIFTON,1 BRUCE G. LYETH,1 LARRY W. JENKINS,1 WILLIAM C. TAFT,2 ROBERT J. DeLORENZO,2 and RONALD L. HAYES1 ABSTRACT One hundred and one rats were administered either d, a-tocopheryl succinate plus polyethylene glycol (PEG), PEG, or saline 30 min prior to or 5 min after moderate fluid percussion brain injury. Mortality rates, performance on beam balance and beam-walking tasks, and body weight were assessed daily for 10 days. With preinjury administration, mortality rate was reduced from 31% with saline to 9% with PEG and 9% with d, a- tocopheryl succinate plus PEG. With postinjury administration, mortality rate was reduced from 36% with saline to 20% with PEG and to 10% with the d, a-tocopheryl succinate plus PEG combination. With administration prior to injury, PEG and d, a- tocopheryl succinate plus PEG reduced the deficits seen on beam balance testing on days 1-3 after injury. On beam walking, PEG and d, a-tocopheryl succinate plus PEG reduced deficits compared to those in saline-injected animals on days 1 and 2 and on day 1 after injury, respectively. A strongly protective effect of PEG and of d, a-tocopheryl succinate plus PEG was seen with preinjury administration. With postinjury administration, d, a- tocopheryl succinate plus PEG reduced deficits on beam balance testing compared to animals receiving both saline and PEG on days 1-3 after injury. On beam-walking latencies, i>, a-tocopheryl succinate plus PEG reduced deficits on days 1 and 2 after injury compared to saline and to PEG. Both PEG and d, a-tocopheryl succinate plus PEG reduced weight loss after injury compared to saline. The protective effects of these agents and their relatively low toxicity and high lipid solubility give them potential for the treatment of human head injury. 'Department of Surgery, Division of Neurosurgery, Richard Roland Reynolds Neurosurgical Research Laboratories, and department of Neurology, Medical College of Virginia, Virginia Commonwealth Univer- sity, Richmond, Virginia. 71
Transcript of Effect of d , α-Tocopheryl Succinate and Polyethylene Glycol on...

JOURNAL OF NEUROTRAUMAVolume 6, November 2, 1989Mary Ann Liebert, Inc., Publishers
Effect of d, a-Tocopheryl Succinate andPolyethylene Glycol on Performance Tests
After Fluid Percussion Brain Injury
GUY L. CLIFTON,1 BRUCE G. LYETH,1 LARRY W. JENKINS,1WILLIAM C. TAFT,2 ROBERT J. DeLORENZO,2 and RONALD L. HAYES1
ABSTRACT
One hundred and one rats were administered either d, a-tocopheryl succinate pluspolyethylene glycol (PEG), PEG, or saline 30 min prior to or 5 min after moderate fluidpercussion brain injury. Mortality rates, performance on beam balance and beam-walkingtasks, and body weight were assessed daily for 10 days. With preinjury administration,mortality rate was reduced from 31% with saline to 9% with PEG and 9% with d, a-
tocopheryl succinate plus PEG. With postinjury administration, mortality rate wasreduced from 36% with saline to 20% with PEG and to 10% with the d, a-tocopherylsuccinate plus PEG combination. With administration prior to injury, PEG and d, a-
tocopheryl succinate plus PEG reduced the deficits seen on beam balance testing on days1-3 after injury. On beam walking, PEG and d, a-tocopheryl succinate plus PEG reduceddeficits compared to those in saline-injected animals on days 1 and 2 and on day 1 afterinjury, respectively. A strongly protective effect of PEG and of d, a-tocopheryl succinateplus PEG was seen with preinjury administration. With postinjury administration, d, a-
tocopheryl succinate plus PEG reduced deficits on beam balance testing compared toanimals receiving both saline and PEG on days 1-3 after injury. On beam-walkinglatencies, i>, a-tocopheryl succinate plus PEG reduced deficits on days 1 and 2 afterinjury compared to saline and to PEG. Both PEG and d, a-tocopheryl succinate plusPEG reduced weight loss after injury compared to saline. The protective effects of theseagents and their relatively low toxicity and high lipid solubility give them potential forthe treatment of human head injury.
'Department of Surgery, Division of Neurosurgery, Richard Roland Reynolds Neurosurgical ResearchLaboratories, and department of Neurology, Medical College of Virginia, Virginia Commonwealth Univer-sity, Richmond, Virginia.
71

CLIFTON ET AL.
INTRODUCTION
Moderately severe human head injury, defined as patients with Glasgow Coma Score9-13 for 6h or more, is characterized clinically by transient unconsciousness with
prolonged alteration of mental status, a low incidence of hematomas, and prolonged or
permanent neuropsychological deficits (Rimel et al., 1982). These patients usually are in thegood outcome category by Glasgow Outcome Scale but may suffer permanently disablingsequelae. The fluid percussion model of brain injury in the rat, recently described by Dixon etal., (1987) has a number of parallels to moderately severe human head injury with transientunconsciousness, little anatomic brain damage, and prolonged deficits in performance testing. Assuch, it provides a useful model for testing potential therapies for the alleviation of neurologicdeficits after human head injury.
Free radical damage has been implicated in the pathophysiology of brain injury. For example,Superoxide anión radicals have been observed in the cerebral extracellular space for up to lhfollowing fluid percussion brain injury in the cat (Kontos and Wei, 1986; Kontos andPovlishock, 1986). In addition, oxygen radical scavengers (mannitol and Superoxide dismutase)have been shown to inhibit cerebral arteriolar abnormalities associated with experimental fluidpercussion brain injury (Wei et al., 1981). Studies reported here were designed to determine ifthere were protective effects of d, a-tocopheryl succinate plus PEG in a model of mechanicalbrain injury. The effects of d, a-tocopheryl succinate plus PEG and PEG vehicle on mortality,performance tests, and weight loss after fluid percussion brain injury were tested with adminis-tration both before injury and after injury.
MATERIALS AND METHODS
Production of Brain InjuryBrain injury was produced with a fluid percussion device that causes distortion of brain tissue
by rapid injection of small volume of saline epidurally into the closed cranial cavity. The fluidpercussion technique produces brief pressure transients similar to those recorded in humancadaver skulls during sudden impact (Lindgren and Rinder, 1966). Injury is associated withsuppression of behavioral and neurologic signs resembling unconsciousness in humans andreduction or abolition of cerebrovascular responsiveness to change in Pco2 and 02 (Dixon et al.,1987; DeSalles et al., 1987; Lewelt et al., 1982; Teasdale, 1976). Fluid percussion injury alsoproduces long-term behavioral deficits in the rat (Dixon et al., 1987). No evidence of ischemiahas been observed in the cat by microsphere studies or in the rat model (unpublishedobservations) at the moderate levels of injury used in these experiments (DeWitt et al., 1986).
The fluid percussion device, which has been described in greater detail previously, consists ofa Plexiglas cylindrical saline reservoir closed at one end by a Plexiglas piston mounted on O-rings (Dixon et al., 1987). The exposed end of the piston is covered with a sponge rubber pad.The opposite end of the reservoir is connected to a metal transducer housing. Injury is producedby striking the piston with a 4.8 kg steel pendulum released from a predetermined height. Theresulting pressure pulse is measured extracranially in atmospheres (atm) and recorded on a
storage oscilloscope (Tektronix 5111).All animals were surgically prepared for fluid percussion injury under sodium pentobarbital
anesthesia (54 mg/kg, IP) 24 h prior to trauma. A 4.8 mm diameter craniotomy was performedover the sagittal suture midway between lambda and bregma. Two stainless steel skull screws (54X 9.5 mm) were placed into burr holes 1 mm rostral to bregma and 1 mm caudal to lambda. Arigid plastic injury tube (modified Luer-Loc syringe hub, 2.6 mm inside diameter) was placedover the exposed dura and bonded to the skull with cyanoacrylate adhesive and dental acrylic.
72

D, a-TOCOPHERYL SUCCINATE AND POLYETHYLENE GLYCOL
Table 1. Beam-Balance Rating Scale
Score Behavior
1 Balances with steady posture; paws on top of beam2 Grasps sides of beam and/or has shaky movement3 One or more paws slip off beam4 Attempts to balance on beam but falls off5 Drapes over beam and/or hangs on beam and falls off6 Falls off beam with no attempt to balance or hang on
Animals were injured the next day within a range of 2.35-2.45 atm. Animals were observedfor the presence of apnea and signs of convulsions, and any animals that convulsed wereexcluded from the studies. As demonstrated in other studies, this injury range is associated withtransient behavioral suppression that we interpret to be analogous to the reversible state ofunconsciousness reported after human head injury. Earlier work has also shown this range ofinjury to be associated with motor deficits for up to 7 days after injury (Dixon et al., 1987).This injury range also produces acute hypertension, bradycardia, increased plasma glucose levels,and suppression of electroencephalographic (EEG) amplitude related to the magnitude of injuryin the absence of significant gross histopathologic alterations (Dixon et al., 1987).
Outcome Measures
Much like the biphasic mortality peaks after human head injury, there is a high incidence ofmortality acutely after fluid percussion brain injury (Clifton et al., 1981). In pretreated animals,both early mortality rates (< 60 min) and late mortality rates (60 min-10 days) were recordedand used as an index of efficacy. In the postinjury administration series, agents were adminis-tered after the time of occurrence of most early deaths (drug administration 5 min after injury).In this series, therefore, late deaths were used as an index of efficacy.
Persistent neurologic disturbances of balance and dizziness are common features of humanhead injury (Rimel et al., 1982). We assessed these components of gross vestibulomotor functionin the rat using a beam-balance task. This consisted of placing the animal on a suspended,narrow wooden beam (1.5 cm wide) and rating the animal's behavior for 60 sec (Table 1).Training consisted of three trials, approximately 1 h prior to trauma, which also served as
preinjury baseline measures.Persistent motor retardation and disturbances in fine motor skills are also common features of
human head injury (Rimel et al., 1982). Components of fine motor coordination in the rat were
assessed using a beam-walking task similar to that used by Feeney and co-workers (1982). Twodays prior to injury, rats were trained to escape a bright light and loud white noise by traversinga narrow wooden beam (2.5 X 100.0 cm) to enter a darkened goal box at the opposite end ofthe beam. Performance was assessed by measuring the animals' latency to traverse the beam.
Weight after injury is an overall index of animals' health. Brain-injured rats typically havereduced body weight for a 10 day period after injury. Therefore, weight was recorded daily forall animals.
Data for each of the behavioral measures were analyzed using a repeated measures analysis ofvariance (drug by time) followed by a Duncan multiple range posthoc test when appropriate.Significance levels were set at p < 0.05.
Experiment 1: Preinjury Treatment
This experiment was designed to assess the effect of preinjury administration of 100 mg/kg d,a-tocopheryl succinate (50 mg/ml) in polyethylene glycol 300 (PEG) on mortality, performance
73

CLIFTON ET AL.
Table 2. Mortality Rates by Treatment Group and Time of Administration
Saline PEG d, a-Tocopheryl succinateplus PEG
Preinjury Administration(n = 35)Early mortality 23% (3/13) 9% (1/11) 0% (0/11)Total mortality 31% (4/13) 9% (1/11) 9% (1/11)
Postinjury Administration(n = 66)Early mortality (All treatment groups) 53% (35/66)Late mortality 36% (4/11) 20% (2/10) 10% (1/10)
tests, and body weight after fluid percussion injury. Thirty-five male Sprague-Dawley rats(300-400 g) were trained on beam-walking and beam-balance tasks and surgically prepared forfluid percussion injury 24 h prior to brain injury. Animals were assigned by latin square designto one of three groups (n = 10 survivors per group): saline (2 ml/kg), PEG (2 ml/kg), and d, a-
tocopheryl succinate plus PEG (100 mg/kg). Drugs were administered intraperitoneally 30 minprior to injury. Animals were anesthetized with methoxyfluorane 5 min prior to injury.Experimenters were blind as to which drug and dosage had been administered. Animals wereassessed daily for 10 days after injury.
Experiment 2: Postinjury Treatment
This experiment was designed to assess the effect of administration of 100 mg/kg d, a-
tocopheryl succinate (50 mg/ml), in PEG 300, given 5 min after injury, on late mortality,performance tests, and body weight. Sixty-six animals were assigned by latin square design toone of three groups (« = 10 survivors per groups): saline (2 ml/kg), PEG (2 ml/kg) and d, o>
tocopheryl succinate plus PEG (100 mg/kg). Male Sprague-Dawley rats (300-400 g) were trainedand assessed using the same procedures as in experiment 1.
RESULTS
Experiment 1: Preinjury Treatment
The mortality rate within 60 min of injury (early mortality) for saline-injected animals was
23%, that of PEG-injected rats was 9%, and that of d, a-tocopheryl succinate plus PEG-injectedrats was 0%. Overall mortality rate after 10 days for saline injected animals was 31%, that ofPEG vehicle-injected rats was 9%, and that of d, a-tocopheryl succinate plus PEG-injected ratswas 9% (Table 2). Although differences in mortality rate were not statistically significant due tothe small sample size, they are consistent with the protective effect on performance tests of PEGand of D, a-tocopheryl succinate plus PEG noted below.
There were significant differences between saline and PEG and d, a-tocopheryl succinate plusPEG-injected groups (F(2,269) = 19.49 p < 0.001) on beam-balance scores. Posthoc testsindicated that the saline-treated group exhibited significant deficits compared to preinjurybaseline values for 3 days after injury. In contrast, groups treated with PEG and with d, a-
tocopheryl succinate plus PEG exhibited significant deficits for only 1 day after injury. PEG-treated and d, a-tocopheryl succinate plus PEG-treated groups exhibited significantly lessimpairment than the saline-treated group on days 1-3 after injury (Fig. 1A). The effect of d, a-
tocopheryl succinate plus PEG was not different from the effect of PEG alone.
74

D, a-TOCOPHERYL SUCCINATE AND POLYETHYLENE GLYCOL
BEAM BALANCE4.00-1
3.75-
3.50
3.25
3.00
g 2.75 How 2.50
| 2.25 H2.00-
1.75-
1.50-
1.25
1.00 J
o Salinen PEG4 d,o tocopheryl succinate
plus PEG
>-oz
<UJ5
45
40-135
30
25
20
15 -
10-
5-
0-
B BEAM WALKING
o Salineû PEGA d,a tocopheryl succinate
plus PEG
3 4 5 6
DAY POST INJURY10
*p<.05 compared to Saline
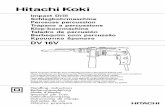
FIG. 1. A. Beam-balance scores with preinjury treatment for 30 animals. The lower the score, the betterthe performance. Values for PEG and d, a-tocopheryl succinate plus PEG are significantly lower than salineon days 1, 2, and 3. PEG was as protective as the combination of agents in this test. B. Latency of beamwalking with preinjury treatment for 30 animals. The lower the latency in seconds, the better theperformance. PEG differed from saline on days 1 and 2. d, rx-Tocopheryl succinate plus PEG differed fromsaline on day 1. PEG was as protective as the combination in this test with preinjury administration.
There were significant differences between the saline and PEG and d, a-tocopheryl succinateplus PEG-injected group (F(2,268) = 9.03, p < 0.001) on beam-walking latencies. Posthoc testsindicated that the saline-treated group exhibited significant deficits compared to preinjurybaseline values for 3 days after injury. In contrast, groups treated with d, a-tocopheryl succinateplus PEG exhibited significant deficits, compared to baseline, for only 1 day after injury, d, a-
75

CLIFTON ET AL.
Tocopheryl succinate plus PEG-treated groups exhibited significantly less impairment than thesaline-treated group on day 1 after injury (Fig. IB). PEG-treated groups exhibited significantlyless impairment than the saline-treated group on days 1 and 2 after injury. PEG exerted a
protective effect equivalent to or better than that of d, a-tocopheryl succinate plus PEG on
beam-walking latencies.There was a significant time effect of injury (F( 10,268) = 8.31, p < 0.001) on body weight.
Posthoc tests indicated that the saline-treated group exhibited significant weight loss compared topreinjury baseline values on days 2-8 after injury. The group treated with PEG exhibitedsignificant weight loss on days 3-6 after injury. The group treated with d, a-tocopheryl succinateplus PEG exhibited significant weight loss on days 4-6 after injury. Weight loss differencesbetween saline, PEG, and d, a-tocopheryl succinate plus PEG-treated groups were not significant(F(2,268) = 1.92, p > 14).
Experiment 2: Postinjury treatment
Late mortality rate (>60 min after injury) in saline-injected rats was 36%, in PEG-injected ratswas 20%, and in d, a-tocopheryl succinate plus PEG-injected rats was 10% (Table 2). Differencesin mortality rates were not statistically significant but were consistent with findings on
performance tests showing a protective effect of both PEG and the combination of d, a-
tocopheryl succinate plus PEG.There were significant differences between saline and PEG and d, a-tocopheryl succinate plus
PEG-injected animals (F2,269) = 21.23, p < 0.001) on beam balance scores. Posthoc testsindicated that the saline-treated group exhibited significant deficits compared to preinjurybaseline values for 5 days after injury. The group treated with PEG exhibited significant deficitsfor 4 days after injury, and animals treated with d, a-tocopheryl succinate plus PEG exhibitedsignificant deficits for only 2 days after injury. Animals treated with d, a-tocopheryl succinateplus PEG exhibited significantly less impairment than the saline-treated animals and lessimpairment than the PEG-treated animals on days 1-3 after injury (Fig. 2A). On beam balancescores, the effect of d, a-tocopheryl succinate plus PEG was significantly superior to PEG alone.
There were significant differences between saline and PEG and d, a-tocopheryl succinate plusPEG-injected animals (F (2,263) = 8.38, p < 0.001) on beam-walking latencies. Posthoc testsindicated that saline-treated and d, a-tocopheryl succinate plus PEG-treated groups exhibitedsignificant deficits compared to preinjury baseline values for 3 days after injury. Animals treatedwith PEG exhibited significant deficits for 7 days after injury compared to baseline values. TheD, a-tocopheryl succinate plus PEG-treated group exhibited significantly less impairment than thesaline-treated group on days 1 and 2 after injury and significantly less impairment than thePEG-treated group on day 1 after injury (Fig. 2B).
There were significant time (F) 10.2690 = 31.09, p < 0.001) and drug effects (F( 10,269) =
93.38, p < 0.001) on body weight. Posthoc tests indicated that the saline-treated group exhibitedsignificant weight loss compared to preinjury baseline values on days 1-10 after injury. Animalstreated with PEG or d, a-tocopheryl succinate plus PEG exhibited significant weight loss on days1-9 after injury (Fig. 3). Animals treated with PEG exhibited significantly less weight loss thansaline-treated rats on days 3-10 after injury. Animals treated with d, a-tocopheryl succinate plusPEG exhibited significantly less weight loss than saline-treated rats on days 5-10 after injury.Differences in weight loss between d, a-tocopheryl succinate plus PEG and PEG-treated groupswere not significant.
DISCUSSION
The fluid percussion model of brain injury in the rat provides several end points with whichto evaluate potential therapeutic interventions for treatment of human head injury: mortality
76

D, a-TOCOPHERYL SUCCINATE AND POLYETHYLENE GLYCOL
rroo
<Lu
4.5-14.2-3.93.63.3-3.0-2.7-2.4-2.1
-
1.81.51.2
BEAM BALANCE
SalinePEGd,a tocopheryl succinateplus PEG
oa>en
>-O-z.UJI-<
<LU
45
40
35
3025
20
15
10
5-
0-
B BEAM WALKING
o Salinea PEGa d,a tocopheryl succinate
plus PEG
2 4 5 7 8 9 10
DAY POST INJURY
+ p<.05 compared to PEG* p<05 compared to Saline
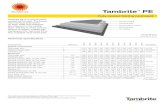
FIG. 2. A. Beam-balance scores with postinjury treatment for 30 animals, d, a-Tocopheryl succinate plusPEG produced significantly better scores than either PEG or saline on days 1, 2, or 3. There was no vehicleeffect in this test. B. Beam-walking latency with postinjury treatment for 30 animals. Score is significantlylower on day 1 for d, a-tocopheryl succinate plus PEG than PEG alone or saline. Vehicle effect was weak inthis test.
rates, performance tests, and body weight. With preinjury administration, mortality rate wasreduced from 31% with saline to 9% with PEG and 9% with d, a-tocopheryl succinate plus PEG.With postinjury administration, mortality rate was reduced from 36% with saline to 20% withPEG and 10% with the d, a-tocopheryl succinate plus PEG combination (Table 2). Withadministration prior to injury, both PEG and d, a-tocopheryl succinate plus PEG reduced thedeficits seen on beam-balance testing on days 1-3 after injury. On beam walking with preinjuryadministration, PEG and d, a-tocopheryl succinate plus PEG reduced deficits seen in saline-
77

CLIFTON ET AL.
ES\-
esLu
>-QOm
340-1330-320 -
310-
300-290-280-270-260-250-240-230-220-.
BODY WEIGHT
o Salinea PEGa d,a tocopheryl succinate
plus PEG
0 2 3 4 5 6 7 8 9110
DAY POST INJURY
* p < .05 compared to Saline
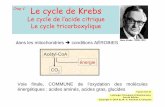
FIG. 3. Body weight with postinjury treatment for 30 animals. Both drug plus vehicle and vehicle alonediminished weight loss after injury.
injected animals on days 1 and 2 and on day 1 after injury, respectively. With preinjuryadministration the effect of PEG was equivalent to the effect of the combination. Withpostinjury administration, d, a-tocopheryl succinate plus PEG reduced deficits on beam balancetesting compared to both saline and PEG on days 1-3 after injury. On beam-walking latencies,D, a-tocopheryl succinate plus PEG reduced deficits on days 1 and 2 after injury compared tosaline and on day 1 after injury as compared to PEG. There was a weak vehicle effect. Weightloss after injury was not decreased by administration of either PEG or d, a-tocopheryl succinateplus PEG prior to injury. With postinjury administration, both PEG and d, a-tocopherylsuccinate plus PEG diminished weight loss over a 10 day period compared to saline-injectedanimals.
d, a-Tocopherol is an inhibitor of lipid peroxidation in nonneural tissue and in the centralnervous system (Halks-Miller et al., 1986; Tappel, 1962). It is presumed that the effectiveness ofd, a-tocopheryl succinate plus PEG in improving outcome following fluid percussion injury isdue to action against trauma-induced free radicals. Superoxide radicals and hydroxyl radicalsinitiate lipid peroxidation. The presence of Superoxide radical in the extracellular space and incerebral endothelium has been shown after brain injury (Kontos and Wei, 1986). Levels ofprostaglandins and phospholipase C activity, associated with free radical production, have beenfound elevated after fluid percussion brain injury (Ellis et al., 1981; Wei et al., 1982). Oraladministration of a-tocopherol and selenium has been shown to diminish abnormalities of lipidmetabolism in the injured spinal cord (Saunders et al., 1987). Hall (1985) has reported improvedoutcome in head-injured mice by pretreatment with steroids in dosages that inhibit lipidperoxidation in vitro. The extensive evidence for lipid peroxidation in models of spinal cordinjury has recently been reviewed (Hall and Braughler, 1986). In a model of compressive brainedema, Yoshida and co-workers (1983, 1985) found a direct correlation between the extent ofhemispheric swelling and plasma a-tocopherol levels, with tocopherol-deficient animals sustainingthe greatest swelling and tocopherol-supplemented animals the least.
78

D, a-TOCOPHERYL SUCCINATE AND POLYETHYLENE GLYCOL
The mechanism by which the vehicle, polyethylene glycol 300, exerts protection in this modelis unknown, but PEG has several effects. Liquid PEG has been used in combination with otherexcipients as a vehicle for many pharmaceuticals for both parenteral and topical applications.PEG has been attached to the enzymes Superoxide dismutase and catalase to reduce immunogen-icity and to extend the plasma half-life of these enzymes (Viau et al., 1986). Ethylene glycol hasbeen shown readily to cross the blood-brain barrier (Rapoport et al., 1979). PEG has beenshown to exert an anticonvulsant effect itself when given in high dosages, although not in thedosages used in this study (Lockard et al., 1979). In addition to its use as an excipient and forenzyme delivery, PEG exerts some biochemical effects and affects membrane structure in vitro.It exerts profound effects on membrane bilayers. Higher molecular weight PEGs (2000-6000) areused to induce membrane fusion (Parente and Lentz, 1986). Low concentrations (3%) of highmolecular weight polyethylene glycols (6000-8000) have been used extensively to induceguanosine triphosphate (GTP) hydrolysis through stimulation of GTPase (Nicchitta et al., 1986).
PEG offers promise as an excipient of low toxicity for highly lipid-soluble antioxidants and asa cytoprotective agent in its own right. We have shown that PEG 300 in a single dose of 2ml/kg intraperitoneally in the rat model of fluid percussion injury exerted a significant protectiveeffect. This effect was found within a range that exerts no known toxicity for a singleintraperitoneal or intravenous dose. The effective intravenous dosage is likely to be lower than 2ml/kg. An extensive literature has demonstrated low toxicity of topical and oral administrationof polyethylene glycols (Smyth et al., 1950). Intramuscular PEG 200 dosages of 1 ml/kg for 8days and single intravenous dosages of 0.5-5 ml/kg have produced no apparent toxicity in dogs(Lee and Anderson, 1962). The intravenous LD50 of PEG 300 in rats has been reported at 9ml/kg and the intraperitoneal LD50 at 21 ml/kg (Spiegel and Noseworthy, 1963). PEG has beenused experimentally as an excipient for highly lipid-soluble anticonvulsants (Korttila et al.,1976). Due to its relatively low toxicity, high lipid solubility, and the protective effectsdemonstrated here, it represents an ideal excipient for highly lipid-soluble cytoprotective agents.
This is the first study showing attenuation of behavioral deficits after brain injury by aderivative of a, tocopherol. Due to the high lipid solubility and lack of aqueous solubility of a-
tocopherol and many of its derivatives, the selection of an excipient is a key to the ability toadminister it in pharmacologie dosages. This combination of agents, therefore, may openopportunities for use of other highly lipid-soluble antioxidants in the treatment of human braininjury. Subjects for future investigation include (1) dose-response relationships of d, a-tocopherylsuccinate plus PEG and for PEG, (2) evaluation of other d, a-tocopherol derivatives for cerebralprotection, and (3) determination of whether the protective effect of both the d, a-tocopherylsuccinate-PEG combination and PEG alone exerted in this head injury model is due toinhibition of lipid peroxidation.
ACKNOWLEDGMENTS
This research was supported by Grant NS21458 to Ronald L. Hayes and by Grant 0002,Merit Review, Veterans Administration, to Guy L. Clifton.
REFERENCES
CLIFTON, G.L., MCCORMICK, W.F., and GROSSMAN, R.G. (1981). Neuropathology of early and latedeaths after head injury. Neurosurgery 8:309-314.
DESALLES, A.A.F., JENKINS, L.W., NEWLON, P.G. et al. (1987). Transient suppression of event-relatedevoked potentials in the rat produced by mild head injury. J. Neurosurg. 66:102-108.
DEWITT, D.S., JENKINS, L.W., WEIR, E.P., et al. (1986). The effects of fluid percussion brain injury onregional and total cerebral blood flow and pial vessel diameter: A combined pial window and microspherestudy. J. Neurosurg. 64:787-79.
79

CLIFTON ET AL.
DIXON, CE., LYETH, B.G., POVLISHOCK, J.T., et al. (1987). A fluid percussion model of experimentalbrain injury in the rat. J. Neurosurg. 67:110-119.
ELLIS, E.F., WRIGHT, K.F., WEI, E.P., et al. (1981). Cyclooxygenase products of arachidonic acidmetabolism in cat cerebral cortex after experimental concussive brain injury in cats. J. Neurochem.37:892-896.
FEENEY, D.M., GONZALEZ, A., and LAW, W.A. (1982). Amphetamine, haloperidol, and experienceinteract to affect rate of recovery after motor cortex injury. Science 217:855-857.
HALKS-MILLER, M„ HENDERSON, M., and ENG, L.F. (1986). Alpha tocopherol decreases lipidperoxidation, neuronal necrosis, and reactive gliosis in reaggregate cultures of fetal rat brain. J.Neuropathol. Exp. Neurol. 45:471-184.
HALL, E.D. (1985). High-dose glucocorticoid treatment improves neurological recovery in head-injuredmice. J. Neurosurg. 62:882-887.
HALL, E.D., and BRAUGHLER, J.M. (1986). Role of lipid peroxidation in post-traumatic spinal corddegeneration: A review. CNS Trauma 3:281-294.
KONTOS, H.A., and POVLISHOCK, J.T. (1986). Oxygen radicals in brain injury. CNS Trauma 3:257-263.KONTOS, H.A., and WEI, E.P. (1986). Superoxide production in experimental brain injury. J. Neurosurg.
64:803-807.
KORTTILA, K., SOTHMAN, A., and ANDERSSON, P. (1976). Polyethylene glycol as a solvent fordiazepam: Bioavailability and clinical effects after intramuscular administration, comparison of oral,intramuscular and rectal administration, and precipitation from intravenous solution. Acta Pharmacol.Toxicol. 39:104-117.
LEE, C.C., and ANDERSON, R.C. (1962). Toxicologie studies on vanomycin and polyethylene glycol 200.Toxicol. Appl. Pharmacol. 4:206-214.
LEWELT, W., JENKINS, L.W., and MILLER, J.D. (1982). Effects of experimental fluid-percussion injuryof the brain on cerebrovascular reactivity to hypoxia and to hypercapnia. J. Neurosurg. 56:332-338.
LINDGREN, S., and RINDER, L. (1966). Experimental studies on head injury. II. Pressure propagation inpercussion-concussion. Biophysik 3:174-180.
LOCKARD, J.S., LEVY, R.H., CONGDON, W.C., et al. (1979). Efficacy and toxicity of the solventpolyethylene glycol 400 in monkey model. Epilepsia 20:77-84.
NICCHITTA, C.V., JOSEPH, S.K., and WILLIAMSON, J.R. (1986). Polyethylene glycol-stimulated micro-somal GTP hydrolysis. FEBS Letts. 209:243-248.
PARENTE, R.A., and LENTZ, B.R. (1986). Rate and extent of polyethylene glycol-induced large vesiclefusion monitored by bilayer and intrnal contents mixing. Biochemistry 25:6678-6688.
RAPOPORT, S.I., OHNO, K., and PETTIGREW, K.O. (1979). Drug entry into the brain. Brain Res.172:354-359.
RIMEL, R.W., GIORDANI, B., BARTH, J.T., et al. (1982). Moderate head injury: Completing the clinicalspectrum of brain trauma. Neurosurgery 11:344-351.
SAUNDERS, R.D., DUGAN, L.L., DEMEDIUK, P. et al. (1987). Effects of methylprednisolone and thecombination of a-tocopherol and selenium on arachidonic acid metabolism and lipid peroxidation intraumatized spinal cord tissue. J. Neurochem. 49:24-31.
SMYTH, H.F., JR., CARPENTER, C.P., and WEIL, C.S. (1950). The toxicology of the polyethylene glycols.J. Am. Pharm. Assoc. 35:349-354.
SPIEGEL, A.J., and NOSEWORTHY, M.M. (1963). Use of non-aqueous solvents in parenteral products. J.Pharm. Sei. 52:917-927.
TAPPEL, A.L. (1962). Vitamin E as the biological lipid antioxidant. Vitamins Hormones 20:493-510.
TEASDALE, G. (1976). Assessment of head injury. Br. J. Anaesth. 49:761-766.
VIAU, A.T., ABUCHOWSKI, A., GREENSPAN, S., et al (1986). Safety evaluation of free radicalscavengers PEG-catalase and PEG-superoxide dismutase. J. Free Radicals Biol. Med. 2:283-288.
80

D, a-TOCOPHERYL SUCCINATE AND POLYETHYLENE GLYCOL
WEI, E.P., KONTOS, H.A., DIETRICH, W.D., et al. (1981). Inhibition by free radical scavengers and bycyclooxygenase inhibitors of pial abnoramlities from concussive brain injury in cats. Circ. Res. 48:95-103.
WEI, E.P., LAMB, R.G., and KONTOS, H.A. (1982). Increased phospholipase C activity after experimentalbrain injury. J. Neurosurg. 56: 695-698.
YOSHIDA, S., BUSTO, R., GINSBERG, M.D., et al. (1983). Compression-induced brain edema: Modifica-tion by prior depletion and supplementation of vitamin E. Neurology 33:166-712.
YOSHIDA, S., BUSTON, R., ABE, K. et al. (1985). Compression-induced brain edema in rats: Effect ofdietary vitamin E on membrane damage in the brain. Neurology 35:126-130.
Address reprint requests to:Guy L. Clifton, M.D.
Division of NeurosurgeryMedical College of Virginia
Box 433 MCV StationRichmond, VA 23298-0433
81