Early Motor Differences Between Infants at High Risk and Low … · 2020. 7. 23. · Maggie E....
1
Sensor-Based Motor Variables Figure 3. Infant wearing a sensor and legwarmer on each ankle. Opal sensor next to a U.S. quarter for scale. Variable β Coef. p-value 95% Confidence Interval Average acceleration, 3 mo -.032386 0.818 [-.3191406, .2543685] Average acceleration, 6 mo -.314417 0.015* [-.5623492, -.0664849] Peak acceleration, 3 mo -.0303809 0.913 [-.5976323, .5368705] Peak acceleration, 6 mo -.6787982 0.019* [-1.237383, -.1202133] Movement rate average, 3 mo -271.5559 0.220 [-716.9131, 173.8012] Movement rate average, 6 mo -326.18 0.099 [-719.0149, 66.65494] At 3 months of age, HR infants demonstrated lower average leg movement rate, average acceleration, and peak acceleration, but the differences were not significant. At 6 months, the differences in average and peak acceleration became significant. Alberta Infant Motor Scale (AIMS) AIMS percentile ranking, prone subscale, and supine subscale scores at 3 and 6 months of age. LR infants were more competent with motor skills overall. HR infants had greater difficulty in prone positions, but performed similarly or better in supine compared to LR infants, but these differences were not significant. Figure 2. Infants demonstrating motor skills expected at 3 and 6 months of age during AIMS assessments. Future Directions Study Design & Methods Discussion References Objectives Background Early Motor Differences Between Infants at High Risk and Low Risk for Autism Spectrum Disorder Maggie E. Tsang, Tabitha Safari, Sebiha M. Abdullahi, Rujuta B. Wilson, MD David Geffen School of Medicine at the University of California, Los Angeles 1. Bhat AN, et al. Relationship between early motor delay and later communication delay in infants at risk for autism. Infant Behav Dev. 2012; 35(4):838-846. 2. West KL. Infant Motor Development in Autism Spectrum Disorder: A Synthesis and Meta-analysis. Child Dev. 2019;90(6);2053-2070. 3. Flanagan JE, et al. Head lag in infants at risk for autism: A preliminary study. Am J Occup Ther. 2012;66(5):577-585. 4. Iverson JM, et al. Early Motor Abilities in Infants at Heightened Versus Low Risk for ASD: A Baby Siblings Research Consortium (BSRC) Study. J Abnormal Psych. 2019;128(1):69-80. 5. Piper M, Darrah J. Motor Assessment of the Developing Infant. Philadelphia, PA: Saunders Publishing; 1994. 6. Wilson RB, et al. What's missing in autism spectrum disorder motor assessments?. J Neurodev Disord. 2018;10(1):33. 7. Abrishami MS, et al. Identification of Developmental Delay in Infants Using Wearable Sensors: Full- Day Leg Movement Statistical Feature Analysis. IEEE J Transl Eng Health Med. 2019;7:2800207. 8. Smith BA, et al. Sample Entropy Identifies Differences in Spontaneous Leg Movement Behavior between Infants with Typical Development and Infants at Risk of Developmental Delay. Technologies (Basel). 2017;5(3):55. 9. Smith BA, et al. Daily Quantity of Infant Leg Movement: Wearable Sensor Algorithm and Relationship to Walking Onset. Sensors (Basel). 2015;15(8):19006-19020. 10. Reindal L, et al. Age of First Walking and Associations with Symptom Severity in Children with Suspected or Diagnosed Autism Spectrum Disorder. J Autism Dev Disord (2019). 11. Gabis LV, et al. Variability of Coordination in Typically Developing Children Versus Children with Autism Spectrum Disorder with and without Rhythmic Signal. Sensors (Basel). 2020;20(10):2769. 1. Examine differences in motor skills and developmental milestones between high risk (HR) and low risk (LR) infants via a standardized motor assessment. 2. Compare characteristics of movement between HR and LR infants by utilizing quantitative sensor-based metrics such as leg movement rate and average and peak acceleration. • Autism spectrum disorder (ASD) is associated with delays in motor development, which can detrimentally impact social and cognitive development. • Motor differences such as hypotonia and delayed motor milestones present early in infants at high risk for ASD and can be leveraged for early risk identification and be an avenue for intervention to improve outcomes. • Standardized assessments evaluate developmental milestones and motor skills, but may not capture subtle differences that could be present before motor differences are clinically observable. • Quantitative wearable sensors could aid in identifying subtle motor differences by measuring features of early infant motor skills such as spontaneous leg movements. These data are from an ongoing prospective study of infant motor development and association with risk for ASD. Participants: 14 HR infants (have older sibling with ASD) and 11 LR infants (have older sibling w/o ASD, no family history of ASD) Alberta Infant Motor Scale (AIMS): 58-item standardized, norm- referenced, observational assessment of infant motor skills in prone, supine, sitting, and standing positions. Sensor Data: Opal sensor worn on each ankle for 8-12 hr during the day in home environment. Derived variables include leg movement rate per hour awake time, average acceleration, peak acceleration. Analysis: Linear regression accounting for age to compare total AIMS scores and sensor variables between HR and LR infants. Figure 1. Study design. Std Motor = standardized motor assessments. SBMV = sensor-based motor variables. • Assess motor differences in later infancy and developmental trajectories across the first year of life. • Incorporate additional sensor measures such as movement magnitude and variability. • Examine relationships between AIMS scores and sensor-based metrics. • Evaluate associations of early motor impairments with ASD symptoms, language, cognition, and social communication at 12 and 24 months of age. • Motor differences between HR and LR infants are present at 3 months of age, but significant differences do not emerge until 6 months of age. • Sensor-based motor variables were able to detect significant differences between groups compared to standardized observational assessments. • HR infants were less skilled in prone positions, perhaps due to difficulty generating adequate leg movements or acceleration to transition to prone. • Differences may become more apparent with age as infants acquire more complex motor skills, and early impairments may constrain development. * *
Transcript of Early Motor Differences Between Infants at High Risk and Low … · 2020. 7. 23. · Maggie E....

Sensor-Based Motor Variables
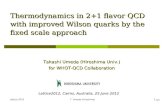
Figure 3. Infant wearing a sensor and legwarmer on each ankle. Opal sensor next to a U.S. quarter for scale.
Variable β Coef. p-value 95% Confidence IntervalAverage acceleration, 3 mo -.032386 0.818 [-.3191406, .2543685]Average acceleration, 6 mo -.314417 0.015* [-.5623492, -.0664849]
Peak acceleration, 3 mo -.0303809 0.913 [-.5976323, .5368705]Peak acceleration, 6 mo -.6787982 0.019* [-1.237383, -.1202133]
Movement rate average, 3 mo -271.5559 0.220 [-716.9131, 173.8012]Movement rate average, 6 mo -326.18 0.099 [-719.0149, 66.65494]
At 3 months of age, HR infants demonstrated lower average leg movement rate, average acceleration, and peak acceleration, but the differences were not significant. At 6 months, the differences in average and peak acceleration became significant.
Alberta Infant Motor Scale (AIMS)
AIMS percentile ranking, prone subscale, and supine subscale scores at 3 and 6 months of age. LR infants were more competent with motor skills overall. HR infants had greater difficulty in prone positions, but performed similarly or better in supine compared to LR infants, but these differences were not significant.
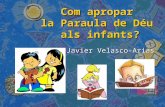
Figure 2.Infants demonstrating motor skills expected at 3 and 6 months of age during AIMS assessments.
Future Directions
Study Design & Methods
Discussion
References
Objectives
Background
Early Motor Differences Between Infants at High Risk and Low Risk for Autism Spectrum Disorder
Maggie E. Tsang, Tabitha Safari, Sebiha M. Abdullahi, Rujuta B. Wilson, MDDavid Geffen School of Medicine at the University of California, Los Angeles
1. Bhat AN, et al. Relationship between early motor delay and later communication delay in infants at risk for autism. Infant Behav Dev. 2012; 35(4):838-846.
2. West KL. Infant Motor Development in Autism Spectrum Disorder: A Synthesis and Meta-analysis. Child Dev. 2019;90(6);2053-2070.
3. Flanagan JE, et al. Head lag in infants at risk for autism: A preliminary study. Am J Occup Ther.2012;66(5):577-585.
4. Iverson JM, et al. Early Motor Abilities in Infants at Heightened Versus Low Risk for ASD: A Baby Siblings Research Consortium (BSRC) Study. J Abnormal Psych. 2019;128(1):69-80.
5. Piper M, Darrah J. Motor Assessment of the Developing Infant. Philadelphia, PA: Saunders Publishing; 1994.
6. Wilson RB, et al. What's missing in autism spectrum disorder motor assessments?. J Neurodev Disord. 2018;10(1):33.
7. Abrishami MS, et al. Identification of Developmental Delay in Infants Using Wearable Sensors: Full-Day Leg Movement Statistical Feature Analysis. IEEE J Transl Eng Health Med. 2019;7:2800207.
8. Smith BA, et al. Sample Entropy Identifies Differences in Spontaneous Leg Movement Behavior between Infants with Typical Development and Infants at Risk of Developmental Delay. Technologies (Basel). 2017;5(3):55.
9. Smith BA, et al. Daily Quantity of Infant Leg Movement: Wearable Sensor Algorithm and Relationship to Walking Onset. Sensors (Basel). 2015;15(8):19006-19020.
10. Reindal L, et al. Age of First Walking and Associations with Symptom Severity in Children with Suspected or Diagnosed Autism Spectrum Disorder. J Autism Dev Disord (2019).
11. Gabis LV, et al. Variability of Coordination in Typically Developing Children Versus Children with Autism Spectrum Disorder with and without Rhythmic Signal. Sensors (Basel). 2020;20(10):2769.
1. Examine differences in motor skills and developmental milestones between high risk (HR) and low risk (LR) infants via a standardized motor assessment.
2. Compare characteristics of movement between HR and LR infants by utilizing quantitative sensor-based metrics such as leg movement rate and average and peak acceleration.
• Autism spectrum disorder (ASD) is associated with delays in motor development, which can detrimentally impact social and cognitive development.
• Motor differences such as hypotonia and delayed motor milestones present early in infants at high risk for ASD and can be leveraged for early risk identification and be an avenue for intervention to improve outcomes.
• Standardized assessments evaluate developmental milestones and motor skills, but may not capture subtle differences that could be present before motor differences are clinically observable.
• Quantitative wearable sensors could aid in identifying subtle motor differences by measuring features of early infant motor skills such as spontaneous leg movements.
These data are from an ongoing prospective study of infant motor development and association with risk for ASD.
Participants: 14 HR infants (have older sibling with ASD) and 11 LR infants (have older sibling w/o ASD, no family history of ASD)
Alberta Infant Motor Scale (AIMS): 58-item standardized, norm-referenced, observational assessment of infant motor skills in prone, supine, sitting, and standing positions.
Sensor Data: Opal sensor worn on each ankle for 8-12 hr during the day in home environment. Derived variables include leg movement rate per hour awake time, average acceleration, peak acceleration.
Analysis: Linear regression accounting for age to compare total AIMS scores and sensor variables between HR and LR infants.
Figure 1. Study design. Std Motor = standardized motor assessments. SBMV = sensor-based motor variables.
• Assess motor differences in later infancy and developmental trajectories across the first year of life.
• Incorporate additional sensor measures such as movement magnitude and variability.
• Examine relationships between AIMS scores and sensor-based metrics.
• Evaluate associations of early motor impairments with ASD symptoms, language, cognition, and social communication at 12 and 24 months of age.
• Motor differences between HR and LR infants are present at 3 months of age, but significant differences do not emerge until 6 months of age.
• Sensor-based motor variables were able to detect significant differences between groups compared to standardized observational assessments.
• HR infants were less skilled in prone positions, perhaps due to difficulty generating adequate leg movements or acceleration to transition to prone.
• Differences may become more apparent with age as infants acquire more complex motor skills, and early impairments may constrain development.
*
*




![GENIE September 1, 2016...Lattice Gauge Theory K. Wilson, PRD 10 (1974) 2445 • Invented to understand asymptotic freedom without the need for gauge-fixing and ghosts [Wilson, hep-lat/0412043].](https://static.fdocument.org/doc/165x107/6141ec072035ff3bc76256cf/genie-september-1-2016-lattice-gauge-theory-k-wilson-prd-10-1974-2445-a.jpg)