Each Degree of Glucose Intolerance in Pregnancy Predicts Distinct Trajectories of β-Cell Function,...
8
Each Degree of Glucose Intolerance in Pregnancy Predicts Distinct Trajectories of b-Cell Function, Insulin Sensitivity, and Glycemia in the First 3 Years Postpartum Diabetes Care 2014;37:3262–3269 | DOI: 10.2337/dc14-1529 OBJECTIVE Glucose intolerance in pregnancy predicts an increased risk of future type 2 di- abetes mellitus (T2DM) that is proportional to the severity of antepartum dysgly- cemia (i.e., highest in women with gestational diabetes mellitus [GDM], followed by those with milder dysglycemia). However, the pathophysiologic changes driv- ing this risk are not known. Thus, we evaluated the longitudinal changes in b-cell function, insulin sensitivity, and glycemia in the first 3 years postpartum after gestational dysglycemia. RESEARCH DESIGN AND METHODS A total of 337 women underwent glucose challenge test (GCT) and oral glucose tolerance test (OGTT) in pregnancy, followed by repeat OGTT at 3 months, 1 year, and 3 years postpartum. The antepartum GCT/OGTT identified four gestational glucose tolerance groups: GDM (n = 105); gestational impaired glucose tolerance (GIGT; n = 60); abnormal GCT, followed by normal glucose tolerance (NGT) on the OGTT (abnormal GCT NGT; n = 96); and normal GCT with NGT (n = 76). RESULTS At each of 3 months, 1 year, and 3 years postpartum, the prevalence of glucose intolerance increased from normal GCT NGT to abnormal GCT NGT to GIGT to GDM (all P < 0.001), whereas b-cell function, assessed by the Insulin Secretion- Sensitivity Index-2 (ISSI-2), and insulin sensitivity (Matsuda index), progressively decreased across the groups (all P < 0.002). Each group predicted distinct trajec- tories of ISSI-2, Matsuda index, and fasting and 2-h glucose (all P < 0.001). Notably, GDM, GIGT, and abnormal GCT NGT predicted varying rates of declining b-cell function and insulin sensitivity, as well as rising glycemia, compared with normal GCT NGT. CONCLUSIONS Each degree of gestational glucose intolerance predicts distinct trajectories of b-cell function, insulin sensitivity, and glycemia in the first 3 years postpartum that drive their differential risk of future T2DM. 1 Leadership Sinai Centre for Diabetes, Mount Sinai Hospital, Toronto, Ontario, Canada 2 Division of Endocrinology, University of Toronto, Toronto, Ontario, Canada 3 Department of Nutritional Sciences, University of Toronto, Toronto, Ontario, Canada 4 Keenan Research Centre for Biomedical Science of St. Michael’s Hospital, Toronto, Ontario, Canada 5 Department of Laboratory Medicine and Patho- biology, University of Toronto, Toronto, Ontario, Canada 6 Division of Obstetrics and Gynecology, Univer- sity of Toronto, Toronto, Ontario, Canada 7 Lunenfeld-Tanenbaum Research Institute, Mount Sinai Hospital, Toronto, Ontario, Canada Corresponding author: Ravi Retnakaran, [email protected]. Received 23 June 2014 and accepted 25 August 2014. © 2014 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered. Caroline K. Kramer, 1,2 Balakumar Swaminathan, 1 Anthony J. Hanley, 1,2,3 Philip W. Connelly, 2,4,5 Mathew Sermer, 6 Bernard Zinman, 1,2,7 and Ravi Retnakaran 1,2,7 3262 Diabetes Care Volume 37, December 2014 PATHOPHYSIOLOGY/COMPLICATIONS
Transcript of Each Degree of Glucose Intolerance in Pregnancy Predicts Distinct Trajectories of β-Cell Function,...

Each Degree of GlucoseIntolerance in Pregnancy PredictsDistinct Trajectories of b-CellFunction, Insulin Sensitivity,and Glycemia in the First 3 YearsPostpartumDiabetes Care 2014;37:3262–3269 | DOI: 10.2337/dc14-1529
OBJECTIVE
Glucose intolerance in pregnancy predicts an increased risk of future type 2 di-abetes mellitus (T2DM) that is proportional to the severity of antepartum dysgly-cemia (i.e., highest in women with gestational diabetes mellitus [GDM], followedby those with milder dysglycemia). However, the pathophysiologic changes driv-ing this risk are not known. Thus, we evaluated the longitudinal changes in b-cellfunction, insulin sensitivity, and glycemia in the first 3 years postpartum aftergestational dysglycemia.
RESEARCH DESIGN AND METHODS
A total of 337 women underwent glucose challenge test (GCT) and oral glucosetolerance test (OGTT) in pregnancy, followed by repeat OGTT at 3 months, 1 year,and 3 years postpartum. The antepartum GCT/OGTT identified four gestationalglucose tolerance groups: GDM (n = 105); gestational impaired glucose tolerance(GIGT; n = 60); abnormal GCT, followed by normal glucose tolerance (NGT) on theOGTT (abnormal GCT NGT; n = 96); and normal GCT with NGT (n = 76).
RESULTS
At each of 3 months, 1 year, and 3 years postpartum, the prevalence of glucoseintolerance increased from normal GCT NGT to abnormal GCT NGT to GIGT toGDM (all P < 0.001), whereas b-cell function, assessed by the Insulin Secretion-Sensitivity Index-2 (ISSI-2), and insulin sensitivity (Matsuda index), progressivelydecreased across the groups (all P < 0.002). Each group predicted distinct trajec-tories of ISSI-2,Matsuda index, and fasting and 2-h glucose (all P < 0.001). Notably,GDM, GIGT, and abnormal GCT NGT predicted varying rates of declining b-cellfunction and insulin sensitivity, as well as rising glycemia, compared with normalGCT NGT.
CONCLUSIONS
Each degree of gestational glucose intolerance predicts distinct trajectories ofb-cell function, insulin sensitivity, and glycemia in the first 3 years postpartumthat drive their differential risk of future T2DM.
1Leadership Sinai Centre for Diabetes, MountSinai Hospital, Toronto, Ontario, Canada2Division of Endocrinology, University of Toronto,Toronto, Ontario, Canada3Department of Nutritional Sciences, Universityof Toronto, Toronto, Ontario, Canada4KeenanResearch Centre forBiomedical Science ofSt. Michael’s Hospital, Toronto, Ontario, Canada5Department of LaboratoryMedicine and Patho-biology, University of Toronto, Toronto, Ontario,Canada6Division of Obstetrics and Gynecology, Univer-sity of Toronto, Toronto, Ontario, Canada7Lunenfeld-Tanenbaum Research Institute,Mount Sinai Hospital, Toronto, Ontario, Canada
Corresponding author: Ravi Retnakaran,[email protected].
Received 23 June 2014 and accepted 25 August2014.
© 2014 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered.
Caroline K. Kramer,1,2
Balakumar Swaminathan,1
Anthony J. Hanley,1,2,3
Philip W. Connelly,2,4,5 Mathew Sermer,6
Bernard Zinman,1,2,7
and Ravi Retnakaran1,2,7
3262 Diabetes Care Volume 37, December 2014
PATH
OPHYS
IOLO
GY/COMPLICATIONS

It is well established that women whoare diagnosed with gestational diabetesmellitus (GDM) have an increased risk ofdeveloping type 2 diabetes mellitus(T2DM) in the years after the index preg-nancy (1–7). Furthermore, it is now rec-ognized that even women with milderdegrees of glucose intolerance in preg-nancy (i.e., less severe than GDM) havean increased risk of ultimately develop-ing prediabetes and T2DM in the future(6,8–15). These diagnoses of mild gesta-tional dysglycemia can be identified dur-ing clinical screening for GDM andinclude 1) women with an abnormal an-tepartum oral glucose tolerance test(OGTT) that does not meet diagnosticcriteria for GDM, and 2) those with anormal OGTT but an abnormal screeningglucose challenge test (GCT) (8,9,12,14).Importantly, the risk of postpartum pro-gression to prediabetes/T2DM is pro-portional to the severity of gestationaldysglycemia, being highest in womenwith GDM and proportionately lowerin those with milder abnormalities ofantepartum glucose tolerance (8).Thus, the spectrum of abnormal glucosehomeostasis in pregnancy identifies agradient of future diabetic risk in theyears thereafter. To date, however, lon-gitudinal study of the pathophysiologicchanges that drive this gradient of riskin the early postpartum years has beenlimited. Therefore, our objective in thisstudy was to elucidate the trajectories ofb-cell function, insulin sensitivity, andglycemia during the first 3 years post-partum in a well-characterized cohortofwomen representing the full spectrumof glucose tolerance in pregnancy.
RESEARCH DESIGN AND METHODS
ParticipantsThe study population consisted ofwomen participating in a prospective ob-servational cohort program at our insti-tution in which we are studying therelationship between glucose tolerancestatus in pregnancy and metabolic func-tion in the years after delivery (9,16,17).In this program, women are first re-cruited into a pregnancy cohort at thetime of antepartum screening for GDMin late second/early third trimester andundergo metabolic characterization atrecruitment in pregnancy and again at3 months and 1 year postpartum. At thelatter visit, they are recruited into an on-going long-term follow-up observational
cohort study in which participatingwomen undergo serial metabolic charac-terization biannually for several yearsthereafter. The current analysis reportsthe metabolic trajectories of 337 partic-ipants from recruitment in pregnancy totheir first assessment in the long-termcohort at 3 years postpartum. The pro-tocols of the pregnancy cohort and thelong-term cohort study were approvedby the Mount Sinai Hospital ResearchEthics Board, and all women providedwritten informed consent for theirparticipation.
Recruitment and Determinationof Glucose Tolerance Statusin PregnancyAs previously described (9,16,17), womenwere first recruited in late second/earlythird trimester at the time of antepartumscreening for GDM. At our institution,women are screened for GDM by a 50-gGCT, followed by referral for diagnosticOGTT if the GCT result is abnormal(plasma glucose$7.8 mmol/L at 1 h afteringestion of 50-g glucose load). In thestudy, all participants undergo a 3-h 100-gOGTT for ascertainment of gestationalglucose tolerance status, regardless ofthe GCT result (i.e., even if the result isnormal). Women were recruited beforeor after the GCT. As previously described(9,17), the recruitment ofwomen after anabnormal GCT served to enrich the studypopulation for thosewith varying degreesof glucose intolerance. The GCT and 3-h100-g OGTT in pregnancy enabled stratifi-cation of participants into the followingfour gestational glucose tolerance groups:
1. GDM, as defined by National Diabe-tes Data Group (NDDG) criteria (18),which require at least two of thefollowing on the OGTT: fastingblood glucose $5.8 mmol/L, 1-hglucose $10.6 mmol/L, 2-h bloodglucose $9.2 mmol/L, or 3-h bloodglucose $ 8.1 mmol/L;
2. Gestational impaired glucose toler-ance (GIGT), as defined by meetingonly one of the above NDDG criteria;
3. Abnormal GCT with normal glucosetolerance (NGT), as defined by havingan abnormal 50-g GCT, followed byNGT on the OGTT (defined by meet-ing none of the NDDG criteria); and
4. Normal GCT NGT, as defined byhaving a normal 50-g GCT, followedby NGT on the OGTT.
Women with GDM received glucose-lowering treatment in pregnancy, con-sisting of dietary and lifestyle counseling(pertaining to pregnancy and postpar-tum) with orwithout antepartum insulintherapy. According to standard clinicalpractice at our institution, women inthe other three glucose tolerancegroups did not receive this glucose-lowering therapy. Baseline data re-garding medical, obstetrical, and familyhistory were collected by an interviewer-administered questionnaire on themorn-ing of the OGTT (at which time gestationalglucose tolerance had not yet beendetermined).
Postpartum Assessments at 3 Months,1 Year, and 3 YearsAt 3 months, 1 year, and 3 years post-partum, participants returned to theclinical investigation unit for reassess-ment, including a 2-h 75-g OGTT oneach occasion. Glucose tolerance statuswas defined on each OGTT according tocurrent Canadian Diabetes Associationguidelines (19). Dysglycemia refers toprediabetes (impaired glucose toler-ance [IGT], impaired fasting glucose[IFG], or combined IFG and IGT) ordiabetes.
At each visit, participants underwentphysical examination, including anthro-pometric assessment and measure-ment of blood pressure. Data regardingmedical, obstetrical, and family historywere collected through an interviewer-administered questionnaire. At 1 yearand 3 years postpartum, physical activityin the preceding year was assessed withthe Baecke questionnaire, an establishedinstrument that has been extensively val-idated in several populations, includingwomen of childbearing age (20,21). Thisquestionnaire was completed during theOGTT (i.e., before the current glucose tol-erance status was known). The Baeckequestionnaire measures total physical ac-tivity and its three component domains:occupation-associated activity (work in-dex), sport-related physical activity (sportindex), and nonsport leisure-time activity(leisure-time index). The work indexquantifies exertion related to occupa-tional activities, such as sitting, stand-ing, lifting, and walking, as well asassociated effects on the person (e.g.,fatigue, perspiration). The sport indexcharacterizes vigorous/sports activitywith respect to intensity (using the
care.diabetesjournals.org Kramer and Associates 3263

updated compendium of physical ac-tivities) (22), duration, and frequency.The leisure-time index quantifies ex-ertion associated with nonsport recrea-tional activities (e.g., walking, watchingtelevision).
Laboratory Measurements andPhysiologic IndicesAll OGTTs were performed in the morn-ing after an overnight fast, with venousblood samples drawn for the measure-ment of glucose and specific insulin lev-els at fasting and at 30, 60, and 120 min(and 180 min in pregnancy) after the in-gestion of the glucose load. Specific in-sulin was measured with the RocheElecsys 1010 immunoassay analyzerand electrochemiluminescence immu-noassay kit (Roche Diagnostics, Laval,Quebec, Canada).Insulin sensitivity was measured on
each OGTT with the Matsuda index, anestablished measure of whole-body in-sulin sensitivity that has been validatedagainst the euglycemic-hyperinsulinemicclamp (23). b-Cell function was assessedon each OGTT with the Insulin Secretion-Sensitivity Index-2 (ISSI-2), a validatedmeasure of b-cell function that is analo-gous to the disposition index obtainedfrom the intravenous GTT (IVGTT)(24,25). The ISSI-2 has been directly val-idated against the disposition index fromthe IVGTT, with which it exhibits stron-ger correlation than do other OGTT-derived measures of b-cell function,including the insulinogenic index–basedmeasures and HOMA b-cell (HOMA-B)function, (25) and has been used in clin-ical trials and observational studies inpatients with and without diabetes(17,26–30). ISSI-2 is defined as the prod-uct of 1) insulin secretion measured bythe ratio of the area-under-the-insulincurve to the area-under-the-glucosecurve and 2) insulin sensitivity measuredby Matsuda index (24,25).
Statistical AnalysesAll analyses were conducted using SAS9.1 software (SAS Institute, Inc., Cary, NC).Continuous variables were tested fornormality of distribution, and naturallog transformations of skewed variableswere used, where necessary, in subse-quent analyses. Univariate differencesacross the four gestational glucose toler-ance groups were assessed at recruit-ment in pregnancy and at 3 months, 1year, and 3 years postpartum using the
Wilcoxon rank sum test for continuousvariables and the x2 test or Fisher exacttest for categorical variables (Table 1). Ateach of 3 months, 1 year, and 3 yearspostpartum, the prevalence of dysglyce-mia was compared among the gesta-tional glucose tolerance groups by thex2 test (Fig. 1). Mixed-models were con-structed to evaluate the trajectories offasting glucose, 2-h glucose, Matsuda in-dex, and ISSI-2 in each group during thepostpartum follow-up (from 3months to3 years; Table 2). Covariates in thesemod-els were model 1: age, ethnicity, familyhistory of diabetes, time-dependentBMI, and months postpartum; model 2:model 1 + duration of breastfeeding inthe first year postpartum + total physicalactivity at 1 year and 3 years; and model3: model 2 + development of diabetesat 3 months or 1 year (i.e., a diagnosisthat might cause subsequent lifestylechanges).
RESULTS
Comparison of Gestational GlucoseTolerance GroupsA comparison of the 337 women com-prising the study population with the103 women who declined to participateshowed no significant differences be-tween the two groups in age, ethnicity,family history of diabetes, glucose toler-ance, smoking, and physical activity at 1year, although the womenwho declinedhad slightly lower BMI than the partici-pants (median 23.8 vs 24.7 kg/m2, P =0.01). Table 1 reports the characteristicsof the study population at recruitmentin pregnancy and at follow-up at 3months, 1 year, and 3 years postpartum,stratified into the following four groupsbased on gestational glucose tolerancestatus: normal GCT NGT (n = 76), abnor-mal GCT NGT (n = 96), GIGT (n = 60), andGDM (n = 105). At recruitment, thesegroups did not differ in age, ethnicity,family history of diabetes, or parity. Pre-pregnancy BMI was highest in the GDMgroup (P = 0.04). As expected, insulinsensitivity (Matsuda index) and b-cellfunction (ISSI-2) in pregnancy both pro-gressively decreased across the four cat-egories of gestational glucose tolerancefrom normal GCT NGT to abnormal GCTNGT to GIGT to GDM (both P , 0.001).Furthermore, these differences in insu-lin sensitivity and b-cell function per-sisted at each postpartum visit (3months, 1 year, and 3 years; all P #
0.002). Of note, BMI, waist circumfer-ence, and physical activity did not differamong the groups at these postpartumassessments (all P $ 0.08).
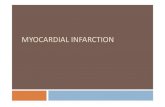
The persistent postpartum differ-ences in insulin sensitivity and b-cellfunction were further reflected in theprevalence of dysglycemia (prediabetesor diabetes) in the four groups. Indeed,at each of 3 months, 1 year, and 3 yearspostpartum, a stepwise increase wasfound in the prevalence of dysglycemiafrom the normal GCT NGT group to ab-normal GCT NGT toGIGT to GDM (all P,0.001; Fig. 1), with rates of 30–38% inwomen with GDM. Most of the dysgly-cemia was prediabetes, with diabetescomprising 10.6% of the dysglycemiaat 3 months, 5.4% at 1 year, and 13.0%at 3 years.
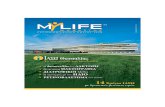
Postpartum Trajectoriesof Glycemia, Insulin Sensitivity,and b-Cell FunctionWe next performed mixed-model anal-yses to determine the predicted post-partum trajectories of fasting glucose,2-h glucose, Matsuda index, and ISSI-2in each of the four gestational glucosetolerance groups, after adjustment forage, ethnicity, family history of diabetes,time-dependent BMI, and months sincedelivery (Fig. 2). As shown in Fig. 2A,there was a significant difference amongthe groups in fasting glucose (P, 0.001)that was most apparent at 3 years post-partum but that was otherwise small inits overall magnitude. In contrast, therewas a clear difference among the groupsin 2-h glucose (P , 0.001), with a step-wise increase from normal GCT NGT toabnormal GCT NGT to GIGT to GDM ateach postpartum visit (Fig. 2B). Further-more, GDM predicted rising 2-h glucosebetween 1 and 3 years postpartum, incontrast to the other groups, whichshowed relative stability of their differ-ent degrees of postprandial glycemiabetween these visits (Fig. 2B).
These differences over time in glyce-mia were mirrored by striking differencesbetween the groups in insulin sensitivity(Matsuda index) and b-cell function (ISSI-2). Indeed, there was a stepwise decreasein the Matsuda index (Fig. 2C) and ISSI-2(Fig. 2D) from normal GCT NGT to abnor-mal GCT NGT to GIGT to GDM (both P,0.001) that was readily apparent at eachpoint in time. Even more revealing werethe patterns of change over time in these
3264 Gestational Dysglycemia and b-Cell Function Diabetes Care Volume 37, December 2014

measures. Indeed, although each gesta-tional glucose tolerance group showedthe same pattern of decreasing insulin
sensitivity from 3 months to 1 year to 3years postpartum, they each did soalong a distinct track (or different level)
of insulin sensitivity (Fig. 2C). Further-more, although each of the four groupsexhibited a different level of b-cell
Table 1—Characteristics of the four gestational glucose tolerance groups at recruitment in pregnancy, 3 months postpartum,1 year postpartum, and 3 years postpartum
Normal GCT NGT(n = 76)
Abnormal GCT NGT(n = 96) GIGT (n = 60) GDM (n = 105) P value
At recruitment in pregnancyAge (years) 34 (32–38) 34 (32–37) 34 (32–38) 35 (33–38) 0.71Ethnicity (%) 0.40White 75.0 75.0 68.3 65.7Asian 6.6 9.4 11.7 17.1Other 18.4 15.6 20.0 17.1
Family history of T2DM (%) 40.8 52.1 55.0 59.1 0.10Prepregnancy BMI (kg/m2) 24.2 (21.5–28.4) 22.8 (21.0–25.8) 23.9 (22.2–29.0) 25.0 (22.1–28.9) 0.04Parity (%) 0.65Nulliparous 56.6 53.1 48.3 50.51 39.5 37.5 38.3 41.0.1 3.9 9.4 13.3 8.6
Matsuda index 5.9 (4.1–7.6) 5.7 (3.8–7.9) 3.3 (2.6–5.0) 3.1 (2.2–4.6) ,0.001ISSI-2 832 (732–993) 843 (688–1,054) 617 (535–760) 522 (426–602) ,0.001
At 3 months postpartumMonths postpartum 3 (3–4) 3 (3–4) 3 (3–4) 3 (3–4) 0.77BMI (kg/m2) 25.6 (22.5–29.7) 25.2 (22.7–28.7) 26.2 (23.3–30.9) 26.5 (23.2–29.8) 0.46Waist circumference (cm) 89 (82–99) 86 (81–92) 88 (83–94) 90 (82–97) 0.11Breastfeeding (months) 3 (3–4) 3 (2–3) 3 (3–4) 3 (2–3) 0.30Current smoking (%) 1.3 2.2 5.3 1.9 0.54OGTTFasting glucose (mmol/L) 4.4 (4.2–4.7) 4.4 (4.2–4.8) 4.7 (4.4–4.9) 4.7 (4.4–5.0) ,0.0012-h glucose (mmol/L) 5.4 (4.7–6.1) 6.1 (5.2–7.2) 6.4 (5.2–7.3) 6.9 (5.7–8.6) ,0.001
Matsuda index 13.6 (8.7–17.4) 10.5 (7.6–16.5) 8.7 (6.0–13.0) 8.3 (5.9–12.2) ,0.001ISSI-2 826 (670–1,086) 776 (634–965) 664 (539–845) 637 (501–825) ,0.001
At 1 year postpartumMonths postpartum 12 (11–13) 12 (12–13) 12 (12–13) 12 (12–13) 0.22BMI (kg/m2) 24.8 (21.5–28.4) 23.8 (21.8–27.9) 25.4 (23.0–30.1) 25.4 (22.5–29.3) 0.15Waist circumference (cm) 85 (77–92) 83 (76–90) 86 (80–96) 87 (80–95) 0.08Breastfeeding (months) 11 (6–12) 10 (6–12) 9 (4–12) 10 (3–12) 0.36Current smoking (%) 2.7 3.2 8.8 2 0.20Total physical activity 8.1 (7.3–9.3) 8.6 (7.3–9.3) 8.3 (7.4–9.0) 8.3 (7.3–9.1) 0.99Sport index 2.6 (1.8–2.8) 2.3 (1.5–2.8) 2.0 (1.8–2.8) 2.3 (1.8–2.8) 0.85Leisure-time index 3.3 (2.8–3.5) 3.0 (2.5–3.5) 3.0 (2.8–3.3) 3.0 (2.8–3.5) 0.67Work index 3.0 (2.6–3.3) 3.1 (2.5–3.5) 3.0 (2.5–3.3) 3.0 (2.4–3.4) 0.67
OGTTFasting glucose (mmol/L) 4.6 (4.4–4.7) 4.6 (4.4–4.95) 4.8 (4.6–5.1) 4.8 (4.5–5.1) ,0.0012-h glucose (mmol/L) 5.3 (4.6–6.0) 6.0 (4.8–7.15) 6.1 (5.2–7.3) 6.8 (5.4–8.4) ,0.001
Matsuda index 11.1 (6.4–15.5) 10.0 (5.8–13.8) 7.5 (4.9–12.5) 7.6 (4.4–11.0) 0.002ISSI-2 832 (680–1,060) 768 (603–1,013) 690 (490–767) 629 (487–797) ,0.001
At 3 years postpartumMonths postpartum 30 (25–37) 36 (29–43) 39 (28–50) 31 (25–37) 0.002BMI (kg/m2) 24.6 (21.8–29.1) 24.0 (21.6–28.3) 24.8 (23.4–30.0) 25.4 (22.4–30.1) 0.20Waist circumference (cm) 85 (79–97) 85 (77–92) 86 (82–96) 88 (80–97) 0.13Current smoking (%) 4.0 2.1 15.5 2.9 0.005Total physical activity 8.8 (7.9–9.4) 8.7 (7.9–9.3) 9.0 (7.9–9.5) 8.5 (8.0–9.1) 0.77Sport index 3.0 (2.8–3.5) 3.0 (2.5–3.3) 3.0 (2.8–3.3) 3.0 (2.5–3.3) 0.55Leisure-time index 3.0 (2.5–3.5) 3.0 (2.5–3.3) 3.0 (2.5–3.3) 3.0 (2.8–3.3) 0.98Work index 2.5 (2.2–3.0) 2.8 (2.3–3.1) 2.8 (2.4–3.1) 2.6 (2.3–3.0) 0.08
OGTTFasting glucose (mmol/L) 4.6 (4.3–4.8) 4.5 (4.3–4.8) 4.8 (4.4–5.2) 4.9 (4.5–5.2) ,0.0012-h glucose (mmol/L) 5.4 (4.7–6.4) 5.9 (4.9–7.1) 6.5 (5.2–7.6) 6.8 (5.8–8.9) ,0.001
Matsuda index 10.0 (7.3–12.8) 8.2 (5.6–12.5) 7.4 (4.4–10.7) 6.3 (4.1–9.7) ,0.001ISSI-2 840 (716–1,087) 820 (629–1,076) 689 (510–937) 579 (453–809) ,0.001
Continuous data are shown as median (interquartile range) and categorical data as proportions. The P values refer to overall differences across thegroups by Wilcoxon rank sum test for continuous variables and by x2 test or Fisher exact test for categorical variables.
care.diabetesjournals.org Kramer and Associates 3265

function, women with recent GDM had apattern of declining b-cell function overtime, unlike the other three groups,which did not show this deterioration(Fig. 2D). Thus, although gestational glu-cose tolerance predicts distinct degreesof postpartum metabolic function (glyce-mia, insulin sensitivity, b-cell function), itis noteworthy that GDM is specificallycharacterized by worsening of postpran-dial glycemia and b-cell function duringthe first 3 years after delivery, after ad-justment for diabetes risk factors. In ad-dition, these findings were unchangedwith adjustment for waist circumference(as a time-dependent variable) in place ofBMI (data not shown).
Rates of Change of Glycemia, InsulinSensitivity, and b-Cell FunctionIn a series of mixed-model analyses, wenext compared the rates of change infasting glucose, 2-h glucose,Matsuda in-dex, and ISSI-2 among the gestationalglucose tolerance groups during the du-ration of follow-up (Table 2). Comparedwith the normal GCT NGT group (refer-ence), the GIGT and GDM groups bothshowed a modest but significantlyhigher rate of increase in fasting glucoseover time (Table 2A). For 2-h glucose, allthree gestational glucose intolerancegroups exhibited higher rates of in-crease than the reference group, whichprogressively rose from abnormal GCTNGT to GIGT to GDM in all models (Table2B). Similarly, these groups showed ananalogous pattern of greater deteriora-tion of insulin sensitivity in all modelsevaluating their rates of change inMatsuda index (Table 2C). Most impor-tantly, compared with the referencegroup, GIGT andGDMboth exhibited sig-nificantly greater worsening of b-cellfunction over time in all models (Table2D). In sensitivity analyses, the findingsin Table 2 were largely unchanged foreach outcome upon further adjustmentof model 3 for 1) having a subsequentpregnancy during follow-up (as did 54women) or 2) mode of contraception(data not shown).
Finally, to elucidate the clinical impli-cation of these distinct trajectories, we
evaluated how the postpartum meta-bolic effect of weight gain of 1 kg mayvary depending on gestational glucosetolerance status. Indeed, for twowomen with identical age, ethnicity,family history, height, weight, and dura-tion of follow-up, a 1-kg increase inweight during the 3-year postpartumfollow-up would have very different ef-fects, depending on their gestationalglucose tolerance. Specifically, in awoman with normal GCT NGT, this 1-kgincrease in postpartum weight wouldlead to a 0.15% decline in ISSI-2, a2.05% decline in Matsuda index, a0.07% increase in fasting glucose,and a 0.11% increase in 2-h glucose. Incontrast, if the woman instead hadGDM, this same 1-kg weight gain wouldlead to an eightfold greater decline inISSI-2 (1.21% vs. 0.15%), an almostidentical fall in the Matsuda index(2.08% vs. 2.05%), a threefold greaterincrease in fasting glucose (0.21% vs.0.07%), and a fivefold greater increasein 2-h glucose (0.59% vs. 0.11%).
CONCLUSIONS
In this study, we demonstrate a stepwiseincrease in the prevalence of dysglycemiaat each of 3 months, 1 year, and 3 yearspostpartum, as gestational glucose toler-ance worsens from normal (normal GCTNGT) to mildly abnormal (abnormal GCTNGT) to moderately abnormal (GIGT) toGDM. At each postpartum time point,
Figure 1—Prevalence of dysglycemia (predi-abetes or diabetes) over time within each ofthe four gestational glucose tolerancegroups. The P values refer to overall com-parison across the groups at the indicatedtime point.
Table 2—Mixed models showing the rate of change in fasting glucose (A), 2-h glucose (B), Matsuda index (C), and ISSI-2 (D) ineach of the four gestational glucose tolerance groups over the duration of follow-up, adjusted for model 1, model 2, andmodel 3
Normal GCT NGT (reference) Abnormal GCT NGT GIGT GDM
Estimate P value Estimate P value Estimate P value Estimate P value
A: Fasting glucoseModel 1a d d 0.0014 0.90 0.0470 <0.001 0.0470 <0.001Model 2b d d 0.0005 0.96 0.0500 <0.001 0.0440 <0.001Model 3c d d 20.0040 0.78 0.0040 0.003 0.0370 0.006
B: 2-h glucoseModel 1 d d 0.1020 0.001 0.1380 <0.001 0.2310 <0.001Model 2 d d 0.1100 0.002 0.1370 <0.001 0.2320 <0.001Model 3 d d 0.0570 0.04 0.0740 0.02 0.1270 <0.001
C: Matsuda indexModel 1 d d 20.1670 0.007 20.1830 0.009 20.2960 <0.001Model 2 d d 20.1790 0.007 20.1750 0.02 20.3100 <0.001Model 3 d d 20.1530 0.02 20.1420 0.05 20.2590 <0.001
D: ISSI-2Model 1 d d 20.0700 0.14 20.2320 <0.001 20.2960 <0.001Model 2 d d 20.0670 0.22 20.2180 <0.001 20.2840 <0.001Model 3 d d 20.0040 0.94 20.1390 0.02 20.1640 <0.001
Boldface indicates P, 0.05. aModel 1: age + ethnicity + family history of diabetes + time-dependent BMI +months postpartum. bModel 2: model 1 +duration of breastfeeding + physical activity at 1 year and 3 years. cModel 3: model 2 + development of diabetes at either 3 months or 1 year.
3266 Gestational Dysglycemia and b-Cell Function Diabetes Care Volume 37, December 2014

there was an analogous gradient of b-celldysfunction, insulin resistance, and in-creasing glycemia across these fourgroups. Most importantly, each degreeof gestational glucose intolerance inde-pendently predicted distinct trajectoriesof b-cell function, insulin sensitivity, andglycemia during the first 3 years postpar-tum. It thus emerges that the spectrumofglucose intolerance in pregnancy may en-able anticipation of the course of meta-bolic function in the first 3 years afterdelivery.A series of previous studies have
demonstrated that each degree of dys-glycemia in pregnancy predicts a pro-portionately increased future risk ofT2DM in the years thereafter, with GDMrepresenting the most extreme elementon both of these related continua (8–14).The presumed physiologic basis for this
relationship is that women who developgestational dysglycemia have a chronicb-cell defect that 1) yields insufficientcompensation for the severe insulin resis-tance of late pregnancy (resulting in theirdiagnostic antepartum hyperglycemia)and 2) underlies their predisposition tothe subsequent development of T2DM(17). Indeed, previous studies have con-firmed that women with each degree ofgestational dysglycemia (GDM, GIGT, andabnormal GCT NGT) have chronic b-celldysfunction that is detectable bothduringpregnancy and on cross-sectional evalua-tion after delivery (9,17,31–33). To date,however, there have been few longitudi-nal studies of the changes over time inb-cell function, insulin sensitivity, and gly-cemia in these groups.
Limiting features of the few longitu-dinal studies comprising this literature
have included the assessment of onlywomen with GDM (without compara-tors), restriction to a single ethnicgroup, and modest duration of follow-up or number of assessments. Specifi-cally, long-term studies in a cohort of72 Mexican American women withGDM showed that b-cell function de-clined over time in this patient popula-tion, although these analyses did nothave a comparison with a control groupwith normal gestational glucose toler-ance (34–36). In a recent study of 235Mexican American women evaluated ontwo occasions in the first 5 years afterpregnancy, Xiang et al. (37) reportedthat the 93 women with previous GDMhad faster deterioration of b-cell com-pensation and insulin sensitivity thanthe 142 women without a history ofGDM (some of whom were siblings orcousins of the women with GDM).Lastly, we previously demonstratedpostpartum deterioration of b-cellfunction after glucose intolerance inpregnancy but with only two measure-ments, at 3 and 12 months after deliv-ery, such that a reliable estimation oflonger-term metabolic trajectories wasnot possible (17,29).
In this context, the current study wasdesigned to address these limitationsthrough specific elements of the studydesign. First, this cohort is large (n =337) and consists of a multiethnic popu-lation (71% of which was white). Second,this study population underwent pro-spective ascertainment of glucose toler-ance in pregnancy, yielding a cohort thatspans the full spectrumof gestational glu-cose tolerance and enabling comparativeassessment of truly normal controls (nor-mal GCT NGT), women with intermediatedegrees of gestational dysglycemia, andthose with GDM. Third, this cohort un-derwent systematic metabolic charac-terization three different times afterpregnancy, thereby making it possi-ble to apply mixed-model analysisand elucidate the trajectories of meta-bolic features during the first 3 yearspostpartum.
These trajectories are particularly in-formative and offer insight into the differ-ential diabetic risk of these groups. First,it is apparent that the spectrum of gesta-tional glucose tolerance translates toanalogous gradients ofb-cell function, in-sulin sensitivity, and glycemia at each of 3months, 1 year, and 3 years postpartum.
Figure 2—Predicted trajectories of fasting glucose (A), 2-h glucose (B), Matsuda index (C), and ISSI-2(D) by gestational glucose tolerance group, after adjustment for age, ethnicity, family history ofdiabetes, time-dependent BMI, and months postpartum. The P values refer to the comparisonamong groups of their average values across all time points. Range bars show the SEM.
care.diabetesjournals.org Kramer and Associates 3267

Second, each strata of gestational dys-glycemia predicts varying rates of declin-ing b-cell function and insulin sensitivity,and rising glycemia, compared withwomen with completely normal glucosehomeostasis in pregnancy, independentof clinical risk factors for diabetes (Table2). However, these changes take placealong distinct tracks (Fig. 2), the patternsof which are revealing. Indeed, besidesthe poorest metabolic profile at eachpoint in time, GDM predicts a pattern ofdeclining b-cell function and rising 2-hglucose in the first 3 years postpartumthat is unlike that of the other groups.In contrast, GIGT and abnormal GCTNGT predict consistently poorer meta-bolic function (b-cell function, insulin sen-sitivity, glycemia) than that of womenwith normal gestational glucose toler-ance (normal GCT NGT) but with compa-rable patterns of change over the 3 years.In other words, the trajectories suggestthat GDM is a chronic metabolic disorderthat is specifically characterized by dete-rioration of b-cell function and risingpostprandial glycemia in the early post-partum years that drives the high risk ofprogression to T2DM in affected women.In contrast, GIGT and abnormal GCT NGTare also chronic metabolic disorders butare characterized by far more gradual de-terioration that will likely require a longerperiod of time for clinicalmanifestation oftheir intermediate diabetic risk. It is alsoof interest that insulin sensitivity declinedin all four gestational glucose tolerancegroups (including normal GCT NGT) dur-ing the first 3 years postpartum (Fig. 2C),raising the question of whether preg-nancy has an adverse long-term effecton insulin resistance. However, at pres-ent, whether this decline in insulin sensi-tivity continues in subsequent years is notknown.These insights hold potential clinical
implications. First, these data suggestthat careful analysis of the glycemic re-sponse to the stress test of pregnancyoffers an opportunity to anticipate thelongitudinal course of metabolic func-tion during the first 3 years after deliv-ery in all pregnant women (not justthose with GDM).Second, the effect of a modifiable fac-
tor, such as postpartum weight gain,may differ markedly depending on thegestational glucose tolerance group, asillustrated earlier by the example ofwomen with GDM experiencing a far
greater adverse effect on metabolismthan those with normal gestationalglucose homeostasis; this concept isconsistent with a previous report thatdemonstrated a more pronounced ef-fect of prepregnancy overweight on fu-ture T2DM in women with GDM than intheir peers (38).
Third, an understanding of these tra-jectories can potentially inform strate-gies that are targeted to an individualwoman’s likely course of metabolicfunction. Specifically, their differingpatterns of change over time suggestthat the gestational glucose tolerancegroups likely warrant different clinicalsurveillance strategies for optimal earlydetection of progression to dysglyce-mia. For example, although GDM willrequire the most intense clinical surveil-lance, GIGT and abnormal GCT NGT maydictate an intermediate approach in thisregard, in contrast to the truly low-riskpatient population with normal GCTNGT. Similarly, clinical advice regardingthe likelymetabolic effect of weight gainmay be tailored according to gestationalglucose tolerance status.
A limitation of this study is that b-cellfunction and insulin sensitivity were as-sessed with OGTT-based surrogate indi-ces rather than with clamp studies.However, their time-consuming and in-vasive nature would have made clampstudies difficult to complete on threeoccasions during 3 years in 337 newmothers. The serial assessments of thecurrent protocol were essential for elu-cidating the patterns of change overtime described in this report. Moreover,the ISSI-2 and Matsuda index are vali-dated measures that have been widelyused in previous studies (17,23–30), andthe serial OGTTs on which they were de-termined made it possible to also assessglucose tolerance status.
Another possible limitation is that thetesting protocol and diagnostic criteriafor GDM in this study may not be thesame as those used at other institutions,which can affect the generalizability ofour findings. However, the applicationof different glycemic thresholds for di-agnosing GDM would not obscure ourkey demonstration that the entire spec-trum of gestational glucose intoleranceis associated with analogous gradientsin the longitudinal changes over timein b-cell function, insulin sensitivity,and glycemia.
Finally, changes in dietary patternswere not assessed in this study andcould have affected the outcomes. How-ever, because major dietary modifica-tion generally translates into changesin weight, the inclusion of time-dependent BMI in all of the models likelymitigated the effect of this potentialconfounder.
In conclusion, each degree of gesta-tional dysglycemia predicts varying ratesof declining b-cell function and insulinsensitivity in the first 3 years postpartumcompared with women with completelynormal glucose homeostasis in preg-nancy. These differential changes likelyunderlie the gradient of future diabeticrisk associatedwith the spectrumof ante-partum dysglycemia. Most importantly,each element of the latter spectrum pre-dicts distinct trajectories of b-cell func-tion, insulin sensitivity, and glycemia, anunderstanding of which may enable thetailoring of clinical strategies for mitigat-ing the manifestation of diabetic risk inyoung women.
Funding. C.K.K. holds a Canadian DiabetesAssociation Postdoctoral Fellowship Award.A.J.H. holds a Tier-II Canada Research Chair inDiabetes Epidemiology. B.Z. holds the Sam andJudy Pencer Family Chair in Diabetes Researchat Mount Sinai Hospital and the University ofToronto. R.R. holds an Ontario Ministry ofResearch and Innovation Early ResearcherAward. This study was supported by operatinggrantsMOP-67063 and 84206 from the CanadianInstitutes of Health Research (CIHR), OG-3-08-2543-RR from the Canadian Diabetes Associa-tion, and NA6747 from the Heart and StrokeFoundation of Ontario.Duality of Interest. No potential conflicts ofinterest relevant to this article were reported.Author Contributions. C.K.K. wrote the firstdraft of the manuscript. C.K.K., B.S., and R.R.contributed to statistical analysis. A.J.H., P.W.C.,M.S., B.Z., and R.R. contributed to study con-ception and design. All authors contributed toanalysis and interpretation of the data and torevision of the manuscript for intellectualcontent. R.R. is the guarantor of this work and,as such, had full access to all of the data in thestudy and takes responsibility for the integrityof the data and the accuracy of the dataanalysis.Prior Presentation. Parts of this study werepresented in abstract form at the 74th ScientificSessions of the American Diabetes Association,San Francisco, California, 13–17 June 2014.
References1. Bellamy L, Casas JP, Hingorani AD, WilliamsD. Type 2 diabetes mellitus after gestational di-abetes: a systematic review and meta-analysis.Lancet 2009;373:1773–1779
3268 Gestational Dysglycemia and b-Cell Function Diabetes Care Volume 37, December 2014

2. Kim C, Newton KM, Knopp RH. Gestationaldiabetes and the incidence of type 2 diabetes:a systematic review. Diabetes Care 2002;25:1862–18683. Feig DS, Zinman B, Wang X, Hux JE. Risk ofdevelopment of diabetes mellitus after diagnosisof gestational diabetes. CMAJ 2008;179:229–2344. Schaefer-Graf UM, Klavehn S, Hartmann R,et al. How do we reduce the number of casesof missed postpartum diabetes in women withrecent gestational diabetes mellitus? DiabetesCare 2009;32:1960–19645. Ekelund M, Shaat N, Almgren P, Groop L,Berntorp K. Prediction of postpartum diabetesin women with gestational diabetes mellitus.Diabetologia 2010;53:452–4576. Egeland GM,Meltzer SJ. Following in mother’sfootsteps? Mother-daughter risks for insulinresistance and cardiovascular disease 15 years af-ter gestational diabetes. Diabet Med 2010;27:257–2657. Noctor E, Crowe C, Carmody LA, et al.ATLANTIC-DIP: prevalence of metabolic syn-drome and insulin resistance in women withprevious gestational diabetes mellitus by Inter-national Association of Diabetes in PregnancyStudy Groups criteria. Acta Diabetol 8 July2014 [Epub ahead of print]8. Retnakaran R. Glucose tolerance status inpregnancy: a window to the future risk of di-abetes and cardiovascular disease in youngwomen. Curr Diabetes Rev 2009;5:239–2449. Retnakaran R, Qi Y, Sermer M, Connelly PW,Hanley AJ, Zinman B. Glucose intolerance inpregnancy and future risk of pre-diabetes or di-abetes. Diabetes Care 2008;31:2026–203110. Carr DB, Newton KM, Utzschneider KM,et al. Modestly elevated glucose levels duringpregnancy are associated with a higher risk offuture diabetes among women without gesta-tional diabetes mellitus. Diabetes Care 2008;31:1037–103911. Vambergue A, Dognin C, Boulogne A, RejouMC, Biausque S, Fontaine P. Increasing inci-dence of abnormal glucose tolerance in womenwith prior abnormal glucose tolerance duringpregnancy: DIAGEST 2 study. Diabet Med2008;25:58–6412. Retnakaran R, Qi Y, Sermer M, Connelly PW,Hanley AJ, Zinman B. An abnormal screening glu-cose challenge test in pregnancy predicts post-partum metabolic dysfunction, even when theantepartum oral glucose tolerance test is normal.Clin Endocrinol (Oxf) 2009;71:208–21413. Retnakaran R, Shah BR. Abnormal screeningglucose challenge test in pregnancy and futurerisk of diabetes in young women. Diabet Med2009;26:474–47714. Retnakaran R, Qi Y, Connelly PW, SermerM,Hanley AJ, Zinman B. Risk of early progression toprediabetes or diabetes in women with recent
gestational dysglycaemia but normal glucosetolerance at 3-month postpartum. Clin Endocri-nol (Oxf) 2010;73:476–48315. Kulkarni SR, Fall CH, Joshi NV, et al. Deter-minants of incident hyperglycemia 6 years afterdelivery in young rural Indianmothers: the PuneMaternal Nutrition Study (PMNS). DiabetesCare 2007;30:2542–254716. Kew S, Ye C, Hanley AJ, et al. Cardiometa-bolic implications of postpartum weightchanges in the first year after delivery. DiabetesCare 2014;37:1998–200617. Retnakaran R, Qi Y, SermerM, Connelly PW,Hanley AJ, Zinman B. Beta-cell function declineswithin the first year postpartum in women withrecent glucose intolerance in pregnancy. Diabe-tes Care 2010;33:1798–180418. National Diabetes Data Group. Classifica-tion and diagnosis of diabetes mellitus andother categories of glucose intolerance. Diabe-tes 1979;28:1039–105719. Canadian Diabetes Association ClinicalPractice Guidelines Expert Committee. Cana-dian Diabetes Association 2013 clinical practiceguidelines for the prevention and managementof diabetes in Canada: definition, classificationand diagnosis of diabetes, prediabetes and met-abolic syndrome. Can J Diabetes 2013;37(Suppl.1):S8–S1120. Baecke JA, Burema J, Frijters JE. A shortquestionnaire for the measurement of habitualphysical activity in epidemiological studies. Am JClin Nutr 1982;36:936–94221. Pereira MA, FitzerGerald SJ, Gregg EW,et al. A collection of Physical Activity Question-naires for health-related research. Med SciSports Exerc 1997;29(Suppl.):S1–S20522. Ainsworth BE, Haskell WL, Whitt MC,et al. Compendium of physical activities: anupdate of activity codes and MET intensities.Med Sci Sports Exerc 2000;32(Suppl.):S498–S50423. Matsuda M, DeFronzo RA. Insulin sensitiv-ity indices obtained from oral glucose tolerancetesting: comparison with the euglycemic insulinclamp. Diabetes Care 1999;22:1462–147024. Retnakaran R, Shen S, Hanley AJ, Vuksan V,Hamilton JK, Zinman B. Hyperbolic relationshipbetween insulin secretion and sensitivity on oralglucose tolerance test. Obesity (Silver Spring)2008;16:1901–190725. Retnakaran R, Qi Y, Goran MI, Hamilton JK.Evaluation of proposed oral disposition indexmeasures in relation to the actual dispositionindex. Diabet Med 2009;26:1198–120326. Zinman B, Harris SB, Neuman J, et al. Low-dose combination therapy with rosiglitazoneand metformin to prevent type 2 diabetes mel-litus (CANOE trial): a double-blind randomisedcontrolled study. Lancet 2010;376:103–111
27. Kayaniyil S, Retnakaran R, Harris SB, et al.Prospective associations of vitamin Dwithb-cellfunction and glycemia: the PROspective Metab-olism and ISlet cell Evaluation (PROMISE) cohortstudy. Diabetes 2011;60:2947–295328. O’Gorman CS, Syme C, Lang J, Bradley TJ,Wells GD, Hamilton JK. An evaluation of earlycardiometabolic risk factors in children and ado-lescents with Turner syndrome. Clin Endocrinol(Oxf) 2013;78:907–91329. Retnakaran R, Qi Y, Ye C, et al. Hepatic insulinresistance is an early determinant of decliningb-cell function in the first year postpartum afterglucose intolerance in pregnancy. Diabetes Care2011;34:2431–243430. Kramer CK, Choi H, Zinman B, Retnakaran R.Glycemic variability in patients with early type 2diabetes: the impact of improvement in b-cellfunction. Diabetes Care 2014;37:1116–112331. Ward WK, Johnston CL, Beard JC, BenedettiTJ, Halter JB, Porte D Jr. Insulin resistance andimpaired insulin secretion in subjects withhistories of gestational diabetes mellitus.Diabetes 1985;34:861–86932. Ryan EA, Imes S, Liu D, et al. Defects in in-sulin secretion and action in women with a his-tory of gestational diabetes. Diabetes 1995;44:506–51233. Catalano PM, Huston L, Amini SB, KalhanSC. Longitudinal changes in glucose metabolismduring pregnancy in obese women with normalglucose tolerance and gestational diabetes mel-litus. Am J Obstet Gynecol 1999;180:903–91634. Xiang AH, Wang C, Peters RK, Trigo E, KjosSL, Buchanan TA. Coordinate changes in plasmaglucose and pancreatic beta-cell function in La-tino women at high risk for type 2 diabetes. Di-abetes 2006;55:1074–107935. Xiang AH, Kawakubo M, Trigo E, Kjos SL,Buchanan TA. Declining beta-cell compensationfor insulin resistance in Hispanic women withrecent gestational diabetes mellitus: associa-tion with changes in weight, adiponectin, andC-reactive protein. Diabetes Care 2010;33:396–40136. Xiang AH, Kjos SL, Takayanagi M, Trigo E,Buchanan TA. Detailed physiological character-ization of the development of type 2 diabetes inHispanic women with prior gestational diabetesmellitus. Diabetes 2010;59:2625–263037. Xiang AH, Takayanagi M, Black MH, et al.Longitudinal changes in insulin sensitivity andbeta cell function between women with andwithout a history of gestational diabetes melli-tus. Diabetologia 2013;56:2753–276038. Pirkola J, Pouta A, Bloigu A, et al. Prepreg-nancy overweight and gestational diabetes asdeterminants of subsequent diabetes and hy-pertension after 20-year follow-up. J Clin Endo-crinol Metab 2010;95:772–778
care.diabetesjournals.org Kramer and Associates 3269