DMOG Ameliorates IFN-γ-Induced Intestinal Barrier Dysfunction by Suppressing PHD2-Dependent HIF-1α...
10
FULL MANUSCRIPT DMOG Ameliorates IFN-g-Induced Intestinal Barrier Dysfunction by Suppressing PHD2-Dependent HIF-1a Degradation Wen-Sheng Wang, 1, * Hong-Yin Liang, 2, * Yu-Jiao Cai, 1 and Hua Yang 1 Hypoxia-inducible factor 1a (HIF-1a) has been well established as a protective factor for intestinal barrier function in intestinal epithelial cells. Recently, a study found that increased HIF-1a-induced intestinal barrier dysfunction. We proposed that lymphocyte-derived interferon-gamma (IFN-g) might be responsible for the intestinal barrier dysfunction caused by increased HIF-1a. HT-29 cell monolayers were grown in the presence or absence of IFN-g under hypoxia. Then, the transepithelial electrical resistance was measured, and HIF-1a- modulated intestinal barrier protective factors were quantified by polymerase chain reaction (PCR). PCR, western blotting, and chromatin immunoprecipitation of HIF-1a were performed. Dimethyloxalyglycine (DMOG), an inhibitor of prolyl-hydroxylases (PHDs) that stabilizes HIF-1a during normoxia, and RNA inter- ference of PHDs were also used to identify the signal pathway between IFN-g and HIF-1a. We demonstrated that IFN-g caused barrier dysfunction in hypoxic HT-29 cell monolayers via suppressing HIF-1a and HIF-1a- modulated intestinal barrier protective factors. We found that IFN-g decreased HIF-1a protein expression in- stead of affecting HIF-1a transcription or transcriptional activity. Study also showed that DMOG reversed the IFN-g-induced decrease in HIF-1a protein expression. Further, we found that PHD2 is the major regulator of IFN-g-induced HIF-1a degradation by PHD inhibition and RNA interference. We conclude that IFN-g caused barrier dysfunction by promoting PHD-, especially PHD2-, dependent HIF-1a degradation, and DMOG or PHD2 inhibition reversed this HIF-1a suppression and ameliorated barrier dysfunction. Combined with other studies demonstrating HIF-1a activation in lymphocytes promotes IFN-g secretion, these findings suggest a mechanism by which increased HIF-1a-induced intestinal barrier dysfunction. Introduction A monolayer of epithelium lines the entire gastroin- testinal tract and forms an essential barrier to the out- side world (Turner 2009). Intestinal barrier dysfunction and the resultant invasion of luminal bacteria and other antigens into the systemic circulation leads to gut inflammation and secondary disruption of the epithelial barrier, inducing or exacerbating systemic inflammatory response syndrome and resulting in 50%–80% of all deaths in surgical intensive care units (Taylor and Colgan 2007; Marchiando and others 2010). To date, the mechanism of intestinal barrier dysfunction re- mains incompletely understood. Hypoxia plays a role in many physiological and patho- logical processes and in a variety of clinical conditions, such as inflammatory bowel disease (Colgan and Eltzschig 2012), celiac disease (Vannay and others 2010), and ischemia/ reperfusion (Conde and others 2012). Recent studies have suggested that hypoxia-regulated pathways are highly as- sociated with the loss of epithelial function because the in- testinal mucosa experiences profound fluctuations in blood flow and metabolism after irritation (Furuta and others 2001). Notably, hypoxia-inducible factor 1 (HIF-1), which plays a key role in the cellular adaptation to hypoxia, triggers the transcription of many genes that enable intestinal epi- thelial cells to act as an effective barrier (Colgan and Taylor 2010). HIF-1 is a heterodimeric complex composed of the HIF-1a subunit and the constitutively expressed HIF-1b subunit. During normoxia, HIF-1a is hydroxylated by a family of prolyl-hydroxylases (PHDs), including PHD1, PHD2, and PHD3, which enables the von Hippel-Lindau factor (VHL) to bind, resulting in ubiquitination and rapid degradation by proteasomes (Brahimi-Horn and Pouyssegur 2009). However, during hypoxia, HIF-1a is stabilized and translocates to the nucleus. Then, HIF-1a binds to the specific sequence motif called the hypoxia response element (HRE) in 1 Department of General Surgery, Xinqiao Hospital, Third Military Medical University, Chongqing, China. 2 PLA Center of General Surgery, General Hospital of Chengdu Military Command, Chengdu, Sichuan Province, China. *These authors equally contributed to this work. JOURNAL OF INTERFERON & CYTOKINE RESEARCH Volume 00, Number 00, 2013 ª Mary Ann Liebert, Inc. DOI: 10.1089/jir.2013.0040 1
Transcript of DMOG Ameliorates IFN-γ-Induced Intestinal Barrier Dysfunction by Suppressing PHD2-Dependent HIF-1α...

FULL MANUSCRIPT
DMOG Ameliorates IFN-g-Induced Intestinal BarrierDysfunction by Suppressing PHD2-Dependent
HIF-1a Degradation
Wen-Sheng Wang,1,* Hong-Yin Liang,2,* Yu-Jiao Cai,1 and Hua Yang1
Hypoxia-inducible factor 1a (HIF-1a) has been well established as a protective factor for intestinal barrierfunction in intestinal epithelial cells. Recently, a study found that increased HIF-1a-induced intestinal barrierdysfunction. We proposed that lymphocyte-derived interferon-gamma (IFN-g) might be responsible for theintestinal barrier dysfunction caused by increased HIF-1a. HT-29 cell monolayers were grown in the presence orabsence of IFN-g under hypoxia. Then, the transepithelial electrical resistance was measured, and HIF-1a-modulated intestinal barrier protective factors were quantified by polymerase chain reaction (PCR). PCR,western blotting, and chromatin immunoprecipitation of HIF-1a were performed. Dimethyloxalyglycine(DMOG), an inhibitor of prolyl-hydroxylases (PHDs) that stabilizes HIF-1a during normoxia, and RNA inter-ference of PHDs were also used to identify the signal pathway between IFN-g and HIF-1a. We demonstratedthat IFN-g caused barrier dysfunction in hypoxic HT-29 cell monolayers via suppressing HIF-1a and HIF-1a-modulated intestinal barrier protective factors. We found that IFN-g decreased HIF-1a protein expression in-stead of affecting HIF-1a transcription or transcriptional activity. Study also showed that DMOG reversed theIFN-g-induced decrease in HIF-1a protein expression. Further, we found that PHD2 is the major regulator ofIFN-g-induced HIF-1a degradation by PHD inhibition and RNA interference. We conclude that IFN-g causedbarrier dysfunction by promoting PHD-, especially PHD2-, dependent HIF-1a degradation, and DMOG orPHD2 inhibition reversed this HIF-1a suppression and ameliorated barrier dysfunction. Combined with otherstudies demonstrating HIF-1a activation in lymphocytes promotes IFN-g secretion, these findings suggest amechanism by which increased HIF-1a-induced intestinal barrier dysfunction.
Introduction
Amonolayer of epithelium lines the entire gastroin-testinal tract and forms an essential barrier to the out-
side world (Turner 2009). Intestinal barrier dysfunction andthe resultant invasion of luminal bacteria and other antigensinto the systemic circulation leads to gut inflammation andsecondary disruption of the epithelial barrier, inducing orexacerbating systemic inflammatory response syndrome andresulting in 50%–80% of all deaths in surgical intensive careunits (Taylor and Colgan 2007; Marchiando and others 2010).To date, the mechanism of intestinal barrier dysfunction re-mains incompletely understood.
Hypoxia plays a role in many physiological and patho-logical processes and in a variety of clinical conditions, suchas inflammatory bowel disease (Colgan and Eltzschig 2012),celiac disease (Vannay and others 2010), and ischemia/reperfusion (Conde and others 2012). Recent studies have
suggested that hypoxia-regulated pathways are highly as-sociated with the loss of epithelial function because the in-testinal mucosa experiences profound fluctuations in bloodflow and metabolism after irritation (Furuta and others2001). Notably, hypoxia-inducible factor 1 (HIF-1), whichplays a key role in the cellular adaptation to hypoxia, triggersthe transcription of many genes that enable intestinal epi-thelial cells to act as an effective barrier (Colgan and Taylor2010). HIF-1 is a heterodimeric complex composed of theHIF-1a subunit and the constitutively expressed HIF-1bsubunit. During normoxia, HIF-1a is hydroxylated by afamily of prolyl-hydroxylases (PHDs), including PHD1,PHD2, and PHD3, which enables the von Hippel-Lindaufactor (VHL) to bind, resulting in ubiquitination and rapiddegradation by proteasomes (Brahimi-Horn and Pouyssegur2009). However, during hypoxia, HIF-1a is stabilized andtranslocates to the nucleus. Then, HIF-1a binds to the specificsequence motif called the hypoxia response element (HRE) in
1Department of General Surgery, Xinqiao Hospital, Third Military Medical University, Chongqing, China.2PLA Center of General Surgery, General Hospital of Chengdu Military Command, Chengdu, Sichuan Province, China.*These authors equally contributed to this work.
JOURNAL OF INTERFERON & CYTOKINE RESEARCHVolume 00, Number 00, 2013ª Mary Ann Liebert, Inc.DOI: 10.1089/jir.2013.0040
1

the promoter region of hypoxia response genes, which en-code a range of intestinal barrier protective factors in intes-tinal epithelial cells that increase mucin production (mucin-3)(Louis and others 2006), modify mucins intestinal trefoilfactor (ITF) (Furuta and others 2001), modify nucleotidemetabolism (5¢-nucleotidase ecto; nt5e; CD73) (Synnestvedtand others 2002; Colgan and others 2006), and regulate nu-cleotide signaling through CD55 (Louis and others 2005).
Nevertheless, the effect of constitutively active HIF-1a onthe intestinal barrier has been controversial. As an extensionof the original studies identifying the induction of HIF ex-pression within the intestinal mucosa, Shah and othersgenerated transgenic mice that constitutively express HIF-1aby disrupting VHL. They found that increased HIF-1aexpression correlated with more severe clinical symptomsand an increase in histological damage in a dextran sulfatesodium (DSS)-induced colitis model (Shah and others2008). Feinman and others (2010) also demonstrated thatpartial HIF-1a deficiency attenuated hemorrhagic shock-induced increases in intestinal permeability and bacterialtranslocation.
HIF-1a activation, which was thought to be protective forthe intestinal barrier commonly, causes epithelial barrierdysfunction in an unclear way. In fact, hypoxia occurs notonly in intestinal epithelial cells but also in intestinal lym-phocytes. More recently, there have been studies showingthat hypoxia can activate lymphocytes, leading to interferon-gamma (IFN-g) secretion (Shibahara and others 2005; Romanand others 2010). IFN-g is a pleiotropic cytokine that exertsa number of biological activities involved in host defenseand immunomodulation (Beaurepaire and others 2009). Theeffect of IFN-g on hypoxia-induced, HIF-1a-dependenttranscription in intestinal epithelial cells remains to bedetermined. However, there is evidence that IFN-g caninfluence HIF-1a transcriptional activity in glioblastomacells (Hiroi and others 2009). Thus, we hypothesized thatlymphocyte-derived IFN-g might be responsible for the in-testinal barrier dysfunction caused by increased HIF-1a.
In this study, we examined the effect of exogenous IFN-gon intestinal barrier function and the expression of HIF-1aand HIF-1a-induced intestinal barrier protective factors inhypoxic or hypoxic-like HT-29 cell monolayers, using thePHD inhibitor dimethyloxalyglycine (DMOG), which stabi-lized HIF-1a in vitro and in vivo (Milkiewicz and others 2004;Cummins and others 2006; Elvidge and others 2006). Ourresults demonstrated that IFN-g led to barrier dysfunctionin hypoxic HT-29 cells by repressing HIF-1a and HIF-1a-regulated intestinal barrier protective factors, and DMOGattenuated the barrier dysfunction caused by IFN-g by in-hibiting PHD2-dependent HIF-1a degradation.
Materials and Methods
Materials
HT-29 (human colorectal adenocarcinoma) cells were pur-chased from the Institute of Biochemistry and Cell Biology ofChinese Academy of Sciences [The same cell lines are used inXu and others (2012)]. IFN-g was purchased from Invitrogen,PHD inhibiter DMOG was purchased from Sigma-Aldrich.Anti-HIF-1a antibody was purchased from Novus Biologicals,Inc. (NB100-105). Anti-PHD1, anti-PHD2, and anti-PHD3antibodies were purchased from Santa Cruz Biotechnology,
Inc. Anti-tubulin antibody was purchased from GoodhereBiotechnology.
Cell culture and treatments
HT-29 was maintained in McCOY’s 5A medium (Hy-Clone; Thermo Fisher Scientific, Inc.) supplemented with10% fetal bovine serum (Gibco, Life Technologies) and an-tibiotics at 37�C with 95% air and 5% CO2. Cells weregrouped according to culturing conditions as normoxia (Nx),hypoxia (Hx), DMOG (DMOG), and IFN-g (IFN) treatment.DMOG or IFN-g treatment was achieved by culturing thecells in the medium containing DMOG (100 mg/mL) or IFN-g(20 ng/mL). Hypoxia was achieved by culturing the cells insealed hypoxic chambers (Thermo Fisher Scientific, Inc.) afterthe chambers had been flushed with a gas mixture composedof 2% O2, 5% CO2, and 93% N2.
Transepithelial electrical resistance measurement
Cells were split at confluence at a ratio of 1:10 using 0.05%trypsin/0.02% EDTA (Invitrogen) and then grown on Milli-pore Transwell in 24-well plates (0.3 mm pore size; 0.33 cm2).The electrical resistance of HT-29 intestinal monolayers wasmeasured by using an epithelial voltohmmeter (Millicell-ERSII; Millipore). Both apical and basolateral sides of themonolayers were bathed with medium. All treatment (Hx,IFN, DMOG, etc.) were achieved after 2 days from seeding.The transepithelial electrical resistance (TER) of monolayerswere reported after subtraction of the background filter re-sistance with the result multiplied with the monolayer areaof 0.33 cm2 leading to TER as O · cm2.
Quantitative polymerase chain reaction
Total RNA was extracted from cultured HT-29 cells usingTrizol (RNAiso Plus; TaKaRa) following the manufacturer’sinstructions. The cDNA was synthesized using the Prime-Script RT reagent Kit (TaKaRa) with oligo (dT) primerthrough reverse transcription. Quantitative polymerasechain reaction (PCR) (qPCR) analysis was performed usingSYBR Premix EX Taq II (TaKaRa) on Bio-Rad IQ5 (Bio-Rad).The sequences of the primers and lengths of the amplifiedproducts are detailed in Table 1. The particular reactionconditions were performed as follows: initial denaturation at95�C for 1 min, template denaturation at 95�C for 20 s, an-nealing at 60�C for 30 s, extension at 72�C for 1 min (total of40 cycles), and final extension at 72�C for 10 min. The cyclethreshold (CT) was determined with automatic baselinecalculations. CT value more than 30 was considered to beunacceptable. The relative gene expression was calculatedusing the 2 -DDCT methods. b-actin in identical reactions wasused to control the starting template.
Western blot analysis
Western blot analysis was performed as previously de-scribed (Sun and others 2012). Nuclear epithelial cell fractionswere prepared using the NE-PER extraction kit (Thermo-scientific). The protein concentration was determined accordingto the Bradford method using BCA assay reagent (Beyotime).Samples (20mg protein) were loaded onto SDS-PAGE gelsand the gels were transferred to polyvinylidene difluoridemembrane (Millipore) after electrophoresis. Membranes were
2 WANG ET AL.

blocked by 5% bovine serum albumin in TBS-T (50 mM Tris–HCl pH 7.5, 140 mM NaCl, and 0.1% Tween) and then incu-bated with the following primary antibodies at 4�C: anti-HIF-1a(1:200), anti-PHD1 (1:500), anti-PHD2 (1:500), anti-PHD3(1:500), and rabbit polyclonal anti-tubulin (1:1000). The mem-branes were then washed thrice and incubated with horserad-ish peroxidase-conjugated secondary antibodies. Membraneimaging was performed using the enhanced chemilumines-cence detection system (ECL; Boster) according to the manu-facturer’s instructions.
Chromatin immunoprecipitation assay
Chromatin immunoprecipitation (ChIP) assays were con-ducted according to the manufacturer’s manual for the ChIPKit (Upstate; Millipore). HT-29 cells were fixed with 1%paraformaldehyde. Chromatin from lysed HT-29 cells weresheared by using an F550 microtip cell solicitor (Fisher Scien-tific). After centrifugation, supernatants containing shearedchromatin were incubated with an anti-HIF-1a antibody(1:200; Novus Biologics) or control IgG (OE). Protein A Se-pharose was then added, incubated overnight, and immunecomplexes were eluted. Complexes were next treated withprotein K, extracted with phenol/chloroform, then with chlo-roform. DNA was precipitated, washed, dried, resuspended inwater, and analyzed by PCR (33 cycles). The primers used inthis analysis spanned 165 bp around the HIF-1 binding sitewithin the HRE (Forward primer, 5¢-CCACTTCCTCCTCACCTTCC-3¢ and Reverse primer, 5¢-TTC TCC CTG AAA TCCCAT CTT-3¢) (Rosenberger and others 2007).
Transient transfection assay
The inhibition of PHD1, PHD2, or PHD3 function, cellswere transiently transfected with short hairpin RNA(shRNA) plasmids, which aimed to interfere with PHD1,PHD2, or PHD3 expression, purchased from Genecopoeia,Inc., according to the manufacturer’s instructions. Briefly, theRNA interference sequence for human PHD1, PHD2, orPHD3 are detailed in Table 2.
Statistical analysis
All of the experiments were independently replicated atleast three separate times. Data were analyzed by SPSS
software (version 11.0 for windows) using Student’s t-test orANOVA and are showed as the mean – SD.
Results
IFN-c mediates barrier dysfunction in hypoxicHT-29 cell monolayers
To determine whether IFN-g modulates intestinal barrierfunction in hypoxic HT-29 monolayers, the TER was mea-sured under different conditions: normoxia (Nx), 20 ng/mLIFN-g (IFN), 2% O2 hypoxia (Hx), and IFN-g with simulta-neous hypoxia (Hx + IFN). The TER in the four groups stea-dily rose by the first 2 days (Fig. 1). All of the treatmentswere performed from this time. For the normoxia-treatedcells (Nx), very little difference in the TERs was seen. How-ever, there were varying decreases in the TER in the Hx, IFN,and Hx + IFN conditions. Forty-eight hours after treatment,there were significant differences among the four groups
Table 1. The Real-time Polymerase Chain Reaction
Primers Used in this Study
Name Primer sequences
Size ofproduct
(bp)
ITF F: CCAAGCAAACAATCCAGAGCA 79ITF R: GCTCAGGACTCGCTTCATGGMucin-3 F: CTGCTGCTACTACTTACAAGGTC 75Mucin-3 R: GCAGGGCAGATAGGCATTCTCD73 F: CCAGTACCAGGGCACTATCTG 136CD73 R: TGGCTCGATCAGTCCTTCCACD55 F: AGGCCGTACAAGTTTTCCCG 80CD55 R: CCTTCTCGCCAGGAATTTTCACb-actin F: GCACCACACCTTCTACAATGAGC 159b-actin R: TAGCACAGCCTGGATAGCAACG
ITF, intestinal trefoil factor.
Table 2. The RNA Interference Sequence
for Human PHD1, PHD2, or PHD3
Name Gene Location Target sequence
si-PHD1-1 EGLN2 561 gcggccgctgcagagtgaasi-PHD1-2 EGLN2 851 gcatgcggtactacggcatsi-PHD1-3 EGLN2 1043 gctgtcgaagcattggtgcsi-PHD1-4 EGLN2 1211 ggcgctgcatcacctgtatsi-PHD2-1 EGLN1 83 cctagtgctcctaatcatasi-PHD2-2 EGLN1 262 caagcaccacatgtgtttasi-PHD2-3 EGLN1 408 ggagttccagaatcgtgttsi-PHD2-4 EGLN1 830 atgagtcctcctagtaaagsi-PHD3-1 EGLN3 766 cctgcatctactatctgaasi-PHD3-2 EGLN3 817 tcctgcggatatttccagasi-PHD3-3 EGLN3 928 cttacgcaaccagatatgcsi-PHD3-4 EGLN3 155 gagttgcgagaaactttcc
PHD, prolyl-hydroxylase.
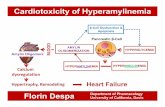
FIG. 1. Transepithelial electrical resistance (TER) measure-ments in the normoxia, interferon-gamma (IFN-g), hypoxia,and hypoxia plus IFN-g groups. The TERs were recorded forthe normoxia (Nx), IFN-g (IFN, 20 ng/mL), hypoxia (Hx, 2%O2), and IFN-g plus hypoxia (Hx + IFN)-treated HT-29 cellmonolayers. All of the treatments were performed 2 daysafter cell seeding. The readings 48 h after treatment weresignificantly different among the four groups (P < 0.05). TheTERs of the cells exposed to IFN-g plus hypoxia (Hx + IFN)were significantly lower than the cells treated with normoxia(Nx), IFN-g (IFN), or hypoxia (Hx) individually. The read-ings were performed in triplicate (n = 5).
PHD-INHIBITION AMELIORATES IFN-c-INDUCED IBF 3

studied (P < 0.05). The TER for the Hx + IFN group(10.467 – 0.746) was the lowest, significantly lower comparedwith the Nx (15.822 – 0.565), IFN (13.111 – 0.550), and Hx(14.600 – 0.551) groups at 48 h after treatment (P < 0.05). Hy-poxia plus IFN-g-induced a significant decrease in the TERcompared with normoxic treatment (5.356 – 0.446) that ex-ceeded the decreases caused by hypoxia or IFN-g individu-ally [(2.711 – 0.550) or (1.222 – 0.416)] (P < 0.05). These resultssuggest that both hypoxia and IFN-g disrupted intestinalbarrier function, but hypoxia combined with IFN-g amplifiedthe disruption caused by either treatment. There is synergybetween hypoxia and IFN-g in the loss of barrier function.
HIF-1a is involved in the IFN-c-induced lossof intestinal barrier function
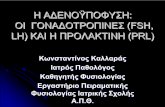
IFN-g suppressed the expression of protective factors. HIF-1awas thought to protect the intestinal barrier during hypoxiaby activating several intestinal barrier protective factors,including ITF, mucin-3, CD73, and CD55, rather than mod-ulating the tight junction proteins occludin and claudin(Colgan and Taylor 2010). However, the mechanism for theprotective factors involved in intestinal barrier function is notwell understood. In this study, we investigated whether theloss of intestinal barrier function caused by simultaneousIFN-g and hypoxia treatment was due to IFN-g-mediatedsuppression of HIF-1a-regulated expression of protectivefactors (Fig. 2). qPCR showed that the mRNA expression ofITF, mucin-3, CD73, and CD55 was significantly increasedafter hypoxia treatment, which is consistent with previous
reports (Furuta and others 2001; Colgan and Taylor 2010;Colgan and Eltzchig 2012). We found that IFN-g did notinfluence the mRNA levels of ITF, mucin-3, CD73, and CD73in the absence of hypoxia. However, the mRNA expressionof ITF, mucin-3, CD73, and CD55 in the Hx + IFN group wassignificantly lower than the Hx group, indicating that IFN-gsuppressed the expression of these HIF-1a-induced protec-tive factors. These results suggest that the downregulation ofintestinal barrier protective factors, ITF, mucin-3, CD73, andCD55, may account for the barrier dysfunction caused byIFN-g in hypoxic HT-29 cells.
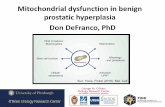
IFN-c regulated intestinal barrier protective factors via modu-lation of HIF-1a. Next, we tried to determine how IFN-gaffected these HIF-1a-induced intestinal barrier protectivefactors (Fig. 3). HIF-1a mRNA expression was determined byreverse transcription-PCR (Fig. 3A). The results confirmedthat HIF-1a transcription also increased during hypoxia(3.245 – 0.154) compared with normoxia (1.024 – 0.087)(P < 0.05). However, there was no significant difference inHIF-1a mRNA expression between the hypoxia (3.245 –0.154) and IFN-g plus hypoxia (3.019 – 0.127) treatmentgroups (P > 0.05). Western blot analysis (Fig. 3C) was alsoperformed to examine the changes in HIF-1a protein ex-pression. The abundance of nuclear HIF-1a protein duringhypoxia was significantly decreased by adding IFN-g(8.966 – 0.527) compared with the hypoxia only group(15.754 – 0.764). To detect the ability of HIF-1a, as a tran-scriptional factor, combined with the HRE, to regulate thetranscription of downstream factors, ChIP assays that usedprimers amplify a sequence within the promoter of VASPgene (Forward primer, 5¢-CCACTTCC TCCTCACCTTCC-3¢and Reverse primer, 5¢-TTC TCC CTG AAA TCC CAT CTT-3¢) were performed. However, the ChIP assays (Fig. 3E)showed that there was no significant difference between theHx (0.874 – 0.091) and Hx + IFN groups (0.848 – 0.075) usingan anti-HIF-1a antibody immunoprecipitation (P > 0.05), in-dicating that IFN-g did not affect the affinity of HIF-1a andHRE (transcriptional activity of HIF-1a). Therefore, theseresults suggest that IFN-g regulates the expression of intes-tinal barrier protective factors via modulation of HIF-1aprotein specifically, possibly by blocking HIF-1a proteintranslation or promoting HIF-1a protein degradation.
The PHD inhibitor DMOG ameliorates barrierfunction via repressing the HIF-1a degradationinduced by IFN-c
DMOG was used as a cell-permeable inhibitor of PHDs,including PHD1, PHD2, and PHD3 (Cummins and others2008). It has been previously shown to activate HIF-1a ex-pression in vitro and in vivo (Cummins and others 2006; El-vidge and others 2006). DMOG was used to replace hypoxiatreatment to stabilize HIF-1a without the harmful effects ofhypoxia and to investigate the mechanism of hypoxic barrierdysfunction caused by IFN-g.
Initially, the TERs were measured for the control, IFN-g(IFN, 20 ng/mL), DMOG (DMOG, 100 mg/mL), and IFN-gplus DMOG (DMOG + IFN)-treated HT-29 cell monolayers(Fig. 4). Identical to previous TER measurements, the TERsfor the four groups rose steadily within the first 2 days. All ofthe treatments were performed at this time. The readings at48 h after treatment were significantly different among thefour groups (P < 0.05). DMOG treatment resulted in a stable
FIG. 2. Effect of IFN-g on hypoxia-inducible factor 1a (HIF-1a)-regulated intestinal barrier protective factors in hypoxicHT-29 cells. Confluent HT-29 monolayers were exposed tonormoxia (Nx, 12 h), IFN-g (Nx, 20 ng/mL IFN-g with nor-moxia), hypoxia (Hx, 2% O2, 12 h), or 20 ng/mL IFN-g withhypoxia (Hx + IFN, 12 h). The total RNA was isolated, andthe mRNA levels of the intestinal barrier protective factorsintestinal trefoil factor (ITF), mucin-3, CD73, and CD55 weredetermined by quantitative polymerase chain reaction usingsemiquantitative analysis. b-actin was chosen as an internalcontrol. As shown, there was no significant difference be-tween the mRNA expression of ITF, mucin-3, CD73, andCD55 in the Nx group and Nx + IFN group. The mRNA ex-pression of ITF, mucin-3, CD73, and CD55 in the Hx groupsignificantly increased compared with the Nx group, but themRNA expression of ITF, mucin-3, CD73, and CD55 in theHx + IFN group was significantly lower than the Hx group(P < 0.05). Each column represents the mean – SD (n = 3,*P < 0.05).
4 WANG ET AL.

TER, and the control group had a slight decrease in TER.Similar results were obtained for the cells exposed to IFN-gand DMOG (DMOG + IFN), which is different from the cellsexposed to IFN-g only, suggesting that DMOG improvedbarrier function, which could not be reversed by IFN-g.
Given the importance of HIF-1a in adapting to hypoxiaand protecting intestinal barrier function (Ratcliffe 2007),western blot assays were performed (Fig. 5). We found thatDMOG treatment resulted in a stable increase in functionallyactive intestinal epithelial HIF-1a protein (8.782 – 0.243)compared with the control group (1.009 – 0.076) (P < 0.05).Interestingly, unlike hypoxia-induced HIF-1a stabilization,DMOG-induced HIF-1a protein expression could not beblocked by adding IFN-g. There was no statistically significantdifference in HIF-1a protein expression between the DMOG(8.782 – 0.243) and DMOG + IFN groups (8.457 – 0.152)(P > 0.05). The decrease of HIF-1a protein expression caused
by IFN-g under hypoxia was not recurrent in HT-29 cellsadministered with DMOG and IFN-g simultaneously,which possibly suppresses HIF-1a protein translation orpromotes HIF-1a protein degradation. Because DMOG in-hibits PHDs, DMOG activates HIF-1a by reducing its deg-radation. All of these results suggest that IFN-g suppressesHIF-1a protein expression by promoting HIF-1a proteindegradation via a PHD-dependent pathway, and DMOGblocked this decrease in HIF-1a protein expression by in-hibiting PHDs.
PHD2 is the key factor for IFN-c-mediated HIF-1adegradation during hypoxia
To further verify our hypothesis that IFN-g suppressedHIF-1a protein by promoting HIF-1a protein degradationvia a PHD-dependent pathway, shRNA plasmids that
FIG. 3. Effect of IFN-g on HIF-1a in hypoxic HT-29 cells. HT-29 cells were exposed to normoxia (Nx, 12 h), hypoxia (Hx, 2%O2, 12 h), or 20 ng/mL IFN-g with hypoxia (Hx + IFN, 12 h). (A) HIF-1a mRNA expression was determined by reversetranscription-PCR using semiquantitative analysis. b-actin was chosen as an internal control. (B) Densitometry analysis of thePCR results indicated there was no statistically significant difference between the Hx and Hx + IFN groups. (C) Western blotanalysis of HIF-1a. Tubulin was chosen as an internal control. (D) Quantitative analyses of the band intensities in (C) showedthat HIF-1a protein expression in the Hx group was lower than the Hx + IFN group (P < 0.05). (E) PCR analysis of the chromatinimmunoprecipitation (ChIP) assays. ChIP was performed using the chromatin from HT-29 cells in the Hx and Hx + IFN groupswith or without anti-HIF-1a antibody (Ab + or Ab - , respectively). Sheared DNA without the immunoprecipitations from eachgroup was also purified as an internal control. Purified DNA was analyzed by PCR using a primer for the hypoxia responseelement (HRE). (F) Densitometry analysis of the PCR results from the ChIP assays showed that there was no statisticallysignificant difference between the Hx and Hx + IFN groups using the anti-HIF-1a antibody. Immunoprecipitation showed thatIFN-g did not affect the affinity of HIF-1a and HRE. Each column represents the mean – SD (n = 3, *P < 0.05).
PHD-INHIBITION AMELIORATES IFN-c-INDUCED IBF 5

specifically inhibit PHD1, PHD2, or PHD3 expression weredesigned. These plasmids and a negative control plasmid(blank plasmid) were transfected into HT-29 cells accordingto the manufacturer’s instructions. Forty-eight hours aftertransfection, western blot analyses were performed to assessthe efficiency of these shRNA plasmids (Fig. 6). Quantitativeanalyses of the band intensities indicated that si-PHD1-4(Fig. 6B), si-PHD2-1 (Fig. 6D), and si-PHD3-4 (Fig. 6F) werethe most effective.
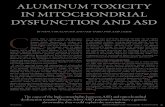
Then, we used si-PHD1-4-, si-PHD2-1-, and si-PHD3-4-transfected HT-29 monolayers (si-PHD1, si-PHD2, and si-PHD3 groups in the graph) to imitate IFN-g injury models.Normal and transfected HT-29 cells were incubated in thepresence or absence of 20 ng/mL IFN-g. Twelve hours aftertreatment, western blot analyses were performed to assessHIF-1a expression (Fig. 7A). PHD1, PHD2, and PHD3 inhi-bition each increased HIF-1a stability. As reported, PHD2 isthe major modulator for HIF-1a degradation (Fujita andothers 2012), and RNA interference (RNAi) of PHD2 pro-moted the greatest HIF-1a stability during normoxia. In ourstudy, HIF-1a protein expression in si-PHD2-transfected cellswas even higher than DMOG-treated cells, perhaps due tothe dose of DMOG used and the efficiency of RNAi. Except
for si-PHD2, PHD inhibition did not block IFN-g-inducedHIF-1a suppression. There was no statistically significantdifference between the si-PHD2 and si-PHD2 + IFN groups(P > 0.05), which was seen between the DMOG andDMOG + IFN groups. HIF-1a protein expression in the si-PHD1 + IFN and si-PHD3 + IFN groups was lower to differ-ent degrees than the si-PHD1 and si-PHD3 groups. Theseresults suggest that PHD2 is the key factor in IFN-g-medi-ated HIF-1a degradation.
All previous studies with RNAi used normoxic conditions.To confirm our observation, we utilized si-PHD2-transfectedHT-29 cells to repeat the hypoxia plus IFN-g treatment ex-periments. First, si-PHD2-transfected HT-29 cells were ex-posed to normoxia (Nx), hypoxia (Hx, 2% O2) or 20 ng/mLIFN-g, and 2% O2 hypoxia (Hx + IFN). Twelve hours aftertreatment, western blot analyses were performed (Fig. 7C),which confirmed that si-PHD2 transfection suppressedPHD2 expression and promoted HIF-1a stability duringnormoxia. The results also confirmed that PHD2 inhibitionreversed IFN-g-induced HIF-1a suppression.
Discussion
The results presented here demonstrated that IFN-g me-diated barrier dysfunction in hypoxic HT-29 cells via re-pression of HIF-1a and HIF-1a-regulated intestinal barrierprotective factors, including ITF, mucin-3, CD55, and CD73.The PHD inhibitor DMOG reversed this repression and at-tenuated the barrier dysfunction caused by IFN-g, and PHD2RNAi reproduced this reversal, indicating that IFN-g pro-motes HIF-1a degradation and decreases HIF-1a-regulatedintestinal barrier protective factors via the PHD2 signalingpathway. Additionally, IFN-g expression increased in hyp-oxic lymphocytes (Shibahara and others 2005). These find-ings provide impressive support for our hypothesis thathypoxia not only activates HIF-1a in intestinal epithelialcells, playing a protective role, but also activates HIF-1a inintestinal lymphocytes, increasing IFN-g expression, whichhas been certified in another study (Roman and others 2010),and suppressing HIF-1a-mediated protection in epithelialcells. These results may explain why overexpression of HIF-1a, an intestinal barrier protective factor, caused more severeintestinal barrier dysfunction in DSS-induced colitis modelsand some other models (Shah and others 2008; Kannan andothers 2011).
Within DMOG treatment, which stabilizes HIF-1a andactivates ITF, mucin-3, CD55, and CD73 during normoxia,we found DMOG stably preserved intestinal barrier functioncompared to the control group. During simultaneous IFN-g
FIG. 4. TER measurements for the control, IFN-g, di-methyloxalyglycine (DMOG), and DMOG plus IFN-ggroups. The TERs were recorded for the control, IFN-g (IFN,20 ng/mL), DMOG (DMOG, 100 mg/mL), and IFN-g plusDMOG (DMOG + IFN)-treated HT-29 cell monolayers. All ofthe treatments were performed 2 days after cell seeding. Thereadings 48 h after treatment were significantly differentamong the four groups (P < 0.05). TERs for the cells treatedwith DMOG (DMOG) or IFN-g and DMOG (DMOG + IFN)were higher compared with the control or IFN-g only (IFN)cells. The readings were performed in triplicate (n = 5).
FIG. 5. Effect of IFN-g on HIF-1a inDMOG-treated HT-29 cells. HT-29 cells weregrown in normal medium as control (Con)and in medium containing IFN-g (IFN,20 ng/mL, 12 h), DMOG (DMOG, 100mg/mL, 12 h), or IFN-g combined with DMOG(Hx + IFN, 12 h). (A) Western blot analysis ofHIF-1a was performed. Tubulin was used asan internal control. (B) Quantitative analysesof the band intensities in (A) indicated thatDMOG promoted HIF-1a stability, whichwas not reversed by IFN-g. Each columnrepresents the mean – SD (n = 3, *P < 0.05).
6 WANG ET AL.

and DMOG treatment, DMOG inhibited IFN-g-induced HIF-1a degradation and increased the expression of these pro-tective factors. Additionally, intestinal barrier function inIFN-g plus DMOG treatment group was also stably pre-served compared with the IFN-g-only treatment group.Thus, we can conclude that HIF-1a stabilization and activa-tion of HIF-1a-induced intestinal protective factors maintainintestinal barrier function. In contrast to the above results,IFN-g caused barrier dysfunction, and IFN-g suppressedHIF-1a-induced intestinal protective factors. So, we speculatethat IFN-g-induced intestinal barrier dysfunction wascaused, at least partially, by inhibition of HIF-1a-inducedintestinal protective factors.
Nevertheless, reports have demonstrated that increasedHIF-1a expression correlates with more severe clinicalsymptoms and increased histological damage in animalmodels (Shah and others 2008). Why overexpression of HIF-1a, an intestinal barrier protective factor, caused more severeintestinal barrier dysfunction is still confusing. According toprevious studies from our group and several studies re-ported by other groups, we hypothesize that lymphocyte-derived IFN-g, which is also induced by HIF-1a activation, isrelated to this phenomenon. IFN-g is a pleiotropic cytokinethat exerts a number of biological activities involved in hostdefense and immunomodulation (Billiau and Matthys 2009).More recently, a study has shown that hypoxia can activatelymphocytes to release IFN-g and that this increase in IFN-g
expression was HIF-1-dependent (Roman and others 2010).Another study has found that acute intestinal ischemia-reperfusion may activate intestinal intraepithelial lympho-cytes (IELs) and increase IELs-derived IFN-g expression(Shibahara and others 2005). Previous studies from ourgroup also have revealed that IELs play an important rolein the loss of intestinal barrier function in a mouse model oftotal parenteral nutrition (Yang and others 2003), whichrecently has been proven to be related to intestinal hypoxia( Jose-Cunilleras and others 2012). However, the effect ofIFN-g on HIF-1a-dependent transcription in intestinal epi-thelial cells remains to be determined. There are reports thatIFN-g modulates HIF-1a transcriptional activity throughthe IFN-g transcription factor signal transducer and acti-vator of transcription 1 (STAT1) (Hiroi and others 2009) orsilencing of the co-stimulatory factor CBP/P300 in othertissues (Gerber and others 2009). Given the protective ef-fect of HIF-1a in intestinal epithelial cells, we propose thathypoxia not only takes place in intestinal epithelial cellsbut also in intestinal lymphocytes. Hypoxia activates in-testinal lymphocytes to release IFN-g through an HIF-1a-dependent signaling pathway, which has been certified inother place, and lymphocyte-derived IFN-g affect HIF-1a-mediated intestinal epithelial cell protection, which hasbeen demonstrated in this study. This proposition may ex-plain why HIF-1a overexpression caused intestinal barrierdysfunction.
FIG. 6. RNA interference (RNAi)of prolyl hydroxylases 1, 2, and 3(PHD1, PHD2, and PHD3). HT-29cells were transiently transfectedwith short hairpin RNA (shRNA)that specifically suppressed PHD1,PHD2, or PHD3. Forty-eight hoursafter transfection, western blot an-alyses were performed to assessPHD1 (A), PHD2 (C), and PHD3 (E)expression. Quantitative analyses ofthe band intensities indicated thatsi-PHD1-4 (B), si-PHD2-1 (D), andsi-PHD3-4 (F) were the most effec-tive. These plasmids were used insubsequent studies. Each columnrepresents the mean – SD (n = 3,*P < 0.05).
PHD-INHIBITION AMELIORATES IFN-c-INDUCED IBF 7

We did not demonstrate that IFN-g affected HIF-1a tran-scriptional activity through STAT1 or CBP/P300, which hasbeen suggested by other studies that researched the rela-tionship between IFN-g and HIF-1a in brain or vascular tis-sues (Gerber and others 2009; Hiroi and others 2009).Alternatively, we found that IFN-g influenced HIF-1a pro-tein expression during hypoxia in intestinal epithelial cells,which may be related to decreased HIF-1a protein transla-tion or increased HIF-1a protein degradation, instead of HIF-1a transcription or transcriptional activity, as indicated byRT-PCR, western blotting, and ChIP (Fig. 3). This differencemay be explained by tissue specificity.
Further, we found that IFN-g-induced HIF-1a suppressioncould be reversed by DMOG, which activated HIF-1a by in-hibiting the classic PHDs-dependent degradation pathway(Chan and others 2002). Thus, the IFN-g-induced HIF-1asuppression may be due to increased PHD-dependent HIF-1adegradation. To identify the signaling pathway involved IFN-g-induced HIF-1a suppression, we designed shRNA plasmidsto inhibit PHD1, PHD2, or PHD3 expression and transfectedthem into HT-29 cells. We confirmed that PHD2 is the mainmodulator of HIF-1a degradation during normoxia, consistentwith a previous report that found that PHD2 was more spe-
cific for HIF-1a degradation and that PHD1 and PHD3 weremore specific for HIF-2a degradation (Fujita and others 2012).PHD2 inhibition also suppressed the IFN-g-induced decreasein HIF-1a effectively, but PHD1 and PHD3 inhibition did notreverse the IFN-g-induced decrease in HIF-1a, suggesting thatPHD2 is the key factor in IFN-g-mediated HIF-1a degradation.
Interestingly, PHDs have been considered to degradeHIF-1a during normoxia. PHDs utilize O2 as a substrate tohydroxylate HIF-1a, triggering HIF-1a degradation. Duringhypoxia, HIF-1a hydroxylation by PHDs is suppressedwithout O2 (Nakayama 2009). Nevertheless, in our study,we found that IFN-g promoted HIF-1a degradation throughPHD2 in hypoxic conditions in which PHDs were thoughtto be ineffective. O2-independent HIF-1a regulation is thefocus of the current HIF-1a research (Greer and others2012). O2-independent HIF-1a regulation functions not onlyas an adaptation to hypoxia but also in tumorigenesis andangiogenesis (Semenza 2012). Currently, O2-independent,HIF-1a-regulated pathways are known to include the smallubiquitin-related modifier (SUMO) (Cheng and others 2007;Ulrich 2007; Chan and others 2011) and hypoxia-associatedfactor (HAF) signaling pathways (Koh and Powis 2009).Few studies about a PHD2-induced, O2-independent,
FIG. 7. Effect of prolyl-hydroxylase (PHD) inhibition on HIF-1a in HT-29 cells with or without IFN-g treatment. (A) RNAiHT-29 cells were incubated in the presence or absence of 20 ng/mL IFN-g in the medium. Twelve hours after treatment,western blot analyses were performed to assess HIF-1a protein expression. (B) Quantitative analyses of the band intensities in(A) showed that PHD1, PHD2, and PHD3 inhibitors all increased HIF-1a stability, but DMOG treatment did not. (C) HT-29cells treated with PHD2-RNAi were exposed to normoxia (Nx, 12 h), hypoxia (Hx, 2% O2, 12 h), or 20 ng/mL IFN-g withhypoxia (2% O2 hypoxia) (Hx + IFN, 12 h). Then, western blot analyses were performed. (D, E) Quantitative analyses of theband intensities in (C) confirmed that PHD2 inhibition suppressed the IFN-g-induced decrease in HIF-1a protein expression.Each column represents the mean – SD (n = 3, *P < 0.05).
8 WANG ET AL.

HIF-1a-regulated pathway have been reported until now.However, recent studies have found that pyruvate kinase-M2(PK-M2) can promote HIF-1a protein degradation throughPHD2 and PHD3, especially PHD2 (Luo and others 2011;Tennant 2011). PK-M2 is the rate-limiting enzyme for gly-colysis and is also regulated by HIF-1a (Kress and others1998; Kosugi and others 2011). Under hypoxia, PK-M2 ac-cumulates and cell glycometabolism shifts from aerobic toanaerobic metabolism. Accumulated PK-M2 conversely pro-motes HIF-1a protein degradation through PHD2 and PHD3to reduce protein translation, conserve energy, and adapt tohypoxia (Luo and others 2011). Does IFN-g affect PK-M2 viaspecific pathways? PK-M2 may be the mechanism for IFN-g-induced HIF-1a degradation under hypoxic conditions.
Notably, another study reported that IFN-g attenuates HIFactivity in intestinal epithelial cells through repression ofHIF-1b (Glover and others 2011). In their research they foundthat IFN-g represses HIF activity in T84 epithelial cells. Theydemonstrated that IFN-g selectively repressed epithelial HIF-1b mRNA expression, but not HIF-1a mRNA, which waspartially coincident with our results. However, in their studythey did not show the change of HIF-1a protein level, whichwas critical to HIF activity, induced by IFN-g. Meanwhile,they mentioned that PHD may be a second potential mech-anism for repression of HIF-1 activity. But in their opinion,PHD-3 might be more important.
In summary, we found that IFN-g facilitated barrier dys-function by promoting PHDs, especially PHD2, leading toHIF-1a degradation, and DMOG or PHD2 inhibition couldreverse this HIF-1a decrease and improve barrier function.This phenomenon may account for how overexpression ofthe intestinal protective factor HIF-1a can induce more se-vere intestinal barrier dysfunction. However, this mechanismhas only been tested in vitro. Future studies in vivo andin vitro are required, and these studies will identify morecomponents along this pathway and lead to a more completeunderstanding of this interesting process.
Acknowledgment
This research was supported by the National NaturalScience Foundation of China (NSFC 30973113 to H.Y. andNSFC 81020108023 to H.Y.).
Author Disclosure Statement
No competing financial interests exist.
References
Beaurepaire C, Smyth D, McKay DM. 2009. Interferon-gammaregulation of intestinal epithelial permeability. J InterferonCytokine Res 29(3):133–144.
Billiau A, Matthys P. 2009. Interferon-gamma: a historical per-spective. Cytokine Growth Factor Rev 20(2):97–113.
Brahimi-Horn MC, Pouyssegur J. 2009. HIF at a glance. J Cell Sci122(Pt 8):1055–1057.
Chan DA, Sutphin PD, Denko NC, Giaccia AJ. 2002. Role ofprolyl hydroxylation in oncogenically stabilized hypoxia-in-ducible factor-1alpha. J Biol Chem 277(42):40112–40117.
Chan JY, Tsai CY, Wu CH, Li FC, Dai KY, Sun EY, Chan SH,Chang AY. 2011. Sumoylation of hypoxia-inducible factor-1alpha ameliorates failure of brain stem cardiovascular regu-lation in experimental brain death. PLoS One 6(3):e17375.
Cheng J, Kang X, Zhang S, Yeh ET. 2007. SUMO-specific pro-tease 1 is essential for stabilization of HIF1alpha duringhypoxia. Cell 131(3):584–595.
Colgan SP, Eltzschig HK. 2012. Adenosine and hypoxia-induc-ible factor signaling in intestinal injury and recovery. AnnuRev Physiol 74:153–175.
Colgan SP, Eltzschig HK, Eckle T, Thompson LF. 2006. Physio-logical roles for ecto-5¢-nucleotidase (CD73). Purinergic Signal2(2):351–360.
Colgan SP, Taylor CT. 2010. Hypoxia: an alarm signal duringintestinal inflammation. Nat Rev Gastroenterol Hepatol7(5):281–287.
Conde E, Alegre L, Blanco-Sanchez I, Saenz-Morales D, Aguado-Fraile E, Ponte B, Ramos E, Saiz A, Jimenez C, Ordonez A,Lopez-Cabrera M, del Peso L, de Landazuri MO, Liano F,Selgas R, Sanchez-Tomero JA, Garcia-Bermejo ML. 2012. Hy-poxia inducible factor 1-alpha (HIF-1 alpha) is induced duringreperfusion after renal ischemia and is critical for proximaltubule cell survival. PLoS One 7(3):e33258.
Cummins EP, Berra E, Comerford KM, Ginouves A, FitzgeraldKT, Seeballuck F, Godson C, Nielsen JE, Moynagh P, Pouys-segur J, Taylor CT. 2006. Prolyl hydroxylase-1 negativelyregulates IkappaB kinase-beta, giving insight into hypoxia-induced NFkappaB activity. Proc Natl Acad Sci USA103(48):18154–18159.
Cummins EP, Seeballuck F, Keely SJ, Mangan NE, Callanan JJ,Fallon PG, Taylor CT. 2008. The hydroxylase inhibitor di-methyloxalylglycine is protective in a murine model of colitis.Gastroenterology 134(1):156–165.
Elvidge GP, Glenny L, Appelhoff RJ, Ratcliffe PJ, Ragoussis J,Gleadle JM. 2006. Concordant regulation of gene expressionby hypoxia and 2-oxoglutarate-dependent dioxygenase inhi-bition: the role of HIF-1alpha, HIF-2alpha, and other path-ways. J Biol Chem 281(22):15215–15226.
Feinman R, Deitch EA, Watkins AC, Abungu B, Colorado I,Kannan KB, Sheth SU, Caputo FJ, Lu Q, Ramanathan M, AttanS, Badami CD, Doucet D, Barlos D, Bosch-Marce M, SemenzaGL, Xu DZ. 2010. HIF-1 mediates pathogenic inflammatoryresponses to intestinal ischemia-reperfusion injury. Am J Phy-siol Gastrointest Liver Physiol 299(4):G833–G843.
Fujita N, Markova D, Anderson DG, Chiba K, Toyama Y, Sha-piro IM, Risbud MV. 2012. Expression of prolyl hydroxylases(PHDs) is selectively controlled by HIF-1 and HIF-2 proteinsin nucleus pulposus cells of the intervertebral disc: distinctroles of PHD2 and PHD3 proteins in controlling HIF-1alphaactivity in hypoxia. J Biol Chem 287(20):16975–16986.
Furuta GT, Turner JR, Taylor CT, Hershberg RM, Comerford K,Narravula S, Podolsky DK, Colgan SP. 2001. Hypoxia-induciblefactor 1-dependent induction of intestinal trefoil factor protectsbarrier function during hypoxia. J Exp Med 193(9):1027–1034.
Gerber SA, Yatsula B, Maier CL, Sadler TJ, Whittaker LW, PoberJS. 2009. Interferon-gamma induces prolyl hydroxylase (PHD)3through a STAT1-dependent mechanism in human endothelialcells. Arterioscler Thromb Vasc Biol 29(9):1363–1369.
Greer SN, Metcalf JL, Wang Y, Ohh M. 2012. The updated bi-ology of hypoxia-inducible factor. EMBO J 31(11):2448–2460.
Glover LN, Irizarry K, Scully M, Campbell EL., Bowers BE,Aherne CM, Kominsky DJ, MacManus CF, Colgan SP. 2011.IFN-g attenuates hypoxia-inducible factor (HIF) activity inintestinal epithelial cells through transcriptional repression ofHIF-1b. J Immunol 186(3):1790–1798.
Hiroi M, Mori K, Sakaeda Y, Shimada J, Ohmori Y. 2009. STAT1represses hypoxia-inducible factor-1-mediated transcription.Biochem Biophys Res Commun 387(4):806–810.
PHD-INHIBITION AMELIORATES IFN-c-INDUCED IBF 9

Jose-Cunilleras E, Viu J, Corradini I, Armengou L, Cesarini C,Monreal L. 2012. Energy expenditure of critically ill neonatalfoals. Equine Vet J Suppl (41):48–51.
Kannan KB, Colorado I, Reino D, Palange D, Lu Q, Qin X,Abungu B, Watkins A, Caputo FJ, Xu DZ, Semenza GL,Deitch EA, Feinman R. 2011. Hypoxia-inducible factor plays agut-injurious role in intestinal ischemia reperfusion injury.Am J Physiol Gastrointest Liver Physiol 300(5):G853–G861.
Koh MY, Powis G. 2009. HAF: the new player in oxygen-independent HIF-1alpha degradation. Cell Cycle 8(9):1359–1366.
Kosugi M, Ahmad R, Alam M, Uchida Y, Kufe D. 2011. MUC1-Concoprotein regulates glycolysis and pyruvate kinase M2 ac-tivity in cancer cells. PLoS One 6(11):e28234.
Kress S, Stein A, Maurer P, Weber B, Reichert J, Buchmann A,Huppert P, Schwarz M. 1998. Expression of hypoxia-induciblegenes in tumor cells. J Cancer Res Clin Oncol 124(6):315–320.
Louis NA, Hamilton KE, Canny G, Shekels LL, Ho SB, ColganSP. 2006. Selective induction of mucin-3 by hypoxia in intes-tinal epithelia. J Cell Biochem 99(6):1616–1627.
Louis NA, Hamilton KE, Kong T, Colgan SP. 2005. HIF-dependentinduction of apical CD55 coordinates epithelial clearance ofneutrophils. FASEB J 19(8):950–959.
Luo W, Hu H, Chang R, Zhong J, Knabel M, O’Meally R, ColeRN, Pandey A, Semenza GL. 2011. Pyruvate kinase M2 is aPHD3-stimulated coactivator for hypoxia-inducible factor 1.Cell 145(5):732–744.
Marchiando AM, Graham WV, Turner JR. 2010. Epithelial bar-riers in homeostasis and disease. Annu Rev Pathol 5:119–144.
Milkiewicz M, Pugh CW, Egginton S. 2004. Inhibition of en-dogenous HIF inactivation induces angiogenesis in ischaemicskeletal muscles of mice. J Physiol 560(Pt 1):21–26.
Nakayama K. 2009. Cellular signal transduction of the hypoxiaresponse. J Biochem 146(6):757–765.
Ratcliffe PJ. 2007. HIF-1 and HIF-2: working alone or together inhypoxia? J Clin Invest 117(4):862–865.
Roman J, Rangasamy T, Guo J, Sugunan S, Meednu N, Pack-irisamy G, Shimoda LA, Golding A, Semenza G, Georas SN.2010. T-cell activation under hypoxic conditions enhances IFN-gamma secretion. Am J Respir Cell Mol Biol 42(1):123–128.
Rosenberger P, Khoury J, Kong T, Weissmuller T, Robinson AM,Colgan SP. 2007. Identification of vasodilator-stimulatedphosphoprotein (VASP) as an HIF-regulated tissue perme-ability factor during hypoxia. FASEB J 21(10):2613–2621.
Semenza GL. 2012. Hypoxia-inducible factors: mediators ofcancer progression and targets for cancer therapy. TrendsPharmacol Sci 33(4):207–214.
Shah YM, Ito S, Morimura K, Chen C, Yim SH, HaaseVH, Gonzalez FJ. 2008. Hypoxia-inducible factor augments
experimental colitis through an MIF-dependent inflamma-tory signaling cascade. Gastroenterology 134(7):2036–2048,2048.e1–3.
Shibahara T, Miyazaki K, Sato D, Matsui H, Yanaka A, Naka-hara A, Tanaka N. 2005. Alteration of intestinal epithelialfunction by intraepithelial lymphocyte homing. J Gastro-enterol 40(9):878–886.
Sun L, Wang W, Xiao W, Liang H, Yang Y, Yang H. 2012. An-giotensin II induces apoptosis in intestinal epithelial cellsthrough the AT2 receptor, GATA-6 and the Bax pathway.Biochem Biophys Res Commun 424(4):663–668.
Synnestvedt K, Furuta GT, Comerford KM, Louis N, KarhausenJ, Eltzschig HK, Hansen KR, Thompson LF, Colgan SP. 2002.Ecto-5¢-nucleotidase (CD73) regulation by hypoxia-induciblefactor-1 mediates permeability changes in intestinal epithelia.J Clin Invest 110(7):993–1002.
Taylor CT, Colgan SP. 2007. Hypoxia and gastrointestinal dis-ease. J Mol Med (Berl) 85(12):1295–1300.
Tennant DA. 2011. PK-M2 Makes Cells Sweeter on HIF1. Cell145(5):647–649.
Turner JR. 2009. Intestinal mucosal barrier function in health anddisease. Nat Rev Immunol 9(11):799–809.
Ulrich HD. 2007. SUMO teams up with ubiquitin to managehypoxia. Cell 131(3):446–447.
Vannay A, Sziksz E, Prokai A, Veres G, Molnar K, Szakal DN,Onody A, Korponay-Szabo IR, Szabo A, Tulassay T, Arato A,Szebeni B. 2010. Increased expression of hypoxia-induciblefactor 1alpha in coeliac disease. Pediatr Res 68(2):118–122.
Xu A, Yao M, Xu G, Ying J, Ma W, Li B, Jin Y. 2012. A physicalmodel for the size-dependent cellular uptake of nanoparticlesmodified with cationic surfactants. Int J Nanomedicine7:3547–3554.
Yang H, Fan Y, Teitelbaum DH. 2003. Intraepithelial lympho-cyte-derived interferon-gamma evokes enterocyte apoptosiswith parenteral nutrition in mice. Am J Physiol GastrointestLiver Physiol 284(4):G629–G637.
Address correspondence to:Dr. Hua Yang
Department of General SurgeryXinqiao Hospital
Third Military Medical UniversityChongqing 400037
China
E-mail: [email protected]
Received April 14, 2013/Accepted July 3, 2013
10 WANG ET AL.