Dacie and Lewis Practical Haematology || Laboratory control of anticoagulant, thrombolytic, and...
15
Click here to load reader
Transcript of Dacie and Lewis Practical Haematology || Laboratory control of anticoagulant, thrombolytic, and...

Anticoagulant and antithrombotic therapy is givenin various doses to prevent formation or propa-
gation of thrombus. Apart from those that act viafibrinolysis, anticoagulant drugs have little if anyeffect on an already-formed thrombus. There are fivemain classes of drugs that require consideration:
1. Oral anticoagulants, coumarins, and indanediones,which act by interfering with the γ-carboxylationstep in the synthesis of the vitamin K–dependentfactors (see p. 385).
2. Heparin and heparinoids (low molecular weightand synthetic compounds), which have a complex
action on haemostasis, the main effect being thepotentiation and acceleration of the effect ofantithrombin on thrombin and factor Xa.
3. Defibrinating agents such as ancrod (Arvin) andReptilase, which induce hypocoagulability by theremoval of fibrinogen from the blood.
4. Direct thrombin inhibitors, such as hirudin(natural or recombinant), which is a highly specificinhibitor of thrombin and thus a potent anti-coagulant. New orally active thrombin inhibitorsare now undergoing clinical trials.
5. Antiplatelet drugs such as aspirin, nonsteroidalanti-inflammatory drugs, dipyridamole and
18 Laboratory control ofanticoagulant,thrombolytic, andantiplatelet therapyMike Laffan and Richard Manning
Oral anticoagulant treatment 466Standardization of oral anticoagulant
treatment control 466Calibration of thromboplastins 467Local calibration of thromboplastins 468Determination of the international
normalized ratio 468Capillary reagent 469Therapeutic range and choice of
thromboplastin 469Management of overanticoagulation 469
Heparin treatment 470Laboratory control 471
Activated partial thromboplastin time for heparin monitoring 472
Heparin monitoring at the bedside 473Anti-Xa assay for heparin 473Protamine neutralization test 474Heparin-induced thrombocytopenia 475Hirudin 477
Thrombolytic therapy 477Laboratory control 477Investigation of a patient who bleeds
while taking thrombolytic agents 478Antiplatelet therapy 478
F06660-Ch18.qxd 2/24/06 3:36 PM Page 465

that the one-stage PT measures the effect of threevitamin K–dependent factors (factors VII, X, and II)and is also affected by the presence of PIVKAs(proteins induced by vitamin K absence or antago-nism) or the acarboxy forms of vitamin K–dependentfactors. It thus gives a better assessment of thesituation in vivo. Chromogenic substrate assays maybe of use where the presence of an inhibitorinvalidates the PT and coagulation-based assays.
The Thrombotest of Owren and the prothrombinand proconvertin (P&P) method of Owren and Aaswere used in the past, but they are no longerrecommended for oral anticoagulant control.
Standardisation of Oral AnticoagulantTreatment
Standardisation of oral anticoagulant therapycomprises the following steps:
1. A thromboplastin is chosen, and its ISI isdetermined by comparison with a referencethromboplastin.
2. The log mean normal PT is determined for thatthromboplastin.
3. PTs are performed on patient samples, and theresults are converted to an INR.
Reference thromboplastins (rabbit and bovine) areavailable as World Health Organization (WHO)Reference Preparations or certified reference materialsfrom the European Union Bureau of Reference (BCR)(see p. 695). All the reference preparations have beencalibrated in terms of a primary WHO reference ofhuman brain thromboplastin, which was establishedin 1967.
The following terms are used in the calibrationprocedure described below:
International Sensitivity Index (ISI)2 This is theslope of the calibration line obtained when thePTs obtained with the reference preparation areplotted on the vertical axis of log–log paper andthe PTs obtained by the test thromboplastin areplotted on the horizontal axis. The same normaland anticoagulated patient’s plasma samples areused for both sets of results.
International Normalized Ratio (INR) This is the PTratio, which, by calculation, would have been
466 PRACTICAL HAEMATOLOGY
clopidogrel, and inhibitors of IIb/IIIa function,some of which are antibodies.
ORAL ANTICOAGULANT TREATMENT
It is not possible to produce a therapeutic reductionin thrombotic tendency without increasing the riskof haemorrhage. The purpose of laboratory controlis to maintain a level of hypocoagulability thateffectively minimises the combined risks of haemor-rhage and thrombosis: the therapeutic range. Indivi-dual responses to oral anticoagulant treatment1 areextremely variable and so must be regularly andfrequently controlled by laboratory tests to ensurethat the anticoagulant effect remains within thetherapeutic range.
Selection of PatientsHaemostasis is not usually investigated before startingoral anticoagulant treatment, but it is advisable toperform the first-line coagulation screen (prothrom-bin time [PT], activated partial thromboplastin time[APTT], thrombin time [TT], and platelet count). Anabnormality of these tests must be investigatedbecause a contraindication to the use of oral anti-coagulants may be revealed and the tests may beused for controlling anticoagulant effect. History andclinical examination should be assessed to ensurethat no local or general haemorrhagic diathesis exists.
Methods Used for the Laboratory Control of Oral Anticoagulant TreatmentThe one-stage PT of Quick is the most commonlyused test. Originally, lack of standardisation of thethromboplastin preparations and methods ofexpressing the PT results led to great discrepanciesin the reported results and hence also in anti-coagulant dosage. The use of ISI, the InternationalSensitivity Index, to assess the sensitivity of anygiven thromboplastin, and the use of INR, theInternational Normalized Ratio, to report the results,has minimised these difficulties and greatly improveduniformity of anticoagulation and interpretationthroughout the world.
Chromogenic substrates have been used for thecontrol of anticoagulant treatment in factor X, VII,or II assays. Although it is possible to use such asingle factor measurement, it must be remembered
F06660-Ch18.qxd 2/24/06 3:36 PM Page 466

obtained had the original primary, humanreference thromboplastin been used to performthe PT.
Calibration of Thromboplastins
PrincipleThe test thromboplastin must be calibrated against
a reference thromboplastin of the same species(rabbit vs. rabbit, bovine vs. bovine).3 All referencepreparations are calibrated in terms of theprimary material of human origin and have anISI, which is assigned after a collaborative trialinvolving many laboratories from differentcountries.
ReagentsNormal citrated plasma. From 20 healthy donors.
Anticoagulated plasma. From 60 patients stabilised on oral anticoagulanttreatment for at least 6 weeks.
The tests need not all be done at the same timebut may be carried out on freshly collected sampleson successive days.
Reference and test thromboplastins.
CaCl2. 0.025 mol/l.
MethodCarry out PT tests as described on p. 398. Allow theplasma and thromboplastin to warm up to 37°C forat least 2 min before mixing or adding CaCl2. Testeach plasma in duplicate with each of the twothromboplastins in the following order withminimum delay between tests:
Record the mean time for each plasma. If there isa discrepancy of more than 10% in the clottingtimes between duplicates, repeat the test on thatplasma.
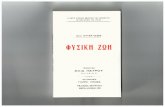
CalibrationPlot the PTs on log–log graph paper, with resultsusing the reference preparation (y) on the verticalaxis and results with the test thromboplastin (x) onthe horizontal axis (Fig. 18.1). On arithmetic paper,it is necessary to plot the logarithms of the PTs (Fig.18.2). The relationship between the two thrombo-plastins is determined by the slope of the line (b).
46718 Laboratory control of anticoagulant, thrombolytic, and antiplatelet therapy
Reference Test Thromboplastin Thromboplastin
Plasma 1 Test 1 Test 2
Test 4 Test 3
Plasma 2 Test 5 Test 6
Test 8 Test 7, etc.
x (s)
AC
By
(s)
20 30 40 50 60 70809010
20
30
40
50
60708090
Figure 18.1 Calibration of thromboplastin. The PTs(in seconds) with the test thromboplastin are plotted onthe horizontal axis (x) and with the referencethromboplastin on the vertical axis (y) on double loggraph paper. The best-fit line is drawn by eye, and theslope is obtained as follows: Points (a) and (b) aremarked on the line just below the lowest recorded PTand just above the longest recorded PT, respectively, (c) and a vertical through (b) meet. The distance between(b) and (c) is measured accurately in mm. The slope
b = . In this example B to C = 55 mm,
A to C = 35 mm, b = 55/35 = 1.57. The ISI of thereference thromboplastin was 1.11. Therefore, the ISI ofthe test thromboplastin = 1.11 × 1.57 = 1.74.
[B to C][A to C]
F06660-Ch18.qxd 2/24/06 3:36 PM Page 467

An estimate of the slope can be obtained asshown in Figures 18.1 and 18.2; this can then beused to obtain an approximation of the ISI of thetest thromboplastin.
Whenever possible, however, to obtain a reliablemeasurement, the following more complicatedcalculation should be used instead.
Calculation of International Sensitivity IndexThe natural logarithms of the PTs obtained usingthe reference thromboplastin and the test throm-boplastin are called yi and xi, respectively, wherei=1,2,3….N for N pairs of results.
The following designations are then made:
x0 and y0 are the arithmetic means of the N valuesof xi and yi, respectively.
Q1 and Q2 are the sums of the squares of (xi – x0)and (yi – y0), respectively.
P is the sum of their products ∑(x i– x0)(yi – y0)E = (Q2 – Q1)
2 + 4P2
And b = Q2 – Q1 + E1/2
2P
where b is the slope of the graph. The ISI of thepreparation under test (ISIt) is then given by thefollowing:
ISIt = ISIIRP × bwhere IRP stands for International ReferencePreparation.
Local Calibration of Thromboplastins
Although the ISI system has been very effective instandardising anticoagulant control and improvingagreement between laboratories, it is not perfect.One reason is that the ISI of a thromboplastin mayvary according to the coagulometer used and evenwith different models of the same instrument. Tocircumvent this, a system of local calibration hasbeen suggested. In this system, a set of plasmas withan assigned INR are tested with the localthromboplastin–machine combination. These resultsare used to generate a standard curve from whichthe INRs of further test plasmas can be read byinterpolation. In effect, the ISI of the system isdetermined in a reverse fashion.3,4
Mean Normal Prothrombin TimeThe mean normal PT for each batch of thrombo-plastin should be determined by testing 20 normalsamples or blood donors. An equal number of malesand females should be tested.
Calibration AuditsExternal quality-assurance surveys (e.g., UKNEQAS,see p. 667) will reflect differences regardingthromboplastin–machine combinations but notdifferences in blood sampling techniques (i.e.,capillary and venous blood sampling). This can be aproblem when capillary blood sampling is used inan outpatient setting, whereas venous samples aretaken for inpatient anticoagulant monitoring.Regular audits comparing results from a range ofpatients whose blood has been sampled by bothcapillary and venous techniques will provideinformation not provided by NEQAS surveys.4,5
Determination of the InternationalNormalized Ratio
It is essential to use a thromboplastin whose ISI hasbeen determined either by the commercial supplier
468 PRACTICAL HAEMATOLOGY
Log PT (x)
A C
BLo
g PT
(y)
1.0 1.2 1.4 1.6 1.8
1.2
1.4
1.6
1.8
Figure 18.2 Calibration of thromboplastin. The PTs(in seconds) are converted to their logarithms which areplotted on arithmetic graph paper. The slope iscalculated as in Figure 18.1. In this example, A to C =42 mm, B to C = 65 mm, b = 65/42 = 1.54. Therefore, ISI= 1.11 × 1.54 = 1.71.
F06660-Ch18.qxd 2/24/06 3:36 PM Page 468

or (preferably) according to a local, regional, ornational procedure. The PT result can then beexpressed as an INR. Using the INR/ISI system, thepatients’ INR should be the same in any laboratoryin the world. To ensure safety and uniformity ofanticoagulation, the results should be reported as anINR, either alone or in parallel with the locallyaccepted method of reporting.
INR = Prothrombin time ratio obtained using thetest thromboplastin to the power of the ISI of thetest reagent. The PT ratio is calculated using the patient’s test result and the log mean normalprothrombin time (LMPT) from 20 normal donors:INR = (PT patient/LMNPT)ISI
For example, a ratio of 2.5 using a thromboplastinwith ISI of 1.4 can be calculated from the formula tobe 2.51.4 = 3.61, which is either read from a logarithmictable or calculated on an electronic calculator.
The LMNPT is the logarithmic mean normal PT(i.e., e(ΣlnPT)/N). In this way the level of anticoa-gulation in all plasma samples can be compared anda meaningful therapeutic range can be establishedregardless of the thromboplastin used.
Capillary ReagentReagents are commercially available for monitoringthe INR using samples of capillary blood. These are usually a mixture of thromboplastin, calcium,and adsorbed plasma so that when whole blood is added the reagent measures the overall clottingactivity; it is sensitive to deficiency of factors II, VII, and X. The reagents have an ISI assigned to
them in the same way as individual thrombo-plastins, and the INR is calculated from the PT ratio.These reagents are frequently used in anticoagulantclinics when a large number of INRs need to be performed rapidly and in point-of-care testing (p. 637).
Therapeutic Range and Choice of Thromboplastin
Several authorities have now published recommendedtherapeutic ranges denoting the appropriate degree ofanticoagulation in different clinical circumstances.1,6,7
These are partly based on controlled clinical trials butto some extent also represent a consensus on practicethat has emerged over many years.
The choice of thromboplastin largely determinesthe accuracy with which anticoagulant control canbe maintained. If the ISI of the thromboplastin ishigh, then a small change in PT represents a largechange in the degree of anticoagulation. This affectsthe precision of the analysis, and the coefficient ofvariation for the test increases with the ISI. More-over, the prothrombin ratio range becomes very smallfor any given range of INR. This is illustrated inFigure 18.3 and Table 18.1. For these reasons it isstrongly recommended that a thromboplastin with alow ISI (i.e., close to 1) is used.
Management of Overanticoagulation
The approach to management of a patient whoseINR exceeds the therapeutic range with or withoutbleeding is shown in Table 18.2.6
46918 Laboratory control of anticoagulant, thrombolytic, and antiplatelet therapy
1
2
3
4
5
6
INR
Vertical lines represent therapeuticrange in terms of prothrombin ratios,for any given ISI
1.0
1.1
1.21.3
1.41.5 1.6 1.7 1.8 1.9 2.0 2.1 2.2 2.3 2.4 2.5
Figure 18.3 The ratiosobtained with thromboplastinswith given ISI valuesequivalent to INR therapeuticrange of 2.0–4.5. (Slightlymodified, from Poller L 1987Oral anticoagulant therapy. In:Bloom AL, Thomas DP (eds)Haemostasis and thrombosis,2nd edn. Churchill Livingstone,Edinburgh with the permissionof the editors and the publisher.)
F06660-Ch18.qxd 2/24/06 3:36 PM Page 469

Point-of-Care TestingThere are now schemes for monitoring INR at pointof care outside the hospital clinic. These requireselection and standardisation of appropriate analysersand a quality-control programme that includesparticipation in an external quality assessmentscheme. It is essential to have liaison with the locallaboratory for training of staff and supervision ofthe quality-control programme. There should be anestablished procedure for checking any problems ofinstrument performance and for referring to thespecialist centre patients who are difficult tocontrol.8,9
Self-management of warfarin treatment akin tohome glucose monitoring may also be an effectivepoint-of-care procedure for selected patients. Theyshould first attend two or more training sessions onthe use and quality control of the appropriateanalyser, interpretation of INR in terms of adjust-ment of their warfarin dosage, and guidance onwhen it is necessary to be seen at the specialistclinic.10 (See p. 634.)
HEPARIN TREATMENT
The anticoagulant action of heparin is primarily aresult of its ability to bind to antithrombin (AT),
thereby accelerating and enhancing the latter’s rateof inhibition of the major coagulation enzymes (i.e.,factors IIa and Xa and to lesser extents IXa, XIa,and XIIa). The two main effects of heparin, the ATand the anti-Xa effects, are differentially dependenton the size of the heparin molecule. The basicminimum sequence needed to obtain anticoagulantactivity has been identified as a pentasaccharideunit. Of the molecules containing this pentasaccha-ride, those comprising less than 18 saccharide unitsand of molecular weight less than 5000 can onlyaugment inhibitory activity of AT against Xa. Incontrast, longer chains can augment AT activity aswell by formation of a tertiary complex bridgingboth AT and thrombin molecules.
Hence low molecular weight heparins (LMWH),which have an average molecular mass of 5000 Da,have a ratio of anti-Xa to antithrombin effect of2–5 compared to that of unfractionated heparin(UFH), which is defined as 1. However, all heparinpreparations are heterogeneous mixtures of moleculeswith different molecular weight and many do not
470 PRACTICAL HAEMATOLOGY
Table 18.1 Therapeutic ranges equivalent to anINR of 2.0–4.0 using different commercialthromboplastins. (Modified from Poller L 1987 Oralanticoagulant therapy. In: Bloom AL, Thomas DP(eds) Haemostasis and thrombosis, 2nd edn.Churchill Livingstone, Edinburgh, p. 870.)
Thromboplastin ISI Ratios equivalent to INR 2.0–4.0
Thrombotest 1.03 2.0–3.8
Thromborel 1.23 1.7–3.1
Dade FS 1.35 1.65–2.8
Simplastin 2.0 1.3–2.0
Boehringer 2.1 1.35–1.9
Ortho 2.3 1.3–1.8
ISI, International Sensitivity Index; INR, InternationalNormalized Ratio
Table 18.2 Recommendations for management ofbleeding and excessive anticoagulation
3.0 < INR < 6.0 (target 1. Reduce warfarin dose INR 2.5) or stop
4.0 < INR < 6.0 (target 2. Restart warfarin when INR 3.5) INR < 5.0
6.0 < INR < 8.0 1. Stop warfarinNo bleeding or minor 2. Restart when INR < 5.0bleeding
INR > 8.0 1. Stop warfarinNo bleeding or minor 2. Restart warfarin when bleeding INR < 5.0
3. If other risk factors forbleeding give 0.5–2.5 mg ofvitamin K (oral or IV)
Major bleeding 1. Stop warfarin2. Give prothrombin complexconcentrate 50 u/kg of FFP 15 ml/kg3. Give 5 mg of vitamin K (oral or IV)
FFP, fresh-frozen plasma; INR, International Normalized Ratio
F06660-Ch18.qxd 2/24/06 3:36 PM Page 470

contain the crucial pentasaccharide sequence. Heparinalso produces some anticoagulant effect by promotingthe release of tissue factor pathway inhibitor (TFPI)from the surface endothelium (see p. 386).
Selection of Patients
It is advisable to perform the first-line tests ofhaemostasis as described in Chapter 16 before startingtreatment. In the presence of a reduced plateletcount or deranged coagulation, heparin may becontraindicated or, if used, the dose must be reduced.
Laboratory Control of Heparin Treatment11
The pharmacokinetics of heparins are extremelycomplicated, partly because of the variation inmolecule size. Large molecules are cleared by arapid saturable cellular mechanism and bind tonumerous acute-phase proteins such as von Wille-brand factor and fibronectin. Smaller molecules arecleared by a nonsaturable renal route and bind lessto plasma proteins. As a result therapeutic doses ofUFH result in a variable degree of anticoagulationand require close monitoring (Table 18.3). The dose-response relationship is much more predictable forthe LMWHs, and most trials have not monitored
therapy with these agents, which are simply givenon a “units per kg” basis. Thus the approach tomonitoring heparin therapy varies according to thetype of heparin used and the clinical circumstance.
Prophylactic therapy with either UFH or LMWH isgiven by subcutaneous injection and is usually notmonitored. However, LMWH may be monitored insome circumstances when it is expected thatpharmacokinetics may be altered, such as duringpregnancy and in renal failure. A blood sample istaken 2–4 hours after injection to detect the peakheparin level. Some authors have also measuredtrough levels prior to injection.
Therapeutic treatment with UFH is given by conti-nuous intravenous infusion and is usually monitoredusing the APTT, which is repeated 6 hours afterevery dose change. Rarely, therapeutic UFH is giventwice daily by subcutaneous injection, in which casesamples for testing should be taken at the midpointbetween injections. If heparin resistance is suspected,then an anti-Xa assay must be performed.
Therapeutic treatment with LMWH is not moni-tored except when the dose-response relationship isexpected to be altered such as in the case of preg-nancy, children, and renal failure. LMWHs producerelatively little effect on the APTT, and if moni-toring is required, a specific heparin assay must be
47118 Laboratory control of anticoagulant, thrombolytic, and antiplatelet therapy
Table 18.3 Tests used in the laboratory control of heparin treatment
Test Advantages Disadvantages
Whole blood clotting Simple, inexpensive, no equipment needed Time consuming, can only be carried out at time the bedside, one at a time, insensitive to
<0.4 iu and to LMW heparins
APTT Simple, many tests can be carried out Not all reagents sensitive to heparin, in parallel insensitive to <0.2 iu and to LMW heparins,
affected by variables other than heparin
TT Simple, many tests can be carried out Insensitive to <0.2 iu and to LMW heparinsin parallel
Protamine neutralisation Sensitive to all concentrations Time consuming and insensitive to LMWheparins
Anti-Xa assays Sensitive to all concentrations and Expensive if commercial kits used; time to LMWT heparins consuming if home-made reagents used
APTT, activated partial thromboplastin time; LMW, low molecular weight; TT, thrombin time
F06660-Ch18.qxd 2/24/06 3:36 PM Page 471

used. The result will then be reported as heparinactivity in u/ml. In general, unless stated otherwise,this is measured as anti-Xa activity. An inter-national standard for LMWH is now available.12
It is important to note that therapeutic levels ofLMWH may be present without producing prolon-gation of PT, APTT, or TT. The dose-response curveof the TT is too steep to make it useful for monitoringheparin therapy. However, it is very sensitive to thepresence of UFH and is a useful laboratory indicatorof its presence.
Activated Partial Thromboplastin Time for Heparin Monitoring
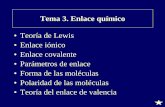
Principle The APTT is currently the most widely used test formonitoring unfractionated heparin therapy.6 It isvery sensitive to heparin but has a number of short-comings that must be kept in mind. First, differentAPTT reagents have different sensitivities toheparin. It is important to establish that the reagentin use has a linear relationship between clottingtimes and heparin concentration in the therapeuticrange (0.3–0.7 iu/ml). An example of differentresponses is shown in Fig. 18.4. The result is expressedas a ratio of the time obtained with that for thenormal pool containing no heparin (often called“the heparin ratio”).
The second shortcoming of the APTT in the controlof heparin treatment is that the APTT is affected bya number of variables not related to heparin. Themost important of these are fibrinogen and factorVIII:C concentration and the presence offibrinogen/fibrin degradation products (FDP). Whenthese factors are abnormal, there may be dissocia-tion of the APTT and heparin level causing “apparentheparin resistance.” In these circumstances aheparin assay must be performed. Last, the use ofthe APTT may be rendered invalid by the presenceof inhibitors, factor deficiency (including liverdisease), or other coagulation active drugs. Inseverely ill patients a significant prolongation of theAPTT may arise from disseminated intravascularcoagulation (DIC) or haemodilution, giving amisleading impression of heparin effect.
Reagents and MethodThe reagents and method are described on p. 400.
Therapeutic RangeThe therapeutic range for heparin is 0.3–0.7 iu/mlby anti-Xa assay and 0.2–0.4 units by protaminetitration. The prolongation of the APTT achievedwith these concentrations varies between reagentsaccording to the reagents and coagulometer used.The results may be expressed as clotting time inseconds or as a ratio. For the majority of sensitivereagents, ratios of 1.5–3.0 cover the therapeuticrange, but this must be determined for each reagentand, ideally, each batch of reagent. It is importantthat samples from patients treated with heparin areused for calibration because these give significantly
472 PRACTICAL HAEMATOLOGY
1.0
1.5
2.0
2.5
3.0
3.5
0 0.1Heparin (iu/ml)
A
B
C
0.2 0.3
APTT
rat
io
Figure 18.4 APTT response to heparin added toplasma in vitro. APTT response expressed as ratio (APTTof heparinized plasma/APTT of plasma without heparin).Three different reagents and methods shown. (Slightlymodified, from Thomson JM (ed) 1985 Blood coagulationand haemostasis. A practical guide. ChurchillLivingstone, Edinburgh, p 370, with the permission ofthe editor and the publisher.)
F06660-Ch18.qxd 2/24/06 3:36 PM Page 472

different results from those obtained when normalplasma is “spiked” with heparin. Regression analysisis used to determine the normal range, and a betterfit may be obtained using logarithmically transformedAPTT values.
Heparin Monitoring at the Bedside13
The whole blood activated clotting time (ACT) isroutinely used to assess heparin effects duringcardiac surgery. However, the ACT is not a specificassay for heparin and may be influenced by severalother factors such as hypothermia, haemodilution,and platelet dysfunction. For these reasons the ACTmay be misleading with regard to the properadministration of heparin and protamine.
PrincipleThe ACT is determined by using one of severaldifferent clotting cascade activators, such as kaolinor celite (diatomaceous earth activator), and a methodof end-point detection such as optical or electro-magnetic. No additional phospholipid is added.
ACT monitors include the Hemochron ACTmonitors (International Technidyne, Inc, Edison, NJ),and the HemoTec Automated Coagulation Timer(HemoTec, Inc., Englewood, CO). The Hemochron ACTmonitor uses 2.0 ml of whole blood in glass tubeswith celite. The HemoTec ACT monitor uses 0.8 mlof whole blood in dual-chamber, high-range kaolincartridges. The ACT is thus primarily a system withlittle laboratory involvement.
Anti-Xa Assay for Heparin
Principle Plasma anti-Xa activity as a result of antithrombinis enhanced by the addition of heparin, and either acoagulation or amidolytic (chromogenic) assay ofanti-Xa activity can be adapted to measure thiseffect. A standard curve is constructed by addingvarying amounts of heparin to a normal plasmapool, which provides the source of the antithrombin.A known amount of Xa is added and after incuba-tion, the amount of Xa remaining is assayed bychromogenic or coagulation-based assay. A numberof commercial kits such as Heptest and Hepaclot, aswell as various kits based on chromogenic substrates,are in use and give linear and reproducible responses.
A standard curve should be constructed that isappropriate for the level of heparin expected. Somebut not all assays add an exogenous source ofantithrombin to the test sample, but it is not clearhow important this is in patients with lowantithrombin levels.
Chromogenic MethodThe assay is performed as instructed with the kit.The concentration of heparin is read off a standardcurve constructed according to the manufacturer’sinstructions.
Clotting Method
Principle The anti-Xa activity of antithrombin III is enhancedby the addition of heparin. The inhibition of factorXa by heparin is measured in a modified factor-Xassay.
ReagentsPooled normal plasma. From 20 normal donors.Patient’s plasma. Citrated platelet-poor plasma
(PPP) should be collected between 2 and 4 hoursafter the injection of heparin; it should be testedas soon as possible after the collection and keptat 4°C or on crushed ice until tested.
Buffer. Trisodium citrate 30 vol, glyoxaline buffer(p. 398) 150 volumes, and 20% bovine albumin 1 volume.
Commercially prepared artificial factor X deficientplasma. Reconstitute according to instructions.
Platelet substitute. Mix equal volumes of factor Xdeficient plasma and platelet substitute. This isthe working reagent and is kept at 37°C.
Factor Xa. Reconstitute as instructed by themanufacturer. Dilute further in the buffer to givea 1 in 100 dilution. Keep on crushed ice untilused.
Heparin. 1000 iu/ml. Dilute in 9 g/l NaCl to 10 iu/ml.Ideally, the same batch of heparin as the patientis receiving should be used.
CaCl2. 0.025 mol/l.
MethodA standard curve is constructed as shown in Table18.4. Add 0.05 ml of each dilution to 0.45 ml of thenormal plasma pool. This will give final concentra-
47318 Laboratory control of anticoagulant, thrombolytic, and antiplatelet therapy
F06660-Ch18.qxd 2/24/06 3:36 PM Page 473

tions of heparin from 0.05 to 0.30 iu/ml in 0.05 iusteps.
Pipette 0.3 ml of diluted factor Xa into a largeglass tube at 37°C.
Add 0.1 ml of the first standard dilution. Start the stopwatch. At 1 min and 30 s exactly transferduplicate 0.1 ml volumes of the mixture into twotubes each containing 0.1 ml of prewarmed CaCl2.
At 2 min after subsampling add 0.2 ml of themixture of factor X deficient plasma and plateletsubstitute, start the stopwatch, mix, and record theclotting time.
Repeat for each dilution of standard. The patient’ssample is tested undiluted in pooled normal plasmaif the clotting time is longer than the times used toconstruct the standard curve.
CalculationPlot the clotting times against the heparin concen-tration on log-linear graph paper, with the clottingtimes on the linear axis. The concentration ofheparin in the patient’s sample can be read directlyfrom the standard curve. It is multiplied by thedilution factor if necessary.
Protamine Neutralization Test
PrincipleThis test is an extension of the TT, various amountsof protamine sulphate being added to the plasmabefore the addition of thrombin. When all theheparin present in plasma has been neutralised, the
clotting time should become normal. The concen-tration of heparin in the plasma can be calculatedfrom the amount of protamine sulphate required toproduce this effect. The protamine neutralisationtest is used mainly to calculate the dose of pro-tamine sulphate needed to neutralise circulatingheparin after cardiopulmonary surgery andhaemodialysis, but it is also used to controltreatment or to calculate the dose of protamine to beadministered if the patient needs rapid reversal ofheparinisation.
ReagentsProtamine sulphate. Prepare dilutions (0–50 mg/ml) in barbitone buffer,pH 7.4. Dilute 5 ml of protamine sulphate (10 g/l) 1 in 20 with buffer to give 1 dl of a stock solutioncontaining 500 μg/ml. Then make working solutionsto cover the range of 0–500 μg/ml in 50 μg stepsfrom the stock solution by dilution with buffer. Thesolutions keep indefinitely at 4°C.
Thrombin. Dilute thrombin in barbitone buffer to a concen-tration of about 20 NIH u/ml. Adjust the concen-tration so that 0.1 ml of thrombin clots 0.2 ml ofnormal plasma at 37°C in 10 ± 1 s. Keep thethrombin in a plastic tube in melting ice during theassay.
Plasma. Citrated PPP from the patient.
MethodPlace 0.2 ml of test plasma and 20 μl of barbitonebuffer in a glass tube kept in a waterbath at 37°C.Allow the mixture to warm and then add 0.1 ml ofthrombin. Record the clotting time. If this is c 10 s,there is no demonstrable heparin in the plasma. If theTT is prolonged, repeat the test using 20 μl of the 500μg/ml protamine solution instead of buffer. Repeat thetest if necessary, until a concentration of protamine isfound that gives a clotting time of c 10 s.
CalculationIf 20 μl of 150 μg/ml protamine sulphate produce anormal TT (whereas the clotting time is prolongedwith 100 μg/ml protamine), then the concentrationof 15 μg of protamine is sufficient to neutralise the
474 PRACTICAL HAEMATOLOGY
Table 18.4 Preparation of a standard curve for ananti-Xa assay
Tube
Reagent 1 2 3 4 5 6
Heparin (10 iu/ml) 0.05 0.10 0.15 0.20 0.25 0.30
Saline (ml) 0.95 0.90 0.85 0.80 0.75 0.70
Concentration ofheparin (iu/ml) 0.5 1.0 1.5 2.0 2.5 3.0
Final conc. of 0.05 0.10 0.15 0.20 0.25 0.30heparin after addition to normal plasma pool
F06660-Ch18.qxd 2/24/06 3:36 PM Page 474

heparin in 1 ml of plasma. Assuming weight-for-weight neutralisation, the patient’s plasmacontains 15 μg of heparin per ml or 1.5 iu, assumingthat 1 mg of heparin is equivalent to 100 iu. Thisfigure can be further converted to concentration of heparin per ml of whole blood by multiplying by 1 – PCV.
In the previous example, for in vivo neutralisationof heparin by protamine sulphate, assuming a totalblood volume of 75 ml per kg body weight, therequired dose of protamine would be as follows:
15 × 75 × body weight × (1 – PCV) mg1000 mg
Heparin-Induced Thrombocytopenia
Most patients receiving unfractionated heparinexperience a small and immediate drop in theirplatelet count. This is referred to as type I HIT(heparin-induced thrombocytopenia) and is com-pletely harmless. It is thought to arise as a result ofheparin binding to platelets. A second more seriousthrombocytopenia (type II HIT) is seen in approxi-mately 5% of patients receiving UFH and is a resultof development of antibodies against heparin-PF4complexes. These bind to and activate platelets viathe FCRγII, resulting in accelerated clearance. TypeII HIT develops 5–12 days after starting heparintherapy and causes a profound decrease in plateletsto <50% of preheparin value and usually <50 ×109/l. The process of activation sometimes results inarterial and venous platelet thrombus formationparticularly in patients who are ill or septic, and skinnecrosis has also been reported. This syndrome ofheparin-induced thrombocytopenia and thrombosis(HITT) has a high mortality. Heparin must bestopped immediately, and alternative immediate-acting anticoagulation must be instituted.14
The diagnosis of HIT is primarily clinical, andthere is no test that can be performed with sufficientspeed, sensitivity, and specificity to be of use inmaking the primary decision to stop heparin. How-ever, confirmatory information is useful and anumber of tests can be performed to substantiatethe diagnosis.15 These may be either functional testsin which platelet activation is detected or immuno-logical tests in which the presence of PF4-heparindependent antibodies are detected. Examples of the
former include what is regarded as the “goldstandard” test, the serotonin release assay,16 but thisis too cumbersome and inconvenient for routineuse. Alternatives are heparin-induced plateletaggregation and flow cytometry–based tests.17,18 Thesimplest for routine use is a modified plateletaggregation test as described in the followingsection. Immunological tests, including enzyme-linked immunosorbent assay (ELISA), which is alsoa particle gel immunoassay.19 Although theimmunological tests appear to have greatersensitivity and are more easily reproducible, they donot demonstrate the functional significance of theantibodies.
Heparin-Induced Thrombocytopenia: Detectionby Platelet AggregationAddition of heparin to the patient’s PPP results inheparin/PF4 complexes that are bound by thepathological antibody. The antibody–heparin/PF4complexes then bind to and activate the platelets.Platelet activation is detected as aggregation.
Principle Blood is centrifuged gently to obtain platelet richplasma (PRP), which is stirred in a cuvette at 37°C,between a light source and a photocell.
ReagentsNormal Control Platelet Rich Plasma (PRP)Preferably blood group O or the same group as thepatient should be used. For method see page 427. A platelet count is performed on the PRP. The numberof platelets will influence aggregation response ifthe count falls outside a range of 200–400 × 109/l.If necessary the PRP is adjusted to give a plateletcount of 300 × 109/l by diluting with control plateletpoor plasma (PPP).
Patient and normal control PPP is obtained bycentrifuging at 2000 g for 20 min. Check that theplatelet count is zero.
HeparinA sample of the type (batch identical) of heparinpreviously given to the patient is required. Theheparin is diluted to give working concentrations of10 and 20 u/ml (final concentration of 1.0 and 2.0 u/ml).
47518 Laboratory control of anticoagulant, thrombolytic, and antiplatelet therapy
F06660-Ch18.qxd 2/24/06 3:36 PM Page 475

MethodFollowing the scheme shown in Table 18.5, fouraggregation cuvettes are set up. Add 300 µl ofnormal PRP to each cuvette. Then add 200 µl of theappropriate patient or control PPP, along with amagnetic stir bar. Set the 100% baselines with thenormal control PPP and the 0% baselines with PRPand PPP. Set the stir rate at 1200 rev/min. Observethe baselines for 1 min. Initiate aggregation by theaddition of 50 µl of either heparin or saline. Observeaggregation for a minimum of 15 min (Fig. 18.5).
Interpretation1. If aggregation is observed in cuvette 4 with a
final heparin concentration of 1.0 and 2.0 u/ml,the test is repeated using normal platelets,patient plasma, and a final heparin concentrationof 0.2 u/ml.
2. Aggregation observed in cuvette 4 only, withsubsequent demonstration of heparin at a finalconcentration of 0.2 u/ml, is considered positivefor heparin-induced platelet aggregation.Alternatively, aggregation can be repeated with amuch higher final concentration of heparin (10 u/ml). Inhibition of aggregation is suggestiveof heparin-induced platelet aggregation.
3. Aggregation observed in cuvette 4 withoutdemonstration of aggregation with the lower con-centration of heparin is considered questionable.
4. Aggregation observed in cuvettes 1, 2, or 3 indi-cates that the reaction may be a result of some-
thing other than heparin-induced platelet aggre-gation and the test is repeated using differentnormal donor platelets and control PPP.
With experience subjective assessment of aggre-gation responses is usually sufficient for clinicalinterpretation. A positive test result is shown inFigure 18.5. The total amount of aggregation seenmay be reported.
Technical ProblemsSee platelet aggregation (p. 427).
The literature suggests that test sensitivity can beimproved by the use of the patient’s own platelets,platelets from selected donors known to be reactive inthe assay, or washed platelets. The reactivity of thedonor platelets can be established by using a knownpositive serum. Test specificity may be enhanced bythe use of two point assays that include neutralisationof the reaction by a high dose of heparin.
Detection by Diamed Heparin-PF4 AntibodyTestThe Diamed Heparin-PF4 antibody test is a particlegel immunoassay consisting of red-coloured polymerparticles coated with Heparin-PF4 complex. Whenthe patient’s serum is mixed with the polymer
476 PRACTICAL HAEMATOLOGY
Black Green Red Blue
Normal control PRP 300 µl 300 µl 300 µl 300 µl
Patient PPP None 200 µl None 200 µl
Normal control PPP 200 µl None 200 µl None
Heparin (10 or 20u/ml) None None 50 µl 50 µl
Saline (0.85%) 50 µl 50 µl None None
100
50
0
0 100 200 300 400 500 600 700 800 900 1000 1100 1200
Figure 18.5 The combinations of platelets, plasma, andheparin required to test for heparin-inducedthrombocytopenia shown in Table 18-5. The aggregationtraces show that platelet aggregation occurs only whenthe patient plasma is exposed to heparin (blue trace).
Table 18.5 The combinations of platelets, plasma,and heparin required to test for heparin-inducedthrombocytopenia
Cuvette 1 Cuvette 2 Cuvette 3 Cuvette 4
Normal control 300 μl 300 μl 300 μl 300 μlPRP
Patient PPP None 200 μl None 200 μl
Normal control 200 μl None 200 μl NonePPP
Heparin (10 or None None 50 μl 50 μl20 iu/ml)
Saline (0.85%) 50 μl 50 μl None None
PRP, platelet-rich plasma; PPP, platelet-poor plasma.
F06660-Ch18.qxd 2/24/06 3:36 PM Page 476

particles, specific antibodies react with the Heparin-PF4 complex on the particle surface, resulting inparticle agglutination. The particles are centrifugedthrough a gel filtration matrix, agglutinated particlesare trapped on top of the gel or within the gel, andnonagglutinated particles form a button at thebottom of the tube. The result can be read visually.
Hirudin
Recombinant manufactured hirudin is now availableand licensed for both prophylactic and therapeuticuse in some indications. It is a direct thrombininhibitor and is given intravenously or subcuta-neously. It is most easily monitored using the APTTwith the same target range as for heparin. The TTmay be prolonged and will be corrected usingReptilase. An alternative measure is the Ecarinclotting time. This is thought to be more accurate athigh doses of hirudin but may give falsely highresults when the amount of prothrombin in thesample is reduced below 50%. It is also useful whenother factors such as antiphospholipid antibodiesare causing prolongation of the APTT.
After 5 days therapy 45% of patients will developantihirudin antibodies, which may enhance orreduce the therapeutic effect. Hirudin is excreted viathe kidneys, and close monitoring is necessary, withdose reduction if renal impairment is present.
THROMBOLYTIC THERAPY
The thrombolytic agents currently in use areprincipally streptokinase and recombinant tissuetype plasminogen activator (rtPA). Tenectplase andReteplase are genetically modified forms of tPA.
StreptokinaseStreptokinase is a purified fraction of the filtratefrom cultures of Streptokinase haemolyticus. Strep-tokinase interacts with plasminogen or plasmin toform a plasminogen activator in plasma. The activatorcomplex in turn cleaves a bond in the plasminogenmolecule to give rise to free plasmin. Streptokinasetherefore results in systemic fibrinogenolysis as wellas lysis of fibrin clot. Streptokinase is a foreignprotein and induces antibody production inhumans, limiting a course of treatment to 3–5 days.
It is recommended that 2 years should elapse beforerepeated administrations of streptokinase. It alsocrossreacts with antistreptococcal antibodies, whichmay cause resistance to therapy, although this isusually overcome with large doses.
Tissue-Type Plasminogen Activator The tissue-type plasminogen activator is a single- ordouble-chain polypeptide obtained by recombinanttechniques or from tissue cultures. It is a potentactivator of plasminogen when the two moleculesare bound to fibrin for which it has a strong affinity.It thus causes less systemic fibrinogenolysis thanany of the previously mentioned agents, althoughsome decrease in circulating fibrinogen does occur,particularly with prolonged administration. Itinduces a thrombolytic state of longer duration thaneither streptokinase or urokinase infusion.
Selection of PatientsThrombolytic treatment carries a serious risk ofbleeding, and thrombolytic agents should not begiven to individuals suffering from a variety ofillnesses where there is a high risk of bleeding. Inaddition, each patient should have haemostaticfunction and platelet count measured beforetreatment is started.
Laboratory Control of Thrombolytic Therapy20
Many laboratory tests are abnormal during throm-bolytic therapy, but a perfect and specific procedurefor monitoring is not available. In practice,thrombolytic therapy is given rapidly according toprotocol, with no time or need for adjustment ofdosage. During thrombolytic therapy all screeningtests of coagulation are prolonged, reflecting thehyperplasminaemic state with the reduction in thefibrinogen concentration and the presence of FDP.The prolongation is most marked with streptokinaseand streptokinase–plasminogen complex; it is lessmarked with urokinase and least with tPA. Thefibrinogen concentration commonly decreases tobelow 0.05 g/l, and the FDP concentration mayincrease to more than 1000 ng/l.
Monitoring of therapy is only recommended fortreatment lasting longer than 24 hours. If possible,a sample should be obtained prior to treatment.Samples taken after fibrinolysis has begun should
47718 Laboratory control of anticoagulant, thrombolytic, and antiplatelet therapy
F06660-Ch18.qxd 2/24/06 3:36 PM Page 477

be taken into citrate plus an inhibitor of fibrinolysissuch as aprotinin (250 u/ml) or ε-aminocaproic acid(EACA: 0.07 mol/l). The fibrinolytic state will affectseveral tests.
Activated Partial Thromboplastin TimeWith effective fibrinolysis the APTT is likely to beprolonged >1.5 times control. This is a result offibrinogen, FV and FVIII depletion, and interferencefrom FDPs. There are, however, no data to correlateAPTT with therapeutic effect.
Thrombin Time The TT can be used to monitor therapy. A few hoursafter the start of the infusion, the TT is prolonged to40 s or more (control 15 ± 1 s); it then settles toapproximately 20–30 s. Very long TTs carry a highrisk of bleeding and are indicative of severehyperplasminaemia.
Plasma Fibrinogen Depending on duration of therapy and the specificplasminogen activator used, there is a variabledecrease in fibrinogen. The fibrinogen should bemeasured by a method dependent on clottablefibrinogen (e.g., Clauss technique, p. 401). The PT-derived fibrinogen is likely to be unreliable.Fibrin(ogen) degradation products will be elevated,but this is unlikely to be helpful.
Investigation of a Patient Who BleedsWhile Taking Thrombolytic Agents orImmediately Afterward
Haemorrhage is an inevitable risk associated withfibrinolytic therapy and may occur despite normalcoagulation tests. When severe, bleeding will neces-sitate cessation of fibrinolysis and administration ofaprotinin or tranexamic acid to inhibit its activity.Coagulation tests may guide replacement therapywith plasma or cryoprecipitate. The tests, the timing,and the likely mechanism of bleeding are shown inTable 18.5.
ANTIPLATELET THERAPY
Many drugs inhibit platelet function in vitro, butonly a few have antiplatelet activity in acceptable
doses. Each category of drugs has a different phar-macological action and requires different methodsto demonstrate its effect on platelets. Antiplateletagents are used in primary and secondary preven-tion of coronary heart disease, in unstable angina, incertain forms of cerebrovascular disease, to preventthrombo-embolism associated with valvular diseaseand prosthetic heart valves, and to preventthrombosis in arteriovenous shunts. Haematologistsare only rarely asked to monitor these aspects ofantiplatelet therapy. Indeed, it is said that theadvantage of these agents is that monitoring isunnecessary.
Interest has been revived in the observation thatsome patients do not respond to aspirin. “Aspirinresistance” is poorly defined and may refer either toa failure to inhibit platelet function or a failure tosuppress thromboxane A2 production. The formermay be detected by platelet function analysers suchas the PFA100 or by platelet aggregation responses;the latter may be detected by serum thromboxaneB2 levels. However, the clinical utility of thisassessment and the appropriate responses are notestablished.21
A proportion of patients with thrombocytosis orthrombocythaemia experience episodes of arterialthrombosis. Such patients are often prescribed anti-platelet drugs, and the effect of these drugs issometimes monitored. Three techniques are availablefor monitoring: prolongation of the bleeding time orPFA (p. 417), inhibition of platelet aggregationresponse to standard agonists (p. 427), andnormalization of platelet survival using 111indium-labelled platelets (p. 376).
REFERENCES
1. Hirsh J, Dalen JE, Anderson DR, et al 1998 Oralanticoagulants: mechanism of action, clinicaleffectiveness, and optimal therapeutic range. Chest114:445s–469s.
2. World Health Organization 1999 Guidelines forthromboplastins and plasma used to control oralanticoagulant therapy. WHO Technical ReportSeries 889:64–93.
3. World Health Organization 1999 Guidelines forthromboplastins and plasma used to control oralanticoagulant therapy. WHO Technical ReportSeries 889:Annex 3.
478 PRACTICAL HAEMATOLOGY
F06660-Ch18.qxd 2/24/06 3:36 PM Page 478

4. Kitchen S, Preston FE 1999 Standardization ofprothrombin time for laboratory control of oralanticoagulant therapy. Seminars ThrombosisHemostasis 25:17–25.
5. Poller L, Barrowcliffe TW, van den Besselaar AM, et al 1997 A simplified statistical method for localINR using linear regression. European ConcertedAction on Anticoagulation [see comments]. BritishJournal of Haematology 98:640–647.
6. Guidelines on oral anticoagulation, 3rd ed 1998.British Journal of Haematology 101:374–387.
7. Hirsh J, Dalen J, Anderson DR, et al 2001 Oralanticoagulants: mechanism of action, clinicaleffectiveness, and optimal therapeutic range. Chest119:8S–21S.
8. Shiach CR, Campbell B, Poller L, et al 2002Reliability of point-of-care prothrombin timetesting in a community clinic: a randomizedcrossover comparison with hospital laboratorytesting. British Journal of Haematology119:370–375.
9. Murray ET, Fitzmaurice DA, McCahon D 2004 Pointpf care testing for INR monitoring: where are wenow? British Journal of Haematology 127:373–378.
10. Fitzmaurice D, Murray ET, Gee KM, et al 2002Training of patients in a randomised controlledtrial of self management of warfarin treatment.British Medical Journal 328:437–438.
11. Hirsh J, Warkentin TE, Raschke R, et al 1998Heparin and low-molecular-weight heparin:mechanisms of action, pharmacokinetics, dosingconsiderations, monitoring, efficacy, and safety[published erratum in Chest 1999 Jun;115(6):1760].Chest 114:489s–510s.
12. Gray E, Heath AB, Mulloy B, et al 1995 Acollaborative study of proposed European
Pharmacopoeia reference preparations of lowmolecular mass heparin. Thrombosis andHaemostasis 74:893–899.
13. Popma JJ, Prpic R, Lansky AJ, et al 1998 Heparindosing in patients undergoing coronaryintervention. American Journal of Cardiology82:19–24.
14. Warkentin TE 2003 Heparin-inducedthrombocytopenia: pathogenesis and management[see comment]. British Journal of Haematology121:535–555.
15. Chong BH 2003 Heparin-inducedthrombocytopenia. Journal of Thrombosis &Haemostasis 1:1471–1478.
16. Sheridan D, Carter C, Kelton JG 1986 A diagnostictest for heparin-induced thrombocytopenia. Blood67:27–30.
17. Warkentin TE 1999 Heparin-inducedthrombocytopenia: a clinicopathologic syndrome.Thrombosis and Haemostasis 82:439–447.
18. Amiral J, Meyer D 1998 Heparin-inducedthrombocytopenia: diagnostic tests and biologicalmechanisms. Baillieres Clinical Haematology11:447–460.
19. Meyer O, Salama A, Pittet N, et al 1999 Rapiddetection of heparin-induced platelet antibodieswith particle gel immunoassay (ID-HPF4). Lancet354:1525–1526.
20. Ludlam CA, Bennett B, Fox KA, et al 1995Guidelines for the use of thrombolytic therapy.Haemostasis and Thrombosis Task Force of theBritish Committee for Standards in Haematology.Blood Coagulation & Fibrinolysis 6:273–285.
21. Patrono C 2003 Aspirin resistance: definition,mechanisms and clinical read-outs [see comment].Journal of Thrombosis & Haemostasis 1:1710–13.
47918 Laboratory control of anticoagulant, thrombolytic, and antiplatelet therapy
F06660-Ch18.qxd 2/24/06 3:36 PM Page 479