CXCR3, Inflammation, and Autoimmune Diseases
8
CONTEMPORARY CHALLENGES IN AUTOIMMUNITY CXCR3, Inflammation, and Autoimmune Diseases St´ ephanie Lacotte, Susana Brun, Sylviane Muller, and H´ el` ene Dumortier CNRS, Institut de Biologie Mol´ eculaire et Cellulaire, Immunologie et Chimie Th´ erapeutiques, Strasbourg, France CXCR3 is a G protein–coupled, seven-transmembrane receptor that binds and is ac- tivated by the three IFN-γ-inducible chemokines of the CXC family named CXCL9, CXCL10, and CXCL11. These chemokines are not constitutively expressed but are up- regulated in a proinflammatory cytokine milieu. Consequently, their major function is to selectively recruit immune cells at inflammation sites, but they also play a role in angiogenesis mechanisms. In the last few years, strong experimental and clinical evidence has been obtained supporting the idea that the CXCR3 pathway is involved in the development of autoimmune diseases, especially by creating local amplification loops of inflammation in target organs, thereby inducing worsening of clinical manifes- tations. This article briefly reviews what we know today about the nature and functions of CXCR3, with special emphasis on its involvement in two main rheumatic systemic autoimmune diseases, namely rheumatoid arthritis and systemic lupus erythematosus. Key words: CXCR3; IFN-γ-induced chemokines; CXCL9; CXCL10; CXCL11; inflamma- tion; autoimmune disease; rheumatoid arthritis; systemic lupus erythematosus What Is CXCR3? CXCR3 is the unique receptor for three chemokines belonging to the CXC chemokine family (where X is any amino acid and C are two conserved cysteine residues present in the N-terminal part of the molecule), namely CXCL9 (initially called MIG, monokine in- duced by interferon-γ [IFN-γ]), CXCL10 (IP- 10, IFN-γ-inducible protein 10), and CXCL11 (I-TAC, IFN-γ-inducible T cell α chemo- attractant) (see Table 1). A truncated coding sequence of this chemokine receptor was first described in 1995, and the complete cDNA was isolated from a human CD4 + T cell– derived cDNA library by Loetscher and col- leagues in 1996. 1 The corresponding protein Address for correspondence: H´ el` ene Dumortier, Institut de Biologie Mol´ eculaire et Cellulaire, UPR9021, Centre National de la Recherche Scientifique, 15 rue Ren´ e Descartes, 67000 Strasbourg, France. Fax: +33 3 88 61 06 80. [email protected] consists in 368 amino acid residues with a molecular weight of approximately 40 kDa. The mouse CXCR3 is 86% identical to the human protein sequence. 2 Both murine and human CXCR3 genes were mapped to chro- mosome X. More recently, another CXCR3 re- ceptor, called CXCR3-B, was described. 3 It re- sults from an alternative splicing of the CXCR3 mRNA and the predicted encoded protein is 416 amino acids long with an extended NH 2 - terminal domain when compared to the ini- tially described CXCR3 sequence. CXCR3 is a G protein–coupled cell surface receptor (GPCR), and as such, it harbors a seven-transmembrane α-helical structure. The extracellular N-terminal domain contains three loops (named ECL-1–3), which are involved in the binding of the chemokine ligand, ECL-2 being essential for effective receptor activation by all CXCR3 ligands. The intracellular C- terminal domain (also containing three loops) allows signal transduction upon chemokine Contemporary Challenges in Autoimmunity: Ann. N.Y. Acad. Sci. 1173: 310–317 (2009). doi: 10.1111/j.1749-6632.2009.04813.x c 2009 New York Academy of Sciences. 310
Transcript of CXCR3, Inflammation, and Autoimmune Diseases

CONTEMPORARY CHALLENGES IN AUTOIMMUNITY
CXCR3, Inflammation, and AutoimmuneDiseases
Stephanie Lacotte, Susana Brun, Sylviane Muller,and Helene Dumortier
CNRS, Institut de Biologie Moleculaire et Cellulaire, Immunologie et ChimieTherapeutiques, Strasbourg, France
CXCR3 is a G protein–coupled, seven-transmembrane receptor that binds and is ac-tivated by the three IFN-γ-inducible chemokines of the CXC family named CXCL9,CXCL10, and CXCL11. These chemokines are not constitutively expressed but are up-regulated in a proinflammatory cytokine milieu. Consequently, their major functionis to selectively recruit immune cells at inflammation sites, but they also play a rolein angiogenesis mechanisms. In the last few years, strong experimental and clinicalevidence has been obtained supporting the idea that the CXCR3 pathway is involvedin the development of autoimmune diseases, especially by creating local amplificationloops of inflammation in target organs, thereby inducing worsening of clinical manifes-tations. This article briefly reviews what we know today about the nature and functionsof CXCR3, with special emphasis on its involvement in two main rheumatic systemicautoimmune diseases, namely rheumatoid arthritis and systemic lupus erythematosus.
Key words: CXCR3; IFN-γ-induced chemokines; CXCL9; CXCL10; CXCL11; inflamma-tion; autoimmune disease; rheumatoid arthritis; systemic lupus erythematosus
What Is CXCR3?
CXCR3 is the unique receptor for threechemokines belonging to the CXC chemokinefamily (where X is any amino acid and Care two conserved cysteine residues present inthe N-terminal part of the molecule), namelyCXCL9 (initially called MIG, monokine in-duced by interferon-γ [IFN-γ]), CXCL10 (IP-10, IFN-γ-inducible protein 10), and CXCL11(I-TAC, IFN-γ-inducible T cell α chemo-attractant) (see Table 1). A truncated codingsequence of this chemokine receptor was firstdescribed in 1995, and the complete cDNAwas isolated from a human CD4+ T cell–derived cDNA library by Loetscher and col-leagues in 1996.1 The corresponding protein
Address for correspondence: Helene Dumortier, Institut de BiologieMoleculaire et Cellulaire, UPR9021, Centre National de la RechercheScientifique, 15 rue Rene Descartes, 67000 Strasbourg, France. Fax: +333 88 61 06 80. [email protected]
consists in 368 amino acid residues with amolecular weight of approximately 40 kDa.The mouse CXCR3 is 86% identical to thehuman protein sequence.2 Both murine andhuman CXCR3 genes were mapped to chro-mosome X. More recently, another CXCR3 re-ceptor, called CXCR3-B, was described.3 It re-sults from an alternative splicing of the CXCR3mRNA and the predicted encoded protein is416 amino acids long with an extended NH2-terminal domain when compared to the ini-tially described CXCR3 sequence.
CXCR3 is a G protein–coupled cell surfacereceptor (GPCR), and as such, it harbors aseven-transmembrane α-helical structure. Theextracellular N-terminal domain contains threeloops (named ECL-1–3), which are involved inthe binding of the chemokine ligand, ECL-2being essential for effective receptor activationby all CXCR3 ligands. The intracellular C-terminal domain (also containing three loops)allows signal transduction upon chemokine
Contemporary Challenges in Autoimmunity: Ann. N.Y. Acad. Sci. 1173: 310–317 (2009).doi: 10.1111/j.1749-6632.2009.04813.x c© 2009 New York Academy of Sciences.
310

Lacotte et al.: CXCR3 in Autoimmunity 311
TABLE 1. Roles of CXC Chemokine Receptors and their Ligands
Receptor Other Names Ligands Presumed Functions
CXCR1 IL8RA, CD128,CD181, CDw128a,IL8R1
CXCL6, CXCL8 Neutrophil recruitment, cell proliferation and inhibitionof apoptosis, negative regulation of myeloid progenitorcells
CXCR2 IL8RB, CD182,CDw128b, IL8R2
CXCL1, CXCL2,CXCL3, CXCL5,CXCL6, CXCL7,CXCL8
Neutrophil recruitment, angiogenesis, macrophagerecruitment, cell proliferation, and inhibition ofapoptosis
CXCR3-A CD182, GPR9 CXCL9, CXCL10,CXCL11
Th1 response, angiostasis, leukocyte recruitment,inflammation, integrin activation, cytoskeletalchanges, and chemotactic migration
CXCR3-B CD182, GPR9 CXCL4, CXCL9,CXCL10, CXCL11
CXCR4 NPYR, CD184,Fusin, HM89,LCR1, LESTR
CXCL12 Organogenesis, lymphopoiesis, hematopoiesis, cellmigration and survival, angiogenesis
CXCR5 BLR1, CD185,MDR15
CXCL13 B-cell migration, Th2 response, organogenesis(cooperative with the CCR7 receptor)
CXCR6 CD186, BONZO,STRL33,TYMSTR
CXCL16 Leukocyte migration and adhesion
CXCR7 RDC1, CMKOR1 CXCL11, CXCL12 Scavenger of CXCL12: inversely correlates withCXCR4 activity
recognition, through phosphorylation of ser-ine and threonine residues. The seven trans-membrane domains contain typical structuralmotifs for GPCRs such as the conserved DRYand NPxxY5,6F motifs at the end of the thirdand seventh cytoplasmic domains, respectively.Like all chemokine receptors, CXCR3 is cou-pled to the pertussis toxin–sensitive Gαi proteinand is internalized upon activation by one of itsligands.4 This leads to calcium influx and acti-vation of a signaling cascade involving kinases,such as p44/p42 mitogen-activated protein ki-nase (MAPK) and Akt, and eventually, most ofthe time, cytoskeleton rearrangement and cellmovement.
Physiological Roles of CXCR3 andCXCR3-binding Chemokines
The CXCR3 receptor–ligand system is in-volved in two main biological mechanisms:(1) chemotaxis of immune cells and (2) an-giogenesis. In contrast to the constitutive
chemokines, the role of which is to orches-trate the homeostatic immune cell traffick-ing during hematopoiesis and immune surveil-lance, the three ligands for CXCR3, namelyCXCL9, CXCL10, and CXCL11, are respon-sible for the recruitment of immune cells at in-fection/inflammation sites. These functions aredirectly correlated to the expression patternsof both the CXCR3 receptor and the cognatechemokines.
Recruitment of Immune Cells
CXCR3 has been reported to be expressedon several immune cell types, among whichare natural killer (NK) cells, plasmacytoidand myeloid dendritic cells, B cells, and,especially, activated T cells. Indeed, the initialcloning data obtained from a human CD4+ Tlymphocyte cDNA library, unambiguously in-dicated that CXCR3 is expressed by such cells.This was further confirmed and extended byseveral groups. Thus, Sallusto and coworkersdemonstrated that CXCR3 is preferentially

312 Annals of the New York Academy of Sciences
expressed by Th1-polarized activated/memoryT cells, whereas Th2 cells bear receptors suchas CCR4 and CCR8, although this di-chotomy might finally not be so clear cut.5
Moreover, CXCR3 expression on T cellshas been shown to require their activationthrough a nonpersistent T-cell receptor (TCR)triggering in the presence of IFN-γ. Veryinterestingly, the three major CXCR3-bindingchemokines are induced in a wide variety ofcells by the typical Th1-associated cytokineIFN-γ. This suggests that there is an am-plification loop of Th1 immune responsesbetween Th1 cells, which produce IFN-γ,and immune/endothelial/epithelial cells,which produce CXCR3-binding chemokinesin response to this cytokine, thereby attractingmore CXCR3-expressing Th1 cells at the samesite and amplifying the ongoing Th1 response.It should be mentioned that, in addition tothis chemotactic property, it has been stronglysuggested that CXCR3-binding chemokines(especially CXCL10) also directly participatein the regulation of T cell responses since theyare able to modulate T cell proliferation inresponse to an antigenic challenge and theyfavor Th1-type cytokine production whiledown-regulating Th2 cytokines.6 Of note,CXCL4, which is expressed by activatedplatelets, has been recently shown to signalthrough the CXCR3-B variant of the receptorand to mediate leukocyte recruitment.
Angiogenesis
Inhibition of angiogenesis is the second im-portant characteristic function of CXCR3-binding chemokines, as of all CXC chemokinesthat do not contain the Glu-Leu-Arg (ELR)sequence next to the CXC motif.7 This an-giostatic effect is mainly mediated by the in-teraction of the cognate chemokines with thealternatively spliced variant of the receptor,namely CXCR3-B, and the subsequent activa-tion of the p38MAPK pathway. Accordingly, theCXCR3-B receptor has been detected on hu-man microvascular endothelial cells only when
they are in a proliferative stage, and its ex-pression can be either constitutive or vari-able, depending on the type of blood vesseland on the environment (healthy or inflam-matory/neoplastic). A role for CXCR3 andits ligands in inhibition of angiogenesis hasbeen demonstrated in the regulation of tumorgrowth as well as in mechanisms of tissue repairand wound healing.
Contribution of CXCR3 andCXCR3-binding Chemokines to the
Pathogenesis of InflammatoryDisorders
As mentioned above, the CXCR3 receptorand its ligands are responsible for the recruit-ment of circulating activated immune cells inareas where inflammation occurs. Although es-sential for effective host defense against infec-tions, such a mechanism may also contributeto the induction and exacerbation of chronicinflammatory reactions classically associated tograft rejection or allergic and autoimmune dis-eases, for example. A large body of experimen-tal data and clinical observations that seem toconfirm this hypothesis has been obtained re-cently. Most of these studies analyze the ex-pression of CXCR3-binding chemokines andof CXCR3 itself in inflamed tissues, trying tocorrelate the information obtained with clini-cal parameters. Another approach consists instudying the consequences of an inhibition ofthe CXCR3 pathway by means of blocking an-tibodies or by using CXCR3–/– mice. For exam-ple, patients with high serum levels of CXCL10before transplantation are more prone to acuteTh1-mediated rejection, and long-term admin-istration of neutralizing anti-CXCR3 antibod-ies leads to the inhibition of alloreactive T cell–mediated graft-versus-host disease in a mousemodel.8 High levels of CXCR3 were shownto be expressed in brain samples from patientswith multiple sclerosis, and CXCL10 serum lev-els are raised during the active phase of thedisease. Detailed information on the complex

Lacotte et al.: CXCR3 in Autoimmunity 313
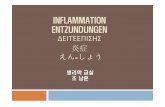
Figure 1. Amplification of inflammation through the CXCR3 pathway in SLE and RA. When an autoim-mune response develops, Th1 cytokines, including IFN-γ, induce CXCR3 expression on lymphocytes anddendritic cells in lymphoid organs. These cells then acquire the capacity to migrate toward inflammatorychemokines (CXCL9, CXCL10, and CXCL11), which are produced by resident cells (such as fibroblasts) insynovial tissue (RA) or skin and kidneys (SLE). Once recruited from the blood in the inflamed organs, thesecells (especially Th1 cells) stimulate resident cells to increase chemokine production, via IFN-γ secretion. Thiscreates an amplification loop responsible for sustaining inflammation in autoimmune diseases.
roles of CXCR3 and its ligands in inflamma-tory/autoimmune disorders affecting the cen-tral nervous system can be found in the reviewby Liu and collaborators.9 Involvement of theCXCR3 pathway has also been described in au-toimmune endocrine diseases such as Graves’disease and type 1 diabetes mellitus (see re-view by Rotondi and colleagues10). The nextparagraphs will focus on the currently avail-able data about the role of CXCR3 and cognatechemokines in two systemic rheumatic autoim-mune diseases, rheumatoid arthritis (RA) andsystemic lupus erythematosus (SLE) (schemati-cally summarized in Fig. 1).
CXCR3 in RA
Results of studies mainly performed on hu-man samples (peripheral blood, synovial fluid,and synovial tissue) collected from RA patientshave provided an overall idea of the implica-tion of CXCR3 in this chronic inflammatory
disorder, which mainly affects joints. The in-flamed synovial tissue of RA patients is char-acterized by a massive infiltration of immunecells, among which Th1-type T CD4+ cells arepredominant. CXCR3 and the correspondingchemokines are very likely to mediate the re-cruitment of these cells participating in inflam-mation. Indeed, T cells detected in RA syn-ovial tissues are intensely stained for CXCR3in immunofluorescence studies,11 and 90% ofCD4+ T cells present in the synovial fluid of pa-tients express this receptor. Not only T cells butalso CXCR3-expressing mast cells and plasmacells are present in the infiltrated synovial tis-sue of RA patients. This strongly suggests thatboth cell types may contribute to and sustainthe inflamed state in arthritic lesions. Moreover,compared with osteoarthritis, CXCR3-bindingchemokines are detected in markedly higherconcentrations in RA patients, both in syn-ovial fluid and tissue. Some studies have identi-fied synovial fibroblasts as the main producers

314 Annals of the New York Academy of Sciences
of the three CXCR3-agonistic chemokinesCXCL9, 10, and 11 in response to the syner-gistic effect of IFN-γ and tumor necrosis factor(TNF)α.12 CXCL10 is also increased in thecollagen-induced arthritis mouse model of RA,and interestingly, Kwak and coworkers have re-cently described in this model the existence ofa cross-talk between CXCL10 produced by os-teoclast precursors and receptor activator ofnuclear factor kappaB ligand (RANK-L) ex-pressed by CD4+ T cells present in RA syn-ovium.13 This amplification loop may be cen-tral to inflammation and bone erosion in RA.Finally, reinforcing the idea that the CXCR3pathway plays a major role in joint inflamma-tion occurring in RA, it has been shown thattherapeutic molecules, such as dual inhibitorsof lipoxygenase and cyclooxygenase and TNF-α inhibitors, inhibit the production of CXCR3ligands by synovial fibroblasts and alter the traf-ficking of CXCR3+ T cells, respectively.
CXCR3 in SLE
Not much is known about the role of CXCR3in this chronic inflammatory autoimmune dis-ease in which biological and clinical mani-festations are polymorphic. The presence ofantinuclear autoantibodies such as anti-double-stranded DNA in the serum of lupus patientsis, however, a hallmark of the disease, and skinand kidneys are two frequent target organs ofthe autoimmune response.
The first report on CXCR3 in lupus waspublished in 2001 by Flier and colleagues, whostudied different types of skin inflammation,including chronic discoid lupus erythematosuscharacterized by lymphocytic infiltrates at thedermal–epidermal junction.14 Using skin biop-sies, they showed that CXCR3 is expressedby a majority of the infiltrating CD4+ andCD8+ T cells and that the CXCR3-activatingchemokines are produced locally, suggestingthat they play a significant role in the recruit-ment of T cells in these inflammatory lesions.The same observation was made in severalother types of cutaneous damages associated
with lupus.15 Moreover, the CXCR3 ligandsCXCL9, 10, and 11 were identified as themost abundantly expressed chemokine familymembers in cutaneous lupus erythematosus le-sions, this expression being triggered by UV-induced injury and leading to the skin-homingof CXCR3+ lymphocytes and plasmacytoiddendritic cells.16
Not only in skin lesions, but also in lu-pus nephritis, is the recruitment of leuko-cytes a characteristic feature of tissue injury.Chemokines and their receptors have beenshown to be key contributors to renal inflam-matory disease, and among these molecules,the CXCR3 receptor and cognate ligands arecentral. T cells expressing CXCR3 infiltrate thetubulointerstitium in renal biopsies of patientswith lupus nephritis, and there is a correlationbetween the number of infiltrating CXCR3+
cells and the degree of kidney dysfunction.17
Very recently, Enghard and colleagues de-scribed the presence of a high number ofCXCR3-expressing T cells in renal biopsies ofpatients with lupus nephritis, and they high-lighted a clear enrichment of CXCR3+CD4+
T cells in the urine of these patients (as com-pared with peripheral blood).18 Importantly,the number of these urinary T cells seems tobe a valuable marker of nephritis activity. Onthe contrary, it had been shown earlier thatthe numbers of circulating CD4+CXCR3+ Tcells were selectively decreased during SLEflares.19 Additional evidence of a role for theCXCR3 pathway in lupus nephritis came fromthe results of an extensive microarray anal-ysis of glomerular gene expression in lupusMRL/lpr mice.20 Indeed, chemokines andchemokine receptors related to inflammatoryTh1 cell accumulation were up-regulated, in-cluding CXCR3 and its three ligands, CXCL9,10, and 11. Interestingly, prednisolone treat-ment of these animals attenuated this up-regulation together with the amplitude ofthe cellular infiltrate. However, renal diseaseis not suppressed in CXCL10–/– MRL/lprmice, nor are CXCL10–/– C57BL/6 miceprotected from nephrotoxic serum nephritis,

Lacotte et al.: CXCR3 in Autoimmunity 315
which suggests that CXCL10 is not the mainpathogenic chemo-attractant actor in theseexperimental models. This is not the casewhen using CXCR3- or CXCL9-deficient micethat exhibit reduced infiltrated T cells andmacrophages and no obvious kidney disease.21
In lupus patients, raised levels of interferon-inducible inflammatory chemokines (includ-ing the CXCR3 ligands) were detected at themRNA and protein levels in peripheral bloodmononuclear cells and in the plasma/serum,respectively, and a strong correlation could beestablished with the severity of the biologicaland clinical signs of the disease.22,23 From allthese results, it has been suggested that thenumber of urinary T cells or the levels of serumchemokines may serve as convenient biomark-ers for disease activity in lupus.
Most studies mentioned above and per-formed on kidney tissues have focused on Tcells, among which a vast majority expressCXCR3. Interestingly, Eriksson and coworkersalso described an increased surface expressionof CXCR3 on circulating T cells from SLE pa-tients with renal involvement,24 which may sug-gest that they exhibit a lower sensitivity thresh-old to secreted inflammatory chemokines.
If few data are available on CXCR3 andT cells in lupus, even less is known about ex-pression of this receptor on B cells and on theresulting homing of these cells. Regulation ofCXCR3 expression on memory B cells hasmainly been described in the context of regularimmune responses. Henneken and colleaguesnoticed that contrary to RA patients, very fewcirculating (memory) B cells from lupus patientsexpress high levels of CXCR3.25 However arecent paper mentions an increase in the ra-tio of CXCR3+ B cells together with an in-crease in CXCL10 serum levels in patients withSLE.26 These apparently contradictory resultsmay be due to differences in flow cytometryanalyses or to different clinical characteristicsof the selected patients. Finally, very interestinginformation came out from a recent paper byNicholas and colleagues, who showed that, insome SLE patients, a population of circulating
memory B cells, expressing high levels of CD19,is enriched in autoreactivity (anti-Smith anti-gen B cells) and specifically expresses elevatedCXCR3 levels.27 This supports the idea thatthese CD19high autoreactive B cells may mi-grate to sites of inflammation where they canexert pathogenic effects. In our laboratory, wehave shown that histone-specific autoreactiveplasma cells home to inflamed kidneys in lupus(NZBxNZW)F1 mice (Lacotte and collabora-tors, in revision), and we are currently explor-ing the phenotype and migratory capacities ofseveral B cell–plasma cell differentiation stagesin order to improve our understanding of B cellmigration behavior in lupus.
Concluding Remarks
Inflammation is central to the develop-ment of immune responses in normal settings(mounting a response to eradicate pathogens)but also in pathologic settings such as systemicautoimmune disorders, which are character-ized by continuous immune responses towardself-antigens and chronic inflammation. Thereis now accumulating evidence that the complexchemokine network is dysregulated in thesediseases, although many more studies will benecessary to get a thorough understanding ofthe underlying mechanisms. Among the largechemokine and chemokine receptor families,CXCR3 and CXCR3-binding chemokines arelikely to be key players in the maintenance andamplification of the autoimmunity-related in-flammatory processes. Consequently, CXCR3has become an attractive target for the drugdiscovery community, and several families ofmolecules with potential clinical applications,such as specific blocking antibodies, protein-based antagonists, and small chemical com-pounds, have been developed.28 Among thesesynthetic molecules, one has reached a phaseIIa clinical trial for psoriasis, but unfortunatelyit has been withdrawn because of an appar-ent lack of efficacy. This disappointing resultshould hamper neither the huge therapeutic

316 Annals of the New York Academy of Sciences
expectations linked to the CXCR3 chemokinereceptor, nor patients’ hopes.
Due to the length of this chapter, we are un-able to summarize all of the cutting-edge issuesthat surround this research. For this reason, werefer to the following recent literature on thissubject.29–33
Conflicts of Interest
The authors declare no conflicts of interest.
References
1. Loetscher, M. et al. 1996. Chemokine receptor spe-cific for IP10 and mig: structure, function, and ex-pression in activated T-lymphocytes. J. Exp. Med.
184: 963–969.2. Lu, B. et al. 1999. Structure and function of the
murine chemokine receptor CXCR3. Eur. J. Immunol.
11: 3804–3812.3. Lasagni, L. et al. 2003. An alternatively spliced vari-
ant of CXCR3 mediates the inhibition of endothelialcell growth induced by IP-10, Mig, and I-TAC, andacts as functional receptor for platelet factor 4. J. Exp.
Med. 197: 1537–1549.4. Thompson B. et al. 2007. Inhibition of G alpha i2 ac-
tivation by G alpha i3 in CXCR3-mediated signaling.J. Biol. Chem. 282: 9547–9555.
5. Sallusto, F. et al. 1998. Flexible programs ofchemokine receptor expression on human polarizedT helper 1 and 2 lymphocytes. J. Exp. Med. 187:875–883.
6. Gangur, V. et al. 1998. Human IP-10 selectively pro-motes dominance of polyclonally activated and en-vironmental antigen-driven IFN-gamma over IL-4responses. FASEB J. 12: 705–713.
7. Romagnani, P. et al. 2004. CXC chemokines: the reg-ulatory link between inflammation and angiogenesis.Trends Immunol. 25: 201–209.
8. He, S. et al. 2008. A new approach to the blocking ofalloreactive T cell-mediated graft-versus-host diseaseby in vivo administration of anti-CXCR3 neutraliz-ing antibody. J. Immunol. 181: 7581–7592.
9. Liu, L. et al. 2005. Chemokine receptor CXCR3: anunexpected enigma. Curr. Top. Dev. Biol. 68: 149–181.
10. Rotondi, M. et al. 2007. Role of chemokines in en-docrine autoimmune diseases. Endocr. Rev. 28: 492–520.
11. Ruth, J. et al. 2001. Selective lymphocyte chemokinereceptor expression in the rheumatoid joint. Arthritis
Rheum. 44: 2750–2760.
12. Tsubaki, T. et al. 2005. Accumulation of plasma cellsexpressing CXCR3 in the synovial sublining regionsof early rheumatoid arthritis in association with pro-duction of Mig/CXCL9 by synovial fibroblasts. Clin.
Exp. Immunol. 141: 363–371.13. Kwak, H. et al., 2008. Reciprocal cross-talk between
RANKL and interferon-gamma-inducible protein 10is responsible for bone-erosive experimental arthritis.Arthritis Rheum. 58: 1332–1342.
14. Flier, J. et al. 2001. Differential expression ofCXCR3 targeting chemokines CXCL10, CXCL9,and CXCL11 in different types of skin inflammation.J. Pathol. 194: 398–405.
15. Wenzel, J. et al. 2005. Enhanced type I interferonsignalling promotes Th1-biased inflammation in cu-taneous lupus erythematosus. J. Pathol. 205: 435–442.
16. Meller, S. et al. 2005. Ultraviolet radiation-inducedinjury, chemokines, and leukocyte recruitment: Anamplification cycle triggering cutaneous lupus ery-thematosus. Arthritis Rheum. 52: 1504–1516.
17. Segerer, S. et al. 2004. CXCR3 is involved in tubu-lointerstitial injury in human glomerulonephritis. Am.
J. Pathol. 164: 635–649.18. Enghard, P. et al. 2008. CXCR3+CD4+ T cells are
enriched in inflamed kidneys and urine and providea new biomarker for acute nephritis flares in sys-temic lupus erythematosus patients. Arthritis Rheum.
60: 199–206.19. Amoura, Z. et al. 2003. Roles of CCR2 and CXCR3
in the T cell-mediated response occurring during lu-pus flares. Arthritis Rheum. 48: 3487–3496.
20. Teramoto, K. et al. 2008. Microarray analysis ofglomerular gene expression in murine lupus nephri-tis. J. Pharmacol. Sci. 106: 56–67.
21. Menke, J. et al. 2008. CXCL9, but not CXCL10, pro-motes CXCR3-dependent immune-mediated kidneydisease. J. Am. Soc. Nephrol. 19: 1177–1189.
22. Bauer, J. et al. 2006. Elevated serum levels ofinterferon-regulated chemokines are biomarkers foractive human systemic lupus erythematosus. PLoS
Med. 3: e491.23. Lit, L. et al. 2006. Raised plasma concentration
and ex vivo production of inflammatory chemokinesin patients with systemic lupus erythematosus. Ann.
Rheum. Dis. 65: 209–215.24. Eriksson, C. et al. 2003. Abnormal expression of
chemokine receptors on T-cells from patients withsystemic lupus erythematosus. Lupus 12: 766–774.
25. Henneken, M. et al. 2005. Differential expression ofchemokine receptors on peripheral blood B cells frompatients with rheumatoid arthritis and systemic lupuserythematosus. Arthritis Res. Ther. 7: R1001–R1013.
26. Watanabe, T. et al. 2008. Striking alteration ofsome populations of T/B cells in systemic lupus

Lacotte et al.: CXCR3 in Autoimmunity 317
erythematosus: relationship to expression of CD62Lor some chemokine receptors. Lupus 17: 26–33.
27. Nicholas, M. et al. 2008. A novel subset of memoryB cells is enriched in autoreactivity and correlateswith adverse outcomes in SLE. Clin. Immunol. 126:189–201.
28. Wijtmans, M. et al. 2008. Towards small-moleculeCXCR3 ligands with clinical potential. Chem. Med.
Chem. 3: 861–872.29. Kulkarni, O. et al. 2008. Chemokines in lupus nephri-
tis. Front. Biosci. 13: 3312–3320.30. Iwamoto, T. et al. 2008. Molecular aspects of rheuma-
toid arthritis: chemokines in the joints of patients.FEBS J. 275: 4448–4455.
31. Vandercappellen, J. et al. 2008. The role ofchemokines and their receptors in cancer. Cancer Lett.
267: 226–244.32. Loos, T. et al. 2008. Citrullination of CXCL10
and CXCL11 by peptidylarginine deiminase: a nat-urally occurring posttranslational modification ofchemokines and new dimension of immunoregula-tion. Blood 112: 2648–2656.
33. Lee, E. et al. 2009. CXCL10 and autoimmune dis-eases. Autoimmun. Rev. 8: 379–383.