CT Evaluation of Colon Carcinoma:Emphasis on Distant Lymph ...
8
1993; 29 (1) : Journal of Korean Radiological Society, January, 199 3 CT Evaluation of Colon Carcinoma:Emphasis on Distant Lymph N ode Invasion and Liver Metastases Kyung Il Chung , M.D. , Kyoung Sik Cho , M.D. , Moon-Gyu Lee , M.D. , Seung Yeon Bael ‘’ M.D. , Yong Ho Auh , M.D. , Jin Cheon Kim* , M.D. 01 Diagnostic Radiology M edical Center, 01 College 01 - Abstract- Even though the value of computed tomography (CT) used to detect the co lon carcinoma with minim al invasion is limited , its usefulness in the evalu ation of the extent of disease such as hepatic metastasis or dis- tant lymph node invasion has been emphasized. To examine the role of CT in the evalu at ion of colon car- ci noma , CT scans obtained during the past 2 years in 56 patients with surgica ll y proven co lon carcin oma were reviewed and the findings correlated with pathologic results. The sensitivity and acc ur acy of CT for fat infiltration were 86 , 58 and 80% respectively. Those of regional node we re 60 , 83 and 75% a nd distant nod e 67 , 100 and 95 %. Li ver metastases sho wed se nsitivity , specificity a nd accuracy of 83 , 98 , 96% a nd periton eal metastases 67 , 94 and 89% respectivel y. CT detected local invasion with fair degree of acc ur acy but the tru e value of CT li e in the detection of distant inv as ions such as liver and distant lymph node metastases thereby leading to preclusion of unne cessary procedures a nd implementation of a ppropri ate procedures. Index Words: Colon Carcinoma Liver , metastases Lymph Nod e , metastases INTRODUCTION Al most two d ecades have pass ed since CT was first introduc ed. Since then , it has b ee n us ed to d etec t and to stage man y tumors includin g col- on carcinoma , recently join ed by MR imaging , endoscopic sonography , and monoclonal an- tibody imagin g. Many conflicting reports on th e ef fect iv en ess of the various me thods has b ee n published in the literature largely due to prem at ur e conclusions (1). Although the a bov e me thod s help to d etect colon carci nom a , non e has th e capacity to show full picture of co lon cance r. Accurate evaluation of co lon carcinoma re quir es both hi gh se nsiti v ity and sp ec ificity for th e prese nce oflocal , regional , and distant tumor spreads. The precise role of these modalities are still be ing deb ate d (2) . Nevertheless , the import ance of an in-d ept h a naly s is of the effec tiveness of these technologies is emph as ized by the fact that colon cancer is one * 01 Asan Medical Cen te r , Uni versity 01 Ulsan College 01 Medicine Received April 28 , Accepted November 20, 199 2 - 118 -
Transcript of CT Evaluation of Colon Carcinoma:Emphasis on Distant Lymph ...

대 한 방 사 선 의 학 회 지 1993; 29 ( 1) : 118~ 1 25
Journal of Korean Radiological Society, January, 1993
CT Evaluation of Colon Carcinoma:Emphasis on Distant
Lymph N ode Invasion and Liver Metastases
Kyung Il Chung, M.D. , Kyoung Sik Cho, M.D. , Moon-Gyu Lee, M.D. , Seung Yeon Bael‘’ M.D. , Yong Ho Auh , M.D. , Jin Cheon Kim* , M.D.
Departmeηt 01 Diagnostic Radiology Asaη M edical Center, U:ηiversity 01 Ulsαη College 01 Mediciηe
- Abstract-
Even thou gh the value of computed tomography (CT) used to detect the colon carcinoma with minimal
invasion is limited , its usefulness in the evaluation of the extent of disease such as hepatic metastasis or dis
tant lymph node invasion has been emphasized. To examine the role of CT in the evaluation of colon car
cinoma , CT scans obtained during the past 2 years in 56 patients with surgically proven colon carcinoma
were reviewed and the findings correlated with pathologic results. The sensitivity and accuracy of CT for
peric이ic fat infiltration were 86 , 58 and 80% respectively. Those of regional node were 60 , 83 and 75%
and distant node 67 , 100 and 95 %. Liver metastases showed sensitivity, specificity and accuracy of 83 , 98 , 96% and peritoneal metastases 67 , 94 and 89% respectively.
CT detected local invasion with fair degree of accuracy but the true value of CT lie in the detection of
distant invasions such as liver and distant lymph node metastases thereby leading to preclusion of unnecessary
procedures and implementation of appropria te procedures.
Index Words: Colon Carcinoma
Liver , metastases
Lymph Node, metastases
INTRODUCTION
Almost two decades have passed since CT was
first introduced . Since then , it has been used to
d etect and to stage many tumors including col
on carcinoma , recently joined by MR imaging, endoscopic sonography , and monoclonal an
tibody imaging . Many conflicting reports on the
effectiven ess of the various m e thods has been
published in the literature largely due to
*울산대학교 의과대학 일반외과학교실
prem ature conclusions (1). Although the above
m ethods help to detect colon carcinoma , none
has the capacity to show full picture of colon
cancer. Accurate evaluation of colon carcinoma
requires both high sensitiv ity and specificity fo r
the presence oflocal , regional , and distant tumor
spreads. The precise role of these modalities are
still b eing debated (2) .
Nevertheless , the importan ce of an in-depth
analysis of the effectiven ess of these technologies
is emphasized by the fact that colon cancer is one
* Departmeηt 01 Geηeral 5;μrgery, Asan Medical Center, University 01 Ulsan College 01 Medicine 이 논문은 1992년 4월 28일 접수하여 1992년 11월 20일에 채택되었음.
Received April 28, Accepted November 20, 1992
- 118 -

of the most common cancer of this age and the
prognosis of patients with this neoplasm largely depend on the extent of tumor at the time of diagnosis (1 ,2)
Colon carcinoma is diagnosed on the basis of a clinical examination , endoscopy , and a double contrast barium enema study. The correct therapeutic choice requires knowledge of the
stage of the tumor obtained by endoscopy , ultrasound , CT, or MR imaging.
CT is the most commonly used method for staging of colon cancer in spite of the debate on its accuracy. Accuracy of CT staging of primary colon carcinoma ranges between 47% to 64 % .
The major errors were caused by inability to detect pericolic extension and lymph nodes involvement (3-6). On the basis of these reports , preoperative local staging of colonic carcinoma
is clinical1y useless , and therefore it is not recommended (3 ,4).
Despite the current general lack of enthusiasm
for preoperative imaging of patients with colon
carcinoma, knowledge of extent of tumor spread before surgery could have a significant impact on therapy, such as preoperative and/or intraoperative radiation therapy to control local
tumor spread or to make previously inoperative lesions resectable (7). Resection of liver metastasis and biopsy of suspected lesions may be facilitated with accurate preoperative imag
ing. Appropriate nonsurgical therapy could be initiated sooner, and noneffective surgical procedures could be avoided (2).
The aim of this study is to document CT role
in evaluation of colon carcinoma by attempting to prove the usefulness of CT in detection of distant lymph nodes and liver metastases.
MATERIALS AND METHODS
CT scans were performed on 56 patients with
colon carcinoma prior to surgery and the diagnosis was confirmed subsequently by exploratory laparotomy and pathological evalua-
Kyung 11 Chung, et al : CT Evaluation of Colon Carcinoma
tion of the resected specimen. Patients were given 700ml of 4.6% barium
sulfate (E-Z-Cat;E-Z-EM, Westberry) per or,al1y one hour before the CT examination. IV bolus
injection of 100ml of 68 % meglumine ioglicate (Rayvist 300;Schering, Germany) and 300ml of 1.5% barium sulfate per rectally were introduced prior to the examination.
With the patient in the supine position , scans
were obtained from the xyphoid process to symphysis pubis using 5mm thickness and 5mm gap on a GE 9800 (GE Medical Systems , Milwaukee) or Picker 1200 (Picker lnternational Inc , Cleveland) scanner.
The CT images were evaluated without the knowledge of surgical or pathological findings , taking into account the morphology of the tumor , penc이ic infiltration , invasion of adjacent organs and lymph nodes , and metastases to distant organs such as liver and distant lymph nodes
The site of the primary tumor, mesentery , and
retroperitoneum were evaluated for tumor involvement along with the presence of ascites. Lymph nodes >10mm in diameter were considered positive involvement.
RESULTS
The locations of the colon cancer (Table 1) were 6 cases involving cecum, 14 cases ascending colon , 3 hepatic fl exure , 9 transverse colon , 2 descending colon , and 22 sigmoid colon dis-
Table 1. Location of Colon Carcinoma
Location No
Mu
m
뼈
C A
6
% 3 9
2
있 -%
Hepatic flexure Transverse Descending Sigmoid
Total
- 119 -

Journal of Korean Radiological Society 1993; 29 (1) 1 18~ 125
Table 2. Cases o[ Pathologic Stages*
Stage No
A/B l B2 C1 C2 D
Total 56
* Modified Dukes Classification
regarding rectal cancer. 8 cases showed obstruc
tion which included 2 cases of intussusseption and cancer perforation was noted in 4 cases . U s
ing the Astler Coller version (8) of Dukes
Classification modified by Turnbull (9) of Col
on Carcinoma (Table 2) there were 5 cases of
stage A or B1 , 15 cases ofB2 , 4 ofC1 , 15 ofC2 , and 17 cases of stage D with the correct stage
shown in 31 cases (55 %). The CT results for
detecting pericolic infùtration are shown in Table
3. Pericolic infiltration was detected in 38 cases
and it showed the sensitivity , specificity , and ac
curacy of86 ,58 , and 80 % respectively. Among
the five false positive cases , two had intussuscep
tion and one h ad synchronous tumor. All of these
apparently did not have pericolic infiltration as
they appeared to have in CT. Among the six false
negative cases , lesion could not be identified in one case and three cases had either liver or
peritoneal metastases without definite sign of
penc이ic infiltration . There were 20 cases with
regional lymph node involvement and CT de
tected 12 of them resulting in the sensitivity and
accuracy of 60 % and 75% (Table 4) (Fig. 1).
Nine cases of distant lymph nodes involvement
included 3 cases of paraaortic (Fig. 2) , 1 each
of rectal shelf, iliac bifurcation, middle colic
artery , and retroperitoneal lymph nodes . One
of the paraortic nodes (Fig. 3) and lymph nodes
at iliac bifurcation and middle colic artery did
not show up in CT. There were n o false positive
cases giving the specificity and accuracy of 100 %
and 95 % for the distant lymph nodes . Overall
ζJ r이) AT
CJ
껴/
1
1
1
Fig. 1. 73 year old female patient with sigmoid adenocarcinoma. Perico\ic fat and lymph node infiltrations shown on CT but pathology proved negative lymph node involvement
Table 3. CT results in Determining Perico\ic Infiltration
Pericolic Infiltration(n = 56)
No . of true positives No. of true negative No. of false positives No. o[ fal se negatives % Sensitivity % Specificity % Accuracy
% 7 5 6
% %
mω
Table 4. CT results in Determining Metastatic Lymphadenopathy
Regional Distant Nodes(n = 20)Nodes(n = 9)
No. of true positives 12 6 No . of true negative 30 47 No. of false positives 6 0 No. of fal se negatives 8 3 % Sensitivity 60 67 % Specificity 83 100
% Accuracy 75 95
- 120-

Kyung 11 Chung, et al : CT Evaluation of Colon Carcinoma
a b
c d
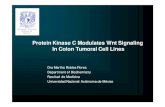
Fig. 2. 35 year old male patient with sigmoid mass. CT revealed cardiophrenic and pa raortic lymph node enlargem ent (a ,b). Eight months after the resection of the lesion and implementation of chemotheraphy , follow-up CT showed complete resolution of the lymph node involovement (c,d)
a b
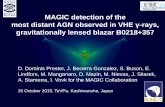
Fig. 3. 48 year old male pa tient with ascending colon mass and pericolic fat infiltration on CT (a). Three months after tumor rescction , follow-up CT revealed extensive retroperitoneal node inva sion (b)
m
ω

Journal of Korean Radiological Society 1993; 29 ( 1) : 1 18~ 125
a b
c d
Fig.4. 47 year old male patient with ascending colonic lesion and a focalliver metastasis on CT (a ,b). During the resection of the main lesion , porthocath was inserted for chemotheraphy of the hepatic lesion (c). 2 month follow-up CT showed resolution of the metastatic lesion (d).
CT gave sensitivity, specificity, and accuracy of Table 5. CT results in Determining Tissue/Organ 52 , 77 , and 66 % . M etastases
There were 6 cases of metastases to liver (Fig
4);two from the ascending, one from transverse , one descending, and two from sigmoid colon.
Although one case was incorrectly interpreted as
having a metastatic lesion while another was
undetected , CT showed high sensitivity , specificity , and accuracy of 83 % , 98 %, and 96 % (Table 5). Peritoneal seeding was correctly
detected by CT in 6 cases in which 2 had cancer
perforation and 2 others had malignant ascites .
Three cases were falsely interpreted as having
peritoneal seeding and 3 cases didn ’ t show (Fig.
5) with the result of sensitivity and accuracy of
Liver Peritoneum (n = 6) (n = 9)
No. of true positives 5 6 No. of true negative 49 44 No. of false positives 3 No. of false negatives 3 % Sensitivity 83 67 % Specificity 98 94 % Accuracy 96 89
m 4

Fig. 5. 59 year old male patient with ascending colon mass and pericolic fat infiltration on CT which showed no evidence of peritoneal involvement but pathology proved otherwise.
67% and 89 %. CT detected metastatic lesions
in 20 cases and 13 of them were proven to be
true lesions which included ureter and stomach
m etastases in each case. There were 4 false
negative cases which included metastases to
uterus , bladder , stomach , and abdominal wall
in each case. Seven false positive cases include
2 cases to pancreas , and 1 each to seminal vesi
cle , lung, and gastrocolic ligamen t. Overall sen
sitivity , specificity , accuracy of CT in
evaluationg distant metastases were 76 , 82 , and
80 % respectively.
DISCUSSION
According to the study by Kelvin (10) , liver
metastases are found in 15 % -20 % of patients at
the time of surgery and 29 % of patients with
disease-free liver at laparotomy develop liver
metastases within 2 years suggesting possible fre
quency of liver metastases as close as 50 % . More
than half of the deaths after the surgery of col
orectal carcinoma are secondary to hepatic
m etastases , and therefore detecting liver
metastases by CT before and after surgery is very
importan t. Freeney reported hepatic metastases
in 11 out of 103 patient (11 %) in his study which
Kyung 11 Chung, et al : CT Eva luation of Colon Carcinoma
gave sensitigity and specificity of 72.7 % and
98 .9% (4) . This series showed hepatic m etastases
in 6 out of 56 patients (11 %) giving sensitivity
and specificity of 83 % and 98 % . These results
are quite similar except for the higher sensitivi
ty shown in this study . Most of the previous
studies reported accuracy rate of 76 % -96 %
which is quite comparable to the value of 96 % in this series (13-15)
In evaluating lymph node involvement , Zaun
bauer (11) reported an accuracy of 100 % , Thompson (3) a sensitivity of 22 % and specificity of75% , and Balthazar (5) a sensitivity of73%
and a specificity of 58 % .
Regional lymph nodes were reported to be
recognizable in only 22 % -35 % by studies before
(10). Freeney also reported 7 true positive and
20 false negative lymph node (out of 80) involvement by colon carcinoma giving sensitivity , dnd
specificity of 25.9% and 96 % (4) .
On the contrary, this study showed correct CT
detection rate oflymph node involvement in 12
out of 56 patients with 60 % sensitivity and 83 %
specificity. These differences in value can part
ly be explained b y different diagnostic criteria
used to detect lymph nodes in each study (e .g . ,>1. 5cm versus>1.0cm in our study) and
also due to this series not including rectal car-
Clnoma.
Contrary to the low values in detecting regionl
lymph nodes , this series showed sensitivity , specificity , and accuracy of 67 , 100 , and 95 %
in detecting distant lymph nodes by CT.
Although sen sitivity of 67 % is not highly
reflected by miss-reading of one paraaortic lymph
node, both high specificity and accuracy suggest
the usefulness of CT in evaluating extensive
diseases .
Previous studies recognized local extension of
tumor into or beyond the pericolic fat in
61 % -77 % (10) . In this series , pericolic fat in
filtration was observed in 68 % (38 out of 56 patients). Freeney reported sensitivity and
specifici ty of 61. 2 % and 80 .6 % (4) whereas this
m
냉

Journal of Korean Radiological Society 1993; 29 (1) : 1 18~ 125
study showed those of 86 % and 58 %. Low
specificity is due to the lack of spatial resolution
necessary for detecting minor degree of pericolic
infiltration by CT limiting its reliability in this
regard.
Resection of solitary hepatic metastases results
in 5-year survival rate of 42 %, and of multiple
metastases to a single lobe rate of 25 % (12). In
view of the poor prognosis of untreated hepatic
metastases , the usefulness of CT is emphasized
in detecting the colon carcinoma metastases to
liver.
With its ability to detect distant lymph nodes
and hepatic metastases with high degree of
specificity and accuracy, and also with its limita
tion in the overall sensitivity and accuracy oflocal
staging of colon carcinoma, the true value of CT
lie in detecting distant metastatic lesions thereby
preduding unnecessary procedures or including
necessary procedures such as preoperative and/or
intraoperative radiation therapy to controllocal
tumor spread or to make previously inoperable
les ion resectable , and implantation of
chemotherapy devices.
REF'ERENCES
1. Theoni RF. Corectal Cancer: Cross-sectional lmaging for Staging of Prima ry Tumor and Detection of Local R ecurrence . AJR 1991; 156:909-915
2. Moss AA. lmaging of Colorectal Carcinoma. Radiology 1989 ;170 :308-310
3. Thompson W , Halvorsen R , FosterW, Roberts
L , Gibbons R . Preoperative and Postoperative CT Staging of Rectosigmoid Cancer. AJR 1986; 146: 703-710
4. Freeney PC , Marks WM , RyanJM , BolenJW.
Colorectal Carcinoma evaluation with CT:
preoperative staging and detection of postoperative recurrence. Radiology 1986;158:347-535
5 . Balthazar EJ , Megibow AJ , Hulnick DB , Naidich DP. Carcinoma ofthe Colon: Detection and Preoperative staging by CT. AJR 1988 ; 150: 301-306
6. Angelellei G , Macarini L , et al. Rectal Carcinoma: CT Staging with Water as Contrast M edium. Radiology 1990;177:511-514
7. Theoni RF. CT Evaluation of Carcinoma of the
Colon and Rectum. CT of Gastrointestinal Tract. 1989 ;27 (4):731-741
8. Astler VB , Coller FA. The prognostic significance of direct extension of carcinoma of the colon and rectum. Ann Surg 1954;1 39 :846-851
9. Turnbull RB J r. The no-touch isolation technique of resection. JAMA 1975 ;23 1:1181-1182
10. Kelvin FM , Maglinte DD. Colorectal Carcinoma: A Radiologic and Clinical Review. Radiology 1987;164:1-8
11. Zaubauer W , Haertel M , Fuchs WA , et al.
Computed tomography in carcinoma ofthe rectum . Gastrointest Radiol 19081;6:79-84
12. Adson MA, Van-Heerdon JA . Major hepatic resections for metastatic colore ctal cancer . Ann Surg 1980 ;191 :576-583
13. Alderson PO , Adams DF , Mc-Neil BJ , et al.
Computed tomography , ultrasound , and scintigraphy of the liver in patients with colon or breast carcinoma: a prospective comparison
R adiology 1983 ;149:225-230 14. KnopfDR , Torres WE , Fajman WJ , Sones PJ
Jr . Liver lesions: comparative accuracy of scintigraphy and computed tomography. AJR 1982; 138:623-627
15. Smith 매, Kemeny MM , Sugarbaker PH , et al.
A prospective study of hepatic imaging in the detection of metastatic disease. Ann Surg 1982 ; 195:486-491
- 124-

Kyung 11 Chung, et al : CT Eva luation of Colon Carcinoma
〈국문 요약〉
대장암의 전산화단층촬영소견 : 원격임파선과 간전이에 대한 고찰
울산대학교 의과대학 진단방사선과학교실, 일반외과학교실*
정 경 일 • 조 경 식 • 이 문 규 • 오 용 호 • 검 진 천*
대장암의 근접부위전이 평가에 대한 전산화단충촬영의 유용성은 그 한계가 제시되고 있고 대신 광범위전이에 대한
이의 이용도가 강조되고 있다. 대장암에 있어서 이와같은 전산화단층촬영의 유용성을 평가하기 위하여 지난 2년간
병리학적으로 대장암으로 판명되었던 56명의 환자들의 전산화단층촬영 소견을 분석하여 근위지방조직침범은 86, 58,
80%의 민감도, 특이도, 정확도를 보였으며 근위임파선침입 60, 83, 75%, 원위임파선전이 67, 100, 95%, 간전이
83, 98, 96%, 복막전이 67, 94, 89%등의 결과를 보였다. 전산화단층촬영은 본 연구에서 근위부침입 평가시 비교적
좋은 정확도를 보였으나 간이나 원위임파선전이 같은 원격광범위전이 평가시 이의 가치가 더 있는 것으로 판명되었
으며 이러한 소견은 환자의 적절한 치료유도에 기여할 것이다.
m
ω