Comparative pharmacokinetics and tissue distribution analysis of systemically administered...
8
Comparative pharmacokinetics and tissue distribution analysis of systemically administered 17-β-estradiol and its metabolites in vivo delivered using a cationic nanoemulsion or a peptide-modified nanoemulsion system for targeting atherosclerosis Dipti Deshpande a , Sravani Kethireddy a , Florence Gattacceca a,b , Mansoor Amiji a, ⁎ a Department of Pharmaceutical Sciences, School of Pharmacy, Bouvé College of Health Sciences, Northeastern University, Boston 02115-5000, USA b Department of Pharmacokinetics, EA4215 Faculté de Pharmacie, Université Montpellier 1, 15 av. Ch. Flahault, 34093 Montpellier Cedex 5, France abstract article info Article history: Received 5 September 2013 Accepted 10 February 2014 Available online 17 February 2014 Keywords: Nanoemulsion CREKA DOTAP Targeting efficiency 17-βE Atherosclerosis The primary objective of this study was to compare the biodistribution and pharmacokinetic profile of 17-β- estradiol (17-βE) on systemic delivery using either the cationic or the CREKA-peptide-modified (Cysteine– Arginine–Glutamic-acid–Lysine–Alanine) omega-3-fatty acid oil containing nanoemulsion system in vivo in the wild type C57BL/6 mice. Higher blood concentrations of 17-βE, higher accumulation in the tissues of interest – heart and aorta, and higher accumulation within the other tissues – liver and kidney was observed on delivering 17- βE using the CREKA-peptide-modified nanoemulsion system (AUC last in plasma — 263.89 ± 21.81 min*%/injected dose/ml) as compared to the cationic nanoemulsion (AUC last in plasma — 20.2 ± 1.86 min*%/injected dose/ml) and solution form (AUC last in plasma — 44.9 ± 1.24 min*%/injected dose/ml) respectively. Both, the cationic nanoemulsion and the CREKA-peptide-modified nanoemulsion showed a higher relative targeting efficiency of 4.57 and 4.86 respectively for 17-βE than the relative targeting efficiency of 1.78 observed with the solution form. In conclusion, since the maximum exposure (highest AUC last for plasma and tissues) for 17-βE was observed with the CREKA-peptide-modified nanoemulsion system, the study shows that CREKA-peptide-modi fied nanoemulsion system was the most suitable vehicle for systemic delivery of 17-βE in the wild type C57BL/6 mice. © 2014 Elsevier B.V. All rights reserved. 1. Introduction Occlusive vascular disorders like atherosclerosis are the primary cause of deaths associated with cardiovascular diseases [1]. Severely oc- cluded vessels and critical stenosis leads to acute coronary syndromes and myocardial infarction, however sudden deaths due to these events are mainly associated with the highly rupture prone-vulnerable plaque that shows only 30% vessel stenosis [2]. Systemic therapy with statins as well as local approaches aimed at focal plaque pacification have shown limited success in targeting and management of vulnerable plaque [2]. In recent years, the field of cardiovascular research has seen some promising research involving the application of nanotechnology for di- agnosis as well as treatment of atherosclerosis [3]. The cardioprotective benefits of 17-βE have been reported in several pre-clinical models [4–6]. While observational studies have reported about 50% reduced incidences of coronary artery disease in postmenopausal women receiv- ing hormone therapy, the results from clinical trials evaluating hormone replacement therapy have always shown large discrepancies and limited success in the treatment of the disease [7–9]. Current research is now focused on designing techniques for improved delivery of this hormone [10]. In our previous study, we have demonstrated the suc- cessful encapsulation of 17-β-estradiol (17-βE) in an omega-3-fatty acid containing flaxseed oil-based cationic nanoemulsion system and the therapeutically beneficial responses of this formulation on vascular cells in vitro [11]. In addition to this formulation system, we have devel- oped a slightly modified 17-βE loaded CREKA-peptide-modified nanoemulsion system (Cysteine-Arginine-Glutamic-acid-Lysine- Alanine). The peptide CREKA shows selective targeting of fibrin clots that are observed in atherosclerotic lesions [12,13]. In the current study, we have compared and contrasted the pharmacokinetic profile and biodistribution of 17-βE when administered using the solution sys- tem, cationic nanoemulsion system and the CREKA-peptide modified nanoemulsion system to identify the most suitable formulation for systemic delivery of 17-βE in vivo in the C57BL/6 mice for treatment of atherosclerosis. 17-βE exerts atheroprotection through local and other pleiotropic mechanisms and circulating plasma levels of 17-βE correlate inversely with the size, development, number and distribution of atherosclerotic lesions in mice [6,14]. 17-βE is a lipophilic molecule and is mainly elim- inated through urinary/fecal excretion by conversion into less active, Journal of Controlled Release 180 (2014) 117–124 ⁎ Corresponding author. Tel.: +1 617 373 3137; fax: +1 617 373 8886. E-mail address: [email protected] (M. Amiji). http://dx.doi.org/10.1016/j.jconrel.2014.02.009 0168-3659/© 2014 Elsevier B.V. All rights reserved. Contents lists available at ScienceDirect Journal of Controlled Release journal homepage: www.elsevier.com/locate/jconrel
Transcript of Comparative pharmacokinetics and tissue distribution analysis of systemically administered...

Journal of Controlled Release 180 (2014) 117–124
Contents lists available at ScienceDirect
Journal of Controlled Release
j ourna l homepage: www.e lsev ie r .com/ locate / j conre l
Comparative pharmacokinetics and tissue distribution analysis ofsystemically administered 17-β-estradiol and its metabolites in vivodelivered using a cationic nanoemulsion or a peptide-modifiednanoemulsion system for targeting atherosclerosis
Dipti Deshpande a, Sravani Kethireddy a, Florence Gattacceca a,b, Mansoor Amiji a,⁎a Department of Pharmaceutical Sciences, School of Pharmacy, Bouvé College of Health Sciences, Northeastern University, Boston 02115-5000, USAb Department of Pharmacokinetics, EA4215 Faculté de Pharmacie, Université Montpellier 1, 15 av. Ch. Flahault, 34093 Montpellier Cedex 5, France
⁎ Corresponding author. Tel.: +1 617 373 3137; fax: +E-mail address: [email protected] (M. Amiji).
http://dx.doi.org/10.1016/j.jconrel.2014.02.0090168-3659/© 2014 Elsevier B.V. All rights reserved.
a b s t r a c t
a r t i c l e i n f oArticle history:Received 5 September 2013Accepted 10 February 2014Available online 17 February 2014
Keywords:NanoemulsionCREKADOTAPTargeting efficiency17-βEAtherosclerosis
The primary objective of this study was to compare the biodistribution and pharmacokinetic profile of 17-β-estradiol (17-βE) on systemic delivery using either the cationic or the CREKA-peptide-modified (Cysteine–Arginine–Glutamic-acid–Lysine–Alanine) omega-3-fatty acid oil containing nanoemulsion system in vivo inthe wild type C57BL/6 mice. Higher blood concentrations of 17-βE, higher accumulation in the tissues of interest –heart and aorta, and higher accumulationwithin the other tissues – liver and kidneywas observed on delivering 17-βE using the CREKA-peptide-modified nanoemulsion system (AUClast in plasma— 263.89 ± 21.81 min*%/injecteddose/ml) as compared to the cationic nanoemulsion (AUClast in plasma — 20.2 ± 1.86 min*%/injected dose/ml)and solution form (AUClast in plasma — 44.9 ± 1.24 min*%/injected dose/ml) respectively. Both, the cationicnanoemulsion and the CREKA-peptide-modified nanoemulsion showed a higher relative targeting efficiency of4.57 and 4.86 respectively for 17-βE than the relative targeting efficiency of 1.78 observed with the solution form.In conclusion, since the maximum exposure (highest AUClast for plasma and tissues) for 17-βE was observed withthe CREKA-peptide-modified nanoemulsion system, the study shows that CREKA-peptide-modified nanoemulsionsystem was the most suitable vehicle for systemic delivery of 17-βE in the wild type C57BL/6 mice.
© 2014 Elsevier B.V. All rights reserved.
1. Introduction
Occlusive vascular disorders like atherosclerosis are the primarycause of deaths associatedwith cardiovascular diseases [1]. Severely oc-cluded vessels and critical stenosis leads to acute coronary syndromesand myocardial infarction, however sudden deaths due to these eventsare mainly associated with the highly rupture prone-vulnerable plaquethat shows only 30% vessel stenosis [2]. Systemic therapywith statins aswell as local approaches aimed at focal plaque pacification have shownlimited success in targeting and management of vulnerable plaque [2].In recent years, the field of cardiovascular research has seen somepromising research involving the application of nanotechnology for di-agnosis as well as treatment of atherosclerosis [3]. The cardioprotectivebenefits of 17-βE have been reported in several pre-clinical models[4–6]. While observational studies have reported about 50% reducedincidences of coronary artery disease in postmenopausalwomen receiv-ing hormone therapy, the results from clinical trials evaluating hormonereplacement therapy have always shown large discrepancies and
1 617 373 8886.
limited success in the treatment of the disease [7–9]. Current researchis now focused on designing techniques for improved delivery of thishormone [10]. In our previous study, we have demonstrated the suc-cessful encapsulation of 17-β-estradiol (17-βE) in an omega-3-fattyacid containing flaxseed oil-based cationic nanoemulsion system andthe therapeutically beneficial responses of this formulation on vascularcells in vitro [11]. In addition to this formulation system, we have devel-oped a slightly modified 17-βE loaded CREKA-peptide-modifiednanoemulsion system (Cysteine-Arginine-Glutamic-acid-Lysine-Alanine). The peptide CREKA shows selective targeting of fibrin clotsthat are observed in atherosclerotic lesions [12,13]. In the currentstudy, we have compared and contrasted the pharmacokinetic profileand biodistribution of 17-βEwhen administered using the solution sys-tem, cationic nanoemulsion system and the CREKA-peptide modifiednanoemulsion system to identify the most suitable formulation forsystemic delivery of 17-βE in vivo in the C57BL/6 mice for treatmentof atherosclerosis.
17-βE exerts atheroprotection through local and other pleiotropicmechanisms and circulating plasma levels of 17-βE correlate inverselywith the size, development, number and distribution of atheroscleroticlesions in mice [6,14]. 17-βE is a lipophilic molecule and is mainly elim-inated through urinary/fecal excretion by conversion into less active,

118 D. Deshpande et al. / Journal of Controlled Release 180 (2014) 117–124
hydrophilic metabolites [15]. In humans, intravenously administered17-βE is rapidly metabolized into estrones and other conjugates, witha plasma half-life of 27.45 ± 5.65 min and a low volume of distribution(0.082± 0.015 l/kg) [16]. Themajor pathways involved in themetabo-lism of 17-βE include mainly oxidative transformation which involveshydroxylation at 2- and 16-positions and the conjugative metabolismthat includes sulfonation, glucuronidation and O-methylation [15]. Es-trogen metabolism mainly occurs in the liver, catalyzed by enzymes ofthe cytochrome P450 family and some isoforms of the estrogen metab-olizing enzymes are also found in extrahepatic tissues [15,17]. Hydrox-ylation at the 16-position leads to the formation of estriol and estriolconjugates predominate themetabolic profile of 17-βE inmice, as com-pared to the estrone conjugates observed in the metabolic profile ofhumans [18,19]. In addition, whereas urinary excretion is prevalent inwomen (63% of intravenously administered 17-βE mainly excretedthrough the urine), 17-βE is mainly excreted through the feces inmice [18,20]. Estradiol sulfate has been reported as one of themajorme-tabolites observed in the plasma of mice on intravenous administration[18]. Thus, in our study we have measured the levels of 17-βE (parentcompound), Estradiol sulfate (ESS) and Estriol (EST), observedin the plasma and other tissues on intravenous administration of17-βE using either solution, cationic nanoemulsion or the CREKA-peptide-modified nanoemulsion system. The pharmacokinetics andbiodistribution studies were performed using tritiated estradioland the radioactive fractions of the parent compound and twometabo-lites –ESS and EST were first separated using high-performance liquidchromatography (HPLC) and then measured by liquid scintillationcounting.
2. Materials and methods
2.1. Chemicals and reagents
17-β-Estradiol, 17-β-estradiol-3-sulfate (ESS) and (17β)-estra1,3,5(10)-triene-3,17-diol EST were purchased from Sigma-Aldrich (StLouis, MO). Extra-virgin, ω-3-PUFA-containing flaxseed oil was kindlyprovided by Jedwards International (Quincy, MA). Egg phosphatidyl-choline (Lipoid® E80) and 1,2-dioleolyl-3-trimethylammonium-propane (DOTAP) was kindly provided by Lipoid GmbH (Ludwigshafen,Germany), and 1,2-distearoyl-sn-glycero-3-phosphoethanolamine-N-[methoxy-(polyethylene glycol)-2000] (DSPE-PEG2000) was fromGenzyme (Cambridge, MA). The peptide sequence cysteine–arginine–glutamic acid–lysine–alanine (CREKA) was synthesized and purchasedfrom Tufts University — peptide synthesis core facility (Boston, MA).Tritiated estradiol, 17-β-[2,4,6,7-3H] (70–120 Ci/mmol) was acquiredfrom American Radiolabeled Chemicals, Inc. (St. Louis, USA). All otherchemicals and solvents were of analytical reagent grade. The maleC57BL/6 mice were ordered from Taconic (Germantown, NY).
Table 1Characterization of 17-βE loaded cationic and CREKA-peptide modified nanoemulsionsystem. Both nanoemulsion systems were prepared by microfluidization technique anddata was represented as mean and standard deviation of particle size and zeta potentialmeasurements (n = 3).
Formulation Mean diameter(nm)
Polydispersityindex
Zeta Potential(mV)
17-βE loaded cationicnanoemulsion
138 + 9.1 0.14 33.8 + 2.4
17-βE loaded CREKA-pepidemodified nanoemulsion
168 + 6.1 0.01 −52.8 + 4.2
2.2. Preparation of the cationic 17-βE loaded nanoemulsion system and theCREKA peptide modified 17-βE loaded nanoemulsion
The 17-βE loaded cationic nanoemulsion systemwas prepared by themicrofluidization technique as described in our previous study [11]. TheCREKA-peptide modified 17-βE loaded nanoemulsion system had a sim-ilar composition and was prepared by the same microfluidization tech-nique. The difference in CREKA-peptide modified nanoemulsion system,consisted of removal of DOTAP and incorporation of the DSPE–PEG–CREKA conjugate in the formulation. DSPE–PEG–CREKA conjugate wassynthesized by dissolving 0.1 g of DSPE–PEG2000 Maleimide (mwt2941.605, 1.36 mmol) in 25 ml of PBS solution (pH 7.4) with continuousmixing until a clear solutionwas formed. To this solution, twicemolar ex-cess amount (0.042 g) of the CREKA peptide (mwt 605.71, 2.72 mmol)
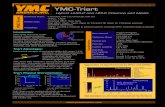
Fig. 1. Plasma concentrations of 17-βE and metabolites ESS and EST after intravenousdosing. Plasma concentrations (% ID = % Injected dose/ml) versus time data of A) 17-βEB) ESS and C) EST following intravenous administration of 17-βE in the solution (n = 4),cationic nanoemulsion (DOTAP) (n = 3) and CREKA-peptide modified nanoemulsionsystems (n = 4) in mice. Data represented as mean and standard deviation of plasmaconcentration (% ID/ml) versus time (n = 4).

119D. Deshpande et al. / Journal of Controlled Release 180 (2014) 117–124
was added, the dissolved oxygen was displaced under a nitrogen streamand the reaction was then sealed and stirred overnight at 4 °C. Themixture was then dialyzed thoroughly using a cellulose dialysis mem-brane (MW cut off ~2000) for 10 h to remove excess unconjugated pep-tide. Following dialysis, the final product was lyophilized and stored at−20 °C until further use.
2.3. Pharmacokinetic study design
Pharmacokinetic and tissue distribution studies were performedusing male mice C57 BL/6 (20-25 g) obtained from Taconic Farms, Inc.(Albany, NewYork). The care andhandling of the animalswas in a path-ogen free environment in the Division of Laboratory Animal Medicine(DLAM) facility and the animals were provided with food and waterad libitum. The mice were dosed intravenously using an insulin syringefittedwith a 26 gauge needle andwere divided into three groups. Group1 received 100 μl (4 μCi) of tritiated 17-βE in solution form (n = 4),group 2 received 100 μl (4 μCi) of tritiated 17-βE encapsulated in thecationic nanoemulsion system (DOTAP) (n = 3) and group 3 received100 μl (4 μCi) of tritiated 17-βE encapsulated in the CREKA-peptidemodified nanoemulsion system (n = 4). At various time points(5 min, 15 min, 30 min and 60 min), the animals were anesthetizedwith isoflurane and blood samples were collected via cardiac punctureinto heparin treated tubes. The blood samples were centrifuged at5000 ×g for 15 min at 4 °C using the Beckman Coulter-microfuge 22Rcentrifuge (Brea, CA); the plasma supernatant was removed and storedat −80 °C until further analysis. After blood collection, the mice wereeuthanized by cervical dislocation and the liver, kidney, heart andaorta were isolated, washed with distilled water, weighed and storedat−80 °C until further analysis.
2.4. Plasma and tissue sample preparation and analysis
The radioactive compoundwas extracted from plasma using an eth-anol: methanol — 1:1 solvent system. To 50 μl of plasma, 200 μl of 1:1ratio of ethanol: methanol mixture was added, vortexed and centri-fuged at 10,000 rpm for 10 min at 4 °C. The supernatant was collectedfor further analysis. Tissue slurrywasprepared byhomogenizing the tis-sues in PBS and the radioactive compoundwas extracted using the eth-anol: methanol — 1:1 solvent system (20% w/v). The extracted slurrywas vortexed, centrifuged at 10,000 rpm for 15 min at 4 °C and the su-pernatant was collected for further analysis. The collected supernatantswere evaporated to dryness under vacuum using the Speedvac VacuumConcentrator fromThermofisher Scientific Inc. (Pittsburgh, PA). The res-idues were reconstituted with the mobile phase (20% acetonitrile inwater), spiked with unlabeled reference standards (17-βE, ESS andEST) and 70 μl of the reconstituted samples were injected into theHPLC for further analysis as described below.
Table 2Plasma PK parameters of 17-βE andmetabolites ESS and EST after intravenous dosing. Pharmacokfollowing intravenous administration of 17-βE in the solution (n = 4), cationic nanoemulsimice. NE = Nanoemulsion, AUClast = AUC until last time point, MRT = Mean residencClearance, Vss = Volume of distribution at steady state, AUCinf = AUC until infinity.
17-BE ESS
Solution DOTAP NE CREKA NE Solution
AUClast ± S.E(min*%ID/ml)
44.9 ± 1.24 20.2 ± 1.86 263.8 ± 21.81 53 ± 3.3
MRT (min) 47.8 48.8 79.3 42t1/2(min) 41.7 34.8 62.3 29.4λz (1/min) 0.0166 0.0199 0.0111 0.023Cl (ml/g·min) 1.57 3.47 0.206Vss (ml) 75 169.4 16.3AUC∞ (min*%ID/ml) 63.8 28.2 485.4
2.5. Analytical method for separation and quantification
Tritiated 17-βE and its twometabolites ESS and ESTwere quantifiedby liquid scintillation counting using the Beckman Coulter-LS6500mul-tipurpose scintillation counter (Brea, CA). The reconstituted sampleswere manually injected into the HPLC system equipped with a pumpand UV-detector. The separation of the parent compound and themetabolites was achieved using an Agilent column (C18, particle size5 μM, 150 mm × 4.6 mm) at a flow rate of 1 ml/min and the elutionwas monitored at 228 nm. The chromatographic separations were per-formed at room temperature under gradient flow conditions where thetwo mobile phases,−20% acetonitrile with 1% ammonium acetate anddistilled water with 1% ammonium acetate were mixed automaticallyaccording to a linear pump programwith starting time0min over a gra-dient run duration of 30min. Based on a standard curve obtained previ-ously using this method and the unlabeled reference standards,fractions of ESS, EST and 17-βE from each reconstituted sample werecollected into scintillation vials. To these collected fractions, 5 ml of Ul-timaGold™ scintillation cocktail from PerkinElmer (Waltham,MA)wasadded, the samples were vortexed and the radioactive counts weremeasured using the scintillation counter.
2.6. Pharmacokinetics and statistical analysis
The pharmacokinetic parameters of 17-βE, ESS and EST were esti-mated using the Phoenix® WinNonlin® v. 1.3 software. Non-compartmental analysis was performed using the non-compartmentalsparse methodology, with uniform weighing. Linear trapezoidal rulewas used to calculate area under the plasma or tissue concentration-time curve (AUC) until the last observation (AUClast). A regression ofthe natural logarithm of concentrations was used to determine theslope of the log-linear terminal part of the curve (λz). Other parameters,including AUC zero to infinity (AUCinf), clearance (CL), mean residencetime (MRT) and volume of distribution at steady state (Vss), concentra-tion at the last timepoint evaluated (Clast) and themaximumconcentra-tion achieved (Cmax) were subsequently calculated by the softwareusing the non-compartmental equations. In addition, the targeting effi-ciency ratio for the different formulationswas also calculated. Statisticalsignificance was determined by one-way ANOVA followed by Tukey'smultiple comparison post-test.
3. Results and discussion
3.1. Biodistribution analysis of 17-βE and its metabolites ESS and EST inplasma
As reported in our previous study, the 17-βE loaded cationicnanoemulsion had a size of ~140 nm and a charge of ~30 mV,[11]while the 17-βE loaded CREKA-peptidemodified nanoemulsion systemhad a size of ~175 nm and charge of ~−53 mV (Table 1). On
inetic parameters of 17-βE, ESS and EST in plasma evaluated by Noncompartmental analysison (DOTAP) (n = 3) and CREKA-peptide modified nanoemulsion systems (n = 4) ine time, t1/2 = Half life, (λz) = slope of the log-linear terminal part of the curve, CL =
EST
DOTAP NE CREKA NE Solution DOTAP NE CREKA NE
40.6 ± 3.0 186.6 ± 10.9 18.0 ± 1.1 9.7 ± 0.5 109.7 ± 10
30.1 92.9 113.9 137 94.720.5 63.2 78.5 97.1 64.10.034 0.011 0.0083 0.0071 0.0108

120 D. Deshpande et al. / Journal of Controlled Release 180 (2014) 117–124
intravenous administration, at all time points, an increase in levels of17-βE in plasma was observed with the CREKA-peptide-modifiednanoemulsion system relative to the solution and the cationicnanoemulsion system (DOTAP) (Fig. 1). Plasma 17-βE exposure, asreflected by AUClast and AUCinf, was higher (5.8-fold higher AUClast, 7.6fold higher AUCinf) with the CREKA-peptide modified nanoemulsionsystem as compared to the solution form (Table 2). The slower elimina-tion with the CREKA-peptide modified nanoemulsion system, was at-tributed to the encapsulation of 17-βE within the oil-core of thenanoemulsion droplet, which prevented immediate inactivation/biotransformation of 17-βE, and also to the PEG chains that decreasedthe opsonization process and increased the circulation time of thenanoemulsion droplets within blood [21,22].
Contrastingly, for the cationic formulation (DOTAP) a decreased ex-posure of 17-βE (2.2 fold lower AUClast) was observed due to increasedVss and CL (2.3 and 2.2 fold respectively) as compared to solution formu-lation. While the major components of the two-nanoemulsion systemswere similar, addition of DOTAP imparted a net positive surface chargeto the cationic nanoemulsion system. The cationic charge along with anaverage droplet size greater than 100 nm presumably led to theopsonization/macrophage uptake of this formulation [23]. This observa-tion was in line with results reported with other nanoformulations —neutral liposomes had a longer half-life than the negatively charged lipo-somes, while the cationic liposomes were rapidly cleared from systemiccirculation [24–27]. The PEG incorporated into the DOTAP formulationcould not neutralize the cationic surface charge of the nanoemulsion sys-tem and thus could not prevent the opsonization of the formulation.
The PK profile of the metabolites, when compared across the threeformulations administered, showed greater concentrations of themetabolites in plasma when the parent compound 17-βE was adminis-tered using the CREKA-peptide modified nanoemulsion system (Fig. 1).Intravenous administration of 17-βE, using the CREKA-peptide modi-fied nanoemulsion system showed a 3.5 fold and 6-fold greater concen-tration of themetabolites ESS and EST in plasma relative to the exposure
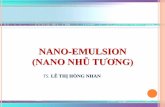
Fig. 2.Heart and aorta concentrations of 17-βE, ESS and EST on intravenous dosing using the natissue) versus time data from the heart and aorta tissue, following intravenous administrationmodified nanoemulsion systems (n = 4) in mice. Data represented as mean and standard dev
observed on intravenous administration of the 17-βE solution (Table 2).Intravenous administration of 17-βE using the cationic nanoemulsionsystem (DOTAP) showed much lower levels of metabolites ESS andEST in plasma as compared to the levels measured on intravenousadministration of 17-βE solution system.
The higher metabolite levels observed after CREKA-peptide modi-fied nanoemulsion system administration paralleled and were ascribedto the higher parent compound level observed in the systemic circula-tion with the use of the CREKA-peptide modified formulation. Circulat-ing levels of the parent compound were the rate-limiting factor of themetabolite kinetics. While it is well known that 17-βE undergoesrapid metabolism into more polar species [17], our studies showedthat themetabolite ESSwas eliminated faster than 17-βE from systemiccirculation. On the other hand, the metabolite EST was eliminatedslower than the parent compound from the systemic circulation. As ob-served (Table 2), the ratio of the t1/2 values for ESS relative to the parentcompound 17-βEwasmostly less than or equal to unity, while the sameratio for ESTwas equal to or greater than zero in case of all the three for-mulations on intravenous administration. A ratio lower than unity im-plied rapid elimination or biotransformation of ESS relative to theparent compound while a ratio greater than unity implied slower elim-ination/biotransformation of the metabolite EST relative to the parentcompound. The ratio of ESS and EST relative to 17-βE in case of admin-istration using the CREKA-peptide modified formulation was close tounity. This wasmainly due to the slowermetabolism of the parent com-pound 17-βE when administered using the CREKA-peptide modifiednanoemulsion system and not due to a different elimination rate forthemetabolites. Lastly, the AUClast values further validated the differentrates of elimination/biotransformation of the metabolites ESS and ESTrelative to the parent compound. The AUClast values of ESS were be-tween 71 and 201% of AUClast of 17-βE, which indicated a high rate ofbiotransformation for ESS and the AUClast of EST were between 40 and48% of AUClast of 17-βE, which indicated a relatively lower rate of bio-transformation for EST.
noemulsion system. The concentrations of 17-βE, ESS and EST (%ID=% Injected dose/g ofof 17-βE in solution (n= 4), cationic nanoemulsion (DOTAP) (n = 3) and CREKA-peptideiation of tissue concentration versus time.

Fig. 3. Liver and kidney concentrations of 17-βE, ESS and EST on intravenous dosing using the nanoemulsion system. The concentrations of 17-βE, ESS and EST (%ID=% Injected dose/g oftissue) versus time data from the liver and kidney tissue, following intravenous administration of 17-βE in solution (n= 4), cationic nanoemulsion (DOTAP) (n= 3) and CREKA-peptidemodified nanoemulsion (n = 4). Data represented as mean and standard deviation of tissue concentration versus time.
121D. Deshpande et al. / Journal of Controlled Release 180 (2014) 117–124
Thus, within an hour of intravenous administration of 17-βE usingthe solution, and the DOTAP nanoemulsion system, the circulatinglevels of the parent compound as well as the metabolites decreased toless than 5% of the injected dose. Similar PK parameters and distributionprofile of 17-βE solution have been observed in humans and rats withslight species based differences on systemic administration of 17-βE so-lution [29–31]. However, in our study, at all time points, the circulatinglevels of both the parent compound and metabolites ESS and EST inplasma were significantly greater when administered using theCREKA-peptide modified nanoemulsion system relative to the solutionas well as the DOTAP nanoemulsion system.
3.2. Biodistribution analysis of 17-βE and its metabolites ESS and EST inheart, aorta, liver and kidney
The heart–aorta and liver–kidney concentration-time data for 17-βEand themetabolites ESS and EST, after intravenous administration of thesolution, cationic nanoemulsion (DOTAP) and CREKA-peptide modifiednanoemulsion system has been reported in Figs. 2 and 3 respectively. Atmost times, an increase in the 17-βE concentrations was observed onadministration using the CREKA-peptide modified nanoemulsion sys-tem as compared to the solution and cationic nanoemulsion treatment.While performing the non-compartmental analysis, λz (slope of thelog-linear terminal part of the curve) could not be evaluated accuratelyhence the biodistribution results were calculated based on the ratio ofClast/Cmax as a reflection of residence time of the parent compoundand the metabolites within the organs, as reported in Table 3. and onAUClast (Fig. 4), as a reflection of tissue exposure.
The Clast/Cmax ratios (Table 4) for 17-βE and themetabolites ESS andEST for both the CREKA-peptidemodified nanoemulsion system and thecationic nanoemulsion (DOTAP) in all studied target and perfusedorganswere higher than the ratio for the solution treatment group, sug-gesting a higher residence of 17-βE and metabolites on delivery usingthe nanoemulsion system. However, the lower level of exposure of
17-βE and themetabolites ESS and EST with the cationic nanoemulsionleads to an overall lower accumulation of 17-βE within the tissues.
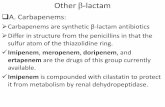
The AUClast of 17-βE (Fig. 4) showed a 3.7 fold increase in the heart,6.8 fold increase in the aorta, a 2.0 fold increase in the liver and a 1.9 foldincrease in the kidney when administered using the CREKA-peptidemodified nanoemulsion system, as compared to the solution treatmentgroup. For the cationic nanoemulsion, organ exposure was similar asfor solution, except for a 25 fold lower kidney AUClast. Trends with me-tabolites were similar to the parent compound. The metabolic profile of17-βE has been extensively studied and the steroid shows highest accu-mulation in the liver where it undergoes rapid metabolism [28]. Whilethe molecule mainly undergoes hydroxylation and oxidation to formmore polar species, it is eliminated primarily through the urine as sul-fate and glucuronide conjugates [28]. There is rapid interconversion be-tween the different 17-βE conjugates in the liver, with enterohepaticcirculation being the primary source and regulating site of the circulat-ing 17-βE levels [32]. Thus in our study, on intravenous administrationof the three formulations, 17-βE and the metabolites ESS and ESTaccounted for less than 10% of the total radioactivity in the liver and asubstantially higher radioactivity could have been observed on includ-ing the other metabolites in this study. A comparative evaluation of17-βE metabolism in the liver microsomes of rats, beagle dogs andhumans revealed rapid formation of 9 major phase-I metabolites of17-βE in the three species [33]. However, the relative amount of eachmetabolite produced was different across the three species [33].
To better compare the three formulations in the study, we calculatedthe targeting efficiency parameter for 17-βE using the formulaTargeting Efficiency (TE) = (AUClast Aorta + AUClast Heart + AUClastPlasma) / (AUClast Kidney + AUClast Liver). Both the nanoemulsionformulations – CREKA-peptide modified and cationic (DOTAP)nanoemulsion system – achieved a similar and better targeting efficien-cy than the solution treatment (Fig. 5). However, the cationicnanoemulsion treatment did not achieve higher exposure of the targetorgans as compared to the solution treatment, but TE was high mainly

Fig. 4. Biodistribution of 17-βE, ESS and EST in different organs measured as AUClast tocompare the tissue exposure upon intravenous administration The pharmacokinetic pa-rameter AUClast for 17-βE, ESS and EST in the plasma, heart, aorta, liver and kidney follow-ing intravenous administration of 17-βE in the solution (n = 4), cationic nanoemulsion(DOTAP) (n = 3) and CREKA-peptide modified nanoemulsion systems (n = 4) in mice.The AUClast values were compared between the different treatment groups and statisticalsignificance was determined by one way ANOVA followed by the Tukey's multiple com-parisons post test. *p b 0.05, **p b 0.01 and ***p b 0.001 were used for comparison tothe solution form and+p b 0.05, ++p b 0.01 and+++p b 0.001were used for compar-ison to the cationic formulation (DOTAP).
Table 3Plasma PKparameters ratio ofmetabolites ESS and EST relative to 17-pE after intravenous dosing. Comparison of pharmacokinetic parameters of themetabolites ESS and EST versus 17-PE(parent compound) in plasma following intravenous administration of 17-PE in the solution (n = 4), cationic nanoemulsion (DOTAP) (n = 3) and CREKA-peptide modifiednanoemulsion systems (n = 4) in mice. The parameters have been reported as a ratio of the metabolites versus the parent compound.
Solution DOTAP nanoemulsion CREKA nanoemulsion
ESS/17-pE EST/17-0E ESS/17-pE EST/17-PE ESS/17-PE EST/17-PE
λz 1.42 0.53 1.7 0.36 0.99 0.97t1/2 0.7 1.88 0.59 2.79 1.01 1.03Cmax 0.74 0.21 2.44 0.45 0.61 0.26Clast 1.19 0.73 1.35 0.7 0.96 0.56AUClast 1.18 0.4 2.01 0.48 0.71 0.42AUCINF 1.08 0.69 1.65 0.92 0.83 0.49MRTINF 0.88 2.38 0.62 2.81 1.17 1.19
122 D. Deshpande et al. / Journal of Controlled Release 180 (2014) 117–124
due to a very low kidney exposure. The primary reason for lesser expo-sure and rapid clearance of 17-βE on delivery using the cationic(DOTAP) nanoemulsion system could be the positive surface charge ofthe nanoemulsion. The rationale for incorporation of a cationic lipid –
DOTAP into the nanoemulsion system was to develop a positivelycharged nanocarrier to enhance the uptake of the droplets at the tissuesite through membrane based endocytosis [34]. The surface chargehowever, induced increased interaction of the nanoemulsion dropletswith non-specific plasma proteins that led to the process ofopsonization [35]. As described previously, the positive surface chargewith a droplet size greater than 100 nm undergoes opsonization,which leads to greater accumulation within the organs of the MPS(mononuclear phagocytic system), thus reducing the accumulationwithin the kidneys [36]. In addition, while positively chargedmoleculesundergo rapid glomerular filtration, the droplet size greater than~100 nm, limits the accumulation and filtration through the kidneys[37,38].
Based on the PK parameters evaluated, the cationic nanoemulsionwas considered unsuitable for systemic administration to test for its ef-fect on experimental atherosclerosis. However, the formulation mayprove beneficial on local delivery into damaged vessels, where thepositive surface charge could aid in rapid uptake within the damagedvessels, a hypothesis based on our previous in vitro cell-based resultsand the targeting efficiency observed in the PK analysis.
In the current study, the CREKA-peptidemodified nanoemulsion sys-tem showed greater exposure and an improved PK profile for 17-βE onintravenous administration, as compared to the 17-βE solution andDOTAP nanoemulsion system. The improved circulation and distributionwas mainly due to the encapsulation within the hydrophobic core,protective stealth layer of PEG and a net negative surface charge. TheCREKA-peptide was incorporated to achieve targeting of the atheroscle-rosis prone tissues — aortic sinus in the heart and the aorta, which areprone to plaque initiation and progression. Previous studies have report-ed the targeting benefits of the CREKA-peptide within atheroscleroticplaques in ApoE-null mice fed with a high fat diet [12,13]. In addition,several researchers have reported the cardioprotective benefits of17-βE in reducing plaque areas and thus in the treatment of atherosclero-sis [4–6]. It has been reported that the beneficial effects of 17-βE dependon the dose and route of administrationwith risks andbenefits associatedwith each of the routes [39].Whilemost studies have explored the subcu-taneous route of 17-βE administrations, a systemic approach that canprolong the circulation of 17-βE, and efficiently target the plaque regionscan prove significantly beneficial in the treatment of atherosclerosis in amurine model. Further study investigating the efficacy and plasma/target tissue distribution of 17-βE in a suitablemodel of atherosclerosis,delivered using the CREKA-peptidemodified nanoemulsionwould helpevaluate the therapeutic potential of this system.
4. Conclusions
The pharmacokinetics parameters, biodistribution studies and cal-culated targeting efficiency ratios clearly demonstrated the increased
exposure of 17-βE in the plasma, heart and aorta and even in the liverand kidney when 17-βE was delivered using the CREKA-peptidemodified nanoemulsion formulation as compared to the solution and

Table 4Comparison of Clast/Cmax ratios of 17-pE, ESS and EST to compare the residence time of 17-pE in tissues upon intravenous administration using the nanoemulsion system. The ratio of C /Cfor 17-PE, ESS and EST in plasma, heart, lastmax aorta, liver and kidney following intravenous administration of 17-PE in the solution (n= 4), cationic nanoemulsion (DOTAP) (n= 3)and CREKA-peptide modified nanoemulsion systems (n = 4) in mice.
Solution DOTAP CREKA Solution DOTAP CREKA Solution DOTAP CREKA
17-βE 17-βE 17-βE ESS ESS ESS EST EST EST
Plasma 0.2 0.3 0.2 0.3 0.1 0.4 0.6 0.4 0.5Heart 0.3 0.7 0.8 0.3 1 0.9 0.4 0.9 0.6Aorta 0.3 0.9 0.8 0.3 0.7 1 0.5 0.7 1Kidney 0.3 1 0.6 0.5 1 0.5 0.6 1 0.5Liver 0.3 0.8 0.9 0.2 0.7 0.9 0.3 1 1
123D. Deshpande et al. / Journal of Controlled Release 180 (2014) 117–124
cationic (DOTAP) nanoemulsion system. The CREKA-peptide modifiednanoemulsion system showed greater exposure of 17-βE to plasmaand target organs, had a high targeting efficiency compared to the solu-tion group and also showed greater circulation/retention of the non-metabolized 17-βE in plasma and tissues as compared to the solutionand the cationic (DOTAP) nanoemulsion system. These significant PKdifferences and beneficial targeting effects demonstrated that theCREKA-peptide modified, omega-3 fatty acid-based nanoemulsion canoffer a delivery platform with the potential to efficiently deliver 17-βEto atherosclerotic lesions.
Conflict of interest
The authors declare that they have no conflict of interest.
Acknowledgments
This study was performed in the radioactive core facility at North-eastern University in Dr. Samuel Gatley's laboratory and the authorswish to thank him for his help with the study design and experimentalsetup. The authorswould also like to thankKinjal Sankhe for assisting inthe beginning of this study.
Fig. 5. The targeting efficiency of 17-βE on intravenous delivery using solution, cationicnanoemulsion (DOTAP) or CREKA-peptide modified nanoemulsion system. The targetingefficiency for 17-βE was calculated based on AUClast. The rations were compared betweenthe different treatment groups and statistical significance was determined by one wayANOVA followed by the Tukey's multiple comparisons post test. *p b 0.05, **p b 0.01 and***p b 0.001 were used for comparison to the solution form and +p b 0.05, ++p b 0.01and +++p b 0.001 were used for comparison to the cationic formulation (DOTAP).
References
[1] A.S. Go, D.Mozaffarian, V.L. Roger, E.J. Benjamin, J.D. Berry,W.B. Borden, D.M. Bravata, S.Dai, E.S. Ford, C.S. Fox, S. Franco, H.J. Fullerton, C. Gillespie, S.M. Hailpern, J.A. Heit, V.J.Howard, M.D. Huffman, B.M. Kissela, S.J. Kittner, D.T. Lackland, J.H. Lichtman, L.D.Lisabeth, D. Magid, G.M. Marcus, A. Marelli, D.B. Matchar, D.K. McGuire, E.R. Mohler,C.S. Moy, M.E. Mussolino, G. Nichol, N.P. Paynter, P.J. Schreiner, P.D. Sorlie, J. Stein,T.N. Turan, S.S. Virani, N.D. Wong, D. Woo, M.B. Turner, Executive summary: heart dis-ease and stroke statistics—2013 update: a report from theAmericanHeart Association,Circulation 127 (2013) 143–152.
[2] S. Kasim, D. Moran, E. McFadden, Vulnerable plaque: from bench to bedside; localpacification versus systemic therapy, Heart Views 13 (2012) 139–145.
[3] A. Jayagopal, M.F. Linton, S. Fazio, F.R. Haselton, Insights into atherosclerosis usingnanotechnology, Curr. Atheroscler. Rep. 12 (2010) 209–215.
[4] B. Chandrasekar, S. Nattel, J.F. Tanguay, Coronary artery endothelial protectionafter local delivery of 17beta-estradiol during balloon angioplasty in a porcinemodel: a potential new pharmacologic approach to improve endothelial function,J. Am. Coll. Cardiol. 38 (2001) 1570–1576.
[5] Y. Han, M. Liang, J. Kang, Y. Qi, J. Deng, K. Xu, C. Yan, Estrogen-eluting stent implan-tation inhibits neointimal formation and extracellular signal-regulated kinase acti-vation, Catheter. Cardiovasc. Interv. 70 (2007) 647–653.
[6] A.C. Villablanca, A. Tenwolde, M. Lee, M. Huck, S. Mumenthaler, J.C. Rutledge,17beta-estradiol prevents early-stage atherosclerosis in estrogen receptor-alpha de-ficient female mice, J. Cardiovasc. Transl. Res. 2 (2009) 289–299.
[7] H.N. Hodis, W.J. Mack, S.P. Azen, R.A. Lobo, D. Shoupe, P.R. Mahrer, D.P. Faxon, L.Cashin-Hemphill, M.E. Sanmarco, W.J. French, T.L. Shook, T.D. Gaarder, A.O. Mehra,R. Rabbani, A. Sevanian, A.B. Shil, M. Torres, K.H. Vogelbach, R.H. Selzer, Hormonetherapy and the progression of coronary-artery atherosclerosis in postmenopausalwomen, N. Engl. J. Med. 349 (2003) 535–545.
[8] T. Fait, M. Vrablik, Coronary heart disease and hormone replacement therapy —
from primary and secondary prevention to the window of opportunity,Neuroendocrinol. Lett. 33 (2012) 17–21.
[9] R.L. Prentice, R. Langer, M.L. Stefanick, B.V. Howard, M. Pettinger, G. Anderson, D.Barad, J.D. Curb, J. Kotchen, L. Kuller, M. Limacher, J. Wactawski-Wende, Combinedpostmenopausal hormone therapy and cardiovascular disease: toward resolvingthe discrepancy between observational studies and the Women's Health Initiativeclinical trial, Am. J. Epidemiol. 162 (2005) 404–414.
[10] J.W. Yoo, C.H. Lee, Drug delivery systems for hormone therapy, J. Control. Release112 (2006) 1–14.
[11] D. Deshpande, D.R. Janero, M. Amiji, Engineering of an omega-3 polyunsaturatedfatty acid-containing nanoemulsion system for combination C6-ceramide and17beta-estradiol delivery and bioactivity in human vascular endothelial and smoothmuscle cells, Nanomedicine: NBM (2013) 885–894.
[12] D. Peters, M. Kastantin, V.R. Kotamraju, P.P. Karmali, K. Gujraty, M. Tirrell, E.Ruoslahti, Targeting atherosclerosis by using modular, multifunctional micelles,Proc. Natl. Acad. Sci. U. S. A. 106 (2009) 9815–9819.
[13] J. Hamzah, V.R. Kotamraju, J.W. Seo, L. Agemy, V. Fogal, L.M. Mahakian, D. Peters, L.Roth, M.K. Gagnon, K.W. Ferrara, E. Ruoslahti, Specific penetration and accumulationof a homing peptide within atherosclerotic plaques of apolipoprotein E-deficientmice, Proc. Natl. Acad. Sci. U. S. A. 108 (2011) 7154–7159.
[14] P.A. Bourassa, P.M. Milos, B.J. Gaynor, J.L. Breslow, R.J. Aiello, Estrogen reduces ath-erosclerotic lesion development in apolipoprotein E-deficient mice, Proc. Natl.Acad. Sci. U. S. A. 93 (1996) 10022–10027.
[15] B.T. Zhu, A.H. Conney, Functional role of estrogen metabolism in target cells: reviewand perspectives, Carcinogenesis 19 (1998) 1–27.
[16] C.M. White, M.J. Ferraro-Borgida, A.T. Fossati, C.C. McGill, A.W. Ahlberg, Y.J. Feng,G.V. Heller, M.S. Chow, The pharmacokinetics of intravenous estradiol — a prelimi-nary study, Pharmacotherapy 18 (1998) 1343–1346.
[17] Y. Tsuchiya, M. Nakajima, T. Yokoi, Cytochrome P450-mediated metabolism of es-trogens and its regulation in human, Cancer Lett. 227 (2005) 115–124.
[18] F.R. Fullerton, D.L. Greenman, J.F. Young, Influence of a purified diet and route of ad-ministration on the metabolism and disposition of estradiol in B6C3F1 mice, DrugMetab. Dispos. Biol. Fate Chem. 15 (1987) 602–607.
[19] G.C. Crowell, M.E. Turner Jr., F.H. Schmidt, C.M. Howard, J.R. Preedy, Estrogenmetab-olism in the human. I. Studies in the male using estrone-6,7-3H, with special

124 D. Deshpande et al. / Journal of Controlled Release 180 (2014) 117–124
reference to estrone production rate determinations, the origin of certain urinary es-trogen conjugates, and the use of a new mathematical model, J. Clin. Endocrinol.Metab. 27 (1967) 807–818.
[20] R. Hobkirk, M. Nilsen, P.R. Blahey, Conjugation of urinary phenolic steroids in thenonpregnant human female with particular reference to estrone sulfate, J. Clin.Endocrinol. Metab. 29 (1969) 328–337.
[21] L.E. van Vlerken, T.K. Vyas, M.M. Amiji, Poly(ethylene glycol)-modifiednanocarriers for tumor-targeted and intracellular delivery, Pharm. Res. 24(2007) 1405–1414.
[22] S. Ganta, P. Sharma, J.W. Paxton, B.C. Baguley, S. Garg, Pharmacokinetics and phar-macodynamics of chlorambucil delivered in long-circulating nanoemulsion, J. DrugTarget. 18 (2010) 125–133.
[23] M. Longmire, P.L. Choyke, H. Kobayashi, Clearance properties of nano-sized particlesand molecules as imaging agents: considerations and caveats, Nanomedicine 3(2008) 703–717.
[24] M.L. Immordino, F. Dosio, L. Cattel, Stealth liposomes: review of the basic science, ra-tionale, and clinical applications, existing and potential, Int. J. Nanomedicine 1(2006) 297–315.
[25] K.Y.R.K.H. Funato, Contribution of complement system on destabilization ofliposomes composed of hydrogenated egg phosphatidylcholine in rat fresh plasma,Biochim. Biophys. Acta 1103 (1992) 198–204.
[26] K. Nishikawa, H. Arai, K. Inoue, Scavanger receptor-mediated uptake and metabo-lism of lipid vesicles containing acidic phospholipids by mouse peritoneal macro-phages, J. Biol. Chem. 265 (1990) 5226–5231.
[27] J.H. Senior, Fate and behavior of liposomes in vivo: a review of controlling factors,Crit. Rev. Ther. Drug Carrier Syst. 3 (1987) 123–193.
[28] Y. Tsuchiya, M. Nakajima, T. Yokoi, Cytochrome P450-mediated metabolism of es-trogens and its regulation in human, Cancer Lett. 227 (2005) 115–124.
[29] D.R. Plowchalk, J. Teeguarden, Development of a physiologically based pharmacoki-netic model for estradiol in rats and humans: a biologically motivated quantitative
framework for evaluating responses to estradiol and other endocrine-active com-pounds, Toxicol. Sci. 69 (2002) 60–78.
[30] C.J. Mathias, M.J. Welch, J.A. Katzenellenbogen, J.W. Brodack, M.R. Kilbourn, K.E.Carlson, D.O. Kiesewetter, Characterization of the uptake of 16 α-([18F]fluoro)-17β-estradiol in DMBA-induced mammary tumors, Int. J. Radiat. Appl. Instrum. PartB Nucl. Med. Biol. 14 (1987) 15–25.
[31] C.M. White, M.J. Ferraro-Borgida, A.T. Fossati, C.C. McGill, A.W. Ahlberg, Y.J. Feng,G.V. Heller, M.S. Chow, The pharmacokinetics of intravenous estradiol — a prelimi-nary study, Pharmacotherapy 18 (1998) 1343–1346.
[32] H.M. Bolt, Metabolism of estrogens — natural and synthetic, Pharmacol. Ther. 4(1979) 155–181.
[33] Y.Q. Song, J. Liao, H.W. Liu, C.H. Ai, F. Zhang, In vivo comparison of estradiol metab-olism in liver microsomes of human, Beagle dog and rat, Yao Xue Xue Bao 47 (2012)210–215.
[34] C.R. Miller, B. Bondurant, S.D. McLean, K.A. McGovern, D.F. O'Brien, Liposome–cellinteractions in vitro: effect of liposome surface charge on the binding and endocyto-sis of conventional and sterically stabilized liposomes, Biochemistry 37 (1998)12875–12883.
[35] B. Romberg, W.E. Hennink, G. Storm, Sheddable coatings for long-circulating nano-particles, Pharm. Res. 25 (2008) 55–71.
[36] D.E. Owens III, N.A. Peppas, Opsonization, biodistribution, and pharmacokinetics ofpolymeric nanoparticles, Int. J. Pharm. 307 (2006) 93–102.
[37] E. Vegt, M. de Jong, J.F. Wetzels, R. Masereeuw, M. Melis, W.J. Oyen, M. Gotthardt,O.C. Boerman, Renal toxicity of radiolabeled peptides and antibody fragments:mechanisms, impact on radionuclide therapy, and strategies for prevention, J.Nucl. Med. 51 (2010) 1049–1058.
[38] B. Haraldsson, J. Nystrom, W.M. Deen, Properties of the glomerular barrier andmechanisms of proteinuria, Physiol. Rev. 88 (2008) 451–487.
[39] T.S. Mikkola, T.B. Clarkson, Estrogen replacement therapy, atherosclerosis, and vas-cular function, Cardiovasc. Res. 53 (2002) 605–619.