Ch22: Pigmentations of the Oral Mucosa and Facial Skin
10
218 Blue, gray, and black skin and mucosal pigmented lesions are usually attributable to exogenous tattoos or melanin. Brown pigmentations are represented by either melanin or hemosiderin. Yellow discolorations may be the result of bilirubin deposition or the inges- tion of large amounts of β-carotene. Blue and purple discolorations are generally the consequence of vascu- lar lakes within the dermis or submucosal connective tissues. Pigmented lesions may be focal and macular or raised, or they may be diffuse or multifocal. In general, diffuse and multifocal pigmentation is attributable to melanosis, and there may be systemic or pharmacologic factors in the etiopathogenesis. The most common causes of oral pigmentations are genetic, related to eth- nicity, and those caused by accidental amalgam implan- tation (Table 22–1). Table 22–1 Pigmentations of the Facial Skin and Oral Mucosa Lesion Macular Nodular Papillary Focal Amalgam tattoo Compound and intradermal (mucosal) nevi Graphite tattoo Seborrheic keratosis (skin) Ephelis, melanotic macule, melanoacanthoma Angiomas, varices, Kaposi sarcoma Junctional nevus Melanoma Blue nevus Ecchymosis, petechia Macular hemangioma, Kaposi sarcoma Diffuse Physiologic (ethnic) pigmentation Malignant melanoma Acanthosis nigricans Addison disease, Cushing syndrome Kaposi sarcoma Black or brown hairy tongue McCune-Albright syndrome Neurofibromatosis Peutz-Jeghers syndrome Minocycline HIV-associated oral melanosis Smoker’s melanosis Melasma, chloasma Molecular and pathologic correlates of disease, 219 Focal pigmentations, 220 Melanotic macule, ephelis, 220 Melanocytic nevi, 220 Amalgam and graphite tattoo, 220 Ecchymosis, 221 Angiomas, 222 Melanoma, 223 Diffuse and multiple pigmentations, 224 Physiologic pigmentation, 224 Black or brown hairy tongue, 224 Smoker’s melanosis, 224 Addison disease, 225 Café au lait pigmentation, 225 Acanthosis nigricans, 225 Minocycline melanosis, 226 Melasma, chloasma, 226 Peutz-Jeghers syndrome, 226 Suggested reading, 226 22 Pigmentations of the Oral Mucosa and Facial Skin L. Roy Eversole, DDS, MSD, MA, and Sol Silverman, Jr, MA, DDS
Transcript of Ch22: Pigmentations of the Oral Mucosa and Facial Skin
218
Blue, gray, and black skin and mucosal pigmentedlesions are usually attributable to exogenous tattoos ormelanin. Brown pigmentations are represented byeither melanin or hemosiderin. Yellow discolorationsmay be the result of bilirubin deposition or the inges-tion of large amounts of β-carotene. Blue and purplediscolorations are generally the consequence of vascu-lar lakes within the dermis or submucosal connective
tissues. Pigmented lesions may be focal and macular orraised, or they may be diffuse or multifocal. In general,diffuse and multifocal pigmentation is attributable tomelanosis, and there may be systemic or pharmacologicfactors in the etiopathogenesis. The most commoncauses of oral pigmentations are genetic, related to eth-nicity, and those caused by accidental amalgam implan-tation (Table 22–1).
Table 22–1 Pigmentations of the Facial Skin and Oral Mucosa
Lesion Macular Nodular Papillary
Focal Amalgam tattoo Compound and intradermal (mucosal) neviGraphite tattoo Seborrheic keratosis (skin)Ephelis, melanotic macule, melanoacanthoma Angiomas, varices, Kaposi sarcomaJunctional nevus MelanomaBlue nevusEcchymosis, petechiaMacular hemangioma, Kaposi sarcoma
Diffuse Physiologic (ethnic) pigmentation Malignant melanoma Acanthosis nigricansAddison disease, Cushing syndrome Kaposi sarcoma Black or brown hairy tongueMcCune-Albright syndromeNeurofibromatosisPeutz-Jeghers syndromeMinocycline HIV-associated oral melanosisSmoker’s melanosisMelasma, chloasma
Molecular and pathologic correlates
of disease, 219
Focal pigmentations, 220
Melanotic macule, ephelis, 220
Melanocytic nevi, 220
Amalgam and graphite tattoo, 220
Ecchymosis, 221
Angiomas, 222
Melanoma, 223
Diffuse and multiple pigmentations, 224
Physiologic pigmentation, 224
Black or brown hairy tongue, 224
Smoker’s melanosis, 224
Addison disease, 225
Café au lait pigmentation, 225
Acanthosis nigricans, 225
Minocycline melanosis, 226
Melasma, chloasma, 226
Peutz-Jeghers syndrome, 226
Suggested reading, 226
22 Pigmentations of the Oral Mucosa and Facial SkinL. Roy Eversole, DDS, MSD, MA, and Sol Silverman, Jr, MA, DDS
P I G M E N T A T I O N S O F T H E O R A L M U C O S A A N D F A C I A L S K I N 219
Molecular and pathologic correlates of disease
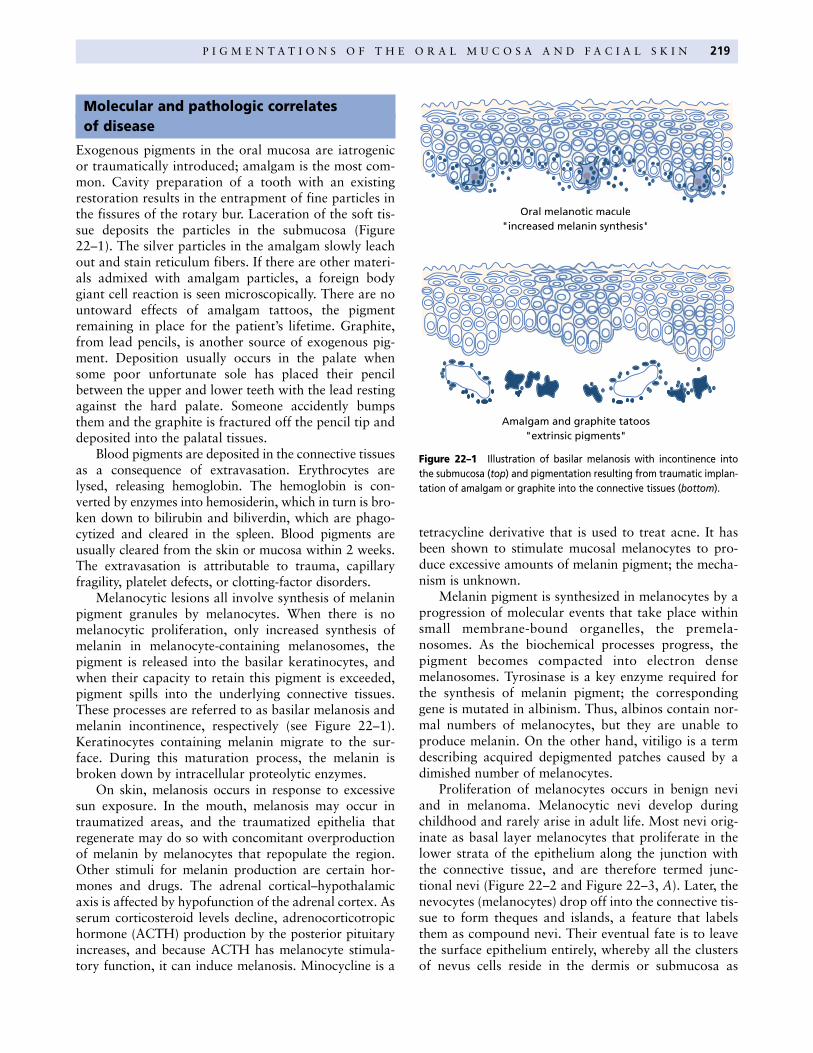
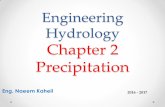
Exogenous pigments in the oral mucosa are iatrogenicor traumatically introduced; amalgam is the most com-mon. Cavity preparation of a tooth with an existingrestoration results in the entrapment of fine particles inthe fissures of the rotary bur. Laceration of the soft tis-sue deposits the particles in the submucosa (Figure22–1). The silver particles in the amalgam slowly leachout and stain reticulum fibers. If there are other materi-als admixed with amalgam particles, a foreign bodygiant cell reaction is seen microscopically. There are nountoward effects of amalgam tattoos, the pigmentremaining in place for the patient’s lifetime. Graphite,from lead pencils, is another source of exogenous pig-ment. Deposition usually occurs in the palate whensome poor unfortunate sole has placed their pencilbetween the upper and lower teeth with the lead restingagainst the hard palate. Someone accidently bumpsthem and the graphite is fractured off the pencil tip anddeposited into the palatal tissues.
Blood pigments are deposited in the connective tissuesas a consequence of extravasation. Erythrocytes arelysed, releasing hemoglobin. The hemoglobin is con-verted by enzymes into hemosiderin, which in turn is bro-ken down to bilirubin and biliverdin, which are phago-cytized and cleared in the spleen. Blood pigments areusually cleared from the skin or mucosa within 2 weeks.The extravasation is attributable to trauma, capillaryfragility, platelet defects, or clotting-factor disorders.
Melanocytic lesions all involve synthesis of melaninpigment granules by melanocytes. When there is nomelanocytic proliferation, only increased synthesis ofmelanin in melanocyte-containing melanosomes, thepigment is released into the basilar keratinocytes, andwhen their capacity to retain this pigment is exceeded,pigment spills into the underlying connective tissues.These processes are referred to as basilar melanosis andmelanin incontinence, respectively (see Figure 22–1).Keratinocytes containing melanin migrate to the sur-face. During this maturation process, the melanin isbroken down by intracellular proteolytic enzymes.
On skin, melanosis occurs in response to excessivesun exposure. In the mouth, melanosis may occur intraumatized areas, and the traumatized epithelia thatregenerate may do so with concomitant overproductionof melanin by melanocytes that repopulate the region.Other stimuli for melanin production are certain hor-mones and drugs. The adrenal cortical–hypothalamicaxis is affected by hypofunction of the adrenal cortex. Asserum corticosteroid levels decline, adrenocorticotropichormone (ACTH) production by the posterior pituitaryincreases, and because ACTH has melanocyte stimula-tory function, it can induce melanosis. Minocycline is a
tetracycline derivative that is used to treat acne. It hasbeen shown to stimulate mucosal melanocytes to pro-duce excessive amounts of melanin pigment; the mecha-nism is unknown.
Melanin pigment is synthesized in melanocytes by aprogression of molecular events that take place withinsmall membrane-bound organelles, the premela-nosomes. As the biochemical processes progress, thepigment becomes compacted into electron densemelanosomes. Tyrosinase is a key enzyme required forthe synthesis of melanin pigment; the correspondinggene is mutated in albinism. Thus, albinos contain nor-mal numbers of melanocytes, but they are unable toproduce melanin. On the other hand, vitiligo is a termdescribing acquired depigmented patches caused by adimished number of melanocytes.
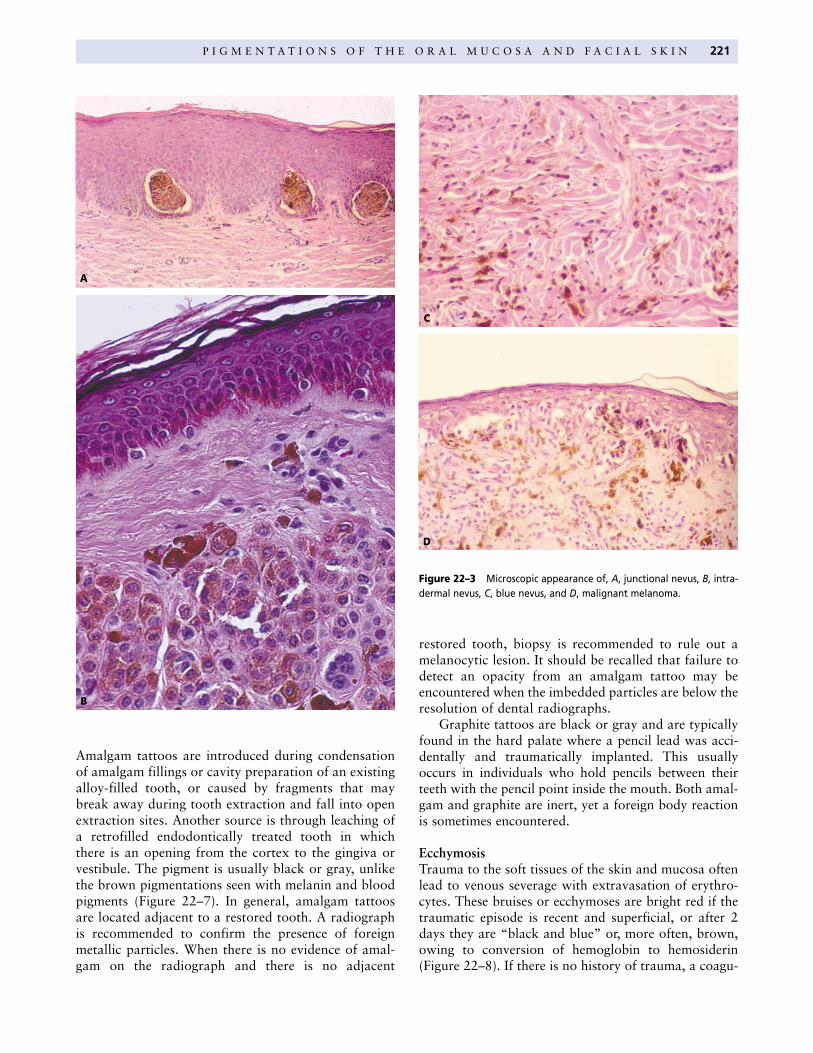
Proliferation of melanocytes occurs in benign neviand in melanoma. Melanocytic nevi develop duringchildhood and rarely arise in adult life. Most nevi orig-inate as basal layer melanocytes that proliferate in thelower strata of the epithelium along the junction withthe connective tissue, and are therefore termed junc-tional nevi (Figure 22–2 and Figure 22–3, A). Later, thenevocytes (melanocytes) drop off into the connective tis-sue to form theques and islands, a feature that labelsthem as compound nevi. Their eventual fate is to leavethe surface epithelium entirely, whereby all the clustersof nevus cells reside in the dermis or submucosa as
Amalgam and graphite tatoos"extrinsic pigments"
Oral melanotic macule"increased melanin synthesis"
Figure 22–1 Illustration of basilar melanosis with incontinence intothe submucosa (top) and pigmentation resulting from traumatic implan-tation of amalgam or graphite into the connective tissues (bottom).

220 C H A P T E R 2 2
intradermal or intramucosal nevi (Figure 22–3, B).Junctional activity is generally lost by age 18. Blue neviare unique in that they arise from dermal or mucosalmelanocytes that remained in the connective tissues dur-ing embryonic neural crest migration and, therefore, didnot evolve from junctional nevi. Blue nevi are comprisedof spindle-shaped melanocytes that synthesize copiousamounts of melanin pigment (Figure 22–3, C).
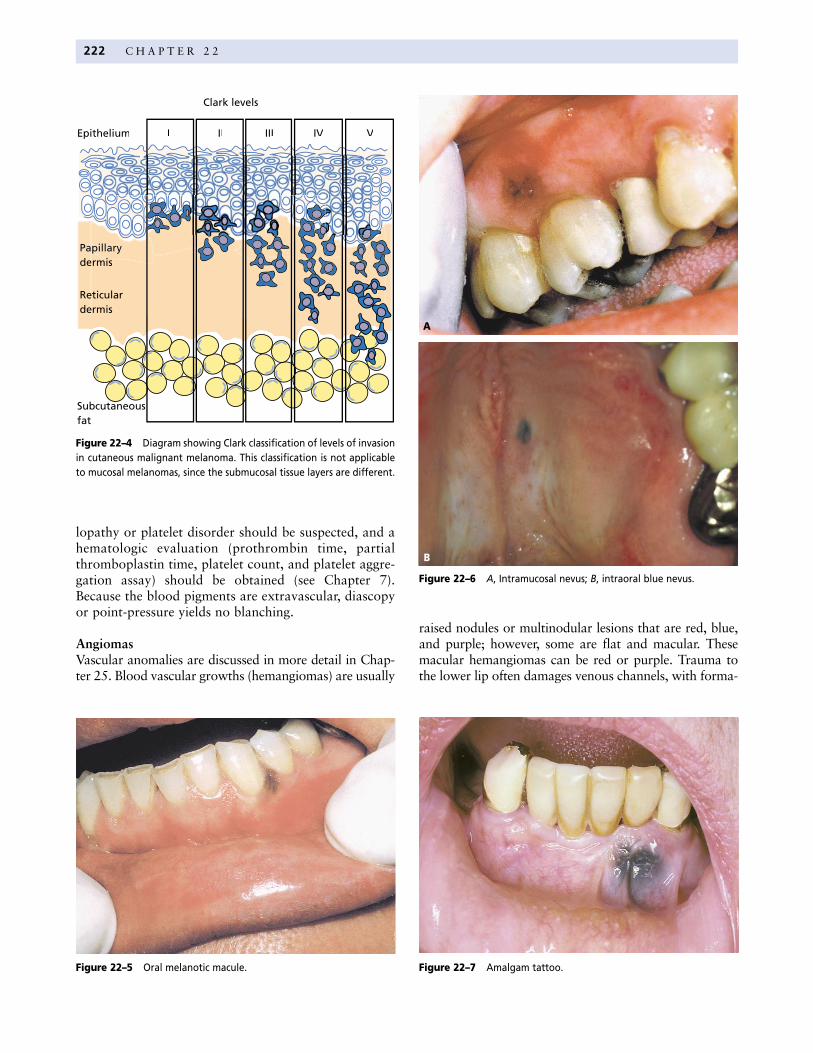
Malignant transformation of melanocytes can oftenbe attributed to genetic alterations that result from solarradiation. The earliest change is junctional. In an adult,junctional proliferation with nuclear atypia is referred toas atypical melanocytic hyperplasia. When cytologicatypia becomes more advanced, the lesions are superficialspreading melanomas (Figure 22–3, D). When invasionof the connective tissue ensues, they are invasive or nodu-lar melanomas and metastatic potential has been reached.There are pathologic stages that correlate the depth orlevel of invasion with survival. The Clark classification
system for skin is commonly used for this purpose (Fig-ure 22–4). Malignant melanocytes confined to the epithe-lium represents level I, invasion into the superficial papil-lary dermis is level II, invasion through the papillarydermis down to the reticular dermis is level III, invasionthrough the reticular dermis is level IV, and deep invasionof the subcutaneous fat is level V. The Breslow system uti-lizes a micrometer to precisely measure depth of invasion.
Focal pigmentations
Melanotic macule, ephelisEphelides, or freckles, are generated or intensified bysun exposure to the skin. They are commonly seen onthe faces of redheads and appear as small brown mac-ules. Focal macular pigmentations of the oral mucosaand lower lip are mucosal equivalents to the ephelis andare termed oral melanotic macules. On the lip, there isoften a history of trauma. Intraoral melanotic maculesare most often seen on the gingiva, palate, and lips, butcan be found anywhere in the mouth, including thetongue. They are usually small, brown or black, andhave smooth borders (Figure 22–5). Biopsy confirma-tion is recommended to rule out a melanocytic prolifer-ation. Melanotic macules are focal forms of basilarmelanosis, a nonproliferative process. A unique form ofmelanotic macule is the melanoacanthoma, a lesion usu-ally encountered in persons of native African descent.This form of macule is microscopically characterized bybasilar melanosis with concomitant presence of den-dritic, pigment-forming melanocytes spread throughoutan acanthotic spinous cell layer.
The differential diagnosis on the skin includessenile lentigo or age spots, melanoacanthoma, andsuperficial spreading melanoma The latter two canarise in oral mucosa.
Melanocytic neviAs previously discussed, junctional, compound, intra-mucosal, and blue nevi can arise on the face or in themouth. Junctional nevi are macular and brown, whereasblue nevi are black or blue, because the melanin pigmentis deep within the connective tissue (Figure 22–6). Com-pound and intramucosal nevi typically present as nod-ules that are round and symmetric. Most, yet not all,compound and intramucosal nevi are pigmented. On theface, nevi can arise in any location. In the mouth, neviare more often encountered on fixed mucosa of thepalate and gingiva. Biopsy is recommended to confirmthe diagnosis, because unlike skin nevi, oral nevi arerare, and it is prudent to obtain histologic confirmation.
Amalgam and graphite tattooTattoos are iatrogenic or factitial and represent themost common focal pigmentation of the oral mucosa.
Junctional nevus
Compound nevus
Intradermal nevus
Figure 22–2 Illustration of the progression of nevi from junctional tocompound to intramucosal (intradermal).
P I G M E N T A T I O N S O F T H E O R A L M U C O S A A N D F A C I A L S K I N 221
Amalgam tattoos are introduced during condensationof amalgam fillings or cavity preparation of an existingalloy-filled tooth, or caused by fragments that maybreak away during tooth extraction and fall into openextraction sites. Another source is through leaching ofa retrofilled endodontically treated tooth in whichthere is an opening from the cortex to the gingiva orvestibule. The pigment is usually black or gray, unlikethe brown pigmentations seen with melanin and bloodpigments (Figure 22–7). In general, amalgam tattoosare located adjacent to a restored tooth. A radiographis recommended to confirm the presence of foreignmetallic particles. When there is no evidence of amal-gam on the radiograph and there is no adjacent
restored tooth, biopsy is recommended to rule out amelanocytic lesion. It should be recalled that failure todetect an opacity from an amalgam tattoo may beencountered when the imbedded particles are below theresolution of dental radiographs.
Graphite tattoos are black or gray and are typicallyfound in the hard palate where a pencil lead was acci-dentally and traumatically implanted. This usuallyoccurs in individuals who hold pencils between theirteeth with the pencil point inside the mouth. Both amal-gam and graphite are inert, yet a foreign body reactionis sometimes encountered.
EcchymosisTrauma to the soft tissues of the skin and mucosa oftenlead to venous severage with extravasation of erythro-cytes. These bruises or ecchymoses are bright red if thetraumatic episode is recent and superficial, or after 2days they are “black and blue” or, more often, brown,owing to conversion of hemoglobin to hemosiderin(Figure 22–8). If there is no history of trauma, a coagu-
A
C
D
Figure 22–3 Microscopic appearance of, A, junctional nevus, B, intra-dermal nevus, C, blue nevus, and D, malignant melanoma.
B
222 C H A P T E R 2 2
lopathy or platelet disorder should be suspected, and ahematologic evaluation (prothrombin time, partialthromboplastin time, platelet count, and platelet aggre-gation assay) should be obtained (see Chapter 7).Because the blood pigments are extravascular, diascopyor point-pressure yields no blanching.
AngiomasVascular anomalies are discussed in more detail in Chap-ter 25. Blood vascular growths (hemangiomas) are usually
raised nodules or multinodular lesions that are red, blue,and purple; however, some are flat and macular. Thesemacular hemangiomas can be red or purple. Trauma tothe lower lip often damages venous channels, with forma-
Figure 22–7 Amalgam tattoo.
Figure 22–6 A, Intramucosal nevus; B, intraoral blue nevus.
A
B
Figure 22–5 Oral melanotic macule.
Clark levels
Epithelium I II III IV V
ermisiidee
Reticulardermis
Subcutaneousfat
Figure 22–4 Diagram showing Clark classification of levels of invasionin cutaneous malignant melanoma. This classification is not applicableto mucosal melanomas, since the submucosal tissue layers are different.
P I G M E N T A T I O N S O F T H E O R A L M U C O S A A N D F A C I A L S K I N 223
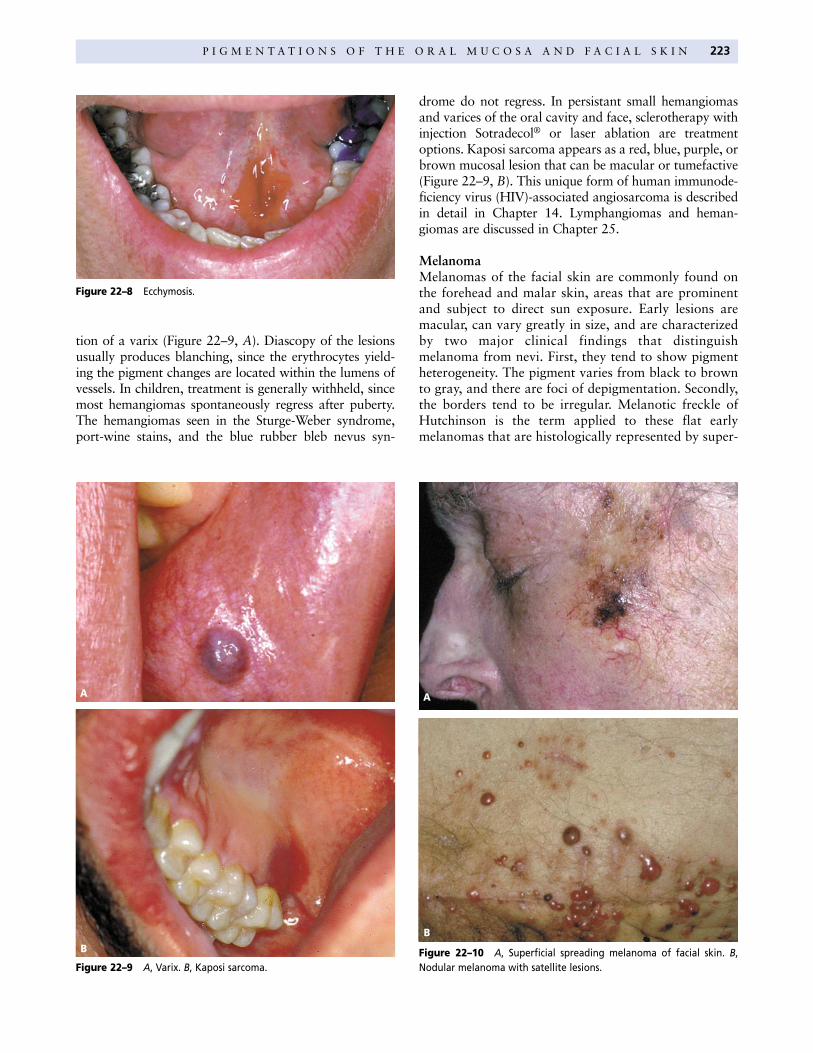
tion of a varix (Figure 22–9, A). Diascopy of the lesionsusually produces blanching, since the erythrocytes yield-ing the pigment changes are located within the lumens ofvessels. In children, treatment is generally withheld, sincemost hemangiomas spontaneously regress after puberty.The hemangiomas seen in the Sturge-Weber syndrome,port-wine stains, and the blue rubber bleb nevus syn-
drome do not regress. In persistant small hemangiomasand varices of the oral cavity and face, sclerotherapy withinjection Sotradecol® or laser ablation are treatmentoptions. Kaposi sarcoma appears as a red, blue, purple, orbrown mucosal lesion that can be macular or tumefactive(Figure 22–9, B). This unique form of human immunode-ficiency virus (HIV)-associated angiosarcoma is describedin detail in Chapter 14. Lymphangiomas and heman-giomas are discussed in Chapter 25.
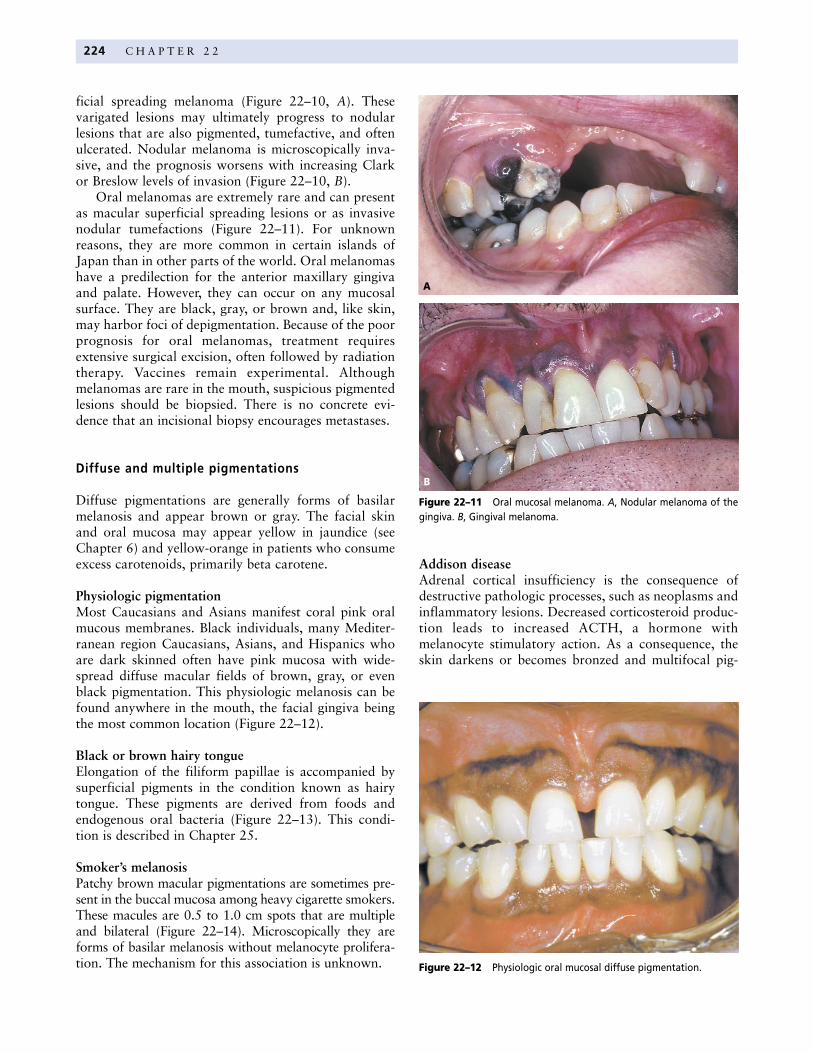
MelanomaMelanomas of the facial skin are commonly found onthe forehead and malar skin, areas that are prominentand subject to direct sun exposure. Early lesions aremacular, can vary greatly in size, and are characterizedby two major clinical findings that distinguishmelanoma from nevi. First, they tend to show pigmentheterogeneity. The pigment varies from black to brownto gray, and there are foci of depigmentation. Secondly,the borders tend to be irregular. Melanotic freckle ofHutchinson is the term applied to these flat earlymelanomas that are histologically represented by super-
Figure 22–9 A, Varix. B, Kaposi sarcoma.
A
B Figure 22–10 A, Superficial spreading melanoma of facial skin. B,Nodular melanoma with satellite lesions.
Figure 22–8 Ecchymosis.
A
B
224 C H A P T E R 2 2
ficial spreading melanoma (Figure 22–10, A). Thesevarigated lesions may ultimately progress to nodularlesions that are also pigmented, tumefactive, and oftenulcerated. Nodular melanoma is microscopically inva-sive, and the prognosis worsens with increasing Clarkor Breslow levels of invasion (Figure 22–10, B).
Oral melanomas are extremely rare and can presentas macular superficial spreading lesions or as invasivenodular tumefactions (Figure 22–11). For unknownreasons, they are more common in certain islands ofJapan than in other parts of the world. Oral melanomashave a predilection for the anterior maxillary gingivaand palate. However, they can occur on any mucosalsurface. They are black, gray, or brown and, like skin,may harbor foci of depigmentation. Because of the poorprognosis for oral melanomas, treatment requiresextensive surgical excision, often followed by radiationtherapy. Vaccines remain experimental. Althoughmelanomas are rare in the mouth, suspicious pigmentedlesions should be biopsied. There is no concrete evi-dence that an incisional biopsy encourages metastases.
Diffuse and multiple pigmentations
Diffuse pigmentations are generally forms of basilarmelanosis and appear brown or gray. The facial skinand oral mucosa may appear yellow in jaundice (seeChapter 6) and yellow-orange in patients who consumeexcess carotenoids, primarily beta carotene.
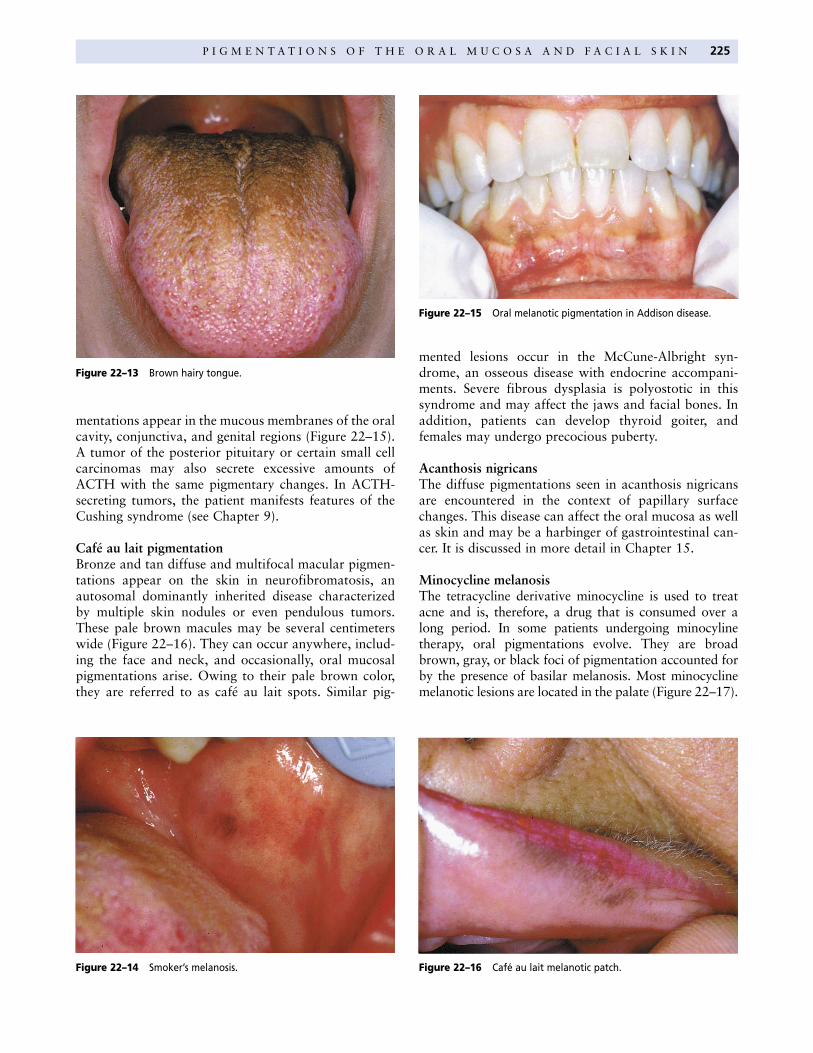
Physiologic pigmentationMost Caucasians and Asians manifest coral pink oralmucous membranes. Black individuals, many Mediter-ranean region Caucasians, Asians, and Hispanics whoare dark skinned often have pink mucosa with wide-spread diffuse macular fields of brown, gray, or evenblack pigmentation. This physiologic melanosis can befound anywhere in the mouth, the facial gingiva beingthe most common location (Figure 22–12).
Black or brown hairy tongueElongation of the filiform papillae is accompanied bysuperficial pigments in the condition known as hairytongue. These pigments are derived from foods andendogenous oral bacteria (Figure 22–13). This condi-tion is described in Chapter 25.
Smoker’s melanosisPatchy brown macular pigmentations are sometimes pre-sent in the buccal mucosa among heavy cigarette smokers.These macules are 0.5 to 1.0 cm spots that are multipleand bilateral (Figure 22–14). Microscopically they areforms of basilar melanosis without melanocyte prolifera-tion. The mechanism for this association is unknown.
Addison diseaseAdrenal cortical insufficiency is the consequence ofdestructive pathologic processes, such as neoplasms andinflammatory lesions. Decreased corticosteroid produc-tion leads to increased ACTH, a hormone withmelanocyte stimulatory action. As a consequence, theskin darkens or becomes bronzed and multifocal pig-
Figure 22–12 Physiologic oral mucosal diffuse pigmentation.
Figure 22–11 Oral mucosal melanoma. A, Nodular melanoma of thegingiva. B, Gingival melanoma.
B
A
P I G M E N T A T I O N S O F T H E O R A L M U C O S A A N D F A C I A L S K I N 225
mentations appear in the mucous membranes of the oralcavity, conjunctiva, and genital regions (Figure 22–15).A tumor of the posterior pituitary or certain small cellcarcinomas may also secrete excessive amounts ofACTH with the same pigmentary changes. In ACTH-secreting tumors, the patient manifests features of theCushing syndrome (see Chapter 9).
Café au lait pigmentationBronze and tan diffuse and multifocal macular pigmen-tations appear on the skin in neurofibromatosis, anautosomal dominantly inherited disease characterizedby multiple skin nodules or even pendulous tumors.These pale brown macules may be several centimeterswide (Figure 22–16). They can occur anywhere, includ-ing the face and neck, and occasionally, oral mucosalpigmentations arise. Owing to their pale brown color,they are referred to as café au lait spots. Similar pig-
mented lesions occur in the McCune-Albright syn-drome, an osseous disease with endocrine accompani-ments. Severe fibrous dysplasia is polyostotic in thissyndrome and may affect the jaws and facial bones. Inaddition, patients can develop thyroid goiter, andfemales may undergo precocious puberty.
Acanthosis nigricansThe diffuse pigmentations seen in acanthosis nigricansare encountered in the context of papillary surfacechanges. This disease can affect the oral mucosa as wellas skin and may be a harbinger of gastrointestinal can-cer. It is discussed in more detail in Chapter 15.
Minocycline melanosisThe tetracycline derivative minocycline is used to treatacne and is, therefore, a drug that is consumed over along period. In some patients undergoing minocylinetherapy, oral pigmentations evolve. They are broadbrown, gray, or black foci of pigmentation accounted forby the presence of basilar melanosis. Most minocyclinemelanotic lesions are located in the palate (Figure 22–17).
Figure 22–16 Café au lait melanotic patch.Figure 22–14 Smoker’s melanosis.
Figure 22–13 Brown hairy tongue.
Figure 22–15 Oral melanotic pigmentation in Addison disease.
oral macular pigmentations that appear around themouth and on the fingers (Figure 22–19). When theselesions are encountered, the patient should be ques-tioned about any gastrointestinal complaints and a fam-ily history of polyps. No treatment is necessary.
Suggested reading
Barrett AW, Bennett JH, Speight PM. A clinicopathological andimmunohistochemical analysis of primary oral mucosalmelanoma. Eur J Cancer Oral Oncol 1995;31:100–5.
Buchner A, Leider AS, Carpenter WM, Littner MM.Melanocytic nevi of the oral mucosa: a clinicopathologicstudy of 60 new cases. Refu Hashinayim 1990;8:3–8.
Buchner A, Leider AS, Merrell PW, Carpenter WM. Melano-cytic nevi of the oral mucosa: a clinicopathologic study of130 cases from northern California. J Oral Pathol Med1990;19:197–201.
Doval DC, Rao CR, Saitha KS, et al. Malignant melanoma ofthe oral cavity: report of 14 cases from a regional cancercentre. Eur J Surg Oncol 1996;22:245–9.
Eisen D, Hakim MD. Minocycline-induced pigmentation.Incidence, prevention, and management. Drug Saf 1998;18:431–40.
Eisen D, Voorhees JJ. Oral melanoma and other pigmentedlesions of the oral cavity. J Am Acad Dermatol 1991;24:527–37.
Gorsky M, Epstein JB. Melanoma arising from the mucosalsurfaces of the head and neck. Oral Surg Oral Med OralPathol Oral Radiol Endod 1998;86:715–9.
Heine BT, Drummond JF, Damm DD, Heine RD 2nd. Bilateraloral melanoacanthoma. Gen Dent 1996;44:451–2.
Kaugars GE, Heise AP, Riley WT, et al. Oral melanotic macules.A review of 353 cases. Oral Surg Oral Med Oral Pathol1993;76:59–61.
Kitagawa S, Townsend BL, Hebert AA. Peutz-Jeghers syn-drome. Dermatol Clin 1995;13:127–33.
Moghadam BK, Gier RE. Melanin pigmentation disorders ofthe skin and oral mucosa. Compendium 1991;12:14,16–20.
226 C H A P T E R 2 2
Melasma, chloasmaMelasma, the so-called mask of pregnancy, is a pigmen-tary lesion of the facial skin that occurs in the thirdtrimester. Chloasma is clinically identical, yet occurs inpatients taking birth control pills. These basilarmelanoses of the skin may also involve the lips, indeed,perioral and periorbital diffuse brown macular pigmen-tations are the hallmark of these two conditions (Figure22–18). Following delivery and upon cessation of birth-control administration, the cutaneous lesions slowlyinvolute. Their genesis is probabably related to hor-monal changes that affect melanosome stimulation.
Peutz-Jeghers syndromeHereditary intestinal polyposis syndromes are variable,some leading to colorectal carcinoma. The polypsencountered in the Peutz-Jeghers syndrome are hamar-tomatous and do not have a propensity for malignanttransformation, although these patients may alsodevelop adenomatous polyps that may indeed undergocarcinomatous change. There are numerous small peri-
Figure 22–19 Perioral melanotic macules in Peutz-Jeghers syndrome.
Figure 22–18 Chloasma presenting with perioral pigmentation in awoman who takes the birth control pill.
Figure 22–17 Minocycline-induced oral melanosis.

P I G M E N T A T I O N S O F T H E O R A L M U C O S A A N D F A C I A L S K I N 227
Tyler MT, Ficarra G, Silverman S Jr, et al. Malignant acan-thosis nigricans with florid papillary oral lesions. OralSurg Oral Med Oral Pathol Oral Radiol Endod 1996;81:445–9.
WESTOP Group. Oral mucosal melanomas: The WESTOPBanff Workshop Proceedings. Oral Surg Oral Med OralPathol Oral Radiol Endod 1997;83:672–79.
Nandapalan V, Roland NJ, Helliwell TR, et al. Mucosalmelanoma of the head and neck. Clin Otolaryngol 1998;23:107–16.
Ramirez-Amador V, Esquivel-Pedraza L, Caballero-Men-doza E, et al. Oral manifestations as a hallmark of malig-nant acanthosis nigricans. J Oral Pathol Med 1999;28:278–81.











![Enolatos - [DePa] Departamento de Programas …depa.fquim.unam.mx/amyd/archivero/E4_21529.pdf · Estrategias para controlar la selectividad facial Estérica Maximizar la diferencia](https://static.fdocument.org/doc/165x107/5ba53cff09d3f2634c8c8e83/enolatos-depa-departamento-de-programas-depafquimunammxamydarchiveroe421529pdf.jpg)