
Host - parasite interaction reveals inter - and intraspecific variation for Phelipanche species
Upload
horatio-owenCategory
view
215download
0
Campylobacter
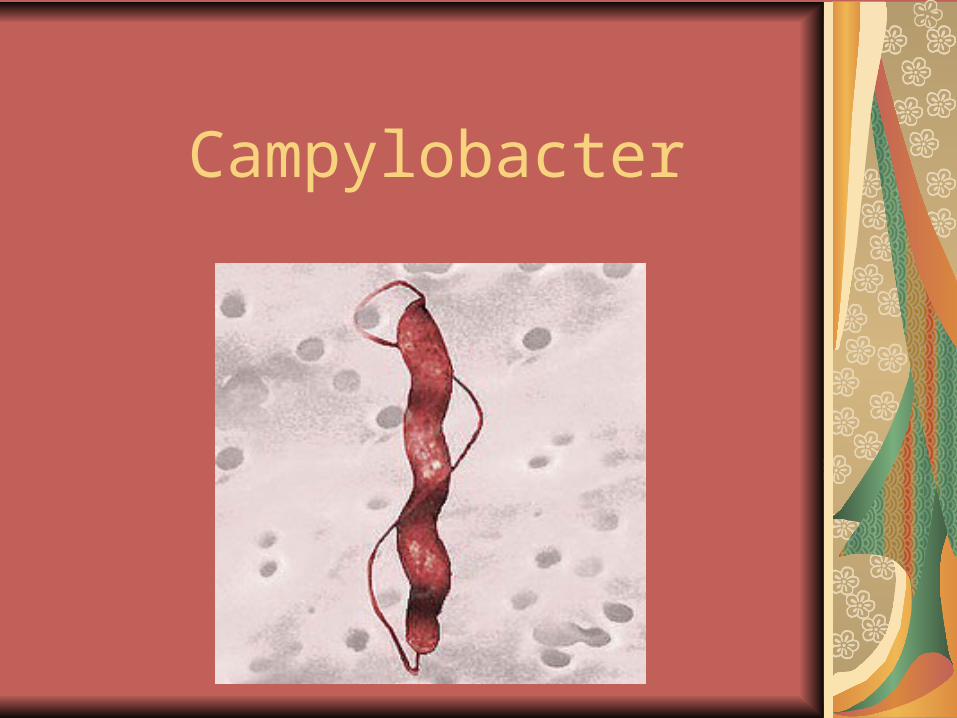
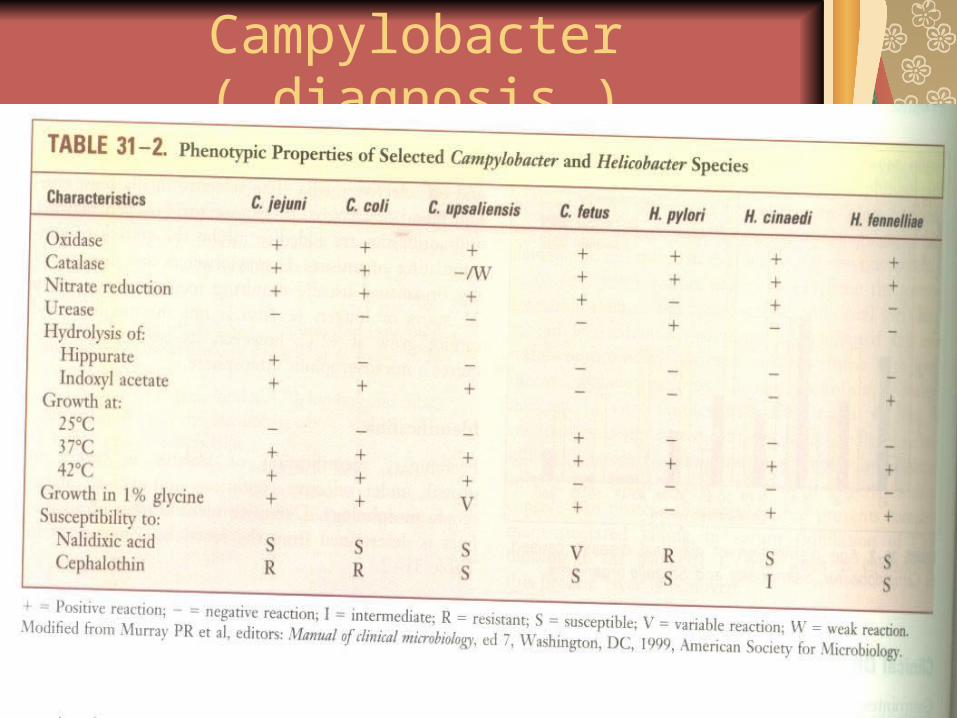
CampylobacterComma shaped ,gram (-) rods,0.2-0.5μm wide ₓ 0.5-5.0 μm
Motile by a polar flagellum
Most species microaerophilic
25 species and 11 subspecies
Different O antigens, heat-labile capsular and flagellar antigens are used for epidemiological classification of clinical isolates
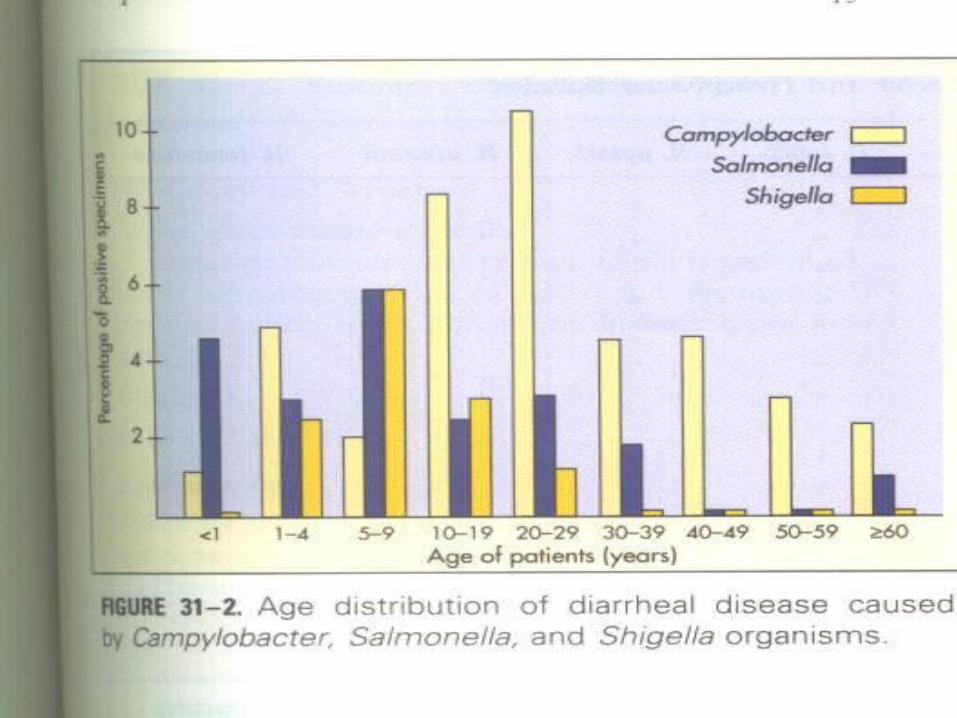
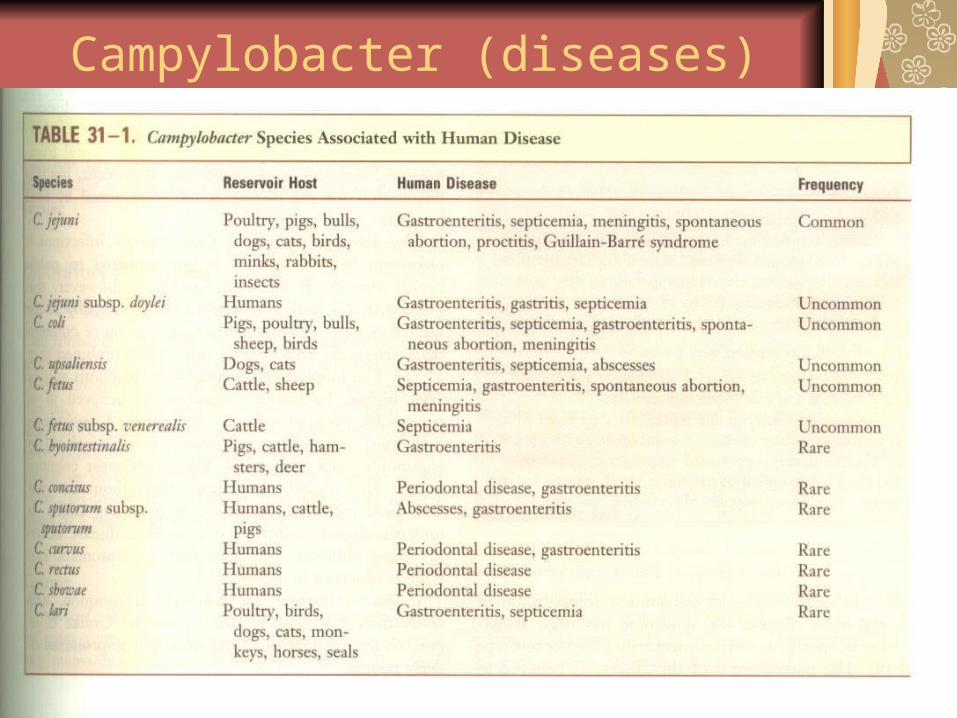
C.jejuni : gastroenteritis
C.coli : gastroenteritis
C.upsalensis: gastroenteritis
C.fetus: systemic infections (bacteremia, septic thrombophlebitis, arthritis, septic abortion, meningitis)
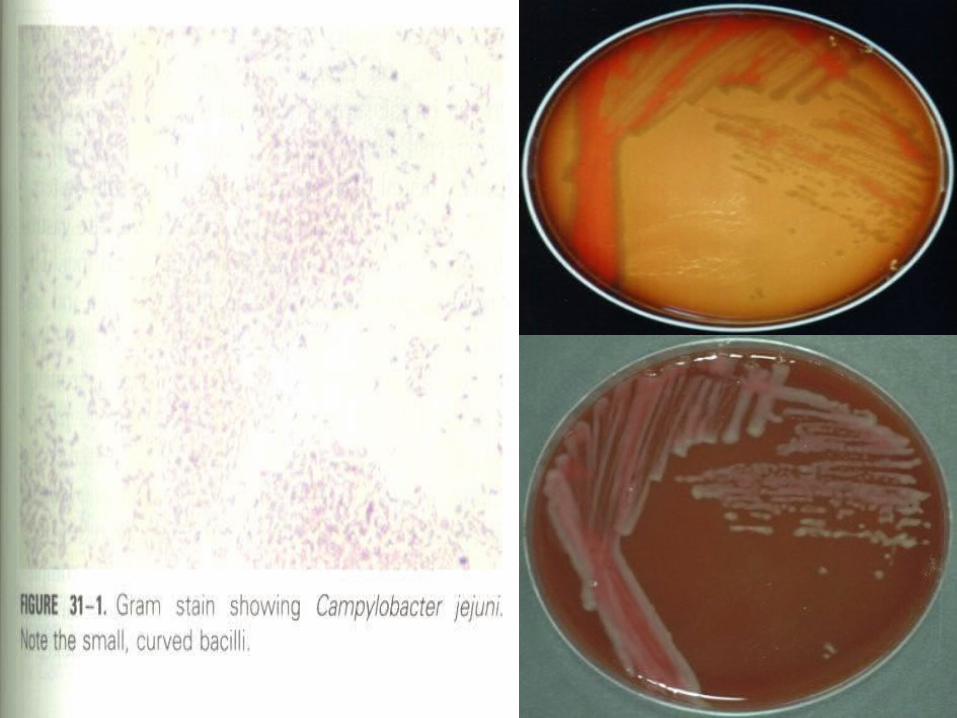
Campylobacter jejuniStructure :Thin ,gram (-) rods with comma , S or gull wings shapes, motile with a single polar flagellum.
Culture: Charcoal or blood (remove toxic oxygen radicals) with antibiotic added media is required grows at 37-42°C in a microaerophilic conditions ( 5%-7% oxygen) and 5%-10%CO2 on selective Skirrow`s medium contains vancomycin ,polymyxin B , and trimethoprim . Colonies are colorless to gray.
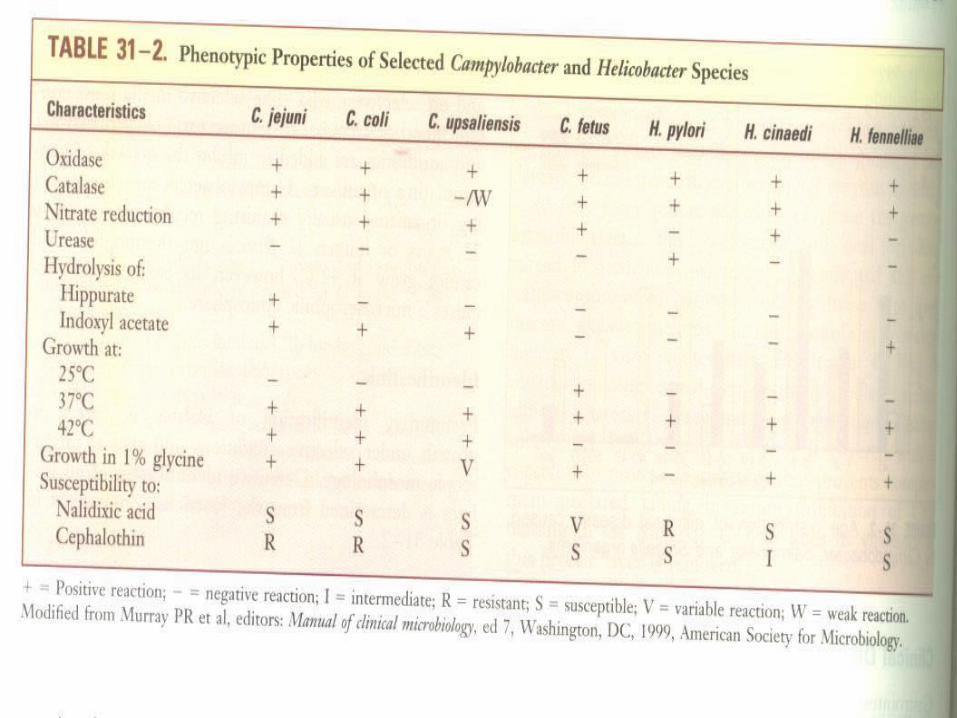
Growth characteristics : oxidase (+), catalase (+)Small size of Campylobacter is used for recovering by filtration of stool specimen ( 0.45 μm filter)Do not oxidize or ferment carbohydrates
Antigenic structure : LPS , enterotoxins

Campylobacter (Virulence)cytotoxic enzymes , enterotoxins, adhesins are detectedFactors that regulate adhesion, motility and invasion into intestinal mucosa are poorly defined.
Guillain – Barre syndrome believed to be an autoimmune disorder of the peripheral nervous system characterized by development of symmetrical weakness over several days and recovery requiring months . caused by antigenic cross-reactivity between oligosaccharides in bacterial capsule and glycosphingolipids on surface of peripheral nerve gangliosidesReactive arthritis: immune-related late complication ; painful joint swelling that may last for weeks to a year
Campylobacter jejuniPathogenesis : Is acquired by the oral from food, drink or contact with infected animals and animal products.Is susceptible to acids, 100-500 organisms is need for infection. Risk of disease is influenced by infectious dose. Patient`s immune status affects the severity of diseasePatients with hypogammaglobulinemia have prolonged , severe disease
Campylobacter jejuni(Pathogenesis)
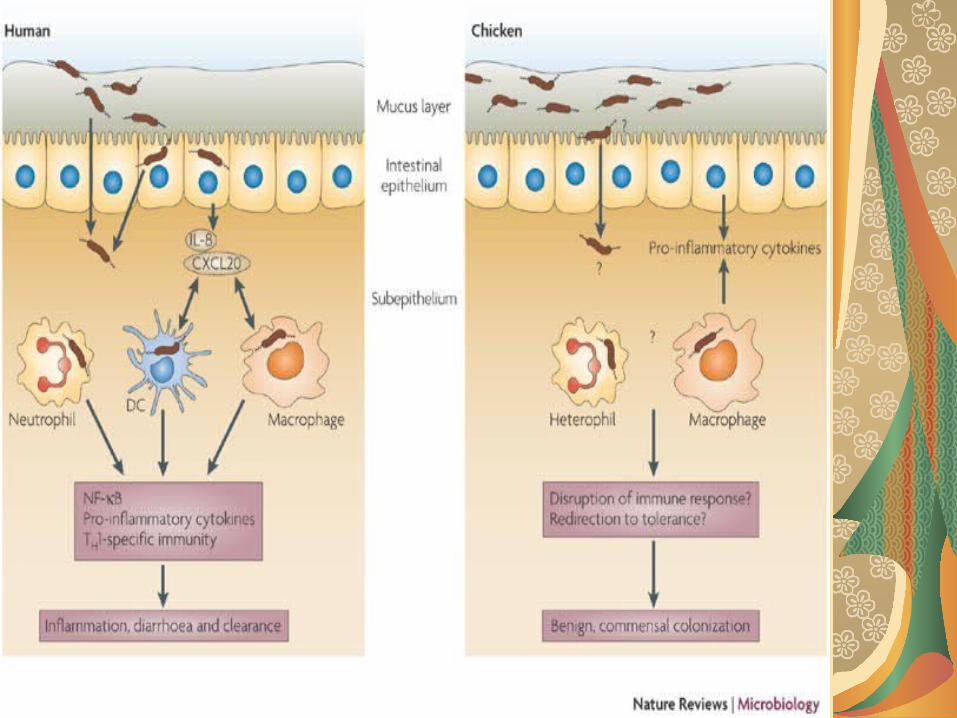
Multiply in the small intestine, invade the epithelium, produce inflammation.
Mucosal surface appears: - ulcerated, edematous, bloody - crypt abscesses in epithelial glands - infiltration of the lamina propria with
neuthrophils, mononuclear cells, and eosinophils
Campylobacterjejuni(Pathogenesis)
Gastrointestinal disease produces histologic damage to the mucosal surfaces of the jejunum, ileum, colonRarely , the bloodstream is invaded (like enteric fever) (1.5/1000)Role of cytopathic toxins, enterotoxins and endotoxic activity have not been definedAre killed rapidly by complement and antibody- mediated serum killing
Campylobacter( epidemiology)
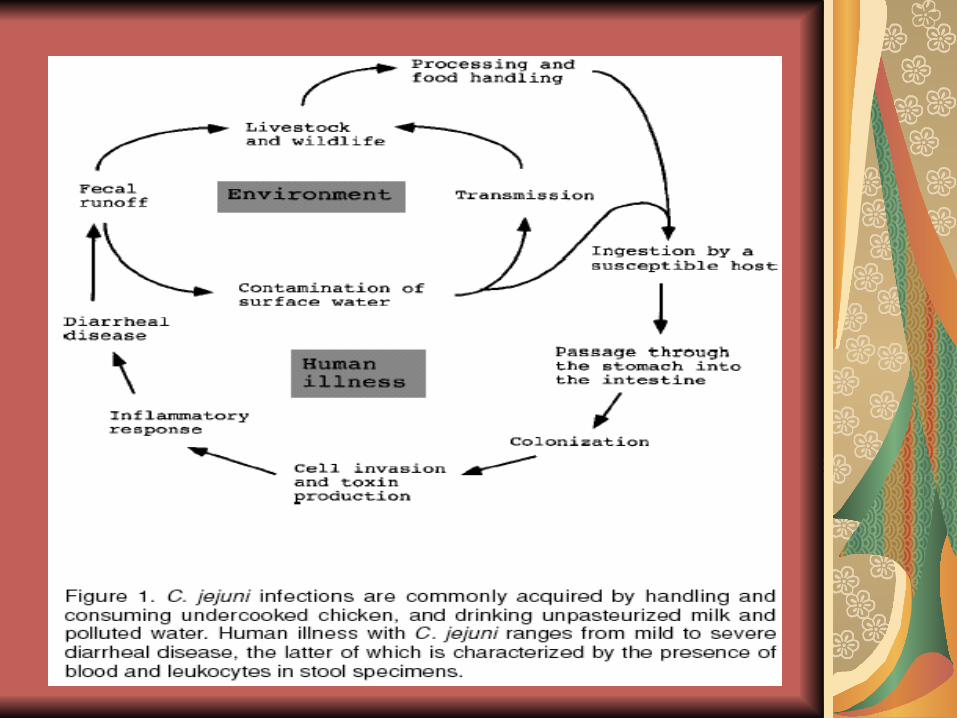
Zoonotic infection ; improperly prepared poultry is a common source of human infections
Infections acquired by ingestion of contaminated food (poultry), unpasteurized milk, or contaminated water
person- to- person (fecal-oral) spread is unusual
Worldwide distribution, with enteric infections most commonly seen in warm months.
Campylobacter (diseases)
Campylobacter jejuni(diseases)Acute enteritis with diarrhea, malaise, fever, and abdominal pain. More than10 bowel movement per day , bloody stools
Most infections are self-limited but can persist for a week or more
Colitis, abdominal pain mimicking acute appedicitis, bacteremia
Chronic enteric infection develop in immunocompromised patients (AIDS) and difficult to treat.
Extraintestinal infections are uncommonComplications:
- C.jejuni ( serotype O:19)and C.upsalensis are associated with Guillain-Barre syndrome(1/1000)
- reactive arthritis
Campylobacter jejuni(Diagnosis)Specimens :stool
smears: typical “gull wing “shaped rod in Gram strain ,Darkfield ,phase contrast microscopy
Culture :requires use of selective media ( Skirrow ) or incubated in 5-10 CO2 (5-7% O2 , microaerophilic condition) and 42 °C ; requires incubation for 2 or more days.
Identification: catalase (+). Oxidase(+)
Campylobacter ( diagnosis )
Campylobacter jejuni(Diagnosis)
Antigen detection: immunoassay detection of C.jejuni and C.coli
Sensitivity 80%-90% , specificity >95%
Antibody detection: serologic testing for IgM and IgG are useful for epidemiological survays
Campylobacter ( treatment, prevention ,and control)
Treatment : for gastroenteritis , infection is self-limited and is managed by fluid and electrolyte replacementServe gastroenteritis and septicemia are treated with erythromycin, azithromycin (drugs of choice) , tetracycline, clindamycin, amoxiclave, imipenem, or fluoroquinolones.More strains are resistant to penicillin, cephalosporins and sulfanamide
Prevention: Gastroenteritis is prevented by proper preparation of food and consumption of pasteurized milk; preventing contamination of water supplies also controls infection.
Campylobacter fetusC.fetus is associated with septicemia and is disseminated to multiple organs and causes diarrhea (uncommon disease)
Spread from the gastrointestinal tract to the blood and distal foci.
Spread is common in debilitated and immunocompromised patients (liver disease, diabetes mellitus, chronic alcoholism, malignancies)
S protein (heat-stable S layer) in C.fetus inhibits C3b binding and subsequent complement and antibody -mediated phagocytosis and killing (resistant to serum killing)
Campylobacter fetus
Diseases: - intravascular infections
(septicemia, endocarditis, septic thrombophlebitis)
- extraintestinal infections (meningoencephalitis, abscesses)
Diagnosis: like C. jejuni, but cannot grow at 42 C
C.upsalensisCatalase (-) or weakly (+).
Growths at 42C
Highly susceptible to drugs in selective media (skirrow )
Filter method is suitable for isolation
Domestic pets and cats are reservoir
Opportunistic agent of infections in children
Present as acute enteritis with diarrhea , fever and abdominal pain
Isolates from stool, blood , fetoplasental material of human
Is associated with Guillain-Barre syndrome

Arcobacter
Arcobacter The genus Arcobacter which is related to Campylobacter was introduced in 1991.
Are aerotolerant
Optimal growth temperature is at 30oC.
Members of this genus inhabit very diverse environments
Distinguishing from Campylobacter:
- Hydrolysis of indoxyl acetate
- growth at 15-36◦ C ,but not at 42◦ C
- Inability to hydrolyze hippurate
• separated to 5 major groups:
A.cryaerophilus (2 subgroups)
A.nitrofigilis
A.butzleri
A.skirrowii
A. halophilus
ArcobacterA.cryaerophilus: grows well under aerobic conditions. May require microaerophilic conditions for initial isolation
Optimal growth at 30◦ C
Resemble C.fetus but is Indoxyl acetate (+)
Sensitive to nalidixic acid, resistant to cephalothin
Growth in CIN agar is better than Skirrow
A. cryaerophilus has been found both in association with diseased as well as healthy humans and animals caused that these bacteria were considered to play a role as food borne or waterborne agents
ArcobacterA.nitrofigilis:
a nitrogen fixing bacterium
a cryophilic species
Grows optimally at 25◦ C
Urea (+)
Non pathogenic for human
A. skirrowii:
isolates from fluids of bulls, aborted fetuses and diarrheal feces from cows , pigs and sheep.
ArcobacterA.butzleri: aerotolerant both at 30◦ C and 36◦C ( separatation from A. cryaerophilus )
Grows on MacConkey and glycine and nitrate containing media and in 1.5% and 3.5% NaCl
Isolated from stools of patients with diarrheal illness.
Rarely isolates from abdominal contents , peritoneal fluid and blood

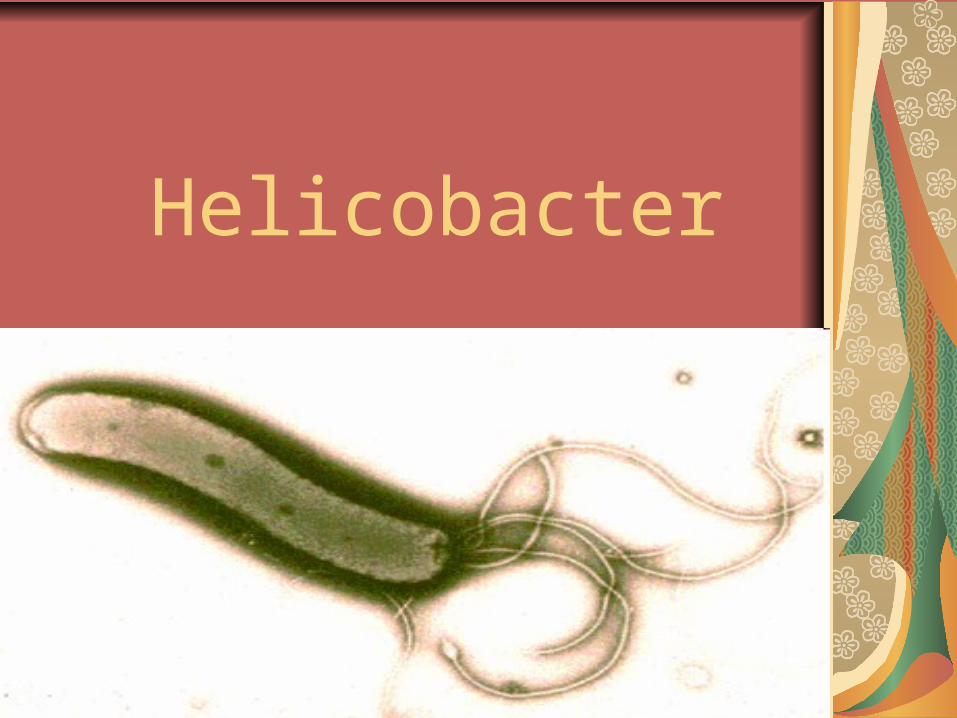
Helicobacter
HelicobacterFirst isolated by Marshal and Warren in1983
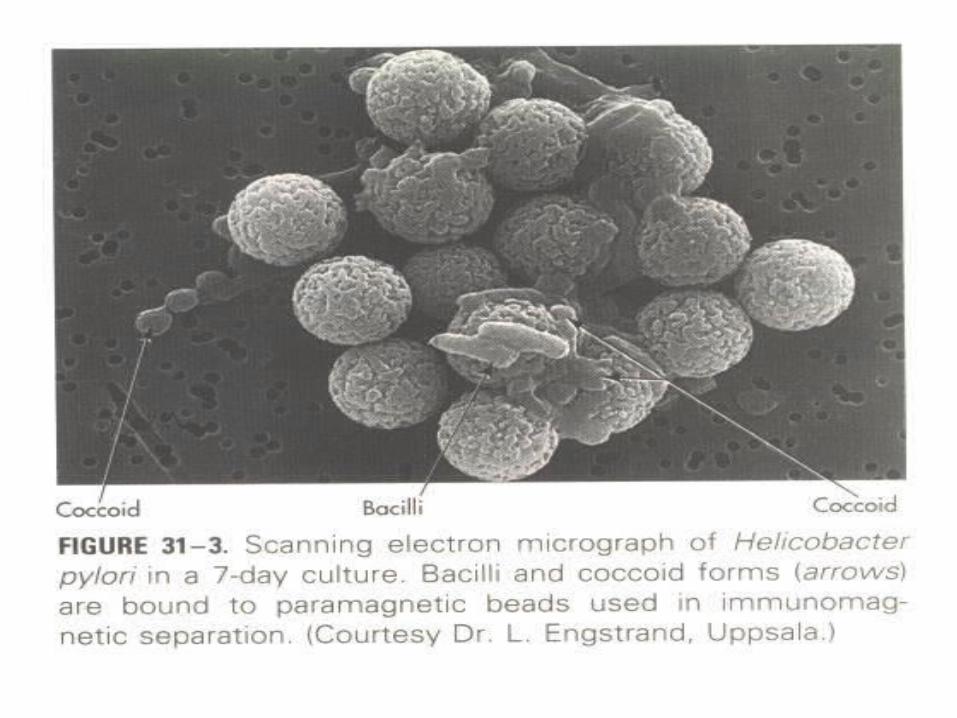
Spiral , G(-) rods resembling campylobacter (0.5-1.0μm wide*2-4 μm long) , coccoid form in older cultures
Motile (polar flagella)
catalase and oxidase (+)
- 30 species are characterized according to:
sequence analysis of their 16S rRNA genes
cellular fatty acid , (different from Campylobacter with high % of O:14 and low O:16 and presence of O:18-OH-3)
presence of polar flagella
Helicobacter ( diseases) H.pylori : (gastric)
Gastritis , peptic ulcer, gastric adenocarcinoma, gastric mucosa-associated lymphoid tissue (MALT) B-cell lymphomasH.cinaedi: enterohepatic (isolated from homosexual men with HIV)
Gastroenteritis, septicemia, proctocolitis, cellulitis H.fennelliae : enterohepatic(isolated from homosexual men with HIV)
Gastroenteritis, septicemia, proctocolitis Helicobacter species flexispira taxon 8:
bactermia with cellulitis in immunocompromised patients H.canadensis : GastroenteritisH.canis:GastroenteritisH.pullorum:Gastroenteritis
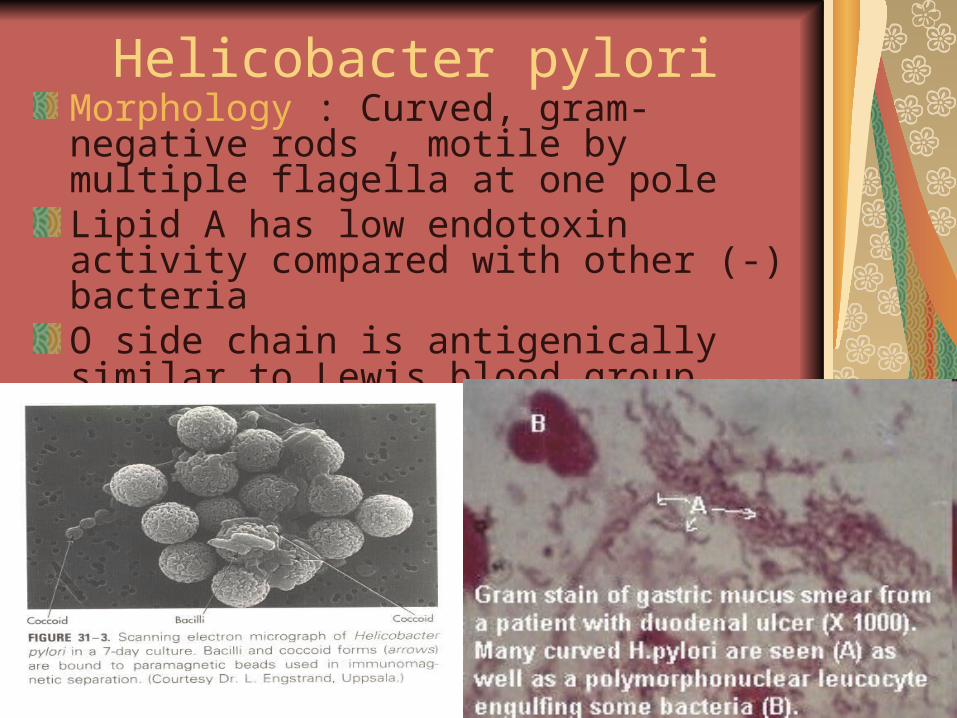
Helicobacter pyloriMorphology : Curved, gram- negative rods , motile by multiple flagella at one pole Lipid A has low endotoxin activity compared with other (-) bacteriaO side chain is antigenically similar to Lewis blood group antigens, which may protect the bacteria from immune clearance
H.pyloriCulture: require complex medium supplemented with 5% defibrinated horse or sheep blood, serum, charcoal, starch, egg yolk( Brucella agar ,BHI,or TSB mediums with supplements and antibiotics ) .Microaerophilic conditions( 10% CO2, 5% O2 and 85% N2 or 10%CO2 with air ). Grows in 3-6 days at 37°C in a microaerophilic environment in Skirrow`s medium with vancomycin, polymyxin B and trimethoprim ; and in chocolate medium
H.pyloriGrowth characteristics : oxidase- positive , catalase-positive, do not ferment or oxidase carbohydrates, metabolize amino acids by fermentative pathways
-Urease production at very high levels is typical of gastric helicobacters, and uncommon in intestinal helicobacters
- Flagella and urease are important for survival in gastric acids and rapid movement through the viscous mucus layer towards a natural pH environment
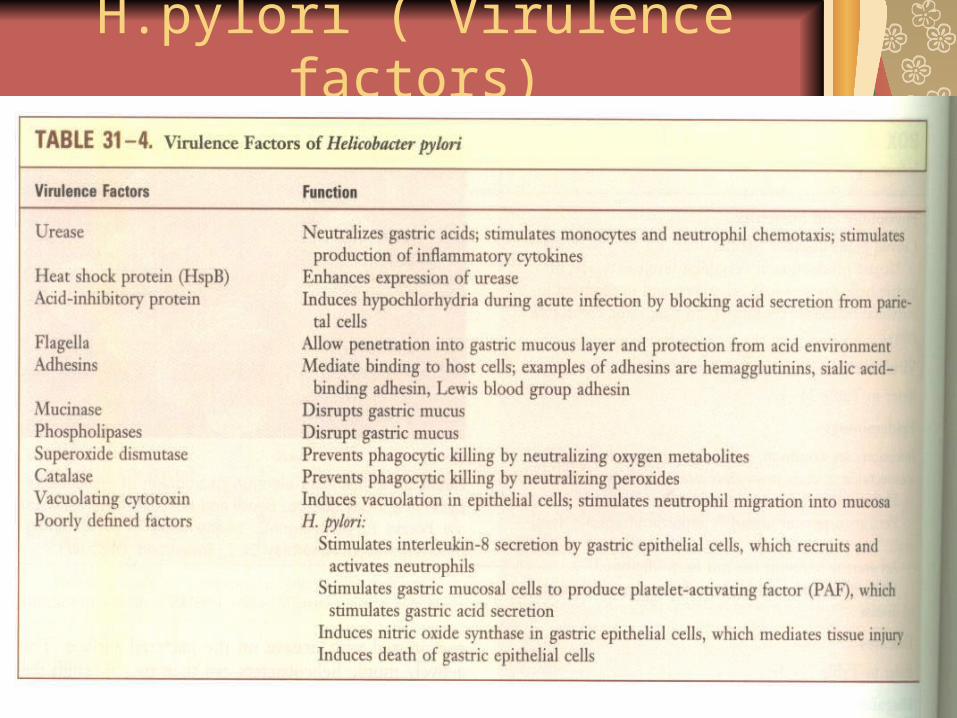
H.pylori ( Virulence factors)
H.pylori (pathogenesis)Virulence factors: A-Initial colonization of H.pylori facilitate by:
1- blockage of acid production by acid inhibitory protein
2- Urease activity ; - neutralization of gastric acids by production of
the ammonia - stimulate monocytes and neuthrophils
chemotaxis - stimulate production of inflammatory cytokines - stimulate production of high amount of gastrin
and acid
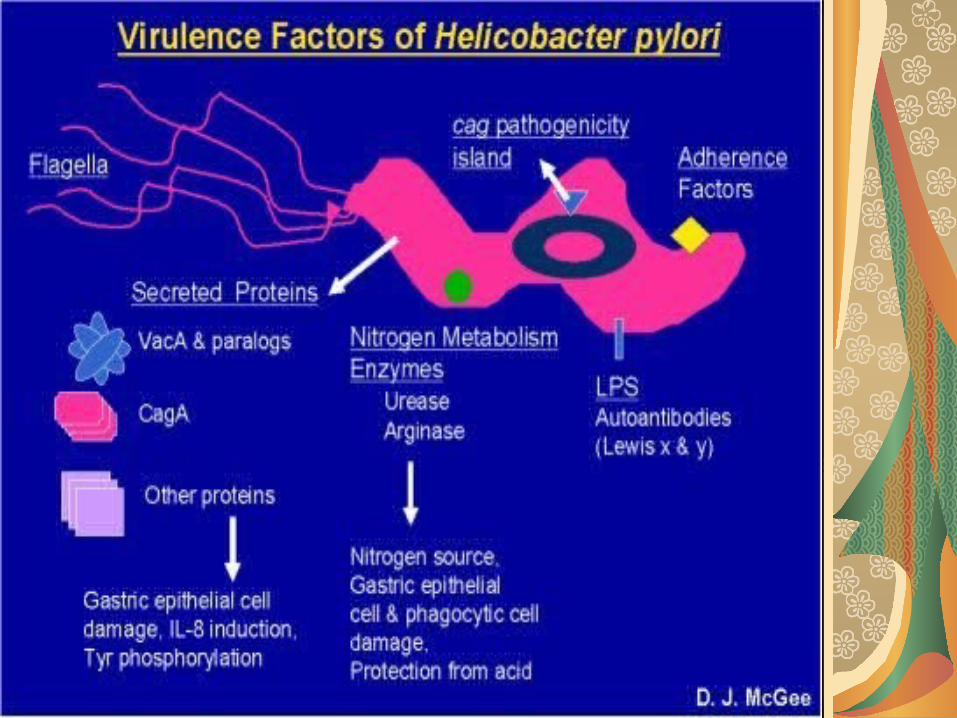
H.pylori (pathogenesis)B- H.pylori can pass through the gastric mucus by actively motility of flagella
C- adhere to the gastric epithelial cells by multiple surface-adhesion proteins
- haemagglutinins ; binding to N-acetyl-noraminil-lactose
- sialic acid- binding adhesin - pili; adhere to phosphatidyl-ethanol amin and
laminin - Lewis blood group adhesin; may protect the
bacteria from immune clearance Surface proteins can also bind host proteins and
help the bacteria evade immune detection.
H.pylori (pathogenesis)D- Localized tissue damage is mediated by:
1- Urease byproducts 2-Mucinase; disrupts gastric mucus 3-Phospholipases; C,A1,A2 ; disrupts gastric
mucus 4-Vacuolating cytotoxin A (VacA); after
endocytosis by epithelial cells, damage the cells by producing vacuoles
- 60% of H.pylori strains produces Vac A but toxin production is not seen in strains of Patient with long time non-ulcerative gastritis
H.pylori (pathogenesis)E- Cag A protein ; interferes with the normal cytoskeletal structure of the epithelial cells
- an important virulence factor of H.pylori is the Cytotoxin-associated gene (cagA) that resides on a pathogenicity island containing approximately 30 genes.
- These genes encode a structural (type IV secretion system) that acts like a syringe to inject the Cag A protein into the host epithelial cellThe cag PAI (phosphoribosylanthranilate isomerase) genes also induce IL-8 production, which attracts neutrophils.Release of proteases and reactive oxygen molecules by the neuthrophils is believed to contribute to gastritis and gastric ulcers
H.pylori (pathogenesis)F- Superoxide dismutase; prevent phagocyting killing by neutralizing oxygen metabolitesCatalase; prevent phagocyting killing by neutralizing oxygen peroxidesHeat- shock proteins; enhances expression of urease
H.pylori (pathogenesis)
Long life colonization in the antrum of stomach of untreated humansGrows at pH = 6-7 Gastric mucus is impermeable to acid and has a buffering capacity.On the lumen side of the mucus pH is low (1-2) ;on the epithelial side pH is about 7.4H.pylori produces a protease urease activity produces ammoniaTNF-α, IL-6 and IL-8 , urease activity and cytokines are caused Chronic inflammation of stomach
H.pylori (pathogenesis)
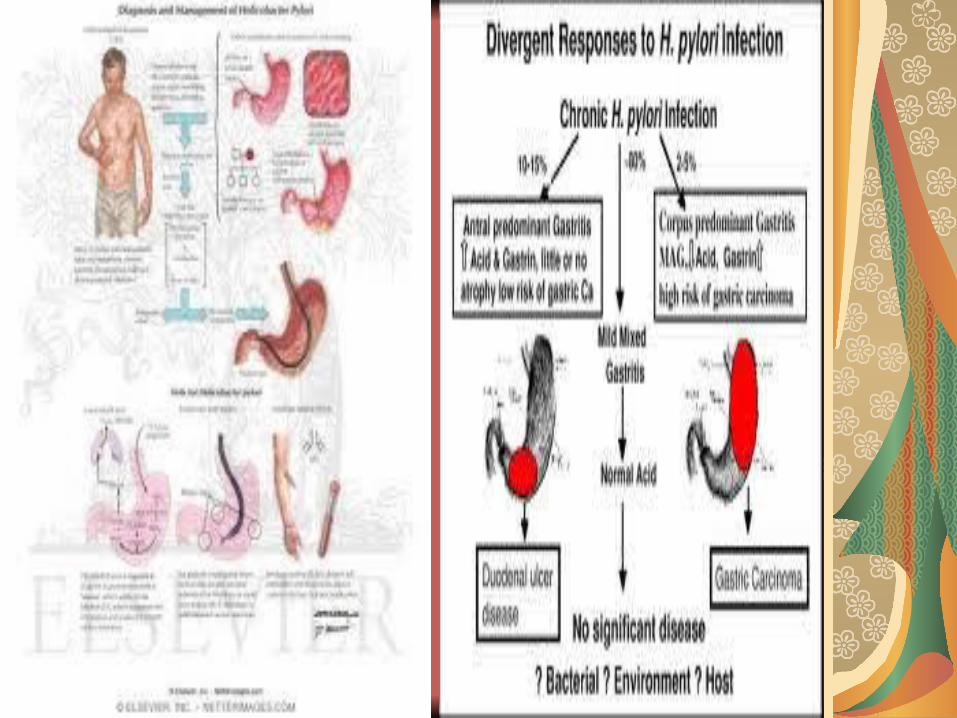
H.pylori infection (weeks to months) chronic superficial gastritis ( years to decades )
- peptic ulcer disease;
- chronic superficial gastritis;
- chronic atrophic gastritis gastric adenocarcinoma
H.pylori ( epidemiology)Infections are common, particularly in people in a low socioeconomic class or in developing nations (70%-90%)
Humans are the primary reservoir; Incidence of carriage in developing nations (70%-90%) most before age 10 years.
Person-to-person spread is important (typically fecal-oral)
is worldwide with no seasonal incidence of disease
70%-100% of patients with gastritis, gastric ulcer, duodenal ulcers are infected with H.pylori
Colonization with H.pylori appears to offer protection from gastroesophagal reflux disease and adenocarcinoma of the lower esophagus and gastric cardia
Diseases Gastritis ; infiltration of neutrophils and mononuclear cells in to gastric mucosa.
Acute phase: feeling of fullness; nausea; vomiting; hypochlorhydria ( decreased acid production );
Chronic phase: disease confined to the gastric antrum in individuals with normal acid secretion, or involve the entire stomach (pangastritis) if acid secretion is suppressed.
Diseases
Peptic ulcer (10-15%) in chronic gastritis. Developing to gastric ulcer (isolate 85%) or duodenal ulcer(isolate 95%)
Gastric cancer; replacement of normal gastric mucosa with fibrosis and proliferation of the epithelium in chronic gastritis. (high risk for cancer is associated with cagA positive strains and high levels of IL-1 production)
MALT lymphoma; monoclonal population of B cells
H.pylori(Diagnosis)
Microscopy : Histological examination of biopsy specimen is sensitive and specific; hematoxylin-eosin stain, Gram stain Warthin-Starry silver stain( 100% sensitivity and specificity)
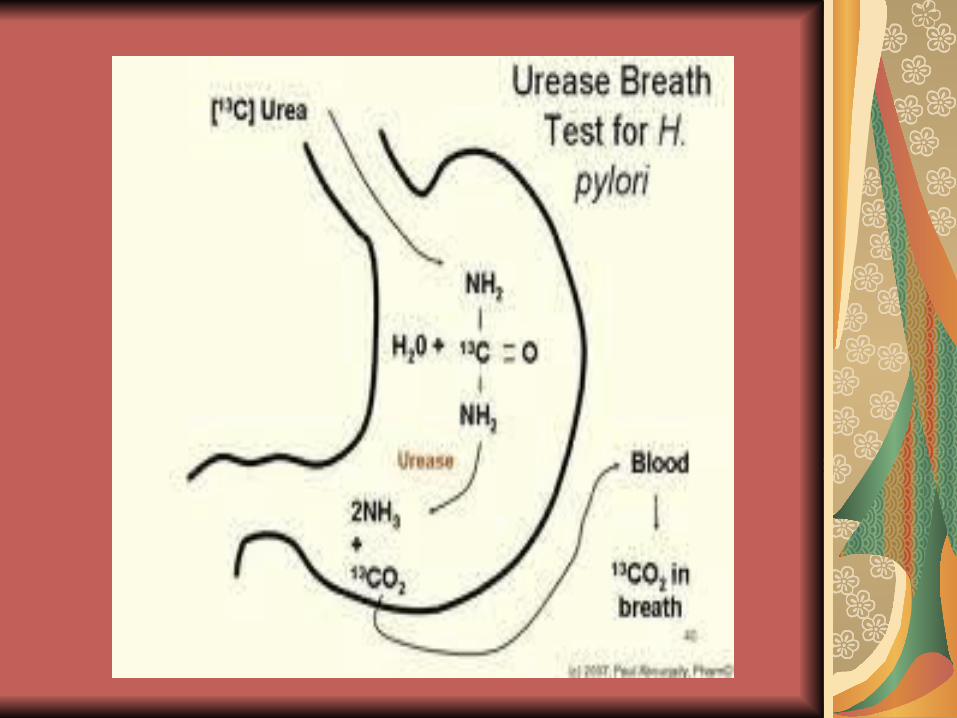
Urease test: relatively sensitive and highly specific; urea breath test is a noninvasive test (detection in 1-2 hours with sen. 75-95%and spe. 100%)Noninvasive urease testing of human breath: C13 or C14 labeled urea solution ( excellent spe. and sen.)
H.pylori(Diagnosis)
H.pylori antigen test : polyclonal and monoclonal immunoassays for H.pylori antigens; performs with stool specimens; sensitive and specific 95%;
Serology: useful for demonstrating exposure to H.pylori .IgM disappears rapidly. IgA and IgG persist for months to years
H.pylori(Diagnosis)Culture : requires incubation in microaerophilic condition ; chocolate agar (nonspecific medium) and modified Skirrow medium (specific medium) are required ; growth is slow (up to 2 weeks) ; relatively insensitive unless multiple biopsies are culturedIdentification; microscopic morphology, oxidase , catalase, urease
Nucleic-Acid based amplification tests: PCR based tests are restricted to research labs and not in clinical use
.
H.pylori ( treatment) Treatment : multiple regimens have been evaluated for treatment of H.pylori infections.
Combined therapy with tetracycline, metronidazole, bismuth, and omperazole for 2 weeks has had high success rateOmperasole + a macrolide (clarithromycin ) a beta-lactam(amoxicillin) for 7-10 days . resistance to clarithromycin and metronidasole is important.( susceptibility testing is recommended)
Prophylactic treatment of colonized individuals has not been useful and potentially has adverse effects, such as predisposing patients to adenocarcinomas of the lower esophagus
prevention and controlHuman vaccines are not currently available
Use of H.pylori antigens in experimental vaccines that stimulate TH1 cells leads to enhanced inflammation
Use of antigens in combination with mucosal adjuvants that induce aTH2 cell response is protective in an animal model
Other Helicobacters ( diseases) H.cinaedi: enterohepatic (isolated from homosexual men with HIV)
Gastroenteritis, septicemia, proctocolitis, cellulitis H.fennelliae : enterohepatic (isolated from homosexual men with HIV)
Gastroenteritis, septicemia, proctocolitis Helicobacter species flexispira taxon 8:
bactermia with cellulitis in immunocompromised patients H.canadensis : GastroenteritisH.canis: GastroenteritisH.pullorum: Gastroenteritis









![ENDANGERED SPECIES ['m ʌ ηki] ['elifənt] [məs'ki:tou]](https://static.fdocument.org/doc/165x107/56649e055503460f94af1718/endangered-species-m-ki-elifnt-mskitou.jpg)


![Name Product Code Host Principal name Expected species ... · Bulk Product List Q1.2015.html[31/03/2015 14:47:12] Company Name Product Code Host Principal name Expected species cross-reactivity](https://static.fdocument.org/doc/165x107/5adc76277f8b9a8b6d8b9273/name-product-code-host-principal-name-expected-species-product-list-q12015html31032015.jpg)


